")
Back to Journals » International Journal of General Medicine » Volume 16
Anti-NMDA Receptor Autoimmune Encephalitis: Diagnosis and Management Strategies
Received 18 November 2022
Accepted for publication 20 December 2022
Published 4 January 2023 Volume 2023:16 Pages 7—21
DOI https://doi.org/10.2147/IJGM.S397429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Linda Nguyen, Cynthia Wang
Department of Neurology, University of Texas Southwestern Medical Center, Dallas, TX, USA
Correspondence: Linda Nguyen, University of Texas Southwestern Medical Center, 5323 Harry Hines Blvd, Dallas, TX, 75390, USA, Tel +1-214-645-0136, Fax +1-214-645-8238, Email [email protected]
Abstract: Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis is the most recognized form of autoimmune encephalitis. It is characterized by a constellation of neurologic and psychiatric features along with positive NMDAR antibody, which is more sensitive and specific in CSF than serum. All patients should be screened at least once for neoplasm, with ovarian teratoma being found in most tumor-related cases. In the acute phase, first-line immunotherapy, often a combination of high-dose steroids, immunoglobulins, and/or plasma exchange, is strongly recommended. When first-line therapy fails, escalation to second-line immunotherapy, particularly rituximab, can further improve outcomes and prevent relapses. In refractory cases, additional complementary immunotherapies, such as cyclophosphamide, bortezomib and/or tocilizumab may be considered. Relapses occur in 10– 30% of cases, mostly within the first two years from onset. Individuals should be followed up to determine if chronic maintenance therapy is required.
Keywords: anti-NMDAR encephalitis, clinical features, immunotherapies, treatment options
Introduction
Autoimmune encephalitis (AE) refers to an increasingly recognized group of non-infectious, immune-mediated inflammatory brain disorders. Presently, the most recognized is anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis, resulting from production of autoantibodies to the neuronal NMDAR NR1 subunit. These autoantibodies are thought to cause internalization of the NMDAR, along with severe impairment of synaptic plasticity and NMDAR network dysfunction.1 Patients with this disorder present with an acute to subacute decline in cognitive function and neuropsychiatric symptoms, often accompanied by new onset seizures, movement disorder, disturbed sleep, and encephalopathy. It was initially classified as a paraneoplastic syndrome, occurring in young females in association with an ovarian teratoma.2 However, it can occur following other stimuli such as infection and impact men and children.3 Despite the rapidly growing literature on this disorder following its original characterization in 2007,2 there have been no published randomized clinical trials to date. In this review, we will discuss the epidemiology, clinical presentation, and diagnostic and management strategies for anti-NMDAR encephalitis.
Epidemiology
While the exact incidence of anti-NMDAR encephalitis is unknown, it is currently considered the most common form of AE. In an early population-based study, Dubey et al reported that the incidence of AE in Olmsted County, Minnesota increased over time from 0.4/100,000 person-years (1995–2005) to 1.2/100,000 person-years (2006–2015).4 The prevalence of AE on January 1, 2014 was 13.7/100,000, which was comparable to all infectious encephalitides combined (11.5/100,000). The prevalence of anti-NMDAR encephalitis cases was 0.6/100,000.4 Similarly, the incidence of anti-NMDAR encephalitis in Denmark increased from 2009 to 2018, with the lowest rates in 2009/2010 (0 and 0.036/100,000 person-years) and highest rates in 2017/2018 (0.123 and 0.173/100,000 person-years).5 In Fall 2007, the California Encephalitis Project began identifying cases of anti-NMDAR encephalitis and found that anti-NMDAR encephalitis was the leading form of encephalitis from 2007 to 2011 and occurred about four times as frequently as herpes simplex virus 1 and about six times as frequently as West Nile virus or varicella zoster virus.6 It also exceeded those of enteroviral encephalitis, comprising 41% compared to 38% of all cases.6 In a retrospective study of 505 young patients admitted to the intensive care unit (ICU) at a single center in Germany with encephalitis of unknown etiology from June 2004 to 2009, anti-NMDAR encephalitis represented 1% of the admissions.7 With increasing awareness and testing, these numbers will likely continue to rise.
In a recent study involving over 40,000 patients tested at the Mayo Clinic Neuroimmunology Laboratory between January 2018 and December 2019, Kunchok et al reported 3.6% serum and 4.2% cerebral spinal fluid (CSF) analyses were positive for AE antibodies in adults and 4.4% serum and 5.5% CSF analyses were positive in children.8 Of the positive cases, anti-NMDAR antibodies were most commonly observed: 24.6% (adult serum), 53.1% (children serum), 39.7% (adult CSF), and 88.1% (children CSF).8 Female sex and younger age were associated with higher rates of NMDAR detection (odds ratio [OR] 1.32, P<0.01 for female sex; 8.11, P<0.001 for ages 0–20; 6.42, P<0.001 for ages 21–40; and 1.46, P=0.05 for ages 40–65). These observations are similar to previously published cohorts. For example, in a multi-center observational study involving 577 NMDAR cases, the median age was 21 years (Table 1), 37% of whom were under 18 years old, 95% were under 45 years old, and 81% were female.9 This female predominance was less evident in children younger than 12 years and adults older than 45 years.9 In two large single center studies in China, female gender predominated to a lesser degree (65% in one and 54% in another).10,11 The median ages in the two studies were 21 and 26 years (Table 1), respectively.10,11
