")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Anti-Hyperglycemic Agents in the Adjuvant Treatment of Sepsis: Improving Intestinal Barrier Function
Authors Wang YF , Li JW, Wang DP, Jin K, Hui JJ, Xu HY
Received 29 January 2022
Accepted for publication 28 May 2022
Published 4 June 2022 Volume 2022:16 Pages 1697—1711
DOI https://doi.org/10.2147/DDDT.S360348
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Georgios Panos
Yi-Feng Wang, Jia-Wei Li, Da-Peng Wang, Ke Jin, Jiao-Jie Hui, Hong-Yang Xu
Department of Critical Care Medicine, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi, Jiangsu, People’s Republic of China
Correspondence: Jiao-Jie Hui; Hong-Yang Xu, Email [email protected]; [email protected]
Abstract: Intestinal barrier injury and hyperglycemia are common in patients with sepsis. Bacteria translocation and systemic inflammatory response caused by intestinal barrier injury play a significant role in sepsis occurrence and deterioration, while hyperglycemia is linked to adverse outcomes in sepsis. Previous studies have shown that hyperglycemia is an independent risk factor for intestinal barrier injury. Concurrently, increasing evidence has indicated that some anti-hyperglycemic agents not only improve intestinal barrier function but are also beneficial in managing sepsis-induced organ dysfunction. Therefore, we assume that these agents can block or reduce the severity of sepsis by improving intestinal barrier function. Accordingly, we explicated the connection between sepsis, intestinal barrier, and hyperglycemia, overviewed the evidence on improving intestinal barrier function and alleviating sepsis-induced organ dysfunction by anti-hyperglycemic agents (eg, metformin, peroxisome proliferators activated receptor-γ agonists, berberine, and curcumin), and summarized some common characteristics of these agents to provide a new perspective in the adjuvant treatment of sepsis.
Keywords: sepsis, sepsis-induced organ dysfunction, intestinal barrier, anti-hyperglycemic agents
Summary
Previous study has confirmed that hyperglycemia can independently drive intestinal barrier dysfunction. Since hyperglycemia and intestinal barrier dysfunction commonly exist and are associated with poor prognosis in sepsis, they might be the targets in the management of sepsis. Interestingly, some anti-hyperglycemic agents (eg, metformin, peroxisome proliferators activated receptor-γ agonists, berberine, and curcumin) have shown positive effects beyond controlling hyperglycemia, such as improving intestinal barrier function and resisting sepsis-induced organ dysfunction. With the ability to inhibit systemic inflammatory response and prevent enterogenous infection, agents capable of controlling hyperglycemia and improving intestinal barrier function might be beneficial in the management of sepsis.
Introduction
Sepsis is a series of pathophysiological events caused by uncontrolled reactions to various infections that result in multiple organ dysfunction syndrome (MODS) and even death.1,2 Nowadays, sepsis has become a huge burden on global health. In 2017, nearly 50 million incident cases of sepsis were recorded, and 11 million sepsis-related deaths were reported, representing about 20% of all global deaths.3 Noteworthy, sepsis is not a single disease but a syndrome comprising many pathophysiological changes caused by aggravated infectious diseases, and available treatment options beside antibiotics and supportive care are limited because of the heterogeneity of pathogenic factors in sepsis.4 Therefore, feasible therapy is vital for sepsis management.5
Intestinal barrier injury is a common phenomenon in sepsis patients and plays an essential role in sepsis occurrence and deterioration. The intestinal barrier includes a mucosal barrier composed of the intestinal epithelium and secreted mucus, a biological barrier composed of intestinal microbiota, and an immune barrier composed of intestinal immune tissues. Normally, the intestinal barrier participates in absorbing nutrients and, meanwhile, prevents bacteria and toxins from crossing the barrier from the intestinal tract to the circulation. However, when the intestinal barrier is impaired, the intestinal permeability of the intestinal contents, such as intestinal bacteria and their metabolites, increases, and some adverse consequences occur.6 In sepsis, lipopolysaccharide (LPS) generated from intestinal gram-negative bacteria crosses the impaired intestinal barrier and enters the circulation, aggravating the systemic inflammatory response and exacerbating the severity of sepsis.7–9 Nevertheless, intestinal barrier injury is not only the accelerator but also the initiator of sepsis; therefore, intestinal barrier injury caused by reasons besides sepsis can initiate enterogenous infection and increase the risk of sepsis.10–12 Consequently, blocking the vicious cycle between intestinal barrier injury and sepsis is a promising strategy for the adjuvant treatment of sepsis.
Another common symptom of sepsis is hyperglycemia. On the one hand, type 2 diabetes mellitus (T2DM) is a cause of pre-existing hyperglycemia, acting as a frequent complication during sepsis. On the other hand, stress-induced hyperglycemia occurs under the severe pathophysiological events of sepsis.13 Notably, the occurrence of hyperglycemia is closely related to worse outcomes in sepsis.14 Interestingly, intestinal barrier injury is independently driven by hyperglycemia,15 and our previous study has further confirmed the relationship between intestinal barrier injury and hyperglycemia in humans.16 In addition to the negative effects of hyperglycemia on the intestinal barrier and sepsis, some anti-hyperglycemic agents have been proven to protect against intestinal barrier injury17 and alleviate sepsis-induced organ dysfunction in numerous animal experiments.18
Therefore, we assumed that by improving the intestinal barrier function, some anti-hyperglycemic agents could block or reduce the severity of sepsis. Accordingly, we explicated the connection between sepsis, intestinal barrier, and hyperglycemia, overviewed the evidence on improving intestinal barrier function and alleviating sepsis-induced organ dysfunction by anti-hyperglycemic agents (eg, metformin, peroxisome proliferators activated receptor-γ agonists, berberine, and curcumin), and summarized some common characteristics of these agents to provide new a perspective in the adjuvant treatment of sepsis.
Metformin
Metformin is a widely used anti-hyperglycemic agent in the treatment of T2DM. Recently, the intestine has been recognized as a major site of metformin pharmacodynamics.19 Sum et al have found that peripheral glucose disposal by intravenous metformin infusion was not better than that by normal saline infusion as control, indicating that the anti-hyperglycemic effect of metformin has barely depended on its substance in the circulation.20 Vancomycin is a broad-spectrum antibiotic, and orally administered vancomycin cannot be absorbed from the intestinal tract21 but induces drastic and consistent changes in the intestinal microbiota.22 Kim et al have found that after receiving oral vancomycin, the anti-hyperglycemic effect of metformin was weakened without pharmacokinetics change, while the relative abundance of intestinal microbiota was changed and associated with the anti-hyperglycemic effect. Taken together, the effect of metformin is more likely to depend on the improvement of intestinal microbiota but not on the concentration of metformin in circulation.23 Given the close relationship between intestinal microbiota and intestinal barrier,24,25 metformin can provide benefits by improving intestinal barrier function. Moreover, metformin can prevent sepsis-induced organ dysfunction with the effects of reducing reactive oxygen species and pro-inflammatory cytokines, inhibiting the activation of transcription factors related to inflammation, decreasing neutrophil accumulation and infiltration, and maintaining mitochondrial membrane potential.26
The main pharmacological effect of metformin is the activation of adenosine monophosphate-activated protein kinase (AMPK), and previous studies have demonstrated that AMPK is vital for intestinal barrier function.27 Wu et al have found that LPS decreased the expression of tight junction (TJ) proteins, causing the pro-inflammatory response, oxidative stress, and intestinal barrier damage in mice, and those effects were attenuated by metformin through the activation of AMPK.28 Since C-Jun N-terminal kinase (JNK) is involved in the disruption of the intestinal barrier, Deng et al have found that metformin prevents intestinal barrier dysfunction by inhibiting the activation of JNK through an AMPK-dependent signaling pathway in Caco-2 cell monolayers, colitis mice models, and ulcerative colitis patients.29
Besides AMPK, metformin improves the intestinal barrier function through other mechanisms. Mucin 2 is the main glycoprotein constituting the intestinal mucosal layer. Ke et al have found that metformin restored intestinal barrier function by increasing the expression of mucin 2 in mice with ulcerative colitis induced by dextran sulfate sodium (DSS).30 Myosin light-chain kinase (MLCK) is an enzyme activating the myosin light chain (MLC) and participating in cytoskeleton contraction and TJ regulation. Zhu et al have demonstrated that metformin stabilizes TJ proteins and improves intestinal barrier function by inhibiting the MLCK-MLC signaling pathway in Caco-2 cell monolayers.31 Li et al have found that metformin protects the intestinal barrier function by normalizing the interaction between claudin-4 and zonula occludens (ZO) −1 and preventing the distribution of claudin-4 in rats with irritable bowel syndrome.32 Recently, an increasing number of studies have focused on the relationship between metformin and intestinal microbiota, and Zhang et al have summarized that metformin was capable of improving intestinal barrier function by maintaining intestinal microbiota homeostasis.33
Given the advantages of intestinal barrier improvement, metformin can theoretically contribute to the management of sepsis. Clinical research has shown that metformin exposure is associated with decreased morbidity and mortality in patients with sepsis and pre-existing hyperglycemia.34–36 Studies on sepsis models have also shown that metformin could prevent sepsis-induced organ dysfunction, and the specific efficacy and associated mechanisms are summarized in Table 1.37–51 Surprisingly, Malik et al have found that metformin provides antimicrobial benefits in various infections in vitro and in vivo,52 fundamentally preventing the occurrence and deterioration of sepsis. In conclusion, metformin might provide benefits in the adjuvant treatment of sepsis by improving intestinal barrier function. And the application of metformin in sepsis needs further clinical investigation.
