")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Antenatal Screening for Toxoplasmosis and Rubella in Saudi Arabia: Assessing the Need for Screening
Authors Al-Mughales J, Al-Rabia MW
Received 6 September 2023
Accepted for publication 29 November 2023
Published 6 December 2023 Volume 2023:16 Pages 3897—3905
DOI https://doi.org/10.2147/JMDH.S438895
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jamil Al-Mughales,1,2 Mohammed W Al-Rabia3
1Department of Clinical Microbiology and Immunology, Faculty of Medicine King Abdul-Aziz University, Jeddah, Kingdom of Saudi Arabia; 2Department of Clinical Laboratories-Diagnostic Immunology Division, King Abdul-Aziz University Hospital, Jeddah, Kingdom of Saudi Arabia; 3Department of Clinical Microbiology and Immunology, King Abdulaziz University, Jeddah, Kingdom of Saudi Arabia
Correspondence: Jamil Al-Mughales, Email [email protected]
Objective: Antenatal screening programs are highly recommended to limit maternal and neonatal infections such as toxoplasmosis and rubella. This study aimed to assess the seroprevalence of maternal toxoplasma and rubella among pregnant women tested during antenatal screening at the King Abdulaziz University Hospital, Saudi Arabia.
Methods: This descriptive cross-sectional study targeted pregnant women attending the King Abdulaziz University Hospital, Jeddah, Saudi Arabia, during the period of 2019– 2022 for antenatal follow-up. This study included 3653 pregnant women who attended an antenatal screening. The clinical consequences of pregnancy were evaluated and categorized into six main categories based on the related complications and comorbidities of the pregnant women. The data were analyzed using the SPSS program as a descriptive statistic, and an ANOVA was used to test the associations.
Results: The study findings showed that 12% of women were seropositive for toxoplasmosis and 71.4% were seropositive for rubella, and it found that almost all women (except two) were seronegative for Toxo IgM (immunoglobulin M) and rubella IgM, which indicates the absence of recent infections during the pregnancy. Approximately 19% and 4% of women who had no comorbidities experienced complicated pregnancies and delivery, respectively. Moreover, 1.3% of the pregnant women had comorbidities, complicated pregnancies, and problems during delivery. The mean Toxo IgG level was significantly higher in women with normal pregnancies than in those with other pregnancies. Rubella immunoglobulin levels did not significantly correlate with pregnancy or delivery problems.
Conclusion: The seropositivity prevalence of toxoplasma Ig M and rubella Ig M were very low at the King Abdulaziz University Hospital, Saudi Arabia, indicating absence of current infections. However, the benefits of routine antenatal screening in pregnant women remain unclear. This study was conducted at one hospital, with a limited sample of participants, and did not yield adequate evidence to recommend a broader implementation of antenatal testing for toxoplasmosis and rubella.
Keywords: antenatal screening, toxoplasmosis, rubella, Saudi Arabia
Introduction
Toxoplasmosis is a disease caused by the obligate intracellular protozoan Toxoplasma gondii and poses a global threat to human health. It is transmitted mainly through primary maternal infection during pregnancy, and rarely from preconception infection or reactivation of latent infection in immunodeficient pregnant women.1 Prevention of toxoplasmosis during pregnancy is based on prenatal screening and precautions to limit further negative consequences of infection on the mother or fetus.2
Prevention of toxoplasmosis and rubella during pregnancy is based on prenatal screening and vaccination to limit further negative consequences of the infection on mother or fetus.2 It was reported that congenital rubella syndrome could be prevented by postpartum immunization, and it was established as an effective strategy for prevention among high-risk women. Toxoplasmosis infection during pregnancy could be associated with negative outcomes such as subclinical infection of intrauterine fetuses.3 In the US and Europe, the incidence of toxoplasmosis affects about 1 to 5 out of the 10,000 live births. Neonatal screening can identify the majority of cases, according to later research from Denmark and Poland.4 On the other hand, reports from numerous developed countries, including Canada and the US, revealed that universal prenatal rubella screening and postpartum immunization are advised for women who test negative for the disease. Although there are screening programs for expectant mothers in many underdeveloped nations, the coverage varies greatly.5,6 The screening for infection is conducted twice or thrice during pregnancy to early detect infections that could harm the mother and fetus.7
A study conducted in Saudi Arabia showed that the prevalence of rubella among pregnant women is high.8 Toxoplasmosis and rubella are maternal infections that can infect the fetus, cause abortion, provoke teratogenic effects on developing embryos, cause congenital anomalies, and sometimes lead to life-threatening conditions.1 Furthermore, a study conducted in Iraq, a neighboring country of Saudi Arabia, showed that the presence of maternal immune response to infections during pregnancy could result in abortion.9
Routine prenatal screening and postnatal rubella immunization programs have been highly recommended since the 1970s to decrease the incidence of toxoplasmosis and rubella infections during pregnancy.2 Thus, this study aimed to assess the necessity of screening for maternal toxoplasmosis and rubella among pregnant women undergoing antenatal screening at King Abdulaziz University Hospital, Saudi Arabia. By investigating the prevalence of these infections among pregnant women and analyzing their association with adverse pregnancy outcomes, this study aimed to provide valuable data that can inform health-care policies and practices, ensuring the well-being of both mothers and their unborn children in the local context.