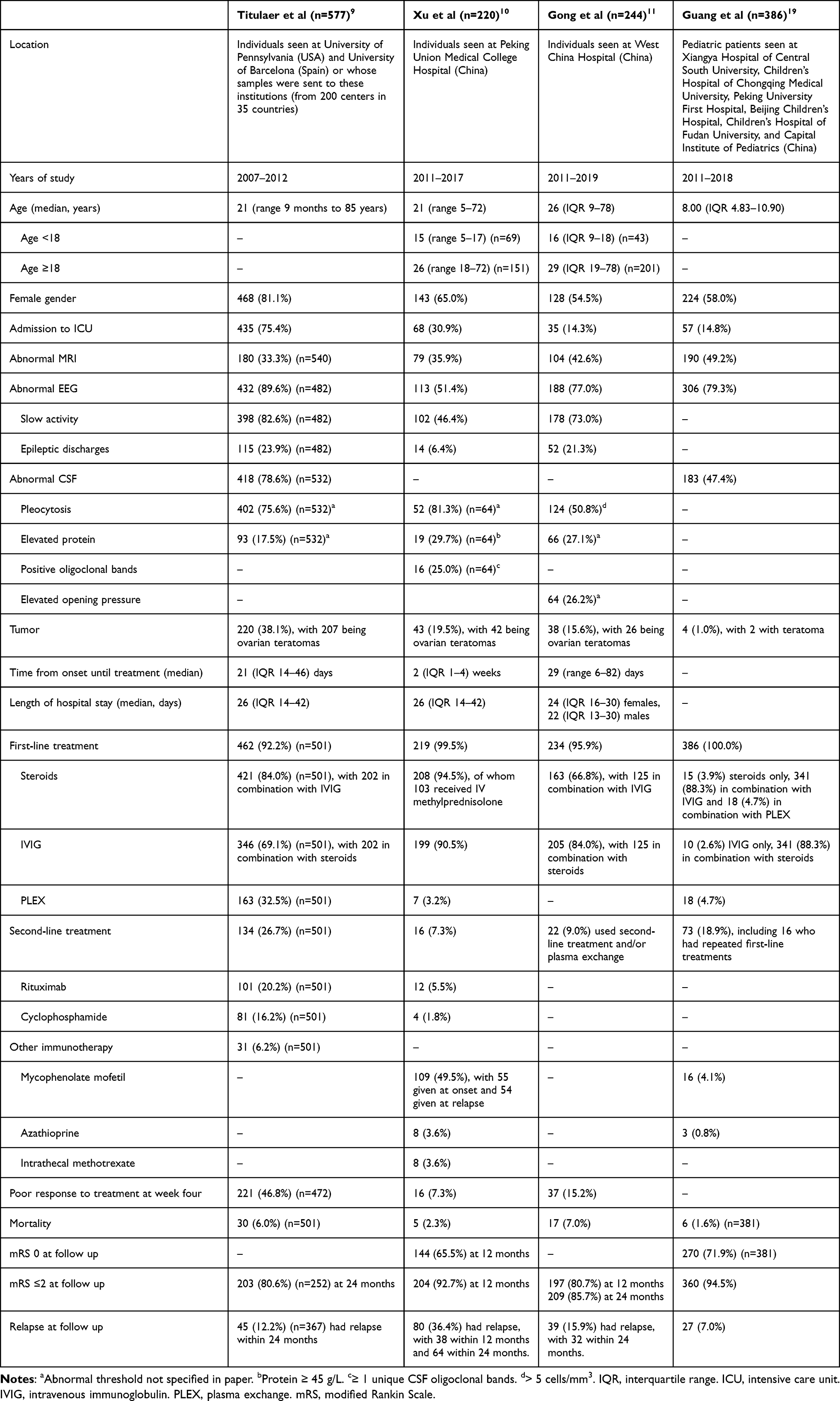 |
Table 1 Summary of Clinical Characteristics, Ancillary Testing, Treatments and Outcomes in Studies with Large Cohort (>200) of Anti-NMDAR Encephalitis Patients |
Clinical Features and Diagnostic Criteria
Anti-NMDAR encephalitis typically presents as a multi-phase clinical deterioration resulting from progressive decrease in NMDAR function due to loss of the receptors from the neuronal cell surface. The initial phase is characterized by the appearance of non-specific prodrome (eg, headache, fever, nausea, vomiting) in 40–70% of patients.3,10–12 Within a few days to two weeks, about 90% of teenagers and adults develop prominent psychiatric or behavioral symptoms that can be difficult to distinguish from a primary psychiatric disease.3 These symptoms are quickly accompanied by neurological findings (seizures, speech dysfunction, involuntarymovements, impaired alertness, memory deficits, autonomic instability, and a decreased level of consciousness). Orolingual-facial dyskinesias are the most characteristic type of involuntary movements. Autonomic manifestations include hyperthermia, hypersalivation, hypo/hypertension, tachy/bradycardia, urinary incontinence, and erectile dysfunction. Central hypoventilation, coma and/or status epilepticus lead 14%-75% of patients to be admitted to the ICU.9–11 Compared to teenagers and adults, young children more frequently present with neurological symptoms (abnormal movements or seizures) instead of psychiatric symptoms. However, behavioral changes can be difficult to interpret as children who often present with temper tantrums, hyperactivity, or irritability rather than frank psychosis. Regardless of the patient’s age and presentation, the clinical picture at three to four weeks after symptom onset is similar in most cases.9
To improve the clinical recognition of anti-NMDAR encephalitis, a group of experts in 2016 developed a set of diagnostic criteria in which a diagnosis of probable anti-NMDAR encephalitis can be made when all three of the proposed criteria are met.20 The first criterion is rapid onset (less than 3 months) of at least four of six major groups of clinical symptoms: abnormal psychiatric, behavior or cognitive dysfunction; speech dysfunction (pressured speech, verbal reduction, mutism); seizures; movement disorder, dyskinesias, or rigidity/abnormal postures; decreased level of consciousness; and autonomic dysfunction or central hypoventilation. The second criterion is presence of abnormal electroencephalogram (EEG) (focal or diffuse slow or disorganized activity, epileptic activity, or extreme delta brush) and/or CSF with pleocytosis or oligoclonal bands. The third criterion is a reasonable exclusion of other disorders. Diagnosis can also be made in the presence of three of the above groups of symptoms accompanied by a systemic teratoma. In a retrospective analysis, 80% (425/532) patients with anti-NMDAR encephalitis met these criteria within the first month of symptom onset, including 74.3% (254/342) without teratoma and 90.5% (171/189) with teratoma.20 These criteria also had good predictive value in a pediatric cohort, in which 89.7% (26/29) of hospitalized anti-NMDAR encephalitis patients fulfilled the criteria compared to 4.1% (3/74) with other causes of encephalitis (acute disseminated encephalomyelitis or enterovirus/herpes simplex virus/mycoplasma encephalitis).13 The sensitivity was 90% and specificity 96%. The median time for fulfilling the criteria was two weeks from symptom onset.
Antibody Testing
A definite diagnosis can be made in the presence of one or more of the six major group of symptoms proposed by Graus et al20 and positive NMDAR antibodies. Demonstration of IgG antibodies against the NR1 subunit of the NMDA receptor in the CSF is more sensitive and specific than serum testing for anti-NMDAR antibodies. Caution should be taken when interpreting an isolated positive result in the serum, as a false positive rate has been reported in as many as 23.2% who had eventual alternative diagnoses or later felt unlikely to have AE.14 In addition, Dahm et al previously reported about 10% positivity for serum NMDA antibody in healthy controls (n=1703) as well as subjects with neuropsychiatric disorders (including schizophrenia, affective disorders, stroke, Parkinson’s disease, amyotrophic lateral sclerosis, and personality disorder; n=2533).15 Several studies have highlighted the importance of CSF testing for NMDAR IgG detection using paired CSF-serum analyses. Gresa-Arribas et al found CSF positivity only in 14.4% (36/250) of presumed anti-NMDAR encephalitis patients in a multi-center retrospective study,16 while Xu et al reported 28.6% CSF positivity only (63/220) in a single-center prospective study.10 Dalmau et al noted of the 431 patients they studied (412 with paired samples), they did not encounter any patient in whom antibodies were only present in the serum.17 A study involving over 10,000 patients uniformly tested for neural antibodies in Bethel, Bielefeld, Germany between December 2011 and 2015 showed that 28% of cases with paired serum-CSF samples were only positive in CSF.18 Similarly, in the Mayo Clinic Laboratory study, CSF was the only compartment that was positive in 38.2% of all patients evaluated for “autoimmune encephalopathy”, CSF and serum were both positive in 48.5%, and serum only positive in 13.3%.8 To avoid false-negative or false-positive results, it is recommended to test NMDAR antibodies in both CSF and serum.
