")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Analysing Home Pharmaceutical Care Under the Combination of Medical Care and Nursing
Authors Zhang Y, Peng J, Sun W, Zhang H, Yang G
Received 7 March 2023
Accepted for publication 30 May 2023
Published 27 June 2023 Volume 2023:16 Pages 1793—1800
DOI https://doi.org/10.2147/JMDH.S411330
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yichun Zhang, Jun Peng, Wenjun Sun, Haipeng Zhang, Guang Yang
Department of Pharmacy, Hebei Yanda Hospital, Langfang City, Hebei Province, People’s Republic of China
Correspondence: Yichun Zhang, Department of Pharmacy, Hebei Yanda Hospital, Yanjiao Simhuilan West Road, Sanhe City, Langfang City, Hebei Province, 065200, People’s Republic of China, Tel +86-316-3306055, Email [email protected]
Objective: Home pharmaceutical care delivers individualised, whole-process and continuous pharmaceutical services and health education. This study aims to explore the feasibility of home pharmaceutical services as a combination of medical and nursing care.
Methods: Patient information was collected from 1 October 2020 to 30 September 2021 and was analysed and evaluated. We then developed a family medication plan and investigated its effectiveness and any issues encountered during the implementation process.
Results: A total of 102 patients received services, and 100% of the patients were satisfied with these. Moreover, using home pharmaceutical care saved approximately USD1,359.64 (RMB9,360.45) in outpatient costs and USD41,077.76 (RMB282,700) in inpatient costs, and the number of hospitalisations was reduced by 16%.
Conclusion: It is beneficial to make home pharmaceutical services available as a combination of medical and nursing care. Pharmacists can help patients solve medication-related problems and reduce the number of hospitalisations and medical costs through standardised service models while ensuring safe, effective, economical and rational drug use for patients.
Keywords: medical care, nursing, home care, home pharmacist, standard services
Introduction
“Home pharmaceutical care” refers to medical institutions’ providing individualised, whole-process and continuous pharmacy services and health education for patients receiving drug treatment at home. This involves drug evaluation and education, helping patients improve drug compliance and ensuring safe and reasonable drug storage and use to improve treatment outcomes.1,2 The elderly have become the focus of home pharmacy care for various reasons, such as poor medication compliance and the coexistence of multiple diseases.2 According to research reports, with the rapid ageing of China’s population, the proportion of the elderly aged 60 years and above has risen to 17.3%, and the prevalence rate of chronic diseases in this group is as high as 59.1%. The proportion of patients suffering from chronic diseases is 23.8%, and the consumption of multiple drugs is common3–5 in the population with chronic disease. The safety concerns associated with long-term drug treatment are also becoming increasingly prominent. According to data from the World Health Organization, China has the world’s largest number of chronic diseases. Every year, 40 million people lose their lives to chronic diseases, accounting for 82.4% of total deaths.6,7 Therefore, managing treatment for patients with chronic diseases poses unprecedented challenges.
Family healthcare is an effective measure for managing chronic diseases in elderly patients.8 Even when battling chronic conditions, the elderly may wish to stay at home. Through innovative healthcare models, patients in China can receive long-term care and advanced support in their homes. Despite the enormous challenges faced by home pharmacies, they still have an important impact on the health of elderly patients with chronic diseases.9 Furthermore, home pharmacy care is not a medication-monitoring model limited to the elderly and chronically ill patients and can provide all groups of people with individualised, whole-process and continuous pharmacy services supported by clinical work.
In recent years, a model of comprehensive prevention and treatment of chronic disease has been gradually developed. Active and comprehensive health management is of great significance to disease control among patients and the prognosis of their condition. Medication therapy management (MTM) is a newly developed service paradigm in pharmacy practice.10 An increasing number of patients’ chronic disease management primarily involves home medication monitoring and management11 (also known as “home pharmaceutical services” or “home pharmaceutical care”). In summary, the home pharmacy model is an innovative model but still faces many challenges, such as medication safety and logistics support.8,9
To better solve the daily medication problems of the elderly discharged from our nursing centre, we collected, analysed and evaluated medication information from patients and developed a family medication plan. We then investigated the effectiveness of the plan and any issues encountered during the implementation process. We aim to promote and develop a model for home-based pharmacy services in China.