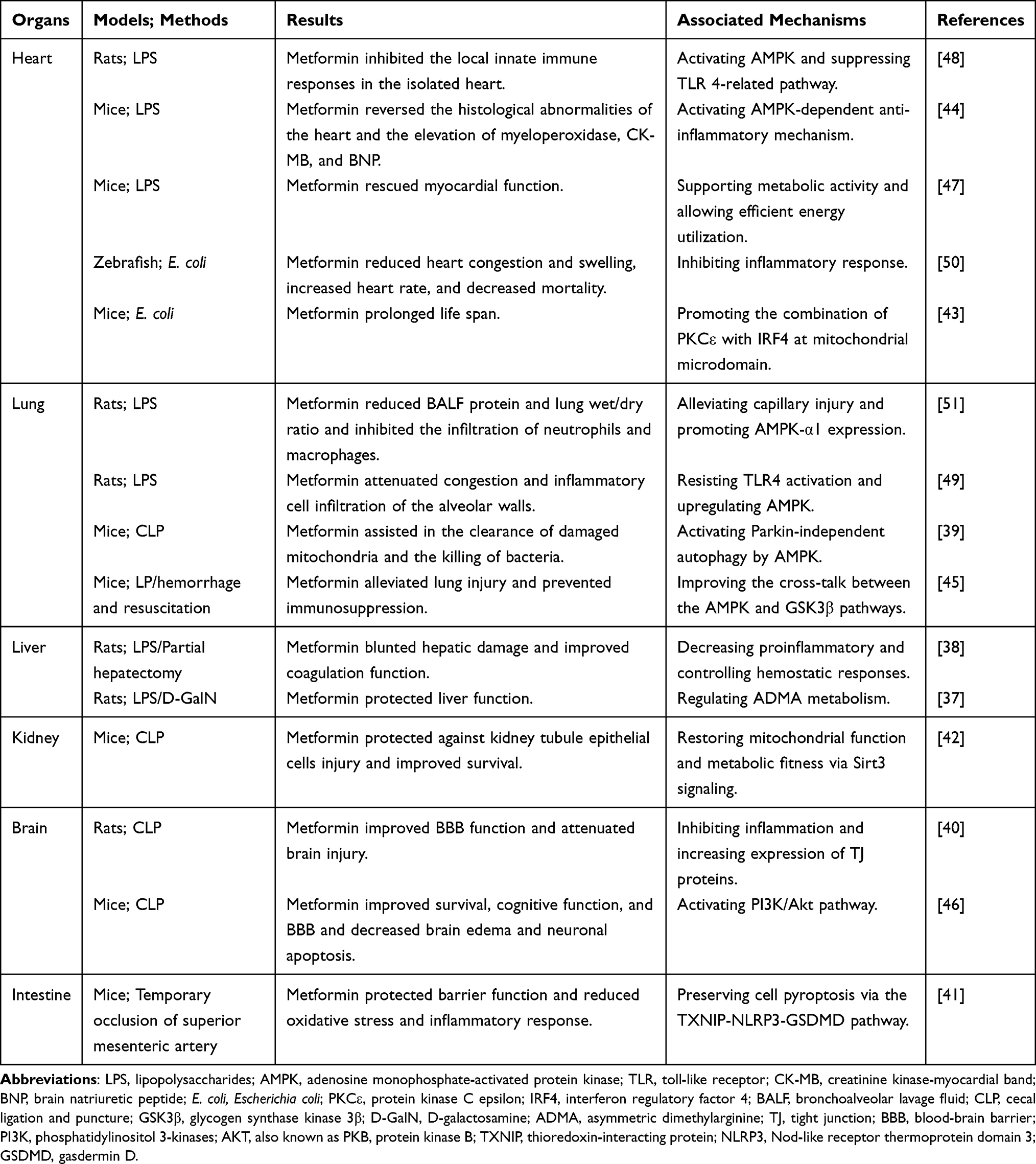 |
Table 1 Beneficial Effects of Metformin on Sepsis-Induced Organ Dysfunction |
Peroxisome Proliferators Activated Receptor-γ (PPAR-γ) Agonists
PPAR-γ agonists are another class of anti-hyperglycemic agents. As the name implies, PPAR-γ agonists act by increasing the activity of PPAR-γ.53 PPAR-γ is abundantly expressed in intestinal epithelial cells,54 and its activation can alleviate intestinal barrier injury.55,56 Zhao et al have found that rosiglitazone effectively promoted the intestinal mucus integrity and prevented the intestinal barrier injury via an MLCK-dependent mechanism in chronic colitis mice.57
Considering the relationship between intestinal barrier injury and sepsis, PPAR-γ agonists with positive effects on the intestinal barrier can make a difference in the management of sepsis. Shih et al have found in a nested case–control study that PPAR-γ agonist exposure was associated with a decreased risk of sepsis in patients with pre-existing hyperglycemia.58 Hsieh et al have shown in a propensity score matching observational study that over 4-week use of pioglitazone within three months was associated with decreased mortality in patients with sepsis and T2DM.59 As early as 2004, Fink et al proposed that PPAR-γ agonists could be useful for adjuvant treatment of sepsis and MODS.60 Li et al have described the role of PPAR-γ in the regulation of inflammatory response and emphasized the potential efficacy of PPAR-γ agonists as a novel therapeutic option in sepsis.61 Many studies on sepsis models have also shown the positive effects of PPAR-γ agonists (rosiglitazone and pioglitazone) on sepsis-induced organ dysfunction, and the specific efficacy and associated mechanisms are summarized in Table 2.62–74 Given the protective effects of PPAR-γ agonists on the intestinal barrier and sepsis, the corresponding clinical research is in progress,75 and whether PPAR-γ agonists improve the prognosis of sepsis will be answered in the future.
 |
Table 2 Beneficial Effects of PPAR-γ Agonists on Sepsis-Induced Organ Dysfunction |
Berberine
Berberine, isolated from traditional Chinese medicine, has been used to treat intestinal inflammation for decades. Recent studies have shown the therapeutic ability of berberine in many parenteral diseases.76 Zhang et al have found in a randomized, double-blind, placebo-controlled trial that berberine significantly reduced glycosylated hemoglobin C and improved hyperglycemia in newly diagnosed T2DM patients.77 Additionally, meta-analyses have indicated that berberine could be used as an anti-hyperglycemic agent in the treatment of T2DM.78,79
Until now, berberine has been proved to improve intestinal barrier function in many intestinal diseases. Xiong et al have overviewed previous studies and concluded that berberine repairs intestinal barrier injury by promoting differentiation of intestinal stem cells through identifying bitter taste receptors on Tuft cells in ulcerative colitis.80 Li et al have demonstrated that berberine restores the intestinal barrier homeostasis, maintains the residence of enteric glial cells, suppresses inflammatory cell infiltrations, and attenuates the overactivation of immune cells in mice with DSS-induced ulcerative colitis.81 Jing et al have found that berberine improves intestinal barrier function by regulating intestinal microbiota-associated tryptophan metabolite and activating the aryl hydrocarbon receptor in rats with DSS-induced colitis.82 Zhang et al have shown that berberine improves intestinal barrier function by promoting anti-inflammatory and antioxidative stress responses in mice with DSS-induced colitis.83 Considering that A20, a ubiquitin-modifying enzyme, can protect cells from necroptosis,84 Hou et al have found that berberine protected intestinal epithelial TJ and repaired intestinal barrier injury by increasing the expression of A20 in mice with diarrhea-predominant irritable bowel syndrome.85
Moreover, the protective effects of berberine on the intestinal barrier have also been confirmed in other diseases. Gong et al have found in T2DM rats that the anti-hyperglycemic effect of berberine might be attributed to the improvement of intestinal barrier function.86 Shan et al have shown in T2DM rats that berberine effectively repairs the damaged intestinal mucosa, restores intestinal permeability, and improves endotoxemia.87 Zhang et al have demonstrated in mice with renal failure and long-term peritoneal dialysis that berberine alleviates intestinal barrier dysfunction by increasing TJ and adhesion junction proteins, improving the morphology of microvilli, and promoting cell migration.88 Yu et al have found in rats with uremia induced by the 5/6 kidney resection that berberine prevents intestinal barrier injury through antioxidant effect.89 Li et al have demonstrated in mice with nonalcoholic fatty liver disease that berberine restores liver function by ameliorating intestinal barrier function.90 Liang et al have found in rats with severe acute pancreatitis that berberine improves the intestinal barrier function and maintains the intestinal membrane permeability by inhibiting MLC phosphorylation.91 Yu et al have shown in blunt snout bream that berberine alleviates intestinal barrier injury by inhibiting pro-inflammatory response and modulating intestinal microbiota.92
Despite the positive effects of berberine in different diseases, the bioavailability of berberine is unexpectedly low; in other words, berberine either plays biological roles through its metabolites93 or through the positive effects on intestinal microbiota and intestinal barrier.94,95 Furthermore, all those benefits generated from the improvement of intestinal barrier function suggest that berberine could be a candidate for the adjuvant treatment of sepsis. Additionally, increasing evidence has indicated that berberine could resist sepsis-induced organ dysfunction, and the specific efficacy and associated mechanisms are shown in Table 3.96–111 However, the effects of berberine in patients with sepsis need to be investigated in the future.
