")
Back to Journals » Journal of Pain Research » Volume 16
Animal-Assisted Psychotherapy for Pediatric Chronic Pain: Case Series of an Open Pilot Study to Test Initial Feasibility and Potential Efficacy
Authors Locher C, Petignat M, Wagner C, Hediger K, Roth B , Gaab J, Koechlin H
Received 31 October 2022
Accepted for publication 23 March 2023
Published 29 May 2023 Volume 2023:16 Pages 1799—1811
DOI https://doi.org/10.2147/JPR.S394270
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Cosima Locher,1,2 Milena Petignat,3 Cora Wagner,3 Karin Hediger,4– 6 Binia Roth,7 Jens Gaab,3 Helen Koechlin8– 10
1Department of Consultation-Liaison Psychiatry and Psychosomatic Medicine, University Hospital Zurich, University of Zurich, Zurich, Switzerland; 2Faculty of Health, University of Plymouth, Plymouth, UK; 3Division of Clinical Psychology and Psychotherapy, Faculty of Psychology, University of Basel, Basel, Switzerland; 4Division of Clinical Psychology and Animal-Assisted Interventions, Faculty of Psychology, University of Basel, Basel, Switzerland; 5Department of Epidemiology and Public Health, Swiss Tropical and Public Health Institute, Allschwil, Switzerland; 6Faculty of Psychology, Open University, Heerlen, the Netherlands; 7Interdisciplinary Pain Consultation, Child and Adolescent Psychiatry of Basel-Landschaft, Binningen, Switzerland; 8Department of Psychosomatics and Psychiatry, University Children’s Hospital Zurich, Zurich, Switzerland; 9Division of Child and Adolescent Health Psychology, Department of Psychology, University of Zurich, Zurich, Switzerland; 10Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children’s Hospital, Harvard Medical School, Boston, MA, USA
Correspondence: Helen Koechlin, Email [email protected]
Objective: Chronic pain is a common complaint in children and adolescents, placing an enormous burden on individuals, their families, and the healthcare system. New innovative approaches for the treatment of pediatric chronic pain (PCP) are clearly warranted, as drop-out rates in intervention studies are high and it can be difficult to engage patients with PCP in therapy. Here, animal-assisted interventions (AAIs) might be promising, since there is preliminary evidence for the approach in adults with chronic pain, and AAIs are generally known to foster the therapeutic motivation of patients. To date, however, AAIs have not been examined in pediatric chronic pain.
Methods: The aim of this open pilot study was to examine the initial feasibility of recruitment and potential efficacy of an animal-assisted group psychotherapy (including horses, rabbits, chickens, goats, and a dog), providing case reports of three children with chronic pain. We applied a mixed-methods approach, including the conductance of semi-structured interviews and assessment of quantitative pre-post data with a focus on pain severity, avoidance behavior, pain acceptance, and ability to defocus from the pain.
Results: The three participating girls (age: 9– 12 years) reported chronic pain in the head and abdomen. The process of recruitment turned out to be challenging. All three children reported reduced pain-related disability and pain-related distress, as well as an increased ability to accept pain and to defocus from the pain. The qualitative data revealed that patients and their parents had a positive attitude towards AAIs.
Conclusion: Our initial open pilot study is the first to investigate AAIs in the context of pediatric chronic pain. Notably, we had difficulties in the recruitment procedure, mostly due to the Covid-19 situation. Based on three case reports, we found some first indication that AAI approaches might be associated with symptom changes. Future randomized-control studies with larger sample sizes are clearly warranted.
Clinicaltrials.gov Identifier: NCT04171336.
Keywords: children and adolescents, chronic pain, animal-assisted psychotherapy, group-based
Introduction
Chronic pain is a prevalent condition in childhood and adolescence, around 25% of the population are affected.1 Pediatric chronic pain (PCP) poses a major health care concern, as it is associated with significant emotional distress and functional disability.2,3 PCP is also associated with an enormous burden on healthcare systems – in the United States, chronic pain costs around $19.5 billion dollars each year and ranks among the most expensive pediatric health problems.4 Chronic pain is best explained by an interplay of biological (eg, genetic predisposition, changes in pain signal transmission), social (eg, interpersonal relationships, social support or isolation), and psychological (eg, emotional state, psychological comorbidities) factors that interact and influence each other.5,6 The biopsychosocial model is widely accepted as a helpful and evidence-based approach to the understanding and treatment of chronic pain (e.g.,5,7,8). Hence, interventions for chronic pain that target all of these domains, so-called interdisciplinary approaches with strong collaborations of pediatricians, psychologists, physiotherapists, and other disciplines, have been established.8–10 This is also in line with the aim to support patients to return to normal functioning in the domains of sleep, school, social activities, and sports.11 However, in clinical practice, the first approach to manage PCP is often pharmacological, which is problematic, given the lack of evidence, the risk of side effects, and limited evidence for long-term efficacy.12,13 Non-pharmacological interventions on the other hand include physiotherapy, occupational therapy, psychotherapy, or complementary treatment, with mixed evidence depending on intervention and pain syndrome.14–17 Strategies in non-pharmacological approaches, such as defocusing,18 accepting the pain,19 and engagement in activity despite the pain20 are helpful to achieve treatment goals.
In clinical practice, however, effective pain management for children and adolescents remains poorly available,21,22 and finding suitable therapy placements in a specialized pain clinic can be very challenging for families.23 A recent study from a large Swiss children’s hospital reported a mean pain duration of 24 months before children and adolescents were referred to the clinic’s specialized pain consultation.24 In addition, clinicians often report that it can be difficult to engage patients with PCP in therapy and that the dropout rate is generally high.18 This is also evident in previous research that has reported dropout rates in intervention studies ranging from 8.4%25 to 32%,26 especially in interventions that span several weeks. New innovations are therefore critically needed for the treatment of PCP, as also claimed by a Lancet Child & Adolescent Health Commission.27
One potential and novel approach for the treatment of PCP might be animal-assisted interventions (AAIs). Previous research has shown that AAIs foster the therapeutic motivation of patients28 and support patients in reaching their therapy goals. Several studies have examined the effect of AAIs in the field of acute pain in children and adolescents, and found that AAIs can lead to a significant reduction of pain in children and adolescents in acute pediatric care settings.29–31 Likewise, a recent meta-analysis suggested that AAIs are associated with pain relief in hospitalized children and adolescents,32 for whom pain often remains under-recognized and under-treated.11 Other studies, however, did not find positive effects.33–35 Thus, the evidence base for the effects of AAIs on acute pain in children and adolescents is still weak, and many questions remain unanswered. Moreover, and to the best of our knowledge, no study has examined the effects of AAIs on chronic pain in children and adolescents. This is noteworthy, since a study in adults reported positive effects on pain, mood, and distress in patients with chronic pain following an animal-assisted intervention.36 Further, AAIs promote movement and provide opportunity and incentive for physical activity.37
The aim of this open pilot study was to examine the initial feasibility of recruitment via psychosomatic and pain consultations and potential efficacy of an animal-assisted intervention for children and adolescents with chronic pain. We describe the development and content of an animal-assisted group-based psychotherapy program for children and adolescents with chronic pain, and we provide three case reports of girls reporting chronic pain in the head and abdomen.