Materials and Methods
Clinical Information
We determined participant eligibility for this study by collecting patient information. The observation participants were 102 service patients treated in our hospital from 1 October 2019 to 30 September 2021. The criteria for the selection of elderly patients for the first phase of the study were individuals who were 1) suffering from two or more chronic diseases (such as cerebrovascular disease, hypertension, hyperlipidaemia, diabetes, coronary heart disease, asthma); 2) taking medication for chronic diseases (including drugs and health products for the above six diseases); 3) willing to cooperate with follow-ups. The exclusion criteria were individuals who were 1) suffering from a severe or terminal disease; 2) suffering from a mental disorder or severe cognitive impairment; 3) unable to complete the questionnaire. The termination criteria included failure to follow up for various reasons and death.
Research Methods
We developed a plan to intervene in participants’ medication, based on the collected information. This prospective cohort study was divided into six steps as follows: 1) information collection, including the general demographic information of the patient, disease information and medication status; 2) analysis and evaluation of the current disease and medication status; 3) creation of the medication plan according to the patient’s personal information; 4) implementation of the plan by providing home medication under the guidance of a pharmacist; 5) satisfaction survey and follow-up; 6) documentation. The satisfaction questionnaire is shown in Appendix 1, and the specific service process is shown in Figure 1.
 |
Figure 1 Participant service process. |
We also calculated cost savings and hospitalisation expenditures. Cost savings were calculated by the sum of the prices of drugs discontinued after adjustment of the treatment regimen minus the sum of the prices of additional drugs and supplies purchased to improve patient adherence. Hospitalisation costs were the costs incurred during the hospital stay of the target population for the corresponding time.
Statistical Analysis
The analysis was performed using the SPSS Statistics (v.26.0) software. The measurement data conforming to a normal distribution were described by  , and the rank-sum test was used for the comparison between groups. Counting data were described using examples and percentages and then compared.
, and the rank-sum test was used for the comparison between groups. Counting data were described using examples and percentages and then compared.
Results
Overall Service Results
We investigated patient satisfaction to evaluate the overall effect. In total, 102 patients – 44 male and 58 female – received services, with a mean age of 85±17. Each patient typically had five types of chronic disease and took a mean of eight medicines to treat these chronic diseases. A total of 421 drug-related problems were found. The proportion of patients who completed this research programme was 95%, and 100% of the patients expressed satisfaction with the medication care services (see Table 1).
 |
Table 1 Basic Information and Satisfaction of Patients |
Problems Related to Drug Therapy
The drug treatment-related problems of patients were evaluated and analysed by a designated researcher, based on the four parameters of adaptability, efficacy, safety and compliance. A total of 421 drug treatment-related problems (a mean of 4.12 per person) were found in 102 patients, and of these, 392 problems were solved (a mean of 3.84 per person). The top three problems were 1) drug overtreatment (28.74%); 2) poor compliance (20.90%); 3) ineffective drugs (16.63%) (see Table 2). “Overtreatment” referred to patients who should be treated with a single drug but who use multiple drugs, patients for whom non-drug treatment is more suitable, based on their diseases, or patients who independently buy traditional Chinese medicine or healthcare products. “Poor compliance” referred to patients who had an insufficient understanding of how the medication works, forgot to take the medication or did not take the medication because they thought it was too expensive. Ineffective drugs were drugs that were taken without indication or the dose was too low.