CSF
Aside from positive antibody testing, CSF can have non-specific abnormalities, such as mild lymphocytic pleocytosis, normal or mildly increased protein, and/or CSF specific oligoclonal bands. In an early study of 100 anti-NMDAR encephalitis patients, Dalmau et al reported 91% had lymphocytic pleocytosis, 32% had elevated protein, and 26% had positive oligoclonal bands.12 Titulaer reported 75.6% (402/532) had pleocytosis and 17.5% (93/532) had elevated protein (Table 1).9 Pooling together individual published patient data up until January 2019, Nosadini et al reported 67.8% (618/911) had pleocytosis (>4 cells/µL), 21.6% (189/873) had elevated protein (>50 mg/dL), and 62.6% (223/356) had positive oligoclonal bands. Xu et al reported pleocytosis (median nucleated cell 14, interquartile range 7 to 22.5 x 106/L) in 81.3% of their anti-NMDAR encephalitis patients who had CSF analysis (n=64), 29.7% had elevated protein (median 0.30, interquartile range 0.21 to 0.42 g/L), and 25.0% had at least 1 unique oligoclonal band.10 Gong et al reported only 50.8% (124/244) had pleocytosis (>5 cells/mm3) and 27.1% (66/244) had elevated protein. Guang et al also reported only 47.4% (183/386) children had abnormal CSF studies.19 Increased intracranial pressure can be seen in 26.2%–39.5% patients.11,17
EEG
Typically, EEG is abnormal and may help distinguish between encephalitis and a primary psychiatric disorder, as the rate of abnormal EEG is higher in the anti-NMDAR encephalitis population than in psychiatric patients undergoing screening EEG (17–19%).21,22 In a systematic review of EEG findings in anti-NMDAR encephalitis, Gillinder et al reviewed 446 cases containing EEG data.23 They found EEG was abnormal in 83.6% cases. Non-specific diffuse slowing was seen in 60.3%. Focal abnormalities (slowing or epileptiform discharges) were seen in 18.4%, most commonly in temporal, frontotemporal, and frontal regions. A pattern of EEG activity called “extreme delta brush”, defined as rhythmic delta activity at 1–3 Hz with bursts of rhythmic beta activity superimposed onto each delta wave, is suggested to be specific of this disorder but occurs only in a small subgroup of patients (6.7%). While clinical seizures were present in 65.9% of cases at some point during the illness, epileptiform discharges were only seen in 15.0% and electrographic seizures in 17.7% cases.23 This may be related to timing of EEG during a long illness and poor sensitivity of standard EEG surface electrodes for deeper locations of the epileptogenic zone, such as the perisylvian or mesial prefrontal regions. The meta-analysis by Nosadini et al reported similar findings, noting 84.8% (725/822) had abnormal EEG, 72.2% (594/822) had focal or diffuse slowing or disorganized activity, 29.4% (244/829) had epileptiform discharges, 15.9% (132/829) had seizures recorded, and 6.8% (56/827) showed extreme delta brush.24 Of note, while the Titulaer, Gong, and Guang cohort studies reported similar percentage of abnormal EEGs (90%, 77%, and 79% respectively), the Xu et al study reported only 51.4% had abnormalities.9,10 These discrepancies may be due to varied timing of the initial EEG (patients who present earlier may have a normal EEG at the onset that can progress to show more abnormal findings over time) and differences in technique, EEG interpretation, and EEG modality (routine study vs prolonged video monitoring).
MRI
Brain magnetic resonance imaging (MRI), in contrast to CSF and EEG findings, are normal in most cases. A recent systematic review on MRI abnormalities collectively assessed a total of 1167 patients and found 440 abnormal MRIs (37.7%) in the acute phase.25 The highest abnormal MRI frequency reported in the included studies was 83.3% and lowest was 11.1%. In studies of pediatric or adult only data, 37.7% pediatric patients had abnormal MRI, while 46.5% adults had abnormal MRI. The most reported abnormalities were T2/FLAIR hyperintensities in the temporal lobe (n=91), followed by cortical gray matter (n=42), subcortical white matter (n=42), frontal lobes (n=25), hippocampus (n=25), periventricular region (n=19), and cerebellum (n=14). Leptomeningeal and cortical enhancement were seen in 25 and 19 cases, respectively. Restricted diffusion was reported in 4 cases, with the most common site being the temporal lobes (n=3). No studies described abnormalities on susceptibility-weighted imaging. These results are similar to the meta-analysis by Nosadini et al, which reported 40.6% (434/1069) patients had abnormal MRI and the large cohort study by Titulaer et al,9 which found 33.3% (180/540) patients had abnormal initial MRI. In addition, Xu et al found 35.9% (79/220) had abnormal MRI at onset (14.1% in the medial temporal lobe, 9.1% in frontal lobe, 5.9% each in parietal and occipital lobe, 2.7% in brainstem, and 1.4% in the cerebellum);10 Gong et al reported 42.6% (104/244) had abnormal MRI (13.9% in hippocampi and insular regions, 18.4% in cerebral cortex, 4.1% in deep white matter, 2.9% in thalamus, 3.7% in basal ganglia, 1.6% in brainstem), while Guang et al reported 49.2% (190/386) pediatric patients had abnormal MRI (54.4% cerebral cortex) (Table 1).
Cancer Screening
The frequency of an underlying tumor varies with age and sex. Titulaer et al reported tumor was present in 38.1% (220/577) of all cases (Table 1) and female patients aged 12 to 44 years old accounted for 93.2% (205/220) of the tumor cases. In females, tumor was detected in 5.9% (4/68) of those less than 12 years old, 53.4% (205/384) between 12 and 44 years old, 7.4% (4/54) 45 years and older. Tumor was detected in only 6.4% (7/109) men. Of the tumors detected, 94.1% (207) were ovarian tumors, 2.3% (5) were extraovarian teratomas, and the remaining 4.1% (9) were: lung, breast, or testicular tumors (2 each) and ovarian carcinoma, thymic carcinoma, or pancreatic cancer (1 each). Six of the nine patients with tumors other than teratomas were older than 45 years. Regarding timing of tumor diagnosis, 4.1% had tumor diagnosis before onset of encephalitis, 80.5% concurrently, and 15.0% after. Asian and Black patients were more likely to have a teratoma (44.5% [81/182] Asian patients and 47.5% [38/80] Black patients) than White patients (31.3% [58/185]) or Hispanic patients (27.1% [23/85]). Pooling the Titulaer data and other studies, Nosadini reported 25.6% (389/1524) had associated tumors, of which 80.2% (312/389) were ovarian teratomas, 3.1% (12/389) were other ovarian tumors, and 17.0% (66/389) were extra-ovarian tumors (lung in 11, mediastinum in 6, brain, uterus and lymphoma in 4 each). In a large single center in China, however, tumors were found in only 19.5% (43/220) of patients (median age 21, range 5–72 years): 42 females had ovarian teratomas and 1 male had lung cancer.10 Similarly, Gong et al found tumor in only 15.6% (38/244): 28 ovarian teratoma, 1 mediastinal teratoma, 3 lung cancers, 2 thyroid tumors, 1 thymoma, 1 brain glioma, 1 adrenal carcinoma, 1 bladder cancer. All the patients with non-teratomas were older than 40 years.11 Guang et al showed tumors in only 4 (1.0%) pediatric patients (2 teratoma, 1 optic glioma, 1 Ewing’s sarcoma).19
Based on these data, we recommend that female patients be screened for an ovarian teratoma. The most useful screening tests include pelvic ultrasound, transvaginal ultrasound (if age appropriate) and/or abdominal-pelvic MRI/computed tomography. Serological tumor markers (eg, cancer antigen 125, carbohydrate antigen 19–9, β-human chorionic gonadotrophin, α-fetoprotein, or testosterone) have not been systematically assessed but are negative in many patients.26 If a tumor is not detected, Titulaer et al have proposed a screening approach similar to that of paraneoplastic syndromes (eg, MRI of the abdomen-pelvis every 6 months for 4 years) in female patients aged 12 years and older.9 The need for repeat screening in young children (age less than 12 years) and male patients is unclear.
