Back to Journals » Risk Management and Healthcare Policy » Volume 18
Analysis of Drug Product Dispensing Error Characteristics, Construction and Evaluation of a Risk Warning Model in Outpatient Pharmacy: A Retrospective Study in China
Authors Xu T ![]() , Wang W, Zhang W, Huang C, Li Y, Chen R
, Wang W, Zhang W, Huang C, Li Y, Chen R
Received 27 August 2025
Accepted for publication 11 December 2025
Published 19 December 2025 Volume 2025:18 Pages 3937—3948
DOI https://doi.org/10.2147/RMHP.S557884
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Keon-Hyung Lee
Tao Xu,* Wanqing Wang,* Wei Zhang, Chunyan Huang, Yi Li, Rong Chen
Department of Pharmacy, The First Affiliated Hospital of Soochow University, Suzhou, Jiangsu, 215006, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rong Chen, Department of Pharmacy, The First Affiliated Hospital of Soochow University, Suzhou, 215006, People’s Republic of China, Email [email protected] Yi Li, Department of Pharmacy, The First Affiliated Hospital of Soochow University, Suzhou, 215006, People’s Republic of China, Email [email protected]
Background/Objectives: Dispensing errors have the potential to cause significant and preventable patient harm, including adverse drug events, hospitalization, or even death. This study aims to analyze the characteristics of drug product dispensing errors in the outpatient pharmacy, identify risk factors, and develop a risk warning model for error prediction.
Methods: A retrospective study analyzed 930 prescriptions with product dispensing errors and 1860 control prescriptions without errors in an outpatient pharmacy of a tertiary hospital from April 2021 to March 2023. Univariate and multivariable logistic regression were used to identify risk factors. A risk warning model with a cutoff value was constructed and its reliability evaluated using Receiver Operating Characteristics(ROC) curve analysis. The cutoff value was then used to assess the model’s test effectiveness with validation dataset.
Results: Logistic regression analysis identified six independent risk factors for product dispensing errors in outpatient pharmacies: work experience, professional title, education level, similar drug names, similar drug appearances, and multiple specifications. A risk warning model (p=ex/(1+ex), x=3.721– 2.133×X1-0.424×X2-0.382×X3+0.736×X4+0.890×X5+0.701×X6) was established. ROC curve analysis showed an AUC of 0.921 (95% CI: 0.908, 0.933), cutoff value of 0.508, sensitivity of 86.0%, specificity of 91.7%, and Youden index of 0.777 for the training dataset. For the validation dataset, results revealed an AUC of 0.928 (95% CI: 0.901, 0.956), sensitivity of 85.90%, specificity of 83.10%, and Youden index of 0.69.
Conclusion: The risk warning model demonstrated high accuracy in predicting product dispensing errors in outpatient pharmacies. Validated externally, it provides a practical reference for preventing such errors.
Keywords: drug dispensing, product errors, risk factors, logistic regression, ROC curve
Introduction
Medication error(ME) refers to any preventable inappropriate use of qualified drugs during the entire clinical application process.1 In March 2017, the World Health Organization(WHO) launched a global initiative aimed at improving medication safety by strengthening systems to reduce MEs and preventable drug-related harms.2 MEs can occur at any stage of the drug treatment process, including prescription writing (or medical orders), drug storage, drug dispensing, preparation for administration, and actual administration.3 MEs are a major cause of harm and preventable patient harm globally, with serious clinical and economic consequences, including adverse drug events, hospitalization, and even death. The annual cost associated with MEs worldwide is estimated to be as high as $42 billion.4 MEs that cause harm or have the potential to cause harm pose significant risks to patients’ health.
Drug dispensing constitutes a crucial aspect of medication therapy, with the primary objective of providing personalized, safe, and effective drug treatment to patients.5 Drug dispensing errors refer to discrepancies between the prescribed medication and the drugs dispensed by the pharmacy to patients or hospital wards.6 Hospital outpatient and inpatient pharmacies play vital roles in the drug dispensing process. However, outpatient pharmacies face higher risks than inpatient pharmacies due to their direct patient-pharmacist interaction. When dispensing errors occur, patients may receive incorrect medications or dosages, leading to treatment failure, life-threatening adverse events, and other adverse outcomes.7 Common types of dispensing errors include drug product errors, quantity errors, labeling errors, and omission errors. Among these errors, drug product errors and drug quantity errors are the most prevalent. Quantity errors rarely result in serious adverse events, as they involve the correct medication. In contrast, product errors occur when dispensed drugs do not match the prescription and often lead to ineffective treatment or serious adverse reactions, such as allergies, poisoning, and harmful drug-drug interactions.8–10
Dispensing error rates reported in the literature vary across practice settings and countries, likely attributed to differences in operational definitions and error reporting methodologies. A comprehensive systematic review of dispensing errors across diverse pharmacy settings and countries revealed that the overall global prevalence of dispensing errors across pharmacy settings was 1.6%.11 In 2024, a total of 27,309 cases of ME from 484 hospitals in 27 provincial administrative regions were collected in the National Clinical Safe Medication Surveillance Network of China. Among these, drug product errors accounted for 5,347 cases (19.13%). Of the 27,030 MEs classified as Grade B to Grade I, the main locations of occurrence were outpatient departments (11,009 cases, 40.73%), inpatient wards (7,393 cases, 27.35%), and pharmacies (6,219 cases, 23.27%).12 Currently, most studies on MEs focus primarily on prescribing and administration errors,13 with relatively less attention paid to drug product dispensing errors.
The Chinese government has issued numerous policies to enhance the safety and accessibility of medication usage. In 2019, the General Office of the State Council issued the “Pilot Program for Centralized Procurement and Use of Drugs Organized by the State”.14 By December 2023, the National Medical Insurance Administration had organized nine rounds of state-organized centralized drug procurement, encompassing a total of 374 drugs. Furthermore, the National Medical Insurance Administration negotiates prices with drug manufacturers to determine payment standards, includes drugs in the medical insurance reimbursement list, and implements national medical insurance negotiation drugs, continuously improving drug accessibility and reducing patients’ medication burden.15 As various drug policies are gradually advanced and implemented, the variety of covered drugs continues to increase, posing new risks and challenges for outpatient pharmacy dispensing. The increasing number of drug types and frequent changes in drug catalogues have posed higher requirements for the accuracy of drug product dispensing.16 In the outpatient pharmacy environment, ensuring the quality of drug dispensing, preventing dispensing errors, and safeguarding safe and rational drug use are the primary responsibilities of pharmacists.
