")
Back to Journals » International Journal of General Medicine » Volume 16
Analysis of Echocardiographic Findings of Patients with Acute Ischemic Stroke Admitted to a Tertiary Care Hospital in Mogadishu, Somalia
Authors Hassan MS , Mire Waberi M, Osman Sidow N , Hassan MO , Akyüz H, Ahmed Abdi I , Bashir AM , Abdirahman Ahmed S
Received 30 March 2023
Accepted for publication 3 July 2023
Published 7 July 2023 Volume 2023:16 Pages 2887—2895
DOI https://doi.org/10.2147/IJGM.S414014
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Mohamed Sheikh Hassan,1 Mohamud Mire Waberi,2 Nor Osman Sidow,1 Mohamed Omar Hassan,2 Hakan Akyüz,2 Ishak Ahmed Abdi,2 Ahmed Muhammad Bashir,3 Said Abdirahman Ahmed2
1Department of Neurology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 2Department of Cardiology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia; 3Department of Internal Medicine, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia
Correspondence: Mohamed Sheikh Hassan, Department of Neurology, Mogadishu Somali Turkish Training and Research Hospital, Mogadishu, Somalia, Email [email protected]
Background and Aims: The etiological investigation of the potential cardiac source of acute ischemic stroke is important for the secondary prevention of recurrent and future embolization. Transthoracic echocardiography is one of the most useful investigations for the assessment of the potential cardiac etiology of ischemic stroke. Our aim is to evaluate echocardiographic findings in patients with acute ischemic stroke admitted to a tertiary care hospital in Mogadishu, Somalia.
Methods: This was a retrospective observational study conducted in the neurology department of a tertiary care hospital in Mogadishu, Somalia. We enrolled 315 patients with acute ischemic stroke admitted to the hospital who had undergone transthoracic echocardiography between March 2019 and March 2022. We analyzed transthoracic echocardiography findings, ischemic stroke subtypes, and their associated comorbidities. We also compared the demographic data, comorbidity, and survival status of patients with abnormal echo findings to those with normal echo findings.
Findings: The mean age of patients was 62± 12 years. Co-morbidities were present in about 251 (80%) of the subjects, hypertension was the most common comorbidity 99 (31.4%), followed by diabetes 72 (23%), and hyperlipidemia 37 (11.7%). Overall cardiac pathology in this study was 170 (54%). Forty-seven (15%) of the patients had low ejection fraction on transthoracic echocardiography. Male patients had slightly less left ventricular systolic dysfunction than female patients. 100 (32%) had left ventricular diastolic dysfunction (LVDD), while 113 (36%) had left ventricular hypertrophy (LVH). Patients with hypertension and diabetes had more echo abnormalities compared to others (P-values of 0.047 and 0.024, respectively). More abnormal echo findings were seen in patients who died during hospitalization than in those who survived (P = 0.008). Severe left ventricular systolic dysfunction was associated with higher mortality (P < 0.001).
Conclusion: Most patients with stroke in this study had abnormal echocardiograms; however, only a few had cardioembolic strokes. Abnormalities in echocardiography were more common in patients who died during hospitalization than in those who survived.
Keywords: acute ischemic stroke, cardiac dysfunction, echocardiography
Introduction
Stroke causes significant mortality and morbidity worldwide and is the third-largest cause of mortality in the developed world. Ischemic stroke represents 85% of all forms of stroke.1 Cardiovascular abnormalities are common in patients with acute ischemic stroke, and they are one of the main causes of stroke mortality. Cardiac abnormalities can cause an acute ischemic stroke through an embolic event.2
Transthoracic echocardiography (TTE) is a useful tool that can be used to diagnose cardiac disorders that may have caused embolism, such as apical hypokinesia, atrial or ventricular thrombus, atrial fibrillation, and heart failure.3–5 These conditions can be managed to prevent cerebrovascular disorders (CVDs) and reduce morbidity and mortality. Transthoracic echocardiography can also be used to diagnose other etiologies of stroke that may need intervention, including patent foramen ovale, atrial septal defect, atrial myxoma, and infective endocarditis.6,7 Reduced left ventricular ejection fraction and left ventricular diastolic dysfunction are known risk factors for cerebrovascular disorders in patients with acute ischemic stroke.8,9 When a patient with an acute ischemic stroke (AIS) is first admitted, a transthoracic echocardiography evaluation should be performed to identify the possibility of a cardiac source of embolism as the cause of the ischemic stroke. Early recognition and treatment of risk factors for future CVD after acute ischemic stroke is clinically essential for enhancing the patient’s prognosis and also preventing future risks of CVD.10 Since TTE is noninvasive and gives detailed information on the structures and functioning of the heart, it should be used for risk stratification in patients with AIS to prevent possible future CVDs.