Treatment Approaches
As specific antibody test results can be delayed, treatment for suspected AE is often given empirically. Early initiation of immunotherapies has been shown to improve outcomes and reduce relapses.9,24 While there remains an absence of randomized clinical trials, there has been recently published management recommendations for all-cause AE in adults and anti-NMDAR encephalitis in children.27–29 Once the diagnosis is confirmed, the treatment approach to anti-NMDAR encephalitis generally involves escalation of immunotherapy alongside teratoma removal where applicable.3,28,29 First-line immunotherapies include high-dose steroids, intravenous immunoglobulins (IVIG) and plasma exchange (PLEX), sequentially or concurrently. Second-line immunotherapies, such as rituximab or cyclophosphamide are used for refractory cases. No studies exist comparing first-line therapies and upfront use of rituximab or cyclophosphamide versus escalation approach. A summary of the treatment options is shown in Table 2.
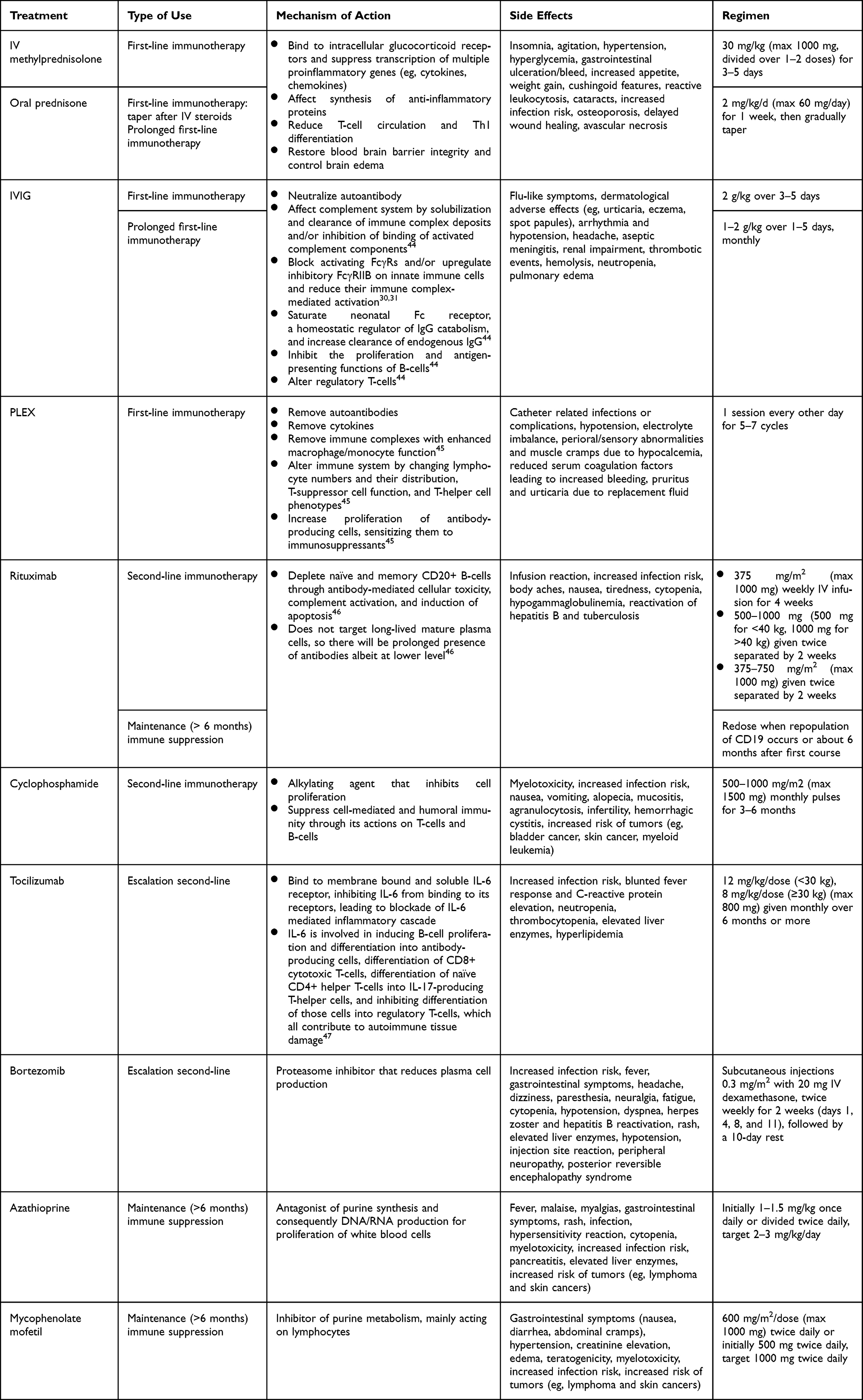 |
Table 2 Summary of Treatment Options |
It is important to note there are no known serological biomarkers to date that help in clinical decision making during the course of the disease. The presence of NMDA antibody is critical to confirming the diagnosis, but there is limited clinical utility in following antibody titers during the disease. This is because 1) absolute titers have only a weak association with clinical severity,32 2) titers in serum do not correlate reliably with disease status, and 3) CSF titers correlate only roughly to disease status within a single patient across multiple samples.16 Thus, treatment decisions should be based on clinical assessment and not changes in antibody titer during the disease. After recovery, most patients still have antibodies in serum and CSF.16 When assessing relapse, CSF titers may be more useful than serum titers and only when compared to earlier samples.16 Therefore, determination of baseline serum and CSF titers after recovery is potentially useful for characterization of clinical worsening or new onset symptoms as possible relapses (ie, increasing titers).
First-Line Therapies
There is consensus that corticosteroids should be the first agent used in anti-NMDAR encephalitis, often in conjunction with IVIG and/or PLEX.28,29
Steroids
Although there is no compelling evidence to suggest the superiority of any specific regimen, IV steroids are frequently the first choice.29 Steroids alone, however, may be insufficient to ameliorate the autoantibody-mediated immune process, and direct removal or neutralization of autoantibodies from the circulation by PLEX and IVIG, respectively, may have a synergistic effect.28 There is increasing evidence to support use of steroid combination therapy over steroid alone. In a prospective study by Gong et al, IVIG plus IV methylprednisolone had a higher response rate compared to IVIG or IV methylprednisolone alone (86.5% vs 55.6% vs 68.7%), improved modified Rankin Scale (mRS) score at 3, 6, and 12 months, and reduced recurrence rate (27.0% vs 24.3% vs 5.4%).33 Moreover, a recent meta-analysis on the use and safety of immunotherapies in anti-NMDAR encephalitis found that use of corticosteroid combination therapy was significantly associated with good functional outcome at 12 months (2.7-fold increased odds with steroids and IVIG, P=0.03; 2.8-fold increased odds with steroids, IVIG and PLEX, P=0.04), while corticosteroids alone was not (1.6-fold increased odds, P=0.32).24
After completing pulsed IV corticosteroid therapy, a common strategy is to start oral prednisone 1–2 mg/kg/day immediately followed by a gradual taper over weeks to months overlapping with long-term immunotherapy if indicated.27 This is used, in theory, to avoid possible relapses. The need for an oral taper and its optimal duration, however, are uncertain.27 In a large multi-center pediatric cohort of anti-NMDAR encephalitis, Guang et al found no difference in complete recovery rate (mRS=0) between patients who received short-term (≤3 months) and long-term (>3 months) regimens, and the absence of an oral prednisolone course was not associated with relapse, suggesting prolonged steroid use may not confer additional benefits.19 An alternative strategy to tapering with oral steroids is repeating another pulse IV steroid therapy (plus optional add-on IVIG) after 4 and 8 weeks to maintain adequate suppression of antibody formation and thereby preventing treatment-related fluctuations.29,34
Steroids have also been utilized for prolonged first-line immunotherapy or maintenance in the form of monthly pulse oral dexamethasone or IV methylprednisolone.29 With regard to corticosteroid therapy as maintenance therapy, Nosadini et al found corticosteroid use for at least 6 months from first event did not significantly affect outcome (2.3-fold increased odds of good outcome, P=0.23) or relapse risk (2.6-fold increased odds relapsing course, P=0.28), suggesting it may not be beneficial in anti-NMDAR encephalitis.