Existing research on drug dispensing has predominantly focused on characterizing errors by examining their types and underlying causes. In 2021, Poole et al conducted a systematic review and meta-analysis, which demonstrated that intervention strategies such as staff training and technology implementation can reduce error rates in hospital pharmacies.17 In another study in 2021, Soubra et al carried out a separate observational study on Lebanese community pharmacies, where they employed logistic regression to examine dispensing errors. They identified key causes of errors, including work overload, illegible handwriting, distractions, and similar drug naming or packaging.18 However, due to variations in culture, laws, and healthcare systems, the generalizability of these findings to other regions remains uncertain. In China, research on multifactorial analysis and risk warning models for drug product dispensing errors is particularly limited. This study therefore aims to analyze the causes of such errors in outpatient pharmacies, construct a risk warning model, and evaluate its ability to predict error occurrence to ultimately enhance dispensing accuracy and safeguard rational drug use.
Methods
Study Design
A retrospective controlled study was conducted using prescription data from the outpatient pharmacy of a tertiary hospital, which was passively divided into an observation group and a control group based on whether product dispensing errors occurred. Specifically, the observation group (error group) included 930 prescriptions with product dispensing errors that happened between April 2021 and March 2023, while the control group (non-error group) consisted of 1860 randomly selected error-free prescriptions from the same period, at a 1:2 ratio to the observation group.19,20 Dispensing errors were classified into two types: internal dispensing errors and external dispensing errors. Internal dispensing errors refer to those occurring during the dispensing process by pharmacists and are corrected through secondary verification, thus not being dispensed to patients. External dispensing errors, on the other hand, refer to errors that are detected and reported by patients, medical staff, or others after the drugs have been dispensed. The focus of this study is specifically on internal dispensing errors related to the dispensed drug product, which encompass medication name errors, dosage form errors, and specification errors.
Intelligent Drug Dispensing in Outpatient Pharmacy Description
The parameter configuration interface of the intelligent dispensing system in outpatient pharmacies is integrated with the Hospital Information System (HIS). The standard setup of this system comprises smart drug baskets and other components. These smart baskets are wirelessly connected to the system, enabling information synchronization with the dispensing machinery and displaying their respective locations. Upon scanning a card reader, the automated dispensing process is initiated, establishing a binding relationship with the patient’s prescription. Once a patient pays for their medication, their prescription details are instantaneously transmitted to the outpatient pharmacy’s data server. The system then automatically designates a pick-up window, and a barcode printer generates a dispensing list. The dispensing pharmacist prepares the medication as per the list and places it in the smart drug basket. Concurrently, scanning the card reader triggers the display of the patient’s name on the screen. Once the patient sees their name on the screen, they proceed to the designated window with their prescription and receipt to collect their medication. Upon receiving the prescription and receipt, the dispensing pharmacist scans the barcode on the pick-up slip. Utilizing radio frequency technology, the smart drug basket prompts and illuminates to indicate its location, enabling the dispensing pharmacist to promptly retrieve the patient’s basket, dispense the medication, and provide the necessary medication instructions.
Intelligent Error Management System Description
Building upon the comprehensive information management of outpatient pharmacy, an intelligent error management system has been developed, leveraging the electronic recording capabilities of operators across various positions, as well as the system’s automated backup functionalities. This system comprises an intelligent error recording system and an error management platform. By digitizing and intelligently recording errors, the system transmits the recorded content in real-time to the error management platform, making errors immediately visible. The “Error Registration” function is integrated into the outpatient pharmacy dispensing system interface. When a dispensing error occurs, the pharmacist promptly logs the relevant details, including specifics of the prescription medication. Upon selecting the medication name, the system automatically saves the corresponding information related to that medicine such as name, specification, quantity, usage, frequency, dosage, and manufacturer. Additionally, the documentation will encompass the various error types encountered during dispensing, including incorrect medication, quantity discrepancies, specification errors, dosage form issues, administration route deviations, contraindications, and other missteps. The pharmacist then delves into the specific details of these errors and identifies their underlying root causes, ranging from non-compliance with procedures to unfamiliarity with standards, chaotic working environments, limited knowledge, fatigue, mixed dispensing practices, lack of responsibility, equipment malfunctions, and errors in manual dispensing. The system’s backend efficiently facilitates real-time data export for in-depth analysis. Furthermore, it automatically generates error reports, enabling individuals to review their error occurrences and their proportion of total errors at any given time. The entire recording process is streamlined with a single mouse click, eliminating the need for manual data entry, thus enhancing efficiency and accuracy.
Collection of Drug Product Error Information
When the checking pharmacists verify prescriptions and drugs, if they detect any discrepancies between the dispensed drugs and the prescriptions, they promptly communicate with the dispensing pharmacist to verify and replace any incorrect drugs. Concurrently, they record the errors that occurred in the dispensing system, including the personnel involved, the cause, and the type of error. The registration information of prescriptions with product dispensing errors and the relevant data of prescriptions with no dispensing errors were exported from the outpatient pharmacy dispensing system’s backend. Relevant data were collected, including the dispensing pharmacists’ work experience, professional title, educational background, and gender, as well as the presence of drugs with similar names, similar appearances, or multiple specifications in the prescribed medications. Additionally, 156 prescriptions with product dispensing errors and 195 prescriptions with no dispensing errors from April 2023 to December 2023 were selected for a validation data set, following the same inclusion criteria as the initial modeling data set. Drug name similarities refer to Look-Alike/Sound-Alike (LASA) characteristics, specifically orthographic and phonetic similarity. Drug appearance similarities are defined by medications’ highly similar visual features: matching packaging (size, color, shape), identical dosage forms, and comparable labeling designs.21
Model Construction and Evaluation
The construction of the final risk warning model for drug product dispensing errors was conducted using both univariate and multivariable logistic regression analysis. Logistic regression is widely applied in medical research for binary outcomes, enables clear interpretation of risk factor effects via coefficients and odds ratios.22 The outcome of internal errors in drug product dispensing in the outpatient pharmacy was designated as the dependent variable, while the relevant objective and human factors related to the error events served as independent variables. Initially, univariate analysis was employed to screen for independent variables influencing drug product dispensing errors, aiming to comprehensively cover potential risk warning variables. Variables with a P-value < 0.2 in the univariate analysis were selected to increase the sensitivity of the risk warning model and incorporate a wider range of potential variables. Subsequently, these variables underwent further scrutiny through multivariable logistic regression analysis. Finally, the significantly influential independent variables (P<0.05) were included in the risk warning model for drug product dispensing errors.
