Back to Journals » Integrated Pharmacy Research and Practice » Volume 13
Antibiotic Dispensing Practices Among Community Retail Pharmacies and Registered Drugstores: Results from a Simulated Client Study in Lilongwe, Malawi
Authors Lubanga AF ![]() , Bwanali AN
, Bwanali AN ![]() , Kamanga W, Kathewera BS
, Kamanga W, Kathewera BS ![]() , Makole TJ
, Makole TJ ![]() , Mpinganjira SL
, Mpinganjira SL ![]() , Mudenda S
, Mudenda S ![]() , Mitambo C, Cho Y
, Mitambo C, Cho Y ![]() , Yeum D, Chung JS, Park J, Nyirenda T
, Yeum D, Chung JS, Park J, Nyirenda T
Received 21 August 2024
Accepted for publication 24 November 2024
Published 28 November 2024 Volume 2024:13 Pages 229—242
DOI https://doi.org/10.2147/IPRP.S487530
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Walid Al-Qerem
Adriano Focus Lubanga,1,2 Akim Nelson Bwanali,1,3 Watipaso Kamanga,1 Bernard Sindani Kathewera,4 Tumaini John Makole,5 Samuel L Mpinganjira,6,7 Steward Mudenda,8 Collins Mitambo,9 Yechan Cho,10 Daniel Yeum,10 Jonathan Sukhee Chung,11,12 Jooheon Park,13 Thomas Nyirenda1,13,14
1Clinical Research Education and Management Services (CREAMS), Lilongwe, Malawi; 2Department of Clinical Services, Kamuzu Central Hospital, Lilongwe, Malawi; 3Department of Clinical Services, Queen Elizabeth Central Hospital, Blantyre, Malawi; 4Department of Pharmacy, Queen Elizabeth Central Hospital, Blantyre, Malawi; 5Pharmacist, Pharmacy Council of Tanzania, Dar Es Salaam, Tanzania; 6School of Global and Public Health, Kamuzu University of Health Sciences, Blantyre, Malawi; 7Department of Global Health, University of Washington, Seattle Campus, Seattle, WA, USA; 8Department of Pharmacy, School of Health Sciences, University of Zambia, Lusaka, Zambia; 9Antimicrobial Resistance National Coordination Centre, Public Health Institute of Malawi, Lilongwe, Malawi; 10Youth with Talents, Fairfax, VA, 22030, USA; 11Stem Research Institute, Inc, Fairfax, VA, 22030, USA; 12Nova Southeastern University, Dr Kiran C. Patel College of Osteopathic Medicine, Fort Lauderdale, FL, USA; 13European and Developing Countries Clinical Trials Partnership (EDCTP), Strategic Partnerships and Capacity Development– Head of Africa Office, Cape Town, Republic of South Africa; 14Department of Global Health, Stellenbosch University, Stellenbosch, Republic of South Africa
Correspondence: Adriano Focus Lubanga, Clinical Research Education and Management Services (CREAMS), Anderson House, Area 43, P. O Box 31045, Lilongwe, Malawi, Tel +265992744497, Email [email protected]; [email protected]
Introduction: Antimicrobial resistance (AMR) is largely driven by the inappropriate use of antibiotics. This has been attributed to the non-prescription sale of antibiotics in retail drug outlets. Despite the rising number of retail drug outlets in Malawi, the practice of drug dispensing in private pharmacies has not been evaluated. This study therefore assessed the prevalence of non-prescription sales of antibiotics in retail drug outlets in Lilongwe, Malawi.
Methods: A community-based simulated client cross-sectional study was conducted in Lilongwe, Malawi from December 2023 to February 2024 using mystery shopping. Data were analyzed using IBM SPSS software version 29 using both descriptive and Analytical statistics. We computed simple proportions and conducted a hypotheses test using Chi-Square to test for Significance.
Results: Antibiotic dispensing practices were surveyed in 51 retail drug outlets comprising 36 retail pharmacies and 15 drugstores. 35.3% (n=18) of the drug outlets had drug dispensing done by pharmacists, 13.7% (n=7) by pharmacy technicians, 21.5% (n=11) by pharmacy assistants and 25.5% (n=15) by drug dispensers who had no pharmacy-related training. The rate of non-prescription sales of antibiotics ranged between 53% for acute diarrhoea and 92% for upper respiratory tract infections. Amoxicillin was the most dispensed antibiotic across all case scenarios. Over 50% of dispensed antibiotics were done upon recommendation of the drug dispensers in the absence of a doctor’s prescription. Furthermore, for all the dispensed antibiotics across all case scenarios, no advice was given for finishing a full course of the antibiotics.
Conclusion: This study found high rates of over-the-counter dispensing of antibiotics, which call for urgent and comprehensive regulatory measures to control antibiotic consumption in an urban part of Malawi that risks increased AMR. These could range from enacting stringent antibiotic dispensing policies to deploying digital systems to monitor prescription practices and community education on rational antibiotic use.
Keywords: Antimicrobial resistance, over-the-counter dispensing, drug outlets, pharmacies, drug stores, non-prescription sales
Introduction
The World Health Organization (WHO) has declared antimicrobial resistance (AMR) as one of the top 10 global public health threats facing humanity.1 Every year, an estimated 1.27 million people die globally due to AMR, with Africa registering the highest number of deaths attributable to AMR.2 Without action, the number of deaths attributable to AMR is expected to rise to as high as 10 million annually by 2050.3
Even though the development of AMR is regarded as a natural evolutionary process, the global health threat is exacerbated by human behaviour such as misuse and overuse of antibiotics in humans, agriculture and animal health, and environmental pollution.4 Additionally, it is being fueled by the usage of substandard and falsified medicines which is a growing problem in most low-and-middle-income countries (LMICs). Furthermore, overuse and inappropriate use of antimicrobial drugs particularly those under WHO Access and Watch categories is a key contributor to AMR. Both overuse and inappropriate use of antimicrobials in LMICs are driven by multiple factors including poor healthcare infrastructure, inadequate access to quality services, ineffectiveness in diagnostic competencies and weak regulatory frameworks.5
Malawi, a low-income country located in Sub-Saharan Africa, is not exempted from the impact of the emerging epidemic of AMR.6–8 The concerning rise in AMR among invasive bacterial species has been reported in national antimicrobial resistance surveillance data obtained from patients of all ages.9–11 There is widespread resistance to the Malawian first-line antibiotics including penicillins, and co-trimoxazole, and emerging resistance to the second-line and third-line antibiotics.11 In 2019, Malawi reported 3,600 deaths attributable to AMR and 15,700 deaths associated with AMR.9 In addition, Malawi ranks 23rd in terms of age-standardized mortality rate per 100,000 populations across 204 countries. In the Global Burden of Disease (GBD) region of Eastern Sub-Saharan Africa, Malawi ranks 7th among the countries with the highest age-standardized mortality across 15 countries.12
In most developing countries, including Malawi, antibiotics can easily be purchased over the counter without a prescription, mainly due to the absence of strict rules or lacking implementation and enforcement of adherence to existing drug-regulatory policies.13,14 Most of these antibiotics are dispensed in community-based clinics, retail pharmacies and drug outlets, commonly for conditions that are self-limiting, and do not require antibiotics.15–17
In Malawi, community retail pharmacies and drug stores play a crucial role in augmenting the weak healthcare system, greatly characterized by limited resources including essential drugs.18 The majority of these pharmacies and drug outlets are located in peri-urban areas and are regulated by the Pharmacy and Medicines Regulatory Authority (PMRA). In contemporary times, there has been an upsurge in several retail pharmacies and drugstores in most communities in Malawi. Even though these pharmacies operate under clear rules and regulations about dispensing of antimicrobial medicines, clear evidence exists from elsewhere of high overuse and inappropriate dispensing of antimicrobial drugs, which could potentially lead to resistance.19–21
Studies focusing on antimicrobial dispensing practices in community retail pharmacies and drug outlets are still lacking in Malawi. One study that exists focused on household use of antibiotics and reported that antibiotic use was mostly limited to a few antibiotics, namely amoxicillin, erythromycin and co-trimoxazole. The study further reported a household use of antibiotics of 6.4%.8
The recent rise in several community pharmacies and drug outlets and the rising concern for AMR due to overuse and inappropriate use of antimicrobial drugs calls for more innovative community-based research, assessing behaviours that could potentially frustrate antimicrobial stewardship efforts. Therefore, this community-based study adopted the simulated client approach to evaluate the prevalence of non-prescription sales of antibiotics in retail drug outlets in Lilongwe, Malawi.