 |
Table 2 Analysis and Summary of Drug Treatment Related Problems |
Each of the 102 patients had a mean of four or more existing or potential medication problems, and the top three – overtreatment, poor compliance and ineffective medications – accounted for more than half of the total medication-related issues; these will be the focus of future services. The primary reason for excessive drug treatment was that patients were taking multiple drugs for diseases that could be treated or controlled by one or two drugs (for example, insomnia patients taking lorazepam, zolpidem and melatonin tablets simultaneously). The primary reasons for insufficient drug treatment were that patients tried health products instead of drugs, ignored the symptoms of certain diseases (eg dizziness caused by high blood pressure), did not take antihypertensive drugs and needed to increase drug treatments. The primary reasons for poor compliance were the patients not fully understanding the role of the drug or being afraid of adverse drug reactions and stopping the medication secretly, as well as being fearful of taking medicine for life or forgetting to take the drug because they had poor memory. To resolve the abovementioned problems, we will refer the patient to the corresponding clinical department, fill in pharmacist–physician communication form 7, and let the patient take this form to see a doctor. The pharmacist will also communicate with the doctor to follow up.
In the current, the home pharmacy service helped patients solve 392 problems. On follow-up, it was found that more than 90% of patients could implement the action plan, and 75% could complete the tasks listed in the action plan. The action plan involved primarily adjusting the medicine dosage according to the plan, taking medication according to the adjusted correct dosage time and referring to the clinical department for treatment according to the recommendation. The main reasons for not being able to complete the action plan were not exercising according to the plan, not losing weight according to the plan, not maintaining strict diet control and not measuring blood pressure and blood sugar as planned.
As shown in Table 2, the patients had sufficient trust in the pharmacist to complete most of the tasks in the action plan. The reasons the patients could not fully implement the action plan were analysed through brainstorming, and the following were determined: 1) the actual situation of the patient was not fully considered while formulating the plan; 2) the action plan was not developed in detail; 3) the patient was unmotivated to change their daily habits, making the final implementation of the plan ineffective. Therefore, in the future, patients should actively participate in formulating action plans. Home pharmacists should pay attention to communicating with patients, understanding the actual situation of patients and adopting appropriate strategies to help patients achieve their goals. They should also enhance the patient’s self-confidence, validate and encourage the changes made by the patient and help them to realise that change is not difficult. The patient should not just be the executor of the entire treatment process but also a participant in its development. Home pharmacists should encourage patients to endorse the plan and proactively implement it to ensure that expectations are met.
Drug Economic Analysis
We analysed the changes in patient medical expenses. Based on the 392 problems solved related to drug treatment, RMB9,360.45 was saved in outpatient expenses (see Table 3). The mean hospitalisation times did not increase with the age of patients but decreased by 16%, and the cost of inpatient medical care decreased by RMB282,700 (see Table 4). The decrease in hospitalisation times and the cost of medical care could be attributed to (and further benefit) from home pharmacy services.
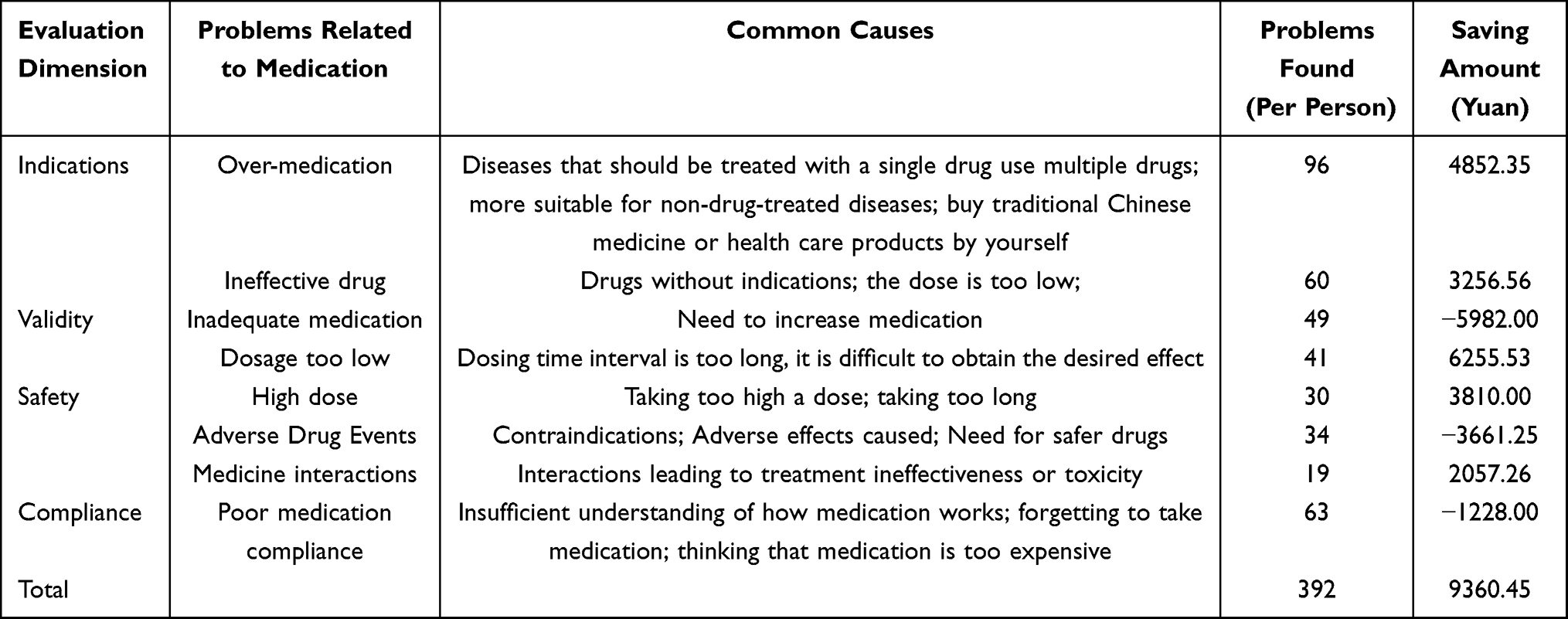 |
Table 3 Table of Cost Savings for Solving Problems Related to Drug Therapy |
 |
Table 4 Statistics of Hospitalization of Patients |
Discussion