Our study’s goal is to analyze the echocardiographic results of AIS patients who were admitted to the neurology department of our hospital in order to ascertain how frequently potential pathologic cardiac findings were seen on transthoracic echocardiogram for secondary stroke prevention as well as to pinpoint circumstances in which echocardiography may be highly or minimally useful.
Methodology
The study was a retrospective observational study conducted in the neurology department of Mogadishu-Somalia Turkish Training and Research Hospital. The study focused on the assessment of echocardiographic findings in patients with acute ischemic stroke admitted to the neurology ward and intensive care unit. The data was retrieved from the electronic records of patients admitted to the neurology department due to an acute ischemic stroke. Patients with acute ischemic stroke who had undergone transthoracic echocardiography from March 2019 to March 2022 were enrolled.
Acute ischemic stroke was defined according to the International Diagnostic Criteria:11 development of new-onset lateralizing/focal neurologic signs or changes in mental status; identification of acute lateralizing/focal neurologic deficits by consultant neurologists, and neuroimaging evidence of acute ischemic stroke (non-contrast brain CT, or brain MRI including diffusion sequences) within 48 hours of neurologic deficits. Stroke severity was assessed using the NIHSS score (National Institute of Health Stroke Scale). Anatomic locations of infarct were classified into middle cerebral artery (MCA) territory, anterior cerebral artery (ACA) territory, vertebrobasilar territory, and lacunar infarct (based on clinical/radiological assessment). A total of 315 patients diagnosed with acute ischemic stroke admitted to the neurology department had undergone transthoracic echocardiography within 24 hours of admission.
Two of the authors (M.S.H. and M.M.W.) retrieved the following data from the patients’ medical records: demographic data of the patients, including age and gender, ischemic stroke subtype and severity, admission status; and intrahospital mortality. The retrieved data also included history of previous ischemic stroke or transient ischemic attacks, prior history of atrial fibrillation, medication history, discharge summary, and echocardiogram findings (atrial diameter, left ventricular functional status, LVID (ed), valvular abnormalities, LVID (es), intra-atrial and intraventricular wall pathologies, presence of pulmonary hypertension, pericardial thickness and effusion, LVDD, LVH, presence of wall motion abnormality, and presence of intracardiac thrombus).
The patients were divided into those with segmental contractility abnormalities (patients with present vs absent contractility dysfunction), ejection fraction (EF) <40% Vs ≥40%, left atrial size (LA ≤ 40 mm vs > 40 mm), left ventricular end-diastolic dimension (EDD 56 mm vs 56 mm), mitral regurgitation severity (MR 2–3), mitral stenosis severity (mild, moderate, and severe), aortic stenosis severity (mild, moderate, and severe), aortic regurgitation (AR1-3), LVDD (normal, grade 1–3) and LVH (mild, moderate, and severe).
According to American Society of Echocardiography guidelines, LV measures were taken at end-diastole and end-systole, and each parameter’s value was averaged across three cardiac cycles. The ventricular septal thickness at end-diastole (VSTd), LV internal diameter at end-diastole (LVTDd) and end-systole, and the posterior wall thickness at end-diastole (PWTd) parameters were evaluated.12 The transmitral Doppler flow velocities, mitral annular e′ velocity, E/e′ ratio, peak velocity of the TR jet, and LA maximum volume index were used for the assessment of left ventricular diastolic dysfunction (LVDD). Results from echocardiograms were taken from final reports written by a cardiologist with echocardiography training.
Statistical Analysis
Continuous variables are represented by means and standard deviations; frequencies and percentages were used to illustrate categorical variables. The Pearson chi-square test was used for the evaluation of categorical data. A P value of <0.05 was considered statistically significant. SPSS software version 26 was used to conduct the statistical analysis.
Ethical Approval
The study was reviewed and accepted by the ethics committee of Mogadishu Somali Turkish Training and Research Hospital (Ethics Protocol No: MSTH/9571). Due to the fact that our hospital is a research and training hospital. An informed consent is taken from every patient/caregiver before admission to use their data without disclosing their names for research purposes. In addition, as per our hospital protocol, informed consent is waived for retrospective studies as long as patients’ data are not disclosed. The study complies with the Declaration of Helsinki, and this research did not receive any specific funding.