 |
Table 3 Beneficial Effects of Berberine on Sepsis-Induced Organ Dysfunction |
Curcumin
Curcumin, an active component in turmeric, is used as spice, seasoning, and pigment in daily life. Due to its anti-inflammatory effect, curcumin has displayed treatment potential in various pro-inflammatory chronic diseases.112 Recent studies have found that curcumin shows an anti-hyperglycemic effect by decreasing insulin resistance, preventing β-cell death, and improving β-cell functions.113 Huang et al have found in T2DM rats that curcumin could ameliorate hyperglycemia and alleviate metabolic endotoxemia, intestinal microbiota imbalance, and intestinal barrier injury.114
The protective effects of curcumin on the intestinal barrier have also been confirmed in many other studies. Burge et al have summarized how curcumin alleviated intestinal barrier injury by inhibiting bacteria, modulating immunity, and regulating intestinal microbiota.115 In the studies on Caco-2 cell monolayers, Wang et al have found that curcumin prevents epithelial barrier damage and TJ disruption via upregulating the expression of heme oxygenase-1.116 Zhou et al have shown that curcumin improves intestinal barrier integrity by controlling endoplasmic reticulum stress and subsequent apoptosis.117 Tian et al have found that curcumin maintains the intestinal permeability and restores epithelial structure by enhancing ZO-1 protein expression through tumor necrosis factor (TNF)-α-related pathway in rats with intestinal ischemia-reperfusion injury.118 Cao et al have unveiled that curcumin enhanced intestinal barrier and mitochondrial function by Parkin-dependent mitophagy through AMPK activation and subsequent nuclear translocation of transcription factor EB in vitro and in pigs with oxidative stress.119
Similar to berberine with low bioavailability, orally administered curcumin cannot be detected in the circulation; as a result, any biological effects of curcumin beyond the intestine are the subsequent results from the intestine.120,121 In other words, all those beneficial effects of curcumin under such a low bioavailability are partly attributed to the improvement of intestinal barrier function.122,123 Considering sepsis, curcumin has shown its therapeutic potential with the ability to inhibit inflammation, reduce oxidative coagulation factors, and regulate the immune response.124 Many studies have proven that curcumin could prevent sepsis-induced organ dysfunction, and the specific efficacy and associated mechanisms are shown in Table 4.125–139 Besides, Siddiqui et al have found that the anti-inflammatory effect of curcumin is mediated by the upregulation of PPAR-γ in sepsis rats, while PPAR-γ was the target of another class of anti-hyperglycemic agents.140 Generally, curcumin might assist the management of sepsis by improving intestinal barrier function and a series of positive effects generated by the improvement of the intestinal barrier. Whether curcumin can improve the prognosis of sepsis patients will be answered in the future.
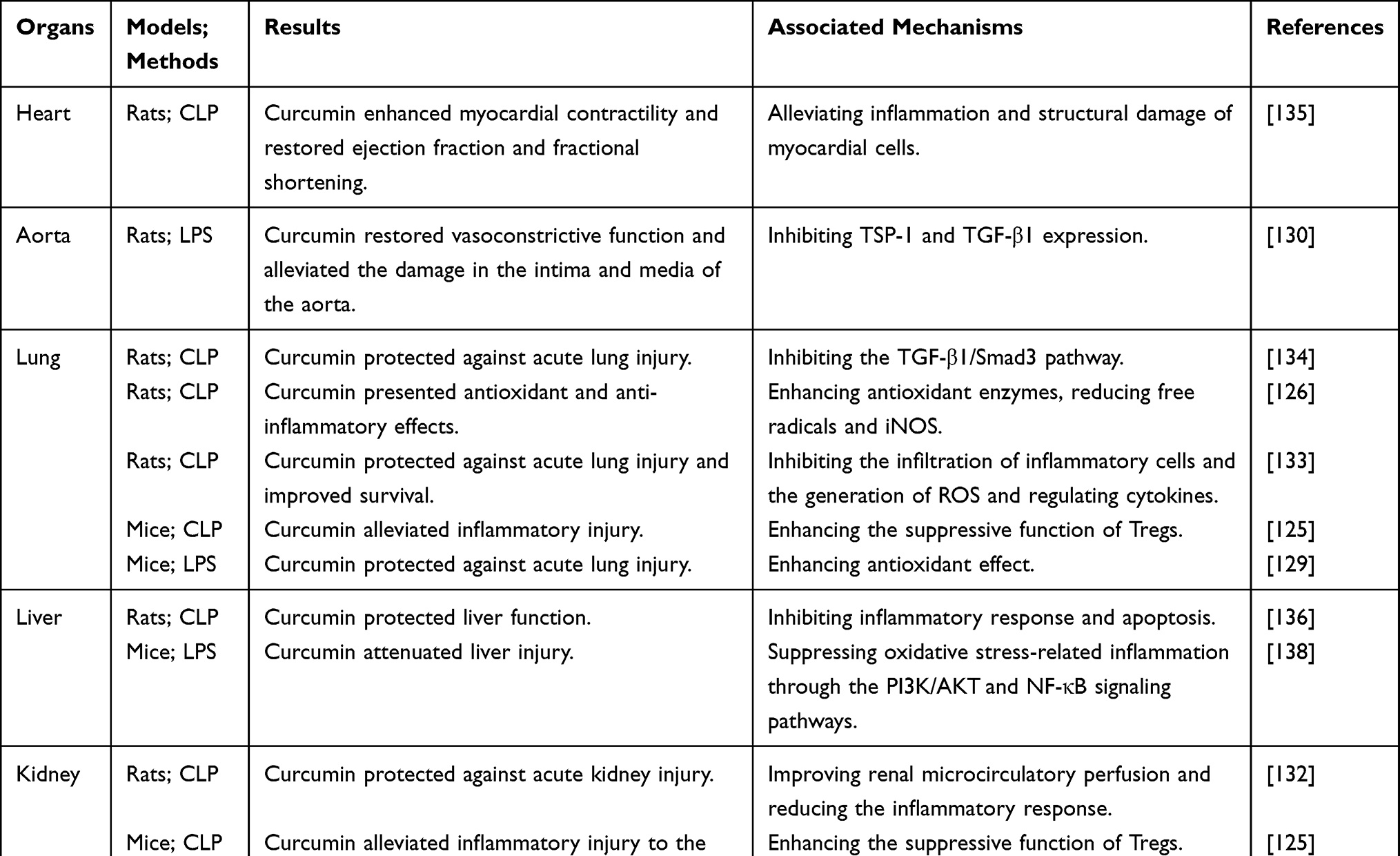 |
Table 4 Beneficial Effects of Curcumin on Sepsis-Induced Organ Dysfunction |
Other Anti-Hyperglycemic Agents
Besides these four above-mentioned agents, some other anti-hyperglycemic agents have displayed positive effects on sepsis. Insulin is the most commonly used anti-hyperglycemic agent in sepsis. In animals with sepsis, insulin treatment improves organ dysfunction through different mechanisms (Table 5).141–144 However, whether insulin improves the intestinal barrier function needs further investigation. Glucagon-like peptide-1 (GLP-1) receptor agonists are another class of anti-hyperglycemic agents. While the critical role of GLP-1 in the intestinal barrier has been gradually recognized,145 the possible application of GLP-1 receptor agonists in sepsis has been well reviewed by Yang.146 Sodium-glucose cotransporter-2 (SGLT2) inhibitors, a new class of anti-hyperglycemic agents, play the anti-hyperglycemic effect by increasing urinary glucose excretion. Some SGLT2 inhibitors have shown positive effects on the intestinal barrier. Zaghloul has found that empagliflozin ameliorated acetic acid-induced intestinal barrier injury in rats via modulation of the SIRT-1/PI3K/AKT pathway.147 Nozu has demonstrated that ipragliflozin improves intestinal hyperpermeability in rats with irritable bowel syndrome.148 Preventive effects of dapagliflozin on sepsis-induced organ damage have also been confirmed in rats.149 The specific effects of SGLT2 inhibitors (empagliflozin and canagliflozin) on sepsis-induced organ dysfunction and the associated mechanisms are displayed in Table 5.150–152 However, whether the positive effects of GLP-1 receptor agonists and SGLT2 inhibitors on sepsis are associated with intestinal barrier improvement requires further investigation, and the efficacy of these anti-hyperglycemic agents in sepsis patients will be evaluated in the future.
