")
Back to Journals » International Journal of General Medicine » Volume 16
Analysis of the Risk Factors for Negative Emotions in Patients with Esophageal Cancer During the Peri-Radiotherapy Period and Their Effects on Malnutrition
Authors Luo F, Lu Y, Chen C, Chang D, Jiang W, Yin R
Received 11 October 2023
Accepted for publication 12 December 2023
Published 27 December 2023 Volume 2023:16 Pages 6137—6150
DOI https://doi.org/10.2147/IJGM.S444255
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Feng Luo, Yingying Lu, Chen Chen, Dongdong Chang, Wei Jiang, Ronghua Yin
Department of Oncology Zone II, Hai’an People’s Hospital, Haian, People’s Republic of China
Correspondence: Ronghua Yin, Department of Oncology Zone II, Hai’an People’s Hospital, No. 17, Zhongba Middle Road, Haian, 226600, People’s Republic of China, Email [email protected]
Background: Esophageal cancer has a high incidence in China. Many patients also have a heavy psychological burden due to clinical features such as wasting and choking on food. This study analyzed the risk factors of negative emotions in esophageal cancer patients during the peri-radiotherapy period and its effects on malnutrition.
Methods: We retrospectively analyzed 339 patients with esophageal cancer during the peri-radiotherapy who received treatment at our hospital from April 2017 to April 2020, and followed up for 3 years. t test and Chi-square test were used to analyze the relationship between patients’ negative emotions and clinical data. Binary logistics regression was performed to analyze the independent risk factors for the occurrence of negative mood and malnutrition in the patients. Kaplan-Meier survival curves were used to analyze survival rates.
Results: Our results showed that 18.3% of patients undergoing radiotherapy for esophageal cancer had negative emotions, and 41.9% suffered from malnutrition. The results of the binary logistic regression analysis showed that monthly household income (OR = 0.470, P = 0.022), the TNM stage (OR = 2.030, P = 0.044), concomitant gastrointestinal symptoms (OR = 2.071, P = 0.024), sleep status (OR = 2.540, P = 0.003), swallowing disorders (OR = 1.919, P = 0.048), and post-radiotherapy complications were independent risk factors for the development of negative emotions in patients. Negative emotions (OR = 2.547, P = 0.038) were also a risk factor for malnutrition in patients with esophageal cancer.
Conclusion: Many patients with esophageal cancer suffer from anxiety and depression in the peri-radiotherapy period, which might lead to complications such as malnutrition or aggravate and affect the prognosis of patients. Therefore, psychological care should be provided based on conventional care to effectively relieve their psychological pressure, and improve their prognosis and quality of life.
Keywords: esophageal cancer, malnutrition, negative emotions, influencing factors
Introduction
Esophageal cancer (EC) is a common malignant tumor of the gastrointestinal tract, with a high incidence rate and a low survival rate. It is the sixth most common cause of death due to malignant tumors worldwide and the fourth most common cause of death due to malignant tumors in China. The annual incidence of new cases is about 50% of the global incidence, and the incidence rate increases every year.1,2 Because of its physiological function and anatomical location, the incidence of malnutrition in patients with esophageal cancer is higher than that in patients with other tumors. More than 60% of patients with esophageal cancer suffer from malnutrition to different degrees, and 22% of patients die because of malnutrition.3 The mechanism of malnutrition is complex and might be related to the special physiological function, anatomical structure, tumor-related factors such as dysphagia and obstruction, and treatment-related factors, such as gastroesophageal reflux caused by surgery and vomiting caused by the administration of chemotherapeutic drugs.4,5 Radiotherapy is an effective method of treating EC and considerably prolongs the survival of patients.6,7 However, radiotherapy has toxic side effects in patients and might also lead to malnutrition.8 Long-term malnutrition reduces the quality of life of patients and their tolerance to radiotherapy and decreases treatment sensitivity, resulting in prolonged hospitalization or shortened survival time, or in severe cases, treatment failure due to lack of tolerance.9,10
Some studies have shown that cancer patients always have negative emotions, and almost 50% of cancer patients suffer from anxiety and depression.11,12 Patients with esophageal cancer experience significant weight loss, and they have difficulty in eating, poor absorption, and concurrent malnutrition. Therefore, esophageal cancer can greatly affect the psychology of patients, which can worsen their negative emotions and psychological stress, thus affecting their treatment effect and reducing their quality of life. The long-term repeated treatment process also brings a heavy burden, economic pressure, and psychological stress to patients and their families.13,14 The high morbidity, mortality, and rate of complications make this disease particularly high risk for emotional distress and psychiatric illness.15 One study found that about 24% of patients with esophageal cancer have depression, which can be complicated by social cognitive impairment in severe cases.16 Thus, the negative emotions of patients with esophageal cancer need to be addressed to improve their prognosis and quality of life. Malnutrition, a common complication in patients with esophageal cancer, is also of concern to clinical staff. However, studies on the effect of negative emotions on malnutrition in patients with esophageal cancer are limited, and the independent risk factors for the development of anxiety and depression need to be identified. We conducted this study following the guidelines of the STROBE checklist.
