Back to Journals » Journal of Pain Research » Volume 19
An Overview of Ischemic Preconditioning as a Potential Therapeutic Target for Chronic Muscle Pain
Received 12 June 2025
Accepted for publication 26 December 2025
Published 13 January 2026 Volume 2026:19 546782
DOI https://doi.org/10.2147/JPR.S546782
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wendy Imlach
Qi Zhang,1 Jian Luo2
1School of Acupuncture and Tuina, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 2Department of Tuina, Hospital of Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China
Correspondence: Jian Luo, Email [email protected]
Abstract: Chronic pain is a prevalent and highly disabling condition, affecting approximately 31% of the global population. Among its various forms, musculoskeletal disorders—particularly Myofascial Pain Syndrome (MPS)—account for a significant proportion. MPS is characterized by muscle spasms, localized ischemia, and pain, making it more easily diagnosable due to its distinct physical signs. Ischemic Preconditioning (IPC), a protective mechanism induced by brief cycles of ischemia followed by reperfusion, has demonstrated promising effects in studies involving cardiac and skeletal muscle tissues. Based on this, we hypothesize that cyclic compressive loading, which induces temporary local ischemia followed by reperfusion, may simulate the physiological effects of IPC. This approach could potentially alleviate ischemia-related muscle spasms and reduce chronic pain. To test this hypothesis, this paper begins with a review of the basic physiological mechanisms underlying ischemia and reperfusion injury, analyzing the relevant molecular pathways. It then systematically examines the protective effects of IPC in skeletal muscle, including the reduction of oxidative stress, suppression of inflammatory responses, and promotion of blood flow restoration. Furthermore, we compare the controllability and limitations of traditional massage, ischemic compression, and mechanically simulated IPC devices within therapeutic designs. In summary, this study provides theoretical support and a feasible framework for non-pharmacological interventions based on IPC mechanisms in the treatment of chronic muscular pain. It lays a foundational hypothesis for the development of standardized and scalable therapeutic devices, offering a stronger scientific basis for chronic pain management and presenting new strategies to address this growing public health challenge.
Keywords: chronic pain, myofascial pain syndrome, ischemic preconditioning, massage, cyclic compressive loading
Introduction
Chronic pain is a prevalent health issue. Unlike acute pain, which serves a survival function, chronic pain should be considered an independent disease with significant consequences for both individuals and society.1 Chronic pain is typically defined as pain lasting more than 12 weeks. This type of pain can originate from any part of the body and may continue even in the absence of a clear underlying injury or cause. Chronic pain is not simply an extension of acute pain; it encompasses a complex interplay of physiological, psychological, and social factors, significantly affecting patients’ quality of life. According to data from the World Health Organization and various international studies, the global prevalence of chronic pain is approximately 31%.2 As the population ages, the incidence of chronic pain is also increasing. Population studies in the United States and worldwide indicate that the prevalence of chronic pain is notably higher among individuals aged 65 and older compared to the general adult population.3 Chronic pain not only severely impacts an individual’s quality of life but also imposes a significant economic burden on families and society.4 Patients may lose their ability to work due to pain, resulting in a reduction in income. Simultaneously, the long-term costs of treatment and care can further exacerbate economic pressure. Consequently, chronic pain is increasingly recognized as a critical public health issue that necessitates attention and support from all sectors of society to promote the development of early diagnosis, effective management, and preventive measures.
The Complexity of Chronic Pain
The causes of chronic pain are intricate and complex, and the terminology patients use to describe their pain sensations can vary significantly. For instance, terms such as “soreness”, “fullness”, and “sharp pain” may be interpreted differently by different individuals and at various times. This variability complicates the ability of doctors to accurately assess the nature of the pain in clinical practice, making it challenging to identify the underlying cause and effectively manage the pain thereafter.5 In clinical practice, we have consistently observed a specific group of chronic pain patients characterized by palpable pain points on the surface of the body, often accompanied by increased muscle tone and localized muscle spasms. This phenomenon is typically diagnosed as myofascial pain syndrome (MPS). MPS is a common musculoskeletal pain condition that primarily affects the muscles and the surrounding fascial structures.6,7 According to an epidemiological study, MPS accounts for up to 85% of patients reporting chronic pain.8 A primary characteristic of MPS is the presence of one or more specific sensitive areas, tender spots, or taut bands in the affected muscles and fascia, commonly referred to as trigger points.9 In this context, we may not take fibromyalgia into consideration, as patients with fibromyalgia experience more widespread pain, with symmetrically distributed tender areas in the soft tissues.8 The local tenderness generally shows no inflammatory changes, and its mechanism is often associated with central sensitization.
Hypotheses on the Pathomechanism of MPS
The currently accepted hypothesis regarding the pathological mechanism of MPS was proposed by Simons.10 This hypothesis posits that repeated low-intensity muscle overload or intense muscle contractions can lead to muscle damage, resulting in dysfunction at the neuromuscular junction. This dysfunction increases the release of acetylcholine (ACh) in the synaptic cleft, triggering high-frequency miniature endplate potentials, which leads to sustained depolarization of the muscle.11 This process causes an increase in calcium ion release, resulting in continuous muscle contraction and the development of a spasm state, which compresses blood vessels and causes local ischemia and hypoxia. During ischemia, released inflammatory mediators further activate pain receptors, leading to hyperalgesia. Additionally, ischemia may exacerbate damage to the neuromuscular junction and activate acetylcholinesterase, promoting the release of ACh and creating a vicious cycle. In this process, energy loss due to ischemia and the increased energy demand for calcium pump activation also become critical factors.11 This energy crisis exacerbates the vicious cycle, further promoting the persistence and intensification of pain.