Results
The echocardiographic findings of 315 acute ischemic stroke patients admitted to the neurology department of the hospital were analyzed. All patients underwent transthoracic echocardiography. The mean age of patients was 62±12 years. The majority of the patients in the study were 60 years of age or older 210 (66.7%). The male subjects in the study population.
Accounted 178 (56.5%), while females accounted for 137 (43.5%). Co-morbidities were present in about 251 (80%) of the subjects. Hypertension was the most common comorbidity 99 (31.4%), followed by diabetes 72 (23%), and hyperlipidemia 37 (11.7%). Other comorbidities were previous stroke, heart disease, respiratory disease, cancer, and thyroid disorders (see Table 1). Hypertension, diabetes, stroke, and heart diseases were more prevalent with increasing age (see Table 2). Diabetes, hypertension, and hyperlipidemia were slightly more prevalent among male patients, while other comorbidities were equally distributed among patients (see Figure 1).
 |
Table 1 Shows Patients’ Related Features |
 |
Table 2 Findings of Transthoracic Echocardiography |
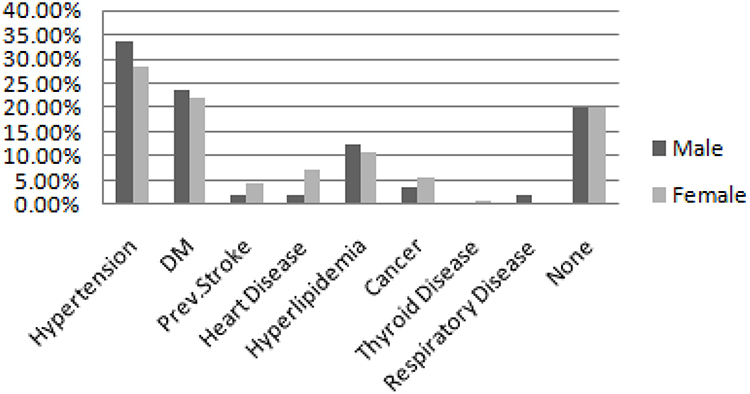 |
Figure 1 Shows distribution of comorbidities versus gender of the patients. |
Regarding echocardiographic findings, the study showed 4% of the patients had right atrial dilation, 8% had left atrial dilatation, and 2% had aortic root dilatation. Patients over 60 years of age and female patients had a higher proportion of left atrial dilatation. 47 (15%) of the patients had low ejection fraction on transthoracic echocardiography. Male patients had slightly less left ventricular systolic dysfunction than female patients. Low ejection fraction was not associated with a particular comorbidity (P = 0.156). Mitral valve disease was present in 72 (23%) of the patients, 53 (17%) of the patients had tricuspid valve abnormality, while 41 (13%) of the patients had an abnormal aortic valve, with AR1 being the most common pathologic finding (see Table 3). Only two patients had pulmonary valve disease. Eight (2.5%) of the patients had atrial septal defect, while 1(0.3) had VSD. Twenty-nine (10%) had been associated with pulmonary hypertension. Ten (3%) had pericardial effusion. One hundred (32%) had LVDD while 113 (36%) had LVH. Left ventricular hypertrophy was more frequent in hypertensive patients (46% of hypertensive patients). Left ventricular diastolic dysfunction (LVDD) was more common among diabetic patients (60% of diabetic patients). 30 (9.5%) had wall motion abnormality. 15 (4.8%) of the patients had intracardiac thrombus. Overall cardiac pathology in this study was 54%.
 |
Table 3 Distribution of Comorbidities Among Different Age Groups |
As shown in Table 4, gender was not a significant factor for abnormal echo findings. Patients with hypertension and diabetes had more echo abnormalities compared to others (P-value of 0.047 and 0.024 respectively). More abnormal echo findings were seen in patients who died during hospitalization than in those who survived (P = 0.008). Intrahospital mortality was higher in patients with severe left ventricular dysfunction, patients with wall motion abnormalities, and patients with severe pulmonary hypertension. Of these, severe left ventricular dysfunction had the most significant association with intrahospital mortality (P < 0.001).