Materials and Methods
Study Design
This community-based simulated cross-sectional client study was part of a mixed methods cross-sectional study employing an explanatory sequential design titled: “A Comprehensive Evaluation of Antimicrobial Medicines Dispensing Practices and Regulatory Frameworks in Community Pharmacies in Lilongwe, Malawi”. The bigger study sought to generate evidence of antimicrobial use, knowledge, and adherence to regulatory guidelines through community-based quantitative surveys of antimicrobial use, qualitative interviews and use of mystery clients to identify over-the-counter non-prescription dispensing of antimicrobial drugs.
This reported study used anonymous clients to evaluate antimicrobial dispensing practices in community drug outlets in Lilongwe, Malawi. In this context, drug outlets refer to community retail pharmacies and drugstores. In Malawi, retail pharmacies imply certified drug-dispensing shops which, as a requirement, are run by a qualified pharmacist whilst drugstores sell first-aid supplies and non-prescription cold medicines, and are run by pharmacy technicians or assistants. The trained mystery clients in our study paused as clients and visited the selected drug outlets within the city. They acted the designated case scenarios that tested antimicrobial dispensing practices within community-based retail pharmacies and drugstores.
The study was conducted between December 2023 and February 2024. Testing of the data collecting tools was done in December 2023 in a few selected pharmacies and retail drug stores. After the testing, all the data collected was evaluated for its alignment with the planned protocol and all challenges were resolved before further data collection commenced in February 2024.
Study Areas
This cross-sectional study was conducted in urban and peri-urban areas of Lilongwe, Malawi. The district was purposively selected based on geographical location, economic activity, and availability of community pharmacies and registered drugstores. Figure 1 shows the topographical location of the areas.
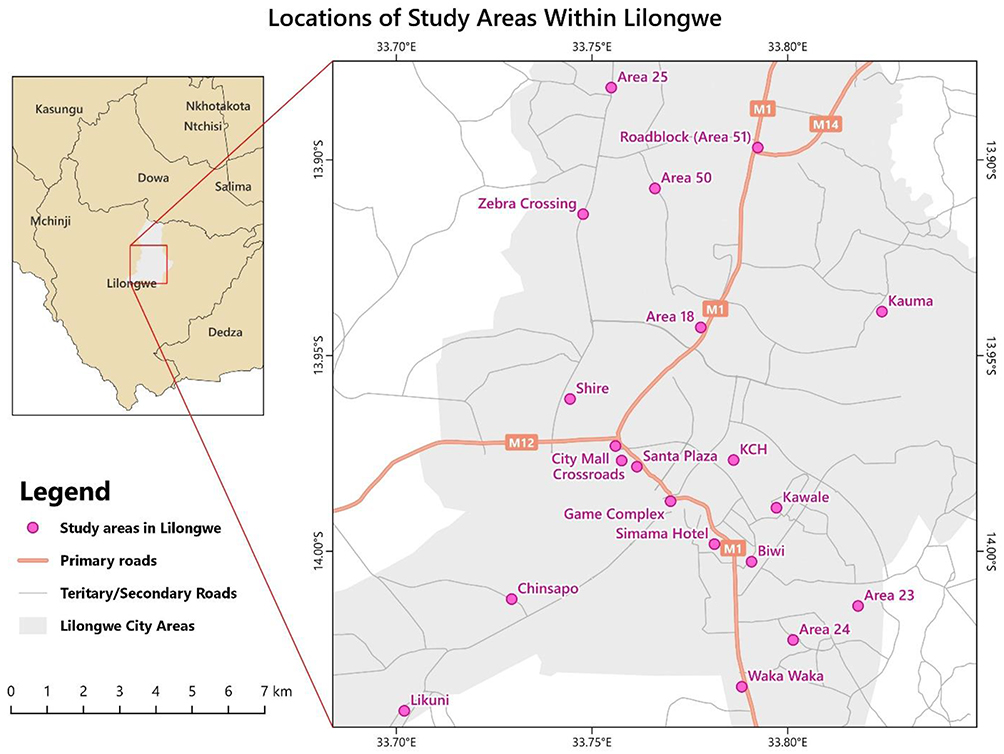 |
Figure 1 The topographical location of the study area. |
Sample Size
To create a comprehensive sampling frame for our study, we undertook a mapping exercise within peri-urban and urban areas of Lilongwe between December 1 and 30, 2023. A team of trained geo-information scientists navigated roads and pedestrian areas, recording the location, and presence of retail pharmacies and drugstores using Global Positioning System (GPS) enabled tablets and a report form developed in the research software package Epicollect5. Figure 2 shows the geographical distribution of retail pharmaceutical outlets in urban and peri-urban areas of Lilongwe.
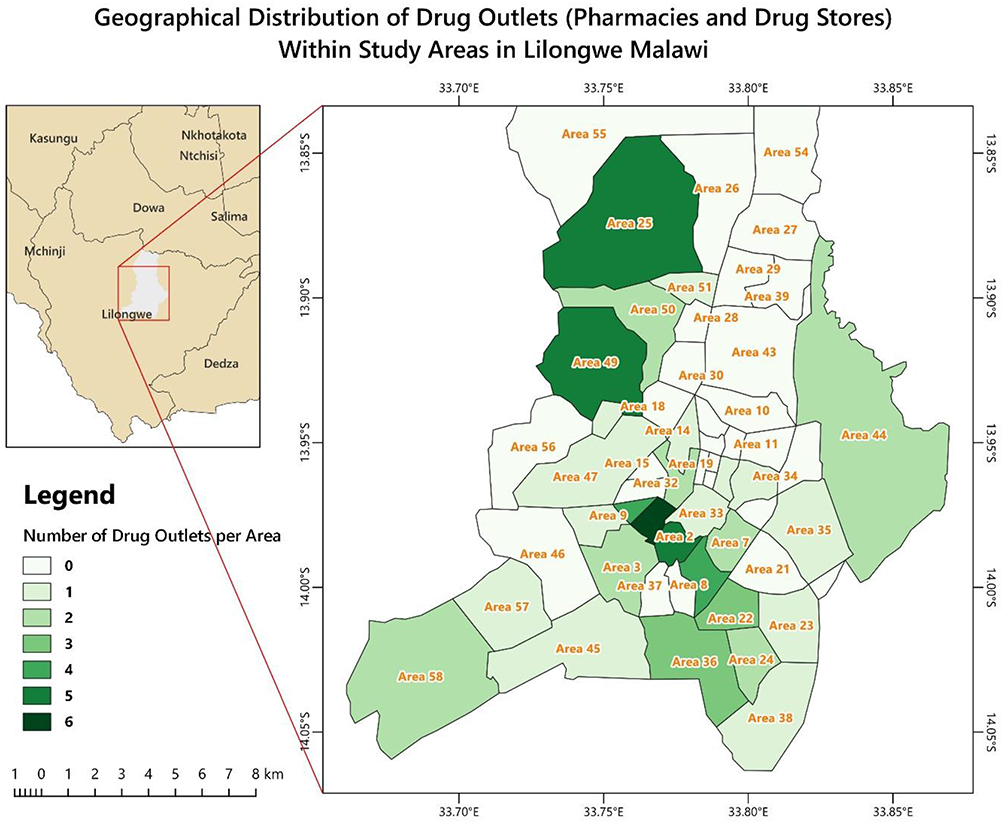 |
Figure 2 Geographical distribution of retail pharmaceutical outlets in urban and peri-urban areas of Lilongwe. |
Sampling
A multistage sampling technique was utilized. We purposively selected facilities in urban and rural areas to be representative in all areas. Following this, a random list of 51 drug outlets was generated for the mystery client study. We later then randomly selected 2 facilities in each cluster. Finally, research assistants purposively selected attending personnel to interact with in the simulated exercise. All agro-vets/traditional medicine shops were excluded from this study as the focus was human antibiotics provision.
