Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Antibodies Targeting Gasdermin E as a Potential Therapeutic Option for Psoriasis – A Pilot Study on a Mouse Model
Authors Nowowiejska-Purpurowicz J, Hermanowicz JM, Pawlak D ![]() , Flisiak I
, Flisiak I ![]() , Lipinski T
, Lipinski T
Received 14 September 2025
Accepted for publication 25 November 2025
Published 18 December 2025 Volume 2025:15 Pages 561—567
DOI https://doi.org/10.2147/PTT.S567601
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mio Nakamura
Julia Nowowiejska-Purpurowicz,1 Justyna M Hermanowicz,2 Dariusz Pawlak,2 Iwona Flisiak,1,* Tomasz Lipinski3,*
1Department of Dermatology and Venereology, Medical University of Bialystok, Bialystok, 15-540, Poland; 2Department of Pharmacodynamics, Medical University of Bialystok, Bialystok, 15-222, Poland; 3Lukasiewicz Research Network - PORT Polish Center for Technology Development, Wrocław, 54-066, Poland
*These authors contributed equally to this work
Correspondence: Julia Nowowiejska-Purpurowicz, Department of Dermatology and Venereology, Medical University of Bialystok, Zurawia 14 Street, Bialystok, 15-540, Poland, Email [email protected]
Background: Psoriasis is a frequent and complex dermatosis of uncertain origin. A few years ago, a family of gasdermin proteins was implicated in psoriasis pathogenesis. Although the number of therapeutic options for psoriasis is growing, considering the burden of the disease, treatment personalization, and the possibility of side effects or loss of the drug’s efficacy, it is important to seek new therapeutic targets.
Objective: The aim of this study was to assess the efficacy of antibodies against gasdermin E (GSDME) in the treatment of psoriatic lesions.
Methods: The study involved 30 male BALB/c mice, 8 weeks old. 5% imiquimod cream was applied topically on the skin to induce psoriatic lesions. The next day after the psoriatic lesions appeared, the antibodies were administered. Mice from the study group received the rabbit polyclonal anti-GSDME antibody intravenously or intraperitoneally. The control group was administered sterile 0.9% saline solution.
Results: The injection of anti-GSDME antibodies to mice with imiquimod-induced psoriasis resulted in the resolution of skin lesions, whereas the injection of saline to the control group did not result in significant changes.
Conclusion: Antibodies targeting GSDME seem to be promising therapeutic agents in psoriasis; however, their utility has to be confirmed in future studies.
Plain Language Summary: Psoriasis is a frequent and incurable skin disease that affects approximately 125 million people worldwide. It is characterized by chronic inflammation, wide comorbidity, and decreased life expectancy. The study was carried out by authorized personnel in the Experimental Medicine Center, Medical University of Bialystok, Poland. The aim of the study was to look for a new medication for psoriasis and test the utility of antibodies that bind a protein called gasdermin E (GSDME), and hence, inhibit GSDME’s role in psoriasis. This is a pre-clinical experiment on 30 mice with psoriasis, which was previously induced by a cream with imiquimod. Subsequently, 20 mice received a polyclonal rabbit anti-GSDME antibody, which was injected intravenously and intraperitoneally, whereas 10 mice received saline solution (no active compound). The injection of an antibody against GSDME to mice with imiquimod-induced psoriasis lead to the resolution of skin lesions, whereas mice that received saline solution did not heal. Antibodies targeting GSDME seem to be a promising future medication in psoriasis.
Keywords: psoriasis, gasdermin, gasdermin E, GSDME, mouse model, antibody
Introduction
Psoriasis is a common and incurable skin disease that affects approximately 125 million people worldwide and significantly reduces patients’ quality of life.1 It is characterized by chronic inflammation, extensive comorbidities, and decreased life expectancy.1 Among several clinical variants, plaque psoriasis is the most frequent, and clinically presents as erythematous-scaly plaques located particularly on extensor surfaces of elbows, knees, in the intragluteal fold or scalp.1 Therapy of psoriasis includes topical medications, phototherapy, oral classic agents, and biological drugs.1 Although the number of therapeutic options for psoriasis is increasing, the disease burden, need for treatment personalization, and challenges such as side effects or loss of drug efficacy highlight the importance of identifying new therapeutic targets.
