")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Analysis of Risk Factors and Screening Results of Neonatal Congenital Hypothyroidism in a Tertiary Care Center of Southern China
Authors Yan X, Wang L, Chen X, Wang A
Received 8 December 2022
Accepted for publication 1 March 2023
Published 18 March 2023 Volume 2023:16 Pages 741—749
DOI https://doi.org/10.2147/JMDH.S400804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xueqin Yan,1,* Li Wang,1,* Xiaolan Chen,1 Anru Wang2
1Department of Child Health Care, Boai Hospital of Zhongshan Affiliated to Southern Medical University, Zhongshan, 528400, People’s Republic of China; 2Department of Pediatrics, The Second of Affiliated Hospital of Nanjing Medical University, Nanjing, 210003, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Anru Wang, Department of Pediatrics, The Second of Affiliated Hospital of Nanjing Medical University, No. 262 of Zhongshan North Road, Nanjing, 210003, People’s Republic of China, Tel +86 25 83575027, Fax +86 25 58509975, Email [email protected] Xueqin Yan, Department of Child Health Care, Boai Hospital of Zhongshan Affiliated to Southern Medical University, No. 6 of Chenggui Road, Zhongshan, 528400, People’s Republic of China, Tel +86 760-88776567, Fax +86 760-88306163, Email [email protected]
Objective: To explore the risk factors for neonatal congenital hypothyroidism (CH) and the influencing factors of false-positive results in CH screening.
Methods: In this study, 255 neonatal patients with CH who completed the screening and further diagnosis and 366 neonates with positive CH screening results and normal thyroid function were selected as the case group. 246 healthy neonates with normal thyroid function were selected as the control group. Gestational age, birth-weight, maternal age, small for gestational age (SGA), perinatal factors (gestational thyroid dysfunction, gestational diabetes mellitus, etc.) were used as influencing factors, using χ2 tests were performed for comparison. The statistically significant variables were analyzed with Logistic multiple regression models, and the difference was considered statistically significant (P< 0.05).
Results: There were statistical differences in the SGA, maternal gestational diabetes mellitus, thyroid disease, and the proportion using assisted reproduction technology among the case group, false-positive screening group, and control group (χ2 was 11.943, 6.857, 6.999, 9.732, respectively, P < 0.05). The results of multivariate logistic regression analysis showed that the gestational thyroid disease (OR = 8.452, 95% CI:1.051– 67.982), gestational diabetes mellitus (OR = 2.654, 95% CI:1.051– 6.706), and assisted reproduction (OR = 0.194, 95% CI:0.041– 0.911) were the influencing factors for neonatal CH, and the difference was statistically significant (P < 0.05). The SGA (OR = 2.556, 95% CI:1.027– 6.361), gestational thyroid disease (OR = 7.801, 95% CI:1.03– 59.057), gestational diabetes mellitus (OR = 2.731, 95% CI:1.18– 6.322), and assisted reproduction (OR = 0.28, 95% CI:0.102– 0.765) were the influencing factors of the false-positive screening results of neonatal CH. The difference was statistically significant (P < 0.05).
Conclusion: Neonatal CH and positive screening results are influenced by assisted reproduction, gestational thyroid dysfunction, gestational diabetes mellitus, and SGA.
Keywords: congenital hypothyroidism, false-positive, influencing factors, neonates
Introduction
Congenital hypothyroidism (CH) is a common endocrine disease in neonates. The most common causes of the disease are thyroid dysplasia and thyroid hormone synthesis disorders, which prevent the thyroid gland from producing sufficient thyroid hormones to meet the body’s needs.1 CH is one of the most common preventable causes of nervous system developmental disorders. Most neonates with CH usually have a normal appearance and non-specific clinical symptoms and signs. Early screening, diagnosis, and treatment can significantly improve the prognosis of neonatal patients with CH.2 CH screening of neonates has been widely conducted in many countries worldwide. With the increase in neonatal screening items, the sensitivity of thyrotropin (TSH) detection, and the survival rate of premature infants, the incidence of CH has also increased worldwide.3
The combination of genetic and environmental factors leads to neonatal CH. Since CH mainly occurs in utero, maternal gestational factors and fetal growth and development are closely related to neonatal CH. Some studies have shown that modifiable environmental risk factors such as air pollution and perfluoroalkyl group contribute to the emergence of CH.4,5 Therefore, the causes of CH may be mitigated by studying the perinatal factors associated with CH. A meta-analysis showed that advanced maternal age, gestational thyroid disease, gestational diabetes mellitus, gestational anxiety, gestational drugs, radiation exposure during the gestation period, family history of thyroid disease, low birth weight, macrosomia, premature infant, post-term infant, twins and multiple births, and birth defects increase the risk of neonatal CH.6
In addition, the neonatal thyroid function of small for gestational age (SGA) is less mentioned. SGA refers to infants whose birth weight is below the 10th percentile of the average weight for the same gestational age. The main characteristics of SGA are the changes in various pathophysiological mechanisms and endocrine metabolism. The thyroid level of full-term SGA is significantly lower than that of full-term appropriate for gestational age (AGA) infants.7 The SGA status is a surrogate marker for intrauterine growth restriction (IUGR), which is usually the result of placental hypoxia and fetal malnutrition. Studies have speculated that malnutrition affects the synthesis of thyroid hormones by reducing the availability of phenylalanine and tyrosine, which results in hypothyroidism. This endocrine metabolic state is associated with reduced oxygen consumption, which has an advantage in malnutrition or growth retardation.
With the development of neonatal screening, the early detection rate of neonatal CH has significantly improved. However, in addition to CH, ignorance of influencing factors of free thyroxine (FT4) and TSH in screening, leads to false-positive and negative results. For example, TSH physiologically surges in the first one to two days after birth and is gradually normalized. Thus, if the specimen is collected within 24 h after birth without considering collection time, the increase in TSH is considered to be cause by CH, thereby leading to false-positive results.8 Birth weight, premature birth, and gender, influence T4 and TSH values. Low or premature birth weight infants show delayed TSH elevation due to the immature hypothalamic-pituitary axis.9,10 Due to the natural differences in thyroid hormone levels between infant boys and infant girls, infant boys are more likely to show false-positive results in screening.11 Maternal gestational factors are known to impact fetal thyroid function, but whether they affect the CH screening results, is unknown.
In this study, we intend to analyze the perinatal factors of neonatal patients with CH and neonates with false-positive results in preliminary CH screening, to explore the risk factors for CH and the influencing factors of false-positive results in CH screening.
Data and Methods
General Study
A total of 255 neonatal patients with CH who completed the screening and further diagnosis from our hospital January 2016 to December 2021 were selected as the case group. Healthy neonates were randomly selected based on a 1:1 pairing principle as the control group and the matching conditions were as follows: 1) the screening results of neonatal diseases, including CH, phenylketonuria, congenital adrenal cortical hyperplasia, G6PD deficiency, and thalassemia, were negative; 2) they were of the same gender and date of birth as neonatal patients with CH. 3) they had no history of birth defects, birth injuries by suffocation, neonatal infection, and others at birth. In this study, 246 neonates were included as the control group. Data of a total of 366 neonates with positive CH screening results and normal thyroid function during the reexamination were collected. Observational indicators in this study included gestational age, birth weight, maternal gestational age, maternal pregestational BMI, gestational method, and gestational disease. All guardians of the tested children were aware of the study content, signed the informed consent, and were approved by the hospital’s ethics committee.
Screening and Diagnostic Methods
The heel blood was collected using dried blood spots 48 h–7 days after the birth of neonates to test the thyroid stimulating hormone (TSH) level. If TSH > 8.5 μIU/mL, the screening results were positive. Neonates with positive screening results were called back for reexamination of thyroid function. The thyroid function detection indexes mainly included serum TSH, FT4, and free triiodothyronine (FT3). Diagnosis and treatment were conducted based on guidelines on neonatal CH.12
Statistical Methods
Data were processed using SPSS 19.0 software. Enumeration data were expressed as percentage (%) and compared with the χ2 test. Statistically significant variables were analyzed using logistic multiple regression model. P < 0.05 was considered a statistical difference.
Results
General Data
In this study, 255 neonatal patients with CH and 366 neonates with false-positive results in CH screening were screened, and 246 neonates with normal thyroid function were screened as the control. Of the 255 neonatal patients with CH, there were 150 males and 105 females, and the male–female ratio was 1.43:1. In the false-positive screening group, there were 222 males and 144 females, and the male-female ratio was 1.54:1. In the control group, there were 144 males and 102 females, and the male-female ratio was 1.41:1. There was no statistically significant difference in the gestational age, birth weight, and the proportion of maternal age among the three groups (P > 0.05, Table 1).
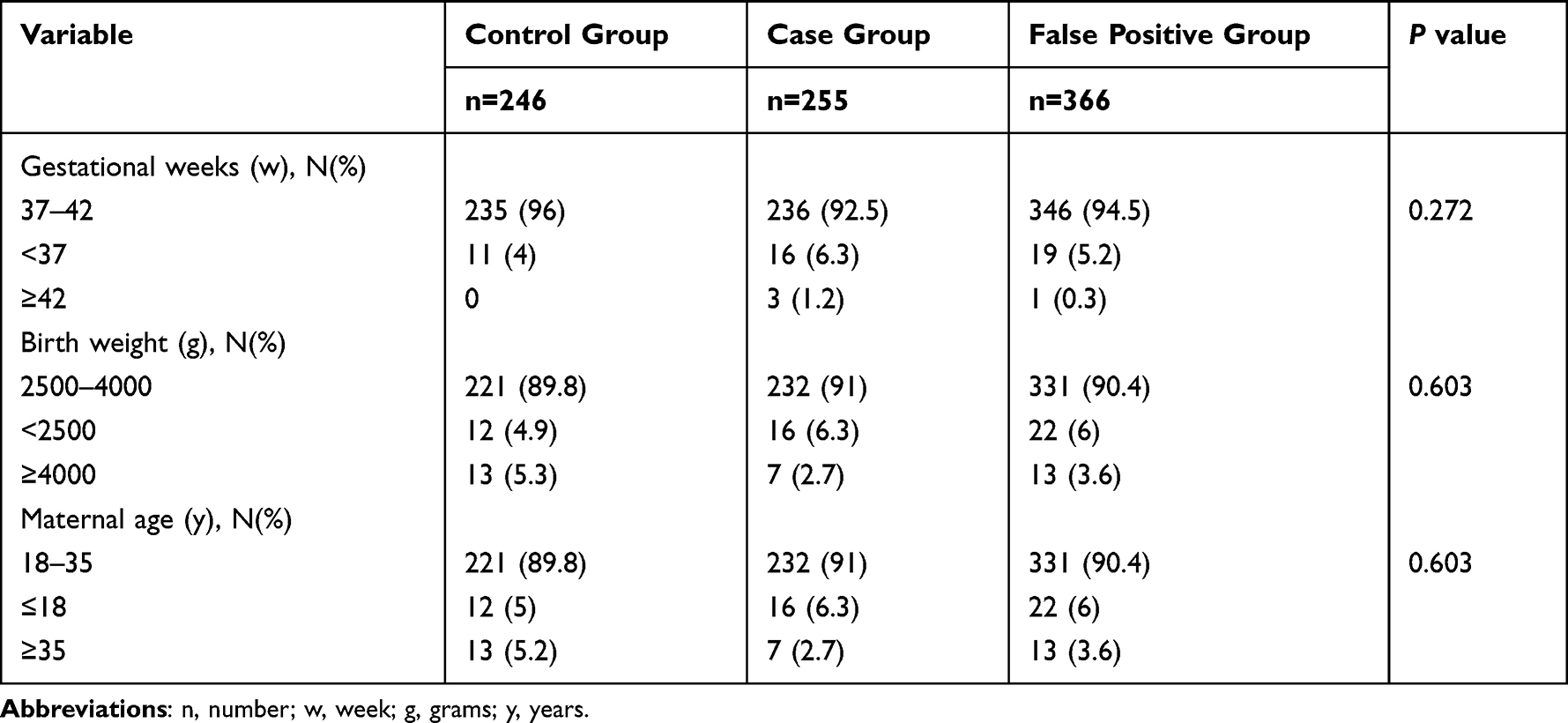 |
Table 1 Univariate Analysis of the General Condition of Neonatal Patients with CH |
Univariate Analysis of Risk Factors for CH
There were statistically significant differences in the proportion of SGA among the case group, false-positive screening group, and control group (χ2=11.943, P < 0.05, Table 2). Since antenatal care was not regularly provided to mothers of some neonatal patients with CH during pregnancy. 143 neonates in the control group, 140 neonates in the case group, and 335 neonates in the false-positive screening group were included in the univariate analysis of maternal gestational factors. There were statistically significant differences in maternal gestational diabetes mellitus (χ2=6.857, P=0.032), gestational thyroid disease (χ2=6.999, P=0.03), and proportion of using assisted reproduction technology among the three groups (χ2=9.732, P=0.008, Table 2). Compared with the control group, the mothers of the case group and false-positive screening group had a higher proportion of diabetes or thyroid diseases during pregnancy, and the proportion of using assisted reproductive technology was lower. There was no significant difference between the three groups in various types of maternal abortion ≥ 3 times, Pregestational BMI, Maternal hepatitis, Gestational hypertension or Gestational anemia (P>0.05).
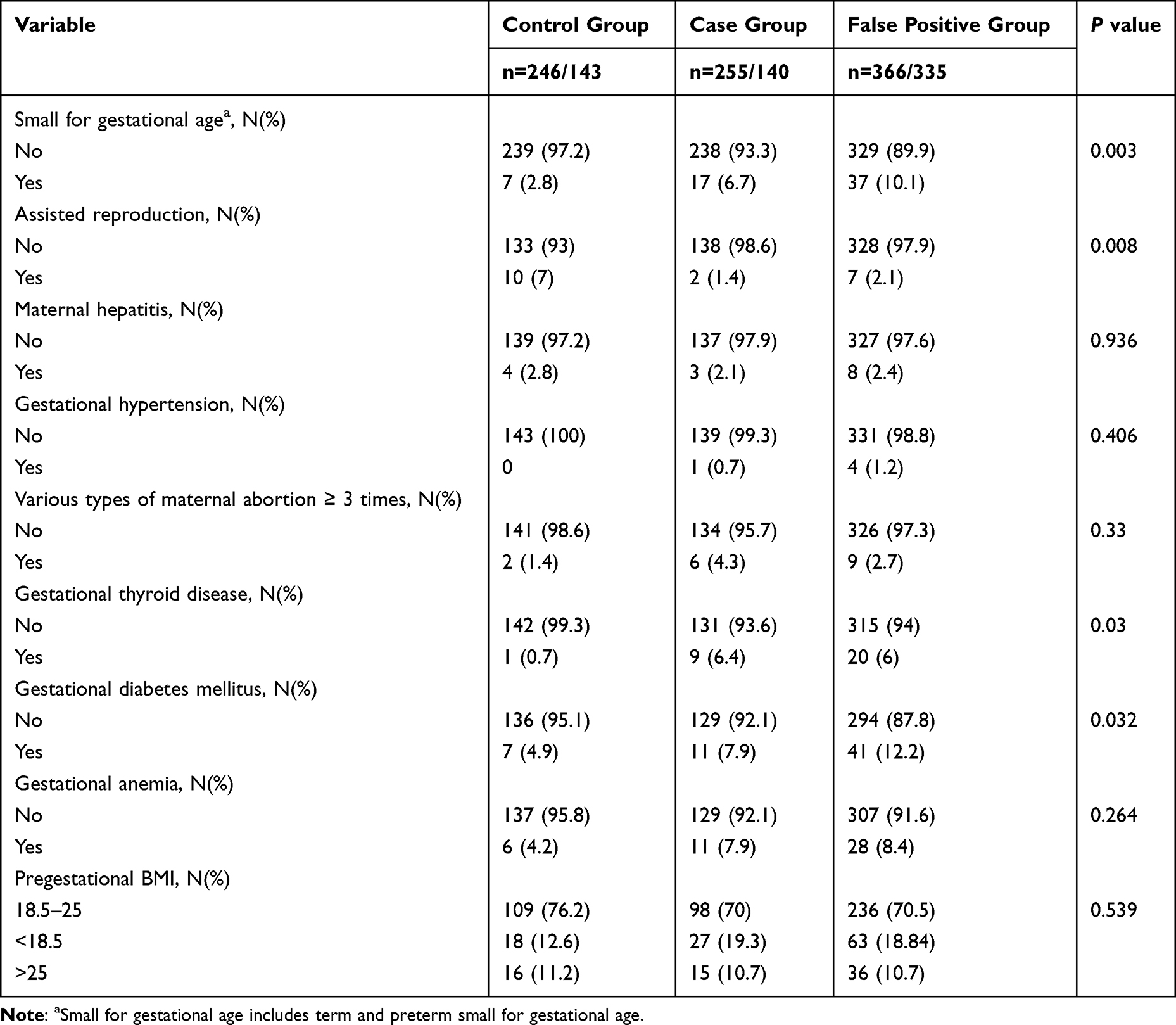 |
Table 2 Univariate Analysis of Perinatal Factors of Neonatal Patients with CH |
Multivariate Analysis of Risk Factors for CH
Multivariate logistic regression analysis was conducted on variables with statistical significance in the univariate analysis. The results showed that gestational thyroid disease (OR=8.452, 95% CI:1.051–67.982) and gestational diabetes mellitus (OR=2.654, 95% CI:1.051–6.706) were the risk factors for neonatal CH, and assisted reproduction (OR=0.194, 95% CI:0.041–0.911) was the protective factor for neonatal CH (Table 3). SGA (OR=2.556, 95% CI:1.027–6.361), gestational thyroid disease (OR=7.801, 95% CI:1.03–59.057), gestational diabetes mellitus (OR=2.731, 95% CI:1.18–6.322), and assisted reproduction (OR=0.28, 95% CI:0.102–0.765) were the influencing factors for the false-positive results of neonatal CH screening (Table 4).
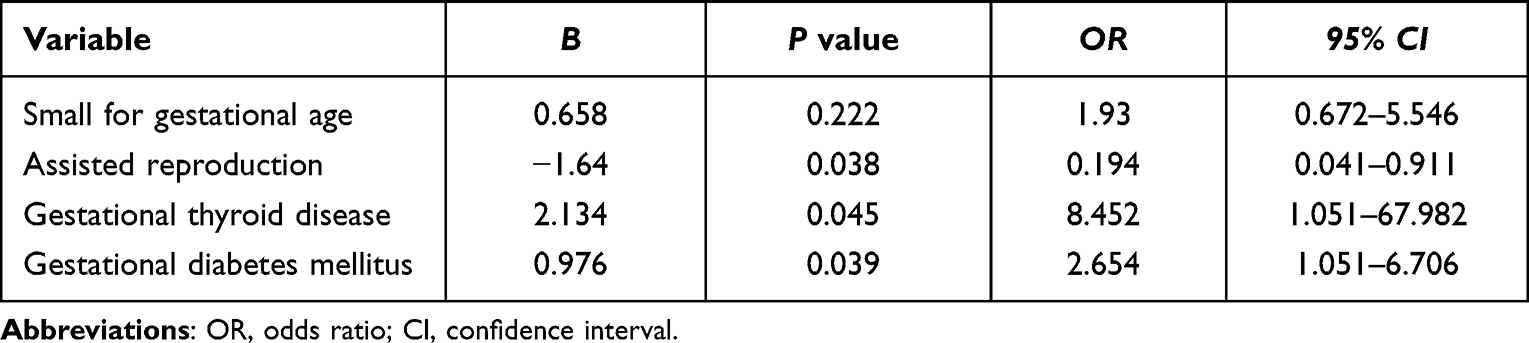 |
Table 3 Multivariate Logistic Regression Analysis of Perinatal Factors of Neonatal Patients with CH |
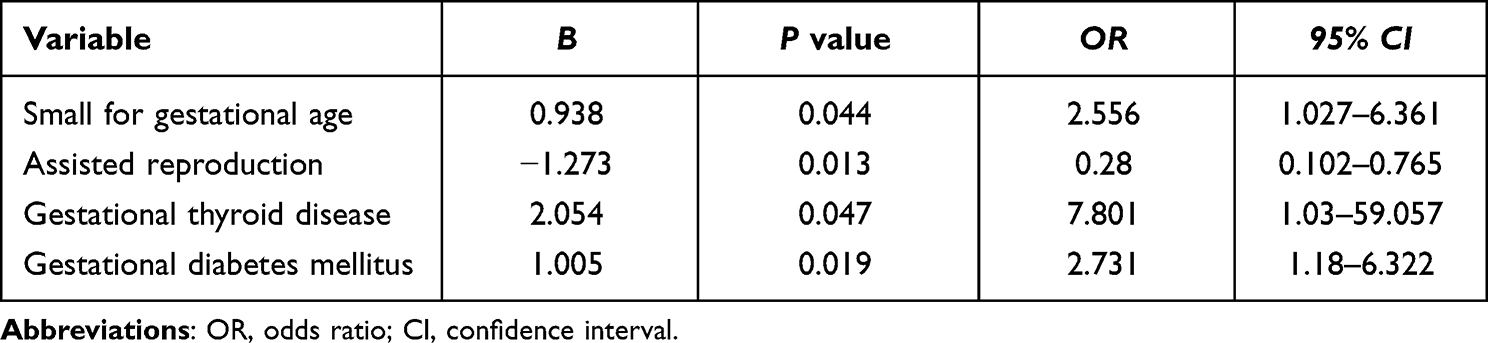 |
Table 4 Multivariate Logistic Regression Analysis of Perinatal Factors of Neonates with False Positive CH Screening Results |
Discussion
This study found that the thyroid function and thyroid function test results of newborns will be affected by SGA, gestational thyroid dysfunction, gestational diabetes mellitus, and assisted reproduction. The incidence of neonatal CH is affected by assisted reproduction, gestational thyroid dysfunction, and gestational diabetes mellitus. The false-positive results of CH primary screening were affected by SGA, assisted reproduction, gestational thyroid dysfunction, and gestational diabetes mellitus. Except for assisted reproduction, the above factors are all negative.
Impact of Maternal Gestational Factors on Neonatal Thyroid Function
Thyroid hormones promote fetal growth and development. The fetal thyroid begins to secrete thyroid hormones at 12 weeks of gestation and is mature at 20 weeks; after 26 weeks, the fetal hypothalamic-pituitary-thyroid (HPT) system is well-developed, but the feedback function is not mature until at full term.13–17 In the first and second trimesters of pregnancy, the fetal demand for thyroid hormones depends on the maternal supply; in the third trimester, the maternal thyroid hormones help the fetus use the thyroid hormones.18,19 Therefore, maternal factors during gestation and factors influencing the thyroid development of neonates contribute to neonatal CH.
Previous studies as well the current study have found that maternal gestational thyroid disease and diabetes mellitus are the risk factors for neonatal CH.6,20–23 For a mother with autoimmune thyroid disease, the TSH receptor antibody (TRAb) in vivo transmits to the fetus via the placenta. It inhibits the binding of TSH to the corresponding thyroid receptor, leading to fetal hypothyroidism.1 For a mother with gestational hyperthyroidism, when the dose of the antithyroid drug is high, the drug inhibits the secretion of fetal thyroid hormones via the placenta, which results in increased compensatory TSH secretion.24
In an experiment on streptozotocin-induced gestational diabetes mellitus in rats, the extent of maternal diabetes mellitus was negatively correlated with fetal thyroid hormone status.25 However, the causal relationship between gestational diabetes mellitus and neonatal CH is unclear. The abnormal glucose metabolism levels of mothers with gestational diabetes mellitus during pregnancy affect fetal development and increase the neonatal birth defect rate.26 Studies have suggested that in pregnant women with gestational diabetes mellitus, the risk of developing subclinical hypothyroidism also increases, but their relationship with offspring CH is unclear.27 Hua et al found that maternal gestational diabetes mellitus and thyroid dysfunction were mutually affected,28 which increased the risk of adverse pregnancy outcomes in the offspring. Controlling the balance of maternal gestational glucose metabolism reduces the occurrence of CH.
Most studies have confirmed that advanced maternal age is a risk factor for CH.6,20,21,29 As the age increases, the reproductive organ function of pregnant women decreases, and the incidence of complications during the gestation period increases, which affects the intrauterine environment and the nutrition supply of the embryo, and increases the risk of neonatal CH.29 In our study, we found no impact of advanced maternal age on neonatal CH.
We also found that assisted reproduction was a protective factor for CH. Previous studies have suggested that compared with single infants conceived naturally, there was no significant increase in the incidence of CH in infants conceived with the assistance of artificial insemination.30,31 Based on our study, it is speculated that assisted reproduction does not increase the incidence of CH and may even reduce it. More studies are needed to test this speculation in the future.
Impact of Fetal Growth and Development on Neonatal Thyroid Function
We found no impact of gestational age and birth weight on neonatal CH. Previous studies have shown that gestational age (premature birth, post-term birth) and birth weight (low birth weight, large for date infant) were the risk factors for CH.20,23,32,33 Due to intrauterine dysplasia, low birth-weight and premature infants have immature functional development of the pituitary-thyroid axis or abnormal thyroid development.34 Other studies have speculated that the placenta function of low birth-weight infants may be deficient and the maternal thyroid hormones transmitted to the fetus via the placenta decrease, thereby leading to hypothyroidism.33 Due to the increase in gestational weeks, post-term neonates have placental aging and decreased fetal organ function, which induces thyroid dysfunction.32 Besides, fetal hypothyroidism induces an increase in gestational weeks and intrauterine distress, which affects the thyroid function of the fetus.21
Analysis of False-Positive Results of Neonate Screening
Previous studies have mainly explored the changes in thyroid hormone levels and thyroid function of neonates from the perspective of premature birth or low birth-weight. Few studies have discussed changes in the thyroid from the perspective of whether birth weight is appropriate for gestational age.
The existing literature has confirmed that the TSH concentration in SGA is significantly higher than that in AGA,35–39 and that in some SGA, it is higher than the upper limit of the normal value.37 Whether the T4 level is low remains controversial. Franco and Thorpe-Beeston reported that the serum T4 level in SGA was significantly reduced.38,39 Radetti et al found no changes in the FT4 level.37 The high TSH and low T4 level in SGA neonates suggests that fetal T4 secretion decreases in the first few days after delivery.
Malnutrition caused by placental hypoxia and intrauterine growth retardation results in thyroid growth retardation and thus, a decrease in T4 secretion. The increase in TSH was interpreted as the pituitary feedback in SGA due to the low T4 level. Therefore, the nutritional condition did not influence the pituitary function.39 However, Chaudhari et al speculated that the factors contributing to the high TSH level in SGA involved the immaturity of the hypothalamic-pituitary-thyroid axis or other non-thyroid diseases.40 In an investigation involving 14,092 infants, 139 (0.98%) infants were called back due to positive CH screening results, including 1.84% SGA infants and 0.93% AGA infants. SGA neonates had a higher positive rate in the screening of congenital hypothyroidism.
Nevertheless, infants subsequently diagnosed with CH were all in the AGA group. Hypothyroidism in SGA neonates disappeared in the subsequent follow-up.39 Therefore, the occurrence of hypothyroidism in SGA neonates may be temporary and the TSH levels return to normal within a few months; this needs to be followed up closely. It is speculated that the recovery of the thyroid function in SGA was due to the improvement of postpartum nutrition.39 Kaluarachchi et al41 also clarified in their study that compared with CH neonates in the non-SGA group, those in the SGA group often developed a more transient congenital hypothyroidism, with TSH levels returning to normal without treatment. Based on previous results, the result of our study could be interpreted as, SGA neonates are more likely to be positive in CH screening and return to normal on the subsequent reexamination of thyroid function.
In addition, we found that gestational diabetes mellitus and thyroid dysfunction are risk factors that resulted in false-positive results in screening of neonatal CH and assisted reproduction is the protective factor. The TSH level was high in neonates born to mothers with a history of autoimmune thyroid disease before pregnancy.42 A retrospective study evaluated the relationship between maternal thyroid dysfunction and adverse birth outcomes. The study showed that infants born to mothers with thyroid dysfunction developed temporary or permanent CH. Venugopalan et al43 considered that the high positive rate of CH screening was attributed to two factors: The first was the influence of neonatal thyroid disease (the anti-TPO antibody was transmitted via the placenta); the second was the poor control over maternal antenatal thyroid disease, which resulted in the high TSH in the third trimester of pregnancy, which was then reflected in neonatal TSH. Among cases diagnosed and requiring lifelong treatment in this study, permanent thyroid defects accounted for 66% of all causes. The result differs from the commonly held belief that infants born to mothers with thyroid disease develop temporary CH. The reason for this result could be that high levels of TRAb are detected in the sera of neonatal patients with CH, and TRAb disrupts the normal growth and development of the fetal thyroid during pregnancy. Other studies also found that compared with the normal TSH preliminary screening group, the proportion of mothers with hypothyroidism was higher in the positive preliminary screening group.44 In the positive preliminary screening group, the proportion of mothers with hypothyroidism was higher in neonates diagnosed with CH compared with neonates who were normal in reexamination. Based on the above studies and our study, it is speculated that there seems to be a linear dimension in the effect of abnormal maternal thyroid on neonatal thyroid; when the effect is small, the neonatal thyroid function is normal, or there is only temporary hypothyroidism; when the effect is large, permanent hypothyroidism may be caused. However, more studies are needed to explore whether the effect is related to the severity of the abnormal maternal thyroid.
The limitation of this study is the lack of analysis of other potential risk factors, such as genetic predisposition, environmental exposure, and iodine deficiency. Since there was a minimum of two complications for part of the sample during pregnancy. We did not consider the influence of this condition on the results, and the reliability of the results may be lower. In addition, for newborns diagnosed as CH, this study did not further analyze the type of CH. Therefore, it is impossible to further explore whether these factors are related to the etiology of CH, such as congenital thyroid deficiency.
In conclusion, neonatal CH is influenced by assisted reproduction, abnormal gestational thyroid function, and gestational diabetes mellitus. In addition, SGA, assisted reproduction, abnormal gestational thyroid function, and gestational diabetes mellitus are the influencing factors for the false-positive results in the preliminary screening of neonatal CH. Based on the influence of the above factors on neonatal thyroid function, multiple screening and follow-ups are required during clinical screening to avoid misdiagnosis and missed diagnosis.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
I confirm that I have read the Editorial Policy pages. This study was conducted with approval from the Ethics Committee of Boai Hospital of Zhongshan Affiliated to Southern Medical University (2017-ky -001). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
Medical Science and Technology Research Foundation of Guangdong Province.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Wassner AJ. Congenital hypothyroidism. Clin Perinatol. 2018;45:1–18. doi:10.1016/j.clp.2017.10.004
2. Wang H, Wang Y, Wu W. The neonatal screening results of 229 336 cases in south region of Xinjiang. Chin J Birth Health Hered. 2019;27(2):176–177.
3. Olivieri A, Fazzini C, Medda E. Multiple factors influencing the incidence of congenital hypothyroidism detected by neonatal screening. Hormone Res Paediatr. 2015;83:86–93. doi:10.1159/000369394
4. Shang L, Huang L, Yang W, et al. Maternal exposure to PM2.5 may increase the risk of congenital hypothyroidism in the offspring: a national database based study in China. BMC Public Health. 2019;19:1412. doi:10.1186/s12889-019-7790-1
5. Kim DH, Kim UJ, Kim HY, et al. Perfluoroalkyl substances in serum from South Korean infants with congenital hypothyroidism and healthy infants-Its relationship with thyroid hormones. Environ Res. 2016;147:399–404. doi:10.1016/j.envres.2016.02.037
6. Zhang J, Li Y. Risk factors for neonatal congenital hypothyroidism: aMeta analysis. Chin J Contemp Pediatr. 2021;23(05):505–512. doi:10.7499/j.issn.1008-8830.2011121
7. Bagnoli F, Farmeschi L, Nappini S, et al. Thyroid function in small for gestational age newborns: a review. J Clin Res Pediatr Endocrinol. 2013;5 Suppl 1(Suppl 1):2–7. doi:10.4274/jcrpe.846
8. LaFranchi StePhen H. Newborn screening strategies for congenital hypothyroidism: an uPdate. J Inherit Metab Dis. 2010;33:S225–S233. doi:10.1007/s10545-010-9062-1
9. Bijarnia S, Wilcken B, Wiley VC. Newborn screening for congenital hypothyroidism in very-low-birth-weight babies: the need for a second test. J Inherit Metab Dis. 2011;34(3):827–833. doi:10.1007/s10545-011-9286-8
10. Zung A, Yehieli A, Blau A, et al. Characteristics of delayed thyroid stimulating hormone elevation in neonatal intensive care unit newborns. J Pediatr. 2016;178:135–140. doi:10.1016/j.jpeds.2016.07.022
11. Lenore D, Rebecca M, Michele C, et al. Gender disparities in screening for congenital hypothyroidism using thyroxine as a primary screen. Eur J Endocrinol. 2018;179:161–167. doi:10.1530/EJE-18-0399
12. van Trotsenburg P, Stoupa A, Léger J, et al. Congenital hypothyroidism: a 2020–2021 consensus guidelines update-an ENDO-European Reference Network Initiative Endorsed by the European Society for Pediatric Endocrinology and the European Society for Endocrinology. Thyroid. 2021;31(3):387–419. doi:10.1089/thy.2020.0333
13. Iwen KA, Lehnert H. Thyroid and pregnancy. Internist. 2018;59(7):654–660. doi:10.1007/s00108-018-0435-0
14. King N, Bernardi LA. Thyroid function and pregnancy: a clinical guide to diagnosis and management.In: Thyroid Disease and Reproduction. Springer; 2019:69–78.
15. de Escobar GM, Obregon MJ, Del Rey FE. Maternal thyroid hormones early in pregnancy and fetal brain development. Best Pract Res Clin Endocrinol Metabol. 2004;18(2):225–248.
16. Williams FL, Simpson J, Delahunty C, et al. Developmental trends in cord and postpartum serum thyroid hormones in preterm infants. J Clin Endocrinol Metab. 2004;89(11):5314–5320. doi:10.1210/jc.2004-0869
17. Thorpe-Beeston JG, Nicolaides KH, Felton CV, Butler J, McGregor AM. Maturation of the secretion of thyroid hormone and thyroid-stimulating hormone in the fetus. N Engl J Med. 1991;324(8):532–536. doi:10.1056/NEJM199102213240805
18. Shields BM, Knight BA, Hill A, et al. Fetal thyroid hormone level at birth is associated with fetal growth. J Clin Endocrinol Metab. 2011;96(6):E934–E938. doi:10.1210/jc.2010-2814
19. KOrevaar TI, Chaker L, Jaddoe VW, et al. Maternal and Birth Characteristics Are Determinants of Offspring Thyroid Function. J Clin Endocrinol Metab. 2016;101(1):206–213. doi:10.1210/jc.2015-3559
20. Li J, Zhang J, Zhou Y. Risk factors for congenital hypothyroidism in neonates. Pract Prevent Med. 2022;29(06):735–737.
21. Ma W. Analysis of perinatal factors of occurrence and evolution of congenital hypothyroidism. Chin J Woman Child Health Res. 2020;31(4):470–474.
22. Zhou J, Luo J, Lin J, et al. Perinatal risk factors for congenital hypothyroidism: a retrospective cohort study performed at a tertiary hospital in China. Medicine. 2020;99(26):e20838. doi:10.1097/MD.0000000000020838
23. Mahmoud AA. Risk factors for congenital hypothyroidism in Egypt: results of a population case-control study (2003–2010). Ann Saudi Med. 2013;33:273–276. doi:10.5144/0256-4947.2013.273
24. Bliddal S, Åk R, Sundberg K, et al. Antithyroid drug-induced fetal goitrous hypothyroidism. Nat Rev Endocrinol. 2011;7:396–406. doi:10.1038/nrendo.2011.34
25. Calvo R, Morrea le De Escobar G, Escobar Del Rey F, et al. Maternal nonthyroidal illness and fetal thyroid hormone status, as studied in the streptozotocin-induced diabetes mellitus rat model. Endocrinology. 1997;138:1159–1169. doi:10.1210/endo.138.3.4997
26. Lacroix M, Battista MC, Doyon M, et al. Lower adiponectin levels at first trimester of pregnancy are associated with increased insulin resistance and higher risk of developing gestational diabetes mellitus. Diabetes Care. 2013;36(6):1577–1583. doi:10.2337/dc12-1731
27. Olivieri A, Valensise H, Magnani F, et al. High frequency of antithyroid autoantibodies in pregnant women at increased risk of gestational diabetes mellitus. Euro J Endocrinol. 2000;143:741–747. doi:10.1530/eje.0.1430741
28. Hua P, Gu Y. Relationship between gestational diabetes mellitus and thyroid dysfunction and its effect on pregnancy outcome. Mater Child Health Care China. 2018;33(22):5062–5065.
29. Li Y, Wang D, Wang C. Analysis on influencing factors of neonatal congenital hypothyroidism. Med Recapit. 2019;25(22):4556–4559.
30. Zheng X, Jiang Y, Ye J, et al. Investigation of birth defects and genetic metabolic diseases in offspring after artificial insemination with donor sperm. Guangzhou Med J. 2017;48(6):93–96. doi:10.3969/j.issn.1000-8535.2017.06.027
31. Xiao Y. Study on the growth of single fetal test tube infants within one year. J Med Inform. 2014;(14):596. doi:10.3969/j.issn.1006-1959.2014.14.733
32. Wu K, Yin L. Study on correlation between neonatal congenital hypothyroidism and birth weight and gestational age. China Pract Med. 2017;12(06):50–51.
33. Tian Q, Cui S. Dynamic variations of thyroid function and risk factors for hypothyroidism and delayed thyroid stimulating hormone elevation in late preterm infants. Chin J Perinat Med. 2021;24(05):360–365.
34. Kaluarachchi DC, Allen DB, Eickhoff JC, et al. Increased congenital hypothyroidism detection in preterm infants with serial newborn screening. J Pediatr. 2019;207:220–225. doi:10.1016/j.jpeds.2018.11.044
35. Liu C, Wang K, Guo J, et al. Small for gestational age is a risk factor for thyroid dysfunction in preterm newborns. BMC Pediatr. 2020;20(1):179. doi:10.1186/s12887-020-02089-7
36. Thorpe-Beeston JG, Nicolaides KH, Snijders RJM, et al. Thyroid function in small for gestational age fetuses. Obstet Gynecol. 1991;77(5):701–706.
37. Radetti G, Renzullo L, Gottardi E, et al. Altered thyroid and adrenal function in children born at term and Preterm, small for gestational age. J Clin Endocrinol Metab. 2004;89(12):6320–6324. doi:10.1210/jc.2003-032185
38. María B-GV, Antonio P-B, Álvaro B-B, et al. Multivariate analysis of thyrotropin in preterm newborns based on adequacy of weight for gestational age. Thyroid. 2017;27:120–124. doi:10.1089/thy.2016.0338
39. Franco B, Laura F, Sara N, et al. Altered thyroid function in small for gestational age newborns: study based on screening test for congenital hypothyroidism. J Pediatr Sci. 2010;2(4):1–9.
40. Chaudhari M, Slaughter JL. Thyroid function in the neonatal intensive care unit. Clin Perinatol. 2018;45(1):19–30. doi:10.1016/j.clp.2017.10.005
41. Kaluarachchi Dinushan C, Nicksic victoria B, Allen David B, et al. Thyroid hormone function in small for gestational age term newborns. J Pediatr. 2021;238:181–186. doi:10.1016/j.jpeds.2021.06.067
42. Giulia DD, Assunta CM, Daniela S, et al. A detailed analysis of the factors influencing neonatal TSH: results from a 6-year congenital hypothyroidism screening program. Front Endocrinol. 2020;11:456. doi:10.3389/fendo.2020.00456
43. Venugopalan L, Rajan A, Prasad HK, et al. Impact of maternal thyroid disease on neonatal thyroid status. J Pediatr Endocrinol Metabol. 2021;34(2):237–241. doi:10.1515/jpem-2020-0349
44. Ming D, Zheng R. Effects of clinical features of neonates and mothers on the screening of congenital hypothyroidism. Tianjin Med J. 2018;46(7):742–746.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.