Back to Journals » Journal of Asthma and Allergy » Volume 15
Anaphylaxis in Chinese Children with Pollen Sensitization: Triggers, Clinical Presentation, and Acute Management
Authors Jiang N, Xu W, Huang H, Hou X, Xiang L
Received 18 February 2022
Accepted for publication 5 May 2022
Published 16 May 2022 Volume 2022:15 Pages 633—643
DOI https://doi.org/10.2147/JAA.S363113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Nannan Jiang, Wei Xu, Huijie Huang, Xiaoling Hou, Li Xiang
Department of Allergy, Beijing Children′s Hospital, Capital Medical University, National Center for Children′s Health; Key Laboratory of Major Diseases in Children, Ministry of Education; National Clinical Research Center for Respiratory Diseases, Beijing, People’s Republic of China
Correspondence: Li Xiang, Department of Allergy, Beijing Children’s Hospital, Capital Medical University, National Center for Children′s Health, No. 56 Nanlishi Road, Xicheng District, Beijing, 100045, People’s Republic of China, Tel +861059616934, Fax +861059616934, Email [email protected]
Purpose: Pollen sensitization is increasing in children. However, there is little evidence regarding the characteristics of anaphylaxis in individuals with pollen sensitization.
Patients and Methods: We conducted a retrospective study of patients with anaphylaxis combined with pollen sensitization who attended an allergy department in a tertiary children’s hospital from 2014 to 2021.
Results: A total of 157 anaphylaxis events in 108 patients were analyzed; the mean age at the reaction was 5.8 ± 4.17 years. A total of 99.1% (107/108) of the patients came from northern China. The most common sensitizing pollen was mugwort (93.5%,101/108), followed by ragweed (68.5%, 74/108) and birch (40.7%, 44/108). A total of 76.9% (83/108) of the patients showed polysensitization to pollen. Allergic rhinitis/conjunctivitis was the most common comorbidity (87.0%, 94/108). Children with severe anaphylaxis were more likely to have a history of recurrent urticaria (16.1% vs 3.9%, p = 0.028). The most frequently implicated foods were fruits/vegetables (22.3%, 35/157), followed by wheat (8.9%, 14/157) and milk (8.3%, 13/157), and the most common fruit allergen was peach (n = 7). Of 14% (22/157) exercise-induced reactions, 63.6% (14/22) occurred in pollen season. Skin symptoms were the most frequent (86.0%, 135/157) symptoms, followed by respiratory (73.9%, 116/157) and gastrointestinal (21%, 33/157) symptoms. Regarding acute management, only 7.4% of the patients were treated with epinephrine.
Conclusion: Our findings revealed the characteristics of anaphylaxis in children with pollen sensitization. Fruits/vegetables accounted for a substantial percentage of anaphylaxis triggers. The suboptimal use of epinephrine highlights the need for educational programs promoting the use of epinephrine.
Keywords: anaphylaxis, pollen, exercise, epinephrine
Introduction
Anaphylaxis is the most severe form of allergy and is characterized by an acute, potentially life-threatening systemic reaction of rapid onset.1 Triggers and epidemiological factors associated with anaphylaxis vary with age, culture, and lifestyle.2 Recent data from England have demonstrated that the level of certain specific pollen, including Fraxinus (Ash), Ambrosia (Ragweed), and Quercus (Oak), are associated with higher risk of seasonality in food-induced anaphylaxis hospital admissions3 Similarly, one study in Sweden showed that the number of food-related anaphylaxis events among children allergic to pollen increased during tree pollen season;4 the above-mentioned studies raise the possibility that sensitization to pollen cross-reactive foods may lead to an increased risk of anaphylaxis during the pollen season. Anaphylactic reactions may occur either because stable cross-reactive proteins (such as LTP), or augmentation factors (large amounts of food, exercise, and pollen season) that increase reaction severity and high-level pollen exposure may trigger anaphylaxis in very rare cases.5–8
Pollen-related foods (eg, fruits, vegetables, nuts, cereals, and legumes) are the main food triggers of anaphylaxis in older children, especially among individuals with pollen allergy or sensitized to pollen, which is also known as pollen-food allergy syndrome (PFAS).2,9,10 About 9% of PFAS patients experience anaphylaxis.11 Given that the etiology of PFAS is related to pollen sensitization, geographical distribution of pollen allergens and regional dietary habits influence pollen-related food trigger sensitization profiles and clinical symptoms. In northern China, birch and mugwort are common pollen that cause seasonal respiratory allergies in the spring and autumn, respectively.12,13 Birch pollen has historically been considered the most common allergen among patients with pollen-related food allergy in Europe.14 However, birch pollen sensitization and PFAS are now also common in China, especially in northern China.12,15 Apples and hazelnuts are identified as the most frequent triggers in birch pollen-related food allergy.16 Anaphylaxis is the primary sign of mugwort pollen-related food allergy in China, and peach is the most common culprit.8
Anaphylaxis in individuals with pollen sensitization may result from PFAS due to thermostable food allergens that cross-reactivity with pollen or an IgE allergy to the pollen protein independent of food allergens.17 There is little evidence regarding the characteristics of anaphylaxis in individuals with pollen sensitization. The aim of this study was to identify the main elicitors of anaphylaxis in pediatric individuals with pollen sensitization, so as to help facilitate prompt recognition and management at an emergency department.
Patients and Methods
Ethics Statement
This study was performed in accordance with the principles stated in the Declaration of Helsinki, and the study protocol was approved by the Research and Ethics Board of Beijing Children’s Hospital (Approval number:2022-E-023-R).