Corticosteroids have various systemic side effects. It may induce or aggravate psychiatric symptoms associated with anti-NMDAR encephalitis, such as depression, insomnia, agitation, and psychosis. The use of corticosteroids may also be difficult in patients with common comorbidities, such as uncontrolled hypertension or diabetes. Close monitoring and good control of blood pressure and blood glucose is needed. To mitigate additional corticosteroid toxicity, it is also important to cotreat with proton pump inhibitors and, if used for an extended period, also vitamin D and calcium supplements and antibiotic prophylaxis against Pneumocystis jiroveci pneumonia when indicated (use of prednisone equivalent doses ≥20 mg/day for more than 4 weeks).
IVIG
IVIG is a pooled preparation of human immunoglobulins obtained from several thousand healthy donors. For patients with medical conditions that restrict the use of corticosteroids, such as uncontrolled hypertension or diabetes or there is concern for active infection, IVIG is often the initial treatment. IVIG has a better side effect profile than corticosteroids and is often more accessible than PLEX.
Certainly, there is evidence to support the use of IVIG in autoimmune neurological diseases. A meta-analysis by Morales-Ruiz et al showed beneficial effect of IVIG administration on patients with various autoimmune neurological conditions over placebo (OR=2.79, P=0.01).35 In addition, a recent randomized blinded study showed IVIG efficacy over placebo in controlling seizures in a small number of patients with leucine-rich glioma-inactivated 1 (LGI1) and contactin-associated protein-like 2 (CASPR2) autoimmune epilepsy.36 Its efficacy compared to other first-line agents, and its clinical benefit as an add-on therapy, remains to be clearly established in AE. As with steroids, there appears to be greater support for the use of IVIG combination therapy rather than monotherapy in first-line treatment of anti-NMDAR encephalitis.24,33 For instance, the meta-analysis by Nosadini et al showed IVIG with steroids or IVIG with steroids and PLEX but not IVIG alone was significantly associated with good functional outcome at 12 months (2.7-fold increased odds, P=0.03 vs 2.8-fold increased odds, P=0.04 vs 2.2-fold increased odds, P=0.19).24 If IVIG is used with PLEX, it is preferable for IVIG to be administered after PLEX because PLEX would clear IVIG from the plasma, negating its benefits. There is some preliminary evidence that patients who receive IVIG after PLEX fared better than those who received IVIG before PLEX.37 Theoretically, after the rapid clearance of pathogenic antibodies and inflammatory mediators by PLEX, the neutralization of reduced autoantibodies by IVIG might help to further improve outcomes of the disease.
Beyond the acute treatment period, some groups have continued IVIG, given every 3–4 weeks, as prolonged first-line immunotherapy or maintenance therapy.24,29 This can be considered relative to a patient’s disease severity and degree of improvement, especially in countries with limited access to second-line therapies.29 The meta-analysis by Nosadini et al found that maintenance IVIG use for 6 months or more from first event was associated with 10.3-fold increased odds of poor functional outcome but 6.3-fold decreased odds of relapsing disease.24 The authors noted that these observations arose from very small subgroup of cases (24/1508), with potential for publication bias of smaller cohorts favoring more atypical clinical features and immunotherapy refractory disease, so caution should be taken in generalizing these findings more widely.
Most of the adverse effects associated with IVIG are mild and transient. Infusion-related reactions including fever and headache are common and can often be controlled by slowing the infusion rate or with symptomatic medications. Serious adverse effects are rare and can include thromboembolic events, renal failure, or aseptic meningitis. To reduce adverse effects, IVIG is usually given in divided doses over 3–5 days. There is also risk of anaphylaxis in patients with selective IgA deficiency, but the incidence is extremely rare. Screening of IgA antibody level prior to the administration of IVIG could be helpful but is not considered mandatory.
PLEX
PLEX is a non-selective extracorporeal blood purification method involving elimination of patient plasma and subsequent substitution with another solution. There is no consensus on the ideal replacement solution, which can be fresh-frozen plasma, albumin, albumin and saline, or albumin and plasma expander solutions. In AE, PLEX is often used in combination with steroids or following steroids rather than initial first-line therapy.24 This is likely in part because it is not easily performed on pediatric patients (due to need for central-line placement) or patients with autonomic instability (due to volume shifts) or those who are poorly cooperative. Another reason may be related to a synergistic effect with combination therapy. A systematic review by Suppiej et al for PLEX in pediatric anti-NMDAR encephalitis suggested a trend toward better outcomes at last follow-up when PLEX is administered early (within 30 days from onset) compared to later (69.4% vs 59.2%) and when given in combination with steroids rather than alone (66.7% vs 46.7%).38 However, in a later meta-analysis, Nosadini et al showed that PLEX alone (5.6-fold increased odds, P=0.03) as well as PLEX plus steroids (3.2-fold increased odds, P=0.05) for first-line immunotherapy were associated with good outcome at 12 months.24 Differences in analyses may be due to the very small subgroup size in both studies (PLEX only in 22/1478 in Nosadini et al study24 and 7/128 in Suppiej et al study38).
There is some evidence that PLEX may provide faster immunomodulation and more rapidly improve clinical manifestations in patients with severe presentations. In a prospective, non-randomized study that enrolled patients with severe anti-NMDA receptor encephalitis who showed no improvement after steroids and/or IVIG for at least 10 days, Zhang et al showed that the PLEX group (n=19) exhibited greater clinical improvement after 1 and 2 months following treatment compared to non-PLEX group (n=21), but not at 3, 6 or 12 months.39 Similarly, in the subsequent analyses that included 51 anti-NMDAR encephalitis patients and 6 other severe refractory antibody-associated AE, the PLEX group (n=33) showed greater clinical improvement after 1 and 2 months, with no significant differences in outcomes after 6 and 12 months compared to non-PLEX group (n=24).40
PLEX is preferred to IVIG in patients with severe renal insufficiency, a prothrombotic tendency, or when IVIG leads to moderate to severe infusion-associated reactions or hyperviscosity syndrome. Most complications of PLEX are mild and related to the use of central venous access, anticoagulation, and/or replacement fluids. Adverse effects that are related to the central venous access are infection and septicemia, thrombosis, and pneumothorax. Citrate infused for anticoagulation or as part of fresh-frozen plasma may lead to hypocalcemia, and less commonly hypomagnesemia, hypokalemia, and metabolic alkalosis. Symptoms of hypocalcemia include paresthesia, muscle cramps, and cardiac arrhythmias in severe cases. Repeated exchanges with albumin replacement may lead to depletion of coagulation factors and immunoglobulins, increasing the risk of bleeding and infections.