Data Collection
The anonymous customers comprised 2 medical doctors and one physiotherapist unknown by the pharmaceutical drug outlets. They received a three-day training on the study aims, protocol and ethical issues, reporting methods, and how to act on the case scenarios. To ensure the genuineness of our findings, the MCs paid for all the drugs recommended by the dispensing personnel during the visits. The data collectors demonstrated consistent performance during both training as well as testing of the data collecting tools.
Antibiotic dispensing practices were assessed at three levels of demand. Pharmacy staff were assessed for their willingness to provide antibiotics based on the three levels of demand. This was designed based on similar previous studies.22 Figure 3 below summarizes levels of demand for the four simulated case scenarios used.
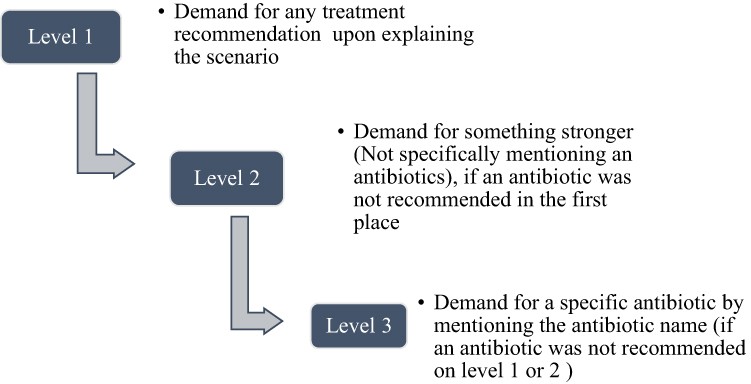 |
Figure 3 Levels of demand for acquiring antibiotics. |
In the beginning, the data collectors (mystery customers (MC’s)) were trained to introduce themselves and ask if they could talk to a pharmacist based on their symptoms. If they did not have such an opportunity, at the end of the encounter with the pharmacy personnel, the client asked; “Are you a pharmacist?”, because several cadres of staff are often present in a community pharmacy in Malawi (medicine counter assistants, pharmacy technicians, pharmacists). Worth noting that in Malawi, pharmacists are the only cadre legally allowed to distribute certain classes of antibiotics based on their clinical judgment.
Four case scenarios were established to be acted by the mystery clients at each of the selected dispensing areas. Scenario 1 recounted symptoms of an adult male relative experiencing symptoms of sore throat, with mild subjective fever. Scenario 2 recounted the symptoms of an adult male relative with diarrhoea without any other symptoms. Scenario 3 recounted an adult female relative with a suspected simple urinary tract infection (UTI), and the last case scenario recounted symptoms of a child with simple diarrhoea. See Supplementary Material 1.
Details for the choice of case scenarios and rationale for selection are recorded in Table 1 below.
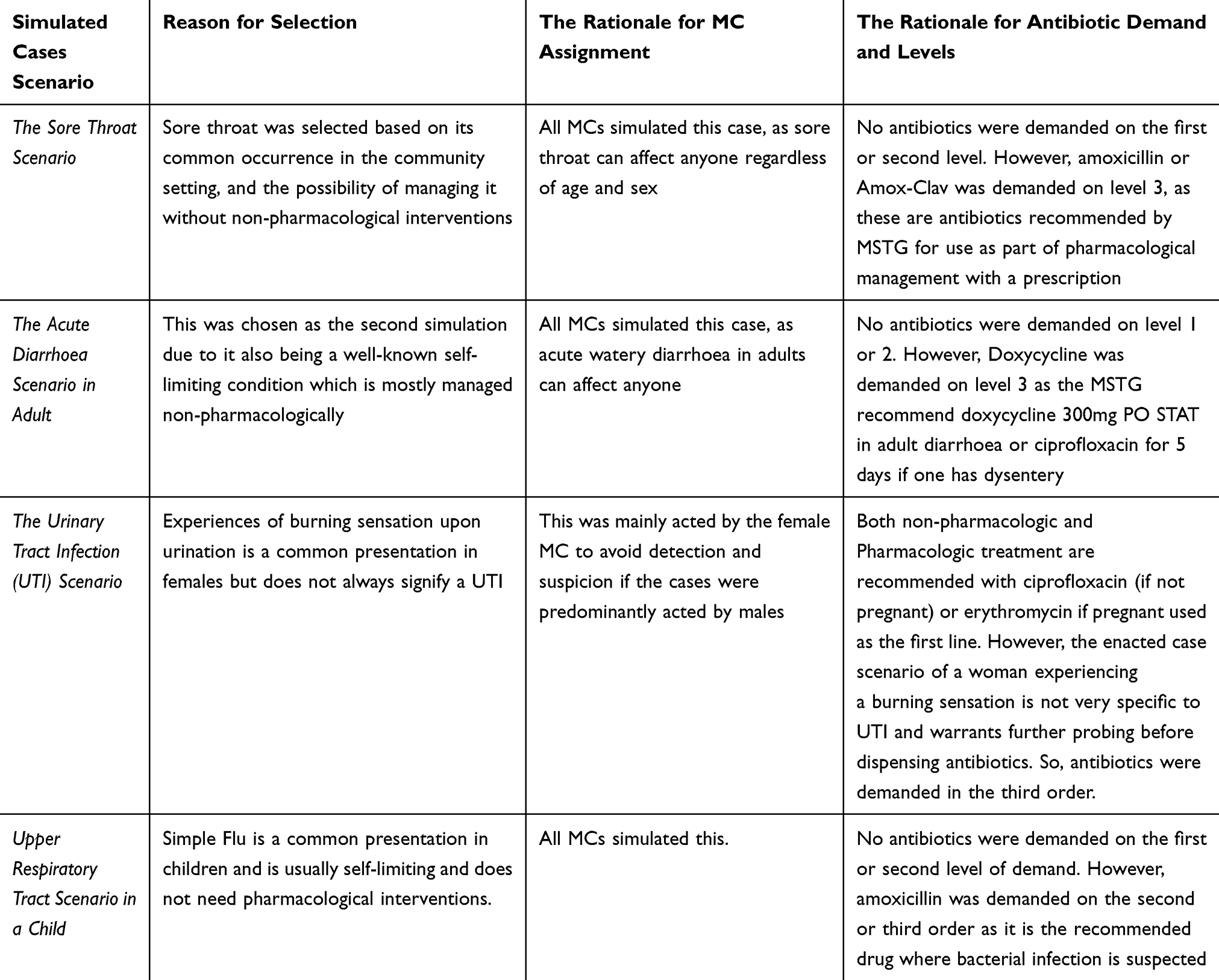 |
Table 1 Simulated Case Scenarios for Assessing Antibiotic Dispensing Practices |
According to the Malawi Standard Treatment Guidelines (MSTG), all these conditions can be managed non-pharmacologically.23 Pharmacological treatment (antibiotics) is recommended in special cases depending on the clinician’s assessment. During the data collection, no antibiotic was demanded on the first order. However, antibiotics were demanded on the second or third order depending on the initial response from the dispensers, the MCs just acted out the case scenario sought the advice of the responsible personnel and observed whether antibiotics were recommended or not.
During each interaction, we also assessed the quality of the interaction between client and seller and the degree to which practices among sellers were in line with Malawi antibiotic stewardship programs. We used the following list of variables: (1). Asked for a prescription (2). Suggested that the MC did not require antibiotics, (3). Suggested that the MC should buy a full course of the drug (4). Inquired about the use of other drugs. (5). Inquired about other symptoms, drug allergies, and pregnancy if female (6). Gave clear directives that the client should finish a full course if antibiotics were dispensed.
The MCs were all natives of Lilongwe district, and fluent speakers of English and the native language, Chichewa, the languages in which the case scenarios were enacted.
Data Analysis
Data analysis was performed using IBM SPSS version 29. The results were analyzed using both descriptive and Analytical statistics. The main outcome of interest, namely non-prescription dispensing of antibiotics, was reported as a proportion with a 95% confidence interval. The chi-square test was to determine the significance of the association between the two variables.
Ethical Consideration
The study received ethical approval from the National Health Sciences Research Committee (NHSRC), (No. 23/10/4213, 08/12/2023). A written ethical clearance was also granted by the Lilongwe District Health Ethics Committee under whose catchment areas was the research conducted. While pharmaceutical workers/dispensers did not consent, the nature of the study did not allow them to do anything outside their normal duties. Furthermore, the responses gathered at particular sites and from particular individuals, are de-identified in the results presented.