Patients and Study Design
This was a retrospective study of children with symptoms and signs of anaphylaxis who were referred to a specialized allergy department in a tertiary children’s hospital. Medical records were retrospectively analyzed to identify the patients who were diagnosed with “anaphylactic shock” (ICD code T78.201), “anaphylaxis” (ICD code T78.402), and “severe allergic reactions” (ICD code T78.402) from January 2014 to December 2021. The patients’ records were manually reviewed by a pediatric allergy specialist to confirm whether the World Allergy Organization (WAO) 2020 diagnostic criteria were met, and then we selected the patients with pollen sensitization according to the report of allergen testing (Serum levels of sIgE testing and/or skin prick testing). A total of 108 patients with anaphylaxis who met the criteria were enrolled in this study. A detailed history was collected by allergists and included a combined allergic disease. Factors evaluated in our analysis included demographic data (eg, age and sex); clinical characteristics of the reaction (possible triggers and severity); comorbidities (prior history of anaphylaxis, asthma, allergic rhinitis, atopic dermatitis); acute management. The flowchart is shown in Figure 1.
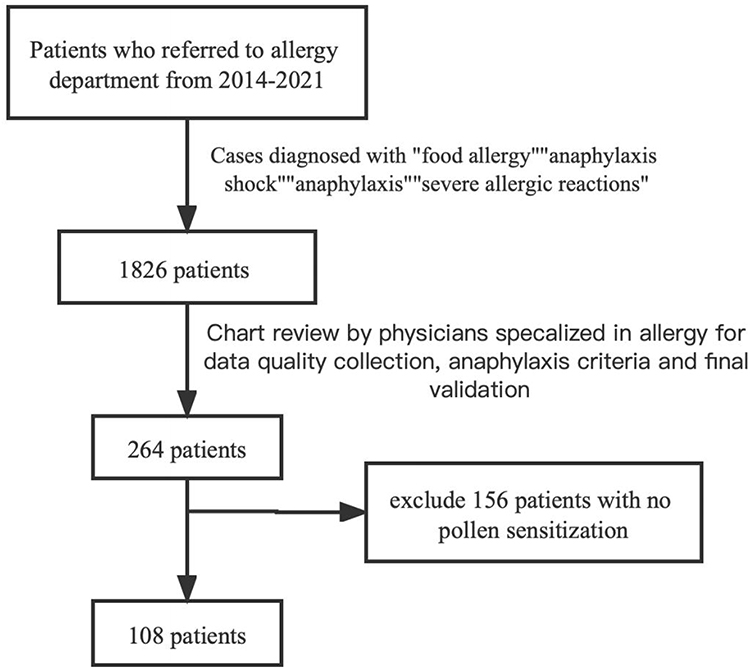 |
Figure 1 Study review flow chart. |
Clinical Diagnostic Criteria and Severity Grading
Assessment of the outpatients with anaphylaxis was based on the WAO 2020 criteria. Based on the current diagnostic criteria, anaphylaxis was defined as an acute allergic reaction involving more than two organ systems or life-threatening compromise in breathing and/or circulation alone. A modified grading system described by Muraro et al was used to classify the severity of anaphylaxis.18 Severe reactions were defined as loss of bowel control, cyanosis, respiratory arrest, hypotension (SBP <70 mm Hg in infants [1 month–1 year old], <70+[2×age] mm Hg in children aged 1–10 years), and <90 mmHg in patients aged >10 years) and/or circulatory collapse, arrhythmia, severe tachycardia and/or cardiac arrest, confusion, and loss of consciousness.
Identification of Triggers
Identification of a food as the trigger for anaphylaxis was based on an acute allergic reaction in which the onset was related to a known or suspected food allergen exposure. Serum levels of specific IgE testing (Phadia AB Uppsala, Sweden) and/or skin prick testing were performed to determine aeroallergen and food allergens. The detection limit was defined as 0.35 kUA/L, in accordance with the manufacturer’s recommendations. Skin tests were regarded as positive if the mean wheal diameter was ≥3 mm in the prick test. The skin testing was performed using standardized allergen extracts (Macro-Union Pharmaceutical Lim, Beijing, China). The diluent was administered as a negative control, and histamine hydrochloride (1 mg/mL) as a positive control. In addition, a positive score based on the wheal size was recorded as follows: Class 1, a wheal diameter between 3 and 5 mm; Class 2, a wheal diameter between 5 and 10 mm; Class 3, a wheal diameter between 1 and 2 cm; and Class 4, a wheal diameter ≥2 cm and the presence of pseudopods. Drug-induced anaphylactic episodes were mainly diagnosed based on medical history. If the medical records did not suggest a potential trigger and allergen-specific tests were negative, the episode was diagnosed as idiopathic.
Statistical Analysis
All statistical analyses were performed using SPSS 20.0 (IBM Inc., Chicago, IL). A descriptive analysis was used for characterization of the study population. The patient’s demographic and clinical characteristics were described as a percentage for categorical data and as mean ± standard deviation for continuous data. To compare frequencies of categorical variables, comparisons between different groups were performed using Pearson’s chi-squared test, or Fisher’s exact test, while t-tests were used to compare continuous variables. P-values lower than 0.05 were considered statistically significant.
Results
General Characteristics of the Patients
There were 108 children meeting the inclusion criteria after manual review using the WAO anaphylaxis criteria. These enrolled children were stratified into two groups based on the severity of anaphylaxis (Table 1). The mean age at the reaction was 5.8±4.17 years, and it was significantly older in severe anaphylaxis than in mild-to-moderate anaphylaxis (6.6 ± 4.94 years vs 5.6 ± 3.88 years, p = 0.01). When analyzing the allergic comorbidities, allergic rhinitis/conjunctivitis was the most common comorbidity (87.0%, 94/108). Children with severe anaphylaxis were more likely to have a history of chronic urticaria (16.1% vs 3.9%, p = 0.028). In terms of the pollen sensitization rate, the most common sensitized pollen was mugwort (93.5%,101/108), followed by ragweed (68.5%, 74/108) and birch (40.7%, 44/108). A total of 76.9% (83/108) of the patients showed polysensitization to pollen. A total of 99.1% (107/108) of the patients came from northern China. The geographic distribution of the patients is shown in Supplement Table 1. Birch sensitization rate was much higher in severe anaphylaxis patients (61.2% vs 32.5%, p = 0.006), while monosensitization to mugwort was more common in the mild-to-moderate group (24.7% vs 3.1, p = 0.009); however, patients co-sensitized to birch and mugwort tended to experience severe anaphylaxis (19.4% vs 6.5%, p = 0.046). Recurrence of anaphylaxis was observed in 43 patients (39.8%).