Methods
Study Design
We applied a mixed method approach: With the help of quantitative data, initial pre-post changes of pain severity (ie, pain intensity, pain-related disability, pain-related distress), pain acceptance, fear of pain, engagement in activities, and defocusing from the pain were assessed. The qualitative approach focused on participants’ subjective attitudes towards the group-based animal-assisted psychotherapy, focusing on families’ expectations before and experiences after the treatment.
Ethical Considerations and Trial Registration
Prior to implementation, the study was approved by the Ethics Committee Northwestern and Central Switzerland (EKNZ, Project-ID: 2020–00135) and registered at clinicaltrials.gov (NCT04171336). The study complies with the Declaration of Helsinki.38 Parental permission was obtained through an informed consent procedure. Children received an age-appropriate information sheet, and parents provided written consent. In the consent document, families were informed that the information they provided would be used for a scientific article, but the published data would not allow any conclusions regarding their identities. Additional institutional approval was not required to publish the case details, as the information used for the case series was based entirely on the questionnaires to which participants and parents consented.
Sample
Patients were recruited using convenience sampling via the psychosomatic and pain consultations at the University Children’s Hospital Basel, Switzerland (UKBB). Children and parents were informed about the possibility to participate in the study by their pain psychologist (author BR). If they were interested, they received further information about the study and could either forward their contact details or contact the investigators directly. Assessment of inclusion and exclusion criteria was done through an initial phone call. Children were included if they were between 7 and 12 years of age and lived with persistent or recurrent pain for three or more months. They had to be fluent in German, willing to participate in the study and to work with animals, as a positive attitude towards animals can be important for the effectiveness of AAIs. Allergy to animals and fear of animals were exclusion criteria. Initially, two animal-assisted psychotherapy groups with 6–8 children each were planned.
Setting
The Covid-19 pandemic prevented the implementation of the study during the spring and summer holidays 2020 (as initially planned), as non-urgent research activities were not permitted at the Faculty of Psychology, University of Basel. The study was then planned for the autumn holidays (October 2020), but recruitment presented with several challenges. The study team therefore decided to stop the recruitment process once we had enough participants for one group. Recruitment was ongoing between December 2019 and September 2020, with interruptions due to the pandemic situation. The Covid-19 protocol at that time allowed the meeting of small groups of up to 10 people, which was always respected – our sessions included a maximum of 6 people (participants and study team members). Further, the Veterinary Office of the Canton of Basel-Stadt, Switzerland, was consulted to ensure animal welfare at all times.
The intervention was conducted by the compas institute that offers nature- and animal-based interventions at the farm “Bäumlihof” in Riehen, Switzerland. The compas institute carries out various interventions in the field of therapy, prevention, and education, and works with horses, goats, rabbits, chickens, and dogs on open ground. All animals are kept in a species-appropriate manner and are specifically trained to work with children. The animals participating in the study are experienced in animal-assisted interventions, both in an individual and in a group format, as the compas institute is specialized in animal-assisted therapy. The individual abilities and preferences of animal species and individual animals are relevant when integrating animals into therapy. Therefore, different types of animals were used to address the various issues and achieve therapeutic goals. The choice of animals for the respective tasks was based on the following factors: use as a herd or individual, place of use, abilities, and physical contact. It is important to choose the animal species in such a way that the content of the therapy can be implemented without stress for the animal species, and that the animals enjoy it. On the farm, all animals live in a herd, some of them can be worked with as individuals, others in their herd only. Rabbits and chickens, for example, can be used exclusively in the herd, but horses can also be used as a single individual. With some animal species, the use is limited to their enclosure (chickens, rabbits), while with others it is possible to plan exercises outside the enclosure, for example going for a walk (horse, dog, goat). Another reason is physical contact, as not every species likes to be touched and it is crucial to respect these preferences. To stimulate the physical sensory system in patients, an animal needs to allow for and enjoy the physical contact without stress. Animal assisted therapy can only be successful if both the animal and the human experience the unity as enrichment.
To ensure animal welfare, the compas institute follows the One Health concept and works according to the guidelines of the International Association for Human-Animal Interaction Organizations39 as well as the leaflets from the Veterinary Association for Animal Welfare40 for animals in social service.
Study Procedure
Once a family agreed to participate in the study, a member of the study team arranged to visit the family at home. After obtaining written informed consent and answering any questions the families had, the study team member conducted a qualitative interview with the parents and the child separately, and audiotaped it. Following the interview, the study team member assisted the parents and the child with the completion of the baseline quantitative questionnaires, using an iPad.
The animal-assisted psychotherapy took place over six consecutive days for three hours each afternoon during the autumn school holidays (ie, October 5th to October 10th 2020). The intervention was conducted by a child and adolescent psychotherapist with special training in AAIs (completion of a Certificate of Advanced Studies in Animal-Assisted Therapy at the University of Basel, Switzerland; author MP). Additionally, three psychology master students assisted during the sessions. Most activities took place outside and were carried out in interaction with the different animals. The intervention included evidence-based psychotherapeutic components, ie, psychoeducation, mindfulness, defocusing, physical activity, and activation of individual resources, each of those components supported and amplified by the involvement of animals. Each of the six sessions focused on one of these specific topics, and different animals were involved (see Figure 1). During each session, a break was taken for snacks, and additional breaks were possible as needed. A specifically designed booklet was given to all participants. In the booklet, several exercises were described (see German original in eAppendix 1, see eAppendix 2 for English translation), and participants had the opportunity to take notes, draw, and glue pictures into the booklet. After the intervention, participants took the booklet home with them as a reminder of the exercises, their experiences, and the friends they had made during the week.