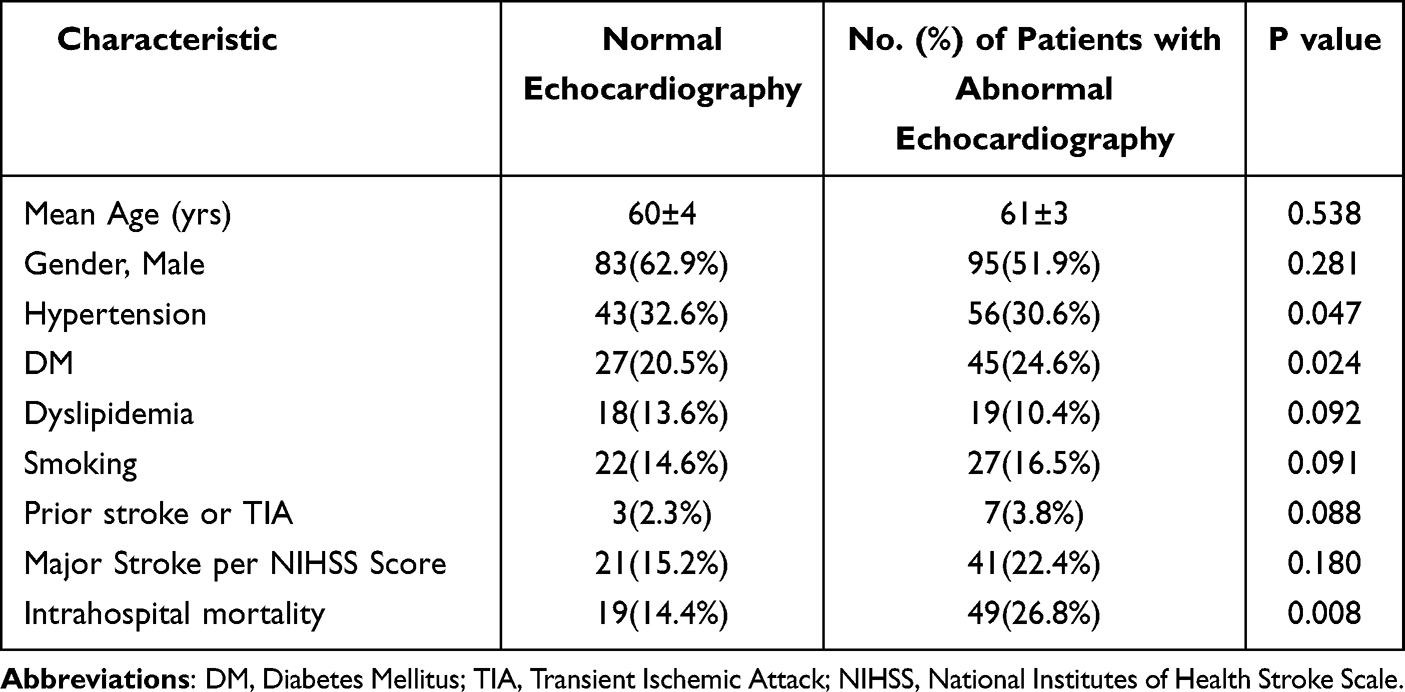 |
Table 4 Characteristics of Patients in Terms of Echo Findings |
The echocardiogram is useful for shaping the management of ischemic stroke with the aim of preventing potential future recurrent strokes. Twenty-four (7.6%) of the patients with acute ischemic stroke had their management strategies changed following their echocardiogram findings. Patients with intracardiac thrombus and those patients with cardiac wall motion abnormalities were the most patients whose medical management strategies were changed.