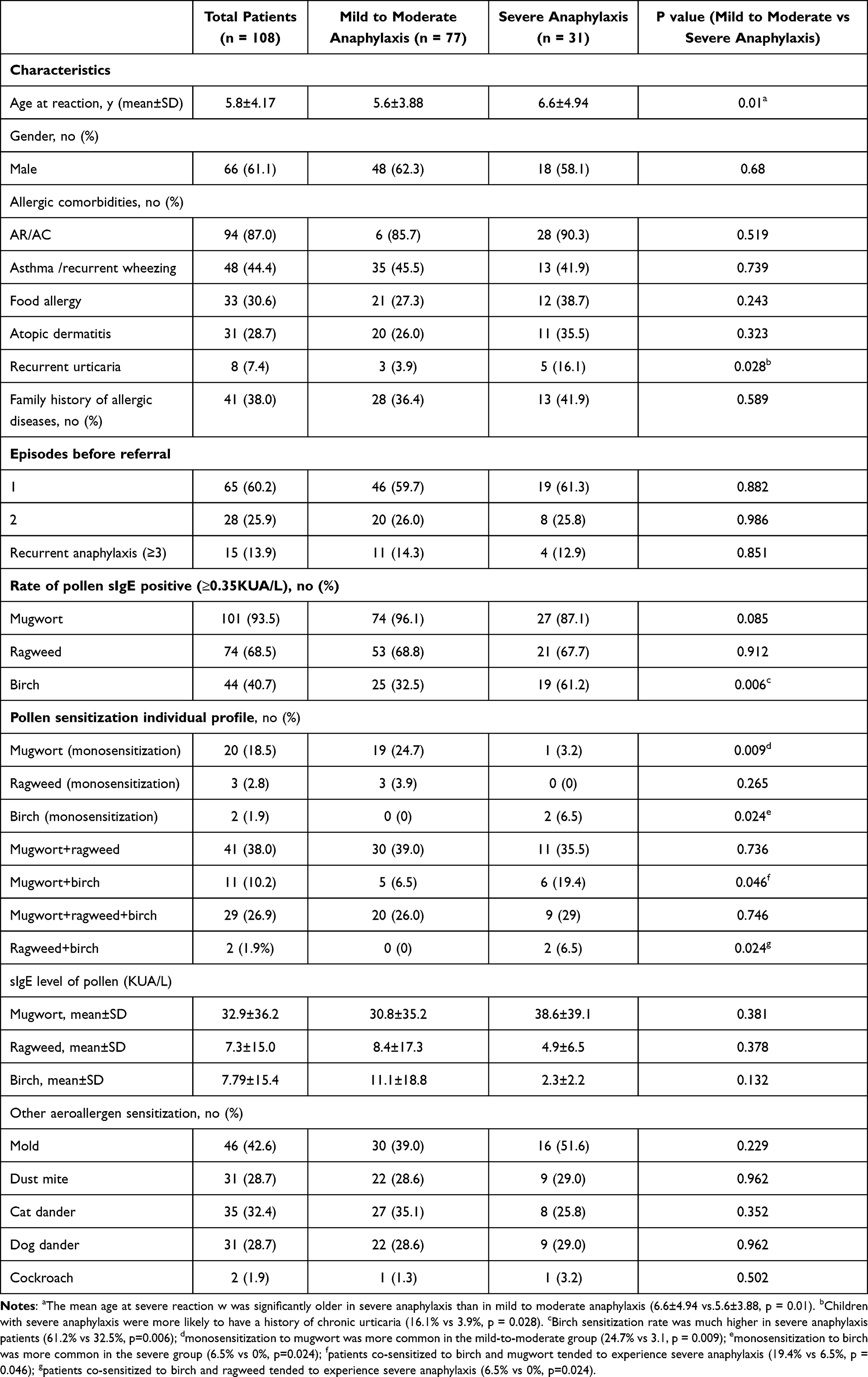 |
Table 1 General Characteristics of 108 Patients |
Triggers of Anaphylaxis
The triggers for 157 anaphylactic events are shown in Table 2 and Figure 2. Foods were the most common causative agents (80.3%, 126/157), followed by food+exercise/exercise (14%, 22/157) and drugs (2.5%, 4/157). The triggers were not determined in 3.2% (5/157) of all reactions, which were classified as idiopathic. Overall, the most frequently implicated foods were fruits/vegetables (22.3%, 35/157), wheat (8.9%, 14/157), and milk (8.3%, 13/157). The most common fruit trigger was peach (n = 7), followed by mango (n = 5) and pitaya (n = 5), and the most common nuts trigger was walnut (n = 4), followed by almond (n = 2) and hazelnut (n = 2). There was no difference in the trigger profile between the mild-to-moderate and severe anaphylaxis group.