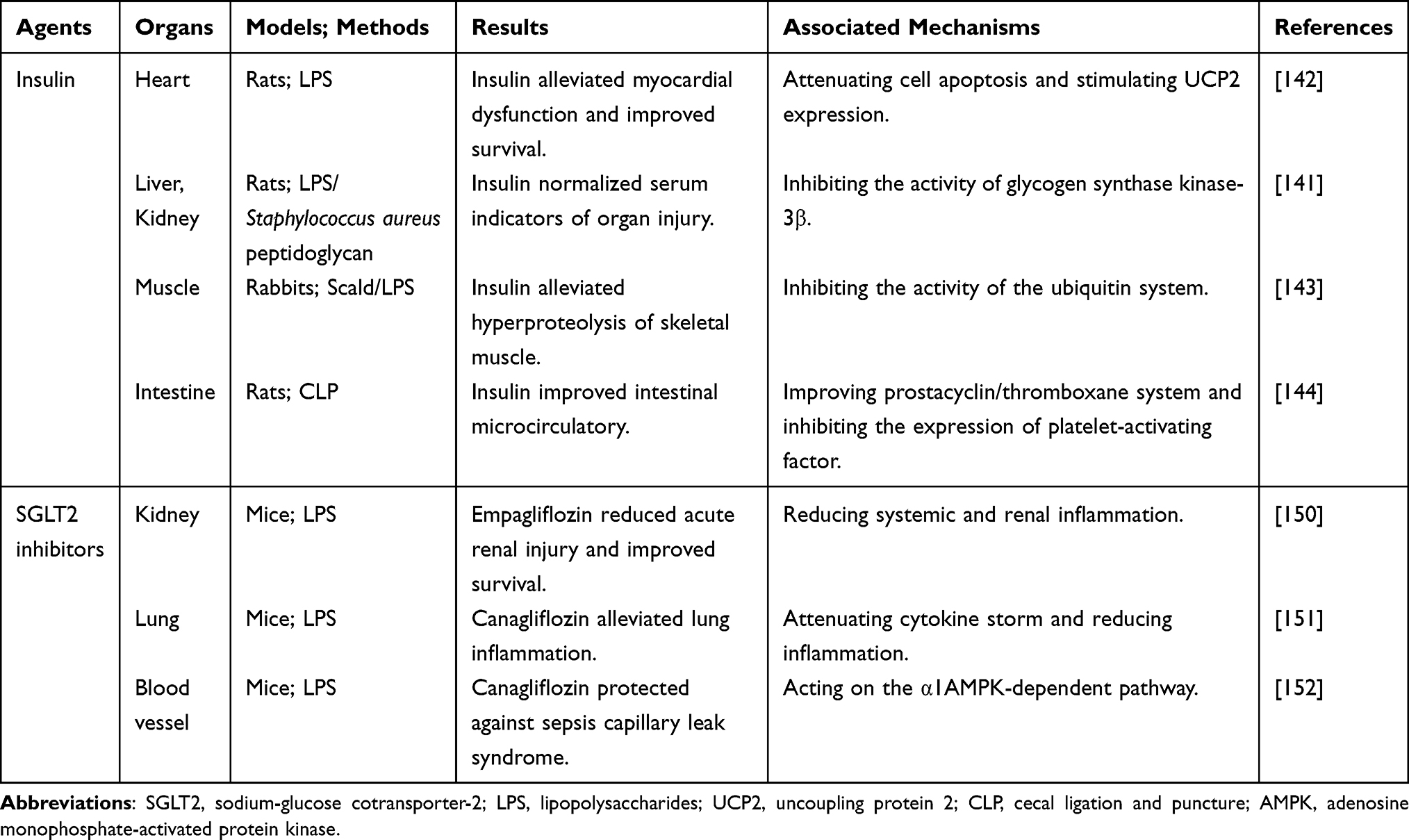 |
Table 5 Beneficial Effects of Insulin and SGLT2 Inhibitors on Sepsis-Induced Organ Dysfunction |
Discussion
Previous studies have proven a connection between sepsis, intestinal barrier, and hyperglycemia. Blocking the vicious cycle of this connection is expected to become a promising strategy for sepsis management.
Although hyperglycemia control can improve the prognosis of infectious diseases,153–155 most clinical studies have not proven the advantages of intensive glycemic control in sepsis. Moreover, intensive glycemic control increases the risk of hypoglycemia, which is associated with worse outcomes in sepsis.18 This contradiction forced us to make a compromise and set the goal of glycemic control at a relatively high level.156 However, the optimal goal of glycemic control in sepsis is still a pending issue. Noteworthy, the deleterious consequences of hyperglycemia are not limited to themselves but also to a series of subsequent pathophysiological results; hence, hyperglycemia can induce intestinal barrier injury, increase intestinal permeability, cause intestinal microbiota imbalance, lead to intestinal mucosal immune disorder, and increase the susceptibility to infection and the risk of sepsis. Therefore, the benefits beyond the anti-hyperglycemic effect would bring advantages to sepsis management.157
The significance of intestinal barrier improvement among these benefits is highlighted by some characteristics of these anti-hyperglycemic agents. First, the effect of metformin does not depend on its concentration in the circulation, leaving the intestinal barrier the possible target to act on. Second, PPAR-γ is abundantly expressed in the intestinal epithelial cells, making the intestinal barrier the first target influenced by PPAR-γ agonists. Third, the bioavailability of berberine and curcumin is extremely low; thus, benefits generated by these agents are attributed to their effects on the intestinal barrier. Interestingly, both berberine and curcumin are isolated from a natural plant, and their positive effects on the intestinal barrier can partly explain how some traditional Chinese medicine work without finding a specific bioactive factor in the circulation.158
In this review, we overviewed the evidence that anti-hyperglycemic agents (eg, metformin, PPAR-γ agonists, berberine, and curcumin) protect against sepsis-induced organ dysfunction by alleviating intestinal barrier injury. However, clinical evidence is limited. In further studies, the efficacy, safety, and adverse effects of these agents need to be evaluated, and whether these agents improve the outcomes in patients with sepsis should be answered. Additionally, we suggested that other agents capable of controlling hyperglycemia and improving the intestinal barrier might be candidates for sepsis management.
Abbreviations
ADMA, asymmetric dimethylarginine; AKT, also known as PKB, protein kinase B; AMPK, adenosine monophosphate-activated protein kinase; ApoM, apolipoprotein M; BALF, bronchoalveolar lavage fluid; BBB, blood-brain barrier; BNP, brain natriuretic peptide; CK-MB, creatinine kinase-myocardial band; CLP, cecal ligation and puncture; COX-2, cyclooxygenase-2; D-GalN, D-galactosamine; DSS, dextran sulfate sodium; E. coli, Escherichia coli; GLP-1, glucagon-like peptide-1; GSDMD, gasdermin D; GSK3β, glycogen synthase kinase 3β; GVB, gut-vascular barrier; HMGB1, high mobility group box 1; ICAM-1, intercellular adhesion molecule-1; IGF-1, insulin-like growth factor I; IGFBP-3, insulin-like growth factor-binding protein 3; IL, interleukin; iNOS, inducible nitric oxide synthase; IRF4, interferon regulatory factor 4; JAK2, Janus kinase 2; JNK, C-Jun N-terminal kinase; lncRNA, long non-coding RNA; LPS, lipopolysaccharide; MIP-2, macrophage inflammatory protein-2; MLC, myosin light chain; MLCK, myosin light-chain kinase; MODS, multiple organ dysfunction syndrome; NET, neutrophil extracellular trap; NF-κB, nuclear factor-κB; NLRP3, Nod-like receptor thermoprotein domain 3; PI3K, phosphatidylinositol 3-kinases; PKCε, protein kinase C epsilon; PPAR-γ, peroxisome proliferators activated receptor-γ; RAGE, advanced glycation end product receptor; ROS, reactive oxygen species; S1P, sphingosine-1-phosphate; SGLT2, sodium-glucose cotransporter-2; STAT3, signal transducer and activator of transcription 3; T2DM, type 2 diabetes mellitus; TGF-β1, transforming growth factor-β1; TJ, tight junction; TLR, toll-like receptor; TNF-α, tumor necrosis factor-α; TSP-1, thrombospondin-1; TXNIP, thioredoxin-interacting protein; UCP2, uncoupling protein 2; VCAM-1, vascular cell adhesion molecule-1; ZO, zonula occludens.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (81401619), the Youth Medical Talent Project from Jiangsu Provincial Commission of Health and Family Planning (QNRC2016178), and Taihu-Talent Project of Wuxi government.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hotchkiss RS, Moldawer LL, Opal SM, Reinhart K, Turnbull IR, Vincent JL. Sepsis and septic shock. Nat Rev Dis Primers. 2016;2:21. doi:10.1038/nrdp.2016.45
2. Rhodes A, Evans LE, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Crit Care Med. 2017;45(3):486–552. doi:10.1097/CCM.0000000000002255
3. Rudd KE, Johnson SC, Agesa KM, et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: analysis for the Global Burden of Disease Study. Lancet. 2020;395(10219):200–211. doi:10.1016/S0140-6736(19)32989-7
4. Abraham E. New definitions for sepsis and septic shock continuing evolution but with much still to be done. JAMA-J Am Med Assoc. 2016;315(8):757–759. doi:10.1001/jama.2016.0290
5. Howell MD, Davis AM. Management of sepsis and septic shock. JAMA-J Am Med Assoc. 2017;317(8):
6. Odenwald MA, Turner JR. The intestinal epithelial barrier: a therapeutic target? Nat Rev Gastroenterol Hepatol. 2017;14(1):9–21. doi:10.1038/nrgastro.2016.169
7. Anhe FF, Barra NG, Cavallari JF, Henriksbo BD, Schertzer JD. Metabolic endotoxemia is dictated by the type of lipopolysaccharide. Cell Rep. 2021;36(11):17. doi:10.1016/j.celrep.2021.109691
8. Haussner F, Chakraborty S, Halbgebauer R, Huber-Lang M. Challenge to the intestinal mucosa during sepsis. Front Immunol. 2019;10:891. doi:10.3389/fimmu.2019.00891
9. Wang CY, Li QR, Ren JN. Microbiota-immune interaction in the pathogenesis of gut-derived infection. Front Immunol. 2019;10:14. doi:10.3389/fimmu.2019.00014
10. Klingensmith NJ, Coopersmith CM. The gut as the motor of multiple organ dysfunction in critical illness. Crit Care Clin. 2016;32(2):203–212. doi:10.1016/j.ccc.2015.11.004
11. Assimakopoulos SF, Triantos C, Thomopoulos K, et al. Gut-origin sepsis in the critically ill patient: pathophysiology and treatment. Infection. 2018;46(6):751–760. doi:10.1007/s15010-018-1178-5
12. Mittal R, Coopersmith CM. Special issue: sepsis redefining the gut as the motor of critical illness. Trends Mol Med. 2014;20(4):214–223. doi:10.1016/j.molmed.2013.08.004
13. Marik PE, Raghavan M. Stress-hyperglycemia, insulin and immunomodulation in sepsis. Intensive Care Med. 2004;30(5):748–756. doi:10.1007/s00134-004-2167-y
14. Zohar Y, Zilberman Itskovich S, Koren S, Zaidenstein R, Marchaim D, Koren R. The association of diabetes and hyperglycemia with sepsis outcomes: a population-based cohort analysis. Intern Emerg Med. 2021;16(3):719–728. doi:10.1007/s11739-020-02507-9