The ROC curve, a commonly used standard in research, was utilized in this study to evaluate the screening effectiveness of the risk warning model. This analysis was conducted to assess the predictive value of the model for drug product dispensing errors. The Area Under the Curve (AUC) is a metric related to the ROC curve.23 An AUC value less than 0.6 indicates low discrimination, while a value between 0.6 and 0.75 represents moderate discrimination. Values greater than 0.75 indicate high discrimination. A high AUC value suggests a higher accuracy of the model.
Statistical Analysis
The statistical analysis was conducted using SPSS 26.0 software. In the univariate analysis, all statistical variables in the error group were compared with the corresponding variables in the control group to determine the P-value for each variable. Count data were represented as frequencies, and categorical variables were evaluated using chi-square tests. Multivariable analysis was performed using a logistic regression model, with variable selection based on the results of univariate analysis. Variables in univariate analysis with a hypothesis test result of P < 0.1 were included in the subsequent multivariable analysis. A test level of α = 0.05 was specified for introducing variables into the model, and α = 0.10 for removing variables from it. Logistic regression was employed to calculate the regression coefficients, standard errors, Wald chi-square values, P-values, corresponding odds ratios (OR), and 95% confidence intervals (CI) for each potential predictor. Based on the independent risk warning indicators for outpatient pharmacy drug product dispensing errors identified by logistic regression analysis, an early warning model was constructed. Its screening performance was evaluated using the ROC curve, and external validation was performed to assess its predictive performance, with P < 0.05 considered statistically significant.
Results
Basic Characteristics of Dispensing Pharmacists
A total of 2,790 prescriptions were analyzed in this study, comprising 930 prescriptions in the error group and 1,860 prescriptions in the control group. Table 1 presents an overview of the fundamental characteristics of the dispensing pharmacists involved in the study. With regard to work experience, 30.9% of the prescriptions were dispensed by pharmacists with 0 to 1 year of experience, 37.1% by those with 1 to 2 years, 23.7% by those with 2 to 5 years, and 8.4% by those with 5 or more years of experience. This distribution indicates that the participating pharmacists generally had relatively short work tenures, with nearly 70% having worked for 2 years or less. In terms of professional titles, 38.6% of the prescriptions were dispensed by Pharmacy Assistants, 40.0% by Pharmacists, and 21.4% by Pharmacists-in-Charge or higher-level pharmacists. This finding reveals that junior professional titles were the dominant qualification among the study population.
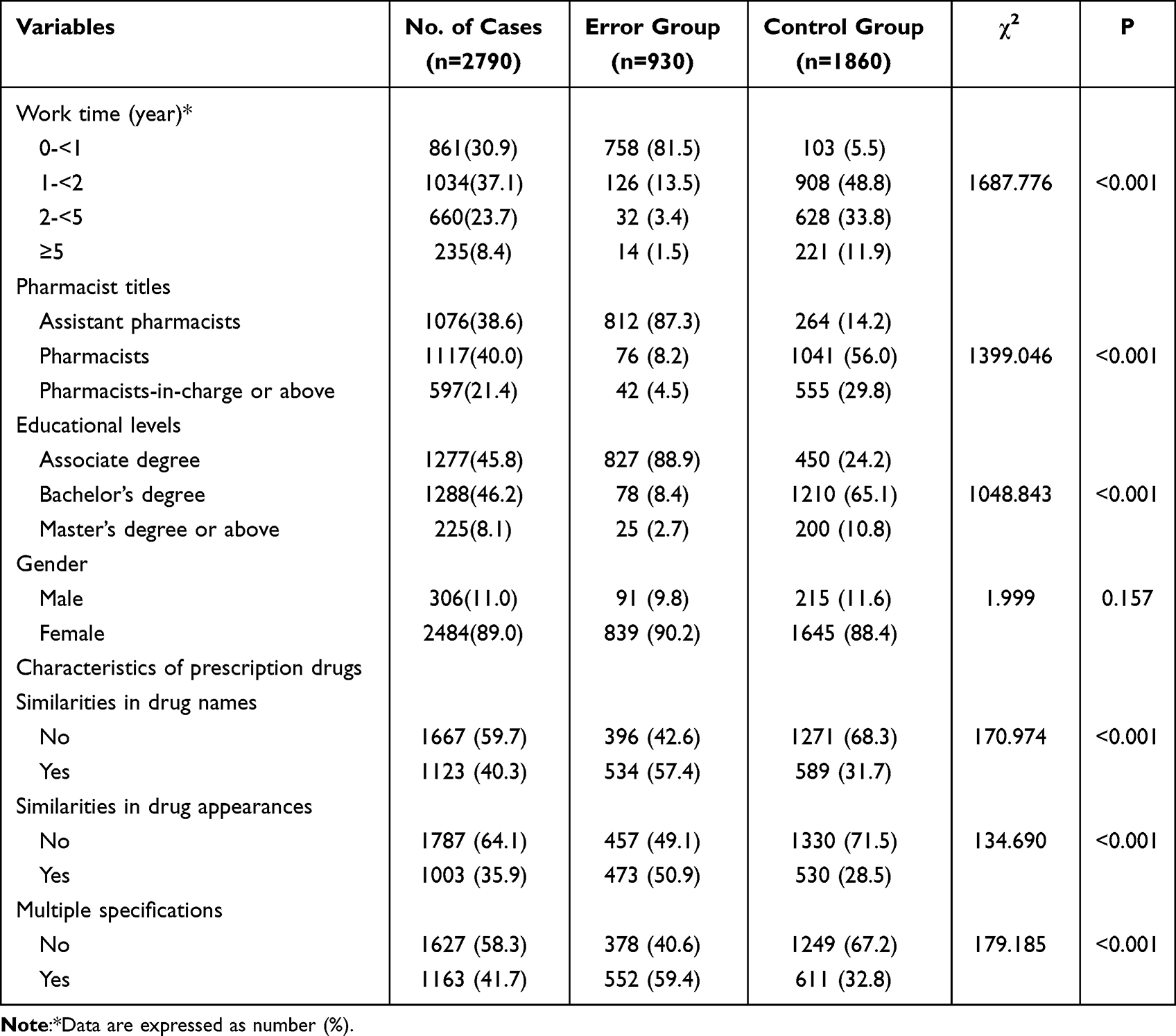 |
Table 1 Single Factor Analysis of Possible Risk Factors for Drug Product Dispensing Errors in Outpatient Pharmacy |
From an educational perspective, 45.8% of the prescriptions were dispensed by pharmacists with associate degrees, 46.2% by those with bachelor’s degrees, and 8.1% by those with master’s degrees or above. This reflects that associate and bachelor’s degrees constituted the primary educational background of the participating pharmacists. Regarding gender distribution, 11% of the prescriptions were dispensed by male pharmacists, while 89% were dispensed by female pharmacists. Collectively, these data demonstrate that the dispensing pharmacists in the outpatient pharmacy were predominantly female, with the overall personnel structure characterized by a noticeable younger profile, junior professional titles, and associate or bachelor’s degree backgrounds.