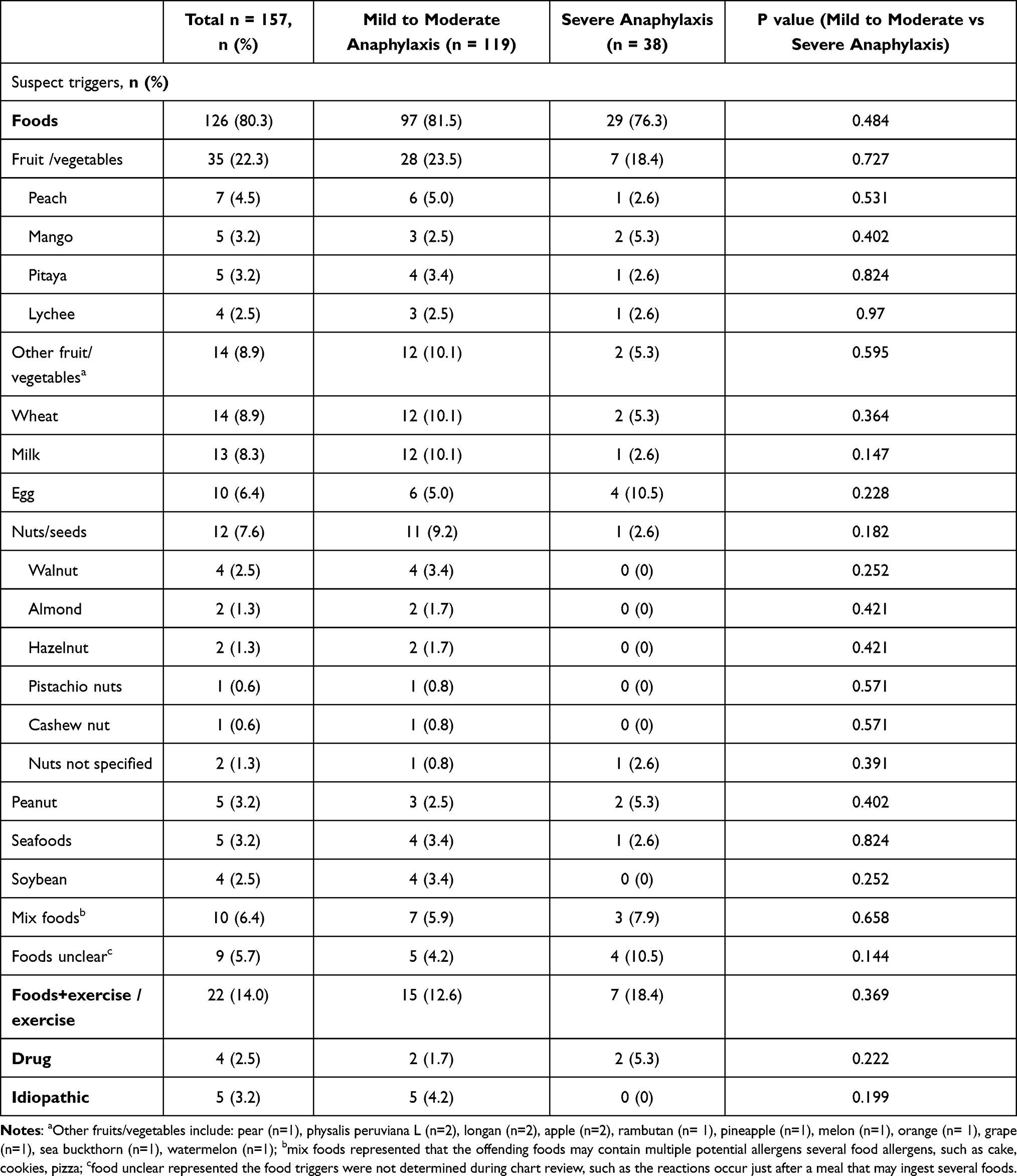 |
Table 2 Triggers of 157 Anaphylactic Reactions |
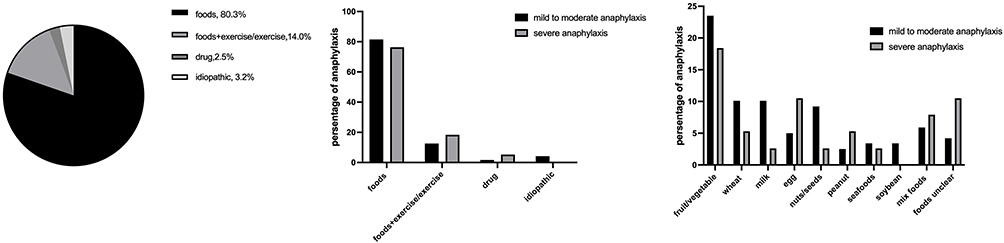 |
Figure 2 Triggers and food triggers of 158 anaphylactic reaction. |
Among the 157 anaphylactic reactions, 14% (22/157) occurred during exercise. Supplement Table 3 shows the detailed clinical characteristics of 16 patients who experienced anaphylaxis during exercise. The mean age at the reaction was 10.1 ± 3.56 years, range (3–17 years); 63.6% (14/22) occurred in pollen season (10 episodes in the autumn, 4 episodes in the spring). A total of 90.9% (20/22) of the episodes occurred during outdoor exercise (running, n = 11; jogging, n = 3; playing basketball, n = 3; quick walking, n = 2; playing golf, n = 1). When analyzing food triggers before exercise, food triggers were not recorded in the chart (n = 11); mix foods (n = 3); wheat (n = 2); banana (n = 2); apple (n = 1), cherry (n = 1); pitaya (n = 1), cauliflower (n = 1); allergic comorbidities in 16 patients, included allergic rhinitis in 75% (12/16), asthma in 37.5% (6/16), food allergy in 18.5% (3/16), and recurrent urticaria in 12.5% (2/16) of the patients.
Symptoms of Anaphylaxis
Supplement Table 2 summarizes the symptoms of anaphylaxis. Skin and mucocutaneous symptoms were the most frequent (86.0%, 135/157), followed by respiratory (73.9%, 116/157), gastrointestinal (21%, 33/157), oropharyngeal (15.9%, 25/157), neurological (6.4%, 10/157), and cardiovascular (8.9%, 14/157) symptoms. Thirty-eight reactions (22.8%,38/157) were classified as severe anaphylaxis.