Results
Characteristics of the Drug Outlets Visited and Drug Dispenser Qualifications
The MCs visited a total of 51 drug outlets within Lilongwe, comprising 36 retail pharmacies and 15 drugstores. The initial pharmaceutical outlet hotspot mapping revealed that some areas did not have registered community retail pharmacies. In these areas, the MCs visited drugstores which serve as main drug outlets within the communities.
Out of the 51 drug outlets visited, 35.3% (n=18) had drug dispensing done by pharmacists, 13.7% (n=7) by pharmacy technicians, 21.5% (n=11) by pharmacy assistants and 25.5% (n=15) by drug dispensers who had no pharmacy-related training. Twenty-five of the drug dispensers during the visits were females, representing (49%), while 26 of the drug dispensers were males representing 51%. Table 2 summarizes the demographic profile of the drug dispensers.
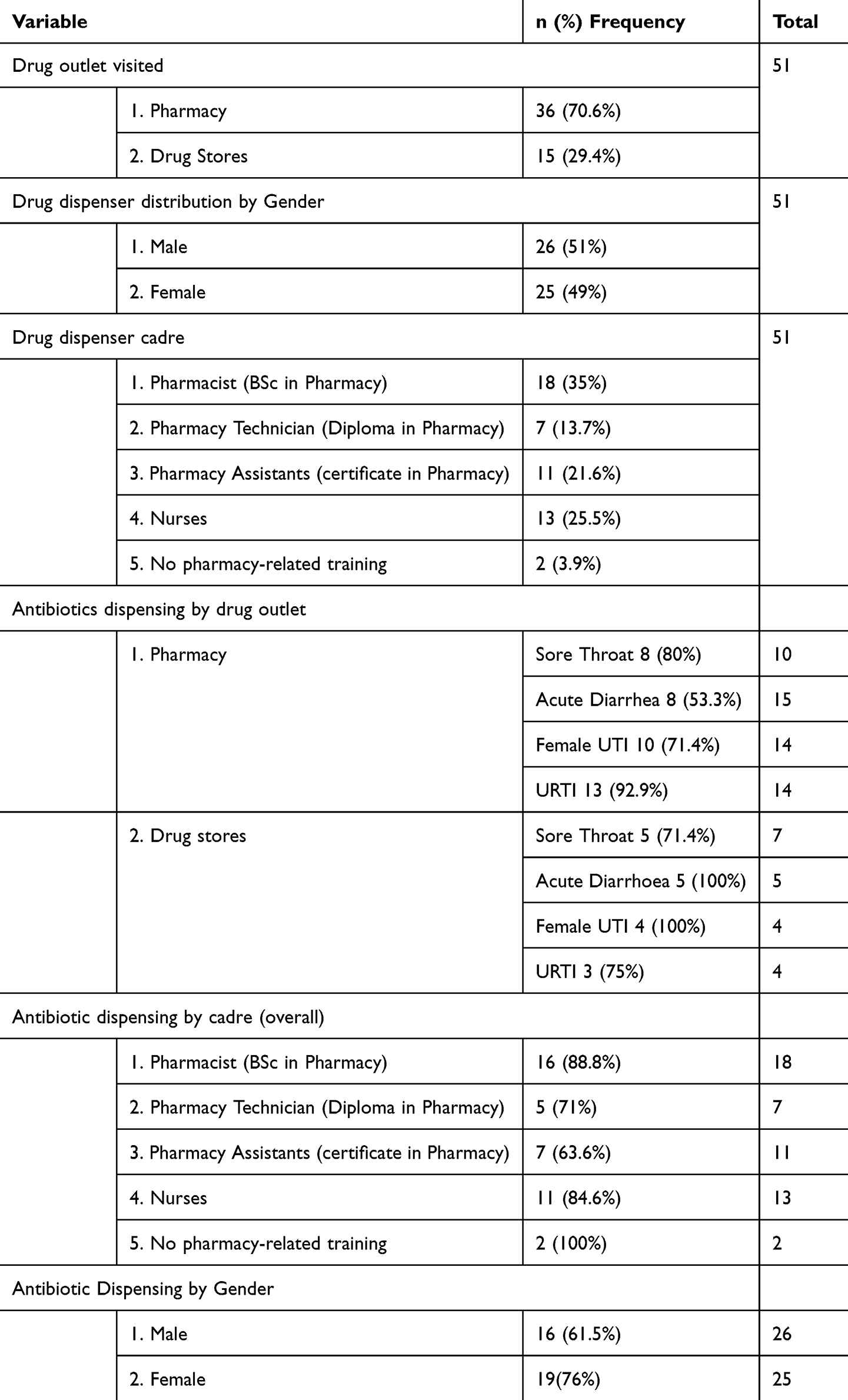 |
Table 2 Social Demographic Characteristics of the Dispensers |
Prevalence of Antibiotics Supplied Without a Prescription Among Community Pharmaceutical Outlets by Case Scenario and Level of Demand
Generally, for all case scenarios, more than 50% of antibiotics were sold at the first level of demand and the results are statistically significant. For the adult sore throat case, antibiotics were offered by 80% (12/15) of the pharmaceutical outlets visited during the study. About 66.7% of these antibiotics were offered at the first level of demand, and the most commonly offered antibiotic was amoxicillin (5/12). One pharmacy sold out benzylpenicillin at the first level of demand. The other drugs that were given out for sore throat include Metronidazole (1st level of demand, n=1), azithromycin (n=2), erythromycin (n=1), and phenoxymethylpenicillin + amoxicillin (n=1). Only three of the visited pharmacies refused to offer antibiotics at all levels, and one recommended an antifungal medication.
For the acute diarrhoea case scenario in adults, antibiotic therapy was offered in 72.7% (16/22) of the pharmacies visited. The most common antibiotic for this scenario was metronidazole alone (56.3%, 9/16). Metronidazole was the most frequent antibiotic given out on first order (n=8).
Two pharmacies recommended doxycycline on the first order while one pharmacy gave out doxycycline on the third order. The other antibiotics that were given out without prescription on the second and third levels of demand included ciprofloxacin (n=1), azithromycin (n=1), cloxacillin (n=1), co-trimoxazole and erythromycin (n=1).
Antibiotics were dispensed by 80% of the pharmacies visited for UTI cases in adult females. Ciprofloxacin was the most frequently offered antibiotic at the first level of demand (9/16) (56.25%). One pharmacy recommended a combination of gentamicin/azithromycin/metronidazole at the first level of demand (n=1), while other dispensaries also gave out azithromycin, erythromycin and doxycycline at the second and third level of demand.
For the URTI scenario in a child, antibiotics were dispensed by 77.8% of pharmaceutical outlets visited (17/21). Antibiotics were only recommended by 50% of the pharmacies at the first level of demand, 28.6% and 21.4% at the second and third level of demand respectively. The most frequently recommended antibiotic at all levels was amoxicillin (n=10). Other antibiotics that were sold at the second level of demand without a prescription for the URTI scenario included phenoxymethylpenicillin, co-trimoxazole, benzylpenicillin, metronidazole and azithromycin. Table 3 summarizes the antibiotic dispensing practices by case scenario and level of demand.