15. Thaiss CA, Levy M, Grosheva I, et al. Hyperglycemia drives intestinal barrier dysfunction and risk for enteric infection. Science. 2018;359(6382):1376–1383. doi:10.1126/science.aar3318
16. Wang Y, Ding L, Yang J, Liu L, Dong L. Intestinal fatty acid-binding protein, a biomarker of intestinal barrier dysfunction, increases with the progression of type 2 diabetes. PeerJ. 2021;9:e10800. doi:10.7717/peerj.10800
17. Chen Y, Wang M. New insights of anti-hyperglycemic agents and traditional Chinese medicine on gut microbiota in Type 2 diabetes. Drug Des Dev Ther. 2021;15:4849–4863. doi:10.2147/DDDT.S334325
18. Costantini E, Carlin M, Porta M, Brizzi MF. Type 2 diabetes mellitus and sepsis: state of the art, certainties and missing evidence. Acta Diabetol. 2021;58(9):1139–1151. doi:10.1007/s00592-021-01728-4
19. McCreight LJ, Bailey CJ, Pearson ER. Metformin and the gastrointestinal tract. Diabetologia. 2016;59(3):426–435. doi:10.1007/s00125-015-3844-9
20. Sum CF, Webster JM, Johnson AB, Catalano C, Cooper BG, Taylor R. The effect of intravenous metformin on glucose metabolism during hyperglycaemia in type 2 diabetes. Diabetic Med. 1992;9(1):61–65. doi:10.1111/j.1464-5491.1992.tb01716.x
21. Rao S, Kupfer Y, Pagala M, Chapnick E, Tessler S. Systemic absorption of oral vancomycin in patients with Clostridium difficile infection. Scand J Infect Dis. 2011;43(5):386–388. doi:10.3109/00365548.2010.544671
22. Isaac S, Scher JU, Djukovic A, et al. Short- and long-term effects of oral vancomycin on the human intestinal microbiota. J Antimicrob Chemother. 2017;72(1):128–136. doi:10.1093/jac/dkw383
23. Kim E, Kim AH, Lee Y, et al. Effects of vancomycin-induced gut microbiome alteration on the pharmacodynamics of metformin in healthy male subjects. CTS-Clin Transl Sci. 2021;14(5):1955–1966. doi:10.1111/cts.13051
24. Di Tommaso N, Gasbarrini A, Ponziani FR. Intestinal barrier in human health and disease. Int J Environ Res Public Health. 2021;18(23):12836. doi:10.3390/ijerph182312836
25. Régnier M, Van Hul M, Knauf C, Cani PD. Gut microbiome, endocrine control of gut barrier function and metabolic diseases. J Endocrinol. 2021;248(2):R67–r82. doi:10.1530/JOE-20-0473
26. Hassan FI, Didari T, Khan F, Niaz K, Mojtahedzadeh M, Abdollahi M. A review on the protective effects of metformin in sepsis-induced organ failure. Cell J. 2020;21(4):363–370.
27. Olivier S, Pochard C, Diounou H, et al. Deletion of intestinal epithelial AMP-activated protein kinase alters distal colon permeability but not glucose homeostasis. Mol Metab. 2021;47:101183. doi:10.1016/j.molmet.2021.101183
28. Wu WC, Wang SS, Liu Q, Shan TZ, Wang YZ. Metformin protects against LPS-induced intestinal barrier dysfunction by activating AMPK pathway. Mol Pharm. 2018;15(8):3272–3284. doi:10.1021/acs.molpharmaceut.8b00332
29. Deng J, Zeng LS, Lai XY, et al. Metformin protects against intestinal barrier dysfunction via AMPK alpha 1-dependent inhibition of JNK signalling activation. J Cell Mol Med. 2018;22(1):546–557. doi:10.1111/jcmm.13342
30. Ke HR, Li F, Deng WL, et al. Metformin exerts anti-inflammatory and mucus barrier protective effects by enriching akkermansia muciniphila in mice with ulcerative colitis. Front Pharmacol. 2021;12:17. doi:10.3389/fphar.2021.726707
31. Zhu H, Yao XM, Qian JP, Yang J, Pan XD, Chen XD. Metformin regulates tight junction of intestinal epithelial cells via MLCK-MLC signaling pathway. Eur Rev Med Pharmacol Sci. 2017;21(22):5239–5246. doi:10.26355/eurrev_201711_13847
32. Li Y, Yang TT, Yao Q, et al. Metformin prevents colonic barrier dysfunction by inhibiting mast cell activation in maternal separation-induced IBS-like rats. Neurogastroenterol Motil. 2019;31(5):14. doi:10.1111/nmo.13556
33. Zhang Q, Hu N. Effects of metformin on the gut microbiota in obesity and Type 2 diabetes mellitus. Diabetes Metab Syndr Obes. 2020;13:5003–5014. doi:10.2147/DMSO.S286430
34. Tan K, Simpson A, Huang S, Tang B, McLean A, Nalos M. The association of premorbid metformin exposure with mortality and organ dysfunction in sepsis: a systematic review and meta-analysis. Crit Care Explor. 2019;1(4):e0009. doi:10.1097/CCE.0000000000000009
35. Yang QL, Zheng JZ, Chen WY, et al. Association between preadmission metformin use and outcomes in intensive care unit patients with sepsis and Type 2 diabetes: a cohort study. Front Med. 2021;8:8.
36. Liang HY, Ding XF, Li LF, et al. Association of preadmission metformin use and mortality in patients with sepsis and diabetes mellitus: a systematic review and meta-analysis of cohort studies. Crit Care. 2019;23:9. doi:10.1186/s13054-019-2346-4
37. Bal F, Bekpinar S, Unlucerci Y, et al. Antidiabetic drug metformin is effective on the metabolism of asymmetric dimethylarginine in experimental liver injury. Diabetes Res Clin Pract. 2014;106(2):295–302. doi:10.1016/j.diabres.2014.08.028
38. Bergheim I, Luyendyk JP, Steele C, et al. Metformin prevents endotoxin-induced liver injury after partial hepatectomy. J Pharmacol Exp Ther. 2006;316(3):1053–1061. doi:10.1124/jpet.105.092122
39. Bone NB, Becker EJ, Husain M, et al. AMPK activates Parkin independent autophagy and improves post sepsis immune defense against secondary bacterial lung infections. Sci Rep. 2021;11(1):15. doi:10.1038/s41598-021-90573-0
40. Hassan FI, Didari T, Baeeri M, et al. Metformin attenuates brain injury by inhibiting inflammation and regulating tight junction proteins in septic rats. Cell J. 2020;22:29–37. doi:10.22074/cellj.2020.7046
41. Jia YF, Cui RX, Wang C, et al. Metformin protects against intestinal ischemia-reperfusion injury and cell pyroptosis via TXNIP-NLRP3-GSDMD pathway. Redox Biol. 2020;32:11. doi:10.1016/j.redox.2020.101534
42. Jin K, Ma YJ, Manrique-Caballero CL, et al. Activation of AMP-activated protein kinase during sepsis/inflammation improves survival by preserving cellular metabolic fitness. FASEB J. 2020;34(5):7036–7057. doi:10.1096/fj.201901900R
43. Li MH, Yu HM, Wang YL, Qin L, Sun W. Role of IRF4 in the protection of metformin-mediated sepsis myocarditis. Dose-Response. 2019;17(1):8. doi:10.1177/1559325819827436
44. Liu G, Wu K, Zhang L, et al. Metformin attenuated endotoxin-induced acute myocarditis via activating AMPK. Int Immunopharmacol. 2017;47:166–172. doi:10.1016/j.intimp.2017.04.002
45. Liu ZY, Bone N, Jiang SN, et al. AMP-activated protein kinase and glycogen synthase Kinase 3 beta modulate the severity of sepsis-induced lung injury. Mol Med. 2015;21:937–950. doi:10.2119/molmed.2015.00198
46. Tang G, Yang H, Chen J, et al. Metformin ameliorates sepsis-induced brain injury by inhibiting apoptosis, oxidative stress and neuroinflammation via the PI3K/Akt signaling pathway. Oncotarget. 2017;8(58):97977–97989. doi:10.18632/oncotarget.20105
47. Tzanavari T, Varela A, Theocharis S, et al. Metformin protects against infection-induced myocardial dysfunction. Metab-Clin Exp. 2016;65(10):1447–1458. doi:10.1016/j.metabol.2016.06.012
48. Vaez H, Najafi M, Rameshrad M, et al. AMPK activation by metformin inhibits local innate immune responses in the isolated rat heart by suppression of TLR 4-related pathway. Int Immunopharmacol. 2016;40:501–507. doi:10.1016/j.intimp.2016.10.002
49. Vaez H, Najafi M, Toutounchi NS, Barar J, Barzegari A, Garjani A. Metformin alleviates lipopolysaccharide-induced acute lung injury through suppressing toll-like receptor 4 signaling. Iran J Allergy Asthma Immunol. 2016;15(6):498–507.
