")
Back to Journals » Infection and Drug Resistance » Volume 16
Antibacterial Activity of Eravacycline Against Carbapenem-Resistant Gram-Negative Isolates in China: An in vitro Study
Authors Zou X , Jin S, Chen L, Li J, Zhang X, Zhou H , Li X , Huang H
Received 13 November 2022
Accepted for publication 23 March 2023
Published 17 April 2023 Volume 2023:16 Pages 2271—2279
DOI https://doi.org/10.2147/IDR.S396910
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xuehan Zou,1,* Shaojun Jin,2,* Lingxia Chen,1,* Jie Li,1 Xiaofan Zhang,3 Hua Zhou,4 Xi Li,3 Haijun Huang1
1Center for General Practice Medicine, Department of Infectious Diseases, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China; 2Department of Emergency, Zhuji People’s Hospital of Zhejiang Province, Shaoxing, Zhejiang, People’s Republic of China; 3Laboratory Medicine Center, Department of Clinical Laboratory, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Respiratory and Critical Care Medicine, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haijun Huang, Center for General Practice Medicine, Department of Infectious Diseases, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, 310014, People’s Republic of China, Tel/Fax +86-0571-8589-3603, Email [email protected] Xi Li, Laboratory Medicine Center, Department of Clinical Laboratory, Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College, Hangzhou, Zhejiang, 310014, People’s Republic of China, Tel/Fax +86-0571-8589-3267, Email [email protected]
Objective: Eravacycline is a novel, fully synthetic fluorocycline antibiotic being developed for the treatment of serious infections, with a broad-spectrum antimicrobial activity, including against carbapenem-resistant gram-negative bacteria (CRGNB). However, the in vitro activity of eravacycline against CRGNB has not been well known in China. In this study, we analysed the antibacterial activity of eravacycline against CRGNB isolates in order to provide a theoretical basis for the clinical treatment.
Methods: A total of 346 isolates of CRGNB were collected from two different tertiary care hospitals in Zhejiang, China. Carbapenem resistance genes of all isolates were detected by polymerase chain reaction. And we analysed the in vitro activity of eravacycline against CRGNB by antimicrobial susceptibility tests. In addition, the time-kill curves were generated to evaluate the antibacterial effect of tigecycline and eravacycline.
Results: Four different types of carbapenem-resistant isolates were collected, including 50 Escherichia coli isolates, 160 Klebsiella pneumoniae isolates, 42 Enterobacter cloacae complex isolates, and 94 Acinetobacter baumannii isolates. The carbapenem resistance genes were identified in 346 isolates, including blaKPC-2 (48.0%), blaOXA-23 (27.2%), blaNDM-1 (23.1%), and blaNDM-16 (0.3%). The antimicrobial susceptibility testing results showed that the minimum inhibitory concentration (MIC) values of 346 isolates were within the sensitivity range (≤ 0.0625~16 mg/L) and that the MIC50 or MIC90 of eravacycline was generally approximately 2-fold lower than tigecycline. In addition, the time-kill curves showed that the bactericidal effect of eravacycline was stronger than that of tigecycline against four different types of isolates.
Conclusion: Our research indicated that eravacycline had a good antibacterial effect on CRGNB, which could provide a theoretical basis for the clinical treatment of drug-resistant bacterial infections in the future.