Skeletal Muscle Spasm Ischemic State
Muscle spasm at the trigger point is described as a sustained, involuntary muscle contraction (distinct from central nervous origin spasms, which are often confused).12 Studies have shown that pain from muscle spasm is primarily due to muscle ischemia, which decreases pH and releases pain mediators like bradykinin, ATP, and H⁺.13–15 Based on this analysis, it is posited that Roger H. Coletti’s proposed ischemic model of chronic muscle cramps and pain merits further consideration. One significant, if not the predominant, etiology of chronic pain is chronic muscle cramps. Extended episodes of muscle cramps, irrespective of their underlying cause, can restrict the muscle’s blood supply.16 Normal functioning of both skeletal and cardiac muscles depends on adequate blood supply. However, compared to myocardial ischemia, skeletal muscle ischemia has been less extensively studied and understood. Myocardial ischemia is primarily caused by coronary artery stenosis,17 and even simple ischemia of the coronary arteries can lead to the phenomenon known as “hibernating myocardium”. Chronic ischemia can lead to fibrosis and scarring in the affected areas, causing pathological remodeling that stiffens the myocardium and impairs diastolic function,18 potentially resulting in heart failure if left unchecked. Over time, the body adapts to chronic myocardial ischemia, with myocardial contractile function decreasing in proportion to reduced local blood flow. This results in a “perfusion-contraction match” state.19 Myocardial ischemia induces tachycardia less frequently, reducing energy loss by regulating contractile function and metabolism. This allows the myocardium to adapt to a low perfusion environment while awaiting vascular regeneration. By reducing energy demand, hibernating myocardium adapts to reduced blood flow, conserving oxygen and protecting cardiomyocytes from necrosis. This process is potentially reversible.20 If blood flow is restored, the hibernating myocardium can return to normal function.21 Therefore, in the treatment of myocardial ischemic diseases, restoring blood flow in the affected vessels is often the primary goal. This is particularly crucial in cases of extensive acute myocardial ischemia that are life-threatening. Early reperfusion achieved through thrombolytic therapy and other interventions has been proven to effectively reduce the incidence of acute myocardial infarction.17 However, subsequent studies have revealed that although reperfusion can save patients’ lives in the short term, it may also induce damage even more severe than ischemia itself, hindering long-term recovery. Consequently, reducing reperfusion injury has become another major research focus.22 Studies by Ugo Carraro et al have demonstrated that skeletal muscle under chronic spastic conditions exhibits adaptive changes similar to the “hibernation” phenomenon observed in the myocardium.23,24 Persistent muscle spasm can lead to chronic local ischemia and may result in a reversible ischemic state. Although skeletal muscle is generally more tolerant to ischemia than cardiac muscle, reperfusion following prolonged ischemia may still exacerbate tissue injury.
Mechanisms of Spastic Ischemic Injury and Reperfusion Injury in Skeletal Muscle
If the muscles persist in a state of continuous contraction, they may develop spasms that compress the blood vessels, consequently resulting in ischemia and hypoxia within the affected tissues. In an ischemic environment, the continuous accumulation of cellular metabolic byproducts occurs, leading to metabolic acidosis.25 Upon restoration of blood supply, the local inflammatory response is likely to intensify, accompanied by a significant increase in the production of reactive oxygen species (ROS), which may contribute to secondary tissue damage. During skeletal muscle ischemia, the metabolic and ionic imbalances resulting from inadequate oxygen supply in the blood are significant contributors to tissue damage. Increasing evidence indicates that ROS can rapidly accumulate during the early stages of striated muscle ischemia, even in conditions of limited oxygen availability. In this context, xanthine oxidase (XO) serves as the primary source of ROS production. Ischemic conditions can activate XO in the endothelial cells of skeletal muscle, thereby facilitating the extensive generation of ROS. Excessive ROS can cause damage to cell membranes via lipid peroxidation. Concurrently, ischemia and hypoxia can disturb the physiological equilibrium of cells, resulting in an inadequate energy supply.26 Decreased levels of adenosine triphosphate (ATP) can diminish the activity of the energy-dependent Na⁺-K⁺-ATPase, consequently leading to an increase in intracellular sodium (Na⁺) concentration. To preserve the stability of the membrane potential, the Na⁺-Ca2⁺ ion exchange mechanism is activated to decrease the intracellular Na⁺ concentration. However, this compensatory mechanism results in an elevation of intracellular Ca2⁺ concentration.22 The accumulation of hydrogen, sodium, and calcium ions within the cell creates a hypertonic intracellular environment, prompting water to influx into the cytoplasm and leading to cellular swelling.27 Intracellular calcium overload transpires during the ischemic phase and is exacerbated during reperfusion.28 The elevation of intracellular Ca2⁺ concentration activates the mitochondrial permeability transition pore (mPTP), resulting in the release of pro-apoptotic factors, including cytochrome C and apoptosis-inducing factor (AIF), into the cytoplasm, which subsequently leads to cell death (Figure 1).29 Research has found that during endothelial ischemia, the expression of certain pro-inflammatory gene products, such as leukocyte adhesion molecules and cytokines, is promoted, inducing the body into a pro-inflammatory state.30,31 In the reperfusion phase, the restored blood flow delivers oxygen to the ischemic tissue through red blood cells. However, due to the lower concentration of antioxidants in ischemic cells, the production of ROS further increases. The massive generation of ROS triggers a more severe inflammatory response, a process that involves the activation, chemotaxis, adhesion, and migration of leukocytes with endothelial cells.30,32 These reactions work together to exacerbate muscle tissue damage. The interaction between leukocytes and vascular endothelium includes a series of different steps, characterized by leukocyte “rolling” on the endothelium, firm adhesion of leukocytes to the endothelium, and endothelial migration33 (Figure 2).