50. Zhang MM, Sun W, Du JA, et al. Protective effect of metformin on sepsis myocarditis in zebrafish. Dose-Response. 2020;18(3):9. doi:10.1177/1559325820938543
51. Zhang XC, Shang FT, Hui LL, Zang K, Sun GY. The alleviative effects of metformin for lipopolysaccharide- induced acute lung injury rat model and its underlying mechanism. Saudi Pharm J. 2017;25(4):666–670. doi:10.1016/j.jsps.2017.05.001
52. Malik F, Mehdi SF, Ali H, et al. Is metformin poised for a second career as an antimicrobial? Diabetes-Metab Res Rev. 2018;34(4):10. doi:10.1002/dmrr.2975
53. Nanjan MJ, Mohammed M, Prashantha Kumar BR, Chandrasekar MJN. Thiazolidinediones as antidiabetic agents: a critical review. Bioorganic Chem. 2018;77:548–567. doi:10.3389/fimmu.2019.01674
54. Fajas L, Auboeuf D, Raspé E, et al. The organization, promoter analysis, and expression of the human PPARgamma gene. J Biol Chem. 1997;272(30):18779–18789. doi:10.1074/jbc.272.30.18779
55. Zong X, Cao XX, Wang H, Xiao X, Wang YZ, Lu ZQ. Cathelicidin-WA facilitated intestinal fatty acid absorption through enhancing PPAR-gamma dependent barrier function. Front Immunol. 2019;10:12.
56. Huang YL, Wang CC, Tian XY, et al. Pioglitazone attenuates experimental colitis-associated hyperalgesia through improving the intestinal barrier dysfunction. Inflammation. 2020;43(2):568–578. doi:10.1007/s10753-019-01138-3
57. Zhao JF, Zhao RF, Cheng L, Yang J, Zhu LR. Peroxisome proliferator-activated receptor gamma activation promotes intestinal barrier function by improving mucus and tight junctions in a mouse colitis model. Dig Liver Dis. 2018;50(11):1195–1204. doi:10.1016/j.dld.2018.04.016
58. Shih CJ, Wu YL, Chao PW, et al. Association between use of oral anti-diabetic drugs and the risk of sepsis: a Nested Case-Control Study. Sci Rep. 2015;5:15260. doi:10.1038/srep15260
59. Hsieh MS, Hu SY, Liao SH, Chang CM, Hsieh VCR, How CK. Type 2 diabetic sepsis patients have a lower mortality rate in pioglitazone use: a nationwide 15-year propensity score matching observational study in Taiwan. Emerg Med Int. 2021;2021:9. doi:10.1155/2021/4916777
60. Fink MP. Peroxisome proliferator-activated receptor-gamma ligands: a pluripotent class of pharmacological agents that may prove to be useful for adjuvant treatment of sepsis and multiple organ dysfunction syndrome. Crit Care Med. 2004;32(2):604–605. doi:10.1097/01.CCM.0000110667.86935.F3
61. Zingarelli B, Cook JA. Peroxisome proliferator-activated receptor-gamma is a new therapeutic target in sepsis and inflammation. Shock. 2005;23(5):393–399. doi:10.1097/01.shk.0000160521.91363.88
62. Araújo CV, Campbell C, Gonçalves-de-albuquerque CF, et al. A PPARγ Agonist enhances bacterial clearance through neutrophil extracellular trap formation and improves survival in sepsis. Shock. 2016;45(4):393–403. doi:10.1097/SHK.0000000000000520
63. Araújo CV, Estato V, Tibiriçá E, Bozza PT, Castro-Faria-Neto HC, Silva AR. PPAR gamma activation protects the brain against microvascular dysfunction in sepsis. Microvasc Res. 2012;84(2):218–221. doi:10.1016/j.mvr.2012.05.006
64. Bu Y, Yu J. [Rosiglitazone protects against endotoxin-induced acute liver injury in rats]. Zhonghua Yi Xue Za Zhi. 2015;95(39):3180–3183. Chinese.
65. Deng J, Yu J. [Rosiglitazone protects acute kidney injury in septic rats]. Zhonghua Yi Xue Za Zhi. 2016;96(29):2311–2315. Chinese. doi:10.3760/cma.j.issn.0376-2491.2016.29.006
66. Drosatos K, Khan RS, Trent CM, et al. Peroxisome proliferator-activated receptor-gamma activation prevents sepsis-related cardiac dysfunction and mortality in mice. Circ-Heart Fail. 2013;6(3):
67. Gao M, Jiang Y, Xiao XF, Peng Y, Xiao XZ, Yang MS. Protective effect of pioglitazone on sepsis-induced intestinal injury in a rodent model. J Surg Res. 2015;195(2):550–558. doi:10.1016/j.jss.2015.02.007
68. Kaplan J, Nowell M, Chima R, Zingarelli B. Pioglitazone reduces inflammation through inhibition of NF-κB in polymicrobial sepsis. Innate Immun. 2014;20(5):519–528. doi:10.1177/1753425913501565
69. Kutsukake M, Matsutani T, Tamura K, et al. Pioglitazone attenuates lung injury by modulating adipose inflammation. J Surg Res. 2014;189(2):295–303. doi:10.1016/j.jss.2014.03.007
70. Lee S, Kim W, Kang KP, et al. Agonist of peroxisome proliferator-activated receptor-gamma, rosiglitazone, reduces renal injury and dysfunction in a murine sepsis model. Nephrol Dial Transplant. 2005;20(6):1057–1065. doi:10.1093/ndt/gfh705
71. Manfredini A, Constantino L, Pinto MC, et al. Mitochondrial dysfunction is associated with long-term cognitive impairment in an animal sepsis model. Clin Sci. 2019;133(18):1993–2004. doi:10.1042/CS20190351
72. Peng S, Xu J, Ruan W, Li S, Xiao F. PPAR-γ activation prevents septic cardiac dysfunction via inhibition of apoptosis and necroptosis. Oxid Med Cell Longev. 2017;2017:8326749. doi:10.1155/2017/8326749
73. Wang GZ, Liu L, Zhang YH, et al. Activation of PPAR gamma attenuates LPS-induced acute lung injury by inhibition of HMGB1-RAGE levels. Eur J Pharmacol. 2014;726:27–32. doi:10.1016/j.ejphar.2014.01.030
74. Zhang SM, Cai XF, Ma YL, Lu Q. Effect of rosiglitazone on myocardial injury in septic rats through NF-κB pathway. Eur Rev Med Pharmacol Sci. 2020;24(1):452–460. doi:10.26355/eurrev_202001_19945
75. Kaplan JM, Zingarelli B, Krallman K, et al. Phase 1 safety and pharmacokinetic study on the use of pioglitazone in critically ill patients with sepsis: a randomized clinical trial. Intensive Care Med. 2018;44(11):2006–2008. doi:10.1007/s00134-018-5374-7
76. Singh S, Pathak N, Fatima E, Negi AS. Plant isoquinoline alkaloids: advances in the chemistry and biology of berberine. Eur J Med Chem. 2021;226:113839. doi:10.1016/j.ejmech.2021.113839
77. Zhang Y, Gu Y, Ren H, et al. Gut microbiome-related effects of berberine and probiotics on type 2 diabetes (the PREMOTE study). Nat Commun. 2020;11(1):5015. doi:10.1038/s41467-020-18414-8
78. Liang Y, Xu X, Yin M, et al. Effects of berberine on blood glucose in patients with type 2 diabetes mellitus: a systematic literature review and a meta-analysis. Endocr J. 2019;66(1):51–63. doi:10.1507/endocrj.EJ18-0109
79. Lan J, Zhao Y, Dong F, et al. Meta-analysis of the effect and safety of berberine in the treatment of type 2 diabetes mellitus, hyperlipidemia and hypertension. J Ethnopharmacol. 2015;161:69–81. doi:10.1016/j.jep.2014.09.049
80. Xiong X, Cheng Z, Wu F, et al. Berberine in the treatment of ulcerative colitis: a possible pathway through Tuft cells. Biomed Pharmacother. 2021;134:111129. doi:10.1016/j.biopha.2020.111129
81. Li H, Fan C, Lu H, et al. Protective role of berberine on ulcerative colitis through modulating enteric glial cells-intestinal epithelial cells-immune cells interactions. Acta Pharm Sin B. 2020;10(3):447–461. doi:10.1016/j.apsb.2019.08.006
82. Jing W, Dong S, Luo X, et al. Berberine improves colitis by triggering AhR activation by microbial tryptophan catabolites. Pharmacol Res. 2021;164:105358. doi:10.1016/j.phrs.2020.105358
83. Zhang LC, Wang Y, Tong LC, et al. Berberine alleviates dextran sodium sulfate-induced colitis by improving intestinal barrier function and reducing inflammation and oxidative stress. Exp Ther Med. 2017;13(6):3374–3382. doi:10.3892/etm.2017.4402
84. Onizawa M, Oshima S, Schulze-Topphoff U, et al. The ubiquitin-modifying enzyme A20 restricts ubiquitination of the kinase RIPK3 and protects cells from necroptosis. Nat Immunol. 2015;16(6):618–627. doi:10.1038/ni.3172
85. Hou Q, Zhu S, Zhang C, et al. Berberine improves intestinal epithelial tight junctions by upregulating A20 expression in IBS-D mice. Biomed Pharmacother. 2019;118:109206. doi:10.1016/j.biopha.2019.109206
86. Gong J, Hu M, Huang Z, et al. Berberine attenuates intestinal mucosal barrier dysfunction in Type 2 diabetic rats. Front Pharmacol. 2017;8:42. doi:10.3389/fphar.2017.00042
87. Shan CY, Yang JH, Kong Y, et al. Alteration of the intestinal barrier and GLP2 secretion in Berberine-treated type 2 diabetic rats. J Endocrinol. 2013;218(3):255–262. doi:10.1530/JOE-13-0184