Acute Management of Anaphylaxis
Table 3 shows the treatment of the 121 anaphylactic episodes. Acute management was not accessible for 36 anaphylactic events. Among the 121 anaphylactic events with detailed management records, 9.9% (12/121) self-resolved and 38.8% (47/121) were home-treated. A total of 59.5% (72/121) of the anaphylactic events were treated in the emergency department; 22.3% (27/121) received with glucocorticoids; and only 7.4% (9/121) were treated with epinephrine.
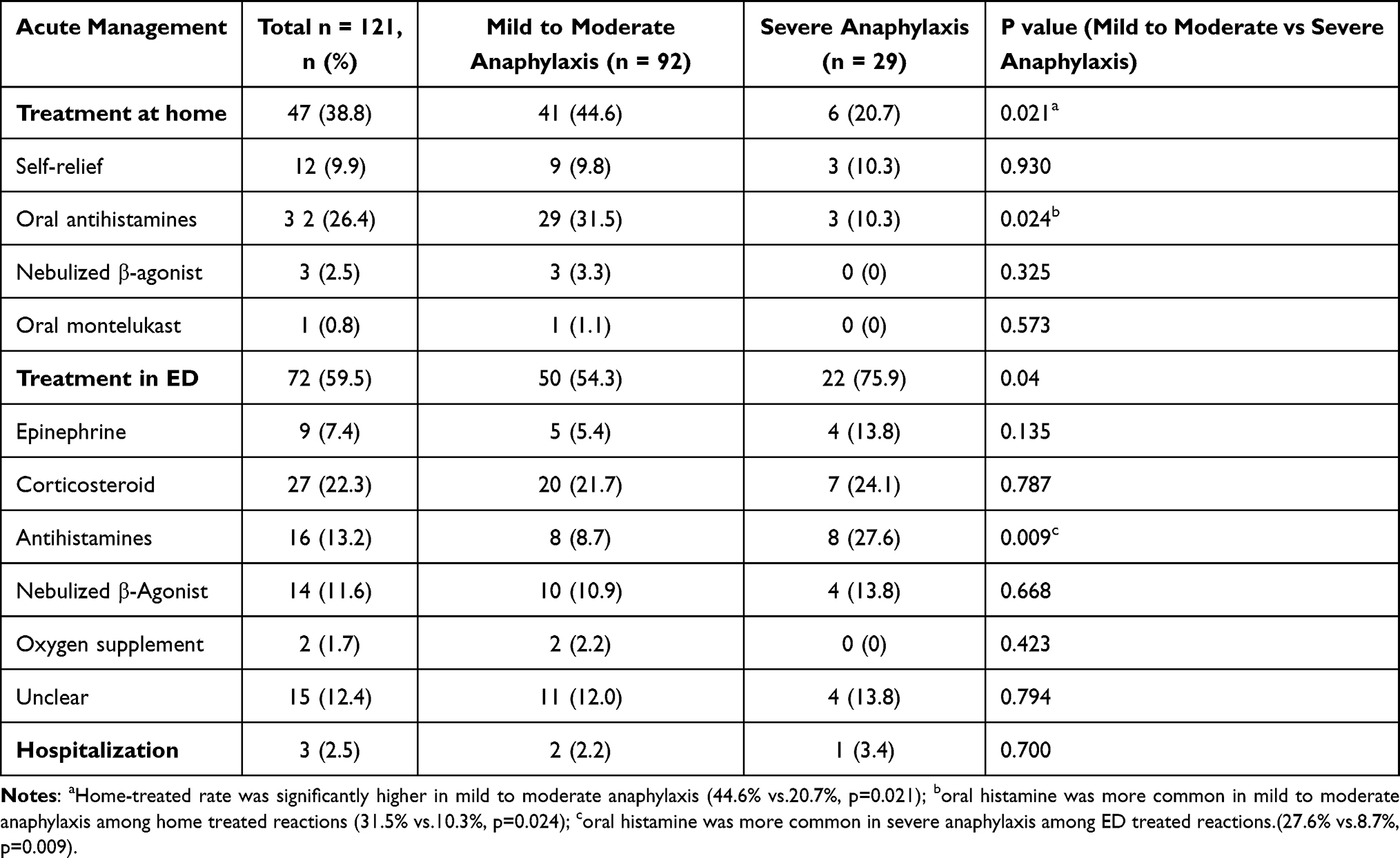 |
Table 3 Acute Management of 121 Anaphylactic Reactions (Unrecorded N = 36) |
Discussion
The findings of this study revealed the characteristics of anaphylaxis in children with pollen sensitization, which demonstrated different profiles from our recently published age-dependent profiles of anaphylaxis in children.2
The present study showed that mugwort was the most common culprit. This may be because almost all children in our cohort were from northern China, and mugwort pollen is the most allergenic pollen in late summer and autumn in northern China.13,19,20 This finding is consistent with our previously published data, where we reported that mugwort sensitization was common in patients with specific food-induced anaphylaxis, especially in fruit/vegetables (67%) and spices (75%).9 Furthermore, compared with oropharyngeal symptoms, systemic reactions are the main manifestation of mugwort pollen-related food allergy in Chinese population.2 Ragweed was the second most common pollen sensitization in our study. Ragweed is one of the major allergen sources causing allergy in North America and Europe.21 However, it has spread and has also become a serious problem in China. One study summarized 215,210 tests with the ImmunoCAP system from 2008 to 2010, and suggested that ragweed sensitization rate in Chinese population was 48%.20 Our study showed that birch pollen sensitization was more common in severe anaphylaxis, we speculate was that the majority of patients (73%) with birch pollen allergy are likely to experience pollen-related food allergy,14 and thus there may be a higher risk of anaphylaxis episodes triggered by a food allergen.