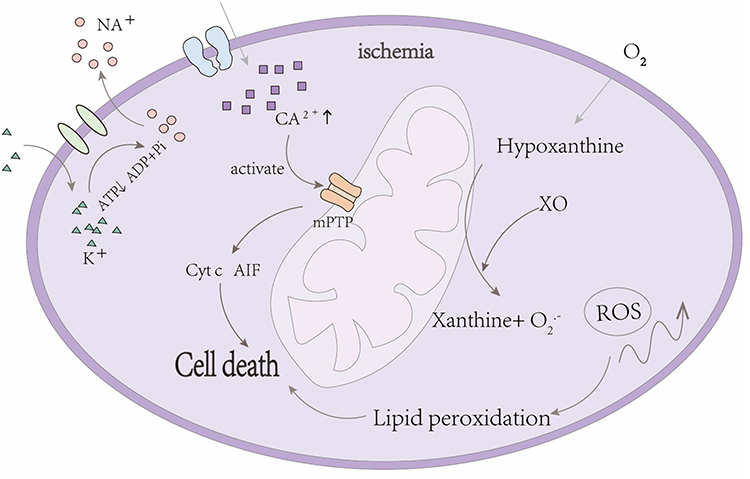 |
Figure 1 Ischemia induces the activation of xanthine oxidase (XO) in the endothelial cells of skeletal muscle. The enzyme XO facilitates the conversion of hypoxanthine to xanthine in the presence of molecular oxygen (O2), which subsequently leads to the generation of reactive oxygen species (ROS). The excessive accumulation of ROS results in lipid peroxidation, thereby compromising the integrity of the cell membrane. Simultaneously, diminished levels of adenosine triphosphate (ATP) reduce the functionality of the energy-dependent Na+-K+-ATPase, resulting in an increase in intracellular sodium (Na+). In an effort to preserve the membrane potential, the Na+-Ca2+ ion exchange mechanism is activated to decrease intracellular Na+ concentration; however, this compensatory response inadvertently elevates intracellular calcium (Ca2+) levels. The increase in intracellular Ca2+ concentration activates the opening of the mitochondrial permeability transition pore (mPTP), which facilitates the release of apoptotic factors, such as cytochrome c and apoptosis-inducing factor (AIF), into the cytoplasm, ultimately triggering the process of cell death. |
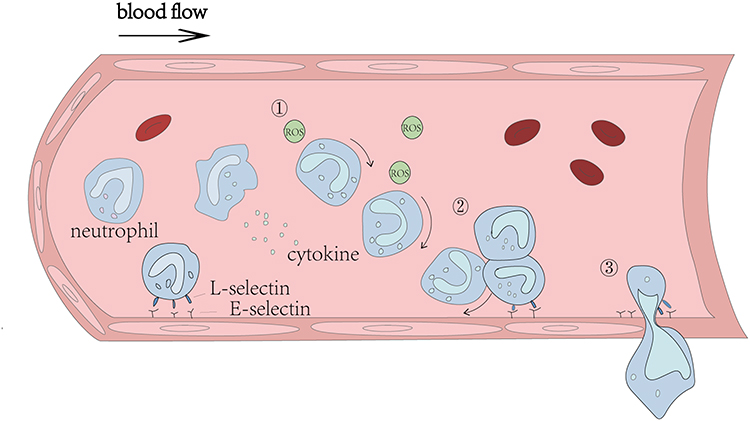 |
Figure 2 The concentration of antioxidants is diminished in the context of ischemia, while the production of reactive oxygen species (ROS) is markedly elevated. The increase in ROS instigates a substantial inflammatory response. Within the vascular system, this inflammatory response is predominantly facilitated by the adhesion of neutrophils and their subsequent migration across the vascular endothelial cells. Simultaneously, macrophages are activated to secrete pro-inflammatory cytokines, such as interleukin-6 and interleukin-1β, which further exacerbate this inflammatory process. The interaction of leukocytes with the vascular endothelium occurs through a series of distinct stages, including: ① leukocyte rolling on the endothelium, ② firm adhesion of leukocytes to the endothelium, and ③ endothelial migration. The process of leukocyte rolling is primarily initiated by the interaction between L-selectin, which is expressed on leukocytes, and E-selectin, which is expressed on endothelial cells. |
Ischemic Compression and Ischemic Preconditioning
Ischemic compression has been utilized for decades as a non-invasive manual therapy technique in the treatment of MPS.34,35 This technique involves applying sustained pressure to the trigger point or its vicinity, typically for 30 to 90 seconds.36 Although mechanical pressure on the trigger point or surrounding area may immediately trigger or exacerbate pain, it can also worsen local ischemia, followed by blood reperfusion. This physiological process increases muscle metabolism, which may help alleviate pain symptoms.37 However, some studies have suggested that there is currently insufficient evidence to support the significant benefits of ischemic compression in pain relief,38 and there remains no clear conclusion regarding whether reperfusion may exacerbate local muscle damage. For patients experiencing this type of pain, we continue to seek effective treatment methods. In 1986, Reimer et al first identified and described the phenomenon of “ischemic preconditioning (IPC)”, which has since been validated by numerous experimental studies.39 IPC refers to the phenomenon where short periods of cyclic tissue ischemia and reperfusion provide subsequent protection against greater ischemia-reperfusion-induced damage. IPC activates the protective mechanisms of tissues against subsequent damage through multiple short ischemic periods.40 This discovery offers a new strategy for cardioprotection in coronary artery disease and holds promise for protecting vital organs, such as the brain, kidneys, and liver, from ischemic injury during surgery.41–43 Ischemic preconditioning is not limited to the heart, brain, kidneys, and liver but is also applicable to skeletal muscle.44 Some studies have also shown that IPC can enhance athletic performance by increasing muscle blood flow and oxygen delivery, which is important for training and performance optimization.45 Skeletal muscle is a vital component of the human body, consisting of muscle fibers. Skeletal muscle contraction is essential for nearly all body activities, and muscle strength directly influences endurance and physical capacity. Adequate blood supply is essential for the normal physiological metabolism of tissues. Tissue ischemia, caused by various factors, can lead to metabolic abnormalities in cells and tissues, resulting in damage. Numerous studies have shown that ischemic preconditioning can improve skeletal muscle ischemia and reperfusion injury through certain mechanisms.46–48
Ischemic Preconditioning Mechanisms
Current studies have demonstrated the protective effects of ischemic preconditioning (IPC) against ischemic injury and reperfusion, and have preliminarily elucidated its potential underlying mechanisms. These mechanisms mainly include the reduction of oxidative stress, inhibition of inflammatory responses, and promotion of increased blood flow.