88. Zhang D, Jiang L, Wang M, et al. Berberine inhibits intestinal epithelial barrier dysfunction in colon caused by peritoneal dialysis fluid by improving cell migration. J Ethnopharmacol. 2021;264:113206. doi:10.1016/j.jep.2020.113206
89. Yu C, Tan S, Zhou C, et al. Berberine reduces uremia-associated intestinal mucosal barrier damage. Biol Pharm Bull. 2016;39(11):1787–1792. doi:10.1248/bpb.b16-00280
90. Li D, Zheng J, Hu Y, et al. Amelioration of intestinal barrier dysfunction by berberine in the treatment of nonalcoholic fatty liver disease in rats. Pharmacogn Mag. 2017;13(52):677–682. doi:10.4103/pm.pm_584_16
91. Liang HY, Chen T, Yan HT, Huang Z, Tang LJ. Berberine ameliorates severe acute pancreatitis‑induced intestinal barrier dysfunction via a myosin light chain phosphorylation‑dependent pathway. Mol Med Rep. 2014;9(5):1827–1833. doi:10.3892/mmr.2014.1996
92. Yu C, Zhang J, Qin Q, Liu J, Xu J, Xu W. Berberine improved intestinal barrier function by modulating the intestinal microbiota in blunt snout bream (Megalobrama amblycephala) under dietary high-fat and high-carbohydrate stress. Fish Shellfish Immunol. 2020;102:336–349. doi:10.1016/j.fsi.2020.04.052
93. Feng X, Wang K, Cao S, Ding L, Qiu F. Pharmacokinetics and excretion of berberine and its nine metabolites in rats. Front Pharmacol. 2020;11:594852. doi:10.3389/fphar.2020.594852
94. Zhang X, Han Y, Huang W, Jin M, Gao Z. The influence of the gut microbiota on the bioavailability of oral drugs. Acta Pharm Sin B. 2021;11(7):1789–1812. doi:10.1016/j.apsb.2020.09.013
95. Song D, Hao J, Fan D. Biological properties and clinical applications of berberine. Front Med. 2020;14(5):564–582. doi:10.1007/s11684-019-0724-6
96. Li HM, Wang YY, Wang HD, et al. Berberine protects against lipopolysaccharide-induced intestinal injury in mice via alpha 2 adrenoceptor-independent mechanisms. Acta Pharmacol Sin. 2011;32(11):1364–1372. doi:10.1038/aps.2011.102
97. He Y, Yuan X, Zuo H, Sun Y, Feng A. Berberine exerts a protective effect on gut-vascular barrier via the modulation of the Wnt/Beta-Catenin signaling pathway during sepsis. Cell Physiol Biochem. 2018;49(4):1342–1351. doi:10.1159/000493412
98. He Y, Yuan X, Zhou G, Feng A. Activation of IGF-1/IGFBP-3 signaling by berberine improves intestinal mucosal barrier of rats with acute endotoxemia. Fitoterapia. 2018;124:200–205. doi:10.1016/j.fitote.2017.11.012
99. Niu L, Qiao W, Hu Z, et al. Berberine attenuates lipopolysaccharide-induced impairments of intestinal glutamine transport and glutaminase activity in rat. Fitoterapia. 2011;82(3):323–330. doi:10.1016/j.fitote.2010.11.007
100. Shi J, Xu H, Cavagnaro MJ, Li X, Fang J. Blocking HMGB1/RAGE signaling by berberine Alleviates A1 astrocyte and attenuates sepsis-associated encephalopathy. Front Pharmacol. 2021;12:760186. doi:10.3389/fphar.2021.760186
101. Feng AW, Gao W, Zhou GR, et al. Berberine ameliorates COX-2 expression in rat small intestinal mucosa partially through PPARγ pathway during acute endotoxemia. Int Immunopharmacol. 2012;12(1):182–188. doi:10.1016/j.intimp.2011.11.009
102. Zheng Y, Shi X, Hou J, et al. Integrating metabolomics and network pharmacology to explore Rhizoma Coptidis extracts against sepsis-associated acute kidney injury. J Chromatogr B. 2021;1164:122525. doi:10.1016/j.jchromb.2021.122525
103. Gu L, Li N, Gong J, Li Q, Zhu W, Li J. Berberine ameliorates intestinal epithelial tight-junction damage and down-regulates myosin light chain kinase pathways in a mouse model of endotoxinemia. J Infect Dis. 2011;203(11):1602–1612. doi:10.1093/infdis/jir147
104. Lv Y, Wang J, Xu D, et al. Comparative study of single/combination use of Huang-Lian-Jie-Du decoction and berberine on their protection on sepsis induced acute liver injury by NMR metabolic profiling. J Pharm Biomed Anal. 2017;145:794–804. doi:10.1016/j.jpba.2017.07.062
105. Li GX, Wang XM, Jiang T, Gong JF, Niu LY, Li N. Berberine prevents intestinal mucosal barrier damage during early phase of sepsis in rat through the toll-like receptors signaling pathway. Korean J Physiol Pharmacol. 2015;19(1):1–7. doi:10.4196/kjpp.2015.19.1.1
106. Li Y, Zhou J, Qiu J, et al. Berberine reduces gut-vascular barrier permeability via modulation of ApoM/S1P pathway in a model of polymicrobial sepsis. Life Sci. 2020;261:118460. doi:10.1016/j.lfs.2020.118460
107. Pierpaoli E, Cirioni O, Simonetti O, et al. Potential application of berberine in the treatment of Escherichia coli sepsis. Nat Prod Res. 2021;35(22):4779–4784. doi:10.1080/14786419.2020.1721729
108. Wang Y, Du P, Jiang D. Berberine functions as a negative regulator in lipopolysaccharide -induced sepsis by suppressing NF-κB and IL-6 mediated STAT3 activation. Pathog Dis. 2020;78(7). doi:10.1093/femspd/ftaa047
109. Chen H, Liu Q, Liu X, Jin J. Berberine attenuates septic cardiomyopathy by inhibiting TLR4/NF-κB signalling in rats. Pharm Biol. 2021;59(1):121–128. doi:10.1080/13880209.2021.1877736
110. Wang YY, Li HM, Wang HD, et al. Pretreatment with berberine and yohimbine protects against LPS-induced myocardial dysfunction via inhibition of cardiac I-[kappa]B[alpha] phosphorylation and apoptosis in mice. Shock. 2011;35(3):322–328. doi:10.1097/SHK.0b013e3181facf73
111. Zhang HQ, Wang HD, Lu DX, et al. Berberine inhibits cytosolic phospholipase A2 and protects against LPS-induced lung injury and lethality independent of the alpha2-adrenergic receptor in mice. Shock. 2008;29(5):617–622. doi:10.1097/SHK.0b013e318157ea14
112. Aggarwal BB, Harikumar KB. Potential therapeutic effects of curcumin, the anti-inflammatory agent, against neurodegenerative, cardiovascular, pulmonary, metabolic, autoimmune and neoplastic diseases. Int J Biochem Cell Biol. 2009;41(1):40–59. doi:10.1016/j.biocel.2008.06.010
113. Pivari F, Mingione A, Brasacchio C, Soldati L. Curcumin and Type 2 diabetes mellitus: prevention and treatment. Nutrients. 2019;11(8):1837. doi:10.3390/nu11081837
114. Huang JZ, Guan BB, Lin LJ, Wang YP. Improvement of intestinal barrier function, gut microbiota, and metabolic endotoxemia in type 2 diabetes rats by curcumin. Bioengineered. 2021;12(2):11947–11958. doi:10.1080/21655979.2021.2009322
115. Burge K, Gunasekaran A, Eckert J, Chaaban H. Curcumin and intestinal inflammatory diseases: molecular mechanisms of protection. Int J Mol Sci. 2019;20(8):1912. doi:10.3390/ijms20081912
116. Wang N, Wang G, Hao J, et al. Curcumin ameliorates hydrogen peroxide-induced epithelial barrier disruption by upregulating heme oxygenase-1 expression in human intestinal epithelial cells. Dig Dis Sci. 2012;57(7):1792–1801. doi:10.1007/s10620-012-2094-7
117. Zhou X, Ren M, Yang J, Pan H, Yu M, Ji F. Curcumin improves epithelial barrier integrity of Caco-2 monolayers by inhibiting endoplasmic reticulum stress and subsequent apoptosis. Gastroenterol Res Pract. 2021;2021:5570796. doi:10.1155/2021/5570796
118. Tian S, Guo R, Wei S, et al. Curcumin protects against the intestinal ischemia-reperfusion injury: involvement of the tight junction protein ZO-1 and TNF-α related mechanism. Korean J Physiol Pharmacol. 2016;20(2):147–152. doi:10.4196/kjpp.2016.20.2.147
119. Cao S, Wang C, Yan J, Li X, Wen J, Hu C. Curcumin ameliorates oxidative stress-induced intestinal barrier injury and mitochondrial damage by promoting Parkin dependent mitophagy through AMPK-TFEB signal pathway. Free Radic Biol Med. 2020;147:8–22. doi:10.1016/j.freeradbiomed.2019.12.004
120. Nelson KM, Dahlin JL, Bisson J, Graham J, Pauli GF, Walters MA. The essential medicinal chemistry of curcumin. J Med Chem. 2017;60(5):1620–1637. doi:10.1021/acs.jmedchem.6b00975
121. Dempe JS, Scheerle RK, Pfeiffer E, Metzler M. Metabolism and permeability of curcumin in cultured Caco-2 cells. Mol Nutr Food Res. 2013;57(9):1543–1549. doi:10.1002/mnfr.201200113
122. Ghosh SS, He H, Wang J, Gehr TW, Ghosh S. Curcumin-mediated regulation of intestinal barrier function: the mechanism underlying its beneficial effects. Tissue Barriers. 2018;6(1):e1425085–e1425085. doi:10.1080/21688370.2018.1425085