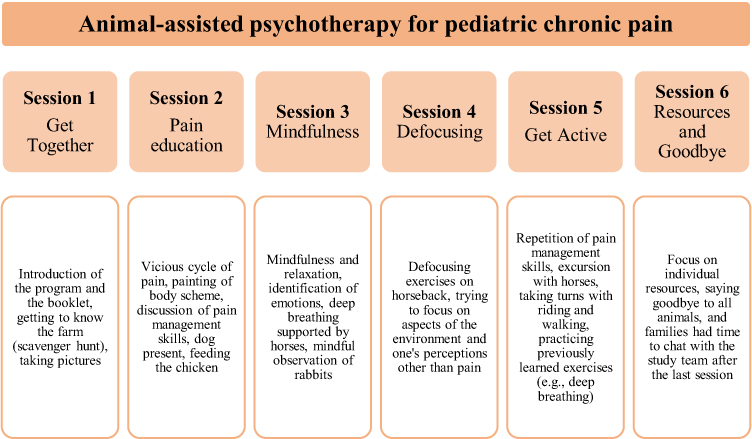 |
Figure 1 Content of intervention (one session per study day). |
After the last session, participants’ families were invited to a final get-together at the farm. They had the opportunity to explore the farm and the animals and ask questions to the study team. Additionally, it allowed families to get to know each other and to connect.
Approximately one week after the last session, a member of the study team visited the families at home again. An additional qualitative interview took place. Children also completed a set of quantitative questionnaires at the post-intervention visit.
Animal-Assisted Group-Based Psychotherapy: Content of the Program
Session 1: Get Together
The first session was used to explain the program to parents and children and allowed children to get to know each other, the animals, and the study team. Once the parents left, and by means of a scavenger hunt, children got to know the farm and all animals, and at the end of the scavenger hunt they found the booklets, which were then introduced in detail. The group took pictures from each participant and an animal of choice for the booklet and had the opportunity to specifically wish for a certain topic or activity to be covered during the intervention week.
Session 2: Pain Education
The focus of the second session was pain education. Therefore, children painted their body shape on the ground with chalk and marked their pain location(s). The group then discussed these paintings and photographed them for the booklet. After a short movement exercise, the vicious cycle of pain was explained, and children were asked what they currently did to manage their pain. The psychotherapist’s dog was present during this part of the session and included by explaining how pain affects dogs and what strategies dogs have to overcome pain. Finally, the group fed the chicken to motivate the children to get physically active, and collected skills against pain that each participant knew.
Session 3: Mindfulness
The third day centered around the topic of mindfulness. The group tried to identify different emotions and practiced deep breathing with the horses. A mindful eating exercise was done while eating a raisin. In addition, children observed the rabbits while being quiet and focusing solely on their observations.
Session 4: Defocusing
The topic of the fourth session was defocusing, ie, the ability to distract oneself from a current feeling, thought, or physical experience (such as pain). On the horseback, the group practiced defocusing in several exercises, for example, each child described five things they heard, then five things they felt, and finally five things they could smell. Once they finished, they started again, this time naming four things each, then three, then two, and then one. The goal of this and other exercises is to focus on aspects of the environment and one’s perception that is different from the pain experience.
Session 5: Get Active
In the fifth session, introduced pain management skills were repeated and further explored. The group got active during an excursion with the horses. Participants took turns with riding and practiced many of the exercises they have learnt during the week, such as deep breathing and defocusing exercises.
Session 6: Activate Resources and Goodbye Event
In the final session, the group focused on their resources, and on saying goodbye. The children said goodbye to all animals and collected resources of each animal on the farm. In the group, they collectively accumulated individual resources of each child. When parents arrived to pick up their child, the study team and all participants had time to connect.
Measures
Quantitative Measures
At the beginning and the end of each session, each child completed several questions on a visual analogue scale (VAS), rated on an 11-point-Likert scale ranging from 0 to 10. The VAS can be found in the supplement (eAppendix 5). As we were interested in changes of subjective pain severity ratings,41,42 we specifically asked about pain intensity (“How much pain you are in right now?”; 0 = No pain, 10 = Worst pain), pain-related interference (“How much does the pain interfere with daily activities?”; 0 = Not at all, 10 = Completely), and pain-related distress (“How distressed do you feel by the pain?”; 0 = Not at all, 10 = Completely). In addition, each child rated the extent to which they were able to defocus: As recommended by Dobe and Zernikow,18 we examined the degree of distraction each child was able to experience (“How much are you able to distract yourself at best?”). Again, this question was rated on a 11-point-Likert scale, ranging from 0 (no distraction) to 10 (maximum distraction). To assess pain acceptance, one item (“My life is going well even though I have chronic pain”.; 0 = Never true, 10 = Always true) from the Chronic Pain Acceptance Questionnaire (CPAQ) was used.43 Fear of pain (“When I feel pain, I am afraid that something terrible will happen”; 0 = Strongly disagree, 10 = Strongly agree) and avoidance behavior (“I put things off because of my pain”; 0 = Strongly disagree, 10 = Strongly agree) were assessed using two items from the German Fear of Pain Questionnaire for Children and Adolescents (GFOPQ-C).44
At the baseline and the post-intervention assessment, both parents and children completed the German Pain Questionnaire for Children, Adolescents and Parents.45 The German Pain Questionnaire for Children, Adolescents and Parents provides a multidimensional anamnestic assessment of chronic pain and is used as a tool for diagnosis and treatment in clinical practice. The questionnaire consists of 34 (self-report version, 11–18 years) or 57 (parent version) items in total. The items were used to receive multidimensional data about sociodemographic variables, previous pain treatment, pain characteristics, triggering factors, cognitive and emotional factors related to the pain experience and pain-related disability. This information can be found in the case descriptions and in eTables 1–9 in the supplement.