Home pharmaceutical care refers to medical institutions providing individualised, whole-process and continuous pharmacy services and education for patients’ home drug treatment. Through this research, we found that the problems encountered during at-home pharmacy treatment could be solved, and the hospitalisation rate and treatment cost decreased compared with previous years’ records.
The findings of this study are consistent with those of existing studies that have demonstrated the benefits of home pharmaceutical care for various patient groups.12,13 Home pharmaceutical care can provide individualised, whole-process and continuous pharmacy services, as well as health education for patients with difficulties accessing community pharmacies or hospitals. Home pharmaceutical care can also enhance communication and collaboration among pharmacists, physicians, nurses and patients to optimise MTM and improve treatment outcomes.14 This study reports positive outcomes for home pharmaceutical care, such as medication safety, patient satisfaction, cost savings and a reduction in hospitalisations if combined with medical care and nursing. Other studies have also reported similar benefits of pharmaceutical home care services. However, research has also identified challenges, such as the need for better communication, coordination, reimbursement, training and resource provision for pharmacists in home care settings.15
Service Process and Model
We explored the service process and model of analysing Home Pharmaceutical Care in this study. Home pharmacy services imply that medical institutions deliver individualised, whole-process, continuous pharmacy services and promote health education for patients’ home drug treatment, carry out drug evaluation and education, help patients improve their drug compliance and ensure safe and reasonable drug storage and use. This can enhance the overall therapeutic effect.16 Home pharmacy services are currently well-developed in countries like Australia, the Netherlands, the United States, the United Kingdom, Canada, Taiwan and China.17–19 Home-based pharmacy services in mainland China started relatively late. There is no unified standard for the degree, method and impact of services provided by hospitals in various provinces and cities.20,21 In 2005 and 2018, the American Pharmacists Association and the American Chain Pharmacy Foundation Association successively announced the MTM service model, which includes five elements:20,22 medication therapy review; personal medication record; a medication-related action plan, intervention and/or referral; documentation; follow-up. The Medication Therapy Management Teaching and Practice Manual (2018) first proposed the concept of Chinese Drug Therapy Management (CMTM) and formulated the standard workflow of CMTM, which is divided into five steps: information collection; analysis and evaluation; plan formulation; planning execution; follow-up visits.21,23 The hospital’s home pharmacy service process has been developed by referring to the service models of MTM and CMTM in the United States and retaining the actual situation of the hospital in context. The process has six steps: interview and information collection; analysis and evaluation; plan formulation; plan implementation; satisfaction survey; follow-up and documentation. A satisfaction survey has been added to the service process of the hospital to help us better understand the needs of caring for the elderly. The home pharmacy service of our hospital is still in its infancy. By learning more, we can serve the elderly better, solve problems related to drug treatment, impart health education, focus on essential nutrition and physical exercise and help inculcate good habits and lifestyles in our patients. With this in mind, we designed the Home Pharmacy Service Effect Evaluation and Recommendation Form, which includes interviews with home pharmacists, details of their services and plans, the professional level expected of them and the referral and handover processes. It also includes topics like etiquette concerning dressing, speech and manners and the service mindset. This evaluation and suggestion form can help us understand the concerns and needs of patients and improve our service model and offerings.