Reducing Oxidative Stress
Studies have demonstrated that under ischemic conditions, XO is activated in the endothelial cells of skeletal muscle, resulting in an increased production of ROS. This rise in ROS can lead to cell membrane damage through lipid peroxidation. When blood flow is restored to ischemic tissues, XO interacts with oxygen to facilitate the conversion of hypoxanthine into xanthine and uric acid, a process that releases superoxide (O2•−) and hydrogen peroxide (H2O2), thereby exacerbating oxidative stress within the tissue.26 The role of ROS is multifaceted: while elevated levels of ROS contribute to cellular oxidative damage, lower concentrations can function as signaling molecules that activate protective preconditioning pathways.49 In this context, the MitoK_ATP channels play a critical role in skeletal muscle ischemic preconditioning.50 It has been suggested that the activation of this channels induces the generation of ROS. In a hypoxic environment, the activation of the MitoK_ATP channel facilitates the synthesis of nitric oxide (NO) and ROS. This activation subsequently prolongs the duration of channel activation via a feedback mechanism. This feedback loop further enhances the production of ROS and NO, which serve as signaling mediators to initiate additional protective preconditioning mechanisms.51 The protective effect of IPC is primarily mediated through several critical signaling pathways, including the mitogen-activated protein kinase (MAPK) pathway,52 the phosphoinositide 3-kinase (PI3K)-Akt pathway,53 and the protein kinase C-epsilon (PKCε) pathway.54 These pathways are essential for the protection of skeletal muscle, as they regulate ion channel function, stabilize cell membrane structure, and inhibit the expression of pro-apoptotic factors. Meanwhile, IPC can upregulate the expression of endogenous antioxidant enzymes, such as superoxide dismutase 2 (SOD2) and catalase, thereby enhancing the cellular capacity to eliminate reactive oxygen species (ROS).55 Notably, exosomes also play an important role in antioxidant responses. Exosomes released in response to IPC stimulation carry various antioxidant-related microRNAs (such as miR-21 and miR-126), which can be taken up by target cells to activate the PI3K–Akt signaling pathway, consequently strengthening the antioxidant defense capacity of recipient cells.56
Reducing the Inflammatory Response
Studies have shown that in peripheral tissues, the beneficial effects of IPC are associated with the inhibition of leukocyte adhesion and migration. Particularly in the small intestine, IPC prevents post-ischemic leukocyte adhesion, thereby reducing the inflammatory response by maintaining the bioavailability of nitric oxide and inhibiting the expression of P-selectin.57 The impact of IPC on the inflammatory system is multifaceted, encompassing the regulation of cytokine and chemokine expression. In rats, remote ischemic preconditioning (RIPC) performed prior to prolonged tourniquet application on the hind limb resulted in reduced inflammatory cell responses, decreased rates of apoptotic cell death, and improved microcirculation. At the molecular level, the expression of pro-inflammatory genes decreases, while the expression of genes associated with alleviating oxidative stress increases, indicating that RIPC mitigates inflammation and oxidative damage through the regulation of gene expression. The protective effects of ischemic preconditioning include downregulation of inflammation and reduction of neutrophil activation, as well as leukocyte-endothelial cell interactions. These effects may be mediated through the tumor necrosis factor-alpha (TNF-α) signaling pathway, with TNF-α playing a crucial role in the development of ischemic tolerance and neurotoxicity. TNF-α can activate NF-kB, which has both pro-inflammatory and cytotoxic effects, as well as anti-inflammatory and cytoprotective properties.58
Promoting Increased Blood Flow
Vascular Endothelial Growth Factor (VEGF) is a critical cell growth factor that is expressed under ischemic conditions in tissues. It plays a vital role in angiogenesis and enhancing blood flow by promoting the formation of new blood vessels and the branching extension of existing ones, thereby mitigating ischemia-reperfusion injury.59 Yoo and other researchers reported the expression pattern of VEGF in IPC. In addition, exosomes can directly deliver VEGF to recipient cells or regulate its gene expression, thereby enhancing angiogenic capacity.56 When investigating the functions of endothelial cells in skeletal muscle, Hotta et al found that extracellular mechanical stimuli, such as shear stress and tensile stress, can trigger biochemical reactions within vascular endothelial cells, thereby initiating the process of angiogenesis.60 The concept of IPC being consistent with massage (as a mechanical factor) in inducing cellular changes aligns with the notion that these changes convert mechanical energy into molecular signals, leading to various cellular responses, including increased expression of angiogenic factors, such as VEGF-A.61 Furthermore, the production of ROS results in a decrease in the generation of nitric oxide (NO), which, as a vasodilator, can inhibit platelet aggregation and leukocyte adhesion. The reduction in NO production diminishes tissue blood flow.59 Research on the effects of IPC on superficial blood flow has revealed that vasodilation is one of the primary mechanisms by which IPC exerts its enhancing effects. In fact, studies have demonstrated that repeated IPC within a month can elevate the levels of endothelium-dependent vasodilators, such as NO.62
Formulation of the Hypothesis
Chronic pain is an increasingly prevalent and distressing condition that imposes substantial physiological, psychological, and economic burdens on individuals and society. MPS is one of the common types of chronic pain, characterized by localized muscle spasm, ischemia, and pain, forming a vicious cycle that is difficult to break. Persistent muscle contraction leads to local ischemia and hypoxia, resulting in metabolic disturbances and oxidative stress, which further aggravate pain and muscle spasm. IPC, as a non-invasive intervention, activates endogenous protective mechanisms through repeated cycles of ischemia and reperfusion. It has been shown to alleviate ischemia–reperfusion injury in organs such as the heart, liver, and skeletal muscle, and no significant safety concerns have been reported to date.63–65 Its protective mechanisms include reducing oxidative stress, suppressing inflammatory responses, and promoting angiogenesis. Given that similar pathophysiological processes—ischemia, oxidative stress, and inflammation—are also present in MPS, these protective effects of IPC may have potential value in alleviating muscle spasm and improving local blood flow. Based on the above analysis, we propose the hypothesis that ischemic preconditioning may help improve local muscle spasm and ischemic conditions in patients with myofascial pain syndrome, thereby relieving chronic pain. However, most current studies on skeletal muscle IPC utilize a tourniquet occlusion method—temporarily restricting blood flow and then releasing the tourniquet to allow reperfusion. While this approach is effective for limb muscles, it is not easily applicable to the whole body and lacks the precision to target specific local muscles. Given that IPC operates on a cyclical pattern of “ischemia–reperfusion–ischemia”, we drew a connection to a traditional therapeutic modality—massage—which seems to follow a similar cycle. Through repetitive manual manipulation, massage exerts mechanical pressure on localized areas, mimicking the IPC cycle to some extent. Compared to ischemic compression techniques, massage emphasizes the repeatability of mechanical force, potentially reducing the risk of damage from excessive blood reperfusion (Figure 3). However, it is clear that the pressure, frequency, and duration of massage are difficult to standardize or control, making it challenging to replicate the optimal timing and cycle count required for IPC. To address these limitations, some researchers have referred to a therapeutic device developed by Butterfield et al in 2008, which simulates Swedish massage in humans.66 This device applies rhythmic compressive loads to muscles, allowing for control over force magnitude and direction, with the pressure sustained over a defined duration.67 A limitation of this approach is that the device cannot fully replicate the nuanced curvature and adaptability of a therapist’s fingers. Still, future developments in device design may overcome this shortcoming.