Keywords: eravacycline, tigecycline, carbapenem-resistant, gram-negative isolates, drug sensitivity, time-kill curves
Introduction
Carbapenem-resistant gram-negative bacteria (CRGNB) strains are highly prevalent around the world and were ranked as the highest priority threat by the World Health Organization (WHO) in 2017.1 In China, the incidence of carbapenem-resistant Enterobacteriaceae infections alone is 4.0/10,000, much higher than in other countries.2,3 Despite major preventative efforts, CRGNB continue to spread rapidly worldwide and pose a considerable threat to public health.4 A systematic meta-analysis reported that the mortality rate attributed to carbapenem-resistant Enterobacteriaceae infection is up to 50%,5 especially bloodstream infections.6 Furthermore, the morbidity and mortality of patients infected with carbapenem-resistant pathogens are significantly higher than those infected with antibiotic-sensitive pathogens in the clinic, which may be due to the poor antibacterial effect of the antibiotics.7,8 Tigecycline, colistin, and ceftazidime-avibactam have become the last choice for the treatment of infections caused by CRGNB.9 With the application of these drugs, the identification of resistant isolates has begun to increase. Notably, some isolates even have multidrug-resistant phenotypes. For example, strains coharboring tigecycline-, colistin-, and ceftazidime-avibactam-resistance phenotypes have been identified,10 which will undoubtedly accelerate the formation of “superdrug bacteria”. Thus, for infections caused by multidrug-resistant bacteria, the options for antimicrobial therapy are very limited. There is an urgent need to develop new drugs or combinations thereof for the treatment of infection by these “superbugs”.
Eravacycline, a novel fully synthetic fluorocycline antibiotic, has broad-spectrum antimicrobial activity against antibiotic-resistant pathogens, including gram-positive cocci, gram-negative bacilli (except Pseudomonas aeruginosa and Burkholderia spp.), anaerobes, atypical bacterial pathogens and Neisseria gonorrhoeae.11,12 This drug was approved in 2014 by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) to treat complicated intra-abdominal infections, complicated urinary tract infections (cUTIs), and pulmonary infections.11,13 Similar to tetracyclines, eravacycline can bind to the 30S subunit of the bacterial ribosome and inhibit bacterial protein synthesis,14 but the antibacterial effect can be enhanced by two key modifications in the chemical structure, the fluorine atom in the C-7 side chain and the pyrrolidine acetamide group in C-9.15 The chemical structures of eravacycline and tigecycline were shown in Figure 1. Therefore, it may have advantages in terms of in vitro activity, pharmacokinetics, and tolerability.16 An impressive safety profile has been demonstrated among members of this class in Phase I to III trials.14 However, eravacycline susceptibility in a large number of CRGNB in China is largely unknown.
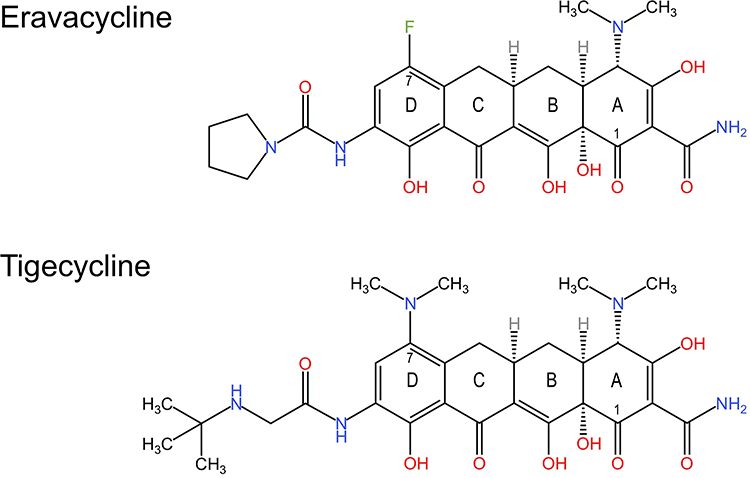 |
Figure 1 Chemical structures of eravacycline and tigecycline. |
The objective of the current study was to evaluate the in vitro activities of eravacycline against CRGNB. In addition, we compared the bactericidal effect of eravacycline and tigecycline on CRGNB by time-kill curves.
Materials and Methods
Bacterial Isolates
A total of 346 CRGNB isolates were collected from two tertiary hospitals in Hangzhou, including 50 E. coli isolates, 160 K. pneumoniae isolates, 42 Enterobacter cloacae complex isolates, and 94 A. baumannii isolates. All isolates were identified using a VITEK MS mass spectrometer (bioMérieux, Marcy l’Etoile, France).