Univariate Analysis of Internal Dispensing Errors in Outpatient Pharmacy Drug Products
The results of univariate analysis revealed that factors such as the dispensing pharmacists’ years of work experience, professional titles, educational backgrounds, gender, as well as the similarity of drug names, similarity of appearance, and the existence of multiple specifications for a single drug were correlated with the occurrence of internal dispensing errors in outpatient pharmacy drug products, showing statistical significance (P < 0.05, see Table 1).
Multivariable Analysis of Internal Dispensing Errors in Outpatient Pharmacy Drug Products
In this study, the occurrence of internal dispensing errors in outpatient pharmacy drug products was designated as the dependent variable. Initially, a univariate analysis was performed to identify potential independent variables that significantly influenced the occurrence of dispensing errors (p < 0.10). Subsequently, significant independent variables were included in a multivariable logistic regression model to further elucidate the relevant factors associated with dispensing errors in outpatient pharmacy drug products. Six independent risk factors were identified: years of work experience (X1) (P < 0.05), professional title (X2) (P < 0.05), educational background (X3) (P < 0.05), similarity of drug names (X4) (P = 0.001), similarity of drug appearance (X5) (P = 0.004), and the presence of multiple specifications for a single drug (X6) (P = 0.001). Logistic regression analysis was conducted to determine the regression coefficients, standard errors, Wald chi-square values, P-values, corresponding odds ratios (OR), and 95% confidence intervals (CI) for these independent risk indicators. The results are presented in Table 2.
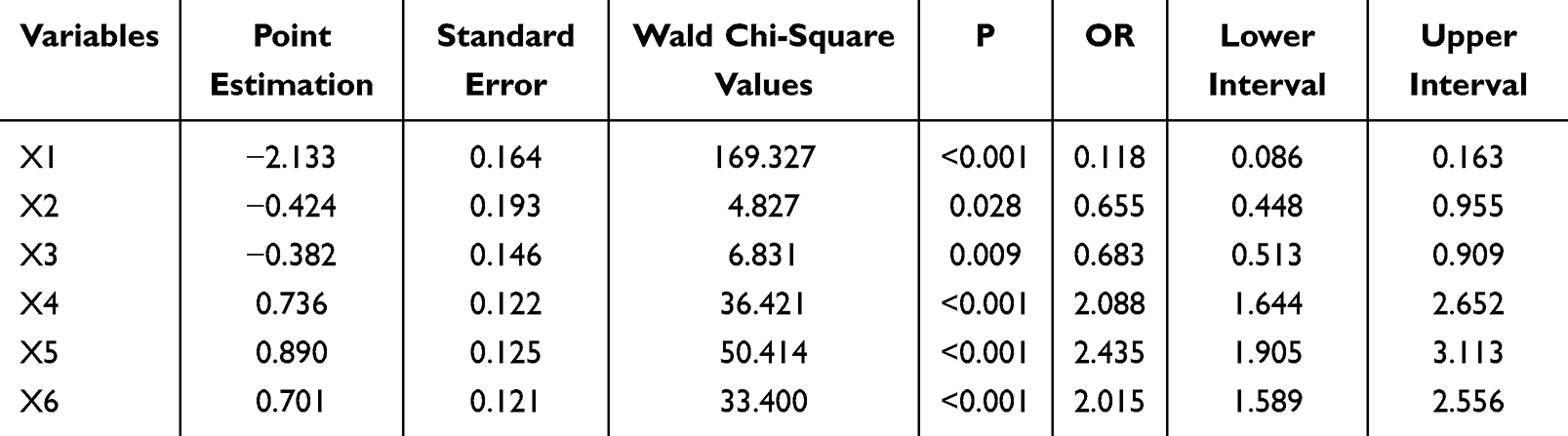 |
Table 2 Multivariable Analysis of Risk Factors for Drug Product Dispensing Errors in Outpatient Pharmacy |
Construction of a Risk Warning Model for Dispensing Errors in Outpatient Pharmacy Drug Products
Based on the results of the multivariable logistic regression analysis, the assignment methods for the independent variables in the model are presented in Table 3. The final risk warning model is formulated as follows:
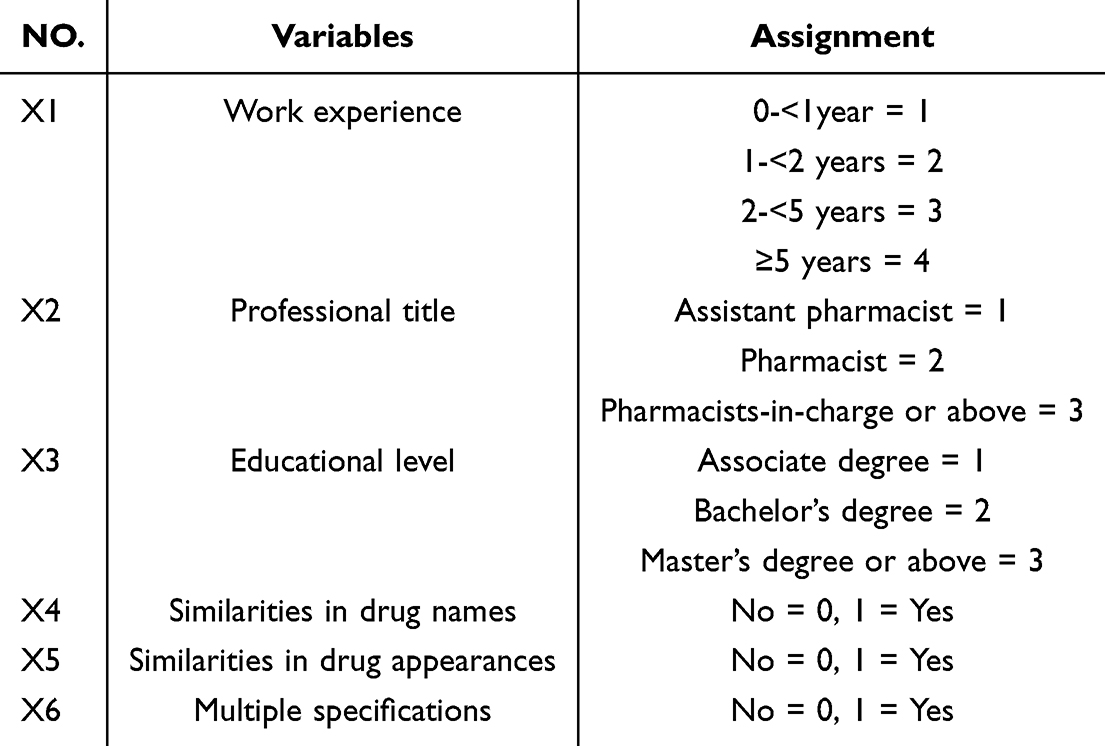 |
Table 3 The Way to Evaluate the Value of the Variable of the Risk Warning Mode |


In this model, p represents the probability of occurrence of dispensing errors, where e is the base of the natural logarithm.