Qualitative Interviews
To get a more nuanced and detailed impression of participants’ and parents’ experience before and after the intervention, we conducted semi-structured interviews at baseline and post assessment. In the initial interview, parents were asked questions regarding the pain (eg, “what worries you regarding your child’s pain”), interest in animals (eg, “what effect do animals have on you and your family”), and specifically about the animal-assisted intervention (eg, “what do you expect and hope with regard to the therapy”). The questions for the children were similar with regard to content, but age-appropriately re-worded to ensure understanding.
The interview at the post assessment referred to the questions from the initial interview, with a special focus on parents’ and children’s experiences during the study. Again, parents and children were interviewed separately, using the same questions, but adapted for children in participants’ interviews. All questions can be found in eAppendix 3.
Statistical Analysis
In terms of quantitative data, we display changes across our primary and secondary outcomes for each participant separately (in their case reports) and discuss them in comparison to baseline assessments.
The qualitative interviews were analyzed by applying the structured content analysis.46 The structured content analysis is suitable for summary, structure, evaluation, and analysis of large datasets. The software MAXQDA was used.47 Similar passages were classified by topic and then combined into major categories, thereby identifying the main themes across participants. Thus, the original content was preserved, while an inductive summary at a higher level of abstraction was produced. Two independent raters (psychology master students trained by the first and last author) independently analyzed the transcripts in a first step, both trying to identify the main themes and factors of the messages. In a second step, the two coding schemes were compared, disagreements were debated with the first and last author (CL and HK), and consensus was reached on one scheme.
All results are reported according to the mission of the Transparent Reporting of Evaluations with Nonrandomized Designs,48 and the checklist can be found in the Supplement (eAppendix 4).
Case Examples
All Names in the Cases are Pseudonyms
Case 1: Sandra
Sandra, a 10-year-old girl with one sibling and who lived with both her parents, has had abdominal pain for almost a year at the time of inclusion into the study. She reported to have had a stomach flu just before the pain started. At the time of the study, Sandra did not take any medication for the pain, and described the pain as recurrent, usually with a pain intensity of 4 on a 0–10 visual analogue scale (VAS). No clear cause of the pain was found during several appointments and physical examinations with Sandra’s pediatrician, and Sandra had tried a herbal remedy for her pain, with no success. Her pain-related disability was high with an 8 on a 0–10 VAS scale, and she said she could not really defocus from her pain (ie, a 2 on a 0–10 VAS scale). She chose words like “cruel”, “woeful”, “hideous”, and “awful” to describe how she perceived her pain. When asked if her life was good despite the pain, Sandra chose a 0 on a 0–10 VAS scale. Sandra reported that both physical activity and rest helped with her pain, and that pain intensity increased with stress, sadness, anger, or nervousness. Her grandmother and grandfather both also experienced chronic pain, as reported by Sandra’s parents. According to Sandra’s parents, the pain was mainly due to stress and intensified when Sandra engaged in maladaptive behavior. Finally, Sandra also mentioned that she really loved animals.
Case 2: Natasha
Natasha, an 11-year-old girl who lived together with both her parents and two siblings, had a history of abdominal pain for about two years and, recurrently, sore throat. Her pain started after her mother received a cancer diagnosis. Natasha took paracetamol and ibuprofen once a month for her pain, with good results. She had not received a pain diagnosis and described her pain as recurrent, with highest pain intensity as 10 on a 0–10 VAS scale. In general, her pain was at a 6 on a 0–10 VAS scale, and her pain-related disability was at an 8. Natasha rated her ability to defocus from the pain as a 4 on a 0–10 VAS scale, and when asked if her life was good despite the pain, Natasha chose an 8. She described her pain with words like “cruel”, “hideous”, “awful”, and “unbearable”. She did not know why the pain started and reported that physical rest and regular standing up and walking around were helpful to decrease her pain. Natasha’s pain intensity increased when she was sad, mad, lonely, argumentative, or nervous. When asked about pain triggers, Natasha said that a heavy meal in the evening would lead to abdominal pain in the morning. She had started regular psychotherapy a few months before the study started. Her parents said they usually noticed early when the pain was about to start: It was when their daughter showed mood swings. Natasha’s parents identified a need for attention, nervousness, and stress as the causes of her pain.
Case 3: Anna
Anna, a 12-year-old girl who lived with both her parents and a sibling, reported chronic headache that persisted all day for a year at the start of the study. The pain started during a family holiday by the sea. Anna took paracetamol two or three times a month against her pain, with good results. Anna’s most intense pain was rated as a 10 on a 0–10 VAS scale, and she reported her mean pain to be around 3 on the same scale. Her pain-related disability was high with a 7 on a 0–10 VAS scale, as was pain-related distress with a 6 on the same scale. When asked whether her life was good despite the pain, Anna chose a 3 on the 0–10 VAS scale, and she rated her ability to de-focus as a 2. To describe her pain, Anna used words such as “cruel”, “dreadful”, “hideous”, “awful”, “pounding”, and “pulsating”. When asked about the causes for her pain, Anna mentioned stress and electronic devices. Physical activity, unfavorable body posture, and a lot of standing up and walking around increased the pain. Her pain also increased with stress, boredom, and nervousness, and Anna further identified sport, stress, boredom, sunlight, and heat as pain triggers. Anna’s headache has stopped her from hiking and doing sports. Anna’s mother lived with chronic migraine, especially triggered through physical exertion. Her parents reported that Anna had undergone neuropediatric assessment and that her reflexes were tested. According to her parents, Anna subsequently received the diagnosis “psychosomatic”, and tried relaxation once against her pain, with no success. Her parents explained Anna’s pain with genetic reasons, high expectations on herself, stress, and pressure.
Results
Initial Feasibility of Recruitment
Due to the onset of the Covid-19 pandemic, the psychosomatic and pain consultations at the UKBB were closed for several weeks, and consequently, recruitment turned out to be much more challenging than anticipated. This was despite the enthusiastic reaction of clinical partners, and a committed recruitment effort of the pain psychologist. The recruitment challenges might further indicate reduced acceptability towards an animal-assisted psychotherapy approach on the patients’ and/or parents’ side, as we received little reaction based on publicly available recruitment information (eg, in pediatricians’ practices).
Individual Changes Across Domains
None of the participants in the study wished for a specific activity or topic to be covered during the study period, hence all sessions were conducted as planned. The information in the cases all stem from the German Pediatric Pain Questionnaire,45 all answers from the child and parent version of the questionnaire can also be found in eTables 1–9 in the supplement.