In general, psoriasis pathogenesis encompasses the interplay between genetic, environmental, and immunological factors.1 Our team has studied plaque psoriasis pathogenesis for many years. We previously proposed a role of the gasdermin (GSDM) protein family in psoriasis pathogenesis. Gasdermins comprise a family of six proteins labeled A through F. The first five (A-E) share a common molecular structure, consisting of an N-terminal domain, a central linker region, and a C-terminal domain. This configuration allows the proteins to remain inactive or become activated, leading to the formation of pores in the cell membrane. Research has demonstrated that the activation of all gasdermin family members requires cleavage by enzymes such as caspases or granzymes, resulting in the release of the N-terminal portion responsible for forming membrane pores that ultimately trigger a type of programmed cell death called pyroptosis.2,3 Gasdermins can be activated by various triggers under different circumstances and contribute to the pathogenesis of numerous human disorders, including skin diseases.3
First, we conducted a study on patients with plaque psoriasis, analyzing the serum and urinary concentration of five gasdermins A-E, which exhibit relatively similar molecular structures. We also analyzed their expression in the psoriatic plaques, unlesional patients’ skin, and healthy skin from controls without dermatoses. Our published results4–8 demonstrated significantly higher serum concentration of gasdermins A, B, C and E in psoriatic patients compared to subjects without dermatoses. Moreover, we observed significantly higher expression of all gasdermins A-E in the psoriatic plaque compared to unlesional patients’ skin, with even greater difference when compared to the healthy skin of controls.4–8
The logical next step was to investigate the potential of antibodies targeting gasdermins as a therapeutic option in psoriasis. To date, there are no drugs specifically targeting gasdermins. We selected GSDME for its pronounced tissue expression level and serum concentration in psoriatic patients over controls in comparison to other gasdermins. Hereby, we present the results of our pilot study on the therapeutic potential of rabbit polyclonal anti-GSDME antibodies in a mouse model of psoriasis.
Methods
The study was carried out in accordance with the EU Directive 2010/63/EU for animal experiments by authorized personnel in the Experimental Medicine Center, Medical University of Bialystok, Poland.
Mice
Thirty male BALB/c mice, aged 8 weeks, were used in the study. They were randomly divided into a study group (20 mice) and a control group (10 mice). The study group was further randomly divided into two subgroups, depending on the route of antibody administration.
Experiment Schedule
The experiment began with a 5-day handling period to familiarize mice with the researchers’ hands and consequently reduce the stress level during the experiment procedure. The study was carried out by authorized personnel with appropriate qualifications and professional experience. Mice were weighed weekly throughout the experiment.
Psoriasis was induced immediately after the handling period. Mice were anesthetized with inhaled isoflurane and then shaved on the dorsal surface (area 10 cm2). Subsequently 5% imiquimod cream (Aldara®, 62.5 mg once a day for 10 consecutive days) was applied topically on the previously shaved region to induce psoriatic lesions. The imiquimod-induced psoriasis-like inflammation is the most commonly used mouse model of this dermatosis.9 The model used in this study is based on literature data and our previous experience.
The severity of the skin lesions was assessed using components of the psoriasis area and severity index (PASI). PASI is the most widely used instrument for the evaluation of skin lesions in psoriasis in the dermatological practice.10 The tool originally includes an evaluation of the three types of lesions: erythema, infiltration, and scaling, and their area in four anatomic regions. However, in our experiment, the assessed area was the same in every mouse, as it was the area of induced psoriasis. It was assessed by the same person every time, the primary investigating dermatologist. Each type of lesion was assessed on a scale of 0–4 (the higher the number, the more severe the lesion), and then added up.
On the day following the appearance of psoriatic lesions (day 6 of imiquimod application), antibody administration was conducted. Before injection, mice were anesthetized with inhaled isoflurane. The study group (20 mice total) was divided into two subgroups of 10 mice each: one group received the rabbit polyclonal anti-GSDME antibody (MyBioSource MBS9610022, San Diego, CA, USA) intravenously into the tail vein, and the other received the same antibodies intraperitoneally. The dose injected accounted for 100 μL of antibody solution (1 mg/mL concentration). The control group was administered 100 μL of sterile, room-temperature 0.9% saline solution. The doses were selected based on the data from previous reported experiments on mice.11–13 Imiquimod application was continued until the 10th day.