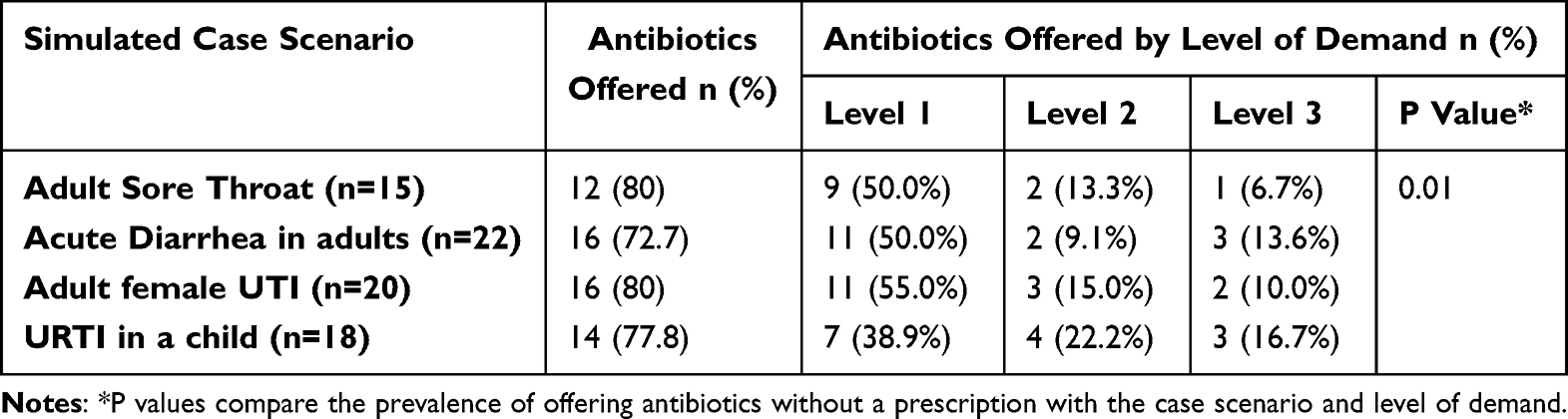 |
Table 3 Prevalence of Antibiotics Supplied Without a Prescription Among Community Pharmaceutical Outlets by Case Scenario and Level of Demand |
Association Between the Type of Drug Outlet and the Dispensing of Antibiotics for Different Scenario Cases
For all the simulated case scenarios, antibiotics were more likely dispensed in community pharmacies as compared to drugstores, and the results are statistically significant as demonstrated in Table 4. Even though the selling of antibiotics in drugstores is restricted in Malawi, most of the drugstores do keep stock of and sell antibiotics secretly. Antibiotic dispensing without a prescription was a common practice for both retail pharmacies and drugstores.
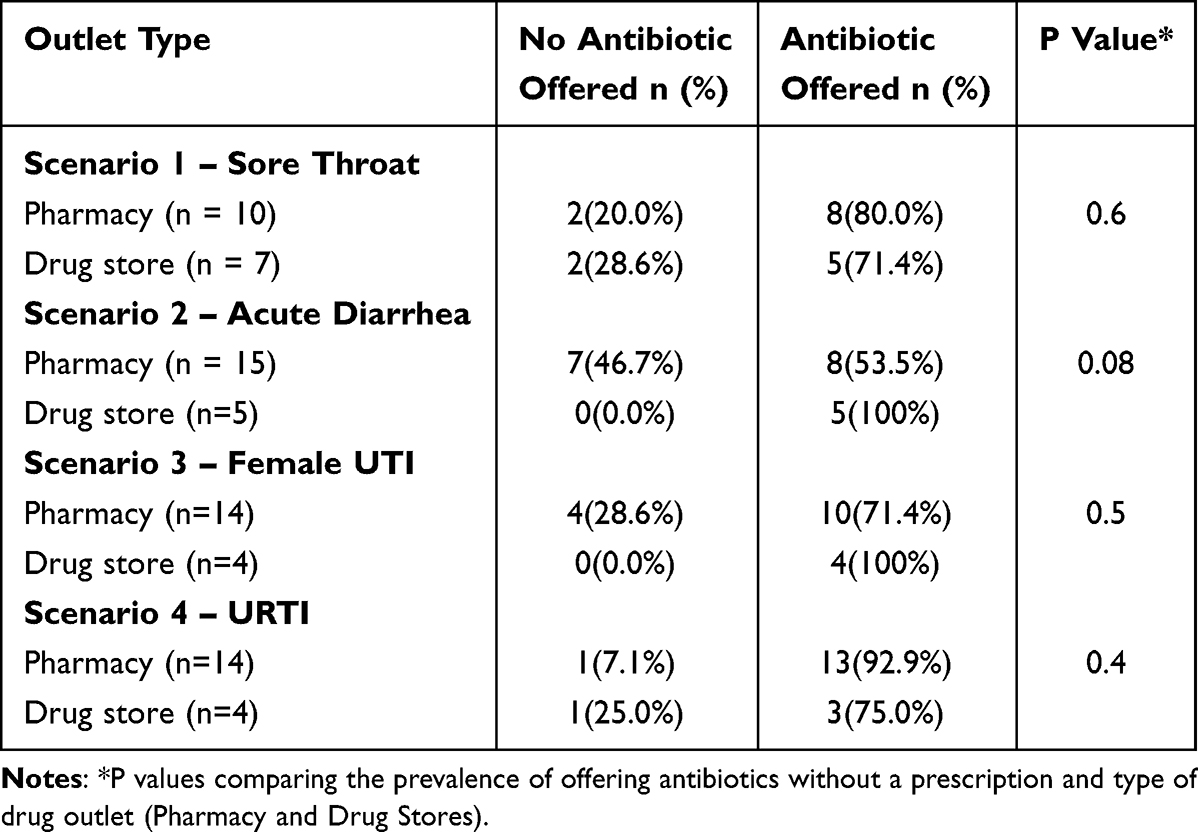 |
Table 4 Association Between the Type of Drug Outlet and the Dispensing of Antibiotics for Different Scenario Cases |
Association of Gender and Cadre of Drug Dispensers with Dispensing of Antibiotic
Regarding dispensing antibiotics without a prescription by cadre and gender, being male was associated with a significant chance of selling antibiotics as compared to females. Pharmacists were also more likely to sell antibiotics, and the results were statistically significant.
Generally, dispensing of antibiotics was still common amongst all cadres as shown in Table 5 below.
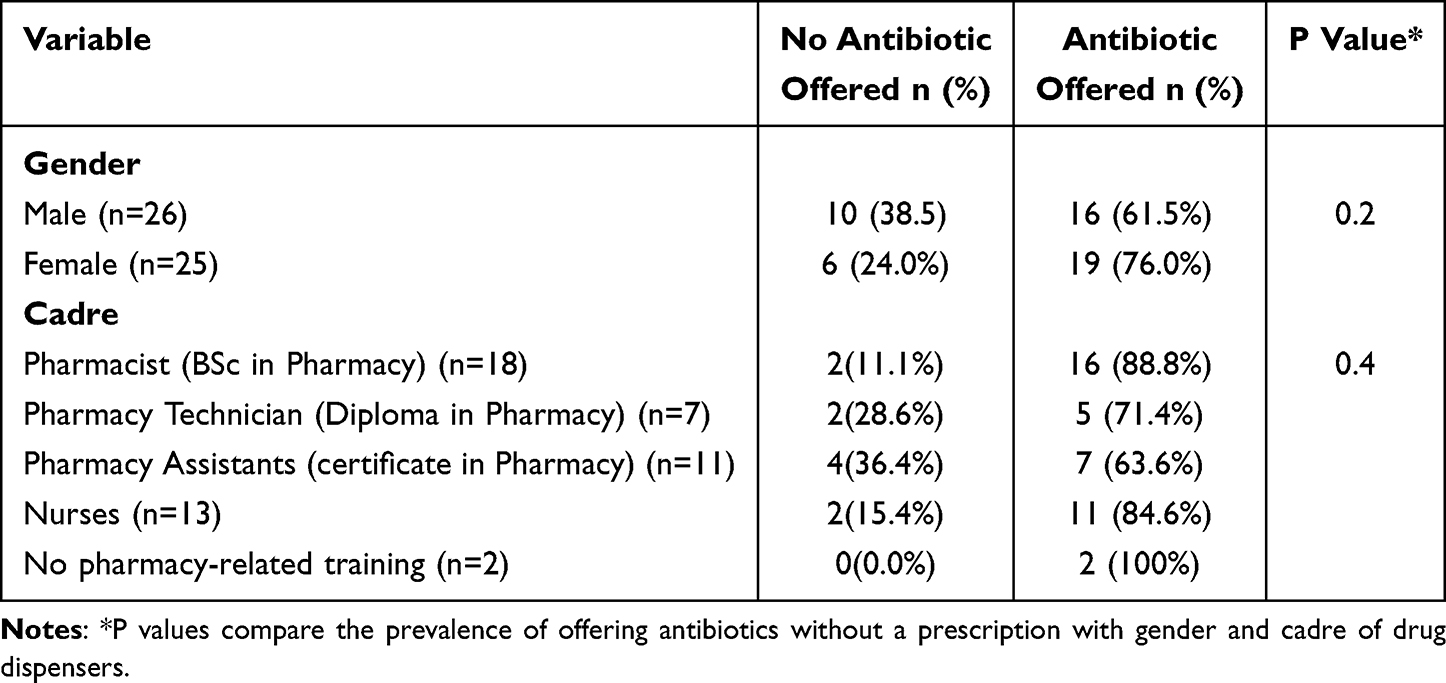 |
Table 5 Association of Gender and Cadre of Drug Dispensers with Dispensing of Antibiotic |
AWaRe Classification of Antibiotics Offered by All Pharmaceutical Outlets in the City of Lilongwe by Case Scenario Without a Prescription
Nearly all the antibiotics sold without a prescription came from the access category of WHO anatomical classification of antibiotics. Few antibiotics were sold from the watch category, and none was sold from the reserve category as shown in Table 6 below.