Detection of Carbapenem Resistance Genes
All isolates were tested for the presence of carbapenem resistance genes by polymerase chain reaction (Biometra GmbH, Germany) with specific primers and conditions as previously described.17,18 The amplification parameters were, initial denaturation at 95 °C for 10 min, 36 cycles of 95 °C for 30s, 52 °C for 30s and 72 °C for 50s, with 6 min at 72 °C for final extension. The amplification products were analysed by electrophoresis on 1.0% agarose gels.
Antimicrobial Susceptibility
Antimicrobial susceptibility testing was performed by the broth microdilution method according to the Clinical and Laboratory Standards Institute (CLSI) guidelines.19 All isolates tested were stored in a −80 °C refrigerator. Eravacycline and tigecycline (MedChemExpress, Shanghai, China) were freshly prepared in sterile water on the day of use. The final inoculum of 1.5×108 CFU/mL was acquired by adjusting the turbidity of the incubated mixture to 0.5 McFarland standards using normal saline.20 Aliquots (100 μL) of the colony suspension were inoculated into 96-well broth microdilution panels (Corning, NY, USA) containing 200 μL aliquots of eravacycline and tigecycline (<0.0625, 0.0625, 0.125, 0.25, 0.5, 1, 2, 4, 8, and 16 mg/L). And 96-well broth microdilution panels were read visually after incubation for 16–20 hours at 37 °C. The results of this study were interpreted according to the criteria of the European Committee on Antimicrobial Susceptibility (EUCAST) (http://www.eucast.org) and the Food and Drug Administration (FDA) (https://www.fda.gov/).21,22 E. coli ATCC 25922 was used as a quality control strain.
Time-Kill Curves
A time-kill assay was performed in triplicate on four representative isolates as described in a previous study.23 Based on all minimum inhibitory concentration (MIC) values of the four types of strains, a strain with the same MIC for tigecycline and eravacycline was selected. The MIC of the isolate was used as the reference concentration of the antibiotic.24–26 Briefly, isolates were incubated in Mueller-Hinton broth (Thermo Fisher, Shanghai, China) to mid-log phase (OD600 of 0.25 to 0.3), at which point antibiotics at concentrations of 1 ×, 2 ×, and 4 × MIC were added (P-values <0.05, Two-way Repeated Measures ANOVA), followed by shaking at 37 °C. Subsequently, culture samples were removed at 0, 2, 4, 6, 8, and 24 hours, serially diluted with saline, plated on Mueller-Hinton agar (Bio-Kont, Wenzhou, China), and incubated for 16–18 hours at 37 °C to determine the number of CFU/mL and to plot the time-kill curves.
Statistical Analysis
The extracted data were entered into Excel version 19 and exported to SPSS version 26 for data analysis. The cumulative percentage of MIC and antimicrobial susceptibility were calculated for 346 isolates using SPSS version 26. The Wilcoxon Signed Ranks Test was used to analyse the significance of the differences between groups. The Two-way Repeated Measures ANOVA was used to analyse the data of the time-kill curves. P-values <0.05 was considered to be significant. Figures were drawn using GraphPad Prism 8 and KingDraw.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki and was reviewed and approved by the Research Ethics Committee of Zhejiang Provincial People’s Hospital (QT2022307).
Results
Carbapenem Resistance Genes
The carbapenem resistance genes of the 346 carbapenem isolates are shown in Table 1. Of the 50 E. coli isolates, 47 isolates were blaNDM-1, one isolate was blaNDM-16, and 2 isolates were blaKPC-2. Of the 160 K. pneumoniae isolates all carried blaKPC-2. Of the 42 E. cloacae complex isolates, 33 isolates were blaNDM-1, 4 isolates were blaKPC-2, and 5 isolates carried other carbapenem resistance genes. And 94 A. baumannii isolates were all blaOXA-23.
 |
Table 1 Carbapenem Resistance Genes of 346 Carbapenem-Resistant Isolates |
MIC Distribution
The cumulative percentage and the MIC distributions of 346 selected carbapenem-resistant bacteria tested with eravacycline and tigecycline are shown in Tables 2–3.