Case 1: Sandra
Sandra’s most intense pain changed from a 5 at baseline to a 7 at the post-intervention assessment (ie, one week after the end of the intervention) on a 0–10 VAS scale. Her mean pain intensity (ie, answer to “how severe was your pain most of the time when you were in pain?”) decreased from a 4 at baseline to a 3 at post intervention. Both pain-related interference and pain-related distress decreased over the course of the study (interference – baseline: 8, post: 5; distress – baseline: 6, post: 5). Similarly, fear of pain (baseline: 6; post: 5), and avoidance (baseline: 4; post: 0) decreased on the VAS scale. Sandra’s self-reported ability to defocus increased drastically, from a 2 at baseline to an 8 at post assessment – as did her pain acceptance (baseline: 0; post: 8). With regard to her pain description, Sandra’s choice of adjectives changed insofar as that she described her pain as less “unbearable” and “stabbing”, compared to her baseline description.
Case 2: Natasha
For Natasha, most intense pain changed from 10 at baseline to 8 at post intervention, while mean pain intensity (ie, answer to “how severe was your pain most of the time when you were in pain?”) remained at a 6 on a 0–10 VAS scale. Pain-related interference and pain-related distress both decreased substantially (interference – baseline: 8, post: 3; distress – baseline: 6, post: 4), whereas the ability to defocus from and accepting the pain increased (defocusing – baseline: 4, post: 10; acceptance – baseline: 8, post: 10). Natasha’s fear of pain decreased from a 5 at baseline to 1 at post assessment, and her avoidance of activities due to the pain slightly increased from 0 at baseline to 1 at post assessment. Compared to her baseline description, Natasha described her pain experience as less “hideous”, “awful”, “unbearable”, and “pressing”, but as a bit more “abject”. Natasha received psychotherapeutic treatment at the time of the intervention, which was paused during the study week.
Case 3: Anna
Anna’s most intense pain remained high with a 10 at both baseline and post assessment, as did her mean pain intensity (ie, answer to “how severe was your pain most of the time when you were in pain?”) with 3 at baseline and post. Pain-related interference and distress both decreased, but to a varying degree (interference – baseline: 7, post: 6; distress – baseline: 6, post: 3). Surprisingly, Anna’s fear of pain increased over the course of the study (baseline: 0, post: 2), but avoidance of activities due to pain decreased (baseline: 5, post: 2). With regard to defocusing, Anna rated her ability to do so as a 2 at baseline, and as a 5 at post assessment on a 0–10 VAS scale. Her acceptance of pain increased from 3 at baseline to 5 at post assessment. When asked to describe her pain, Anna’s choice of words was more negative compared to baseline, with more emphasis on her pain being “grueling”, “abject”, “excruciating”, and “pulsating”, but as less “pounding”.
Baseline and Post Assessment Interviews
All interviews were transcribed by two independent psychology students (Master level). Child and parent interviews were evaluated together for both assessment points, baseline and post. The responses in the interviews varied in form and length. In total, four main categories were generated: importance of animals; expectations and wishes regarding the intervention; experienced effects of AAI approaches; and general feedback on the AAI approach in the study. Topics are presented by frequency of mention. Interrater reliability was between 62% and 83% for the initial and the final interviews and reached 100% after a final consensus meeting with the first and last author.
Importance of Animals (Number of Quotations =23)
Parents and children emphasized the importance of animals for them in general and for the intervention specifically. They reported on their favorite animals, their interests and curiosity regarding animals, animals fulfilling a play function, and the effects animals had on them. All but one family reported that they had pets (chickens, cats, a turtle, slugs).
Example statement of a parent: “I believe that animals have a positive effect on you anyway. Certain animals reflect very well what you do, so I think it’s a very positive effect”. Example statement of a child: “I cannot explain it, somehow it’s just awesome”.
Expectations and Wishes Regarding the Intervention (Number of Quotations= 22)
Parents and children shared what they expected or wished from the intervention, such as pain improvement, receiving tips or making new experiences either with or without animals. Children specifically wished to make experiences with the animals. Example statement of a parent: “Hopefully [name of the child] will have a good experience and maybe learn a little bit about mindfulness or feeling herself and well, just making many positive experiences, that’s the most important thing”. Example statement of a child: “Um well, so it [the intervention] could help”.
Experienced Effects of the AAI Approach (Number of Quotations=12)
Parents made statements about current and potential future effects of the therapy. Regarding effects that were already visible, they mentioned that defocusing from pain worked well, how it was helpful to learn new strategies to break the vicious cycle of pain, and making positive experiences despite the pain. Example of a parent statement: “I think so, at least she liked it. So, it has been what we hoped for. That she would make positive experiences, which she did”.
General Feedback on the AAI Approach (Number of Quotations =10)
Parents and children made statements about what they liked about the intervention, such as the exercises, the booklet, learning strategies to break the vicious cycle of pain or what their experiences with the animals. All children mentioned the same exercise that stuck with them most: In this exercise in session 3 (mindfulness), children were asked to solely focus on the rabbits and to watch them closely. Example statement of a parent: “Forgetting, distracting, which puts pain in the background, that’s certainly something that’s positive”. Example statement of a child: “I really liked that we did a lot of different things with various animals. And, yes, we also learned some exercises, like what we can do against pain and how we break the vicious cycle, I just really liked it”. Parents and children had nothing to criticize about the content of the intervention but mentioned that they would prefer a longer duration across several weeks.
Discussion
This small open pilot trial is an initial attempt to examine the recruitment feasibility and potential efficacy of an animal-assisted psychotherapy program for children with chronic pain. In terms of recruitment, the Covid-19 pandemic might in part explain why we had difficulties: It was challenging to inform patients and their parents about the planned study, as the specialized pain and psychosomatic consultations were closed for several weeks, and direct information about the study was therefore impossible. Furthermore, recruitment difficulties might also be an indicator for limited acceptability of the approach on the part of patients and their families. However, and in contrast to this, those patients and their parents who did participate showed enthusiastic reactions, and a high acceptability and openness towards AAIs.