Materials and Methods
Study Design
This retrospective descriptive study was conducted at King Abdulaziz University Hospital, a tertiary referral hospital in the western region of Saudi Arabia, in Jeddah City.
This study design was similar to other previous studies conducted in different regions in Saudi Arabia.10,11
Study Setting and Period
This study was conducted at the King Abdulaziz University Hospital in Jeddah, Makkah, Saudi Arabia. Records of women who attended antenatal care between 2019 and 2022 were included in the study.
Sampling and Sample Size
All the women who underwent antenatal follow-up at the hospital during the study period were included in this retrospective study. A total of 3653 pregnant women screened for toxoplasmosis and rubella at the hospital were included in this study. Screening for toxoplasmosis and rubella during pregnancy is a routine investigation for pregnant women to ensure the safety of pregnancy and delivery. Enzyme-linked immunosorbent assay (ELISA) is used to detect antibodies against infections during the first trimester of pregnancy. Blood samples for toxoplasmosis and throat or blood samples were used to detect rubella during pregnancy, based on the Ministry of Health protocol for screening. Screening refers to a single test for toxoplasmosis and rubella that is routinely performed in pregnant women.
Data Collection
Data, including the incidence of maternal toxoplasmosis and other related maternal infections, were collected retrospectively from hospital records. In addition, the clinical outcomes of pregnancy were identified and grouped into six main categories based on the complications and comorbidities of pregnant women.
Data Analysis
The Statistical Package for the Social Sciences (SPSS) (IBM Corp., Armonk, NY, USA, 2021), version 26 was used to conduct a detailed analysis of the acquired data. The dataset was thoroughly analyzed using descriptive statistics, which included frequencies and percentages. This study also explored the complex connections between maternal infection and clinical pregnancy outcomes. Analysis of variance (ANOVA) was used for all the analyses. The investigation of possible correlations and differences between maternal infections and a variety of crucial clinical outcomes of pregnancy was made possible using this statistical technique.