Discussion
In high-income countries, stroke is the third leading cause of death and causes serious morbidity in survivors.13,14 The main cause of an ischemic stroke is a thrombotic or embolic event, and emboli frequently come from the heart.15 Few patients with stroke or TIA had clinically actionable echocardiography findings for subsequent stroke prevention, whereas the majority of patients with stroke or TIA had normal echocardiograms. Patients with a cryptogenic stroke had a higher frequency of clinically useful findings, particularly PFO.16 Similar to transesophageal echocardiography (TEE), transthoracic echocardiography (TTE) with agitated saline can identify PFOs. Therefore, agitated saline was given to those suspected of having a patent foramen ovale or even dropping out.17
Transthoracic echocardiography can also spot other stroke etiologies that could need intervention, such as atrial anomalies (like a patent foramen ovale or an atrial myxoma) or infected endocarditis.6,18,19 The most frequent cause of cardio-embolic events is a thrombus in the left atrium (LA) or, more commonly, the LA appendage (LAA), which is frequently linked to atrial fibrillation. The risk of thromboembolism is comparable for paroxysmal and persistent AF. However, it is heavily influenced by related cardiovascular risk factors.20 Echocardiography is crucial for identifying other embolic heart conditions after an ECG, which can detect atrial fibrillation, which accounts for 50% of cardioembolic strokes.21 The degree of LA enlargement and, subsequently, the chance of AF-associated thrombus development are influenced by the severity and duration of these risk factors. Clinical prediction tools like CHADS2 and CHA2DS2-VASc scores can be used to stratify stroke risk.22 Patients with ejection fractions below 40%, anterior wall MI, and LV aneurysms had a higher risk of developing an LV thrombus.23,24
Left ventricular (LV) thrombus development due to stasis brought on by localized or systemic cardiac dysfunction is most often linked to myocardial infarction (MI) and dilated cardiomyopathy (DCM). Between 1% and 2.5% of patients with acute MI get stroke within 4 weeks, with 50% happening during the first 5 days.25,26
TEE is more sensitive than TTE for most other therapeutically important diseases, with the exception of left ventricular thrombus (LVT).15 As such, the left ventricular thrombus is used in routine normal echocardiography for those suspected of having an intracardiac thrombus.27
Acute ischemic stroke, which can appear in up to 40% of these patients, is the most frequent neurological consequence in the context of IE, occurring in 25–70% of cases. Despite the fact that IE only accounts for less than 10% of all cardioembolic strokes and is a very infrequent stroke risk factor due to its low global incidence, there is a strong correlation between IE and subsequent stroke.28 Mitral stenosis-related thromboembolism presents in 10% of all ischemic strokes and 50% of all cardioembolic strokes. Stroke incidence is higher in mitral stenosis patients with a history of AF, DM, male sex, HTN, hyperlipidemia, and obesity.29,30 The clinical implications of LV diastolic dysfunction are significant. Exercise intolerance is a common symptom of LV diastolic dysfunction.31 Even in asymptomatic subjects, LV diastolic dysfunction has been linked to the development of heart failure, future cardiovascular events, and increased mortality, even after controlling for comorbidities.32,33 In our echocardiography assessment, left ventricular diastolic dysfunction was the most common finding among the assessed variables.
Hypertensive left ventricular hypertrophy (LVH) is an early manifestation of cardiovascular target organ damage in patients with arterial hypertension and those patients with acute ischemic stroke (AIS) or transient ischemic attack (TIA). Since hypertensive left ventricular hypertrophy (LVH) is common, these patients need more rigorous therapy as they are at a greater risk of stroke. To ensure that these patients are managed as effectively as possible, transthoracic echocardiography (TTE) should be performed on all AIS and TIA patients.34,35
Although pulmonary hypertension (PH) was associated with a longer hospital stay and an unfavorable discharge status, it was not substantially linked to in-hospital death. In previous studies, male patients with pulmonary hypertension had a higher hospital mortality rate than female patients.26
Limitations
Our investigation exclusively examined the echocardiographic findings of patients admitted to the hospitals for ischemic stroke; therefore, the higher prevalence of echocardiographic abnormalities seen in the study. This might be because individuals managed in the inpatient and intensive care units often have more comorbidities and severe forms of stroke when compared to patients managed in the outpatient department. Another limitation is that we enrolled only patients admitted to the neurology department with a stroke code. Similar patients admitted in other departments due to concomitant comorbidities could have been missed.
Conclusion
The current study emphasizes how important echocardiography is for assessing the functional and structural integrity of the heart and for detecting abnormalities that could have therapeutic implications for stroke survivors. Due to the necessity to adapt it in the event of left ventricular dysfunction, TTE may be helpful in the planning of post-stroke rehabilitation.