The assignment of years of work experience (X1) is as follows: 0 to less than 1 year is assigned a value of 1, 1 to less than 2 years is assigned a value of 2, 2 to less than 5 years is assigned a value of 3, and 5 or more years is assigned a value of 4. For professional titles (X2), Pharmacy Assistant is assigned a value of 1, Pharmacist is assigned a value of 2, and Senior Pharmacist and higher titles are assigned a value of 3. Similarly, for educational backgrounds (X3), Associate degree is assigned a value of 1, Bachelor’s degree is assigned a value of 2, and Master’s degree or higher is assigned a value of 3. The variables for similarity of drug names (X4), similarity of drug appearance (X5), and multiple specifications for a single drug (X6) are binary values, with “1” indicating the presence of the respective factor in the prescription and “0” indicating its absence.
Evaluation of the Risk Warning Model of Drug Product Dispensing Errors in Outpatient Pharmacy
Utilizing the risk warning model formula for drug product dispensing errors in outpatient pharmacy, ROC curve analysis was conducted to estimate the predictive probability of drug product dispensing errors. The area under the ROC curve (AUC) was 0.921 (95% CI: 0.908, 0.933), with a standard error of 0.007, showing high discrimination for drug product dispensing errors in outpatient prescriptions. Additionally, the Hosmer-Lemeshow test (H-L test) was performed on the risk warning model, and the χ2 value was 724.416. The risk warning model was utilized to determine the cutoff value, which was established as 0.508. The predicted sensitivity was 86.0%, specificity was 91.7%, and the Youden index was 0.777, as illustrated in Figure 1.
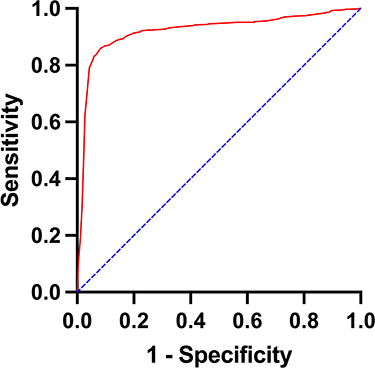 |
Figure 1 ROC curve of drug product errors risk warning model in outpatient pharmacy. |
External Validation of the Risk Warning Model
The validation data set, consisting of 156 prescriptions with drug product dispensing errors and 195 prescriptions with no dispensing errors, was input into the established risk warning model to calculate the prediction probability of drug product dispensing errors occurring in each prescription. The model’s cutoff value was then used to evaluate the predictive performance of the validation data set. The results revealed a sensitivity of 85.90%, specificity of 83.10%, accuracy of 84.30%, and a Youden index of 0.69. These findings indicate that the risk warning model exhibited a high predictive efficiency in both internal and external validations.
Discussion
Drug dispensing is a crucial component of the pharmacy’s direct provision of pharmaceutical services to patients, and the quality of dispensing directly impacts the safety and effectiveness of medication use.24,25 Both internal and external dispensing errors are mistakes or oversights that occur during the dispensing process, which can have adverse effects on drug management and patient medication. Internal dispensing errors can, to a certain extent, increase the risk of external errors occurring. If pharmacists make mistakes during the dispensing process, it can further lead to patients receiving incorrect medications, thereby increasing the rate of external feedback errors.26 Therefore, reducing the occurrence of internal errors is one of the important means to lower the risk of external errors. Currently, research on dispensing errors in outpatient pharmacies has mainly focused on identifying the causes of these errors, while there is a paucity of studies utilizing logistic regression analysis to identify risk factors influencing such errors. This study aims to establish a risk prediction model by applying logistic regression analysis to the occurrence of dispensing errors in outpatient pharmacies, specifically focusing on the perspective of product dispensing errors.
A study analyzing the impact of drug name similarity on dispensing errors, which classified all drugs stored in the dispensary in terms of both drug name similarity and drug efficacy similarity, demonstrated that drug name similarity increases the risk of dispensing errors. It also indicated that prioritizing the differentiation of medicines with similar packaging over those with similar names is more important when arranging drug shelving.27 Another study found that the number of medication orders on a prescription (≥4 medications) and pharmacy busyness significantly predicted the occurrence of medication dispensing errors. The causes of dispensing errors have been explored in various countries and factors, such as work overload and pharmacists fatigue, have been highlighted as contributory factors.10 This study combined model construction with a conceptual framework to scientifically and comprehensively assess both objective and subjective factors related to product dispensing errors in outpatient pharmacies. In univariate analysis, the consideration of confounding factors and/or the interaction between various factors is often overlooked, whereas further multivariable analysis can fully account for the interactions among these factors.28–30 Therefore, it is necessary to conduct multivariable analysis after univariate analysis to determine the true factors leading to errors and avoid false positive results. Consequently, evaluating the model after its establishment is crucial to ensure its authenticity and reliability. Utilizing logistic regression analysis and ROC curve evaluation, we identified work experience, professional title, educational background, similarity of drug names, similarity of drug appearance, and multiple specifications for a single drug as independent risk factors for product dispensing errors. Using logistic regression to fit multiple risk factors, we established a model to predict the risk of product dispensing errors in outpatient pharmacies. The final results of logistic multivariable analysis revealed that work experience, professional title, and educational background had a negative correlation with the occurrence of errors, suggesting that longer work experience, higher professional titles, and higher educational backgrounds are associated with a lower risk of errors. Conversely, similarity of drug names, similarity of drug appearance, and the presence of multiple specifications for a single drug had a positive correlation with error occurrence, indicating a higher risk of errors when these factors are present. Furthermore, the evaluation results of the model showed that the AUC under the ROC curve for predicting product dispensing errors in outpatient pharmacies was 0.921, indicating good predictive ability. This model can be utilized in practical work for early warning of potential product dispensing errors.
