")
Back to Journals » International Journal of General Medicine » Volume 16
Analysis on the Selection of Herbs in TCM COVID-19 Treatment Protocols Between Malaysia and China
Authors Wang X , Wang J, Pang F
Received 15 June 2023
Accepted for publication 16 August 2023
Published 21 August 2023 Volume 2023:16 Pages 3655—3663
DOI https://doi.org/10.2147/IJGM.S426168
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xing Wang,1,* Jing Wang,2,* Fang Pang3
1M. Kandiah Faculty of Medicine and Health Sciences, Universiti Tunku Abdul Rahman, Kajang, Selangor, Malaysia; 2Department of Ophthalmology, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 3College of Traditional Chinese Medicine, Chongqing Medicine University, Chongqing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fang Pang, College of Traditional Chinese Medicine, Chongqing Medical University, 1 Medical College Road, Chongqing, 400016, People’s Republic of China, Email [email protected]
Objective: Both Malaysian and Chinese populations have benefited from the utilization of Traditional Chinese Medicine (TCM) in the treatment of COVID-19. This study aims to analyze the herb selection in TCM COVID-19 treatment protocols employed by Malaysia and China.
Methods: Based on TCM theories, a comparative analysis was conducted on the treatment protocols of the two countries. This analysis encompassed syndrome differentiation and classification, therapeutic principles and formulas, as well as herb characteristics. The herbs within the protocols were subjected to frequency statistics and cluster analysis using SPSS 25, and network analysis was performed using SPSS Modeler 18.0 software.
Results: The properties (cold, warm, ping and bitter, pungent, sweet) and meridian (lung, stomach, spleen) associated with the herbs in both protocols exhibit fundamental similarities. Furthermore, the propensity for selecting pairs of herbs is also consistent. The herb pairs selected also have the same propensity. The clustering results reveal six categories, of which in the two protocols are good. The top three herb-pairs in Malaysian Protocols are Gan Cao - Yi Yi Ren, Ban Xia - Gan Cao, Chen Pi - Gan Cao, while the top three in Chinese Protocol are Huo Xiang - Ma Huang, Shi Gao - Gan Cao, Cang Zhu - Gan Cao.
Conclusion: Characteristics of herbs in Both Malaysian and Chinese Protocols herb reflect the advantages and regional adaptation of TCM principles. These findings offer valuable guidance in the application of herbs or herb pairs for the treatment of COVID-19.
Keywords: COVID-19, TCM protocol, herbs and formulas, Malaysia, China
Coronavirus disease-2019 (COVID-19) is a rapidly spreading acute respiratory infectious disease worldwide. As of 24 July 2023, there have been 768,654,968 global confirmed cases of COVID-19, including 6,953,483 fatality cases reported to WHO.1 The pathogenesis of COVID-19 involves three main inflammatory processes: local manifestations of classical general inflammation, acute systemic inflammation, and chronic low-intensity systemic inflammation.2,3 OVID-19 originated from the SARS-CoV-2 outbreak. The infection’s pathological process in humans ranges from mild symptoms to severe organ failure.4 SARS-CoV-2 replicates within epithelial cells, migrating from the airways to alveolar cells in the lungs, triggering a robust immune response. Recent advances in medicine, biology, and medicine have enabled a better understanding of COVID-19-causing virus’ structure, function, life cycle, and pathophysiology. Few specific antiviral drugs are available for treating SARS-CoV-2 infection, and therapeutic trials are exploring molecular mechanisms and genomic organization.5 Convalescent plasma therapy has been significant in managing COVID-19 patients.6,7 COVID-19 mRNA vaccines are gaining attention due to their potential for broad application, rapid development cycles, ease of industrialization, simple production processes, adaptability to new variants, and capacity to induce stronger immune responses.8–10 Additionally, microRNAs play a crucial role in antiviral immunity against COVID-19.11 However, effective clinical treatment for the entire course of COVID-19 remains limited.