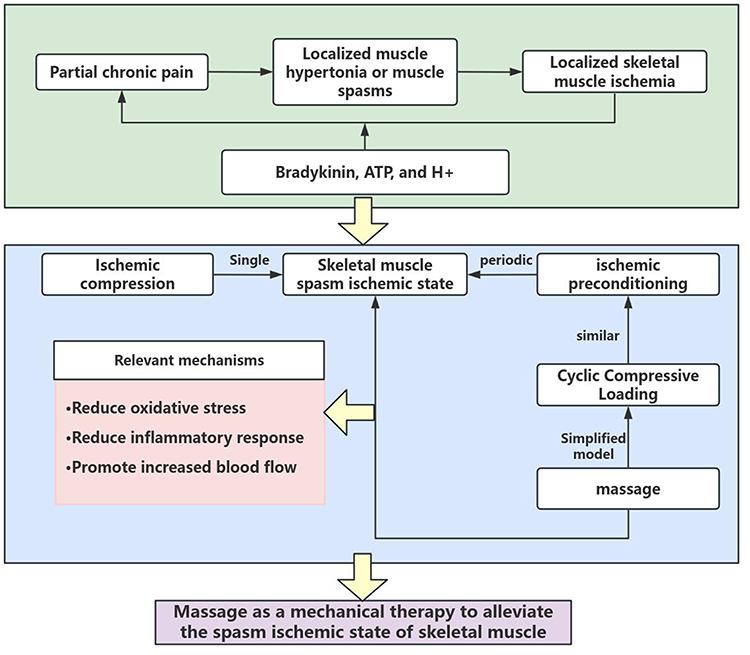 |
Figure 3 A graphical representation of the relationship between ischemic preconditioning and massage therapy in the context of chronic muscle pain. |
Conclusions
Accordingly, for patients with chronic pain—particularly those exhibiting localized muscle spasm and ischemia—new technologies that simulate ischemic preconditioning may represent a promising therapeutic option. By externally mimicking the physiological process to activate endogenous protective mechanisms, such approaches may offer novel strategies for the management of chronic pain. Although ischemic compression can induce a localized muscle ischemic state to some extent, it inevitably carries the potential risk of reperfusion injury. In contrast, mechanical devices have higher controllability in parameter settings (such as pressure intensity, duration, frequency, etc)., which helps to more accurately simulate the timing and cycles of IPC. However, existing devices are mostly focused on specific areas or single muscle groups, and are still insufficient in terms of clinical application and whole-body adaptability. Future treatment devices should fully consider these factors in their design and aim to improve the flexibility of the devices as much as possible. In comparison, massage is more suitable for clinical practice, but traditional massage lacks a standardized operational system. Different therapists may vary in the direction and intensity of the applied force, leading to inconsistent and difficult-to-verify therapeutic effects. In addition, the therapeutic effect of massage may not only come from mechanical manipulation itself, but may also involve psychological benefits brought by tactile sensation.68 Studies have found that the effects of IPC may be closely related to blood flow perfusion volume, duration of a single ischemic episode, and the number of ischemia–reperfusion cycles.69,70 To further explore intervention strategies for skeletal muscles under spasm and ischemia, the current treatment method can be simplified into a type of mechanical therapy. This involves applying directional, intermittent pressure to localized muscles to induce temporary ischemia, then releasing the pressure to restore blood perfusion, forming a repeated cycle of “ischemia–reperfusion”. This not only helps to standardize mechanistic studies, but also facilitates future laboratory modeling and clinical validation. At present, the specific settings of various parameters (blood perfusion volume, single ischemia duration, number of cycles) in IPC remain a new challenge and have guiding significance for the formulation of clinical treatment protocols. A systematic and in-depth study of these variables has important theoretical and practical value for the future development of scientific, standardized treatment strategies and the construction of scalable mechanical devices or massage technique standards.
Abbreviations
MPS, myofascial pain syndrome; IPC, Ischemic preconditioning; ACh, acetylcholine; VEGF, vascular endothelial growth factor; ROS, reactive oxygen species; XO, xanthine oxidase; ATP, adenosine triphosphate; mPTP, mitochondrial permeability transition pore; AIF, apoptosis-inducing factor; RIPC, remote ischemic preconditioning; TNF-α, tumor necrosis factor-alpha.
Acknowledgments
We would like to express our gratitude to our colleagues for their valuable discussions and feedback throughout this study.