Overall, our initial findings based on three case reports potentially indicate that an animal-assisted psychotherapy program may be efficacious in reducing pain-related disability, pain-related distress, and increase the ability to accept pain and to defocus. Our participants showed improvements across most domains, except for pain intensity. In pain clinics, it is a well-known phenomenon that pain-related disability and pain-related distress decrease, while pain intensity remains the same, which indicates that often a return to normal functioning precedes a reduction of pain intensity.11 However, as expectancies can modulate and treatment effects,49 it is still important to define the therapeutic goal of becoming (mostly) pain-free. Further, studies with adult patients with chronic pain show that a reduction of pain intensity is the highest ranked goal, mentioned before improvements in social activities, household tasks, sleep, and taking part in family or social activities.50 In semi-structured interviews, youth with chronic pain who took part in a multidisciplinary treatment explained that their preferred outcomes of therapy changed over the course of treatment: While pain and pain-related disability were their main focus in the beginning, emotional functioning gained more importance during treatment.51 In this sample, and similarly to our own results, pain intensity was the last area to change over the course of the study.
With regard to the other domains assessed, we found that across participants, acceptance of pain increased over time, while fear of pain decreased (for all but one participant). Acceptance of pain emphasizes functioning despite the pain and has been linked to greater adaptive functioning in pediatric chronic pain samples.19,52 Significant increases in pain acceptance have been reported in previous studies, eg, in an analysis of pre- vs posttreatment acceptance scores in pediatric participants of an interdisciplinary chronic pain rehabilitation program.53 Increases in pain acceptance are thought to contribute largely to positive changes in psychological variables.53,54 Similarly, fear of pain has also been found to be an important factor influencing functioning.55,56 For our participants, fear of pain decreased for two of them, while pain-related inference decreased as well. For our third participant, however, fear of pain increased slightly, as did pain-related interference. This makes sense, as according to the Fear Avoidance Model of Chronic Pain, those individuals with fear of pain might continuously exhibit avoidance or guarding behaviors that maintain or increase pain, leading to more pain-related interference.57,58
Our qualitative results reveal that, in general, patients and their parents had a very positive attitude towards the intervention and emphasized positive experiences. The strategies and exercises learned during the sixth session were perceived as helpful, especially learning how to break the vicious cycle of pain. All participants stated that the experiences they had made with the animals were most important to them. Specifically, an exercise during which participants were asked to solely observe the rabbits was mentioned by all participants as being the one moment that stuck with them most. A quote by one participant summarizes these experiences: “I’m never in pain when I’m here”.
Given the positive effects on all our participants, we have initial reasons to believe that AAIs might be well suited to increase the ability to defocus and engage in physical activity, as both are facilitated substantially in an animal-assisted context: In order to stay in contact with the animal, patients need to be focused on the animals, supporting them in learning how to defocus from the pain. Additionally, animals can have stress-regulating effects59 which helps children to feel at ease during the sessions and facilitates learning. Finally, animals provide spontaneity, fun, and being at a farm is often an appreciated change from a “standard” therapy setting. However, this must be further tested in larger and randomized trials that include a more diverse sample.
Our open pilot study has several limitations. First, and due to the non-randomized nature of the study, evaluators of outcomes were aware of participants’ treatment. Evaluators were psychology master students with an interest in animal-assisted interventions, which might have led to certain biases. Second, and relatedly, patients were also self-selected in a sense that children who were afraid of or allergic to animals did not participate and motivation to interact with animals was a prerequisite. Third, patients and their parents enthused on the setting and the environment of the compas institute, and research has shown that the environment itself can already have a healing effect.60 Fourth, the sample size was small, all participants were from a very similar socioeconomic background, and all participants identified as female. Thus, our results only allow very preliminary evidence for the potential effects of animal-assisted approaches for chronic pain in children, and the generalizability of the presented results is highly limited. Further, participants stated the wish for a longer intervention duration, which might also increase the chances for long-term changes. Finally, we did not conduct a follow-up assessment; hence, the duration of observed effects and their transfer to the daily life of participants remains unclear.
Conclusion
In conclusion, the preliminary findings of our small initial open study are promising, indicating that children with chronic pain might benefit from an animal-assisted psychotherapy program. The AAI approach seems especially helpful to support patients in improving their defocusing skills and to increase physical activity. Nevertheless, our hurdles with the recruitment process clearly warrant further exploration on the acceptability of the approach on the part of patients and their families. To further determine the efficacy of our program, an evaluation in a larger randomized-controlled trial is advisable.
Data Sharing Statement
Data can be made available upon request to the corresponding author.
Acknowledgments
The authors would like to thank Jorinde Straub, Paula Muser, and Silea Häusermann for their support with study procedures.
Funding
This study was supported by a grant from the “Stiftung für psychosomatische, ganzheitliche Medizin” given to Dr. Cosima Locher, Dr. Helen Koechlin and Mrs. Milena Petignat. At the time of manuscript submission, Dr. Koechlin was further supported by a grant of the Swiss National Science Foundation (SNSF; P5R5PS_203064), as were Dr. Locher (PZ00P1_201972) and Dr. Hediger (PCEFP1_194591).
Disclosure
The authors report no conflicts of interest in this work.
References
1. King S, Chambers CT, Huguet A, et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Elsevier. 2011;152:2729–2738. doi:10.1016/j.pain.2011.07.016
2. Schechter NL. Functional pain: time for a new name. JAMA Pediatr. 2014;168(8):693–694. doi:10.1001/jamapediatrics.2014.530
3. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
4. Groenewald CB, Essner BS, Wright D, Fesinmeyer MD, Palermo TM. The economic costs of chronic pain among a cohort of treatment-seeking adolescents in the United States. J Pain. 2014;15(9):925–933. doi:10.1016/j.jpain.2014.06.002
5. Bevers K, Watts L, Kishino ND, Gatchel RJ. The Biopsychosocial model of the assessment, prevention, and treatment of chronic pain. US Neurol. 2016;12(2):98–104. doi:10.17925/USN.2016.12.02.98
6. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
7. Nicholas MK. The biopsychosocial model of pain 40 years on: time for a reappraisal? PAIN. 2022;163(S1):S3. doi:10.1097/j.pain.0000000000002654
8. Gatchel RJ, McGeary DD, McGeary CA, Lippe B. Interdisciplinary chronic pain management: past, present, and future. Am Psychol. 2014;69(2):119–130. doi:10.1037/a0035514
9. Hechler T, Kanstrup M, Holley AL, et al. Systematic review on intensive interdisciplinary pain treatment of children with chronic pain. Pediatrics. 2015;136(1):115–127. doi:10.1542/peds.2014-3319