To continually reduce dispensing errors in outpatient pharmacies, it is imperative to address both personnel and medication aspects based on the relevant risk factors identified in our research. Specifically: (1) Personnel Aspect: Pharmacists play a pivotal role in drug handling and dispensing, particularly at outpatient dispensing counters where they have direct contact with patients. Dispensing errors often occur due to human factors. Our study reveals that pharmacists with less than one year of work experience may possess insufficient knowledge and comprehension of drugs due to their limited exposure. Consequently, outpatient pharmacies should establish standardized training programs for drug dispensing, emphasizing training and assessments for staff, particularly those with shorter work experience, lower professional titles, and fewer academic qualifications. Layered and targeted training should be undertaken to enhance pharmacists’ familiarity with drugs and ensure the safety of dispensed medications. Additionally, a robust quality control system for outpatient pharmacies should be established to regularly review and analyze dispensing errors, propose optimization and rectification measures, and continuously track their effectiveness. The oversight of the drug dispensing process should also be fortified, with regular inspections and prompt corrective measures for pharmacists’ irregular practices. Notably, pharmacist absence duration is another non-negligible factor under the personnel aspect. A separate study identified that the longer a pharmacist is absent from work, the more likely they are to make a dispensing error upon their return. Accordingly, the study recommends that when a pharmacist has been away from work for more than 72 hours, they should first find their way back to work before dispensing, which will also reduce the number of errors.31 (2) Medication Aspect: Medications are also a significant factor leading to dispensing errors in outpatient pharmacies.32,33 As the last line of defense for patients’ safe and rational use of drugs, outpatient pharmacies face high patient volume and a diverse medication inventory, which can easily lead to dispensing errors.34,35 Therefore, outpatient pharmacies should implement zoning management for the storage and placement of drugs with similar names, similar appearances, and multiple specifications that are prone to errors. Additionally, warning labels such as “similar in appearance,” “similar in pronunciation,” and “multiple specifications” should be prominently displayed to remind pharmacists to strengthen verification when dispensing drugs. Printed and digital drug names may be optimized for readability and distinctiveness by modifying font color, weight, kerning, or capitalization. Tall Man lettering is a popular typographic strategy for this purpose. Technologically, it has been reported that integrating barcode scanning into dispensing enables verification of physically selected drugs against on-screen prescriptions. Theoretically, proper use eliminates most dispensing errors. However, a key limitation is that it may perpetuate pre-dispensing errors, as neglected manual checks reduce their detection.36
Driven by healthcare reform policies, the variety and specifications of drugs are constantly increasing, with new and specialized drugs emerging frequently. Changes in drug varieties, packaging, and manufacturers pose a challenge for pharmacists to continuously update their knowledge and familiarize themselves with new drugs’ indications, dosages, adverse reactions, and other drug information to ensure accurate drug dispensing.37 Furthermore, the diversity of drug varieties and the high similarity of packaging among different manufacturers or even within the same manufacturer can easily lead to confusion and errors during dispensing.38 As competition in the pharmaceutical market intensifies, manufacturers and specifications of drugs are constantly changing. This requires pharmacists to be well-versed in the drugs from various manufacturers and to be familiar with the differences between drugs of different specifications and manufacturers to avoid dispensing errors.39,40 To address these challenges, medical institutions can leverage information technology.41 For instance, electronic bulletin systems can be established on internal networks to real-time post information about new drugs, packaging changes, and manufacturer changes. Pharmacists and relevant staff can access this information at any time to stay updated. Mobile applications can also be developed to provide pharmacists with convenient access to drug information, including indications, dosages, manufacturers, and updates.42 These applications enable pharmacists to learn about new drugs and changes in real-time. Additionally, intelligent reminder functions can be integrated into outpatient pharmacy information systems. When there are changes in drug packaging or manufacturers, the system can automatically alert pharmacists to these changes. Social media and instant messaging tools can also be utilized to establish pharmacist communication groups for timely sharing of new drug training, drug changes, and other relevant information, ensuring rapid dissemination and sharing of knowledge.43–45 By comprehensively utilizing these information technology tools, pharmacists and relevant staff can promptly access information on new drug training, packaging and manufacturer changes, and take corresponding measures to improve the accuracy of drug dispensing and ensure patient safety.
In summary, the construction of a prediction model for product dispensing errors in outpatient pharmacies can provide theoretical support for preventing risks. Based on the results of the model, pharmacy managers in medical institutions can optimize drug dispensing and rationalize the management of personnel and drugs in the outpatient pharmacy workflow to more effectively control the occurrence of related risks and ensure the quality of drug dispensing. Additionally, by providing quantitative information about potential future risks, it can assist decision-makers in better understanding and managing drug risks, providing valuable theoretical references for managers to design preventive strategies for risk events. However, this study has certain limitations. Due to constraints in personnel and other resources, the sample size and scope of this study in a single hospital may limit the establishment of more comprehensive and in-depth conclusions. Therefore, future research plans focus on conducting larger-scale multi-center studies to further clarify the accuracy and reliability of the research results.
Conclusion
This study explored the factors that contribute to product dispensing errors in outpatient pharmacies and constructed a risk warning model for such errors. The model incorporates six independent risk factors: years of work experience, professional title, educational background, similarity in drug names, similarity in drug appearance, and multiple specifications for a single drug. By effectively predicting potential errors, this model can assist pharmacists in implementing targeted interventions, ultimately improving patient safety and medication accuracy. Particularly, it demonstrates high predictive performance for product dispensing errors in outpatient pharmacies and holds practical application value.