123. Lopresti AL. The problem of curcumin and its bioavailability: could its gastrointestinal influence contribute to its overall health-enhancing effects? Adv Nutr. 2018;9(1):41–50. doi:10.1093/advances/nmx011
124. Karimi A, Ghodsi R, Kooshki F, Karimi M, Asghariazar V, Tarighat-Esfanjani A. Therapeutic effects of curcumin on sepsis and mechanisms of action: a systematic review of preclinical studies. Phytother Res. 2019;33(11):2798–2820. doi:10.1002/ptr.6467
125. Chen L, Lu Y, Zhao L, et al. Curcumin attenuates sepsis-induced acute organ dysfunction by preventing inflammation and enhancing the suppressive function of Tregs. Int Immunopharmacol. 2018;61:1–7. doi:10.1016/j.intimp.2018.04.041
126. Emel A, Hilal Y. Antioxidant and antiinflammatory efficacy of curcumin on lung tissue in rats with sepsis. J Tradit Chin Med. 2020;40(5):820–826. doi:10.19852/j.cnki.jtcm.2020.05.012
127. He D, Qiu M, Wang S, Yin H. [Protection of curcumin to intestinal mucosal barrier by inhibiting enterocyte apoptosis in septic rats]. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021;33(9):1052–1056. Chinese. doi:10.3760/cma.j.cn121430-20210105-00008
128. Huang W, Li X, Wang D, et al. Curcumin reduces LPS-induced septic acute kidney injury through suppression of lncRNA PVT1 in mice. Life Sci. 2020;254:117340. doi:10.1016/j.lfs.2020.117340
129. Kumari A, Tyagi N, Dash D, Singh R. Intranasal curcumin ameliorates lipopolysaccharide-induced acute lung injury in mice. Inflammation. 2015;38(3):1103–1112. doi:10.1007/s10753-014-0076-y
130. Lu W, Jiang JP, Hu J, Wang J, Zheng MZ. Curcumin protects against lipopolysaccharide-induced vasoconstriction dysfunction via inhibition of thrombospondin-1 and transforming growth factor-beta1. Exp Ther Med. 2015;9(2):377–383. doi:10.3892/etm.2014.2105
131. Vachharajani V, Wang SW, Mishra N, El Gazzar M, Yoza B, McCall C. Curcumin modulates leukocyte and platelet adhesion in murine sepsis. Microcirculation. 2010;17(6):407–416. doi:10.1111/j.1549-8719.2010.00039.x
132. Wang S, Zhao P, Zhang Y, et al. The therapeutic effects of curcumin in early septic acute kidney injury: an experimental study. Drug Des Dev Ther. 2021;15:4243–4255. doi:10.2147/DDDT.S332623
133. Xiao X, Yang M, Sun D, Sun S. Curcumin protects against sepsis-induced acute lung injury in rats. J Surg Res. 2012;176(1):e31–39. doi:10.1016/j.jss.2011.11.1032
134. Xu F, Lin SH, Yang YZ, Guo R, Cao J, Liu Q. The effect of curcumin on sepsis-induced acute lung injury in a rat model through the inhibition of the TGF-beta 1/SMAD3 pathway. Int Immunopharmacol. 2013;16(1):1–6. doi:10.1016/j.intimp.2013.03.014
135. Yang C, Wu K, Li SH, You Q. Protective effect of curcumin against cardiac dysfunction in sepsis rats. Pharm Biol. 2013;51(4):482–487. doi:10.3109/13880209.2012.742116
136. Yin H, Qiu M, He D, et al. Protective effect of curcumin on hepatocytes in rats with sepsis. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2017;29(2):162–166. doi:10.3760/cma.j.issn.2095-4352.2017.02.013
137. Zhao ML, Wang YL, Yue YF, et al. Curcumin alleviates neuronal apoptosis and cerebral mitochondrial dysfunction in septic mice. Int J Clin Exp Med. 2016;9(3):6107–6113.
138. Zhong W, Qian K, Xiong J, Ma K, Wang A, Zou Y. Curcumin alleviates lipopolysaccharide induced sepsis and liver failure by suppression of oxidative stress-related inflammation via PI3K/AKT and NF-κB related signaling. Biomed Pharmacother. 2016;83:302–313. doi:10.1016/j.biopha.2016.06.036
139. Zhu H, Wang X, Wang X, Liu B, Yuan Y, Zuo X. Curcumin attenuates inflammation and cell apoptosis through regulating NF-κB and JAK2/STAT3 signaling pathway against acute kidney injury. Cell Cycle. 2020;19(15):1941–1951. doi:10.1080/15384101.2020.1784599
140. Siddiqui AM, Cui XX, Wu RQ, et al. The anti-inflammatory effect of curcumin in an experimental model of sepsis is mediated by up-regulation of peroxisome proliferator-activated receptor-gamma. Crit Care Med. 2006;34(7):1874–1882. doi:10.1097/01.CCM.0000221921.71300.BF
141. Dugo L, Collin M, Allen DA, et al. Insulin reduces the multiple organ injury and dysfunction caused by coadministration of lipopolysaccharide and peptidoglycan independently of blood glucose: role of glycogen synthase kinase-3beta inhibition. Crit Care Med. 2006;34(5):1489–1496. doi:10.1097/01.CCM.0000215457.83953.E3
142. Chen YT, Chen GD, Zhang JL, et al. Uncoupling protein 2 facilitates insulin-elicited protection against lipopolysaccharide-induced myocardial dysfunction. Mater Express. 2020;10(3):337–349. doi:10.1166/mex.2020.1642
143. Shen CA, Chai JK, Yao YM, Du XH, Sheng ZY. [Effect of insulin intensive treatment on hyper-proteolysis of skeletal muscle in scalded rabbit with sepsis]. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2006;18(3):139–142. Chinese.
144. Shi B, Yin C, Guo H, Li B, Liu LP. [Influence of intensive insulin therapy on the intestinal microcirculatory dysfunction in rats with sepsis]. Zhongguo Wei Zhong Bing Ji Jiu Yi Xue. 2009;21(8):492–494. Chinese.
145. Osinski C, Moret D, Clément K, Serradas P, Ribeiro A. Enteroendocrine system and gut barrier in metabolic disorders. Int J Mol Sci. 2022;23(7):3732. doi:10.3390/ijms23073732
146. Yang F, Zeng F, Luo X, et al. GLP-1 receptor: a new target for sepsis. Front Pharmacol. 2021;12:706908. doi:10.3389/fphar.2021.706908
147. Zaghloul MS, Elshal M, Abdelmageed ME. Preventive empagliflozin activity on acute acetic acid-induced ulcerative colitis in rats via modulation of SIRT-1/PI3K/AKT pathway and improving colon barrier. Environ Toxicol Pharmacol. 2022;91:103833. doi:10.1016/j.etap.2022.103833
148. Nozu T, Miyagishi S, Ishioh M, Takakusaki K, Okumura T. Phlorizin attenuates visceral hypersensitivity and colonic hyperpermeability in a rat model of irritable bowel syndrome. Biomed Pharmacother. 2021;139:111649. doi:10.1016/j.biopha.2021.111649
149. Kingir ZB, Özdemir Kural ZN, Cam ME, et al. Effects of dapagliflozin in experimental sepsis model in rats. Ulus Travma Acil Cerrahi Derg. 2019;25(3):213–221. doi:10.5505/tjtes.2018.82826
150. Maayah ZH, Ferdaoussi M, Takahara S, Soni S, Dyck JRB. Empagliflozin suppresses inflammation and protects against acute septic renal injury. Inflammopharmacology. 2021;29(1):269–279. doi:10.1007/s10787-020-00732-4
151. Niu Y, Chen Y, Sun P, et al. Intragastric and atomized administration of canagliflozin inhibit inflammatory cytokine storm in lipopolysaccharide-treated sepsis in mice: a potential COVID-19 treatment. Int Immunopharmacol. 2021;96:107773. doi:10.1016/j.intimp.2021.107773
152. Angé M, De Poortere J, Ginion A, et al. Canagliflozin protects against sepsis capillary leak syndrome by activating endothelial α1AMPK. Sci Rep. 2021;11(1):13700. doi:10.1038/s41598-021-93156-1
153. Carey IM, Critchley JA, DeWilde S, Harris T, Hosking FJ, Cook DG. Risk of Infection in Type 1 and Type 2 diabetes compared with the general population: a matched cohort study. Diabetes Care. 2018;41(3):513–521. doi:10.2337/dc17-2131
154. Abu-Ashour W, Twells L, Valcour J, et al. The association between diabetes mellitus and incident infections: a systematic review and meta-analysis of observational studies. BMJ Open Diabetes Res Care. 2017;5(1):10. doi:10.1136/bmjdrc-2016-000336
155. Fang M, Ishigami J, Echouffo-Tcheugui JB, Lutsey PL, Pankow JS, Selvin E. Diabetes and the risk of hospitalisation for infection: the Atherosclerosis Risk in Communities (ARIC) study. Diabetologia. 2021;64(11):2458–2465.
156. Brunkhorst FM, Engel C, Bloos F, et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 2008;358(2):125–139. doi:10.1056/NEJMoa070716
157. Arnone D, Chabot C, Heba AC, et al. Sugars and gastrointestinal health. Clin Gastroenterol Hepatol. 2021. doi:10.1016/j.cgh.2021.12.011
158. Zhang B, Liu K, Yang H, Jin Z, Ding Q, Zhao L. Gut microbiota: the potential key target of TCM’s therapeutic effect of treating different diseases using the same method-UC and T2DM as examples. Front Cell Infect Microbiol. 2022;12:855075. doi:10.3389/fcimb.2022.855075
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.