Based on the present study, recurrent urticaria was more common in children with severe anaphylaxis. According to the new grading system, allergic reaction is classified into five grades, from generalized urticaria, to hypotension, collapse, and loss of consciousness (ie, anaphylaxis).22 It has been reported that wheat-induced anaphylaxis could manifest as a mild reaction, such as urticaria and angioedema.23 Thus, recurrent urticaria and anaphylaxis may be two different degrees or phases of food allergy. Severe allergic reactions occur when potentially exacerbating co-factors exist, such as physical activity, use of aspirin and nonsteroidal anti-inflammatory drugs, and alcohol consumption. Certain co-factors are well documented to aggravate or precipitate wheat-induced anaphylaxis (WIA)/wheat-dependent exercise induced anaphylaxis (WDEIA).24 Hence, the clinical progression of recurrent urticaria may be relevant for evaluating the risk of anaphylaxis among patients with pollen sensitization.
Foods were confirmed to be the most frequent trigger for anaphylaxis in the current study, which is consistent with other studies of anaphylaxis in children.2 The most common food triggers were fruits/vegetables, which is in accordance with our previous study that demonstrated that fruits/vegetables were the most common food allergens in preschool-age children (35.9%) and school-age children (31.6%),2 and other published data in China suggested that fruit/vegetables were the most common food triggers in children aged 4–9 years (59%).9 In contrast, relatively lower rates of fruits/vegetables-induced anaphylaxis have been reported in studies from European countries. Alvarez-Perea et al25 reported that 7% of Spanish children attending hospital for reported anaphylaxis had a confirmed allergy to fruits, and data from the European Anaphylaxis Registry also show that fruits are responsible for 5% of all causes of anaphylaxis to foods in children and adolescents.26 Fruits/vegetable-induced anaphylaxis may result from PFAS due to cross-reactivity with a heat stable pollen allergen component.27 In the current cohort, the most common fruit allergen causing anaphylaxis was peach, which is in line with a previous study from China,15 and a nationwide survey conducted in Korea that showed that peach was the top pollen-related food trigger.11 Nevertheless, kiwi is the top fruit trigger in the North America.7 Sensitization patterns of cross-reactive allergens are related to pollen sensitization; thus, geographical distribution of pollen allergens and regional dietary habits influence plant-derived food trigger sensitization profiles and clinical symptoms. Severe or anaphylactic reactions to fruits and vegetables are more likely to occur due to lipid transfer proteins (LTP), originally described only in southern Mediterranean countries but more recently also recognized in Chinese population where it is related to sensitization to peach, tree nuts, peanuts, and also to pollens, such as plane tree and mugwort.8,15,28
Exercise was the most common factor for aggravating or triggering anaphylaxis in our study. This finding is consistent with that from a previous study on anaphylaxis in children and teenagers in Europe.29 In our study, about 64% of exercise-induced anaphylaxis occurred during pollen season, especially in the autumn. In contrast, Gabrielli et al7 revealed that severe anaphylactic reactions to fruits in a Canadian population were more likely to occur during the spring; the authors concluded that the increased risk in the spring may be related to higher pollen counts that would sensitize the immune system and reduce the reaction threshold. Given these data and the recognized cofactors of anaphylaxis, it would be worthwhile to advise patients with pollen allergy who have a known fruit/vegetable allergy to avoid exercise in association with food consumption. Previously described food-dependent exercise-induced anaphylaxis (FDEIA) is a rare subtype of anaphylaxis occurring after exposure to an offending food followed by physical activity, while both the implicated food and exercise, isolated, are tolerated independently.30 Our present study showed that pollen-related fruits are the most common food triggers before exercise, which may be due to the cross-reactive allergen components such as LTP, which are thermostable and less susceptible to enzymatic degradation due to their compact, folded structure.31 As mentioned above, allergic reactions to LTP tend to be more severe.32 Moreover, according to Romano et al.33 LTPs were the most frequent primary allergen (78%) in a group of Italian patients with FDEIA. However, wheat is the most commonly reported allergen; as the best-studied subtype of FDEIA,34 recently published data have demonstrated that wheat anaphylaxis is highly dependent on the presence of co-factors (eg, exercise) and is less frequently associated with atopic diseases compared with other food allergies.35 Unfortunately, although we speculated that the FDEIA cases in our study may be induced by LTPs, we did not conduct a component allergen test.
The risk factors for severe anaphylactic reactions in pollen sensitization individuals have not been reported to date. In our study, sensitization to birch and recurrent urticaria were more common in patients with severe anaphylaxis, indicating that these may be risk factors for severe reactions. A nationwide study in South Korea demonstrated that the sensitization to specific pollen (hazel, timothy and ragweed) and the presence of atopic dermatitis (AD) were the risk factors for anaphylaxis in PFAS.36 Furthermore, the current study indicated that exercise, especially exercise during pollen season, was a co-factor or augmenting factor that triggered anaphylactic reactions dependently or independently of food allergens. Thus, if pollinosis patients have pollen-related food allergies, sIgE positive to birch and the presence of recurrent urticaria may be related to the development of severe anaphylaxis, and other risk factors, such as augmentation factors (pollen sensitization profile, exercise, pollen season, and atopy status), may increase the reaction severity.
In this cohort, there was under-use of epinephrine in the treatment, considering that only 7.4% of the patients received epinephrine in the emergency department. The finding is consistent with previously published studies in China,2,9,37 and the low use of epinephrine demonstrates the need for education promoting the use of epinephrine in all cases of anaphylaxis. However, there is controversy regarding the need to prescribe epinephrine to patients with PFAS because it has been reported that only a minority of PFAS progress to anaphylaxis.11 Although guidelines on epinephrine auto-injector (EAI) prescription remain controversial,28 we suggest that children with a history of anaphylaxis should be prescribed EAI even if the diagnosis is PFAS.