Existing Problems and Improvement Measures
The home pharmacy service has established a standard service model and process, but it is still in its initial stage, and several problems still need to be addressed. There is a lack of educational equipment, making it difficult for home pharmacists to prepare pill boxes, teaching aids for administering drugs (eg insulin pens and inhalation preparation devices) and measuring instruments (eg blood glucose meters, sphygmomanometers, weight scales and tape measures). There is also a lack of necessary reference books, eg National Formulary, Clinical Diagnosis, Treatment Norms and Guidelines, Clinical Pathways and Pharmacy Service Procedures. Additionally, the importance of teamwork must be reinforced. Home pharmacists must work closely with family doctors, nurses and public health personnel. They also need to be aware of the patients’ understanding of the disease and their experience with medication, as well as explain the physician’s diagnosis and treatment to patients. Finally, pharmacists must manage drug treatment correctly. Therefore, cooperation between the physician and the pharmacist is required to serve patients better. In the future, pharmacists must strengthen communication and collaboration with physicians, engage more with clinicians in nursing centres and form a treatment team so that physicians can understand that pharmacists can solve medication problems for patients, thereby reducing physician workload. This will augment physicians’ acknowledgement of pharmacists and allow physicians to create active referrals.
Limitations of This Study
The research group is small and not representative of the Asian population, and there is a lack of high-quality evaluation criteria. The study did not compare home pharmaceutical care outcomes with other care models, such as community pharmacy or hospital pharmacy services. This study reflects only a preliminary research discussion. Due to limitations in sample size and an inability make comparisons with other nursing models, the results of this study cannot represent the Asian region. In the future, additional research methods, such as randomised controlled studies and survey research, are needed to conduct specific data analysis and in-depth research on the current factors influencing family pharmacy services.
Conclusion
In summary, the home pharmacy service in the hospital’s medical and nursing integration model can help patients solve medication-related problems and reduce the number of hospitalisations and medical expenses through a standardised service model that offers patients safe, effective, economical and rational drug use. Therefore, providing home pharmacy services under the format of combined medical and nursing care is feasible.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Hebei Yanda Hospital. Written informed consent was obtained from all participants.
Funding
Hebei Pharmaceutical Society Hospital Pharmaceutical Research Special Project (2020-Hbsyxhqn0034).
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately.
References
1. Fujita K, Kushida K, Moles RJ, et al. Home healthcare professionals’ perspectives on quality dimensions for home pharmaceutical care in Japan. Geriatr Gerontol Int. 2019;19(1):35–43.
2. Lee CY, Su HH, Chang YC, Tsai TH, Lai YR, Huang KH. The impact of pharmaceutical home care on medical utilization for frequent users of outpatient services in Taiwan. Int J Environ Res Public Health. 2021;18(14):7336. doi:10.3390/ijerph18147336
3. Cai M, Xie XQ, Wu SY. Health status and health service utilization of the elderly population in my country. Chin J Health Inf Manag. 2021;18(1):27–34.