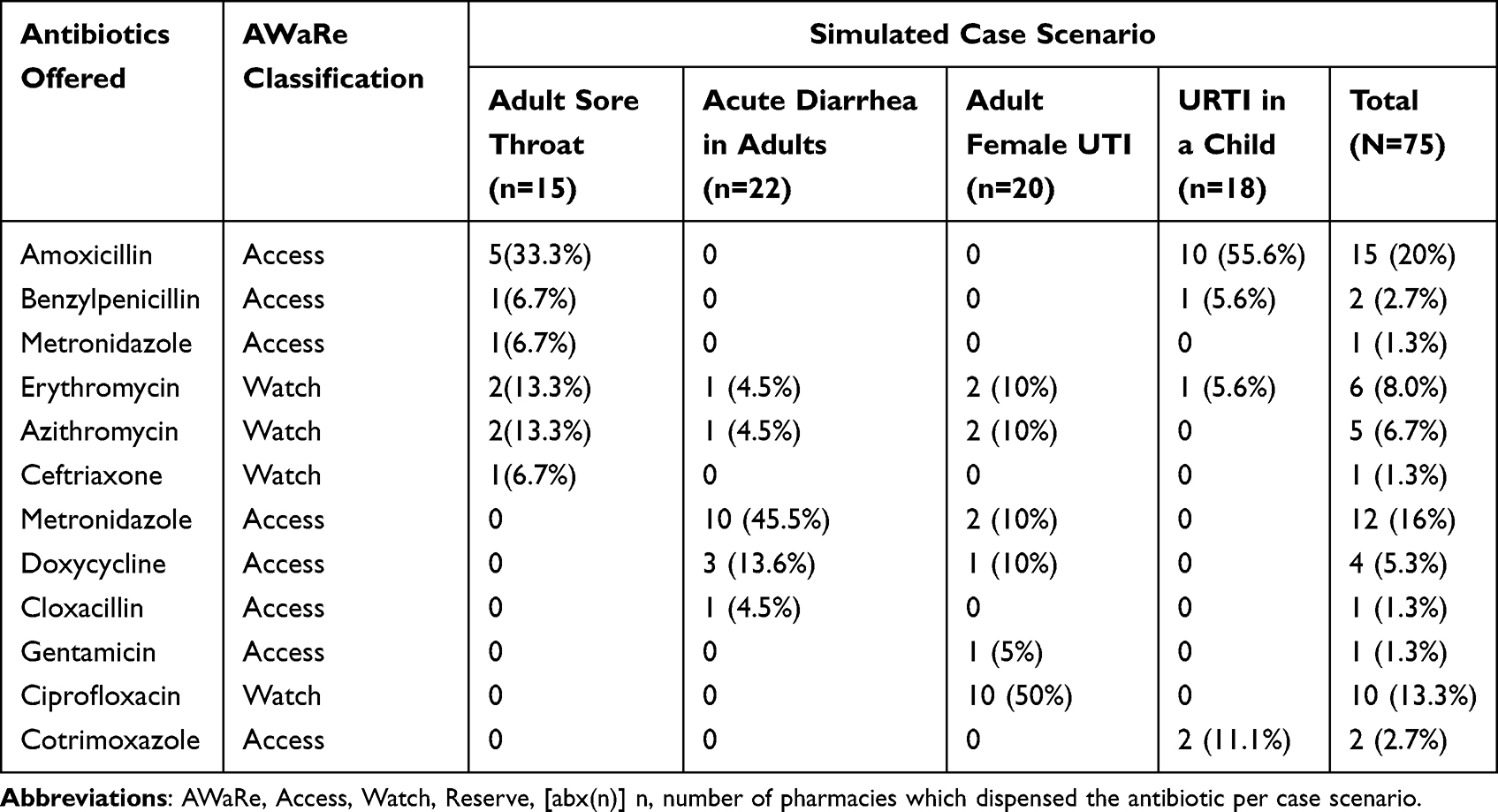 |
Table 6 AWaRe Classification of Antibiotics Offered by All Pharmaceutical Outlets in the City of Lilongwe by Case Scenario Without a Prescription |
Antibiotic Dispensing Practices and Quality of Interaction with Clients
Regarding the quality of interaction and antimicrobial stewardship, only three drug outlets asked for a prescription and/or wanted a patient available before dispensing antibiotics. Only 5 of the visited drug outlets recommended alternative non-antibiotic treatment for the simulated case scenarios. For all the dispensed antibiotics across all case scenarios, no advice was given for finishing a full course of the antibiotics. About asking for other symptoms, only four dispensing areas asked for the UTI case scenario, 3 for sore throat, 3 for diarrhoea case scenario and 3 for the upper respiratory tract case.
Discussion
To our knowledge, this study is the first simulated client exercise assessing antibiotic dispensing practices in Malawi. Simulated client studies are common in pharmaceutical practice, and have been largely used in assessing compliance with regulatory guidelines in many LMICS.16 They provide a first-hand encounter, thereby helping to minimize observer bias. The study reveals a common practice of dispensing/and or offering antibiotics without a prescription. Additionally, there was minimal patient education on drug compliance and finishing the dispensed course of antibiotics.24
The study revealed a high rate of non-prescription sales of antibiotics. Drug dispensers were offering antibiotics without even being requested and without inquiring about the clinical symptoms of the patient. A similar trend has been reported in multiple countries across the SSA including Uganda, Tanzania, Zambia and Nigeria.24–27 This is the case despite existing regulatory frameworks that admonish off-prescription sale of antibiotics in these countries.28 Antimicrobial drug regulatory infringements are common in SSA.24 This reflects occasional regulatory inspections, negligence or failure of regulatory authorities to implement sanctions and generally weak and unstable health systems that are currently underperforming in their efforts to promote safe drug use and contain the various dynamics of drug resistance.29,30 Recognizing the massive impact that inappropriate antibiotic use has on spearheading the development of AMR, it is crucial to strengthen and empower drug regulatory authorities to ensure that community drug outlets promote safe and appropriate dispensing of antibiotics.
The majority of the pharmacies and drugstores had qualified drug dispensers, which are approved by the Pharmacy and Medicines Regulatory Authority (PMRA) in the country. However, a worrying third of the drug outlets were operating without qualified personnel. The lack of qualified pharmacy personnel in retail drug outlets is a well-known and old problem in African settings.31 Despite the clear directive from the PMRA that retail pharmacies should be overseen by registered pharmacists and drugstores by pharmacy technicians, our study reveals that there are existing drug outlets that overlooked the directive. Not only is this a threat in the fight against AMR, through antibiotic overconsumption but it also jeopardizes patient safety due to medication errors leading to toxicity when wrong drugs are prescribed or when prescribed drugs are taken in high doses. Availability of qualified personnel in pharmacies is imperative to enhance prescription-based dispensing of antibiotics and enhance overall appropriate antibiotic use.
Another concern revealed in the present study is that antibiotics were mostly dispensed with little to no patient education. This results in self-medication and improper antibiotic use which has been heavily reported in SSA. A systematic review on self-medication and antibiotic consumption in SSA conducted in 2021 reported a self-medication prevalence as high as 93% (median prevalence of 70%) with the commonest source of antibiotics being community pharmacies.32 Among graduates in Nigeria, a study found that about half self-medicate and up to 70% stop taking antibiotics once they start feeling better.33 The conditions that called for antibiotic use are the same used in our simulated client exercise, all of which are self-limiting and do not always warrant antibiotic use. This speaks volumes as to what the burden of the problem might be among community members, some of whom never attended school. Pharmacist-driven patient education has been shown to increase adherence, reduce medication errors, and lower 30-day readmission rates among inpatients.34 However, there is a paucity of data on the quality of patient education on antimicrobial drug use in community pharmacies in SSA. This threatens to sustain the lethal practice of improper antibiotic use. Improper antibiotic use encompassing (excessive consumption and under-dosing) is an important contributor to antimicrobial drug resistance.35,36 It is a matter of urgency, therefore, to ensure that drug dispensers provide the necessary client education when dispensing antibiotics. This should encompass the proper indications for taking antibiotics, appropriate frequency, dosage and duration as well as encouraging physician consultation for proper prescriptions to follow adequate clinical evaluation.