 |
Table 2 Cumulative Percentage of MIC Values of Eravacycline and Tigecycline (%) |
 |
Table 3 Drug Sensitivity Distribution of 346 Carbapenem-Resistant Isolates to Eravacycline and Tigecycline (Mg/L) |
For carbapenem-resistant E. coli (CRE) isolate, the MIC50 and MIC90 for both eravacycline and tigecycline were 0.25 mg/L and 0.5 mg/L, respectively. The MIC distribution range of eravacycline was ≤0.0625 to 4 mg/L and that of tigecycline was ≤0.0625 to 1 mg/L. The results showed that tigecycline had a lower MIC distribution than eravacycline for CRE isolates.
For CRKP isolates, the MIC50 and MIC90 for eravacycline were 0.5 mg/L and 2 mg/L, respectively. The MIC50 and MIC90 for tigecycline against CRKP isolates were 1 mg/L and 2 mg/L, respectively. Eravacycline and tigecycline had the same MIC distribution against K. pneumoniae and A. baumannii (≤0.0625 to 16 mg/L).
For carbapenem-resistant E. cloacae complex (CREC) isolates, the MIC50 and MIC90 for eravacycline were 1 mg/L and 4 mg/L, respectively. The MIC50 and MIC90 of tigecycline against these CREC isolates were 0.5 mg/L and 4 mg/L, respectively. In addition, the same MIC distribution (0.25 mg/L to 8 mg/L) for tigecycline and eravacycline was observed in the CREC isolates.
For carbapenem-resistant A. baumannii (CRAB) isolates, the MIC50 and MIC90 for eravacycline were 1 mg/L and 4 mg/L, and the MIC50 and MIC90 for tigecycline were 2 mg/L and 8 mg/L. The results showed that A. baumannii had lower MIC50 and MIC90 values for eravacycline than for tigecycline.
Antimicrobial Susceptibility
Table 4 provides details on the in vitro activities of eravacycline and tigecycline agents against CRE, CRKP, CREC, and CRAB isolates, including percent susceptibility according to the EUCAST and FDA breakpoints. A total of 6.0% of E. coli, 3.1% of K. pneumoniae, 4.8% of E. cloacae complex, and 14.9% of A. baumannii isolates were tigecycline-resistant. Tigecycline had a high antibacterial activity against Enterobacteriaceae, and the susceptibility rate was greater than 90%. The susceptibility of E. coli was 92% to eravacycline and 94% to tigecycline. The susceptibility of K. pneumoniae and the E. cloacae complex to eravacycline was 53.1% and 45.2%, respectively. Since A. baumannii did not have breakpoints for eravacycline, the sensitivity rate could not be calculated.
 |
Table 4 Sensitivity Analysis of 346 Carbapenem-Resistant Isolates to Eravacycline and Tigecycline |
Time-Kill Curves Assay
Four selected CRGNB in vitro were evaluated by time-kill curves to compare the bactericidal effect between eravacycline and tigecycline (Figure 2).
 |
Figure 2 Time-kill curves of four types of carbapenem-resistant bacteria against eravacycline and tigecycline. (A and B): Isolate CRE4032. (C and D): Isolate CRKP5146. (E and F): Isolate CREC5512. (G and H): Isolate CRAB4124. The dashed line indicates the lower limit of detection. Abbreviations: CRE, carbapenem-resistant E. coli; CRKP, carbapenem-resistant K. pneumoniae; CREC, carbapenem-resistant E. cloacae complex; CRAB, carbapenem-resistant A. baumannii; CFU, colony-forming unit. |
Isolate CRE4032 had the same MIC for eravacycline and tigecycline (0.25 mg/L), and the time-kill curves showed that 1 ×, 2 ×, and 4 × MIC of tigecycline and eravacycline showed stable bactericidal or inhibitory effects against it (Figure 2A and B).