Abbreviations
ROC, Receiver Operating Characteristics; AUC, Area Under Curve; ME, Medication Error; WHO, World Health Organization; HIS, Hospital Information System; LASA, Look-Alike/Sound-Alike; OR, Odds Ratio; CI, Confidence Interval; H-L test, Hosmer-Lemeshow test.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and are available from the corresponding author Rong Chen upon reasonable request.
Human Ethics
The Ethics Committee of the First Affiliated Hospital of Soochow University approved this retrospective study, waiving the need for formal ethics approval and individual patient consent. All methods were carried out in accordance with the Declaration of Helsinki. All data accessed in this study have been anonymized to comply with relevant data protection and privacy regulations.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by 2023 Suzhou Pharmaceutical Association - Jiangsu Hengrui Pharmaceutical Clinical Pharmacy Scientific Research Fund (Syhky202302), Hospital Pharmaceutical Research Fund of Chia Tai Tianqing, Jiangsu Pharmaceutical Association in 2022 (Q202230) and Suzhou science and technology development plan (Medical and health science and technology innovation - Applied Basic Research) project (SKJYD2021160).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Nelson KL, Morvay S, Neidecker M, et al. Evaluation of medication safety resources in pediatric hospitals. Am J Health Syst Pharm. 2020;77(Suppl 3):S78–S86. doi:10.1093/ajhp/zxaa177
2. World Health Organization. Medication without harm - global patient safety challenge on medication safety; 2017. Available from: https://iris.who.int/bitstream/handle/10665/255263/WHO-HIS-SDS-2017.6-eng.pdf?sequence=1.
3. World Health Organization. Reporting and learning systems for medication errors: the role of pharmacovigilance centres; 2014. Available from: https://iris.who.int/bitstream/handle/10665/137036/9789241507943_eng.pdf;jsessionid=F2D9DE19B0CEF65047D93E00E1FD796D?sequence=1.
4. Institute for Healthcare Informatics. Advancing the responsible use of medicines: applying levers for change; 2012. Available from: https://ssrn.com/abstract=2222541.
5. Pizetta B, Raggi LG, Rocha KSS, Cerqueira-Santos S, de Lyra DP, Dos Santos GA. Does drug dispensing improve the health outcomes of patients attending community pharmacies?A systematic review. BMC Health Services Research. 2021;21(1):764. doi:10.1186/s12913-021-06770-0
6. Anacleto TA, Perini E, Rosa MB, César CC. Medication errors and drug-dispensing systems in a hospital pharmacy. Clinics. 2005;60(4):325–332. doi:10.1590/s1807-59322005000400011
7. James KL, Barlow D, McArtney R, Hiom S, Roberts D, Whittlesea C. Incidence, type and causes of dispensing errors: a review of the literature. Int J Pharm Pract. 2009;17(1):9–30. doi:10.1211/ijpp.17.1.0004
8. Gao XY, Yan WP, Cai Z, Liu Y, Wang LY. Retrospective analysis and improvement of dispensing errors in the outpatient pharmacy of a tertiary hospital. Capital Food Medicine. 2025;32(17):85–88.
9. Liang J. Analysis of prescriptions with western medicine dispensing errors and related preventive measures. Chin Sci Technol Periodical Database. 2024;(1):172–175.
10. Abdel Qader DH, Al Meslamani AZ, Lewis PJ, Hamadi S. Incidence, nature, severity, and causes of dispensing errors in community pharmacies in Jordan. Int J ClinPharm. 2021;43(1):165–173. doi:10.1007/s11096-020-01126-w
11. Um IS, Clough A, Tan ECK. Dispensing error rates in pharmacy: a systematic review and meta-analysis. Res Social Administrat Pharm. 2024;20(1):1–9. doi:10.1016/j.sapharm.2023.10.003
12. Bai XR, Zhang QX, Wang YQ, et al. Annual report of national monitoring network for clinical safe medication (2024). Adverse Drug Reactions J. 2025;27(8):449–457. doi:10.3760/cma.j.cn114015-20250522-00281
13. Beso A, Franklin BD, Barber N. The frequency and potential causes of dispensing errors in a hospital pharmacy. Pharm World Sci. 2005;27(3):182–190. doi:10.1007/s11096-004-2270-8
14. Lin LM, Peng XQ, Tang R, Liu GD, Liu H, Yin JY. Effects of the national centralized drug procurement policy on drug availability and the structure of hospital drug use. China Pharmacy. 2023;34(24):2968–2974.
15. Qiu ZG, Ke L, Wan YS, et al. Study on the current situation and influencing factors of drug accessibility in a hospital under the negotiation of National Health Insurance. Chin J Hosp Pharm. 2022;42(18):1918–1922.
16. Li Q. Analysis of misallocation errors in easily confused drugs and corresponding strategies. The Medical Forum. 2023;27(16):120–125.