Funding
This research was supported by the Sichuan Administration of Traditional Chinese Medicine (No. 2023MS534) and Guangan social field key research and development project (No. 2023SYF03).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–10. doi:10.1016/s0140-6736(21)00393-7
2. Steingrímsdóttir ÓA, Landmark T, Macfarlane GJ, Nielsen CS. Defining chronic pain in epidemiological studies: a systematic review and meta-analysis. Pain. 2017;158(11):2092–2107. doi:10.1097/j.pain.0000000000001009
3. Domenichiello AF, Ramsden CE. The silent epidemic of chronic pain in older adults. Prog Neuropsychopharmacol Biol Psychiatry. 2019;93:284–290. doi:10.1016/j.pnpbp.2019.04.006
4. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
5. Mense S. Muscle pain: mechanisms and clinical significance. Dtsch Arztebl Int. 2008;105(12):214–219. doi:10.3238/artzebl.2008.0214
6. Kuan TS. Current studies on myofascial pain syndrome. Curr Pain Headache Rep. 2009;13(5):365–369. doi:10.1007/s11916-009-0059-0
7. Urits I, Charipova K, Gress K, et al. Treatment and management of myofascial pain syndrome. Best Pract Res Clin Anaesthesiol. 2020;34(3):427–448. doi:10.1016/j.bpa.2020.08.003
8. Steen JP, Jaiswal KS, Kumbhare D. Myofascial pain syndrome: an update on clinical characteristics, etiopathogenesis, diagnosis, and treatment. Muscle Nerve. 2025;71(5):889–910. doi:10.1002/mus.28377
9. Rivers WE, Garrigues D, Graciosa J, Harden RN. Signs and symptoms of myofascial pain: an international survey of pain management providers and proposed preliminary set of diagnostic criteria. Pain Med. 2015;16(9):1794–1805. doi:10.1111/pme.12780
10. Simons DG. Review of enigmatic MTrPs as a common cause of enigmatic musculoskeletal pain and dysfunction. J Electromyogr Kinesiol. 2004;14(1):95–107. doi:10.1016/j.jelekin.2003.09.018
11. Travell JG, Simons DG. Myofascial Pain and Dysfunction: The Trigger Point Manual. Vol. 2. Lippincott Williams & Wilkins; 1992.
12. Therkildsen ER, Kaster P, Nielsen JB. A scoping review on muscle cramps and spasms in upper motor neuron disorder-two sides of the same coin? Front Neurol. 2024;15:1360521. doi:10.3389/fneur.2024.1360521
13. Issberner U, Reeh PW, Steen KH. Pain due to tissue acidosis: a mechanism for inflammatory and ischemic myalgia? Neurosci Lett. 1996;208(3):191–194. doi:10.1016/0304-3940(96)12576-3
14. Birdsong WT, Fierro L, Williams FG, et al. Sensing muscle ischemia: coincident detection of acid and ATP via interplay of two ion channels. Neuron. 2010;68(4):739–749. doi:10.1016/j.neuron.2010.09.029
15. Santos D, Melo Aquino B, Jorge CO, et al. Muscle pain induced by static contraction in rats is modulated by peripheral inflammatory mechanisms. Neuroscience. 2017;358:58–69. doi:10.1016/j.neuroscience.2017.06.041
16. Coletti RH. The ischemic model of chronic muscle spasm and pain. Eur J Transl Myol. 2022;32(1). doi:10.4081/ejtm.2022.10323
17. Xiang Q, Yi X, Zhu XH, Wei X, Jiang DS. Regulated cell death in myocardial ischemia-reperfusion injury. Trends Endocrinol Metab. 2024;35(3):219–234. doi:10.1016/j.tem.2023.10.010
18. Prabhu SD, Frangogiannis NG. The biological basis for cardiac repair after myocardial infarction: from inflammation to fibrosis. Circ Res. 2016;119(1):91–112. doi:10.1161/circresaha.116.303577
19. Heyndrickx G. Hibernating myocardium. In: New Paradigms of Coronary Artery Disease: Hibernation, Stunning, Ischemic Preconditioning. 1996:36–38.
20. Bhatia G, Sosin M, Leahy JF, Connolly DL, Davis RC, Lip GY. Hibernating myocardium in heart failure. Expert Rev Cardiovasc Ther. 2005;3(1):111–122. doi:10.1586/14779072.3.1.111
21. Recchia FA. Revascularization of hibernating myocardium: uneven reflorescence after the drought. J Am Coll Cardiol. 2015;65(7):698–700. doi:10.1016/j.jacc.2014.12.024
22. Wu MY, Yiang GT, Liao WT, et al. Current mechanistic concepts in ischemia and reperfusion injury. Cell Physiol Biochem. 2018;46(4):1650–1667. doi:10.1159/000489241
23. Ravara B, Gobbo V, Carraro U, Gelbmann L, Pribyl J, Schils S. Functional electrical stimulation as a safe and effective treatment for equine epaxial muscle spasms: clinical evaluations and histochemical morphometry of mitochondria in muscle biopsies. Eur J Transl Myol. 2015;25(2):4910. doi:10.4081/ejtm.2015.4910
24. Schils S, Carraro U, Turner T, et al. Functional electrical stimulation for equine muscle hypertonicity: histological changes in mitochondrial density and distribution. J Equine Veterinary Sci. 2015;35(11–12):907–916. doi:10.1016/j.jevs.2015.08.013
25. Kalogeris T, Baines CP, Krenz M, Korthuis RJ. Cell biology of ischemia/reperfusion injury. Int Rev Cell Mol Biol. 2012;298:229–317. doi:10.1016/b978-0-12-394309-5.00006-7
26. Zhou T, Prather ER, Garrison DE, Zuo L. Interplay between ROS and antioxidants during ischemia-reperfusion injuries in cardiac and skeletal muscle. Int J Mol Sci. 2018;19(2):417. doi:10.3390/ijms19020417