At the end of the experiments, mice were euthanized by isoflurane overdose (5% concentration). Afterwards, the blood was collected from the right ventricle and basic laboratory parameters were analyzed, including white blood cells (WBC), red blood cells (RBC), platelets (PLT), and hemoglobin (HGB).
Statistical Analysis
The Shapiro–Wilk’s W-test was used to assess data normality. Normally distributed data were analyzed using the Student’s t-test and presented as mean ± SD. Statistical analysis was conducted using GraphPad Prism 10.2.2 software (La Jolla, San Diego, CA, USA). Differences were considered statistically significant at p < 0.05.
Results
Thirty male BALB/c mice were enrolled in the study. Topical application of 5% imiquimod cream successfully induced psoriasis-like lesions in accordance with the results of our previous preliminary experiment, and imiquimod application was continued up to day 10. The skin lesions appeared on the 6th day, and their severity was assessed using components of PASI (Table 1 and Figure 1A–C). Representative photographs of mice from each group at different stages are presented in Figure 1. The mean skin lesion severity score in the study group before treatment was 5.8 ± 0.28 points, and 5.4 ± 0.28 in the control group. The initial difference between the groups was not statistically significant (p > 0.05).
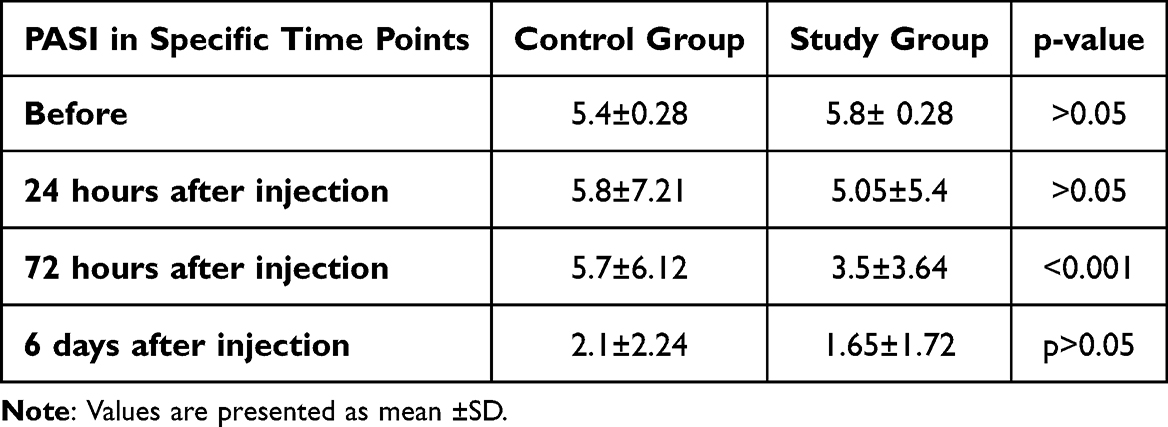 |
Table 1 The Table Illustrates the Mean PASI Values in Mice from the Study and Control Groups in Particular Time Points: Before the Injection of the Antibodies/Saline, 24 Hours After, 72 Hours After the Injection, and Additionally at the End of Experiment, 6 Days After the Injection |
 |
Figure 1 Photographs representing mice during different stages of experiments. Before the treatment (A–C), after 24 hours from the injection (D–F), after 72 hours from the injection (G–I). Study group treated i.v. (A, D, G), study group treated i.p. (B, E, H), control group (C, F, I). |
After the injection of rabbit polyclonal anti-GSDME antibodies (study group) and saline solution (control group), the mice were monitored daily. Skin lesion severity was reassessed after 24 and 72 hours from the injection, and at the end of the experiment: 48 hours after the final imiquimod application (Table 1).
At 24 hours post-administration, the mean PASI score in the study group was 5.05 ± 5.4 compared to 5.8 ± 7.21 points in the control group (Table 1). The difference between the study and control groups was not statistically significant (p > 0.05) (Figures 1D–F and 2A). At 72 hours post-administration, the mean PASI score in the study group was 3.5 ± 3.64, compared to 5.7 ± 6.12 in the control group (Table 1). This difference was statistically significant (p < 0.001) (Figures 1G–I and 2A).