Isolate CRKP5146 had the same MIC for eravacycline and tigecycline (0.5 mg/L). The time-kill curves showed that it was inhibited by 1 × and 2 × MIC of tigecycline for the first 8 hours compared to the initial counts and then resumed a normal growth rate and exceeded the initial inoculum, while 4 × MIC of tigecycline stably inhibited its growth rate. For eravacycline, 1 × MIC inhibited this isolate, although it resumed a normal growth rate after 8 hours, while 2 × and 4 × MIC of eravacycline had a stronger bactericidal effect (Figure 2C and D). The results indicated that eravacycline exhibited a better bacterial inhibitory effect against CRKP than tigecycline.
Isolate CREC5512 had the same MIC for eravacycline and tigecycline (0.25 mg/L), and the time-kill curves showed that 1 ×, 2 ×, and 4 × MIC of tigecycline had a good inhibitory effect in the first 8 hours, after which normal growth resumed in all cases. The 1×, 2 ×, and 4 × MIC of eravacycline inhibited this isolate; at 1× and 2 × MIC, this isolate resumed growth after 8 hours at a slow rate, while the 4 × MIC maintained a stable inhibitory effect (Figure 2E and F). The results indicated that eravacycline had a better inhibitory effect than tigecycline.
Isolate CRAB4124 had the same MIC for eravacycline and tigecycline (0.5 mg/L), and the time-kill curves showed that at 1× and 2 × MIC of tigecycline, the bacterial solution concentration decreased to 0 after 6 and 8 hours, respectively. At 4 × MIC of tigecycline, the bacterial solution concentration decreased to 0 after six hours, followed by regrowth, but tigecycline still exerted a strong bactericidal effect. Eravacycline at 1 ×, 2 ×, and 4 MIC had a robust bactericidal effect on this isolate (Figure 2G and H). The results indicated that both eravacycline and tigecycline had a good bactericidal effect on CRAB.
In the time-kill curves, the results showed that eravacycline and tigecycline did not achieve complete bactericidal effects in long-term treatment. Some of these strains appeared to show evidence of transient bactericidal activity after treatment with high concentrations of eravacycline or tigecycline, but they returned to normal or slow growth after 8 hours. However, all isolates treated with eravacycline and tigecycline achieved early bactericidal effects, even at lower concentrations.
Discussion
In the present study, we investigated 346 strains containing four different types of carbapenem-resistant strains, which fell within the range (≤0.0625 to 16 mg/L) indicating drug sensitivity. Previous study results indicated that most carbapenem-resistant Enterobacteriaceae and CRAB isolates had an MIC range of ≤0.06 to 8 mg/L for eravacycline.27,28 Our results are similar to those reported above.
The FDA susceptibility breakpoint is ≤ 0.5 mg/L for eravacycline against E. coli.22 Our data suggested that the MIC90 of eravacycline against E. coli was 0.5 mg/L. The results indicated that eravacycline had robust in vitro antibacterial activity. In addition, a recent study suggested that K. pneumoniae isolates from China have a higher MIC for eravacycline than isolates from Europe, USA, and Canada.12,29 In this study, the MIC90 for eravacycline was 2.0 mg/L against K. pneumoniae, which is consistent with this statement. This may be due to the expression of efflux pumps, resistance mutations, and environmental and regional differences.12,29–32 In a previously published study, we reported two plasmids co-harboring the tmexCD2-toprJ2 gene cluster and carbapenem resistance genes in two clinical ST11 CRKP strains. In addition, we identified tigecycline resistance gene clusters in CRKP strains carrying blaNDM-1 or blaKPC-2. The spread of these resistance gene clusters in CRKP poses a substantial threat in the clinical therapeutic setting and exacerbates the antimicrobial resistance crisis.10 Notably, Table 3 shows that the MIC50 and MIC90 of eravacycline were 2-fold lower than those of tigecycline, especially CRAB, in accordance with previous studies.12,15,33,34 In short, the in vitro activity of eravacycline is much more potent than that of tigecycline. This phenomenon is attributed to the modification of two key positions in the structure of eravacycline, resulting in enhanced antimicrobial potency in vitro.15,35