10. Schatman ME. Interdisciplinary chronic pain management: international perspectives. PAIN. 2012;20:1–6.
11. Friedrichsdorf SJ, Giordano J, Desai Dakoji K, Warmuth A, Daughtry C, Schulz CA. Chronic pain in children and adolescents: diagnosis and treatment of primary pain disorders in head, abdomen, muscles and joints. Children. 2016;3(4):42. doi:10.3390/children3040042
12. Eccleston C, Fisher E, Cooper TE, et al. Pharmacological interventions for chronic pain in children: an overview of systematic reviews. PAIN. 2019;160(8):1698–1707. doi:10.1097/j.pain.0000000000001609
13. Locher C, Kossowsky J, Koechlin H, et al. Efficacy, safety, and acceptability of pharmacologic treatments for pediatric migraine prophylaxis: a systematic review and network meta-analysis. JAMA Pediatr. 2020;174(4):341–349. doi:10.1001/jamapediatrics.2019.5856
14. Ayling CA, Amaria K, Campbell F, McGrath PA. Clinical impact and evidence base for physiotherapy in treating childhood chronic pain. Physiother Can. 2011;63(1):21–33. doi:10.3138/ptc.2009-59P
15. Koechlin H, Kossowsky J, Lam TL, et al. Nonpharmacological interventions for pediatric migraine: a network meta-analysis. Pediatrics. 2021. doi:10.1542/peds.2019-4107
16. Usichenko TI, Wolters P, Anders EF, Splieth C. Acupuncture reduces pain and autonomic distress during injection of local anesthetic in children: a pragmatic crossover investigation. Clin J Pain. 2016;32(1):82–86. doi:10.1097/AJP.0000000000000222
17. Yazdani S, Zeltzer L. Treatment of chronic pain in children and adolescents. Pain Manag. 2013;3(4):303–314. doi:10.2217/pmt.13.25
18. Dobe M, Zernikow B. Therapie von Schmerzstörungen im Kindes- und Jugendalter [Therapy of pain disorders in childhood and adolescence]. Springer; 2013. Available from: https://www.springer.com/de/book/9783642326714.
19. Wicksell RK, Melin L, Lekander M, Olsson GL. Evaluating the effectiveness of exposure and acceptance strategies to improve functioning and quality of life in longstanding pediatric pain – a randomized controlled trial. PAIN. 2009;141(3):248–257. doi:10.1016/j.pain.2008.11.006
20. Beeckman M, Simons LE, Hughes S, Loeys T, Goubert L, Network A. Analysis of potential antecedents and consequences of pain-related activity avoidance and activity engagement in adolescents. Pain Med. 2020;21(2):e89–e101. doi:10.1093/pm/pnz211
21. Birnie KA, Nguyen C, Do Amaral T, et al. A parent–science partnership to improve postsurgical pain management in young children: co-development and usability testing of the Achy Penguin smartphone-based app. Canad J Pain. 2018;2(1):280–291. doi:10.1080/24740527.2018.1534543
22. Curtis S, Wingert A, Ali S. The Cochrane library and procedural pain in children: an overview of reviews. Evide Based Child Health. 2012;7(5):1363–1399. doi:10.1002/ebch.1864
23. Palermo TM, Slack M, Zhou C, Aaron R, Fisher E, Rodriguez S. Waiting for a pediatric chronic pain clinic evaluation: a prospective study characterizing waiting times and symptom trajectories. J Pain. 2019;20(3):339–347. doi:10.1016/j.jpain.2018.09.009
24. Schneider T, Pfister D, Wörner A, Ruppen W. Characteristics of children and adolescents at the Switzerland-wide first ambulatory interdisciplinary pain clinic at the University Children’s Hospital Basel – a retrospective study. Swiss Med Wkly. 2019;15. doi:10.4414/smw.2019.20073
25. Palermo TM, Wilson AC, Peters M, Lewandowski A, Somhegyi H. Randomized controlled trial of an Internet-delivered family cognitive-behavioral therapy intervention for children and adolescents with chronic pain. Pain. 2009;146(1–2):205–213. doi:10.1016/j.pain.2009.07.034
26. Carter BD, Kronenberger WG, Cruce-Spurling S, et al. Factors associated with dropout versus completion of a manualized treatment for pediatric chronic pain. Clin Pract Pediatr Psychol. 2015;3(4):327–339. doi:10.1037/cpp0000119
27. Eccleston C, Fisher E, Howard RF, et al. Delivering transformative action in paediatric pain: a Lancet Child & Adolescent Health Commission. Lancet Child Adolesc Health. 2021;5(1):47–87. doi:10.1016/S2352-4642(20)30277-7
28. Hediger K, Thommen S, Wagner C, Gaab J, Hund-Georgiadis M. Effects of animal-assisted therapy on social behaviour in patients with acquired brain injury: a randomised controlled trial. Sci Rep. 2019;9(1):1–8. doi:10.1038/s41598-019-42280-0
29. Braun C, Stangler T, Narveson J, Pettingell S. Animal-assisted therapy as a pain relief intervention for children. Complement Ther Clin Pract. 2009;15(2):105–109. doi:10.1016/j.ctcp.2009.02.008
30. Calcaterra V, Veggiotti P, Palestrini C, et al. Post-operative benefits of animal-assisted therapy in pediatric surgery: a randomised study. PLoS One. 2015;10(6):e0125813. doi:10.1371/journal.pone.0125813
31. Silva NB, Osório FL. Impact of an animal-assisted therapy programme on physiological and psychosocial variables of paediatric oncology patients. PLoS One. 2018;13(4):e0194731. doi:10.1371/journal.pone.0194731
32. Feng Y, Lin Y, Zhang N, Jiang X, Zhang L. Effects of animal-assisted therapy on hospitalized children and teenagers: a systematic review and meta-analysis. J Pediatr Nurs. 2021;60:11–23. doi:10.1016/j.pedn.2021.01.020
33. Barker SB, Knisely JS, Schubert CM, Green JD, Ameringer S. The effect of an animal-assisted intervention on anxiety and pain in hospitalized children. Anthrozoös. 2015;28(1):101–112.