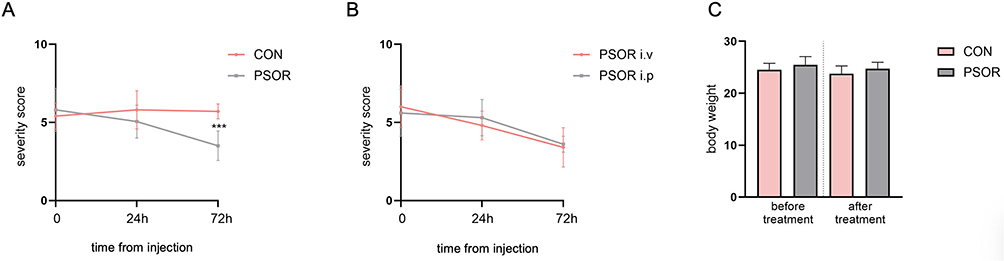 |
Figure 2 Skin lesions severity in mice from the study (PSOR) and control (CON) groups initially, after 24 h and 72 h from the injection (A); skin lesions severity in mice from the study group treated i.v. (PSOR i.v.) or i.p. (PSOR i.p.) (B); body weight of the mice from the study (PSOR) and control (CON) groups before and after the treatment (C). ***mean statistically significant difference between the study and control group with p<0.001. |
When we compared mice from the study group that received antibodies intravenously and intraperitoneally, the severity of skin lesions after 24 hours from the injection in the first group was 4.8 and in the other 5.3, and after 72 hours – 3.4 and 3.6, respectively. The differences were not statistically significant (p > 0.05) (Figure 2B). Similarly, intravenous or intraperitoneal administration of sterile saline in the control group gave statistically insignificant results: 4.8 and 6.8, and 5.5 and 6, respectively.
Additional observations noted that all of the mice exhibited reduced activity and slower movements after imiquimod application. Upon the appearance of skin lesions, mice began scratching. Following the administration of antibodies, mice in the study group regained activity concurrent with the skin healing process. In contrast, mice from the control group, which received no treatment, remained less active until the end of the experiment. No significant changes in their body weight were observed in any group before or after the experiment (Figure 2C).
We also compared the basic laboratory parameters (white blood cells, red blood cells, platelets, hemoglobin) between the study and control groups post-euthanasia, but no significant differences were observed (p > 0.05, data not shown).
Discussion
Our previous studies identified a potential role of the gasdermin protein family in psoriasis. To the best of our knowledge, this study is the first to analyze the role of antibodies targeting gasdermins in a psoriatic inflammation model. The results of the current experiment further encourage the hypothesis that these proteins play a key role in psoriasis pathogenesis and can serve as a therapeutic target.
At the beginning of the experiment, mice in the study and control groups exhibited comparable psoriasis-like skin lesion severity, as assessed by the components of PASI. The skin lesions clearly were a source of discomfort, with mice displaying scratching behavior and reduced activity. Following administration of the rabbit polyclonal anti-GSDME antibodies to the study group and the saline solution to the control group, clear differences emerged. After 24 hours, the lesions in the study group started to heal, whereas lesions in the control group became even more severe. By 72 hours, the study group showed significant improvement in lesion severity (p < 0.001), while the control group remained unchanged. This experiment encourages the potential of anti-GSDME antibody as a therapeutic agent in psoriasis. We assume that the antibody binds GSDME and prevents its function as a pore-forming agent.
GSDME, formerly known as the DFNA5 protein, is implicated in multiple forms of programmed cell death, including pyroptosis, apoptosis, and necroptosis.5,14 GSDME can be cleaved by caspase-3 or by granzyme B, releasing N-terminal domains that form pores in a cell membrane. In consequence, cell swelling and release of cellular components occur. The process leads to the release of inflammatory cytokines such as IL-1β and IL-18 as well as pro-apoptotic molecules, leading to further stimulation of caspase-3.5,14 Moreover, the formation of GSDME-mediated membrane pores can trigger activation of the NLRP3 inflammasome, further promoting IL-1β maturation.5,14
The role of GSDME in psoriasis is emerging, but not fully elucidated yet, and our team was among the first to investigate its role in this dermatosis. We previously proposed a mechanism wherein GSDME, beyond cleavage by granzyme B or caspase-3, indirectly triggers GSDMD cleavage through feedback mechanisms, leading to pyroptosis and inflammatory cytokine release.5,14 Inflammasomes, whose role in psoriasis is well established,15 can activate caspase 1, which transforms pro- IL-1β into mature IL-1β, which has the ability to stimulate secretion of IL-1716 – one of the main psoriatic cytokines. Currently, it has been suggested that pyroptosis, cell death driven by GSDME, is closely linked to apoptosis through the action of caspase 3.17 Our perception is that GSDME-mediated pyroptosis contributes to ongoing inflammation and potentially accounts for the reduction of apoptosis observed in the psoriasis pathogenesis.