Since the occurrence of COVID-19, Traditional Chinese Medicine (TCM) has made a significant contribution to preventing and managing the epidemic. Malaysia, a country where TCM is widely applicated, has adopted TCM treatment as complementary medicine in prevention and treatment of COVID-19. In September 2021, the Malaysian Chinese Medicine Society of Epidemic Control and Prevention (CMEC) published the “Chinese Medicine Practice Guidelines for Malaysia (3rd Trial Version)” (Abbreviated as “Malaysian Protocol”)12. Similarly, in China, the COVID-19 treatment protocol was updated to the 9th version on March 15, 2022. Both countries benefit from TCM for the COVID-19 treatment. This study aims to compare syndrome differentiation and classification, therapeutic principles and formulas, the characteristics of herbs in Malaysian TCM COVID-19 treatment Protocol with the TCM treatment protocol in the “Protocol for the Treatment of COVID-19 (the 9th Trial Version) published by the National Health Commission of China and National Administration of Traditional Chinese Medicine of China (Abbreviated as “Chinese Protocol”),13 in order to enhance our understanding of the application of Chinese herbal medicine in disease treatment.
Syndrome Differentiation and Classification
In terms of TCM treatment for confirmed patients, both Protocols categorize patients into five periods based on disease severity: mild, normal, severe, critical and recovery. Based on this, the Malaysian Protocol has subdivided the treatment into five clinical grades according to the “Guidelines for the Clinical Management of Adult and Paediatric Patients with Coronavirus disease-2019” issued by the Ministry of Health (Malaysia).12 For example, mild patients are divided into clinical grade 1 and grade 2, which were classified as non-clinical symptom type, dampness-turbidity bias pattern, dampness constraint of lung pattern, damp-heat constraint of lung pattern, heat-toxin attacking the lung pattern. The moderate type was classified as damp-heat accumulation in the lung pattern. The severe type was classified as epidemic toxin blocking the lung pattern. The critical type was classified as lung blocking and asthma pattern. The patients in the convalescence period were classified as spleen-stomach qi deficiency with phlegm-dampness accumulation of lung pattern and lung-spleen qi deficiency pattern. In contrast, Chinese Protocol designates mild patients with cold-damp constraint in the lung pattern and damp-heat accumulation in the lung pattern. Moderate patients were classified as damp-toxin constraint in the lung pattern, cold-damp obstructing the lung pattern, and epidemic toxin with dryness pattern. Severe patients were identified as epidemic toxin blocking the lung pattern and blazing of both qi and yin. Critical patients were identified as internal blockage and external desertion pattern. Patients in the convalescence period were identified as lung-spleen qi deficiency pattern and deficiency of both qi and yin pattern.
Therapeutic Principles and Formulas
Based on the classification and clinical manifestations of COVID-19 as outlined in the Malaysian Protocol, the specific therapeutic principles and formulas are as follows (Table 1).
 |
Table 1 Formulas Recommended in Malaysian Protocol |
In China, given the extensive utilization of TCM and substantial pre-clinical and clinical research, various clinical stages of COVID-19 are dominated by proprietary Chinese medicines or self-prescribed formulas (Table 2). Additionally, the latest Chinese Protocol includes recommended acupuncture and moxibustion treatments for each period.
 |
Table 2 Formulas Recommended in Chinese Protocol |
Analysis of Herbs
Analysis of Frequency, Properties and Meridian of Herbs
Analysis of Frequency
In the Malaysian Protocol, a total of ten formulas were compiled, incorporating 81 kinds of herbs. The top 4 herbs in terms of frequency are Yi Yi Ren (8), Gan Cao (8), Fu Ling (6), Bai Zhu (6), Ban Xia (6), Chen Pi (6), Jie Geng (6), Xing Ren (5), Bai Kou Ren (5), Bo He (4), Zi Su (4), Lu Gen (4), Ren Shen (4). In the Chinese Protocol, ten formulas were collated, utilizing 63 different herbs. The top 4 herbs in terms of frequency of use are Gan Cao (7), Shi Gao (6), Huo Xiang (6), Ma Huang (5), Cang Zhu (5), Xing Ren (4), Fu Ling (4), Ting Li Zi (4), Hou Pu (4), Cao Guo (4) (Table 3).
 |
Table 3 Frequency of Herbs of Formulas in Different Protocols |
Distribution of the Four Qi in TCM
Within the herbs of the Malaysian Protocol formula, the Four Qi frequencies were categorized as Cold (33), Warm (32), Ping (9), Cool (5) and Hot (2). Conversely, the herbs of the Chinese Protocol formula were categorized in terms of Four Qi frequencies as Cold (27), Warm (25), Ping (7), Cool (3) and Hot (1) (Table 4).