Results
All 3653 pregnant women who underwent prenatal screening between 2019 and 2022 were included in this study. Their ages ranged from 31.1 (±6) years on average, which was normally scattered. Table 1 demonstrates the level of diagnostic parameters within the recommended cutoff points among pregnant women. ToxoIgM, IgG, and rubella IgG were the most frequently tested parameters among pregnant women, while only a small fraction of women were tested for other parameters. Almost all included women were tested for Toxo-M and Toxo-G. Regarding rubella Ig G antibodies, 94% of the pregnant women were tested for rubella IgG, while only 2.7% were tested for rubella-M (Table 2). For other parameters, the proportion of tested women ranged from 8.2% to 0.01% (Table 1). Among the women tested, the majority were within the normal range of immunological and hormonal parameters.
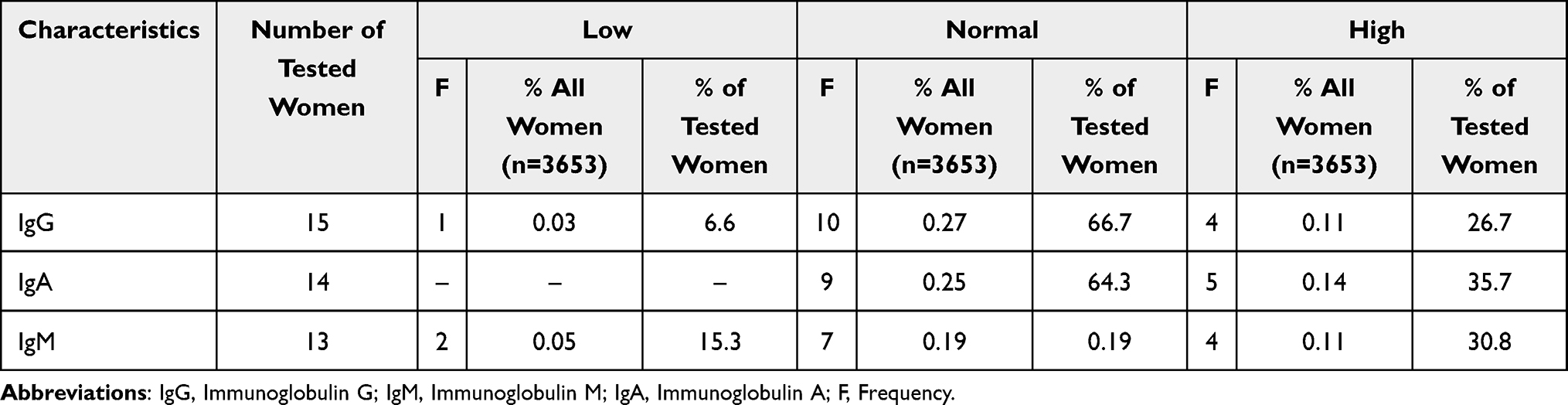 |
Table 1 The Distribution of Clinical Diagnostic Parameters of the Included Pregnant Women |
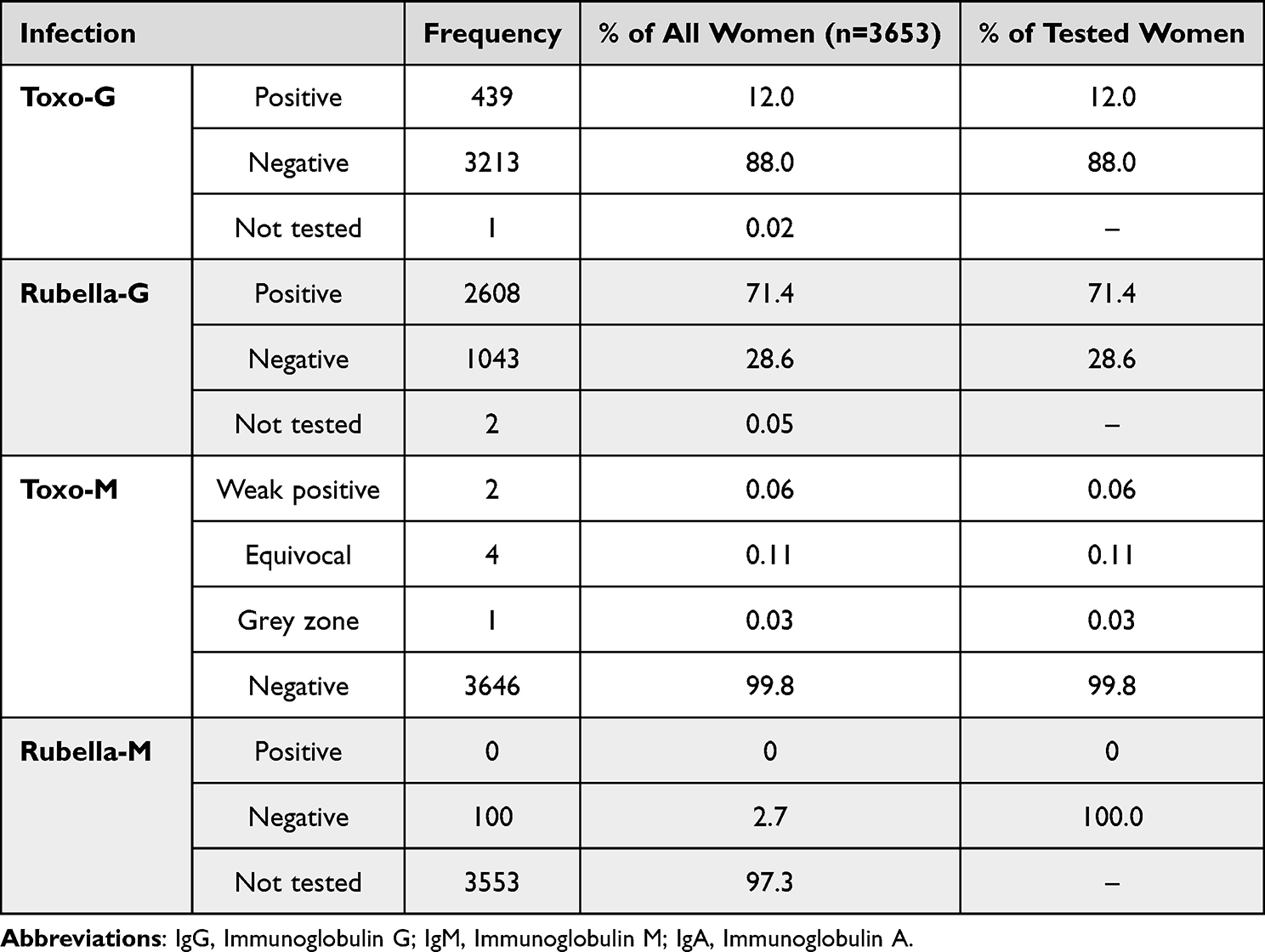 |
Table 2 Prevalence of Seropositivity of Toxoplasmosis and Rubella Among All Pregnant Women (n = 3653) |
Table 2 illustrates that almost all women were seronegative for Toxo-M and rubella-M, indicating the absence of recent infections with these microorganisms among pregnant women. In terms of Ig G antibodies, 12% of pregnant women tested positive for Toxo-G, whereas 71.4% tested positive for rubella-G.
Table 3 shows the six categories of clinical outcomes of pregnancy based on comorbidities, pregnancy complications, and course of delivery. It shows that the majority of women (75.9%) experienced normal prenatal and natal conditions either in the presence or absence of other chronic diseases. About 18.7% and 4.1% of participants experienced problems during pregnancy and delivery, respectively, in the absence of chronic diseases, while 1.3% of those with chronic diseases have experienced problems during labor, in addition to the problems in delivery and pregnancy.