Ethical Approval
The study was reviewed and accepted by the ethics committee of Mogadishu Somali Turkish Training and Research Hospital (Ethics Protocol No: MSTH/9571). Due to the fact that our hospital is a research and training hospital. An informed consent is taken from every patient/caregiver before admission to use their data without disclosing their names for research purposes. In addition, as per our hospital protocol, informed consent is waived for retrospective studies as long as patients’ data are not disclosed. The study complies with the Declaration of Helsinki, and this research did not receive any specific funding.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Bejot Y, Caillier M, Salem DB, et al. Ischaemic stroke subtypes and associated risk factors: a French population based study. J Neurol Neurosurg Psychiatry. 2008;79(12):1344–1348. doi:10.1136/jnnp.2008.150318
2. Ois A, Cuadrado-Godia E, Jiménez-Conde J, et al. Early arterial study in the prediction of mortality after acute ischemic stroke. Stroke. 2007;38(7):2085–2089. doi:10.1161/STROKEAHA.107.482950
3. Evangelista A, Flachskampf F, Lancellotti P, et al. European Association of echocardiography recommendations for standardization of performance, digital storage and reporting of echocardiographic studies. Eur J Echocardiogr. 2008;9(4):438–448. doi:10.1093/ejechocard/jen174
4. Menon BK, Coulter JI, Bal S, et al. Acute ischaemic stroke or transient ischaemic attack and the need for inpatient echocardiography. Postgrad Med J. 2014;90(1066):434–438. doi:10.1136/postgradmedj-2013-132220
5. Kim Y, Lee SH. Embolic stroke and after-admission atrial fibrillation. Int J Cardiol. 2016;222:576–580. doi:10.1016/j.ijcard.2016.07.265
6. Mas JL, Derumeaux G, Guillon B, et al. Patent foramen ovale closure or anticoagulation vs. antiplatelets after stroke. N Engl J Med. 2017;377(11):1011–1021. doi:10.1056/NEJMoa1705915
7. Brott T, Adams HP Jr, Olinger CP, et al. Measurements of acute cerebral infarction: a clinical examination scale. Stroke. 1989;20(7):864–870. doi:10.1161/01.STR.20.7.864
8. Burkot J, Kopec G, Pera J, Slowik A, Dziedzic T. Decompensated heart failure is a strong independent predictor of functional outcome after ischemic stroke. J Card Fail. 2015;21(8):642–646. doi:10.1016/j.cardfail.2015.03.008
9. Milionis H, Faouzi M, Cordier M, D’Ambrogio-Remillard S, Eskandari A, Michel P. Characteristics and early and long-term outcome in patients with acute ischemic stroke and low ejection fraction. Int J Cardiol. 2013;168(2):1082–1087. doi:10.1016/j.ijcard.2012.11.036
10. Kim M, Kim HL, Park KT, et al. Echocardiographic parameters determining cardiovascular outcomes in patients after acute ischemic stroke. Int J Cardiovasc Imaging. 2020;36(8):1445–1454. doi:10.1007/s10554-020-01841-5
11. Powers WJ, Rabinstein AA, Ackerson T, et al; American Heart Association Stroke Council. 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2018;49(3):e46–e110. doi:10.1161/STR.0000000000000158
12. Lang RM, Bierig M, Devereux RB, et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr. 2005;18(12):1440–1463. doi:10.1016/j.echo.2005.10.005
13. Bogousslavsky J, Kaste M, Olsen TS, Hacke W, Orgogozo JM. Risk factors and stroke prevention. Cerebrovasc Dis. 2000;10(Suppl. 3):12–21. doi:10.1159/000047577
14. Abdi IA, Karataş M, Abdi AE, Hassan MS, Mohamud MF. Simultaneous acute cardio-cerebral infarction associated with isolated left ventricle non-compaction cardiomyopathy. Ann Med Surg. 2022;80:104172.