27. Iurova E, Rastorgueva E, Beloborodov E, et al. Protective effect of peptide calcium channel blocker omega-hexatoxin-Hv1a on epithelial cell during ischemia-reperfusion injury. Pharmaceuticals (Basel). 2023;16(9):1314. doi:10.3390/ph16091314
28. Hausenloy DJ, Yellon DM. Myocardial ischemia-reperfusion injury: a neglected therapeutic target. J Clin Invest. 2013;123(1):92–100. doi:10.1172/jci62874
29. Delay C, Paradis S, Charles AL, et al. Physiopathologie de l’ischémie-reperfusion et du conditionnement ischémique du muscle squelettique – applications cliniques pour le chirurgien vasculaire [Skeletal muscle ischemia-reperfusion and ischemic conditioning pathophysiology-clinical applications for the vascular surgeon]. J Med Vasc. 2017;42(1):29–38. doi:10.1016/j.jmv.2016.11.001
30. Carden DL, Granger DN. Pathophysiology of ischaemia–reperfusion injury. J Pathol. 2000;190(3):255–266. doi:10.1002/(SICI)1096-9896(200002)190:3<255::AID-PATH526>3.0.CO;2-6
31. Maxwell SR, Lip GY. Reperfusion injury: a review of the pathophysiology, clinical manifestations and therapeutic options. Int J Cardiol. 1997;58(2):95–117. doi:10.1016/s0167-5273(96)02854-9
32. Panés J, Perry M, Granger DN. Leukocyte-endothelial cell adhesion: avenues for therapeutic intervention. Br J Pharmacol. 1999;126(3):537–550. doi:10.1038/sj.bjp.0702328
33. Collard CD, Gelman S. Pathophysiology, clinical manifestations, and prevention of ischemia-reperfusion injury. Anesthesiology. 2001;94(6):1133–1138. doi:10.1097/00000542-200106000-00030
34. Nikam P, Varadharajulu G. Effect of variants of positional release technique vs. ischemic compression technique on trigger point in myofascial pain syndrome: a randomized controlled trial. Int J Life Sci Pharma Res. 2021;11(2):L54–L57.
35. Birinci T, Mustafaoglu R, Kaya Mutlu E, Razak Ozdincler A. Stretching exercises combined with ischemic compression in pectoralis minor muscle with latent trigger points: a single-blind, randomized, controlled pilot trial. Complement Ther Clin Pract. 2020;38:101080. doi:10.1016/j.ctcp.2019.101080
36. Pecos-Martin D, Ponce-Castro MJ, Jiménez-Rejano JJ, Nunez-Nagy S, Calvo-Lobo C, Gallego-Izquierdo T. Immediate effects of variable durations of pressure release technique on latent myofascial trigger points of the levator scapulae: a double-blinded randomised clinical trial. Acupunct Med. 2019;37(3):141–150. doi:10.1136/acupmed-2018-011738
37. da Silva AC, De Noronha M, Liberatori-Junior RM, et al. The effectiveness of ischemic compression technique on pain and function in individuals with shoulder pain: a systematic review. J Manipulative Physiol Ther. 2020;43(3):234–246. doi:10.1016/j.jmpt.2019.10.013
38. Lu W, Li J, Tian Y, Lu X. Effect of ischemic compression on myofascial pain syndrome: a systematic review and meta-analysis. Chiropr Man Therap. 2022;30(1):34. doi:10.1186/s12998-022-00441-5
39. Pang CY, Yang RZ, Zhong A, Xu N, Boyd B, Forrest CR. Acute ischaemic preconditioning protects against skeletal muscle infarction in the pig. Cardiovasc Res. 1995;29(6):782–788. doi:10.1016/S0008-6363(96)88613-5
40. Hausenloy DJ, Yellon DM. Ischaemic conditioning and reperfusion injury. Nat Rev Cardiol. 2016;13(4):193–209. doi:10.1038/nrcardio.2016.5
41. Banga NR, Homer-Vanniasinkam S, Graham A, Al-Mukhtar A, White SA, Prasad KR. Ischaemic preconditioning in transplantation and major resection of the liver. Br J Surg. 2005;92(5):528–538. doi:10.1002/bjs.5004
42. Zarbock A, Kellum JA, Van Aken H, et al. Long-term effects of remote ischemic preconditioning on kidney function in high-risk cardiac surgery patients: follow-up results from the RenalRIP trial. Anesthesiology. 2017;126(5):787–798. doi:10.1097/aln.0000000000001598
43. Dawson VL, Dawson TM. Neuronal ischaemic preconditioning. Trends Pharmacol Sci. 2000;21(11):423–424. doi:10.1016/S0165-6147(00)01560-1
44. Pasupathy S, Homer-Vanniasinkam S. Ischaemic preconditioning protects against ischaemia/reperfusion injury: emerging concepts. Eur J Vasc Endovasc Surg. 2005;29(2):106–115. doi:10.1016/j.ejvs.2004.11.005
45. Jeffries O, Waldron M, Pattison JR, Patterson SD. Enhanced local skeletal muscle oxidative capacity and microvascular blood flow following 7-day ischemic preconditioning in healthy humans. Front Physiol. 2018;9:463. doi:10.3389/fphys.2018.00463
46. Leurcharusmee P, Sawaddiruk P, Punjasawadwong Y, et al. Ischemic preconditioning upregulates Mitofusin2 and preserves muscle strength in tourniquet-induced ischemia/reperfusion. J Orthop Translat. 2022;35:113–121. doi:10.1016/j.jot.2022.09.012
47. Bushell AJ, Klenerman L, Davies H, Grierson I, McArdle A, Jackson MJ. Ischaemic preconditioning of skeletal muscle 2. Investigation of the potential mechanisms involved. J Bone Joint Surg Br. 2002;84(8):1189–1193. doi:10.1302/0301-620x.84b8.9362
48. Attkiss KJ, Suski M, Hunt TK, Buncke HJ. Ischemic preconditioning of skeletal muscle improves tissue oxygenation during reperfusion. J Reconstr Microsurg. 1999;15(3):223–228. doi:10.1055/s-2007-1000095
49. D’Apolito E, Sisalli MJ, Tufano M, Annunziato L, Scorziello A. Oxidative metabolism in brain ischemia and preconditioning: two sides of the same coin. Antioxidants. 2024;13(5). doi:10.3390/antiox13050547
50. Grover GJ, Burkett DE, Parham CS, Scalese RJ, Sadanaga KK. Protective effect of mitochondrial KATP activation in an isolated gracilis model of ischemia and reperfusion in dogs. J Cardiovasc Pharmacol. 2003;42(6):790–792. doi:10.1097/00005344-200312000-00014
51. Lebuffe G, Schumacker PT, Shao ZH, Anderson T, Iwase H, Vanden Hoek TL. ROS and NO trigger early preconditioning: relationship to mitochondrial KATP channel. Am J Physiol Heart Circ Physiol. 2003;284(1):H299–308. doi:10.1152/ajpheart.00706.2002
52. Heidbreder M, Naumann A, Tempel K, Dominiak P, Dendorfer A. Remote vs. ischaemic preconditioning: the differential role of mitogen-activated protein kinase pathways. Cardiovasc Res. 2008;78(1):108–115. doi:10.1093/cvr/cvm114
53. Duan Q, Madan ND, Wu J, et al. Role of phosphoinositide 3-kinase IA (PI3K-IA) activation in cardioprotection induced by ouabain preconditioning. J Mol Cell Cardiol. 2015;80:114–125. doi:10.1016/j.yjmcc.2014.12.021
54. Simkhovich BZ, Przyklenk K, Kloner RA. Role of protein kinase C in ischemic “conditioning”: from first evidence to current perspectives. J Cardiovasc Pharmacol Ther. 2013;18(6):525–532. doi:10.1177/1074248413494814
55. Moses MA, Addison PD, Neligan PC, et al. Mitochondrial KATP channels in hindlimb remote ischemic preconditioning of skeletal muscle against infarction. Am J Physiol Heart Circ Physiol. 2005;288(2):H559–67. doi:10.1152/ajpheart.00845.2004
56. Moeinabadi-Bidgoli K, Rezaee M, Hossein-Khannazer N, et al. Exosomes for angiogenesis induction in ischemic disorders. J Cell Mol Med. 2023;27(6):763–787. doi:10.1111/jcmm.17689
57. Ishida T, Yarimizu K, Gute DC, Korthuis RJ. Mechanisms of ischemic preconditioning. Shock. 1997;8(2):86–94. doi:10.1097/00024382-199708000-00003
58. Watters O, O’Connor JJ. A role for tumor necrosis factor-α in ischemia and ischemic preconditioning. J Neuroinflammation. 2011;8(1):87. doi:10.1186/1742-2094-8-87
59. Morikawa T, Shimasaki M, Ichiseki T, Ueda S, Ueda Y, Takahashi K. The possibility of IPC to prevent ischemic-reperfusion injury in skeletal muscle in a rat. J Clin Med. 2023;12(4):1501. doi:10.3390/jcm12041501
60. Hotta K, Behnke BJ, Arjmandi B, et al. Daily muscle stretching enhances blood flow, endothelial function, capillarity, vascular volume and connectivity in aged skeletal muscle. J Physiol. 2018;596(10):1903–1917. doi:10.1113/jp275459
61. Janota CS, Calero-Cuenca FJ, Gomes ER. The role of the cell nucleus in mechanotransduction. Curr Opin Cell Biol. 2020;63:204–211. doi:10.1016/j.ceb.2020.03.001
62. Valenzuela PL, Martín-Candilejo R, Sánchez-Martínez G, Bouzas Marins JC, de la Villa P, Sillero-Quintana M. Ischemic preconditioning and muscle force capabilities. J Strength Cond Res. 2021;35(8):2187–2192. doi:10.1519/jsc.0000000000003104
63. Thielmann M, Kottenberg E, Kleinbongard P, et al. Cardioprotective and prognostic effects of remote ischaemic preconditioning in patients undergoing coronary artery bypass surgery: a single-centre randomised, double-blind, controlled trial. Lancet. 2013;382(9892):597–604. doi:10.1016/S0140-6736(13)61450-6
64. Tian C, Wang A, Huang H, Chen Y. Effects of remote ischemic preconditioning in hepatectomy: a systematic review and meta-analysis. BMC Anesthesiol. 2024;24(1):118. doi:10.1186/s12871-024-02506-9
65. Trybulski R, Clemente FM, Ryszkiel I, et al. Effect of ischemic preconditioning on microvascular post-occlusive hyperemic reactions and quadriceps morphology in MMA: a randomized clinical trial. Eur J Appl Physiol. 2025. doi:10.1007/s00421-025-05914-y
66. Van Pelt DW, Lawrence MM, Miller BF, Butterfield TA, DuPont-Versteegden EE. Massage as a mechanotherapy for skeletal muscle. Exerc Sport Sci Rev. 2021;49(2):107–114. doi:10.1249/jes.0000000000000244
67. Butterfield TA, Zhao Y, Agarwal S, Haq F, Best TM. Cyclic compressive loading facilitates recovery after eccentric exercise. Med Sci Sports Exerc. 2008;40(7):1289–1296. doi:10.1249/MSS.0b013e31816c4e12
68. Kutner JS, Smith MC, Corbin L, et al. Massage therapy versus simple touch to improve pain and mood in patients with advanced cancer: a randomized trial. Ann Intern Med. 2008;149(6):369–379. doi:10.7326/0003-4819-149-6-200809160-00003
69. Saita Y, Yokoyama K, Nakamura K, Itoman M. Protective effect of ischaemic preconditioning against ischaemia-induced reperfusion injury of skeletal muscle: how many preconditioning cycles are appropriate? Br J Plast Surg. 2002;55(3):241–245. doi:10.1054/bjps.2002.3809
70. Qi W, Kan SL. Protective effect of ischemic preconditioning duration against ischemia-reperfusion injury of skeletal muscle in rats. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2005;19(4):274–277.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.