In the time-kill curves of tigecycline, we also found that CRKP5146 and CREC5512 treated with 1 × and 2 × MIC of tigecycline resumed normal growth after 8 hours. However, the two isolates treated at 4 × MIC of tigecycline were well inhibited (Figure 2). This suggests that we are prone to treatment failure when we apply insufficient starting drug concentrations and should pay more attention to drug doses in clinical settings. Moreover, it was also clearly observed in the time-kill curves that the bactericidal effect of eravacycline was stronger than that of tigecycline for four different types of strains (Figure 2). In Table 4, we identified 24 tigecycline-resistant isolates, including 3 E. coli isolates, 5 K. pneumoniae isolates, 2 E. cloacae complex isolates, and 14 A. baumannii isolates. We observed that tigecycline showed poor in vitro antibacterial activity against A. baumannii relative to other bacteria. Interestingly, the results also showed that 90% of tigecycline-resistant isolates were equally resistant to eravacycline. This phenomenon may be attributed to the presence of resistance genes and efflux pumps.36–40 In addition, comparing the drug sensitivity results of K. pneumoniae and E. coli in Table 4 showed that K. pneumoniae was less susceptible to eravacycline and tigecycline than E. coli. This was also demonstrated in the time-kill curves (Figure 2). In brief, the time-kill curves showed that eravacycline had better bactericidal activity and a longer drug half-life against Enterobacteriaceae and A. baumannii than tigecycline, further indicating that eravacycline is promising for clinical application and may be an important option for the treatment of CRGNB infections.
Notably, our study has some potential limitations. Our studies are based on in vitro evidence of antimicrobial activity; therefore, the effect of application in humans could not be determined, and it is not known whether there is an effect in humans. The number of cases and specimens is not representative of the whole population, and more studies are needed to more fully evaluate the antibacterial activity of eravacycline.
Conclusions
In this study, we demonstrated that eravacycline exhibited a high antibiotic potency on CRGNB, especially on CRKP and CREC. In addition, we observed that CRGNB showed an increasing trend in MIC values for eravacycline and tigecycline, and carried carbapenem resistance genes such as blaKPC and blaNDM. Therefore, eravacycline usage in clinics should receive more surveillance in its susceptibility.
Ethical Approval
This study was conducted in accordance with the Declaration of Helsinki and was reviewed and approved by the Research Ethics Committee of Zhejiang Provincial People’s Hospital (QT2022307).
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No. 82172306), Public Technology Research Projects of Zhejiang Province, China (LGD21H190001), and the Medical and Health Research Project of Zhejiang Province, China (2022KY531).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. Prioritization of pathogens to guide discovery, research and development of new antibiotics for drug resistant bacterial infections, including tuberculosis. World Health Organization; 2017; Available from: http://www.who.int/medicines/areas/rational_use/prioritization-of-pathogens/en/.
2. Zhang Y, Wang Q, Yin Y, et al. Epidemiology of carbapenem-resistant enterobacteriaceae infections: report from the China CRE network. Antimicrob Agents Chemother. 2018;62(2):e01882–17.
3. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of carbapenem-resistant enterobacteriaceae: data from a longitudinal large-scale CRE study in China (2012–2016). Clin Infect Dis. 2018;67(suppl_2):S196–S205.
4. Ambler RP. The structure of beta-lactamases. Philos Trans R Soc Lond B Biol Sci. 1980;289(1036):321–331.
5. Zhou R, Fang X, Zhang J, et al. Impact of carbapenem resistance on mortality in patients infected with Enterobacteriaceae: a systematic review and meta-analysis. BMJ Open. 2021;11(12):e054971.
6. Gutiérrez-Gutiérrez B, Salamanca E, de Cueto M, et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae (INCREMENT): a retrospective cohort study. Lancet Infect Dis. 2017;17(7):726–734.
7. El Chakhtoura NG, Saade E, Iovleva A, et al. Therapies for multidrug resistant and extensively drug-resistant non-fermenting gram-negative bacteria causing nosocomial infections: a perilous journey toward ‘molecularly targeted’ therapy. Expert Rev Anti Infect Ther. 2018;16(2):89–110.