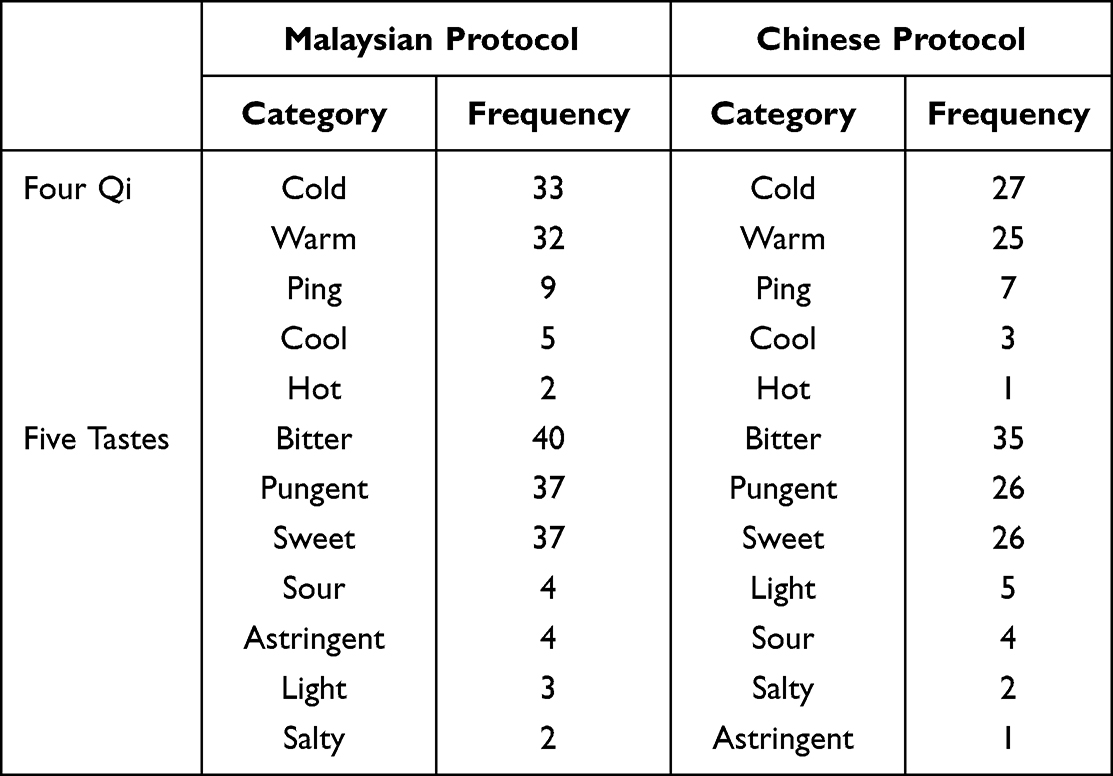 |
Table 4 Distribution of the Four Qi and Five Tastes of Herbs in Different Protocols |
Distribution of the Five Tastes in Chinese Medicine
The frequency rankings of the Five Tastes in the herbs of Malaysian Protocol formula are bitter (40), pungent (37), sweet (37), sour (4), astringent (4), light (3) and salty (2). The frequency rankings of the Five Tastes in the herbs of Chinese Protocol formula are bitter (35), pungent (26), sweet (26), light (5), sour (4), salty (2) and astringent (1) (Table 4).