Furthermore, the study supports the fact that most of the dispensed antibiotics were from the Access and Watch categories of the WHO AWaRe classification of antibiotics. This pattern correlates with the national antimicrobial consumption rate in SSA.37,38 This could also be explained by the relatively lower cost of this antibiotic as compared to other antibiotics of the same Access category. As a regulation to antimicrobial use, in 2019, the WHO proposed a global monitoring indicator requiring that by 2023, 60% of all antibiotics consumed come from the Access category, including antibiotics with the lowest risk of resistance.39 This would mean decreasing the Access antibiotics consumption from >90% observed in Malawi between 2016 and 2018, according to the Mapping Antimicrobial Resistance and Antimicrobial Use Partnership (MAAP) Country Reports.40 However, since the 2017 MAAP report, there has not been a recent update on trends in antibiotic consumption within the country. With the high consumption of Access antibiotics sourced from retail pharmacies, it is important to closely monitor the antibiotic consumption trends to curb excessive consumption and preserve the antibiotics with the least resistance. If we are to win this fight against AMR and preserve the efficacy of the current antimicrobial-sensitive antibiotics, it is essential to regulate and control the consumption of antibiotics.
Amoxicillin was the most dispensed antibiotic. This is an important broad-spectrum antibiotic used in various conditions including lower respiratory tract infections, ear and eye infections, as well as urinary tract infections with minimal and self-limiting side effects.41,42 This could be due to the relatively lower cost of the drug compared to other antibiotics of the same WHO Access category. However, there is a rising concern in Africa for the development of resistance to this commonly used antibiotic especially to Enterobacteriaceae.43,44 The emerging resistance to this important antibiotic threatens the fight against the existing and emerging infectious diseases in SSA.
Strengths and Limitations
Our study is the first to explore trends in the non-prescription sale of antibiotics in Malawi. We believe it lays a good precedent and foundation for further studies in the future to explore trends in drug dispensing and associated factors in different settings. A key strength of our study is the design used which conferred an objective assessment by the mystery client approach, making our results much more reliable than self-reported responses to a questionnaire. In addition, the scenario used allowed us to assess pharmacist antimicrobial stewardship practices through direct observations which could not be achieved with any other approach. However, due to the difficulties associated with obtaining a list of all registered pharmacies and other drug outlets, our sample size may not have been powered enough to detect differences and not be representative of the entire Lilongwe City.
Recommendations
Our study reveals a huge regulatory void. In the presence of clear guidelines and policies in Malawi, a strong concerted approach is needed to promote judicious dispensing and use of antibiotics in community-based drug outlets. Appropriate measures may include regular monitoring, staff training, public education, development as well as enforcement of strong pharmacy practice surveillance systems. Digital platforms may be adopted to promote monitoring of antimicrobial medicines dispensing from community pharmacies and associated stewardship practices. This may include the adoption of electronic recording systems which can be linked to national antimicrobial use databases for antimicrobial use surveillance in non-hospital-based areas.
Area for Further Studies
More studies are needed to assess factors associated with drug-dispensing practices within community drug outlets. The studies could be expanded to explore their knowledge of drug dispensing, attitudes and practices toward antimicrobial stewardship as well as their patient education practices. The current study was only conducted in peri-urban and urban areas of one city. Therefore, the results may not be generalized for the whole country due to systemic differences (rural or other cities).
Furthermore, more studies assessing the role of national regulatory bodies in promoting antimicrobial stewardship as well as law enforcement in reducing the non-prescribed supply of antibiotics are needed. These will guide the possible need for multifaceted interventions and the most appropriate approaches in addressing the over-the-counter use of antibiotics.
Conclusion
Our study found a high prevalence of non-prescription sales of antibiotics. The study also revealed that a significant proportion of pharmacies do not have qualified workers, and a huge proportion of non-qualified workers sold non-prescription antibiotics. Finally, our study reveals that most drug dispensers sold antibiotics without proper instructions on use, side effects, and treatment adherence.
This raises a big concern in the fight against AMR in the country. Hence, there is a need for urgent and comprehensive measures. These could range from enacting stringent antibiotic dispensing policies to deploying the use of digital systems for tracking prescription practices and community education on rational antibiotic use.
Acknowledgments
We would like to acknowledge the following individuals who collaborated on the manuscript and provided their inputs at various stages of the work, Dr. Chisomo Mhura, Mr. Frank Kaphesi, Dr. Frank Kambiri, Dr. Chisomo Mtonga, Dr. Byenala Kawonga, Dr. Kondwani Ngoma, Mr. Yewo Mhango, Dr. Gracian Harawa and Ms. Tapiwa Elizabeth Moyo We would also like to thank the National Antimicrobial Resistance Coordinating Committee, under the Public Health Institute of Malawi for their collaboration in this study. This work has not been previously presented as an abstract at a conference or similar forum.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This manuscript was funded by Clinical Research Education and Management Services (CREAMS Mw), under the Small-scale Mentorship Grant Scheme.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Vanderwall M, Strine MS. Antimicrobial Resistance. Yale J Biol Med. 2022;95(4):405–406.
2. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
3. Outterson K, Orubu ESF, Rex J, Ardal C, Zaman MH. Incentivising the development of new antibacterial treatments 2023. Clinl Infect Dis. 2022;74(7):1183–1190. doi:10.1093/cid/ciab612
4. Holmes AH, Moore LSP, Sundsfjord A, et al. Understanding the mechanisms and drivers of antimicrobial resistance. Lancet. 2016;387(10014):176–187. doi:10.1016/S0140-6736(15)00473-0
5. Kanan M, Ramadan M, Haif H, et al. Empowering Low- and Middle-Income Countries to Combat AMR by Minimal Use of Antibiotics: a Way Forward. Antibiotics. 2023;12(10):1–13. doi:10.3390/antibiotics12101504
6. Focus Lubanga A, Bwanali N, Kambiri F, et al. Expert Review of Anti-infective Therapy Tackling antimicrobial resistance in sub-Saharan Africa: challenges and opportunities for implementing the new people-centered WHO guidelines Tackling antimicrobial resistance in sub-Saharan Africa: challenges and opportunities for implementing the new people-centered WHO guidelines. 2024;
7. Lutterloh E, Likaka A, Sejvar J, et al. Multidrug-resistant typhoid fever with neurologic findings on the Malawi-Mozambique border. Clinl Infect Dis. 2012;54(8):1100–1106. doi:10.1093/cid/cis012
8. MacPherson EE, Mankhomwa J, Dixon J, et al. Household antibiotic use in Malawi: a cross-sectional survey from urban and peri-urban Blantyre. PLOS Global Public Health. 2023;3(8):e0001946. doi:10.1371/journal.pgph.0001946
9. Feasey NA, Masesa C, Jassi C, et al. Three epidemics of invasive multidrug-resistant salmonella bloodstream infection in Blantyre, Malawi, 1998-2014. Clinl Infect Dis. 2015;61(Suppl 4):S363–71. doi:10.1093/cid/civ691
10. Lester R, Musicha P, Kawaza K, et al. Effect of resistance to third-generation cephalosporins on morbidity and mortality from bloodstream infections in Blantyre, Malawi: a prospective cohort study. Lancet Microbe. 2022;3(12):e922–30. doi:10.1016/S2666-5247(22)00282-8
11. Haigh K, Dube Q, Kasambara W, Feasey NA, Lester R. Cephalosporin resistance in Malawi. Lancet Infect Dis. 2020;20(3):285–286. doi:10.1016/S1473-3099(20)30047-5
12. Institute for Health Metrics and Evaluation. The burden of antimicrobial resistance (AMR) in Indonesia. Global Res Antimicrob Res. 2011;2011:1–4.