Second-Line Therapies
The majority of patients respond to first-line immunotherapy.9,11,19,24 In those who fail to improve within two weeks of initiation of two or more first-line therapies, second-line treatment is recommended over continuing or repeating first-line therapies, with rituximab preferred over cyclophosphamide.29
Rituximab
Rituximab is a B-cell depleting, partially humanized monoclonal antibody directed against CD20 with established efficacy in many autoimmune neurological diseases. Rituximab dosing protocols vary but are all generally accepted (Table 2) as there are no data to support one protocol over another. Circulating levels of B-cells are usually below the detectable range for 6–8 months after treatment. Due to its relatively favorable safety profile, rituximab is the most often used second-line immunotherapy, particularly in children.29
Rituximab use in patients not responding adequately to first-line immunotherapy is generally associated with better outcomes and fewer relapses. In 149 patients with AE from a German registry cohort (54.4% anti-NMDAR), relapses occurred in 19.1% (13/68) for anti-NMDAR, 20.0% (5/25) for anti-LGI1, and 11.1% (1/9) for anti-CASPR2, with fewer relapses occurring after rituximab treatment.41 Although more severely affected prior to treatment, rituximab-treated patients with anti-NMDAR encephalitis more frequently reached independent living (mRS ≤2) than those who did not receive rituximab (94.1% vs 87.5%). Nosadini et al also showed that rituximab was associated with reduced relapses in patients with anti-NMDAR encephalitis (5.9-fold reduced odds of relapse, P<0.001).24 However, in their meta-analysis, rituximab use was not associated with good functional outcome at 12 months (1.12-fold increased odds poor outcome, P=0.66). In addition, in their analysis of changes in immunotherapy use over time, Nosadini et al showed that rituximab use was increased after 2013 (when the Titulaer et al paper9 was published) compared to before 2013. This coincided with a falling relapse rate, but overall functional outcomes did not improve with time, suggesting other factors may be at play.
As rituximab’s effects on suppressing B-cells last for several months and there is a relatively low relapse rate of anti-NMDAR encephalitis, redosing is generally not considered unless there is a relapse or prolonged impairments attributed to ongoing encephalitis.29 Supporting the notion that short-term rituximab might be sufficient to control the disease, the German registry cohort study showed that patients treated with induction or maintenance therapy did not significantly differ in the outcome.41
Mild infusions reactions are frequent after the first infusion and less with the subsequent infusions. Patients are therefore typically premedicated with an antihistamine and acetaminophen prior to dosing. Patients treated with rituximab are at increased risk for infections (mostly upper respiratory tract infections and urinary tract infections), especially in patients with low IgG. Before the start of rituximab, it is important to screen for chronic/latent infections, such as hepatitis B and tuberculosis to avoid disease reactivation during treatment. While the risk is extremely low and has not been reported in AE, there is a black box warning for progressive multifocal leukoencephalopathy, which is a fatal brain infection caused by the JC polyomavirus.
Cyclophosphamide
Cyclophosphamide is an alkylating agent that impairs DNA replication or transcription, eventually leading to programmed cell death. In addition to anti-mitotic and anti-replicative effects, it has immunosuppressive as well as immunomodulatory properties that affect both B and T cells. In contrast to rituximab, which cannot cross the blood-brain barrier, cyclophosphamide has good bioavailability within the central nervous system and may induce local immunomodulation and immunosuppression. However, due to its potentially serious side effects, such as myelosuppression, infertility, hemorrhagic cystitis, and increased risk of malignancy, it is usually less preferable than rituximab as a second-line agent in anti-NMDAR encephalitis. Many reports on cyclophosphamide use, in the absence of rituximab use, are case reports or case series. Large cohort data or systematic reviews often analyze cyclophosphamide together with rituximab under the umbrella of “second-line” immunotherapy, which makes it difficult to interpret the efficacy of cyclophosphamide alone. The multivariate modeling by Nosadini et al found cyclophosphamide was not associated with good outcome (OR=1.29, P=0.40) or non-relapsing disease (OR=0.63, P=0.35).24 A caveat is that 57.1% (79/184) of patients receiving cyclophosphamide also received rituximab, suggesting the patients who received cyclophosphamide may have had a more severe phenotype.
Repeating First-Line Therapy
The use of second-line immunotherapy is still variable globally and can be considerably less frequent in some countries.10,11 In a multicenter pediatric study in China, 21.8% (84/386) patients were treated with a repeated course of first-line immunotherapy (48.1% received IV methylprednisolone and IVIG, 44.2% received IVIG only) followed by second-line agents in 16 patients, while 14.8% (57/386) went directly to second-line immunotherapy. Patients who received second-line, repeated first-line, or both did not show significant differences in complete recovery rate (mRS=0). These data suggest that repeated first-line immunotherapy can be considered when second-line immunotherapy is not possible due to severe adverse effects and high costs, and delaying second-line immunotherapy in patients who received repeated first-line treatments did not affect outcome.19 The authors also found second-line and/or repeat use of first-line immunotherapy were beneficial at reducing relapse rate.
Escalation Second-Line Therapy
In patients with inadequate response to second-line therapies and exhibit persistent neurological issues, it is important to note that anti-NMDAR encephalitis symptoms may take weeks or months to improve. Data from large cohorts reveal that patients continue to improve at 24, even 42 months, after onset.9,11 Therefore, clinicians should allow time for treatments to take effect. In general, it is prudent to wait 1–3 months before making judgements on the effect of second-line agents, with 6 weeks recommended in most accepted guidelines.29 In severe and refractory cases, use of bortezomib and tocilizumab have been reported in a small number of studies.
Bortezomib
Bortezomib is a proteasome inhibitor particularly effective at depleting plasma cells and is approved for the treatment of multiple myeloma. Since long-lived plasma cells are not the target of rituximab and are also resistant to antiproliferative agents, such as cyclophosphamide, bortezomib can represent an alternative option for refractory cases. A recent systematic review on bortezomib in anti-NMDAR encephalitis reported 55.2% (16/29) patients had a favorable outcome.42 Most of the patients were severely disabled when bortezomib was administered with a median mRS of 5 (range 3–5) and had tried a median of 4 prior treatments (range 3–7). Bortezomib was utilized at a median time of 4.9 months after onset and 1 month after the last immunosuppressant treatment. The mRS improved to a median value of 2 (range 0–5) after treatment. Side effects were reported in 37.9% patients, including hematological (8 patients), infectious (3), or gastrointestinal (3), and neuropathy (1) and elevated liver enzymes (2).
Tocilizumab
Tocilizumab is a humanized monoclonal antibody targeting the IL-6 receptor and prevents binding of IL-6. It has potent anti-inflammatory properties and direct impact on plasma cell survival, and thereby antibody production. Similar to bortezomib, tocilizumab may provide added benefit by targeting antibodies produced by long-lived plasma cells that are not directly impacted by rituximab or cyclophosphamide.
There are emerging studies suggesting that tocilizumab is efficacious in refractory AE. Randell et reports on 3 pediatric AE patients (0% anti-NMDAR) who improved within 2–3 weeks of the first dose.43 In a retrospective study of 91 patients (28.6% anti-NMDAR, 65.9% seronegative) who had inadequate response 1 month following an induction regimen of rituximab, Lee et al reported that the addition of tocilizumab was associated with more favorable clinical response at 1 month, 2 months, and at last follow-up compared to additional rituximab and/or observation only.44 The same group conducted a prospective study of 78 patients with anti-NMDAR encephalitis and used mRS and Clinical Assessment Scale for Autoimmune Encephalitis (CASE) as outcome measures. Combination therapy with steroid, IVIG, rituximab, and tocilizumab (SIRT) with or without tumor removal (T) was more effective than SIR or SI regimens in lowering CASE scores. Completion of SIRT-T within 1 month of onset resulted in better 6-month and 1-year improvements in CASE score and mRS compared to other regimens within 1 month or delaying teratoma removal for more than 1 month. Notably, there were relatively high rates of infectious complications in the study (pneumonia in 66.7%, neutropenia in 20.5%).31 Tocilizumab can both increase the risk of infection and hamper the recognition of an infection by diminishing the fever response and the levels of C-reactive protein. For this reason, clinicians should be vigilant about systemic infection in treated patients, especially in those treated with multiple immunomodulatory agents.