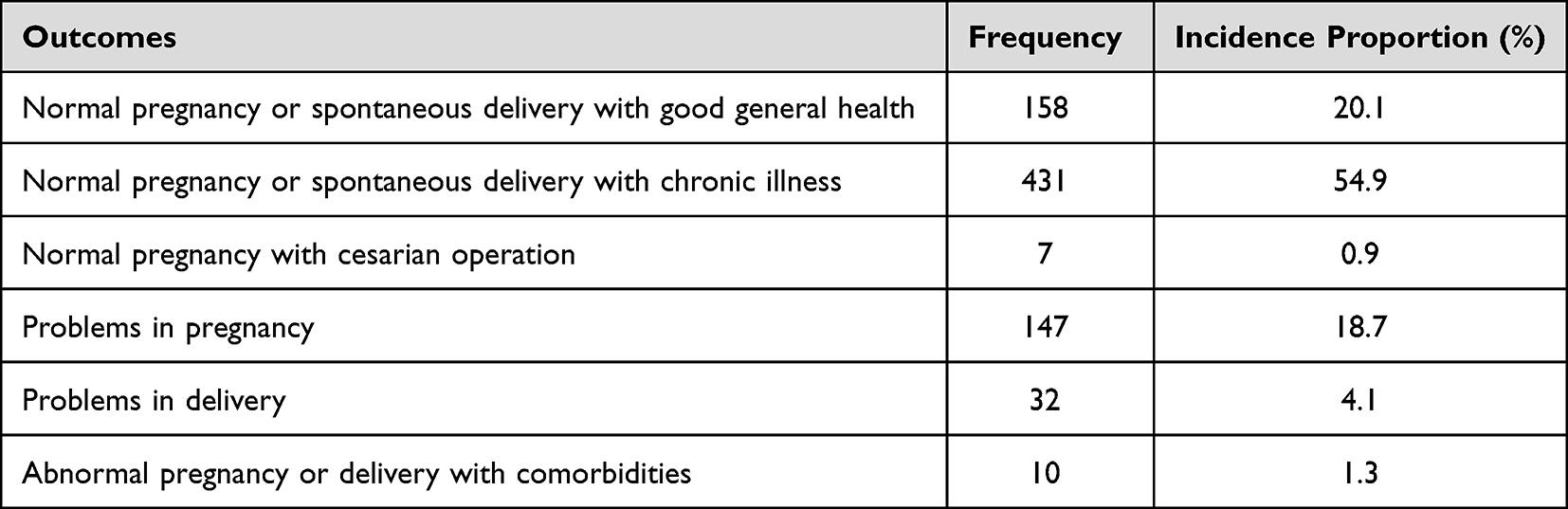 |
Table 3 Clinical Outcomes of the Pregnant Women Based on Comorbidities, Pregnancy Complications, and Course of Delivery (n = 785) |
Table 4 shows the differences between certain clinical parameters among pregnant women based on the course of pregnancy and/or delivery. When categorical variables of the diagnostic parameters (normal/abnormal) were used to detect statistically significant associations, no significant differences were detected using the chi-squared test. However, comparing the means of some important clinical parameters based on pregnancy and/or delivery status using a t-test identified significant differences between the groups.
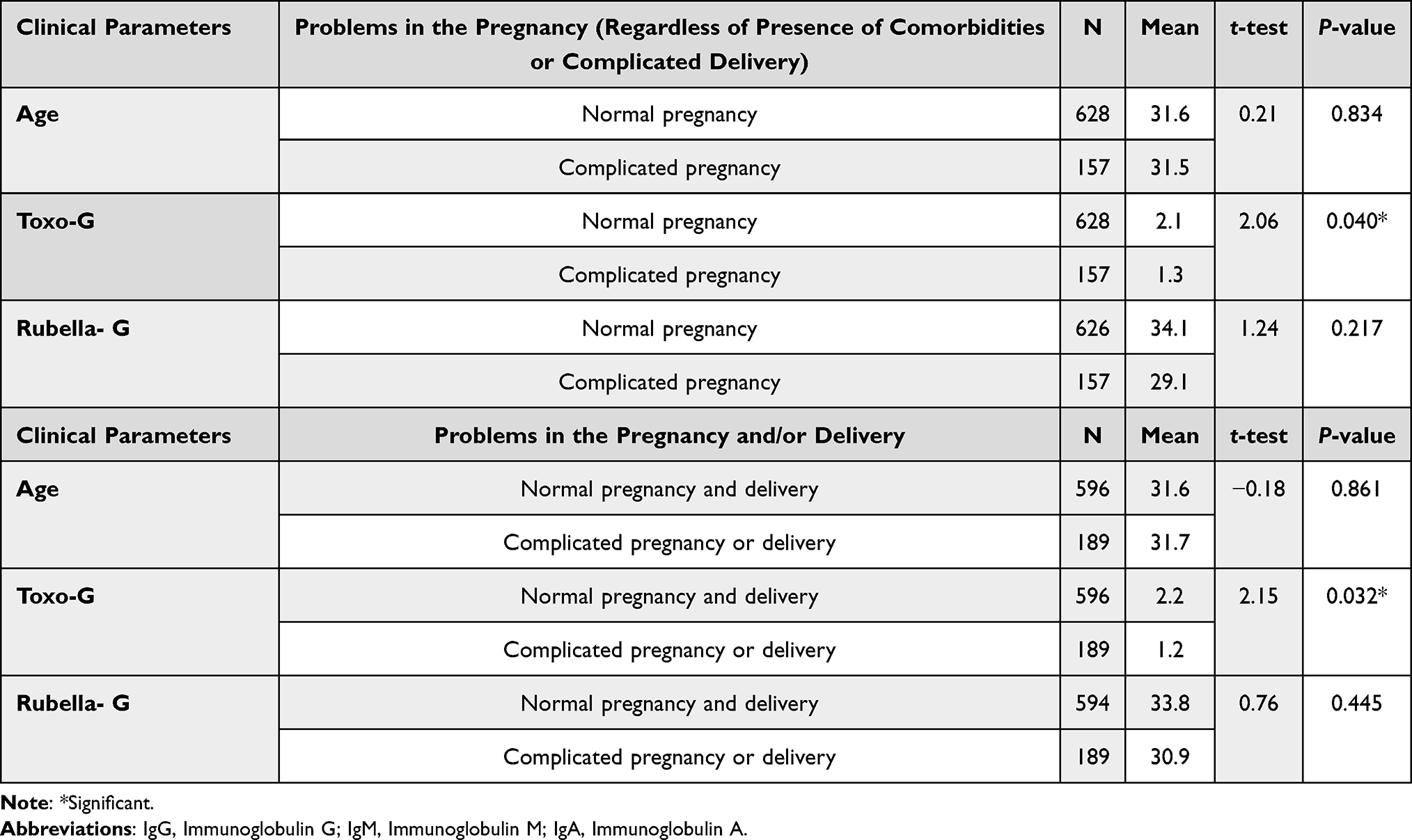 |
Table 4 Difference Between Certain Clinical Parameters Among Pregnant Women Based on the Course of Pregnancy and Delivery |
Regardless of delivery and general health condition, the mean Toxo-G level was significantly higher in women with normal pregnancies than in those with complicated pregnancy. It poses risk for pregnant women or/and her developing fetus such as caesarean delivery, antenatal hemorrhage, or chorioamnionitis (2.1 vs 1.3, p = 0.040). Other parameters, including age and rubella-G level, were not statistically different between women with normal pregnancies and those with complicated pregnancies. The average Toxo-G level was significantly higher in women with normal natal and prenatal conditions than in those with complicated pregnancies or delivery (2.2 vs 1.2, p = 0.032). Other parameters, including age and rubella-G level, were not statistically different between women who had both normal pregnancy and delivery and those with complicated pregnancy or delivery.
Discussion
The findings of this study indicate that 3653 pregnant women who underwent prenatal screening were included in the analysis. Antenatal screening protocol in Saudi Arabia focuses on toxoplasmosis and rubella. In our data, Toxo IgG, rubella IgG, and IgM antibodies were the most frequently tested parameters among the included women, and only a few missed the screening. This could be attributed to the recommended policy of antenatal screening with a focus on rubella prevention by detection and vaccination of unimmunized women, whereas the cornerstone in toxoplasma prevention is to detect recent cases and bring them to treatment. However, global antenatal screening remains controversial, despite the presence of effective interventions against these infections.
Several studies have indicated that many toxoplasmosis cases are not reported or are not detected because of mild conditions or because the disease is prevalent.12,13 Preliminary results showed the significant effectiveness of antibiotic therapy in preventing transmission and decreasing the severity of toxoplasmosis infections; however, not all studies have supported such dramatic improvement.14 Postnatal vaccination is acknowledged to be an effective approach for the prevention of congenital rubella syndrome.