This study had several limitations. The study was performed in a single center in north China; hence, our findings may not apply to the general population of China. A major limitation of the study was the lack of information about skin prick testing or specific IgE measurements to fruit and vegetable allergens to support assumptions about pollen cross-reactivity, and due to the limitation of allergen-specific IgE panel, in our cohort, sIgE level of only three common pollen (mugwort, ragweed and birch) were quantified by Phadia system (immunoCAP) in our cohort. Furthermore, the diagnosis of anaphylaxis was established on the basis of reported information, rather than laboratory testing and challenge tests.
Conclusion
Fruits/vegetables account for a substantial percentage of anaphylaxis cases in children with pollen sensitization. Exercise is the most common factor that aggravates or triggers anaphylaxis.
The suboptimal use of epinephrine highlights the need for educational programs promoting the use of epinephrine. Because severe anaphylaxis to plant-derived food could result from cross-reactivity to pollen, it is important to promote awareness among parents and caregivers regarding this increased risk in children with pollen sensitization.
Abbreviations
FDEIA, food-dependent exercise-induced anaphylaxis; LTP, lipid transfer proteins; EAI, epinephrine auto-injector; PFAS, pollen-food allergy syndrome; IgE, immunoglobulin E.
Data Sharing Statement
The data and materials are available from the corresponding authors based on reasonable requirement.
Ethics Approval and Informed Consent
This study has been performed in accordance with the principles stated in the Declaration of Helsinki, and the study protocol was approved by the Research and Ethics Board of Beijing Children’s Hospital. (Approval number:2022-E-023-R) Because this study was based on the retrospective analysis of medical electronic record, the informed consent was deemed exempt by the Research and Ethics Board.
Consent for Publication
All authors have approved the manuscript and agree with its submission to the Journal of Asthma and Allergy.
Acknowledgments
We appreciated all the patients and investigators who participated in this study.
Funding
This study was supported by Beijing Hospitals Authority Youth Programme, (code: QML20201203), and Respiatory Research Project of National Clinical Research Center for Respiratory Diseases (code. HXZX-20210203, HXZX-20210204, HXZX-202107).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cardona V, Ansotegui IJ, Ebisawa M, et al. World allergy organization anaphylaxis guidance 2020. World Allergy Organ J. 2020;13(10):100472. doi:10.1016/j.waojou.2020.100472
2. Jiang N, Xu W, Xiang L. Age-related differences in characteristics of anaphylaxis in Chinese children from infancy to adolescence. World Allergy Organ J. 2021;14(11):100605. doi:10.1016/j.waojou.2021.100605
3. Lam HCY, Turner PJ, Hemming D, Jarvis DL. Seasonality of food-related anaphylaxis admissions and associations with temperature and pollen levels. J Allergy Clin Immunol Pract. 2021;9(1):518–520.e512. doi:10.1016/j.jaip.2020.07.032
4. Vetander M, Helander D, Flodström C, et al. Anaphylaxis and reactions to foods in children–a population-based case study of emergency department visits. Clin Exp Allergy. 2012;42(4):568–577. doi:10.1111/j.1365-2222.2011.03954.x
5. Sicherer SH, Warren CM, Dant C, Gupta RS, Nadeau KC. Food allergy from infancy through adulthood. J Allergy Clin Immunol. 2020;8(6):1854–1864. doi:10.1016/j.jaip.2020.02.010
6. Hayashi M, Pawankar R, Yamanishi S, Itoh Y. Food-dependent exercise-induced anaphylaxis to soybean: gly m 5 and Gly m 6 as causative allergen components. World Allergy Organ J. 2020;13(7):100439. doi:10.1016/j.waojou.2020.100439
7. Gabrielli S, Clarke AE, Morris J, et al. Fruit-induced anaphylaxis: clinical presentation and management. J Allergy Clin Immunol. 2021;9(7):2825–2830.e2822. doi:10.1016/j.jaip.2021.02.055
8. Deng S, Yin J. Mugwort pollen-related food allergy: lipid transfer protein sensitization and correlation with the severity of allergic reactions in a Chinese Population. Allergy Asthma Immunol Res. 2019;11(1):116–128. doi:10.4168/aair.2019.11.1.116
9. Jiang N, Yin J, Wen L, Li H. Characteristics of Anaphylaxis in 907 Chinese patients referred to a tertiary allergy center: a retrospective study of 1952 episodes. Allergy Asthma Immunol Res. 2016;8(4):353–361. doi:10.4168/aair.2016.8.4.353
10. Egger M, Mutschlechner S, Wopfner N, et al. Pollen-food syndromes associated with weed pollinosis: an update from the molecular point of view. Allergy. 2006;61(4):461–476. doi:10.1111/j.1398-9995.2006.00994.x
11. Kim MA, Kim DK, Yang HJ, et al. Pollen-food allergy syndrome in Korean Pollinosis Patients: a Nationwide Survey. Allergy Asthma Immunol Res. 2018;10(6):648–661. doi:10.4168/aair.2018.10.6.648
12. Hao G-D, Zheng Y-W, Wang Z-X, et al. High correlation of specific IgE sensitization between birch pollen, soy and apple allergens indicates pollen-food allergy syndrome among birch pollen allergic patients in northern China. J Zhejiang Univ. 2016;17(5):399–404. doi:10.1631/jzus.B1500279
13. Wang X-Y, Ma -T-T, Wang X-Y, et al. Prevalence of pollen-induced allergic rhinitis with high pollen exposure in grasslands of northern China. Allergy. 2018;73(6):1232–1243. doi:10.1111/all.13388
14. Biedermann T, Winther L, Till SJ, et al. Birch pollen allergy in Europe. Allergy. 2019;74(7):1237–1248. doi:10.1111/all.13758
15. Li J-D, Du Z-R, Liu J, et al. Characteristics of pollen-related food allergy based on individual pollen allergy profiles in the Chinese population. World Allergy Organ J. 2020;13(5):100120. doi:10.1016/j.waojou.2020.100120
16. Tolkki L, Alanko K, Petman L, et al. Clinical characterization and IgE profiling of birch (Betula verrucosa)–allergic individuals suffering from allergic reactions to raw fruits and vegetables. J Allergy Clin Immunol. 2013;1(6):623–631.e621. doi:10.1016/j.jaip.2013.07.010
17. Choi JH, Jang YS, Oh JW, Kim CH, Hyun IG. Bee pollen-induced anaphylaxis: a case report and literature review. Allergy Asthma Immunol Res. 2015;7(5):513–517. doi:10.4168/aair.2015.7.5.513
18. Muraro A, Roberts G, Clark A, et al. The management of anaphylaxis in childhood: position paper of the European Academy of Allergology and Clinical Immunology. Allergy. 2007;62(8):857–871. doi:10.1111/j.1398-9995.2007.01421.x
19. Tang R, Sun J-L, Yin J, Li Z. Artemisia allergy research in China. Biomed Res Int. 2015;2015:179426. doi:10.1155/2015/179426
20. Wrz H. Analysis of two hundred thousand results of allergen specific IgE test. Chin J Allergy Clin Immunol. 2012;6(1):18–23.