Subsequent studies have corroborated our findings. Nevertheless, there is still a paucity of data regarding the role of gasdermins in psoriasis. Additionally, some gasdermins are more frequently studied than others, and, based on our studies and literature review, particular gasdermins may play slightly different roles in this dermatosis. Li et al discovered, similar to us, that GSDME was upregulated in psoriasis lesions compared to normal skin. Moreover, in GSDME-deficient and caspase-3 inhibitor-deficient mice, the severity of skin inflammation was reduced.18 Long et al also carried out an experiment on the imiquimod-induced psoriasis mouse model, and stated that both full-length and cleaved forms of caspase-3 and GSDME were elevated in the epidermis. Abnormal proliferation and differentiation of keratinocytes, as well as skin inflammation, were less pronounced in GSDME-deficient mice.19
In our study, mice receiving anti-GSDME antibodies intravenously showed slightly less severe lesions than those treated intraperitoneally, although the differences were not statistically significant (p > 0.05). Moreover, mice treated intravenously improved faster than those treated intraperitoneally. Notably, treatment with anti-GSDME antibody was well-tolerated and improved the animals’ general condition and reduced pruritus.
Certainly, we must take into account other potential explanations for the therapeutic effect in our study. We should consider the possibility of broader immunomodulation due to non-specific antibody influence, such as binding to several other epitopes or interference with antigen presentation.
The limitations of this experiment include, certainly, its pre-clinical nature, the use of only one psoriatic inflammation model, the administration of a single antibody dose, and no pharmacokinetic assessment or pathology validation.
In further work, we plan to expand this experiment by assessing the efficacy of monoclonal antibodies against GSDME, as well as other gasdermins, including different dosing. Certainly, further experiments are required to fully establish the therapeutic potential of such a strategy.
Conclusions
Gasdermin E seems to play a significant role in psoriasis pathogenesis. Administration of anti-GSDME antibodies to mice with imiquimod-induced psoriasis resulted in skin lesion healing, which encourages further analysis of GSDME as a potential therapeutic target. The observed improvement in skin lesions following antibody administration may suggest effective modulation of the inflammatory cascade driving psoriasis in this mouse model, likely mediated by interrupting processes that lead to the release of key inflammatory cytokines, consequently reducing immune cell infiltration, and normalizing epidermal proliferation.
Ethics
The study was conducted according to EU Directive 2010/63/EU and received the approval of the Animal Bioethics Committee, University of Warmia and Mazury, Olsztyn, Poland, no 49/2024 and 09/P/2025.
Funding
The study was funded by the Medical University of Bialystok, no B.SUB.25.441.
Disclosure
The Authors declare no conflicts of interest in this work.