4. Wu TX, Xing Y, Huang F, Chang X, Yu JX. Evaluation of medication status and pharmacist’s intervention effect in elderly multidrug inpatients. China Pharm. 2019;30(22):3150–3154.
5. Chen ZY, Li F, Zhao ZG, Sun LL. Research progress of pharmacists’ participation in polypharmacy management in elderly patient. Chin J Hospital Pharm. 2018;38(4):450–453.
6. Xianji Network. Analysis of the status quo of chronic diseases at home and abroad and the status and pain points of chronic diseases in my country. Available from: https://www.xianjichina.com/news/details172910.html.
7. Liu YQ. Research on the Status Quo of Chronic Disease Prevention and Control in Hebei Province Thesis. Hebei Medical University; 2020: 6.
8. Fathollahi-Fard AM, Ahmadi A, Karimi B. Multi-objective optimization of home healthcare with working-time balancing and care continuity. Sustainability. 2021;13(22):12431.
9. Fard AF, Keshteli MH, Moghaddam RT, et al. Bi-level programming for home health care supply chain considering outsourcing. J Industr Inf Integr. 2021;25:100246.
10. Benjamin MB. Definition of medication therapy management: development of professionwide consensus. J Am Pharm Assoc. 2005;45(5):566–572. doi:10.1331/1544345055001274
11. Rational Drug Use Encyclopedia & Pharmacy Tool Network. Implementing home pharmacy services to reflect the professional value of pharmacists. Available from: https://www.sohu.com/a/314447106-120051604.
12. Kushida K, Hirohara M. Advanced pharmaceutical management functions in home pharmaceutical care. Yakugaku Zasshi. 2020;140(7):877–884. doi:10.1248/yakushi.19-00237-5
13. Berenguer B, La Casa C, de la Matta MJ, Martín-Calero MJ. Pharmaceutical care: past, present and future. Curr Pharm Des. 2004;10(31):3931–3946. doi:10.2174/1381612043382521
14. Dodd MA, Haines SL, Maack B, et al. ASHP statement on the role of pharmacists in primary care. Am J Health Syst Pharm. 2022;79(22):2070–2078. doi:10.1093/ajhp/zxac227
15. Shi J, Chen N, Liu N, et al. Options for care of elderly inpatients with chronic diseases: analysis of distribution and factors influencing use of care in Shanghai, China. Front Public Health. 2021;9:631189. doi:10.3389/fpubh.2021.631189
16. Cao AL, Ding N, Meng L, Yang HY, Yang N, Zhang TJ. Pharmacy service specification for medical institutions part 8 home pharmacy service. China Pharm. 2019;30(24):3321–3324.
17. Theising KM, Fritschle TL, Scholfield AM, Hicks EL, Schymik ML. Implementation and clinical outcomes of an employer sponsored, pharmacist provided medication therapy management program. Pharmacotherapy. 2015;35(11):e159–e163. doi:10.1002/phar.1650
18. Wang JL, Qiao YR, Shih YC, et al. Potential health implications of medication therapy management eligibility criteria in the patient protection and affordable care act across racial and ethnic group. J Manag Care Spec Pharm. 2015;21(11):993–1003. doi:10.18553/jmcp.2015.21.11.993
19. Cipolle RJ, Linda M, Peter C, Morley KZ, Jin YY, Zhu Z. Translation. Pharmacy Care Practice Methods Patient-Centered Medication Management Services Original Book.
20. Wu MF, Zhu B, Liu X, Zhao ZG. Exploration and practice of outpatient service model of drug therapy management (MTM). Zhongnan Pharm. 2019;17(08):1336–1341.
21. Tian LL, Zhu DQ. Research progress of home pharmaceutical services. Shanxi Med J. 2020;49(15):1962–1964.
22. Li D, Yan SY. Teaching and Practice Manual of Drug Therapy Management. Beijing: People’s Health Publishing House; 2018:237.
23. Tan YH. The implementation and effect of home care for pharmaceutical affairs in Taiwan. China Licensed Pharm. 2012;9(11):13–16.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.