The guidelines of the National Institute for Clinical Excellence for routine antenatal follow-up do not recommend routine antenatal screening for toxoplasmosis for several reasons, including unnecessary treatment, unnecessary termination of pregnancies, distress and discomfort of frequent investigations, and follow-up, which may outweigh the expected benefits of the screening program. Furthermore, available evidence supporting the treatment of toxoplasmosis is not robust. Some studies have concluded that incorporating routine antenatal screening for toxoplasmosis is not recommended, particularly in countries without full access to treatment.15
In several developed countries, including the US and Canada, comprehensive antenatal screening for rubella in addition to subsequent postpartum vaccination is highly recommended for seronegative women. In the US, the recommendation is actually to ideally obtain pre-conception labs including rubella and immunize prior to conception.16 This would actually help protect the fetus from infection. Although many developing countries have screening programs for pregnant women, their coverage differs broadly.5,6 However, some studies have reported a high prevalence of toxoplasmosis and rubella. A study of 738,588 pregnancies found 183 seroconversions for Toxoplasma with an overall incidence of seroconversion and suspected infection in pregnancy of 0.8 per 1000 live births and an incidence of congenital toxoplasmosis in 0.1 per 1000 live births.17 Furthermore, a systematic review of toxoplasmosis in Saudi Arabia showed that more than one-third of the population is seropositive for IgG or IgM.18
As an alternative approach, some studies have suggested conducting neonatal screening, which has been implemented in many countries to detect maternal infections, enable medical intervention, and prevent complications.19,20
In the present study, almost all women were seronegative for Toxo-M and Rubella-M, indicating the absence of recent infections in pregnant women. These findings could be attributed to high living standards and reduced contact with soil and cats, which are potential risk factors for toxoplasmosis. In the case of rubella, interruption of the transmission chain has been achieved through successful immunization programs in Saudi Arabia. Before the introduction of the expanded immunization program of immunization (EPI) in 1991, the incidence risk of congenital rubella syndrome was high with 7–27 cases per live births.21 In the late 1990s, routine screening for rubella IgG among pregnant women was implemented to identify unimmunized mothers. This syndrome has also been reported in many countries since the vaccination period.22–24 The present study found that 71.4% of pregnant women were seropositive for rubella-G, which highlights a gap of 28.6% among unimmunized women, representing a considerable proportion of unimmunized women in the community. These women should be vaccinated; otherwise, their babies are vulnerable to complications from rubella congenital syndrome. In the Western region, an immunity gap was reported by Alsibiani, who conducted a study in Jeddah, and she found that 8.4% of 10,276 pregnant women were seronegative for rubella IgG.25 Our data had a larger sample size and were more generalizable to the western region.