References
1. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960. doi:10.1001/jama.2020.4006
2. Kovacs SB, Miao EA. Gasdermins: effectors of pyroptosis. Trends Cell Biol. 2017;27:673–684. doi:10.1016/j.tcb.2017.05.005
3. Zou J, Zheng Y, Huang Y, Tang D, Kang R, Chen R. The versatile gasdermin family: their function and roles in diseases. Front Immunol. 2021;12:751533. doi:10.3389/fimmu.2021.751533
4. Nowowiejska J, Baran A, Hermanowicz JM, et al. Gasdermin D (GSDMD) is upregulated in psoriatic skin-a new potential link in the pathogenesis of psoriasis. Int J Mol Sci. 2023;24(17):13047. doi:10.3390/ijms241713047
5. Nowowiejska J, Baran A, Pryczynicz A, et al. Gasdermin E (GSDME)-A new potential marker of psoriasis and its metabolic complications: the first combined study on human serum, urine and tissue. Cells. 2023;12(17):2149. doi:10.3390/cells12172149
6. Nowowiejska J, Baran A, Pryczynicz A, et al. Gasdermin A (GSDMA) tissue expression, serum and urinary concentrations with clinicopathologic outcome in psoriasis. Dermatol Pract Concept. 2024;14(3):e2024177. doi:10.5826/dpc.1403a177
7. Nowowiejska J, Baran A, Pryczynicz A, et al. Gasdermin B (GSDMB) in psoriatic patients-a preliminary comprehensive study on human serum, urine and skin. Front Mol Biosci. 2024;11:1382069. doi:10.3389/fmolb.2024.1382069
8. Nowowiejska J, Baran A, Hermanowicz JM, et al. Gasdermin C (GSDMC) is overexpressed in psoriatic tissue and elevated in psoriatic serum: a potential marker of cell proliferation and local hypoxia in psoriasis? Dermatologic Ther. 2023;2023:7813287. doi:10.1155/2023/7813287
9. Gangwar RS, Gudjonsson JE, Ward NL. Mouse models of psoriasis: a comprehensive review. J Invest Dermatol. 2022;142(3 Pt B):884–897. doi:10.1016/j.jid.2021.06.019
10. Choi CW, Kim BR, Park JS, Youn SW. Both educational lectures and reference photographs are necessary to improve the accuracy and reliability of Psoriasis Area and Severity Index (PASI) assessment: results from Korean nationwide PASI educational workshop. Ann Dermatol. 2018;30:284–289. doi:10.5021/ad.2018.30.3.284
11. Zaidi D, James KA, Wagner GF. Passive immunization of lactating mice with stanniocalcin-1 antiserum reduces mammary gland development, milk fat content, and postnatal pup growth. Am J Physiol Endocrinol Metab. 2006;291:E974–81.
12. Zhang J, Yang F, Zhang X, et al. Protective efficacy and mechanism of passive immunization with polyclonal antibodies in a sepsis model of Staphylococcus aureus infection. Sci Rep. 2015;5:15553. doi:10.1038/srep15553
13. Kang HJ, Kim MJ, Chu KB, Lee SH, Moon EK, Quan FS. Passive immunity and antibody response induced by Toxoplasma gondii VLP immunization. Vaccines. 2021;9:425. doi:10.3390/vaccines9050425
14. Kuc-Ciepluch D, Ciepluch K, Arabski M. Gasdermin family proteins as a permeabilization factor of cell membrane in pyroptosis process. Postep Hig Med Dosw. 2021;75:337–344. doi:10.5604/01.3001.0014.8985
15. Ciążyńska M, Narbutt J, Skibińska M, Lesiak A. The role of inflammasomes in cutaneous pathology. Postepy Dermatol Alergol. 2022;39(1):39–46. doi:10.5114/ada.2022.113802
16. Grän F, Kerstan A, Serfling E, Goebeler M, Muhammad K. Current developments in the immunology of psoriasis. Yale J Biol Med. 2020;93:97–110. doi:10.1038/jid.2012.339
17. Liao XX, Dai YZ, Zhao YZ, Nie K. Gasdermin E: a prospective target for therapy of diseases. Front Pharmacol. 2022;13:855828. doi:10.3389/fphar.2022.855828
18. Li Y, He Y, Yang F, et al. Gasdermin E-mediated keratinocyte pyroptosis participates in the pathogenesis of psoriasis by promoting skin inflammation. Br J Dermatol. 2024;191(3):385–396. doi:10.1093/bjd/ljae179
19. Long F, Wei X, Chen Y, et al. Gasdermin E promotes translocation of p65 and c-jun into nucleus in keratinocytes for progression of psoriatic skin inflammation. Cell Death Dis. 2024;15(3):180. doi:10.1038/s41419-024-06545-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Chronic Psoriasis Mouse Model via Optimized Imiquimod Dosing and Machine Learning Evaluation
Zhu H, Yu X, Wang Y, Zhao N, Qu B, Ma H, Meng Y, Zhao J, Wang Y, Li P
Journal of Inflammation Research 2026, 19:590945
Published Date: 23 April 2026