21. D’amato G, Cecchi L, Bonini S, et al. Allergenic pollen and pollen allergy in Europe. Allergy. 2007;62(9):976–990. doi:10.1111/j.1398-9995.2007.01393.x
22. Dribin TE, Schnadower D, Spergel JM, et al. Severity grading system for acute allergic reactions: a multidisciplinary Delphi study. J Allergy Clin Immunol. 2021;148(1):173–181. doi:10.1016/j.jaci.2021.01.003
23. Xu YY, Jiang NN, Wen LP, Li H, Yin J. Wheat allergy in patients with recurrent urticaria. World Allergy Organ J. 2019;12(2):100013. doi:10.1016/j.waojou.2019.100013
24. Scherf KA, Brockow K, Biedermann T, Koehler P, Wieser H. Wheat-dependent exercise-induced anaphylaxis. Clin Exp Allergy. 2016;46(1):10–20. doi:10.1111/cea.12640
25. Alvarez-Perea A, Ameiro B, Morales C, et al. Anaphylaxis in the pediatric emergency department: analysis of 133 cases after an allergy workup. J Allergy Clin Immunol. 2017;5(5):1256–1263. doi:10.1016/j.jaip.2017.02.011
26. Grabenhenrich LB, Dölle S, Moneret-Vautrin A, et al. Anaphylaxis in children and adolescents: the European Anaphylaxis Registry. J Allergy Clin Immunol. 2016;137(4):1128–1137.e1121. doi:10.1016/j.jaci.2015.11.015
27. Carlson G, Coop C. Pollen food allergy syndrome (PFAS): a review of current available literature. Ann Allergy Asthma Immunol. 2019;123(4):359–365. doi:10.1016/j.anai.2019.07.022
28. Katelaris CH. Should patients with pollen fruit syndrome be prescribed an automatic epinephrine injector? Curr Opin Allergy Clin Immunol. 2016;16(4):370–374. doi:10.1097/aci.0000000000000278
29. Hompes S, Köhli A, Nemat K, et al. Provoking allergens and treatment of anaphylaxis in children and adolescents–data from the anaphylaxis registry of German-speaking countries. Pediatr Allergy Immunol. 2011;22(6):568–574. doi:10.1111/j.1399-3038.2011.01154.x
30. Feldweg AM. Food-dependent, exercise-induced anaphylaxis: diagnosis and management in the outpatient setting. J Allergy Clin Immunol. 2017;5(2):283–288. doi:10.1016/j.jaip.2016.11.022
31. Skypala IJ. Can patients with oral allergy syndrome be at risk of anaphylaxis? Curr Opin Allergy Clin Immunol. 2020;20(5):459–464. doi:10.1097/aci.0000000000000679
32. Skypala IJ. When nutrition and allergy collide: the rise of anaphylaxis to plant foods. Curr Opin Allergy Clin Immunol. 2017;17(5):338–343. doi:10.1097/aci.0000000000000387
33. Romano A, Scala E, Rumi G, et al. Lipid transfer proteins: the most frequent sensitizer in Italian subjects with food-dependent exercise-induced anaphylaxis. Clin Exp Allergy. 2012;42(11):1643–1653. doi:10.1111/cea.12011
34. Wong GK, Krishna MT. Food-dependent exercise-induced anaphylaxis: is wheat unique? Curr Allergy Asthma Rep. 2013;13(6):639–644. doi:10.1007/s11882-013-0388-2
35. Kraft M, Dölle-Bierke S, Renaudin J-M, et al. Wheat Anaphylaxis in adults differs from reactions to other types of food. J Allergy Clin Immunol. 2021;9(7):2844–2852.e2845. doi:10.1016/j.jaip.2021.03.037
36. Kim M, Ahn Y, Yoo Y, et al. Clinical manifestations and risk factors of anaphylaxis in pollen-food allergy syndrome. Yonsei Med J. 2019;60(10):960–968. doi:10.3349/ymj.2019.60.10.960
37. Jiang C, Li H, Wang L, Liu C, Hao X. Gaps between actual initial treatment of anaphylaxis in China and international guidelines: a review and analysis of 819 reported cases. Allergy. 2020;75(4):968–971. doi:10.1111/all.14090
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Anaphylaxis in Chinese Children: Different Clinical Profile Between Children with and without a History of Asthma/Recurrent Wheezing
Jiang N, Xu W, Huang H, Hou X, Xiang L
Journal of Asthma and Allergy 2022, 15:1093-1104
Published Date: 18 August 2022
A Patient Education Intervention to Address Allergic Anaphylaxis-Related Quality-of-Life and Self-Efficacy
Belin C, Tomori C
Journal of Asthma and Allergy 2026, 19:573932
Published Date: 13 February 2026