13. Sharma A, Singh A, Dar MA, et al. Menace of antimicrobial resistance in LMICs: current surveillance practices and control measures to tackle hostility. J Infect Public Health. 2022;15(2):172–181. doi:10.1016/j.jiph.2021.12.008
14. Belachew SA, Hall L, Selvey LA. Non - prescription dispensing of antibiotic agents among community drug retail outlets in Sub - Saharan African countries: a systematic review and meta - analysis. Antimicrob Resist Infect Control. 2021;10(1):1–15. doi:10.1186/s13756-020-00855-x
15. Godman B, Haque M, McKimm J, et al. Ongoing strategies to improve the management of upper respiratory tract infections and reduce inappropriate antibiotic use particularly among lower and middle-income countries: findings and implications for the future. Curr Med Res Opin. 2020;36(2):301–327. doi:10.1080/03007995.2019.1700947
16. Godman B, Egwuenu A, Haque M, et al. Strategies to Improve Antimicrobial Utilization with a Special Focus on Developing Countries. Life. 2021;11(6):528. doi:10.3390/life11060528
17. Edessa D, Assefa N, Dessie Y, Asefa F, Dinsa G, Oljira L. Non-prescribed antibiotic use for children at community levels in low- and middle-income countries: a systematic review and meta-analysis. J Pharm Policy Pract. 2022;15(1):1–17. doi:10.1186/s40545-022-00454-8
18. Muula AS. Recent changes in the Malawi health system: a time for reflection. Malawi Med J. 2019;31(4):223–224. doi:10.4314/mmj.v31i4.1
19. Ndaki PM, Mwanga JR, Mushi MF, et al. Practices and motives behind antibiotics provision in drug outlets in Tanzania: a qualitative study. PLoS One. 2023;18(8):1–14. doi:10.1371/journal.pone.0290638
20. Erku DA, Aberra SY. Correction to: non-prescribed sale of antibiotics for acute childhood diarrhea and upper respiratory tract infection in community pharmacies: a 2 phase mixed-methods study (Antimicrobial Resistance and Infection Control. Antimicrob Resist Infect Control. 2019;8(1):13756. doi:10.1186/s13756-018-0458-2
21. Gebretekle GB, Serbessa MK. Exploration of over the counter sales of antibiotics in community pharmacies of Addis Ababa, Ethiopia: pharmacy professionals’ perspective. Antimicrob Resist Infect Control. 2016;5(1):1–7. doi:10.1186/s13756-016-0101-z
22. Saleem Z, Hassali MA, Godman B, et al. Sale of WHO AWaRe groups antibiotics without a prescription in Pakistan: a simulated client study. J Pharm Policy Pract. 2020;13(1):1–8. doi:10.1186/s40545-020-00233-3
23. The Ministry of Health Malawi. Malawi Standard Treatment Guidelines (MSTG) 5th Edition 2015 Guidelines. 2015:687
24. Sono TM, Yeika E, Cook A, et al. Current rates of purchasing of antibiotics without a prescription across sub-Saharan Africa; rationale and potential programmes to reduce inappropriate dispensing and resistance. Expert Rev Anti Infect Ther. 2023;21(10):1025–1055. doi:10.1080/14787210.2023.2259106
25. Ndaki PM, Mushi MF, Mwanga JR, et al. Dispensing antibiotics without prescription at community pharmacies and accredited drug dispensing outlets in Tanzania: a cross-sectional study. Antibiotics. 2021;10(8):1–15. doi:10.3390/antibiotics10081025
26. Kalungia AC, Burger J, Godman B, de O CJ, Simuwelu C. Non-prescription sale and dispensing of antibiotics in community pharmacies in Zambia. Expert Rev Anti Infect Ther. 2016;14(12):1215–1223. doi:10.1080/14787210.2016.1227702
27. Abubakar U, Tangiisuran B. Knowledge and practices of community pharmacists towards non-prescription dispensing of antibiotics in Northern Nigeria. Int J Clin Pharm. 2020;42(2):756–764. doi:10.1007/s11096-020-01019-y
28. Salim AMA, Elgizoli B. Exploring the reasons why pharmacists dispense antibiotics without prescriptions in Khartoum state, Sudan. Int J Pharm Pract. 2017;25(1):59–65. doi:10.1111/ijpp.12317
29. Goodman C, Kachur SP, Abdulla S, Bloland P, Mills A. Drug shop regulation and malaria treatment in Tanzania - Why do shops break the rules, and does it matter? Health Pol Plan. 2007;22(6):393–403. doi:10.1093/heapol/czm033
30. Shomuyiwa DO, Lucero-Prisno DE, Manirambona E, et al. Curbing antimicrobial resistance in post-COVID Africa: challenges, actions and recommendations. Health Sci Rep. 2022;5(5):1. doi:10.1002/hsr2.771.
31. Smith F. The quality of private pharmacy services in low and middle-income countries: a systematic review. Pharm World Sci. 2009;31(3):351–361. doi:10.1007/s11096-009-9294-z
32. Yeika EV, Ingelbeen B, Kemah BL, Wirsiy FS, Fomengia JN, van der Sande MAB. Comparative assessment of the prevalence, practices and factors associated with self-medication with antibiotics in Africa. Trop Med Int Health. 2021;26(8):862–881. doi:10.1111/tmi.13600
33. Popoola OO, Adepitan DS, Adeyemi AS, Oladeru OF, Yusuff SI. A national survey of the antibiotic use, self-medication practices, and knowledge of antibiotic resistance among graduates of tertiary institutions in Nigeria. Sci Afr. 2024;23:e01978.
34. Park D, Patel S, Yum K, Smith CB, Tsao CK, Kim S. Impact of Pharmacist-Led Patient Education in an Ambulatory Cancer Center: a Pilot Quality Improvement Project. J Pharm Pract. 2020;35(2):268–273. doi:10.1177/0897190020970770
35. Wu CT, Chen CL, Lee HY, et al. Decreased antimicrobial resistance and defined daily doses after implementation of a clinical culture-guided antimicrobial stewardship program in a local hospital. J Microbiol Immunol Infect. 2017;50(6):846–856. doi:10.1016/j.jmii.2015.10.006
36. Lautenbach E, Perencevich EN. Addressing the Emergence and Impact of Multidrug-Resistant Gram-Negative Organisms: a Critical Focus for the Next Decade. Infect Control Hosp Epidemiol. 2014;35(4):333–335. doi:10.1086/675592
37. Mbwasi R, Mapunjo S, Wittenauer R, et al. National Consumption of Antimicrobials in Tanzania: 2017–2019. Front Pharmacol. 2020;11:2017–2019. doi:10.3389/fphar.2020.585553
38. Mthombeni TC, Burger JR, Lubbe MS, Julyan M. Antibiotic consumption by Access, Watch and Reserve index in public sector of Limpopo province, South Africa: 2014–2018. S Afr J Infect Dis. 2022;37(1):1–9.
39. Klein EY, Milkowska-Shibata M, Tseng KK, et al. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–15: an analysis of pharmaceutical sales data. Lancet Infect Dis. 2021;21(1):107–115. doi:10.1016/S1473-3099(20)30332-7
40. MAAP Annual Report. National Situation of Antimicrobial Resistance and Consumption Analysis from 2017–2019: Cameroon. 2017.;
41. Huttner A, Bielicki J, Clements MN, et al. Oral amoxicillin and amoxicillin–clavulanic acid: properties, indications and usage. Clin Microbiol Infect. 2020;26(7):871–879. doi:10.1016/j.cmi.2019.11.028
42. Kaur SP, Rao R, Nanda S. Amoxicillin: a broad spectrum antibiotic. Int J Pharm Pharm Sci. 2011;3(3):30–37.
43. Tadesse BT, Ashley EA, Ongarello S, et al. Antimicrobial resistance in Africa: a systematic review. BMC Infect Dis. 2017;17(1):1–17. doi:10.1186/s12879-017-2713-1
44. Kowalski M, Minka Obama B, Catho G, et al. Antimicrobial resistance in Enterobacterales infections among children in sub-Saharan Africa: a systematic review and meta-analysis. EClinlMed. 2024;70(March):102512. doi:10.1016/j.eclinm.2024.102512
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.