With regard to toxoplasmosis, we found that only 12% of the pregnant women were seropositive for Toxo-G. In the absence of a vaccine, this level of immunity was obtained by infection with toxoplasma before conception. The ethical issues related to stopping screening for pregnant women, regardless of the expensive cost of testing for toxoplasma, in addition to the negative consequences of toxoplasmosis, which could be associated with increased intervention and treatment, indicate the need for antenatal screening for these two infections.26 The most suitable alternative is to focus on prevention through early identification of cases and their risk factors and to enhance pregnant women’s awareness through health education during the first antenatal visit.27,28 Screening in prenatal settings for such an infection is inevitable to avoid adverse consequences, as reported in a study conducted in Saudi Arabia,8 which indicated that more than one million women underwent screening and about 9000 women during pregnancy. Another study in Rize province highlighted the importance of antenatal screening for rubella and toxoplasmosis.29
Despite the clear effect associated with congenital toxoplasmosis as a TORCH syndrome (ie, toxoplasmosis, syphilis, rubella, cytomegalovirus, and herpes infections), several aspects of surveillance and management of the disease have remained ongoing due to a lack of information and the benefits of medical treatment.30 Our study found that even in women with good health conditions, approximately 18.7% and 4.1% of women have experienced problems during pregnancy and labor, respectively. There is no reasonable association between the history of toxoplasmosis infection and a more “complicated” pregnancy or delivery. This link cannot be drawn from a retrospective cohort study on a limited sample and with undefined characteristics for what defines a “complicated” delivery. As a result, based solely on our investigation, this cannot definitively prove the preventive role of toxoplasmosis IgG on adverse gynecological outcomes in mothers and fetuses. Early identification and rapid management of cases are the standards of toxoplasmosis care in the absence of vaccination programs. This finding indicates further research into the underlying processes or confounding factors that may justify this association. In the US, the 1-year treatment regimen is the standard treatment, but its long-term benefits are not well known. Previous studies have shown that most asymptomatic infected children develop clinical symptoms.31,32 Neonatal tests can frequently reveal lesions; however, standard well-child examinations frequently miss congenital toxoplasmosis. Congenital toxoplasmosis monitoring requirements and clinical toxoplasmosis management strategies are still debatable, largely because of the lack of comprehensive information on the nature of the disease.
In European countries, there is a lack of public awareness regarding the prevention of congenital toxoplasmosis and rubella, which is best reflected in the variety of national public health policies for the prevention of these diseases.33,34 Furthermore, many countries have conducted wide and extensive antenatal and neonatal screening procedures.35 Of the many studies on diagnostic methods used in congenital toxoplasmosis and rubella, only a few allow reliable assessment of the performance of different tests involved in screening or clinical diagnosis.36 Implementing such a demanding screening program requires the full cooperation of general practitioners and women as well as making the sampling and testing accessible for public and target women because of the low uptake rate of follow-up services.37 European countries such as Denmark and Switzerland have stopped national maternal screening programs for these diseases.15,38 It is difficult to determine the incidence of maternal infection during pregnancy in countries with a long-standing screening protocol. Interestingly, neither country added screening protocols with proper surveillance systems for congenital infections for about three decades, until at least France instituted compulsory reporting in 2007.39 Furthermore, the UK National Screening Committee recently recommended that there be insufficient evidence for screening in the UK after a comprehensive review of antenatal and neonatal screening for toxoplasma infection.40
Despite providing valuable insights, this study has several notable limitations that should be acknowledged. The first noteworthy limitation is that it lacks generalizability of the findings. This study was conducted at one hospital in Saudi Arabia, and the results could only reflect the situation in this hospital. Another significant limitation is the retrospective design of the study. Relying on retrospective data collection can introduce inherent bias and limitations. This study, conducted at King Abdulaziz University Hospital, relied on historical data from medical records, potentially leading to incomplete or inconsistent data and hindering the establishment of robust causal relationships. This study primarily aimed to find any association between these infections and pregnancy outcomes using data available at the hospital. As a result, we did not include an analysis of other risk factors, such as geographical area, contact with cats, and eating habits. Finally, a notable constraint of the study lies in the relatively small sample size of pregnant women included. This limited sample size could potentially undermine the statistical power of the analyses and make it challenging to draw definitive conclusions regarding the efficacy and value of antenatal screening for maternal infection. These results, although suggestive, may not have sufficient weight to guide robust clinical recommendations, so further investigation is highly recommended to approve the casual relations.
Conclusion
The seropositivity prevalence of toxoplasma Ig M, which indicates new cases, is near zero at the King Abdulaziz University Hospital, Saudi Arabia. Thousands of women were routinely tested to detect only two weakly positive cases of toxoplasmosis, which were clinically selected and referred for further immunological confirmation. The benefits of routine antenatal testing for toxoplasmosis in pregnant women cannot be determined based on the limited data. This study, conducted at King Abdulaziz University Hospital, Saudi Arabia, with a limited sample of participants, did not yield adequate evidence to recommend the implementation of antenatal testing for toxoplasmosis and rubella in Saudi Arabia. In contrast, rubella antenatal testing for IgG revealed a significant gap in the coverage of rubella vaccination among pregnant women, as more than a quarter of pregnant women were unimmunized based on serological assessments.