Maintenance Therapy
Relapses can occur in 10–30% of cases, usually within the first two years from onset.9–11,19,24 There is no convincing evidence for chronic maintenance immunotherapy in anti-NMDAR encephalitis except for patients with relapses despite second-line immunotherapy or those with severe and prolonged impairments. Re-dosing of rituximab, monthly IVIG for greater than 6 months, and long-term maintenance of prednisolone or steroid-sparing agents, such as azathioprine and mycophenolate mofetil, are among the options that have been used so far.
Emerging Clinical Trials
Inebilizumab
Inebilizumab is a humanized monoclonal antibody against the CD19 B-cell surface antigen. Compared to rituximab, inebilizumab not only depletes CD20+ B-cells but also CD20- plasmablasts and plasma cells, which results in broader and more sustained suppression of B-cells. The ExTINGUISH trial is a Phase 2B randomized double-blind placebo-controlled trial designed to evaluate the safety and efficacy of inebilizumab for the acute treatment of moderate to severe anti-NMDAR encephalitis. The trial is currently underway (NCT04372615). All recruited patients will receive standard first-line immunotherapies prior to randomization. IV cyclophosphamide will be used as rescue for patients who fail to respond to initial treatment (inebilizumab or placebo) after 6 weeks.
Satralizumab
Satralizumab is a subcutaneously administered humanized monoclonal antibody that targets the membrane bound and soluble IL-6 receptor. It was designed based on tocilizumab with a novel antibody-recycling technology, allowing for increased duration of antibody circulation. A Phase III randomized clinical trial in patients with anti-NMDAR and anti-LGI1 encephalitis is pending (NCT05503264).
Conclusions
Anti-NMDAR encephalitis is increasingly being encountered in clinical care. The diagnosis is confirmed with positive antibody testing preferably in the CSF and is supported by abnormal EEG and inflammatory CSF profile, often with normal MRI. Tumor association can be seen in 15–38% of cases, most commonly in females ages 12-45 years old. With regard to treatment, each immunotherapeutic agent has its own strengths and weaknesses, and an appropriate combination of these agents can provide complementary and synergistic modes of action. Early initiation of first-line immunotherapy, often a combination of steroids and IVIG and/or PLEX, is critical. In those who have an inadequate response to first-line immunotherapies, second-line immunotherapy, particularly rituximab, has beneficial effects on outcome and reduces risk of relapse. While much progress has been made in the past 15 years, further studies are needed to optimize currently used regimens and dosing schedules and to develop more targeted and effective treatments with a favorable safety profile.
Abbreviations
AE, autoimmune encephalitis; CASE, clinical assessment scale for autoimmune encephalitis; CASPR2, contactin-associated protein-like 2; CSF, cerebral spinal fluid; EEG, electroencephalogram; ICU, intensive care unit; IVIG, intravenous immunoglobulins; LGI1, leucine-rich glioma-inactivated 1; MRI, magnetic resonance imaging; mRS, modified Rankin Scale; NMDAR, N-methyl-d-aspartate receptor; PLEX, plasma exchange; SIRT-T, steroid, IVIG, rituximab and tocilizumab with tumor removal.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hughes EG, Peng X, Gleichman AJ, et al. Cellular and synaptic mechanisms of anti-NMDA receptor encephalitis. Neurosci J. 2010;30(17):5866–5875. doi:10.1523/JNEUROSCI.0167-10.2010
2. Dalmau J, Tüzün E, Wu H, et al. Paraneoplastic anti–N‐methyl‐D‐aspartate receptor encephalitis associated with ovarian teratoma. Ann Neurol. 2007;61(1):25–36. doi:10.1002/ana.21050
3. Dalmau J, Armangué T, Planagumà J, et al. An update on anti-NMDA receptor encephalitis for neurologists and psychiatrists: mechanisms and models. Lancet Neurol. 2019;18(11):1045–1057. doi:10.1016/S1474-4422(19)30244-3
4. Dubey D, Pittock SJ, Kelly CR, et al. Autoimmune encephalitis epidemiology and a comparison to infectious encephalitis. Ann Neurol. 2018;83(1):166–177. doi:10.1002/ana.25131
5. Nissen MS, Ørvik MS, Nilsson AC, Ryding M, Lydolph M, Blaabjerg M. NMDA-receptor encephalitis in Denmark from 2009 to 2019: a national cohort study. J Neurol. 2022;269(3):1618–1630. doi:10.1007/s00415-021-10738-9
6. Gable MS, Sheriff H, Dalmau J, Tilley DH, Glaser CA. The frequency of autoimmune N-Methyl-D-aspartate receptor encephalitis surpasses that of individual viral etiologies in young individuals enrolled in the California encephalitis project. Clin Infect Dis. 2012;54(7):899–904. doi:10.1093/cid/cir1038
7. Prüss H, Dalmau J, Harms L, et al. Retrospective analysis of NMDA receptor antibodies in encephalitis of unknown origin. Neurology. 2010;75(19):1735–1739. doi:10.1212/WNL.0b013e3181fc2a06
8. Kunchok A, McKeon A, Zekeridou A, et al. Autoimmune/paraneoplastic encephalitis antibody biomarkers: frequency, age, and sex associations. Mayo Clin Proc. 2022;97(3):547–559. doi:10.1016/j.mayocp.2021.07.023
9. Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013;12(2):157–165. doi:10.1016/S1474-4422(12)70310-1
10. Xu X, Lu Q, Huang Y, et al. Anti-NMDAR encephalitis: a single-center, longitudinal study in China. Neurol Neuroimmunol Neuroinflamm. 2020;7(1). doi:10.1212/nxi.0000000000000633
11. Gong X, Chen C, Liu X, et al. Long-term functional outcomes and relapse of anti-NMDA receptor encephalitis: a cohort study in Western China. Neurol Neuroimmunol Neuroinflamm. 2021;8(2). doi:10.1212/NXI.0000000000000958
12. Dalmau J, Lancaster E, Martinez-Hernandez E, Rosenfeld MR, Balice-Gordon R. Clinical experience and laboratory investigations in patients with anti-NMDAR encephalitis. Lancet Neurol. 2011;10(1):63–74. doi:10.1016/S1474-4422(10)70253-2
13. Ho ACC, Mohammad SS, Pillai SC, et al. High sensitivity and specificity in proposed clinical diagnostic criteria for anti-N-methyl-D-aspartate receptor encephalitis. Dev Med Child Neurol. 2017;59(12):1256–1260. doi:10.1111/dmcn.13579
14. Zandi MS, Paterson RW, Ellul MA, et al. Clinical relevance of serum antibodies to extracellular N-methyl-D-aspartate receptor epitopes. J Neurol Neurosurg Psychiatry. 2015;86(7):708–713.