15. Hassan MS, Sidow NO, Gökgül A, et al. Pattern of neurological disorders among patients evaluated in the emergency department; cross–sectional study. Arch Acad Emerg Med. 2023;11(1):e20. doi:10.22037/aaem.v11i1.1813
16. Fralick M, Goldberg N, Rohailla S, et al. Health services: value of routine echocardiography in the management of stroke. Cmaj. 2019;191(31):E853–E859. doi:10.1503/cmaj.190111
17. McGrath ER, Paikin JS, Motlagh B, Salehian O, Kapral MK, O’Donnell MJ. Transesophageal echocardiography in patients with cryptogenic ischemic stroke: a systematic review. Am Heart J. 2014;168(5):706–712. doi:10.1016/j.ahj.2014.07.025
18. Ahmed SA, Karataş M, Öcal L, Mohamud MA, Abdi IA, Hassan MO. A 28-year-old male with spontaneous coronary artery dissection complicated by apical thrombus and acute ischemic stroke: an interesting case. Radiol Case Rep. 2023;18(1):246–249. doi:10.1016/j.radcr.2022.10.001
19. De Rosa S, Sievert H, Sabatino J, Polimeni A, Sorrentino S, Indolfi C. Percutaneous closure versus medical treatment in stroke patients with patent foramen ovale: a systematic review and meta-analysis. Ann Intern Med. 2018;168(5):343–350. doi:10.7326/M17-3033
20. Nakanishi K, Homma S. Role of echocardiography in patients with stroke. J Cardiol. 2016;68(2):91–99. doi:10.1016/j.jjcc.2016.05.001
21. Ustrell X, Pellisé A. Cardiac workup of ischemic stroke. Curr Cardiol Rev. 2010;6(3):175–183. doi:10.2174/157340310791658721
22. Kittner SJ, Sharkness CM, Price TR, et al. Infarcts with a cardiac source of embolism in the NINCDS stroke data bank: historical features. Neurology. 1990;40(2):281. doi:10.1212/WNL.40.2.281
23. Ahmed SA, Karataş M, Öcal L, et al. Isolated left ventricular non-compaction cardiomyopathy complicated by acute ischemic stroke: a rare case repor. Ann Med Surg. 2022;81:104543. doi:10.1016/j.amsu.2022.104543
24. Chiarella F, Santoro E, Domenicucci S, Maggioni A, Vecchio C. Predischarge two-dimensional echocardiographic evaluation of left ventricular thrombosis after acute myocardial infarction in the GISSI-3 study. Am J Cardiol. 1998;81(7):822–827. doi:10.1016/S0002-9149(98)00003-4
25. Mooe T, Eriksson P, Stegmayr B. Ischemic stroke after acute myocardial infarction: a population-based study. Stroke. 1997;28(4):762–767. doi:10.1161/01.STR.28.4.762
26. Pana TA, Dawson DK, Mohamed MO, et al. Sex differences in ischemic stroke outcomes in patients with pulmonary hypertension. J Am Heart Assoc. 2021;10(6):e019341. doi:10.1161/JAHA.120.019341
27. Abdi IA, Sidow NO, Hassan MS, Mohamud MF, Karataş M. Spontaneous bilateral subdural hematoma in a patient with a prosthetic valve and association with plasmodium vivax malaria: a rare case report. Ann Med Surg. 2022;80:104191. doi:10.1016/j.amsu.2022.104191
28. Witt BJ, Brown RD Jr, Jacobsen SJ, Weston SA, Yawn BP, Roger VL. A community-based study of stroke incidence after myocardial infarction. Ann Intern Med. 2005;143(11):785–792. doi:10.7326/0003-4819-143-11-200512060-00006
29. Powers WJ. Clinical utility of echocardiography in secondary ischemic stroke prevention. In: Handbook of Clinical Neurology. Vol. 1. Elsevier; 2021:359–375.
30. Sheikh Hassan M, Yucel Y. Factors influencing early hospital arrival of patients with acute ischemic stroke, cross-sectional study at teaching hospital in Mogadishu Somalia. J Multidiscip Healthc. 2022;Volume 15:2891–2899. doi:10.2147/JMDH.S392922
31. Maheshwari R, Wardman D, Cordato DJ, Bhaskar SM. Acute ischaemic stroke in infective endocarditis: pathophysiology and clinical outcomes in patients treated with reperfusion therapy. Immuno. 2021;1(4):347–359. doi:10.3390/immuno1040023
32. Islam H, Puttagunta SM, Islam R, et al. Risk of stroke with mitral stenosis: the underlying mechanism, treatment, and prevention. Cureus. 2022;14(4). doi:10.7759/cureus.23784
33. Park HK, Kim BJ, Yoon CH, Yang MH, Han MK, Bae HJ. Left ventricular diastolic dysfunction in ischemic stroke: functional and vascular outcomes. J Stroke. 2016;18(2):195. doi:10.5853/jos.2015.01697
34. Halley CM, Houghtaling PL, Khalil MK, Thomas JD, Jaber WA. Mortality rate in patients with diastolic dysfunction and normal systolic function. Arch Intern Med. 2011;171(12):1082–1087. doi:10.1001/archinternmed.2011.244
35. Castilla-Guerra L, Del Carmen Fernández-Moreno M, Alvarez-Suero J, Gonzalez A. Echocardiographic assessment of hypertensive left ventricular hypertrophy in patients with acute ischemic stroke or transient ischemic attack. J Stroke Cerebrovasc Dis. 2012;21(8):745–748. doi:10.1016/j.jstrokecerebrovasdis.2011.03.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.