17. Poole SG, Kwong E, Mok B, et al. Interventions to decrease the incidence of dispensing errors in hospital pharmacy: a systematic review and meta-analysis. J Pharm Pract Res. 2021;51(1):7–21. doi:10.1002/jppr.1709
18. Soubra L, Karout S. Dispensing errors in Lebanese community pharmacies: incidence, types, underlying causes, and associated factors. Pharmacy Practice. 2021;19(1):2170. doi:10.18549/PharmPract.2021.1.2170
19. Von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
20. Kardos Z, Szabó M, Baráth Z, et al. Tocilizumab in combination with corticosteroids in COVID-19 pneumonia: a single-centre retrospective controlled study. Biomedicines. 2023;11(2):349. doi:10.3390/biomedicines11020349
21. Bryan R, Aronson JK, Williams A, Jordan S. The problem of look-alike, sound-alike name errors: drivers and solutions. Br J Clin Pharmacol. 2021;87(2):386–394. doi:10.1111/bcp.14285
22. Zabor EC, Reddy CA, Tendulkar RD, Patil S. Logistic regression in clinical studies. Int J Radiation Oncol Biol Phys. 2022;112(2):271–277. doi:10.1016/j.ijrobp.2021.08.007
23. Shen C, Ge BQ, Liu XQ, Chen H, Qin Y, Shen HW. Predicting the occurrence of venous thromboembolism: construction and verification of risk warning model. BMC Cardiovascular Disorders. 2020;20(1):249. doi:10.1186/s12872-020-01519-9
24. Amirthalingam P, Alruwaili AS, Albalawi OA, et al. Comparing patient satisfaction with automated drug dispensing system and traditional drug dispensing system: a cross-sectional study. Patient Prefer Adherence. 2024;18:2337–2345. doi:10.2147/PPA.S492802
25. Neves CV, Cerqueira-Santos S, Silva Rd OS, Luz TCB, Tavares NUL. Drug dispensing in public community pharmacies: evidence from the MedMinas project. BMC Health Services Res. 2024;24(1):1354. doi:10.1186/s12913-024-11816-0
26. Lv L, Yao Y, Zhang MW, Xin CW. Impact of implementing the lean management on internal errors at an outpatient hospital pharmacy in China. Patient Preference Adherence. 2025;19:139–147. doi:10.2147/PPA.S486478
27. Sagawa H, Kizaki H, Yoshikawa K, et al. Analyzing the impact of drug name similarity on dispensing errors: an examination using a drug name similarity index. Biol Pharm Bull. 2024;47(8):1460–1466. doi:10.1248/bpb.b24-00365
28. Muisyo T, Bernardo EO, Camazine M, et al. Mortality prediction in pediatric trauma. J Pediatric Surg. 2019;54(8):1613–1616. doi:10.1016/j.jpedsurg.2018.08.045
29. Xu TT, Weng ZH, Pei C, et al. The relationship between neutrophil-to-lymphocyte ratio and diabetic peripheral neuropathy in Type 2 diabetes mellitus. Medicine. 2017;96(45):e8289. doi:10.1097/MD.0000000000008289
30. Hong HY, Pourghasemi HR, Pourtaghi ZS. Landslide susceptibility assessment in Lianhua County (China): a comparison between a random forest data mining technique and bivariate and multivariate statistical models. Geomorphology. 2016;259:105–118. doi:10.1016/j.geomorph.2016.02.012
31. Chou H, Wang YQ, Liao LW, et al. Exploring susceptibility factors to medication dispensing errors through a retrospective study of patient-reported dispensing errors over 11 years: are dispensing errors indeed due to personal reasons for pharmacists? Eur J Hosp Pharm. 2025;32(4):342–347. doi:10.1136/ejhpharm-2023-004064
32. Luo J, Wei KX, Huang ZG, Liu GP, He W. Reduction of dispensing errors of similar drugs in hospital outpatient pharmacy and realizing of drug traceability system by using drug electronic regulatory code. China Pharmacy. 2017;28(28):3956–3960.
33. Bowdle TA, Jelacic S, Webster CS, Merry AF. Take action now to prevent medication errors: lessons from a fatal error involving an automated dispensing cabinet. British J Anaesthesia. 2023;130(1):14–16. doi:10.1016/j.bja.2022.09.017
34. Aldhwaihi K, Schifano F, Pezzolesi C, Umaru N. A systematic review of the nature of dispensing errors in hospital pharmacies. Integrat Pharm Res Pract. 2016;5:1–10. doi:10.2147/IPRP.S95733
35. Gao YY, Guo Y, Zheng ML, et al. A refined management system focusing on medication dispensing errors: a 14-year retrospective study of a hospital outpatient pharmacy. Saudi Pharmaceut J. 2023;31(12):101845. doi:10.1016/j.jsps.2023.101845
36. Emmerton L, Rizk MFS, Bedford G, Lalor D. Systematic derivation of an Australian standard for Tall Man lettering to distinguish similar drug names. J Evaluat Clin Pract. 2015;21(1):85–90. doi:10.1111/jep.12247
37. Cerqueira-Santos S, Rocha KSS, Araújo DCSA, et al. Which factors may influence the implementation of drug dispensing in community pharmacies? A qualitative study. J Eval Clin Pract. 2023;29(1):83–93. doi:10.1111/jep.13731
38. Emmerton LM, Rizk MFS. Look-alike and sound-alike medicines: risks and ‘solutions’. Int J Clin Pharm. 2012;34(1):4–8. doi:10.1007/s11096-011-9595-x
39. Billstein-Leber M, Carrillo JD, Cassano AT, Moline K, Robertson JJ. ASHP guidelines on preventing medication errors in hospitals. AM J Health Syst Pharm. 2018;75(19):1493–1517. doi:10.2146/ajhp170811
40. Sims L, Campbell J. Ills, pills, and skills: developing the clinical skills of pharmacists in general practice. British J General Pract. 2017;67(662):417–418. doi:10.3399/bjgp17X692453
41. Westbrook JI, Sunderland NS, Woods A, Raban MZ, Gates P, Li L. Changes in medication administration error rates associated with the introduction of electronic medication systems in hospitals: a multisite controlled before and after study. BMJ Health Care Inform. 2020;
42. Long CM, Hameed MA, Lee DD, et al. Use of medical mobile applications among hospital pharmacists in malaysia. Therapeutic Innovat Regulat Sci. 2016;50(4):419–426. doi:10.1177/2168479015624732
43. Crilly P, Hassanali W, Khanna G, et al. Community pharmacist perceptions of their role and the use of social media and mobile health applications as tools in public health. Res Soc Administrat Pharm. 2019;15(1):23–30. doi:10.1016/j.sapharm.2018.02.005
44. Cole KA, Zhou AY, Jones T, et al. How to harness the power of social media for quality drug information in infectious diseases: perspectives on behalf of the society of infectious diseases pharmacists. Clin Infect Dis. 2022;74(Suppl 3):e23–e33. doi:10.1093/cid/ciac081
45. Pizzuti AG, Patel KH, McCreary EK, et al. Healthcare practitioners’ views of social media as an educational resource. PLoS One. 2020;15(2):e0228372. doi:10.1371/journal.pone.0228372
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Risk Factors for Chronic Obstructive Pulmonary Disease in the Middle-Aged and Elderly Rural Population of Northeast China Using Logistic Regression and Principal Component Analysis
Wang R, Zhang W, Li Y, Jiang Y, Feng H, Du Y, Jiao Z, Lan L, Liu X, Li B, Liu C, Gu X, Chu F, Shen Y, Zhu C, Shao X, Tong S, Sun D
Risk Management and Healthcare Policy 2022, 15:1717-1726
Published Date: 11 September 2022
Construction of a Multi-Indicator Model for Abscess Prediction in Granulomatous Lobular Mastitis Using Inflammatory Indicators
Du NN, Feng JM, Shao SJ, Wan H, Wu XQ
Journal of Inflammation Research 2024, 17:553-564
Published Date: 1 February 2024