15. Dahm L, Ott C, Steiner J, et al. Seroprevalence of autoantibodies against brain antigens in health and disease. Ann Neurol. 2014;76(1):82–94. doi:10.1002/ana.24189
16. Gresa-Arribas N, Titulaer MJ, Torrents A, et al. Antibody titres at diagnosis and during follow-up of anti-NMDA receptor encephalitis: a retrospective study. Lancet Neurol. 2014;13(2):167–177. doi:10.1016/S1474-4422(13)70282-5
17. Freund B, Ritzl EK. A review of EEG in anti-NMDA receptor encephalitis. J Neuroimmunol. 2019;332:64–68. doi:10.1016/j.jneuroim.2019.03.010
18. Bien CG, Bien CI, Dogan Onugoren M, et al. Routine diagnostics for neural antibodies, clinical correlates, treatment and functional outcome. J Neurol. 2020;267(7):2101–2114. doi:10.1007/s00415-020-09814-3
19. Guang S, Ma J, Ren X, et al. Immunotherapies for anti-N-M-methyl-D-aspartate receptor encephalitis: multicenter retrospective pediatric cohort study in China. Front Pediatr. 2021;9:691599. doi:10.3389/fped.2021.691599
20. Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis. Lancet Neurol. 2016;15(4):391–404. doi:10.1016/S1474-4422(15)00401-9
21. O’Sullivan S, Mullins G, Cassidy E, McNamara B. The role of the standard EEG in clinical psychiatry. Hum Psychopharmacol. 2006;21(4):265–271. doi:10.1002/hup.767
22. Manchanda R, Malla A, Harricharan R, Cortese L, Takhar J. EEG abnormalities and outcome in first-episode psychosis. Can J Psychiatry. 2003;48(11):722–726. doi:10.1177/070674370304801103
23. Gillinder L, Warren N, Hartel G, Dionisio S, O’Gorman C. EEG findings in NMDA encephalitis – a systematic review. Seizure. 2019;65:20–24. doi:10.1016/j.seizure.2018.12.015
24. Nosadini M, Eyre M, Molteni E, et al. Use and safety of immunotherapeutic management of N-methyl-d-aspartate receptor antibody encephalitis: a meta-analysis. JAMA Neurol. 2021;78(11):1333–1344. doi:10.1001/jamaneurol.2021.3188
25. Bacchi S, Franke K, Wewegama D, Needham E, Patel S, Menon D. Magnetic resonance imaging and positron emission tomography in anti-NMDA receptor encephalitis: a systematic review. J Clin Neurosci. 2018;52:54–59. doi:10.1016/j.jocn.2018.03.026
26. Jiang H, Ye H, Wang Y, Li Y, Wang Y, Li X. Anti-N-Methyl-D-aspartate receptor encephalitis associated with ovarian teratoma in South China-clinical features, treatment, immunopathology, and surgical outcomes of 21 cases. Dis Markers. 2021;2021:1–7. doi:10.1155/2021/9990382
27. Abboud H, Probasco J, Irani SR, et al. Autoimmune encephalitis: proposed recommendations for symptomatic and long-term management. J Neurol Neurosurg Psychiatry. 2021;92(8):897–907. doi:10.1136/jnnp-2020-325302
28. Abboud H, Probasco JC, Irani S, et al. Autoimmune encephalitis: proposed best practice recommendations for diagnosis and acute management. J Neurol Neurosurg Psychiatry. 2021;92(7):757–768. doi:10.1136/jnnp-2020-325300
29. Nosadini M, Thomas T, Eyre M, et al. International consensus recommendations for the treatment of pediatric NMDAR antibody encephalitis. Neurol Neuroimmunol Neuroinflamm. 2021;8(5):e1052. doi:10.1212/NXI.0000000000001052
30. Galeotti C, Kaveri SV, Bayry J IVIG-mediated effector functions in autoimmune and inflammatory diseases. Int Immunol. 2017;29(11):491–498. doi:10.1093/intimm/dxx039
31. Lee W-J, Lee S-T, Shin Y-W, et al. Teratoma removal, steroid, IVIG, rituximab and tocilizumab (T-SIRT) in anti-NMDAR encephalitis. Neurotherapeutics. 2021;18(1):474–487. doi:10.1007/s13311-020-00921-7
32. Cai M-T, Zheng Y, Wang S, et al. Clinical relevance of cerebrospinal fluid antibody titers in anti-N-methyl-d-aspartate receptor encephalitis. Brain Sci. 2021;12(1):4. doi:10.3390/brainsci12010004
33. Gong X, Luo R, Liu J, et al. Efficacy and tolerability of intravenous immunoglobulin versus intravenous methylprednisolone treatment in anti‐N‐methyl‐d‐aspartate receptor encephalitis. Eur J Neurol. 2022;29(4):1117–1127. doi:10.1111/ene.15214
34. de Vries JM, Titulaer MJ. Treatment approaches in autoimmune neurology: focus on autoimmune encephalitis with neuronal cell surface antibodies. In: Piquet AL, Alvarez E, editors. Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related Diseases. Springer International Publishing; 2021:261–278.
35. Morales-Ruiz V, Juárez-Vaquera VH, Rosetti-Sciutto M, Sánchez-Muñoz F, Adalid-Peralta L. Efficacy of intravenous immunoglobulin in autoimmune neurological diseases. Literature systematic review and meta-analysis. Autoimmun Rev. 2022;21(3):103019. doi:10.1016/j.autrev.2021.103019
36. Dubey D, Britton J, McKeon A, et al. Randomized placebo‐controlled trial of intravenous immunoglobulin in autoimmune LGI1/CASPR2 epilepsy. Ann Neurol. 2020;87(2):313–323. doi:10.1002/ana.25655
37. Pham HP, Daniel-Johnson JA, Stotler BA, Stephens H, Schwartz J. Therapeutic plasma exchange for the treatment of anti-NMDA receptor encephalitis. J Clin Apher. 2011;26(6):320–325. doi:10.1002/jca.20311
38. Suppiej A, Nosadini M, Zuliani L, et al. Plasma exchange in pediatric anti-NMDAR encephalitis: a systematic review. Brain Dev. 2016;38(7):613–622. doi:10.1016/j.braindev.2016.01.009
39. Zhang Y, Liu G, Jiang M, Chen W, Su Y. Efficacy of therapeutic plasma exchange in patients with severe refractory anti-NMDA receptor encephalitis. Neurotherapeutics. 2019;16(3):828–837. doi:10.1007/s13311-019-00725-4
40. Zhang Y, Huang H, Chen W, Liu G, Liu F, Su YY. Clinical efficacy of plasma exchange in patients with autoimmune encephalitis. Ann Clin Transl Neurol. 2021;8(4):763–773. doi:10.1002/acn3.51313
41. Thaler FS, Zimmermann L, Kammermeier S, et al. Rituximab treatment and long-term outcome of patients with autoimmune encephalitis: real-world evidence from the GENERATE registry. Neurol Neuroimmunol Neuroinflamm. 2021;8(6):e1088. doi:10.1212/NXI.0000000000001088
42. Dinoto A, Cheli M, Bratina A, Sartori A, Manganotti P. Bortezomib in anti-N-Methyl-d-Aspartate-Receptor (NMDA-R) encephalitis: a systematic review. J Neuroimmunol. 2021;356:577586. doi:10.1016/j.jneuroim.2021.577586
43. Randell RL, Adams AV, Van Mater H. Tocilizumab in refractory autoimmune encephalitis: a series of pediatric cases. Pediatr Neurol. 2018;86:66–68. doi:10.1016/j.pediatrneurol.2018.07.016
44. Lee W-J, Lee S-T, Moon J, et al. Tocilizumab in autoimmune encephalitis refractory to rituximab: an institutional cohort study. Neurotherapeutics. 2016;13(4):824–832. doi:10.1007/s13311-016-0442-6
45. Reeves HM, Winters JL The mechanisms of action of plasma exchange. Br J Haematol. 2014;164(3):342–351.
46. Tanaka T, Narazaki M, Kishimoto T IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. ;6(10):a016295. doi:10.1101/cshperspect.a016295
47. Abulayha A, Bredan A, Enshasy HE, Daniels I Rituximab: modes of action, remaining dispute and future perspective. Future Oncology. 2014;10(15):2481–2492.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.