Ethics Approval and Consent to Participate
Data were collected retrospectively from medical records after obtaining ethical approval from the King Abdulaziz University Hospital Ethics Committee. This study did not involve direct participation of patients, and only records of included patients were reviewed without names or identity. The authors confirm that confidentiality of patient data was strictly maintained throughout the study in accordance with the Declaration of Helsinki.
Data Sharing Statement
Data are available upon request from the corresponding author.
Acknowledgments
The author thanks the Deanship of Scientific Research of King Abdul-Aziz University, Jeddah, Saudi Arabia (RG-12-140-42) for funding this research. In addition, authors also thank Mrs olaa Saatti and Mrs Fatema Al-Jaberi From our Diagnostic Immunology division for the helping in the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Deanship of Scientific Research of King Abdul-Aziz University, Jeddah, Saudi Arabia (RG-12-140-42).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Milne G, Webster JP, Walker M. Toxoplasma gondii: an underestimated threat? Trends Parasitol. 2020;36(12):959–969. doi:10.1016/j.pt.2020.08.005
2. Robinson JL, Lee BE, Preiksaitis JK, Plitt S, Tipples GA. Prevention of congenital rubella syndrome—what makes sense in 2006? Epidemiol Rev. 2006;28(1):81–87. doi:10.1093/epirev/mxj007
3. Martin S. Congenital toxoplasmosis. Neonatal Netw. 2001;20(4):23–30. doi:10.1891/0730-0832.20.4.23
4. Havelaar A, Kemmeren J, Kortbeek L. Disease burden of congenital toxoplasmosis. Clin Infect Dis. 2007;44(11):1467–1474. doi:10.1086/517511
5. Gyorkos TW, Tannenbaum TN, Abrahamowicz M, Delage G, Carsley J, Marchand S. Evaluation of rubella screening in pregnant women. CMAJ. 1998;159(9):1091–1097.
6. Lim GH, Harris T, Desai S, et al. Rubella immunity among prenatal women in Ontario, 2006–2010. BMC Infect Dis. 2013;13:1–9. doi:10.1186/1471-2334-13-362
7. Lange A, Thyrian J, Wetzka S, et al. The impact of socioeconomic factors on the efficiency of voluntary toxoplasmosis screening during pregnancy: a population-based study. BMC Pregnancy Childbirth. 2016;16(1):1–9. doi:10.1186/s12884-016-0966-0
8. Asiri AYS, Alsawa ITA, Anas MOF, et al. Cost-effectiveness analysis of serological prenatal screening for pregnant women in King Abdulaziz University Hospital: a single-center retrospective study. 2020.
9. Baqer NN, Saheb EJ, Ahmed NS, Alhadad NAA. The association of IL-3, IL-17A, and IL 27 serum levels with susceptibility to toxoplasmosis in recurrent abortion of Iraqi women. Exp Parasitol. 2022;234:108217. doi:10.1016/j.exppara.2022.108217
10. Almalki SSR, Ahmed WA, Elhaj YHA, et al. Demographical and clinical features of suspected cases of rotavirus gastroenteritis at Al-Baha region, Saudi Arabia. Saudi J Health Sci. 2022;11(1):43–47. doi:10.4103/sjhs.sjhs_38_22
11. Hazazi AA, Alhaj YH, Ahmed WA, et al. Seroprevalence of TORCH agents in women with spontaneous miscarriage in Jizan, Saudi Arabia. Egypt Acad J Biol Sci. 2023;15(2):79–90. doi:10.21608/eajbsc.2023.309933
12. Damar Çakırca T, İN C, Deniz M, Torun A, Akçabay Ç, Güzelçiçek A. Toxoplasmosis: a timeless challenge for pregnancy. Trop Med Infect Dis. 2023;8(1):63. doi:10.3390/tropicalmed8010063
13. Dubey J, Murata F, Cerqueira-Cézar C, Kwok O, Villena I. Congenital toxoplasmosis in humans: an update of worldwide rate of congenital infections. Parasitology. 2021;148(12):1406–1416. doi:10.1017/S0031182021001013
14. Mandelbrot L. Congenital toxoplasmosis: what is the evidence for chemoprophylaxis to prevent fetal infection? Prenat Diagn. 2020;40(13):1693–1702. doi:10.1002/pd.5758
15. Boubaker K, Raeber P, Vaudaux B, et al. Toxoplasmosis during pregnancy and infancy. A new approach for Switzerland. Swiss Med Wkly. 2008;138(49–50):1–8. doi:10.4414/SMW.2008.w30271
16. Centers for Disease Control Prevention. Revised ACIP recommendation for avoiding pregnancy after receiving a rubella-containing vaccine. MMWR Morb Mortal Wkly Rep. 2001;50(49):1117.