34. Havener L, Gentes L, Thaler B, et al. The effects of a companion animal on distress in children undergoing dental procedures. Issues Compr Pediatr Nurs. 2001;24(2):137–152.
35. Vagnoli L, Caprilli S, Vernucci C, Zagni S, Mugnai F, Messeri A. Can presence of a dog reduce pain and distress in children during venipuncture? Pain Manage Nurs. 2015;16(2):89–95. doi:10.1016/j.pmn.2014.04.004
36. Marcus DA, Blazek-O’Neill B, Kopar JL. Symptomatic improvement reported after receiving reiki at a cancer infusion center. Am J Hosp Palliat Care. 2013;30(2):216–217. doi:10.1177/1049909112469275
37. Velde BP, Cipriani J, Fisher G. Resident and therapist views of animal-assisted therapy: implications for occupational therapy practice. Aust Occup Ther J. 2005;52(1):43–50. doi:10.1111/j.1440-1630.2004.00442.x
38. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
39. IAHAIO. The IAHAIO definitions for animal assisted intervention and guidelines for wellness of animals involved in AAI; 2018. Available from: http://iahaio.org/wp/wp-content/uploads/2018/04/iahaio_wp_updated-2018-final.pdf.
40. TVT: Tiere im sozialen Einsatz. Tierärztliche Vereinigung für Tierschutz e.V [Animals in social use. Veterinary association for animal welfare]; 2022. Available from: https://www.tierschutz-tvt.de/arbeitskreise/tiere-im-sozialen-einsatz/.
41. Barke A, Koechlin H, Korwisi B, Locher C. Emotional distress: specifying a neglected part of chronic pain. Eur J Pain. 2019. doi:10.1002/ejp.1525
42. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the international classification of diseases (ICD-11). PAIN. 2019;160(1):19. doi:10.1097/j.pain.0000000000001384
43. McCracken LM, Vowles KE, Eccleston C. Acceptance of chronic pain: component analysis and a revised assessment method. Pain. 2004;107(1–2):159–166. doi:10.1016/j.pain.2003.10.012
44. Flack F, Gerlach AL, Simons LE, Zernikow B, Hechler T. Validation of the German fear of pain questionnaire in a sample of children with mixed chronic pain conditions. Eur J Pain. 2017;21:1224–1233. doi:10.1002/ejp.1022
45. Schroeder S, Hechler T H, Denecke H, et al. Deutscher Schmerzfragebogen für Kinder, Jugendliche und deren Eltern (DSF-KJ) [German Pediatric Pain Questionnaire for Children, Adolescents, and Their Parents]. Der Schmerz. 2010;24:23–37. doi:10.1007/s00482-009-0864-8
46. Mayring P. Qualitative content analysis: theoretical background and procedures. In: Bikner-Ahsbahs A, Knipping C, Presmeg N, editors. Approaches to Qualitative Research in Mathematics Education: Examples of Methodology and Methods. Springer Netherlands; 2015:365–380. doi:10.1007/978-94-017-9181-6_13
47. VERBI Software. MAXQDA 2022 [Computer Software]. Berlin, Germany: VERBI Software; 2022. Available from: maxqda.com.
48. CDC. TREND statement; 2019. Available from: https://www.cdc.gov/trendstatement/index.html.
49. Kong J, Wang Z, Leiser J, et al. Enhancing treatment of osteoarthritis knee pain by boosting expectancy: a functional neuroimaging study. NeuroImage. 2018;18:325–334. doi:10.1016/j.nicl.2018.01.021
50. Goudman L, De Smedt A, Linderoth B, et al. Identifying goals in patients with chronic pain: a European survey. Eur J Pain. 2021;25(9):1959–1970. doi:10.1002/ejp.1814
51. Joslin R, Donovan-Hall M, Roberts L. Exploring the outcomes that matter most to young people treated for chronic pain: a qualitative study. Children. 2021;8(12):1170. doi:10.3390/children8121170
52. McCracken LM, Gauntlett‐Gilbert J, Eccleston C. Acceptance of pain in adolescents with chronic pain: validation of an adapted assessment instrument and preliminary correlation analyses. Eur J Pain. 2010;14(3):316–320. doi:10.1016/j.ejpain.2009.05.002
53. Weiss KE, Hahn A, Wallace DP, Biggs B, Bruce BK, Harrison TE. Acceptance of pain: associations with depression, catastrophizing, and functional disability among children and adolescents in an interdisciplinary chronic pain rehabilitation program. J Pediatr Psychol. 2013;38(7):756–765. doi:10.1093/jpepsy/jst028
54. Dahl J, Luciano C, Wilson K. Acceptance and Commitment Therapy for Chronic Pain. New Harbinger Publications; 2005.
55. Leeuw M, Goossens MEJB, Linton SJ, Crombez G, Boersma K, Vlaeyen JWS. The fear-avoidance model of musculoskeletal pain: current state of scientific evidence. J Behav Med. 2007;30(1):77–94. doi:10.1007/s10865-006-9085-0
56. Simons LE, Kaczynski KJ. The fear avoidance model of chronic pain: examination for pediatric application. J Pain. 2012;13(9):827–835. doi:10.1016/j.jpain.2012.05.002
57. Kashikar-Zuck S, Vaught MH, Goldschneider KR, Graham TB, Miller JC. Depression, coping, and functional disability in juvenile primary fibromyalgia syndrome. J Pain. 2002;3(5):412–419. doi:10.1054/jpai.2002.126786
58. Simons LE, Kaczynski KJ, Conroy C, Logan DE. Fear of pain in the context of intensive pain rehabilitation among children and adolescents with neuropathic pain: associations with treatment response. J Pain. 2012;13(12):1151–1161. doi:10.1016/j.jpain.2012.08.007
59. Beetz A, Kotrschal K, Turner DC, Hediger K, Uvnäs-Moberg K, Julius H. The effect of a real dog, toy dog and friendly person on insecurely attached children during a stressful task: an exploratory study. Anthrozoös. 2011;24(4):349–368.
60. Bernstein MH, Locher C, Kube T, Buergler S, Stewart-Ferrer S, Blease C. Putting the ‘Art’ Into the ‘Art of Medicine’: the under-explored role of artifacts in placebo studies. Front Psychol. 2020;11:75.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.