Distribution of Meridians in Chinese Medicine
The meridian of herbs in the Malaysian Protocol formula involves 12 meridians, ranked in order of lung (54), stomach (43), spleen (36), heart (21), liver (18), kidney (14), large intestine (10), gall bladder (5), small intestine (5), bladder (2), triple jiao (1) and pericardium (1). The meridian of herbs in Chinese Protocol formula involves 11 meridians, ranked in order of lung (35), spleen (28), stomach (27), liver (18), kidney (18), heart (17), bladder (7), large intestine (6), Gallbladder (4), small intestine (3) and pericardium (1) (Table 5).
 |
Table 5 Distribution of Meridian of Herbs in Different Protocols |
Cluster Analysis
SPSS 25 was used to conduct cluster analysis on herbs in the both Protocols. The clustering results of 81 herbs in Malaysian Protocol and 63 herbs in the Chinese Protocol are shown (Figure 1). When the clustering results are 6 categories, the clustering results in the two protocols are good.
 |
Figure 1 Protocol herbs cluster analysis (Left: Malaysia. Right: China). |
Network Analysis of Compatibility of TCM
The analysis of association rules for the recommended herbs in both Protocols was conducted using SPSS Modeler 18.0 with the Apriori algorithm. The support level was set at 50%, and the confidence level at 80%. Duplicate items were removed, and the top ten rules were selected based on the percentage support for each Protocol. In the Malaysian Protocol, the top three are Gan Cao - Yi Yi Ren, Ban Xia - Gan Cao, Chen Pi - Gan Cao. The top three in the Chinese Protocol are Huo Xiang - Ma Huang, Shi Gao - Gan Cao, Cang Zhu - Gan Cao (Table 6), the network analysis of TCM herbs in the both Protocols was also carried out (Figure 2).
 |
Table 6 Association Rules of Herbs in Different Protocols |
 |
Figure 2 Protocol herbs network analysis (Left: Malaysia. Right: China). |
Discussion
COVID-19 is linked to TCM disease of pestilence, acknowledged in both the Chinese Protocol and Malaysian Protocol. In overview of the TCM protocols developed by medical experts in Malaysia and China for COVID-19 prevention and treatment, disparities in understanding of the various periods of the disease between the Protocols. These differences are reflected in the recommended formulas in each Protocol.
Considering the hot and rainy nature of the local tropical climate, the Malaysian Protocol offers precise insight by pinpointing “dampness, heat, and epidemic air entering through the nose and mouth” as direct causes of the disease. Conversely, the Chinese Protocol provides a generalized identification that the disease is caused by the epidemic toxin, and states that each region should apply methods of syndrome differentiation and treatment based on the patient’s constitution of TCM, disease syndromes, and regional climate.
Different Understandings of Disease Under the Principle of TCM Place-Based interventions
Due to China’s extensive geographic expanse, the Chinese Protocol recommends regional syndrome differentiation treatment. The Malaysian Protocol, however, outlines clear TCM syndromes and formulas throughout the disease progression. With a hot and rainy climate and the principle of TCM place-based interventions,14 the Malaysian Protocol determines “dampness” throughout various phases of disease, which can easily transform into heat and dryness, reflecting the characteristics of “dampness, toxin, blocking and deficiency”. In China, given the broad range of climatic variations, the protocol outlines a general framework of “dampness, toxin and epidemics” within TCM, with “dampness” as the main cause of the disease, susceptible to cold, heat and dryness, as well as blood stasis.15 The symptoms are characterized by “dampness, heat, toxin, stagnation, blocking and deficiency”.16
Prescriptions with Different Characteristics
Considering the distinct syndrome differentiation characteristics between the Protocols, the employed herbs reflect each Protocols’ individual characteristics. In the Malaysian Protocol, the combination of San Ren Tang is applied to treat Grade 1–2 disease. Network pharmacological analysis shows that San Ren Tang can exert antiviral effects through multiple target proteins, affecting cytokine signaling, interleukin signaling pathway and the mitogen-activated protein kinase signaling pathway in the immune system,17 and combining of heat-clearing, detoxifying and cough-relieving formulas to achieve the goal of treating disease. In the Chinese Protocol, the herbs for cold and dampness was added to the formulas, tailored to syndrome attributes. The Self-prescribed Hanshiyi Fang,18 uses warm herbs such as Ma Huang, Qiang Huo, Cang Zhu, Sheng Jiang and Cao Guo to dispel cold. For moderate and severe patients, both Protocols employed the same method of clearing heat and detoxifying, expelling dampness and opening up the door. The Chinese Protocol added the syndrome of cold-damp obstructing the lung pattern and epidemic toxin with dryness pattern due to the causes of cold, dampness, epidemic toxin, giving a self-prescribed formula named Xuanfei Baidu Decoction. Network pharmacology studies of this formula suggest19 that its key targets mainly involve anti-inflammatory and anti-apoptotic aspects. For severe and critical patients, the Malaysian Protocol recommends the use of the classical formulas, while the Chinese Protocol provides mostly the relatively well-researched proprietary TCM injection for treatment. In the convalescence period, the Malaysian Period provides classical formulas for strengthening the spleen and tonifying the lung, and similarly, the Chinese Protocol also emphasizes strengthening the spleen, benefiting the lung, and nurturing yin, but still suggests a self-prescribed formula.
Differences Within Similarities of Herbs and Formulas Selection
The frequency, property and meridian characteristics of TCM herbs under both Protocols showed differences within overall similarities. All recommended formulas in both Protocols were based on heat-clearing and detoxifying herbs. Considering climate traits, the Malaysian Protocol make more use of expelling dampness herbs such as Yi Yi Ren, Fu Ling and Bai Zhu. A network analysis of the selected formulas showed that the trends in the pairs of herbs was consistent with the unit herb. The top Four Qi and Five Tastes properties of the herbs used in both Protocols are cold, warm, ping and bitter, pungent and sweet. Commonly chosen herbs, belonging to the lung, spleen, stomach, liver meridians of TCM in the formulation of both Protocols. The view that the disease is first located in the lung, spleen, and then involve multiple viscera is fully reflected in the medication characteristics of both Protocols.20 These similarities also highlight the convergent understanding TCM practitioners from both countries possess concerning COVID-19 within TCM principles. The “dampness, heat, toxin” characteristics of the disease has been widely recognized in both countries.
TCM has achieved reliable results in COVID-19 prevention and treatment in both countries. The Malaysian Protocol and Chinese Protocol share the same understanding of the core pathogenesis, TCM syndrome, therapeutic principles and formulas. The most crucial difference between the Protocols is whether or not the dampness would transform into cold. In northern China, driven by geographical and climatic attributes, cold and dampness are the cause of the disease, and dampness tends to transform into cold; whereas in southern areas, such as Guangdong Province with similar climatic characteristics to Malaysia, the cause of the disease is also similar, starting with damp-heat trapping the surface and then dampness turning into heat and dryness.21 Furthermore, given the limited availability of TCM treatment for COVID-19 patients in Malaysia, with many receiving remote interventions, the Malaysian Protocol has opted to use classical formulas that can be easily disseminated and applied as a result. Meanwhile, in China, where a substantial proportion of diagnosed COVID-19 cases undergo face-to-face TCM interventions and information collection, the Chinese Protocol uses more self-prescribed formulas, capitalizing on adaptable nature of TCM in tailoring personalized treatments for the same disease. Although it is inevitable that this study may be adversely affected due to scope of recommended formulas under both Protocols, certain differences can be observed between the Protocols.
Conclusion
Rooted in fundamental Chinese medicine theories, both protocols adhere to the same principle-methodology-formula-medication framework. Nonetheless, a critical contrast emerges between the two protocols based on the geographical variance between the two countries—whether dampness transforms into cold. Notably, TCM has achieved remarkable results in COVID-19 prevention and treatment within both nations. TCM practitioners from each country can use findings of this study in epidemic prevention and treatment, thereby fostering the advancement of a shared human destiny community.
Acknowledgment
Xing Wang and Jing Wang have contributed equally to this work and should be considered as co-first author.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO Coronavirus (COVID-19) Data; 2023. Available from: https://covid19.who.int.
2. Gusev E, Sarapultsev A, Hu D, et al. Problems of Pathogenesis and Pathogenetic Therapy of COVID-19 from the Perspective of the General Theory of Pathological Systems (General Pathological Processes). Int J Mol Sci. 2021;22(14):7582. doi:10.3390/ijms22147582
3. Gusev E, Sarapultsev A, Solomatina L, et al. SARS-CoV-2-Specific Immune Response and the Pathogenesis of COVID-19. Int J Mol Sci. 2022;23(3):1716. doi:10.3390/ijms23031716
4. Hu B, Guo H, Zhou P, et al. Characteristics of SARS-CoV-2 and COVID-19. Nat Rev Microbiol. 2021;19(3):141–154. doi:10.1038/s41579-020-00459-7
5. Chilamakuri R, Agarwal S. COVID-19: characteristics and Therapeutics. Cells. 2021;10(2):206. doi:10.3390/cells10020206
6. Dhawan M, Priyanka, Parmar M, et al. Convalescent plasma therapy against the emerging SARS-CoV-2 variants: delineation of the potentialities and risks. Int J Surgery. 2022:97. doi:10.1016/j.ijsu.2021.106204
7. Zhang X, Xi L, Pang F, et al. Convalescent plasma in the treatment of severe covid-19: a systematic review and meta-analysis. Iran J Public Health. 2020. doi:10.18502/ijph.v49i11.4716
8. Priyanka, Chopra H, Choudhary OP. mRNA vaccines as an armor to combat the infectious diseases. Travel Med Infect Dis. 2023;52. doi:10.1016/j.tmaid.2023.102550
9. Fang E, Liu X, Li M, et al. Advances in COVID-19 mRNA vaccine development. Signal Transduct Target Ther. 2022;7(1):56.
10. Choudhary OP, Priyanka, Ahmed JQ, et al. Heterologous prime-boost vaccination against COVID-19: is it safe and reliable? Human Vaccines Immunotherapeutics. 2021;17(12):5135–5138. doi:10.1080/21645515.2021.2007015
11. Ahmed JQ, Maulud SQ, Dhawan M, et al. MicroRNAs in the development of potential therapeutic targets against COVID-19: a narrative review. J Infect Public Health. 2022;15(7):788–799. doi:10.1016/j.jiph.2022.06.012
12. ZHeng JQ, Chen BM, Zhang JX. Chinese Medicine Practice Guidelines for COVID-19 in Malaysia (3rd Trial Version). J Beijing Unv Traditional Chine Med. 2021;44(09):784–788.
13. National Health Commission of the People’s Republic of China. Protocol for the Treatment of COVID-19 (the 9th Trial Version); 2022. Available from: http://www.nhc.gov.cn/yzygj/s7653p/202203/b74ade1ba4494583805a3d2e40093d88tp:shtml.
14. Liang YH. The Study of Relationship Between Characteristic of Climate Changes in Malaysia with Syndrome Type of Disease Caused by Six Evil in Externally Contracted Heat Disease. Guangzhou University of Chinese Medicine; 2013.
15. Li JS, Feng ZZ, Chun L, et al. Diagnosis Standard of Traditional Chinese Medicine Syndromes for Coronavirus Disease 2019 (Trial). J Traditional Chine Med. 2021;62(01):86–90. doi:10.13288/j.11-2166/r.2021.01.020
16. Li JS, Feng ZZ, Chun L, et al. Research Progress of Etiology and Syndrome Differentiation of Traditional Chinese Medicine of Corona Virus Disease 2019. Liaoning J Traditional Chine Med. 2022;49(02):213–216. doi:10.13192/j.issn.1000-1719.2022.02.056
17. Li JL, Yang JL, Zhou HL, et al. Mechanism of sovereign medicines in Sanren Decoction on COVID-19 based on network pharmacology and molecular docking. Chine Traditional Herbal Drugs. 2020;51(09):2345–2353.
18. Yang YY, Li QW, Bao TT, et al. Syndrome Differentiation and Treatment of COVID-19 by Academician Tong Xiaolin: origin, Innovation, and Development of “Cold-Dampness Plague” Theory. World Chine Med. 2021;17:1–6.
19. Zhang P, Wang C, Zou JB, et al. Investigation on Mechanism and Active Components of Hanshizufei Formula Treating COVID-19 Based on Network Pharmacology and Molecular Docking. Pharmacol Clin Chine Materia Medica. 2020;36(05):38–44. doi:10.13412/j.cnki.zyyl.20200727.001
20. Zong Y, Zhao KH. Analysis of Corona Virus Disease 2019 in the field of epidemic disease of TCM. Pharm Clin Chine Materia Medica. 2021;12(01):30–32+37.
21. Traditional Chinese Medicine Bureau of Guangdong Province. Protocol for the Treatment of COVID-19 of Guangdong Province; 2022. Available from: http://szyyj.gd.gov.cn/zwgk/gsgg/content/post_2902010.html.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.