17. Donadono V, Saccone G, Maruotti GM, et al. Incidence of toxoplasmosis in pregnancy in Campania: a population-based study on screening, treatment, and outcome. Eur J Obstet Gynecol Reprod Biol. 2019;240:316–321. doi:10.1016/j.ejogrb.2019.07.033
18. Mohamed K. Toxoplasmosis in humans and animals in Saudi Arabia: a systematic review. J Infect Dev Ctries. 2020;14(08):800–811. doi:10.3855/jidc.12648
19. Lago EG, Neto EC, Melamed J, et al. Congenital toxoplasmosis: late pregnancy infections detected by neonatal screening and maternal serological testing at delivery. Paediatric Perinatal Epidemiol. 2007;21(6):525–531. doi:10.1111/j.1365-3016.2007.00869.x
20. Tanimura K, Yamada H. Maternal and neonatal screening methods for congenital cytomegalovirus infection. J Obstetrics Gynaecol Res. 2019;45(3):514–521. doi:10.1111/jog.13889
21. Cutts F, Vynnycky E. Modelling the incidence of congenital rubella syndrome in developing countries. Int J Epidemiol. 1999;28(6):1176–1184. doi:10.1093/ije/28.6.1176
22. Mawson AR, Croft AM. Rubella virus infection, the congenital rubella syndrome, and the link to autism. Int J Environ Res Public Health. 2019;16(19):3543. doi:10.3390/ijerph16193543
23. Shanmugasundaram D, Awasthi S, Dwibedi B, et al. Burden of congenital rubella syndrome (CRS) in India based on data from cross-sectional serosurveys, 2017 and 2019–20. PLoS Negl Trop Dis. 2021;15(7):e0009608. doi:10.1371/journal.pntd.0009608
24. Su Q, Feng Z, Hao L, et al. Assessing the burden of congenital rubella syndrome in China and evaluating mitigation strategies: a metapopulation modelling study. Lancet Infect Dis. 2021;21(7):1004–1013. doi:10.1016/S1473-3099(20)30475-8
25. Alsibiani SA. Rubella immunity among pregnant women in Jeddah, Western region of Saudi Arabia. Obstet Gynecol Int. 2014;2014:1–6. doi:10.1155/2014/659838
26. Nori W, Ali AI. Toxoplasmosis, a zoonotic infection; A critical and updated analysis: a Review Article. Iraqi J Vet Sci. 2021;35(Supplement I–III):95–99. doi:10.33899/ijvs.2021.131607.1980
27. Varella IS, Wagner MB, Darela AC, Nunes LM, Muller R. Seroprevalence of toxoplasmosis in pregnant women. J Pediatr. 2003;79(1):69–74.
28. Adeniyi OT, Adekola SS, Oladipo OM. Seroprevalence and risk factors associated with Toxoplasma gondii infection among pregnant women in Ile Ife, Southwestern Nigeria; 2023.
29. Gurlek B, Colak S. Antenatal toxoplasma gondii, rubella and cytomegalovirus infection screening among pregnant women attending tertiary university hospital. Obstet Gynaecol Reprod Med. 2019;25(2):74–80. doi:10.21613/GORM.2019.903
30. Campos VS, Calaza KC, Adesse D. Implications of TORCH diseases in retinal development—special focus on congenital toxoplasmosis. Front Cell Infect Microbiol. 2020;10:577. doi:10.3389/fcimb.2020.585727
31. McAuley JB. Congenital toxoplasmosis. J Pediatric Infect Dis Soc. 2014;3(suppl_1):S30–S35. doi:10.1093/jpids/piu077
32. Garweg JG, Kieffer F, Mandelbrot L, Peyron F, Wallon M. Long-term outcomes in children with congenital toxoplasmosis—a systematic review. Pathogens. 2022;11(10):1187. doi:10.3390/pathogens11101187
33. Gargaté MJ, Ferreira I, Vilares A, et al. Toxoplasma gondii seroprevalence in the Portuguese population: comparison of three cross-sectional studies spanning three decades. BMJ open. 2016;6(10):e011648. doi:10.1136/bmjopen-2016-011648
34. Shwab EK, Zhu X-Q, Majumdar D, et al. Geographical patterns of Toxoplasma gondii genetic diversity revealed by multilocus PCR-RFLP genotyping. Parasitology. 2014;141(4):453–461. doi:10.1017/S0031182013001844
35. Schmidt DR, Hogh B, Andersen O, Fuchs J, Fledelius H, Petersen E. The national neonatal screening programme for congenital toxoplasmosis in Denmark: results from the initial four years, 1999–2002. Arch Dis Child. 2006;91(8):661–665. doi:10.1136/adc.2004.066514
36. Jones JL, Lopez A, Wilson M, Schulkin J, Gibbs R. Congenital toxoplasmosis: a review. Obstet Gynecol Surv. 2001;56(5):296–305. doi:10.1097/00006254-200105000-00025
37. De Paschale M, Agrappi C, Manco MT, Cerulli T, Clerici P. Implementation of screening for Toxoplasma gondii infection in pregnancy. J Clin Med Res. 2010;2(3):112–116. doi:10.4021/jocmr2010.05.321w
38. Röser D, Nielsen HV, Petersen E, Saugmann‐Jensen P, Nørgaard‐Pedersen PB. Congenital toxoplasmosis—a report on the Danish neonatal screening programme 1999–2007. J Inherit Metab Dis. 2010;33:241–247. doi:10.1007/s10545-010-9124-4
39. Picone O, Fuchs F, Benoist G, et al. Toxoplasmosis screening during pregnancy in France: opinion of an expert panel for the CNGOF. J Gynecol Obstet Hum. 2020;49(7):101814. doi:10.1016/j.jogoh.2020.101814
40. Gilbert R, Peckham C. Congenital toxoplasmosis in the United Kingdom: to screen or not to screen? J Med Screen. 2002;9(3):135–141. doi:10.1136/jms.9.3.135
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.