Materials and Methods
Research Participants
In total, 339 patients with peri-radiotherapy esophageal cancer who were treated at Hai’an People’s Hospital from April 2017 to April 2020 were included in this study.
The inclusion criteria were as follows: (I) esophageal cancer diagnosed by cytology or pathology; (II) inpatients with primary esophageal cancer; (III) Karnofsky (kPS) score >70; (IV) physical examination and ancillary diagnostic tests were performed according to medical orders; (V) complete medical records were available; (Ⅵ) patients provided signed informed consent.
The exclusion criteria were as follows: (I) combination of mania and other psychiatric diseases; (II) combination of other malignant tumors; (III) combination of acute and chronic infectious diseases: (IV) lactating or pregnant women; (V) presence of serious organ diseases; (Ⅵ) serious mental disorders, loss of the ability to communicate; (Ⅶ) missing medical records (see Figure 1).
 |
Figure 1 A flowchart describing the details of patient selection. |
We conducted a cross-sectional study to investigate the relationship between negative emotions and malnutrition in patients with peri-radiotherapy esophageal cancer. According to our previous study and published studies of other researchers, the incidence rate of negative emotions in peri-radiotherapy esophageal cancer patients was found to be approximately 20%. In this study, a tolerance error of 3% and a confidence level of 1-α = 0.95 were specified, and the sample size of 264 cases to be investigated was calculated using the PASS 15 software. Assuming a non-response rate of 10% among patients, the required sample size was found to be 294 cases (N = 264 ÷ 0.9). Assuming a questionnaire pass rate of 90%, the total sample size required was 327 cases (N = 294 ÷ 0.9). Additionally, the general rule of logistic regression requires a ratio of items to a sample size of 1:5 to 1:10. Therefore, the planned sample size for this study was 350 cases. There were 11 cases of attrition and lost access partial cases, and thus, the final count was 339 cases.
The study was conducted following the Declaration of Helsinki (as revised in 2013). The study was approved by the Ethics Committee of Hai’an People’s Hospital (No. 202230), and informed consent was provided by all participants.
General Information Questionnaire
The general information questionnaire included demographic data (eg, age, gender, body mass index (BMI), monthly household income, education level, marital status, history of smoking, and history of alcohol consumption) and clinical data (presence of underlying diseases, whether or not surgery was performed, tumor size, tumor stage, primary site of tumor, pathological type, concomitant gastrointestinal symptoms, radiation dose, whether or not chemotherapy was administered, sleep status, and presence of swallowing disorder).
Assessment of Negative Emotions
We used the anxiety self-assessment scale (SAS) and the depression self-assessment scale (SDS) to evaluate the negative mood of the beneficiaries at different time points before and after the intervention. The SAS consists of 20 items, four points for each item, with 50 points as the cut-off value. A score of ≤50 points indicates no anxiety, whereas a score of >50 points indicates anxiety; the higher the score, the more severe the level of anxiety. The SDS consists of 20 items, and the cut-off value is 53 points. A score of ≤53 points indicates no depression, whereas a score of >53 points indicates depression; the higher the score, the more severe the level of depression.
We assessed patients one week after radiotherapy. Based on the SAS and SDS scores, patients were considered to be in the negative mood group if they presented with either or both anxiety and/or depression.
Patient-Generated Subjective Global Assessment
The PG-SGA (patient-generated subjective global assessment) score,17 including weight loss (score: 0–5), disease status (score: 0–6), stress status (score: 0–3), and physical examination (score: 0–9), was used to analyze the nutritional deficiencies of patients according to the PG-SGA. The sum of all four scores was the total score, and the PG-SGA score was 0–1 for normal nutrition, 2–3 for mild malnutrition, 4–8 for moderate malnutrition, and ≥9 for severe malnutrition.
Kaplan-Meier Survival Curve
A three-year follow-up visit was conducted by telephone, SMS, and outpatient review. The follow-up included routine physical examination, tumor marker test, etc. In case, when patients experience any discomfort; they could visit the hospital at any time. The follow-up endpoint was death, and the follow-up deadline was April 2023.
Statistical Analysis
The results obtained for each scale were entered into a computer for score conversion, and statistical analysis was performed using SPSS 26 (IBM SPSS, USA). The measurement data were expressed as the mean and standard deviation, and the count data were expressed as frequency and percentage. The differences between groups were compared by performing t-tests and Chi-squared tests, and the factors influencing the occurrence of postoperative infection and prognosis were analyzed by binary logistic regression. Survival rates were determined from Kaplan-Meier survival curves. All differences between groups were considered to be statistically significant at p < 0.05 (two-sided).
