Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 19
An Observational Study of Maternal Hypoglycemia in Pregnancy
Authors Bleicher I ![]() , Einav S, Perlov Gavze R, Lev Shalem L, Sammour R
, Einav S, Perlov Gavze R, Lev Shalem L, Sammour R
Received 28 November 2025
Accepted for publication 21 April 2026
Published 13 July 2026 Volume 2026:19 584881
DOI https://doi.org/10.2147/DMSO.S584881
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ernesto Maddaloni
Inna Bleicher,1,2 Sharon Einav,3,4 Revital Perlov Gavze,5 Liat Lev Shalem,5 Rami Sammour1,2
1Department of Obstetrics and Gynecology, Bnai -Zion Medical Center, Haifa, Israel; 2The Ruth and Bruce Rappaport Faculty of Medicine, Technion - Israel Institute of Technology, Haifa, Israel; 3Faculty of Medicine, Hebrew University of Jerusalem, Jerusalem, Israel; 4Hod HaSharon Maccabi Healthcare Services, Hod Hasharon, Israel; 5Medical Division, Maccabi Healthcare Services, Tel Aviv, Israel
Correspondence: Inna Bleicher, Department of Obstetrics and Gynecology, Bnai -Zion Medical Center, Haifa, Israel, Email [email protected]
Background: Hypoglycemia in pregnancy is relatively understudied, with conflicting evidence suggesting either outcomes similar to normal oral glucose tolerance test (OGTT) or associations with poor neonatal outcomes. Maternal glucose crosses the placenta, thus maternal hypoglycemia may affect the fetus.
Objective: This study aimed to evaluate the association between maternal hypoglycemia and neonatal birth weight, specifically the risk of small-for-gestational-age (SGA) neonates, and to examine maternal metabolic outcomes in comparison to normoglycemic and hyperglycemic individuals.
Study Design: This retrospective cohort study included 39,306 primiparous individuals aged 18– 50 years. Participants were classified as hypoglycemic (glucose < 70 mg/dL) hyperglycemic (≥ 1 abnormal OGTT value), or normoglycemic. The primary outcome was the rate of SGA (< 10th percentile) and large-for-gestational-age (LGA, > 90th percentile) neonates. Secondary outcomes included maternal hypertensive disorders, gestational diabetes requiring treatment (GDMA2), and long-term risk of diabetes mellitus (DM).
Results: Among the cohort, 16,062 (40.9%) were hypoglycemic, 8543 (21.7%) were hyperglycemic, and 14,701 (37.4%) were normoglycemic. Compared to normoglycemic individuals, hypoglycemia was associated with an increased likelihood of SGA (OR 1.2, 95% CI 1.1– 1.4), particularly in the second and third trimesters. Hyperglycemia was associated with an increased likelihood of LGA (OR 1.2, 95% CI 1.1– 1.4). Hypoglycemia was also linked to a higher prevalence of gestational diabetes (GDMA2) and dysglycemia during pregnancy, yet a lower likelihood of developing DM later in life compared to hyperglycemic individuals.
Conclusion: Maternal hypoglycemia during pregnancy is associated with an increased risk of SGA neonates and may serve as an early marker of underlying glucose dysregulation. Given these findings, repeated glucose monitoring and closer follow-up for individuals with hypoglycemia may be warranted. Future research should investigate long-term neonatal and maternal metabolic outcomes to refine clinical management strategies for hypoglycemia in pregnancy.
Keywords: hypoglycemia, small for gestational age, gestational diabetes, diabetes mellitus
Introduction
Gestational diabetes mellitus (GDM) is a common pregnancy complication, affecting approximately 15% of pregnant individuals globally.1 GDM poses significant short- and long-term health risks for both the mother and the offspring, emphasizing the importance of early detection and management. In the short term, GDM is associated with maternal and fetal complications such as macrosomia (birth weight >4500 grams), large-for-gestational-age (LGA) infants, increased rates of operative vaginal deliveries and cesarean sections, birth trauma, severe perineal tears, preeclampsia, polyhydramnios, and intrauterine fetal demise. Long-term complications include a heightened risk of metabolic syndrome, cardiovascular disease, and type 2 diabetes mellitus for both mother and child.2–6
The American College of Obstetricians and Gynecologists (ACOG) outlines that GDM diagnosis involves either a one-step or two-step process, often requiring at least two abnormal glucose values, though a single abnormal value may suffice in specific circumstances. “Abnormal values” are predominantly defined as elevated glucose levels.7
Hypoglycemia, defined as plasma glucose levels below 54–70 mg/dL, is a less frequently studied condition. Its implications, particularly in the context of the glucose challenge test (GCT) and oral glucose tolerance test (OGTT), remain a subject of debate. Some studies suggest that individuals with normal OGTT results exhibit comparable maternal and neonatal outcomes to those with hypoglycemia during OGTT. Other studies report a higher prevalence of pathological glucose patterns on self-monitoring, an increased prevalence low-birth-weight (<2500 grams), and a higher likelihood of subsequent GDM diagnosis in individuals with hypoglycemia during OGTT.8–10
Given that maternal glucose diffuses to the fetus, maternal hypoglycemia could induce fetal hypoglycemia, potentially leading to fetal hypoxia and suboptimal growth. These findings underscore the need for a nuanced understanding of glucose abnormalities during pregnancy and their implications for maternal and neonatal health.11
However, important knowledge gaps remain. Available studies are largely single-center, use heterogeneous hypoglycemia thresholds and testing strategies, and have limited ability to examine whether the timing of hypoglycemia during pregnancy modifies fetal growth risk. In addition, maternal metabolic outcomes beyond pregnancy, including subsequent diabetes risk, have rarely been evaluated in individuals with hypoglycemia detected on screening or diagnostic glucose testing.
The current study aimed to assess the rate of small-for-gestational-age (SGA) and large for gestational age (LGA) neonates among individuals with hyperglycemia, hypoglycemia and normoglycemia. We hypothesized that maternal hypoglycemia will be associated with an increased risk of small-for-gestational-age (SGA) just as hyperglycemia is associated with large for gestational age (LGA) neonates, in addition to pathological maternal metabolic outcomes and neonatal complications, when compared to normoglycemic individuals.
Methods
Study Design
This retrospective analysis of data from electronic medical records of Maccabi Healthcare Services (January 2000–December 2022) is reported according to the Reporting of Studies Conducted Using Observational Routinely Collected Data recommendations.12
Setting
The Maccabi Health Service (MHS) is the second-largest health maintenance organization (HMO) in Israel. Founded in 1940, it currently covers approximately 2.4 million insurees. Like all HMOs in the country, the MHS operates according to the guidelines of the national insurance law. The national health insurance law ensures that all residents of the country are entitled to a basket of healthcare services predetermined by a national committee. The costs of all pregnant individuals are mandatorily covered, and this population undergoes scheduled follow-up and testing. Medical treatment follows national guidelines which are written and updated periodically by the Israeli society of obstetrics and gynecology according to international guidelines. Follow-ups and tests are routinely recorded in a standard electronic medical record (EMR). GCT and OGTT are performed according to ACOG recommendations, usually during the second trimester, between 24–28 gestational weeks.
Participants
The MHS database was used to identify those fulfilling the following criteria: Primiparous individuals, aged 18–50 years at the time of their last menstrual period, with a 100-gram oral glucose tolerance test (OGTT) results available, and a live birth. We also included patients with a 50-gram glucose challenge test (GCT) result <70 mg/dl, even if OGTT results were not available. Excluded were individuals with multiple gestation and those with missing data of neonatal outcomes or birthweight. Data were extracted up to a year after delivery.
Variables
The primary study outcome was the rate of large for gestation (LGA) or small for gestation (SGA) neonates. We defined LGA as birthweight >90th centile and SGA as birthweight <10th centile according to local birth charts.13 Individuals were classified as hyperglycemic if they had one or more elevated glucose level, as hypoglycemic if they had any glucose levels <70 mg/dl (with or without hyperglycemia) or as normoglycemic.7 Analysis was performed according to the trimester during which the pathological glucose level was measured. Since there is no standard definition for GDM, we chose to use the conservative definition of a single pathological value.7
The secondary study outcomes were the rates of complications (hypertensive disorder, DM later in life) among individuals with hypoglycemia as compared to those with normoglycemia, and whether these individuals with hypoglycemia were classified as dysglycemic (ie. defined as the presence of any ICD-10 diagnosis related to abnormal glucose metabolism recorded in the patient’s medical chart; the diagnosis was made and documented by the treating physician during the index pregnancy) and required glucose lowering agents. We therefore also collected data on maternal demographics (maternal age at diagnosis, socio-economic status) and co-morbidities (smoking, body mass index [BMI]), the details of the current pregnancy (eg. maternal fetal medicine clinic follow-up, gestational age at diagnosis, glucose test results, gestational age at delivery), pregnancy complications (hypertensive disorders, diagnosis of GDMA1 and GDMA2), medical treatment for GDM and on later presentation of diabetes mellitus (DM according to the diabetes registry).
A list of codes used to identify the variables is provided in Supplementary Table 1.
We also collected data on neonatal outcomes (birthweight, jaundice, hypoglycemia, rates of referral to a pediatrician or the department of emergency medicine during the first year of life, and failure to thrive [FTT]) and data on maternal follow up and outcomes (number of obstetrical medical visits, ultrasound examinations, referrals to the department of emergency medicine, and hospitalizations).
Data Sources/Measurement
All the data were extracted by MHS data analysts from the EMRs of relevant patients identified in the MHS database. All MHS tests are sent to standardized ISO-accredited central laboratories and results are sent electronically directly to the treating clinicians as well as being automatically documented in the EMRs. Measurements were unrelated to the study and were performed by independent clinicians and laboratory workers.
Bias
Selection bias is less likely given that MHS is the second-largest HMO and covers almost a third of the population in the country. Self-selection for testing is always a possibility despite full coverage of costs. Measurement bias is not likely given the rigorous standards upheld by the central MHS laboratories. Some doctors may have failed to document the presence of diabetes in the list of diagnoses. We overcame this issue by classifying patients according to their blood test results rather than through these lists.
Study Size
Study power was not calculated since this study covered the full database population rather than a sample.
Quantitative Variables
We studied age both as a continuous variable and as age above and below 35 years, due to the American Diabetes Association recommendation to screen for DM at this age in populations at risk.14 Blood pressure was classified according to the American Heart Association classification of hypertension.15 Neonatal weight categories and LGA and SGA were defined as commonly accepted.
Statistical methods
Missingness is reported. Categorical data were reported as the number (%) and compared using the Chi-square test. Continuous variables were reported as mean ± SD and median [Interquartile Range (Q1-Q3]]. Between-group comparisons were performed using analysis of variance (ANOVA) for normally distributed data and the Kruskal–Wallis test for non-parametric data. Logistic regression analysis was used to examine neonatal and maternal outcomes. All models were adjusted for maternal age at diagnosis, dysglycemia and GDMA2 unless GDMA2 was studied as an outcome. Models studying GDMA2 as an outcome were adjusted only for maternal age at diagnosis and dysglycemia. Models studying dysglycemia as an outcome were adjusted for maternal age at diagnosis and GDMA2. All data were analyzed using SPSS version 29 (IBM Corp. Released 2023. IBM SPSS Statistics for Windows, Version 29.0.2.0 Armonk, NY: IBM Corp). P-values less than 0.05 were considered significant.
Data Access and Cleaning Methods
MHS provides data analysts and statistical support. Aggregate data are provided to the researchers following data cleaning. Data cleaning included the following: OGTT with the value of “0” were considered missing, illogical neonatal weights (eg. 6666, 38). All analyses are performed by the support team as per request.
Linkage
Maternal and neonatal files were linked (person level) across a single data base using IDs with a proprietary code unique to the MHS.
Results
Participants
Overall, 169,346 potentially eligible primiparous individuals aged 18–50 years at the time of their last menstrual period with a pregnancy resulting in a live birth were identified in the MHS database. After excluding individuals with incomplete 100-gram oral glucose tolerance test (OGTT) and adding individuals who had hypoglycemic value (<70 mg/dl) in their 50-gram glucose challenge test (GCT), there were 47,086 eligible individuals. After further exclusion for multiple gestation and missing data regarding neonatal outcome or neonatal weight, the final study cohort included 39,306 individuals (Figure 1).
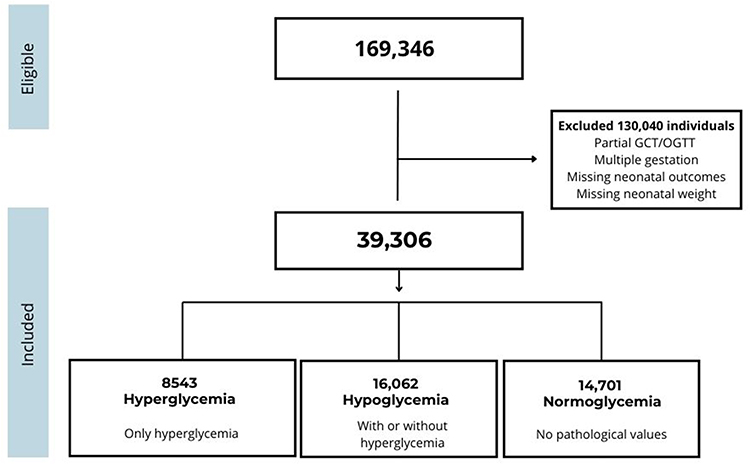 |
Figure 1 Inclusion exclusion flow chart. |
Missingness
Variables with the greatest amount of missing data were BMI in early pregnancy (84%), BMI at delivery (90%), weight in early pregnancy (60%), weight at delivery (53%) and fasting glucose in early pregnancy (50%).
Descriptive Data
The average maternal age at the time of diagnosis ranged between 28–31 years regardless of trimester of diagnosis. Diagnostic tests were performed during first, second and third trimester at an average of 9, 25 and 32 weeks of gestation, respectively. Most individuals were diagnosed during the second trimester of pregnancy. