")
Back to Journals » International Journal of General Medicine » Volume 16
Analysis of Emergency Department Use by Non-Urgent Patients and Their Visit Characteristics at an Academic Center
Authors Alnasser S , Alharbi M, AAlibrahim A , Aal ibrahim A, Kentab O, Alassaf W, Aljahany M
Received 24 September 2022
Accepted for publication 21 December 2022
Published 20 January 2023 Volume 2023:16 Pages 221—232
DOI https://doi.org/10.2147/IJGM.S391126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Woon-Man Kung
Sara Alnasser,1 Maryam Alharbi,1 Ahmad AAlibrahim,2 Ali Aal ibrahim,3 Osama Kentab,2 Wajdan Alassaf,2 Muna Aljahany1
1Department of Clinical Sciences, College of Medicine, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2Department of Emergency, King Abdullah Bin Abdulaziz University Hospital, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia; 3College of Medicine, Sulaiman Al Rajhi University, Bukairiyah, Saudi Arabia
Correspondence: Muna Aljahany, Department of Clinical Sciences, College of Medicine, Princess Nourah Bint Abdulrahman University, P.O. Box 84428, Riyadh, Saudi Arabia, Email [email protected]
Objective: We studied the extent and reasons for non-urgent emergency department (ED) visits in a single university hospital, their predictors, and patient outcomes to propose solutions suitable for Middle Eastern healthcare systems.
Design: We conducted a retrospective review of electronic medical records, including all non- and less-urgent ED visits with complete triage records (levels 4 and 5 triage based on the Canadian Triage and Acuity Scale (CTAS) over one year. The data on patient demographics, visit characteristics, and patient disposition were analyzed using SPSS software.
Setting: The study was conducted in the ED at King Abdullah Bin Abdul-Aziz University Hospital (KAAUH), a Saudi university hospital located within the campus of Princess Nourah Bint Abdulrahman University.
Participants: A chart review was carried out for 18,880 patients with CTAS 4 or 5 visiting the KAAUH ED between July 2020 and July 2021. Additionally, a total of “ 11,857” patients with missing triage acuity or CTAS levels 1, 2, or 3 were excluded from the study.
Results: The majority (61.4%) of the 30,737 ED visits were less-urgent or non-urgent. The most common reasons for non-urgent visits were routine examination/investigation (40.9%), medication refilling (14.6%), and upper respiratory tract infection/symptoms (9.9%). Most visits (73.4%) were during weekdays and resulted in the prescription of medication (94.2%), laboratory tests (62.8%), sick leaves (4.7%), radiology examinations (3.6%), and a visit to primary healthcare clinics (family medicine) within a week of the emergency visit (3.6%).
Conclusion: Less- and non-urgent ED visits often did not need any further follow-ups or admission and represented a burden better managed by a primary healthcare center. Policymakers should mitigate unnecessary ED visits through public awareness, establish clear regulations for ED visits, improve the quality of care in primary healthcare centers, facilitate booking for outpatient department appointments, and regulate the systems of payment coverage/insurance and referral by other organizations.
Keywords: emergency department, triage, non-urgent visits
Corrigendum for this paper has been published.
Introduction
Emergency departments (EDs) are designed to provide rapid, accessible, high-quality, and unscheduled care for urgent and emergency cases.1 In an ED, patients are prioritized based on triage categories, where urgent cases are admitted to the ED immediately and non-urgent cases are taken to the waiting room and are examined in turns. This triage system distinguishes urgent from non-urgent patients, and increases the quality of care for the patients who require urgent care. For over 16 years, most hospitals in Saudi Arabia have adhered to the Canadian Triage and Acuity Scale (CTAS).2 As per the CTAS, healthcare providers categorize ED patients into a five-level triage system according to their conditions. The first three levels include the cases that require resuscitation, emergent cases, or urgent cases, while the fourth and fifth levels represent the less- or non-urgent cases, respectively.2
The use of EDs by non-urgent patients has become an important public health burden both locally and globally. Such use negatively affects the quality of patient care as well as the satisfaction of patients and ED staff.3 The ultimate result is the overcrowding of patients in the ED and a longer waiting time. It also compels the ED to provide more complex and prolonged care than usual, leading to reduced care quality and an increased risk of adverse outcomes.4
Inappropriate ED visits are a global public health problem, and there are different reasons that account for these visits. For example, the patients may want rapid, convenient, and well-equipped, specialized ED services. Occasionally, the patients overestimate the urgency of their condition or are poorly aware of the scope of ED and primary healthcare center (PHCC) services. Other recognized factors found in Saudi Arabia includes the low cost of ED services, inappropriate referrals from other specialties, and overcrowding in other departments.5 Uthman et al6 revealed that 6.7–89% of ED visits are non-urgent; this large discrepancy is due to the varying definitions of non-urgent cases among researchers. Even in developed countries, such as France and the United States, there is evidence of an increase in non-urgent ED visits (44.9% and 13.7–27.1%, respectively).7,8 In Saudi Arabia, the number is as high as 78.5%.9 In contrast, individuals with regular physician visits showed a 40–67% reduction in inappropriate ED use.10–12 Thus, PHCCs, general practitioners (GPs), and family medicine specialists must play a significant role in reducing non-urgent visits. However, despite availability, the patients avoid PHCCs for reasons, such as long distance, long waiting time, difficulty in getting an appointment, and shortage of resources.10,13
Previous researchers focused mainly on non-urgent visit characteristics; however, a study conducted by Honigman et al compared non-urgent and less-urgent ED visits and found that less-urgent patients were more likely to arrive by ambulance (9%) and requested additional diagnostic investigations (91%) than non-urgent patients (6.5% and 87.8%, respectively). However, non-urgent visits were more likely to spend less than 1 h in the ED (20%) than less-urgent visits (14.7%).14
In Saudi Arabia, the citizens have access to unlimited, free medical care through a network of PHCCs throughout the country; notably, some centers are available 24/7. Citizens can also use the MAWID mobile application or the 937 call center for book appointments.15,16 Despite the continuous improvement and gradually increasing patients’ satisfaction in PHCC services,17 Saudis tend to visit EDs for healthcare services when they are sick, perceiving their condition to be serious.18,19
Previous studies have reported that a high volume of non-urgent visits is attributed to pain, upper-respiratory tract infection/symptoms, and the renewal of medication prescriptions.5,7 This study investigates non-urgent ED visits in our current local setting at an academic medical center. The primary objectives were to identify the main complaints for non-urgent ED visits and patient disposition and to compare them with less-urgent visits. We also aimed to identify the determinants of such visits.
Methods
Study Design and Setting
This retrospective study analyzed the electronic medical records of all patients who visited the Emergency Department at King Abdullah Bin Abdul-Aziz University Hospital (located within the campus of Princess Nourah Bint Abdulrahman University) from July 2020 to July 2021. Patients with a CTAS of 4 or 5 were included, and those with missing triage acuity (N=0) or CTAS levels 1 (N=17), 2 (N=361), or 3 (N=11479) were excluded from the study (N=11857), in addition to patients less than 15 years old (N=5059). The institutional review board exempt approval was obtained (log No.21-0317) before conducting the study.
The data were collected from the patients’ electronic medical records using a standardized data abstraction form that was created after reviewing similar studies.9,18
Study Protocol
The ED visits were grouped according to their CTAS levels representing patients who required resuscitation, emergent, urgent, less-urgent, or non-urgent cases based on the judgment of the triage nurse about the patient’s need for immediate evaluation, stabilization, and/or treatment. Triage 1 (resuscitation) is a severe condition in which any delay in medical attention results in death or a major trauma/medical problem. Triage 2, or emergency visit, requires evaluation within 1–14 min and immediate care to combat danger to life or limbs; any delay would result in deterioration. Triage 3 or urgent visit requires treatment within 60 min. Triage 4, or less-urgent visit, must be evaluated between 1 and 2 h. A triage 5, or non-urgent visit, represents conditions where a delay of up to 24 h would make no appreciable difference to the clinical condition, and subsequent referral may be made to the appropriate alternative specialty.
The patient-level characteristics, including age, sex, past medical history, employment status, and residential distance from the hospital (in/out campus) were analyzed. Additionally, the following data were collected: arrival time, day of arrival (weekend or weekday), mode of arrival, CTAS level, chief complaint, duration of complaint, period of stay in the ED, and primary clinic visits on the same day. We included consultations with other specialties, final diagnosis, prescribed medication, sick leave, and case disposition (discharge, referral, or admission) as the visit outcomes.
Statistical Analysis
The categorical data are presented as frequencies and percentages, whereas the continuous data are presented as median and interquartile range (due to non-normal distributions). The demographic and emergency visit characteristics, as well as diagnosis and complaints of the patients, were compared among the CTAS groups (less-urgent and non-urgent). The chi-square or Fisher’s exact test, as appropriate, was used to examine the differences in categorical variables, while the t-test was used to examine differences in continuous variables. To detect potential predictors of non-urgent visits, multivariate logistic regression analysis model was run after adjusting for the variables shown in Table 1 (demographic and visit characteristics) and 3 (diagnoses). Backward elimination was used to allow non-significant variables to leave the model. All P-values were two-tailed. Statistical significance was set at P<0.05. SPSS (version 25.0; IBM Corp., Armonk, NY, IBM Corp) was used for all statistical analyses.
 |
Table 1 Demographic and Emergency Visit Characteristics by CTAS Levels (N = 18,880) |
Results
Demographic Characteristics of Patients (Less- and Non-Urgent Cases)
As shown in Figure 1, as per the CTAS, of the 30,737 patients who visited the ED, 17 (0.1%) were classified as requiring resuscitation, 361 (1.2%) as emergent, 11,479 (37.3%) as urgent, 17,338 (56.4%) as less-urgent, and 1542 (5.0%) as non-urgent. Resuscitation, emergent, and urgent patients were excluded (N=11857); CTAS 4 and 5 patients were the focus of this study, leaving 18,880 patients for further analyses.
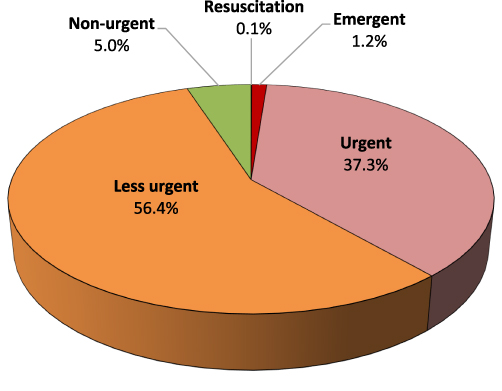 |
Figure 1 CTAS classification of patients visiting the ED (N = 30,737). |
Table 1 shows the demographic and emergency visit characteristics based on the CTAS levels. The presented descriptive data show less-urgent and non-urgent ED visits. Approximately 63.2% of non-urgent patients were women. The median (IQR) age was 27 (13–38) years, with the majority of the patients aged between 16 and 35 years (44.2%), followed by those between the ages of 36 and 65 years (37.7%), children up to 15 years (15.8%), and those above 65 years (2.3%). Almost half of the patients were married (49.3%), while the remainder were either single (48.2%) or divorced/widowed (2.5%). The majority of patients were of Saudi nationality (80.9%). The most common non-Saudi nationalities were Arab in origin (10.0%) and Southeast Asian (6.9%). The most frequent health plan providers (service payers) were Princess Nourah Bint Abdulrahman University (PNU, 36.3%), King Abdullah Bin Abdulaziz University Hospital (KAAUH; 29.5%), ED (22.6%), and referred patients (9.1%). The majority of the visits were from Sunday to Thursday (73.4%), whereas 26.6% were on weekends (Friday to Saturday). The median (IQR) time to triage was 2 (1–7) minutes, with the majority (66.1%) of visits lasting between 0 and 5 min. The median (IQR) length of stay was 1 (1–3) hours, with the majority (77.4%) of visits lasting 2 hours or fewer.
A univariable analysis indicated that, compared with less-urgent visits, non-urgent visits were associated with distinct demographic characteristics, such as older age, being married, and being non-Saudi (P<0.001). Significantly higher proportions of non-urgent visits occurred in patients whose treatment expenses were covered by KAAUH or the ED (P<0.001) and for patients who visited during weekends (P=0.049). Non-urgent cases had a longer duration before triage and a shorter length of hospital stay than less-urgent cases (P<0.001 for both; see Table 1).
Outcomes of Less- and Non-Urgent Emergency Visits
As shown in Figure 2, the main outcomes of non-urgent emergency visits were prescription medications (94.2%), performing laboratory tests (62.8%), obtaining sick leave (4.7%), performing a radiology examination (3.6%), and visiting PHCCs (family medicine) within a week of the emergency visit (3.6%). Very few (1.3%) non-urgent emergency visits ended up in outpatient department (OPD) referral (0.1%), consultation (0.3%), admission (0.4%), or visiting the PHCC on the same day (0.5%).
 |
Figure 2 Outcomes of non-urgent visits to the ED (N = 1542). |
Table 2 shows the outcomes of emergency visits based on the CTAS levels. Compared with less-urgent cases, a lower proportion of non-urgent cases were prescribed medication (P<0.001), underwent a radiology examination (P<0.001), received a consultation (P<0.001), or received a sick leave (P<0.001). A lower proportion of non-urgent patients were hospitalized (P=0.001), and they did not visit a PHCC within one week of the ED visit (P=0.002). However, laboratory testing was performed for a significantly higher proportion of non-urgent patients compared to less-urgent patients (P<0.001; Table 2).
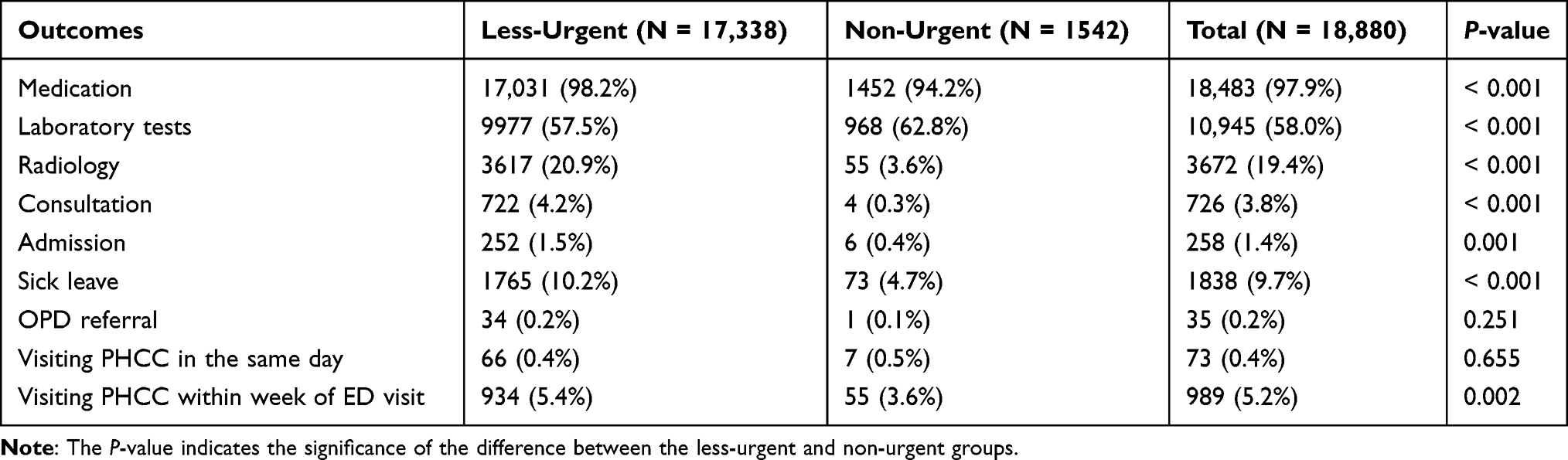 |
Table 2 Outcomes of Emergency Visits by CTAS Levels (N = 18,880) |
Clinical Presentation and Diagnosis of Less-Urgent and Non-Urgent Cases at the ED
As shown in Figure 3, the main reasons for non-urgent emergency visits included routine examinations and investigations (40.9%); medication refills (14.6%); upper-respiratory infections/symptoms (9.9%); skin and allergic problems (4.8%); non-specific symptoms (4.0%); ear, nose, and throat infection/problems (3.6%); headaches and migraines (3.3%); musculoskeletal/joint pain and bone fractures (3.2%); injury, trauma, and falls (2.3%); other infections (2.3%); eye problems (2.1%); and other diagnoses/complaints.
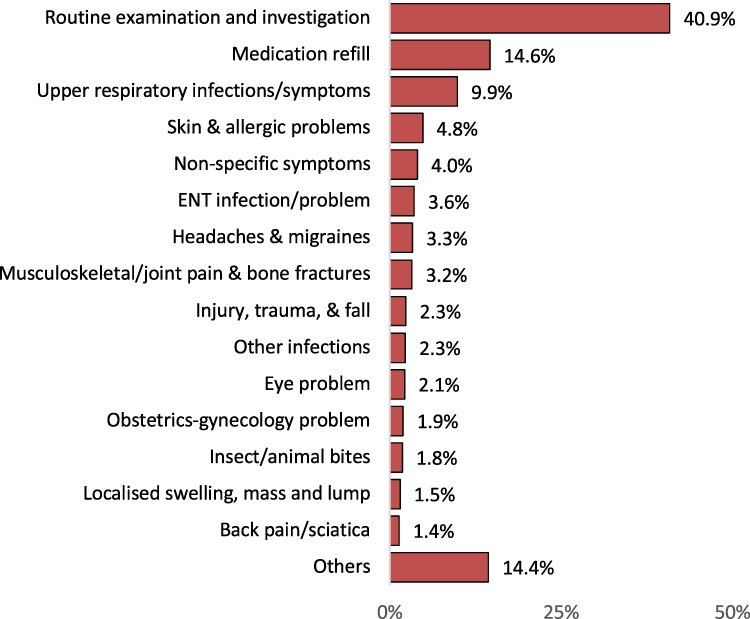 |
Figure 3 Most common diagnoses and complaints among non-urgent patients visiting the ED (N = 1542). |
Table 3 shows the diagnoses during emergency visits based on the CTAS levels. Compared with less-urgent visits, non-urgent visits were associated with higher proportions of a single diagnosis, routine examination and investigation, medication refill, insect/animal bites, wound care, and fatigue and malaise (P<0.001 for all, except fatigue and malaise). Conversely, non-urgent visits were associated with lower proportions of multiple presentations, such as upper respiratory infections/symptoms, abdominal pain/acute abdomen, non-specific chest discomfort/acute cardiac problems, headaches/migraines, and renal problems (P<0.001). Table 3 provides additional details about the differences between non-urgent and less-urgent visits in terms of presenting conditions/diagnoses.
 |
Table 3 Diagnoses During Emergency Visit by CTAS Levels (N = 18,880) |
As shown in Table 4, demographic and emergency visit characteristics that were independently predicting non-urgent visits included older age, higher number of minutes to triage, and payers who were covering referred or other patients. Diagnoses that independently predict non-urgent visits included (in descending order) medication refill, counselling, examination, investigation, and follow-up, wound care, insect/animal bites, non-specific diagnosis, and upper respiratory infections/symptoms. All other diagnoses remaining in Table 4 were independent predictors of less-urgent rather than non-urgent visits. These included (but not limited to) high/low blood pressure, back pain/sciatica, syncope, dizziness, and vertigo, renal problem, constipation, palpitations/arrhythmia, abdominal pain/acute abdomen, urinary tract infections/symptoms, fever, injury, trauma, and fall.
 |
Table 4 Multivariate Logistic Regression Analysis of Potential Predictors of Non-Urgent Visits |
Discussion
Patients tend to visit the ED for immediate attention so that hospital staff can perform tests and administer medications to relieve symptoms immediately. Misuse of ED places a significant burden on the health system and increases the demand of the ED, which can be managed better at other levels. More importantly, it intuitively competes with actual cases requiring emergency care.10
In our study, 61.4% of the patients who visited the ED presented as less-urgent or non-urgent cases; their visit purposes included routine examination or investigation, refilling of prescriptive medication, and upper-respiratory symptoms, all of which could be addressed by PHCCs. This result is in agreement with that of previous studies that focused on hospitals within and outside Saudi Arabia, revealing that CTAS 4 and 5 cases accounted for 64.9% of ED visits.4 Studies conducted in other countries also showed relatively similar results, with 6.7–89.0% of ED visits triaged as CTAS 4 and 5 in the UK and one-third of visits in Iran.1,6
Our results indicate that a high proportion of ED visitors were women; a systematic review of inappropriate use of emergency services found that women have higher odds of inappropriately visiting the ED, with a rate varying from 1.12 to 1.56.10 However, our findings can be justified by the fact that the data were collected from a hospital located within the women’s university campus.
Individuals between 16 and 35 years of age were found to frequently visit the ED in both CTAS levels; this result agrees with Al-Otmy’s study on western Saudi Arabia and Hsia and Niedzwiecki’s multi-ethnic study focused on Florida, US.9,20
Furthermore, we found that Saudi citizens visited the ED more than citizens of other nationalities. This may be because of the Saudi setting and the fact that KAAUH is considered an educational hospital where treatment can be provided to non-Saudis with limited eligibility. Patients who visited the ED were usually employees of Princess Nourah Bint Abdulrahman University and the KAAUH. Hence, these services may be more feasible and accessible to employees; however, referrals accounted for 15.8% of the ED visits. Most ED visits (73.4%) occurred during weekdays. The mean time spent in the ED for patients with CTAS 4 and 5 were 1 (1–3) and 1 (0–2) hours, respectively, compared with a previous study that measured these values at 2.2 (1.3–3.5) and 2.0 (1.2–3.3), respectively,14 indicating the propensity for non-significant complaints.
The main purposes of non-urgent ED visits were prescription medication and laboratory tests. This finding is consistent with that of Honigman et al, who reported that 76% and 53% of non-urgent patients received medication and diagnostic/screening services, respectively.14 Al-Otmy et al found that in addition to laboratory investigations, which were conducted for the majority of cases, imaging studies were ordered for more than half of non-urgent ED visiting patients.9 However, in our study, only a small percentage (3.6%) of the non-urgent patients required imaging studies. Furthermore, there was a minimal need for admission (0.4%), consultation (0.3%), or OPD referral (0.1%) among non-urgent patients. This result confirms the lack of urgency in these visits, as these patients required no follow-up or admission and could have been serviced by a PHCC.
We further buttress our results by referring to earlier studies that show that ED visits are convenient because they require no appointments. Difficulty in reserving an OPD appointment could be related to the patient’s own schedule, such as the need to book a same-day visit or the inaccessibility of electronic devices required for booking.5,18 Second, patients find ED services to be convenient and trustworthy, which increases the number of non-urgent ED visits.7,10,18 However, expanding services, increasing business hours, and hiring more health professionals in primary care have not substantially reduced inappropriate ED use.10,21,22 Honigman et al suggested that the ED may be an appropriate site of service for non-urgent presentation or complaints if there are no other available sites to provide timely care to the patient.14 Based on our results, we suggest that hospitals should provide a separate section within the ED for less-urgent and non-urgent complaints. Such a service can be managed by a GP or family physician, thus ensuring timely care without compromising ED services. This may be especially effective given that GPs are known to manage patients under more resource constraints than standard care in the ED without increasing the re-attendance rate.6
The preference for ED visits by patients rather than primary care settings can be perceived from a dual perspective. On the one hand, a considerable proportion of patients trust the clinical services provided by emergency physicians. However, there are significant gaps in the physician–patient communication in PHCCs.23 As a result, patients find it more convenient to visit the ED. These challenges could potentially be resolved by improving communication and raising patient awareness regarding the roles of GPs and family physicians.
Similarities were observed between CTAS 4 and 5, including middle-aged women (16–35 years) who had the highest ED visits, aside from an increase in visits during the weekdays, with a frequent outcome of medication dispenses.
Notably, sick leave was not an important factor that encouraged non-urgent visits to the ED; only 4.7% of the patients with CTAS 4 and 5 received sick leave. However, since we analyzed only secondary data (chart review), it is unclear whether the patients requested for such leave only to be rejected by a physician.
Finally, routine examination/investigation and medication refilling were the most common reasons for non-urgent ED visits (40.9% and 14.6%, respectively), followed by upper respiratory tract infections/symptoms (9.9%). However, Carret et al found that during non-urgent visits, the chief diagnosis or complaint was respiratory problems, along with digestive problems, abdominal pain, and chest pain.10 As these complaints are not urgent and can be diagnosed by the OPD staff, the patients need to be educated on the proper use of healthcare services and improving pathways and access to other primary healthcare settings that are more suitable for low acuity treatment. With increased access and options, burden on EDs would likely not be as high.
Limitations and Strengths
This study is limited by its retrospective design that analyzed the electronic medical records of all patients who visited the KAAUH ED. The use of a retrospective chart review for patients’ final diagnoses may not be correlated with their chief complaint or primary triage level.
This study was also conducted during the COVID-19 pandemic between July 2020 and July 2021, based on the fact that it may not reflect the pattern of regular ED visits. However, the selected time period of the study was after the peak of the pandemic in Saudi Arabia.
The generalizability of this study could be limited because this single-center study was conducted at a hospital within a women’s university. In addition, more comparisons and further statistical tests should be performed in follow-up studies. CTAS was used to triage ED visitors subjectively according to the judgment of the triage nurse. However, the results of this study may be used to develop policies for the appropriate use of primary healthcare centers.
Conclusion
We conclude that non-urgent ED visits, which usually do not need any further follow-up or admission, are a burden on the EDs and compete with cases that require urgent intervention. This will result in overcrowding of patients in the ED and a longer waiting time. Which will negatively affect the quality of patient care as well as the satisfaction of patients and ED staff. These non-urgent visits can be effectively managed in patients with PHCC. Hence, we urge policymakers to implement effective strategies to raise public awareness regarding the proper use of EDs, set clear rules and regulations for ED visits, improve the quality of care in PHCCs, facilitate booking for OPD appointments, and regulate the systems of payment coverage/insurance and referral by other organizations. It is also necessary to improve the quality of care in PHCCs and to emphasize the significant role of family physicians in patient care. Our most important recommendation is to establish special services within the ED that can be managed by GP or family physicians. Such a service could provide non-urgent patients with the necessary dedicated services outside the available OPD services, without compromising ED care.
Data Sharing Statement
The data are available upon reasonable request.
Ethical Approval
Ethical approval was obtained from the Princess Nourah Bint Abdulrahman University Institutional Review Board. The study granted a waiver for informed consent (log No.21-0317) as the data were collected anonymously as collective numbered information without distinct patient identifiers. The current study complies with the Declaration of Helsinki.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This research did not receive any funding.
Disclosure
The authors declare that there are no conflicts of interest.
References
1. Bahadori M, Mousavi SM, Teymourzadeh E, Ravangard R. Non-urgent visits to emergency departments: a qualitative study in Iran exploring causes, consequences and solutions. BMJ Open. 2020;10(2):e028257. doi:10.1136/bmjopen-2018-028257
2. Alquraini M, Awad E, Hijazi R. Reliability of Canadian Emergency Department Triage and Acuity Scale (CTAS) in Saudi Arabia. Int J Emerg Med. 2015;8:1. doi:10.1186/s12245-015-0080-5
3. Idil H, Kilic TY, Toker İ, Dura Turan K, Yesilaras M. Non-urgent adult patients in the emergency department: causes and patient characteristics. Turk J Emerg Med. 2018;18(2):71–74. doi:10.1016/j.tjem.2017.10.002
4. Bakarman M, Njaifan N. Assessment of non-emergency cases attending emergency department at King Fahad general hospital, Jeddah: pattern and outcomes. Life Sci J. 2014;11:20–25.
5. Alyasin A, Douglas C. Reasons for non-urgent presentations to the emergency department in Saudi Arabia. Int Emerg Nurs. 2014;22(4):220–225. doi:10.1016/j.ienj.2014.03.001
6. Uthman OA, Walker C, Lahiri S, et al. General practitioners providing non-urgent care in emergency department: a natural experiment. BMJ Open. 2018;8(5):e019736. doi:10.1136/bmjopen-2017-019736
7. Şimşek P, Gürsoy A. Turkish health care providers’ views on inappropriate use of emergency department: who, when and why? Int Emerg Nurs. 2016;27:31–36. doi:10.1016/j.ienj.2015.11.004
8. Williams CA, Haffizulla F. Factors associated with avoidable emergency department visits in Broward County, Florida. Cureus. 2021. doi:10.7759/cureus.15593
9. Al-Otmy SS, Abduljabbar AZ, Al-Raddadi RM, Farahat F. Factors associated with non-urgent visits to the emergency department in a tertiary care centre, western Saudi Arabia: cross-sectional study. BMJ Open. 2020;10(10):e035951. doi:10.1136/bmjopen-2019-035951
10. Carret MLV, Fassa ACG, Domingues MR. Inappropriate use of emergency services: a systematic review of prevalence and associated factors. Cad Saude Publica. 2009;25:7–28. doi:10.1590/S0102-311X2009000100002
11. Stein A. The relevance of continuity of care: a solution for the chaos in the emergency services. Fam Pract. 2002;19(2):207–210. doi:10.1093/fampra/19.2.207
12. Petersen LA, Burstin HR, O’Neil AC, Orav EJ, Brennan TA. Nonurgent emergency department visits. Med Care. 1998;36(8):1249–1255. doi:10.1097/00005650-199808000-00012
13. Dawoud SO, Ahmad AMK, Alsharqi OZ, Al-Raddadi RM. Utilization of the emergency department and predicting factors associated with its use at the Saudi ministry of health general hospitals. Glob J Health Sci. 2015;8(1):90. doi:10.5539/gjhs.v8n1p90
14. Honigman L, Wiler J, Rooks S, Ginde A. National study of non-urgent emergency department visits and associated resource utilization. West J Emerg Med. 2013;14(6):609–616. doi:10.5811/westjem.2013.5.16112
15. Ministry of Health. E-Services: (Mawid) Service: MOH; 2021. Available from: https://www.moh.gov.sa/en/eServices/Pages/cassystem.aspx.
16. Ministry of Health. Interactive Map: MOH; 2021. Available from: https://www.moh.gov.sa/en/eServices/interactive-maps/Pages/default.aspx#/.
17. Alanzi TM, Althumairi A, Aljaffary A, et al. Evaluation of the Mawid mobile healthcare application in delivering services during the COVID-19 pandemic in Saudi Arabia. Int Health. 2021. doi:10.1093/inthealth/ihab018
18. AlOmar RS, AlShamlan NA, AlAmer NA, et al. Perceived barriers to primary care services utilization and its associations with overall satisfaction of patients in Saudi Arabia: a cross-sectional questionnaire-based study. J Prim Care Community Health. 2021;12:215013272110140. doi:10.1177/21501327211014065
19. El Bcheraoui C, Tuffaha M, Daoud F, et al. Access and barriers to healthcare in the Kingdom of Saudi Arabia, 2013: findings from a national multistage survey. BMJ Open. 2015;5(6):e007801. doi:10.1136/bmjopen-2015-007801
20. Hsia RY, Niedzwiecki M. Avoidable emergency department visits: a starting point. Int J Qual Health Care. 2017;29(5):642–645. doi:10.1093/intqhc/mzx081
21. Roberts E, Mays N. Can primary care and community-based models of emergency care substitute for the hospital accident and emergency (A & E) department? Health Policy. 1998;44(3):191–214. doi:10.1016/s0168-8510(98)00021-9
22. van Uden CJT. Does setting up out of hours primary care cooperatives outside a hospital reduce demand for emergency care? Emerg Med J. 2004;21(6):722–723. doi:10.1136/emj.2004.016071
23. Elagi AAA, Jaber BA, Wassly AHA, Ahmed RMS, Bosily FAA. Public’s perception and satisfaction on the role and services provided by family physicians in Saudi Arabia: a cross-sectional study. J Family Med Prim Care. 2019;8(10):3282–3286. doi:10.4103/jfmpc.jfmpc_621_19
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.