Results
Baseline Data
The baseline data are presented in Table 1. In total, 339 patients with esophageal cancer who underwent radiotherapy were included in this study. The difference in the mean SAS score between the groups was significant in terms of gender, monthly household income, education level, whether surgery was performed, tumor size, TNM stage, radiotherapy dose, whether concurrent chemotherapy was administered, sleep status, and whether patients had dysphagia (p < 0.05). Female patients (N = 163; 48.1%) had a mean SAS score of 44.85 ±7.15, whereas male patients (N = 176; 51.9%) had a mean SAS score of 43.13 ±6.43. In total, 169 patients (49.9%) had a monthly household income of ≥ RMB 5000 and their mean SAS score was 42.51 ±5.63; 170 patients (50.1%) had a monthly household income of < RMB 5000 and their mean SAS score was 45.39 ±7.60. The mean SAS score was higher for patients with a higher level of education (44.69 ±7.52). In total, 129 patients (38.1%) who underwent surgery had a higher mean SAS score of 45.19 ±7.42. In total, 243 patients (71.7%) with a tumor diameter of <5 cm had a mean SAS score of 43.19 ±6.90, which was significantly lower than that of patients with a tumor diameter of ≥5 cm. In total, 194 patients (57.2%) with TNM stage < stage II had a mean SAS score of 42.55 ±5.86, which was significantly lower than that of patients with TNM stage ≥ stage II. The mean SAS scores were higher in patients with a radiotherapy dose >60Gy (45.01 ±7.86), simultaneous chemotherapy (45.18 ±8.10), and poor sleep status (45.11 ±7.57), and in those with swallowing disorders (45.01 ±7.70). The difference in the mean SDS scores between the groups was significant (p < 0.05) in terms of gender, whether surgery was performed, tumor size, the TNM stage, number of concomitant gastrointestinal symptoms, radiotherapy dose, and whether they underwent concurrent chemotherapy. The mean SDS score was 47.25 ±7.36 for female patients and 45.35 ±7.36 for male patients. Patients who underwent surgery had a higher mean SDS score of 47.49 ±7.69. Patients with a tumor diameter of <5 cm had a mean SDS score of 45.53 ±7.46, which was significantly lower than that of patients with a tumor diameter of ≥5 cm. Patients with a TNM stage <II had a mean SDS score of 45.32 ±7.04, which was significantly lower than that of patients with a TNM stage ≥II. Patients with ≥2 concomitant gastrointestinal symptoms, a radiotherapy dose >60 Gy, and concurrent chemotherapy had higher mean SDS scores of 47.37 ±8.34, 47.31 ±7.77, and 47.75 ±7.84, respectively.
 |
Table 1 The SAS and SDS Scores of the Participants |
Comparison of Complications Between the Groups of Patients
The results of the Chi-squared test showed that radiographic dermatitis, radiographic pneumonia, and edema were significantly different between the groups (p < 0.05). Among the patients in the negative mood group, five (8.1%), six (9.7%), and six (9.7%) patients had radiation dermatitis, radiation pneumonia, and edema, respectively, whereas six (2.2%), nine (3.2%), and 10 (3.6) % patients in the non-negative mood group had radiation dermatitis, radiation pneumonia, and edema, respectively (see Table 2).
 |
Table 2 Comparison of the Complications Between the Groups of Patients |
Comparison of Laboratory Indicators Between the Groups of Patients
The results of the t-test showed that the levels of Hb (Hemoglobin), Alb (Albumin), and TF (Transferrin) after radiotherapy were significantly different between the groups (p < 0.05). In patients in the negative mood group, the mean Hb concentration after radiotherapy was 115.86 ±11.31 g/L, the mean Alb concentration after radiotherapy was 28.48 ±5.44 g/L, and the mean TF concentration after radiotherapy was 1.79 ±0.28 g/L. In patients in the non-negative mood group, they were 119.62 ±10.79 g/L, 30.43 ±3.54 g/L, and 1.88 ±0.29 g/L, respectively (Table 3).
 |
Table 3 Comparison of Laboratory Indicators Between the Groups of Patients |
Comparison of PG-SGA Scores Between the Groups of Patients Before and After Treatment
The results of the t-test showed that PG-SGA after one, three, and six months of treatment were significantly different between the groups of patients (p < 0.05). The mean PG-SGA after one, three, and six months of treatment was 2.79 ±1.88, 3.47 ±2.25, and 4.21 ±2.58, respectively, in patients in the negative mood group and 1.97 ±2.11, 2.19 ±2.42, and 2.56 ±2.67, respectively, in patients in the non-negative mood group (Table 4).
 |
Table 4 Comparison of the PG-SGA Scores Between the Groups of Patients Before and After Treatment |
Binary Logistic Regression Analysis of the Negative Emotion and Malnutrition in Patients
The results of the binary logistic regression analysis showed that monthly household income <5000 yuan, tumor stage ≥II, concomitant gastrointestinal symptoms, poor sleep status, dysphagia, concomitant radiation dermatitis, and edema were independent risk factors for negative emotion in patients with esophageal cancer (p < 0.05) (see Table 5 and Figure 2).
 |
Table 5 Binary Logistic Regression Analysis of the Negative Emotions of Patients |
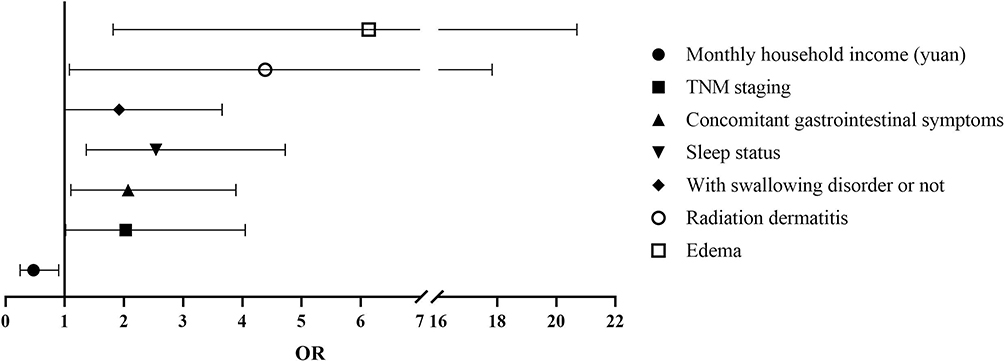 |
Figure 2 Binary logistic regression analysis of the negative emotion of patients. |
The results also showed that negative mood, advanced age, tumor diameter ≥5 cm, concomitant gastrointestinal symptoms >2, radiation dose >60 Gy, dysphagia, concomitant radiation esophagitis, hemoglobin concentration before and after radiotherapy, and a lower concentration of albumin before radiotherapy were independent risk factors for the development of malnutrition in patients with esophageal cancer (p < 0.05) (see Table 6 and Figure 3).
 |
Table 6 Binary Logistic Regression Analysis of the Patients Suffering from Malnutrition |
 |
Figure 3 Binary logistic regression analysis of the patients suffering from malnutrition. |
Survival Curves
The patients were followed up for three years. The difference in the cumulative survival function between patients in the negative emotion group and those in the non-negative emotion group was not statistically significant (p > 0.05), which indicated that negative emotions did not affect the short-term survival of the patients (Figure 4).
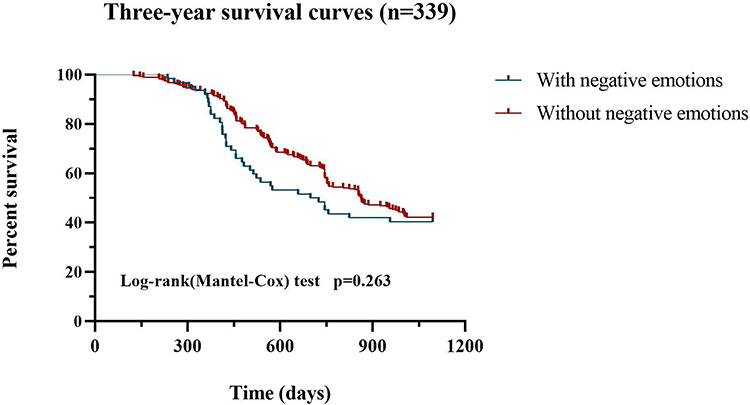 |
Figure 4 Kaplan-Meier survival curves of the patients in the negative emotion group and those in the non-negative emotion group. |
Discussion
Esophageal cancer often causes choking, difficulty in swallowing, sensation of a foreign body, and pain behind the sternum. If it metastasizes or invades adjacent organs, it causes pain and discomfort in the affected organs. It is the eighth leading cause of cancer-related deaths and the 10th most common malignancy worldwide.18 In 2020, approximately 641,100 new cases of esophageal cancer and 544,100 deaths were reported worldwide. Squamous cell carcinoma of the esophagus accounted for 85% of these cases.19 The incidence and mortality rates in different regions of the world are different; the highest incidence rates are recorded in East Asia and Southern and East Africa. China is one of the countries with the highest incidence and mortality rates of esophageal cancer.20 Radiotherapy is an effective treatment strategy for esophageal cancer and considerably prolongs the survival of patients.6,7,21 Patients with esophageal cancer who are administered radiotherapy are prone to negative emotions, anxiety, and depression during treatment, which can greatly affect the postoperative recovery and prognosis, thus reducing the effectiveness of treatment and the quality of life of patients. Additionally, several studies have shown that depression and anxiety are significantly higher in patients with esophageal cancer than in the general population and in patients with other types of cancer.22–24 The prevalence of anxiety and depression in this population is significant, with one study finding that 34% of patients reported anxiety and 23% reported depression prior to surgery.25 Therefore, the risk factors for negative emotions in patients with esophageal cancer during the peri-radiotherapy period need to be identified to improve the prognosis of the patients.
The results of this study showed that the monthly household income, tumor stage, concomitant gastrointestinal symptoms, sleep status, swallowing disorders, and post-radiotherapy complications, such as radiation dermatitis and edema, were independent risk factors for negative emotions during the peri-radiotherapy period in patients with esophageal cancer. In another study, household income and psychological distress were found to be negatively correlated.26 Esophageal cancer is a chronic wasting disease and is expensive to treat. Patients have no source of income during radiotherapy and recuperation, and the financial pressure on the family directly translates to psychological pressure for the patients, and it further increases their chances of suffering from depression. The more advanced the stage of the tumor, the more gastrointestinal symptoms accompanied, and the more negative the patient’s perception of the disease. The cognition of different patients for esophageal cancer is related to their education level and region.27 Some patients even have serious misunderstandings. These include not being able to truly agree on the effectiveness of the treatment, or even being so persistently negative that they abandon the treatment. Some studies have also found that sleep disorders, especially insomnia, affect 50% of patients with anxiety disorders, and sleep deprivation can trigger or further exacerbate anxiety disorders.28 Insomnia is a very common symptom in cancer patients, and some studies have shown that insomnia peaks after cancer diagnosis and during oncology treatment.29,30 Chronic insomnia can negatively affect the mood, somatic symptoms, pain sensitivity, fatigue, and quality of life of cancer patients.31 Cancer patients with insomnia are prone to fatigue, reduced energy levels, and they might also suffer from mood problems (eg, anxiety and depression). These changes might lead to a poorer quality of life in terms of physical and emotional functioning.32–34 Insomnia might also lead to depression or a relapse of depression in patients with a history of depression.35–37 Insomnia is also associated with impaired daily activities, sudden events or falls, impaired cognitive function, treatment decision-making ability, treatment compliance, immune function, and many other functions. It can even increase all-cause mortality in cancer patients.38 Patients with swallowing dysfunction who develop negative emotions, such as stress and irritability, are prone to anorexia and refusal to eat and lose their sense of conviction. These problems seriously affect the recovery, disease treatment, and prognosis of patients. For the treatment of dysphagia, it is often relieved by placing a self-expanding metal stent (SEMS). Studies have shown that SEMS can effectively relieve inoperable esophageal cancer and prolong survival.39 Post-radiotherapy complications not only increase the physical suffering of patients but also make them doubt the effectiveness of the treatment, thus increasing the psychological burden of the patients. Therefore, besides administering medication to patients, medical staff should also pay attention to the emotional value of the patients for maintaining a relaxed and happy psychological state, presenting a sincere and gentle attitude, providing more care and companionship, listening patiently to the complaints of the patients, and quickly understanding their true feelings and psychological and emotional changes. This can help formulate relevant and effective psychological intervention measures. For patients with low family income, the cost of treatment needs to be reduced based on the efficacy of the treatment and the condition of the patients and their families to adopt a personalized treatment plan to reduce the psychological burden on the patient and the economic burden on the family.
Some studies have shown that about 60–85% of patients suffer from malnutrition during the treatment of esophageal cancer. The mechanism of malnutrition is complex and might be associated with the special physiological function of the disease, anatomical structure, tumor-related factors, such as dysphagia and obstruction, and treatment-related factors, such as gastroesophageal reflux caused by surgery and vomiting caused by chemotherapeutic drugs.4,5 Malnutrition is very harmful and can reduce the treatment tolerance of patients and decrease treatment sensitivity, resulting in longer hospital stays or shorter survival times.40,41 Therefore, ways to prevent malnutrition during the peri-radiotherapy period in patients with esophageal cancer need to be determined. In this study, we found that negative emotions were an independent risk factor for malnutrition in patients with esophageal cancer. Patients with negative emotions were more likely to develop malnutrition (Table 4), as determined by the results of the regression analysis. This relationship occurred probably because negative emotions can disrupt cytokine levels in patients, leading to psychological anorexia, and they may also cause sympathetic excitation, which inhibits gastrointestinal motility and the secretion of digestive juices, thus leading to a loss of appetite, inadequate protein intake, and greater malnutrition in patients.42 Severe depression can also lead to malnutrition by producing an inflammatory response that promotes muscle protein hydrolysis, which might result in abnormal iron metabolism and increase the risk of inadequate synthesis of human blood albumin.43
The results of the logistic regression also showed that age >60 years, tumor >5 cm, concomitant gastrointestinal symptoms >2, radiotherapy dose >60 Gy, dysphagia, radiation esophagitis, the concentration of hemoglobin before and after radiotherapy, and the concentration of albumin before radiotherapy were also independent risk factors for malnutrition in patients with esophageal cancer. With age, gastrointestinal function gradually decreases; especially, the elderly have a poorer ability to digest and absorb food, and radiotherapy affects their intake of nutrients, which easily leads to malnutrition.44–46 Patients with large tumors are more prone to malnutrition, mainly because the metabolic abnormalities of patients with larger tumors are more serious, and proteins and other nutrients are metabolized and consumed faster, but the daily intake of nutrients cannot meet the energy demands for the growth and proliferation of cancer cells.9,47,48 Radiotherapy can lead to gastrointestinal symptoms, such as nausea and vomiting, diarrhea, and loss of appetite, and when the number of gastrointestinal symptoms is very high, the intake and absorption of nutrients are seriously affected, which increases the likelihood of malnutrition.49 This also occurs in patients with dysphagia and radiation esophagitis, where restricted feeding results in inadequate intake of nutrients. The high energy consumption during radiotherapy makes the patients vulnerable to malnutrition.50 Additionally, the dose of radiotherapy strongly affects malnutrition. A high dose of radiotherapy can aggravate the damage to the esophageal mucosa and neuromuscular damage. This can result in weakened peristalsis, prolonging the passage of harmful substances through the esophagus and causing symptoms such as edema, congestion, and erosion to persist for a long time,40 which in turn can cause patients to experience discomfort or pain while eating. For example, the nutritional status of elderly patients should be monitored, their diet should be planned according to their condition and nutritional requirements, and they should be instructed to exercise moderately. For patients with many gastrointestinal symptoms and postoperative comorbidities, symptomatic treatment is administered to alleviate discomfort, and food is provided to improve the appetite and correct electrolyte disturbances for reducing nausea and vomiting. For patients with swallowing disorders, swelling and pain relief might be provided, and patients may be given training on swallowing to reduce the damage to the laryngeal nerve and help them consume as much food as possible.
To summarize, patients with esophageal cancer are more likely to have negative emotions during the peri-radiotherapy period. The American Society of Clinical Oncology (ASCO) and the American Cancer Society have both emphasized the importance of assessing patients for distress, depression, and anxiety.51 They recommend offering in-office counseling and/or pharmacotherapy and/or referral to appropriate psycho-oncology and mental health resources as clinically indicated if signs of distress, depression, or anxiety are present.52 Therefore, clinical staff should quickly identify the relevant risk factors and actively provide psychological counseling to improve compliance with treatment and enhance the quality of life of patients after radiotherapy.
Due to limited time and manpower, the sample size of this study was small. Also, this was a single-center study. Future researchers should consider increasing the sample size and sample source to conduct a comprehensive study that might be used as a reference for improving the prognosis of patients with esophageal cancer.
Conclusions
Many patients with esophageal cancer suffer from anxiety and depression in the peri-radiotherapy period, which might lead to complications such as malnutrition or aggravate and affect the prognosis of patients. Therefore, psychological care should be provided based on conventional care to effectively relieve their psychological pressure, help them face cancer more calmly, and improve their prognosis and quality of life.
Ethical Statement
The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). The study was approved by Ethics Committee of Hai’an People Hospital (No. 202230) and informed consent was taken from all the patients.
Funding
Application of precision nursing model in nutritional support for patients with esophageal cancer during periradiotherapy (No. 202230).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Hiroshima Y, Ishikawa H, Sumiya T, et al. Clinical impact of proton beam therapy for postoperative lymph node oligorecurrence of esophageal cancer. In Vivo. 2023;37:1791–7549.
2. Wang XS, Kong DJ, Lin TY, et al. A versatile nanoplatform for synergistic combination therapy to treat human esophageal cancer. Acta Pharmacol Sin. 2017;38:1745–7254.
3. Cong MH, Li SL, Cheng GW, et al. An interdisciplinary nutrition support team improves clinical and hospitalized outcomes of esophageal cancer patients with concurrent chemoradiotherapy. Chin Med J. 2015;128:2542–5641.
4. Nakano T, Koyama K. 低栄養・栄養障害合併例における食道癌手術と周術期管理 [Surgery and perioperative management of esophageal cancer patients with malnutrition]. Kyobu Geka J JPN INT ECON. 2020;73:0021–5252. Japanese.
5. Wang C, Lu M, Zhou T, et al. Intensity-modulated radiotherapy does not decrease the risk of malnutrition in esophageal cancer patients during radiotherapy compared to three-dimensional conformal radiation therapy. J Thorac Dis. 2019;11:2072.
6. Wang SX, Marshall MB. Chemoradiation therapy as definitive treatment of esophageal cancer. Surg Clin. 2021;101:1558–3171.
7. Anderluh F, Toplak M, Velenik V, et al. Definitive radiochemotherapy in esophageal cancer - a single institution experience. Radiat Oncol J. 2019;53:1581–3207.
8. Lyu JH, Li T, Han YT, et al. Effect of weight loss on survival in esophageal cancer patients undergoing neoadjuvant chemoradiotherapy and Surgery. J Nutr Oncol. 2020;5(3):137–146. doi:10.34175/jno202003005
9. Zhou XL, Zhu WG, Zhu ZJ, et al. Lymphopenia in esophageal squamous cell carcinoma: relationship to malnutrition, various disease parameters, and response to concurrent chemoradiotherapy. Oncologist. 2019;24(8):e677–e86. doi:10.1634/theoncologist.2018-0723
10. Nakamura Y, Momoki C, Okada G, et al. Preoperative depressive mood of patients with esophageal cancer might delay recovery from operation-related malnutrition. J Clin Med Res. 2019;11(3):188–195. doi:10.14740/jocmr3704
11. Reich M. Depression and cancer: recent data on clinical issues, research challenges and treatment approaches. Curr Opin Oncol. 2008;20(4):353–359. doi:10.1097/CCO.0b013e3282fc734b
12. Pasquini M, Biondi M. Depression in cancer patients: a critical review. Clin Pract Epidemiol Ment Health. 2007;3(1):2. doi:10.1186/1745-0179-3-2
13. Donnelly M, Anderson LA, Johnston BT, et al. Oesophageal cancer: caregiver mental health and strain. Psychooncology. 2008;17(12):1196–1201. doi:10.1002/pon.1337
14. Haj Mohammad N, Walter AW, Van Oijen MG, et al. Burden of spousal caregivers of stage II and III esophageal cancer survivors 3 years after treatment with curative intent. Support Care Cancer. 2015;23(12):3589–3598. doi:10.1007/s00520-015-2727-4
15. Housman B, Flores R, Lee DS. Narrative review of anxiety and depression in patients with esophageal cancer: underappreciated and undertreated. J Thoracic Dis. 2021;13(5):3160–3170. doi:10.21037/jtd-20-3529
16. Jia L, Jiang SM, Shang YY, et al. Investigation of the incidence of pancreatic cancer-related depression and its relationship with the quality of life of patients. Digestion. 2010;82(1):4–9. doi:10.1159/000253864
17. Abbott J, Teleni L, Mckavanagh D, et al. Patient-generated subjective global assessment short form (PG-SGA SF) is a valid screening tool in chemotherapy outpatients. Support Care Cancer. 2016;24(9):3883–3887. doi:10.1007/s00520-016-3196-0
18. Torre LA, Bray F, Siegel RL, et al. Global cancer statistics 2012. CA Cancer J Clin. 2015;65(2):87–108. doi:10.3322/caac.21262
19. Morgan E, Soerjomataram I, Rumgay H, et al. The global landscape of esophageal squamous cell carcinoma and esophageal adenocarcinoma incidence and mortality in 2020 and projections to 2040: new estimates From GLOBOCAN 2020. Gastroenterology. 2022;163(3):649–58.e2. doi:10.1053/j.gastro.2022.05.054
20. Bo Y, Wang K, Liu Y, et al. The geriatric nutritional risk index predicts survival in elderly esophageal squamous cell carcinoma patients with radiotherapy. PLoS One. 2016;11(5):e0155903. doi:10.1371/journal.pone.0155903
21. Wang S, Zhang C, Wang Y, et al. Risk factors and prognosis for esophageal fistula in patients with esophageal squamous cell carcinoma during radiotherapy. Esophagus. 2022;19(4):660–669. doi:10.1007/s10388-022-00919-4
22. Wikman A, Ljung R, Johar A, et al. Psychiatric morbidity and survival after surgery for esophageal cancer: a population-based cohort study. J Clin Oncol. 2015;33(5):448–454. doi:10.1200/JCO.2014.57.1893
23. Hellstadius Y, Lagergren J, Zylstra J, et al. A longitudinal assessment of psychological distress after oesophageal cancer surgery. Acta Oncol. 2017;56(5):746–752. doi:10.1080/0284186X.2017.1287945
24. Hu LY, Ku FC, Wang YP, et al. Anxiety and depressive disorders among patients with esophageal cancer in Taiwan: a nationwide population-based study. Support Care Cancer. 2015;23(3):733–740. doi:10.1007/s00520-014-2403-0
25. Hellstadius Y, Lagergren J, Zylstra J, et al. Prevalence and predictors of anxiety and depression among esophageal cancer patients prior to surgery. Dis Esophagus. 2016;29(8):1128–1134. doi:10.1111/dote.12437
26. Chen B, Gong W, Lai AY, et al. Family context as a double-edged sword for psychological distress amid the COVID-19 pandemic with the mediating effect of individual fear and the moderating effect of household income. Front Public Health. 2023;11:1109446. doi:10.3389/fpubh.2023.1109446
27. Duron V, Bii J, Mutai R, et al. Esophageal cancer awareness in bomet district, Kenya. Afr Health Sci. 2013;13(1):122–128. doi:10.4314/ahs.v13i1.17
28. ChellappasL, Aeschbach D. Sleep and anxiety: from mechanisms to interventions. Sleep Med Rev. 2022;61:101583. doi:10.1016/j.smrv.2021.101583
29. Savard J, Liu L, Natarajan L, et al. Breast cancer patients have progressively impaired sleep-wake activity rhythms during chemotherapy. Sleep. 2009;32(9):1155–1160. doi:10.1093/sleep/32.9.1155
30. Savard J, Hervouet S, Ivers H. Prostate cancer treatments and their side effects are associated with increased insomnia. Psychooncology. 2013;22(6):1381–1388. doi:10.1002/pon.3150
31. Léger D, Mc M, Uchiyama M, et al. Chronic insomnia, quality-of-life, and utility scores: comparison with good sleepers in a cross-sectional international survey. Sleep Med. 2012;13(1):43–51. doi:10.1016/j.sleep.2011.03.020
32. Lourenço A, Dantas AAG, De Souza JC, et al. Sleep quality is associated with disability and quality of life in breast cancer survivors: a cross-sectional pilot study. Eur J Cancer Care. 2020. e13339. doi:10.1111/ecc.13339
33. Fortner BV, Stepanski EJ, Wang SC, et al. Sleep and quality of life in breast cancer patients. J Pain Symptom Manage. 2002;24(5):471–480. doi:10.1016/S0885-3924(02)00500-6
34. Chen ML, Yu CT, Yang CH. Sleep disturbances and quality of life in lung cancer patients undergoing chemotherapy. Lung Cancer. 2008;62(3):391–400. doi:10.1016/j.lungcan.2008.03.016
35. Campbell P, Tang N, Mcbeth J, et al. The role of sleep problems in the development of depression in those with persistent pain: a prospective cohort study. Sleep. 2013;36(11):1693–1698. doi:10.5665/sleep.3130
36. Irwin MR, Olmstead RE, Ganz PA, et al. Sleep disturbance, inflammation and depression risk in cancer survivors. Brain Behav Immun. 2013;30(Suppl):S58–67. doi:10.1016/j.bbi.2012.05.002
37. Jim HS, Jacobsen PB, Phillips KM, et al. Lagged relationships among sleep disturbance, fatigue, and depressed mood during chemotherapy. Health Psychol. 2013;32(7):768–774. doi:10.1037/a0031322
38. Hiller RM, Johnston A, Dohnt H, et al. Assessing cognitive processes related to insomnia: a review and measurement guide for harvey’s cognitive model for the maintenance of insomnia. Sleep Med Rev. 2015;23:46–53. doi:10.1016/j.smrv.2014.11.006
39. White Russell E, Parker Robert K, Fitzwater John W, et al. Stents as sole therapy for oesophageal cancer: a prospective analysis of outcomes after placement. Lancet Oncol. 2009;10(3):240–246. doi:10.1016/S1470-2045(09)70004-X
40. Yang K, Oh D, J.m N, et al. Feasibility of an interactive health coaching mobile app to prevent malnutrition and muscle loss in esophageal cancer patients receiving neoadjuvant concurrent chemoradiotherapy: prospective pilot study. J Med Internet Res. 2021;23(8):e28695. doi:10.2196/28695
41. Movahed S, Norouzy A, Ghanbari-motlagh A, et al. Nutritional status in patients with esophageal cancer receiving chemoradiation and assessing the efficacy of usual care for nutritional managements. Asian Pac J Cancer Prev. 2020;21(8):2315–2323. doi:10.31557/APJCP.2020.21.8.2315
42. Li ZJ, An X, Maoh P, et al. Association between depression and malnutrition-inflammation complex syndrome in patients with continuous ambulatory peritoneal dialysis. Int Urol Nephrol. 2011;43(3):875–882. doi:10.1007/s11255-011-9917-x
43. Maes M, Kubera M, Leunisj C. The gut-brain barrier in major depression: intestinal mucosal dysfunction with an increased translocation of LPS from gram negative enterobacteria (leaky gut) plays a role in the inflammatory pathophysiology of depression. Neuro Endocrinol Lett. 2008;29(1):117–124.
44. Holder H. Malnutrition in the elderly: a public health concern. Br J Nurs. 2020;29(2):118–119. doi:10.12968/bjon.2020.29.2.118
45. Doğan Akagündüz D, Türker PF. Nutritional support in older patients with esophageal cancer undergoing chemoradiotherapy. Nutr Cancer. 2022;74(10):3634–3639. doi:10.1080/01635581.2022.2096245
46. Song T, Fang M, Wu S. Concurrent chemoradiation therapy tailored to the older adults with esophageal cancer: state of the art and the future. Clin Interv Aging. 2018;13:2275–2287. doi:10.2147/CIA.S179014
47. Jachnis A, M.t S. The relationship between nutritional status and body composition with clinical parameters, tumor stage, ca19-9, cea levels in patients with pancreatic and periampullary Tumors. Curr Oncol. 2021;28(6):4805–4820. doi:10.3390/curroncol28060406
48. Takeda K, Umezawa R, Takahashi N, et al. Impact of change in serum albumin level during and after chemoradiotherapy in patients with locally advanced esophageal cancer. Esophagus. 2018;15(3):190–197. doi:10.1007/s10388-018-0612-1
49. Wang B, Xu C, Ying K, et al. Prognostic value of hemoglobin combined with geriatric nutritional risk index scores in patients undergoing postoperative radiotherapy for esophageal squamous cell carcinoma. Future Oncol. 2022;18(2):179–191. doi:10.2217/fon-2021-0439
50. Blanař V, Hödl M, Lohrmann C, et al. Dysphagia and factors associated with malnutrition risk: a 5-year multicentre study. J Adv Nurs. 2019;75(12):3566–3576. doi:10.1111/jan.14188
51. Andersen BL, DeRubeis RJ, Berman BS, et al. Screening, assessment, and care of anxiety and depressive symptoms in adults with cancer: an American society of clinical oncology guideline adaptation. J Clin Oncol. 2014;32(15):1605–1619. doi:10.1200/JCO.2013.52.4611
52. Rk P, Sm D, Cc A, Re W. Frequent occurrence of esophageal cancer in young people in western Kenya. Dis Esophagus. 2010;23(2):128–135. doi:10.1111/j.1442-2050.2009.00977.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.