8. Martin A, Fahrbach K, Zhao Q, Lodise T. Association between carbapenem resistance and mortality among adult, hospitalized patients with serious infections due to enterobacteriaceae: results of a systematic literature review and meta-analysis. Open Forum Infect Dis. 2018;5(7):ofy150.
9. Doi Y. Treatment options for carbapenem-resistant gram-negative bacterial infections. Clin Infect Dis. 2019;69(Suppl 7):S565–S575.
10. Li X, Wang W, Jin X, et al. Emergence of plasmids co-harboring carbapenem resistance genes and tmexCD2-toprJ2 in sequence type 11 carbapenem resistant Klebsiella pneumoniae strains. Front Cell Infect Microbiol. 2022;12:902774.
11. Scott LJ. Eravacycline: a review in complicated intra-abdominal infections. Drugs. 2019;79(3):315–324.
12. Zhanel GG, Baxter MR, Adam HJ, Sutcliffe J, Karlowsky JA. In vitro activity of eravacycline against 2213 gram-negative and 2424 GRAM-positive bacterial pathogens isolated in Canadian hospital laboratories: CANWARD surveillance study 2014–2015. Diagn Microbiol Infect Dis. 2018;91(1):55–62. doi:10.1016/j.diagmicrobio.2017.12.013
13. Thakare R, Dasgupta A, Chopra S. Eravacycline for the treatment of patients with bacterial infections. Drugs Today. 2018;54(4):245–254.
14. Alosaimy S, Abdul-Mutakabbir JC, Kebriaei R, Jorgensen SCJ, Rybak MJ. Evaluation of Eravacycline: a Novel Fluorocycline. Pharmacotherapy. 2020;40(3):221–238.
15. Lee YR, Burton CE. Eravacycline, a newly approved fluorocycline. Eur J Clin Microbiol Infect Dis. 2019;38(10):1787–1794.
16. Thaden JT, Pogue JM, Kaye KS. Role of newer and re-emerging older agents in the treatment of infections caused by carbapenem-resistant Enterobacteriaceae. Virulence. 2017;8(4):403–416.
17. Poirel L, Walsh TR, Cuvillier V, Nordmann P. Multiplex PCR for detection of acquired carbapenemase genes. Diagn Microbiol Infect Dis. 2011;70(1):119–123.
18. Woodford N, Ellington MJ, Coelho JM, et al. Multiplex PCR for genes encoding prevalent OXA carbapenemases in Acinetobacter spp. Int J Antimicrob Agents. 2006;27(4):351–353.
19. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing. M100-S30. Pittsburgh, PA: Clinical and Laboratory Standards Institute; 2020.
20. Fakri Mustafa Y, Riyadh Khalil R, Tareq Mohammed E, Bashir MK, Khudhayer Oglah M. Effects of structural manipulation on the bioactivity of some coumarin-based products. Arch Razi Inst. 2021;76(5):1297–1305.
21. European Committee on Antimicrobial Susceptibility Testing (EUCAST). Breakpoint tables for interpretation of MICs and zone diameters. Version 9.0; 2019. Available from: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_9.0_Breakpoint_Tables.pdf.
22. US Food and Drug Administration (FDA). Eravacycline–injection products. FDA-identified interpretive criteria. MD: Food and Drug Administration; 2019. Available from: https://www.fda.gov/drugs/development-resources/tigecycline-injection-products.
23. Soudeiha M, Dahdouh EA, Azar E, Sarkis DK, Daoud Z. In vitro evaluation of the colistin-carbapenem combination in clinical isolates of A. baumannii using the checkerboard, etest, and time-kill curve techniques. Front Cell Infect Microbiol. 2017;7:209.
24. Flamm RK, Rhomberg PR, Lindley JM, Sweeney K, Ellis-Grosse EJ, Shortridge D. Evaluation of the bactericidal activity of fosfomycin in combination with selected antimicrobial comparison agents tested against gram-negative bacterial strains by using time-kill curves. Antimicrob Agents Chemother. 2019;63(5):e02549–18.
25. Ferro BE, Van Ingen J, Wattenberg M, Van Soolingen D, Mouton JW. Time-kill kinetics of antibiotics active against rapidly growing mycobacteria. J Antimicrob Chemother. 2015;70(3):811–817.
26. Schwameis R, Erdogan-Yildirim Z, Manafi M, Zeitlinger MA, Strommer S, Sauermann R. Effect of pulmonary surfactant on antimicrobial activity in vitro. Antimicrob Agents Chemother. 2013;57(10):5151–5154.
27. Clark JA, Kulengowski B, Burgess DS. In vitro activity of eravacycline compared with tigecycline against carbapenem-resistant Enterobacteriaceae. Int J Antimicrob Agents. 2020;56(6):106178.
28. Seifert H, Stefanik D, Sutcliffe JA, Higgins PG. In-vitro activity of the novel fluorocycline eravacycline against carbapenem non-susceptible Acinetobacter baumannii. Int J Antimicrob Agents. 2018;51(1):62–64.
29. Zheng JX, Lin ZW, Sun X, et al. Overexpression of OqxAB and MacAB efflux pumps contributes to eravacycline resistance and heteroresistance in clinical isolates of Klebsiella pneumoniae. Emerg Microbes Infect. 2018;7(1):139.
30. Lee YL, Ko WC, Lee WS, et al. In-vitro activity of cefiderocol, cefepime/zidebactam, cefepime/enmetazobactam, omadacycline, eravacycline and other comparative agents against carbapenem-nonsusceptible Enterobacterales: results from the Surveillance of Multicenter Antimicrobial Resistance in Taiwan (SMART) in 2017–2020. Int J Antimicrob Agents. 2021;58(3):106377.
31. Xu C, Wei X, Jin Y, et al. Development of resistance to eravacycline by Klebsiella pneumoniae and collateral sensitivity-guided design of combination therapies. Microbiol Spectr. 2022;10(5):e0139022.
32. Abdallah M, Olafisoye O, Cortes C, Urban C, Landman D, Quale J. Activity of eravacycline against Enterobacteriaceae and Acinetobacter baumannii, including multidrug-resistant isolates, from New York City. Antimicrob Agents Chemother. 2015;59(3):1802–1805.
33. Monogue ML, Thabit AK, Hamada Y, Nicolau DP. Antibacterial efficacy of eravacycline in vivo against gram-positive and gram-negative organisms. Antimicrob Agents Chemother. 2016;60(8):5001–5005.
34. Grossman TH, Murphy TM, Slee AM, Lofland D, Sutcliffe JA. Eravacycline (TP-434) is efficacious in animal models of infection. Antimicrob Agents Chemother. 2015;59(5):2567–2571.
35. Zhanel GG, Cheung D, Adam H, et al. Review of eravacycline, a novel fluorocycline antibacterial agent. Drugs. 2016;76(5):567–588.
36. Yaghoubi S, Zekiy AO, Krutova M, et al. Tigecycline antibacterial activity, clinical effectiveness, and mechanisms and epidemiology of resistance: narrative review. Eur J Clin Microbiol Infect Dis. 2022;41(7):1003–1022.
37. Boukthir S, Dejoies L, Zouari A, et al. In vitro activity of eravacycline and mechanisms of resistance in enterococci. Int J Antimicrob Agents. 2020;56(6):106215.
38. Wen Z, Shang Y, Xu G, et al. Mechanism of eravacycline resistance in clinical Enterococcus faecalis isolates from China. Front Microbiol. 2020;11:916.
39. Shi Y, Hua X, Xu Q, et al. Mechanism of eravacycline resistance in Acinetobacter baumannii mediated by a deletion mutation in the sensor kinase adeS, leading to elevated expression of the efflux pump AdeABC. Infect Genet Evol. 2020;80:104185.
40. Sun J, Chen C, Cui CY, et al. Plasmid-encoded tet(X) genes that confer high-level tigecycline resistance in Escherichia coli. Nat Microbiol. 2019;4(9):1457–1464.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.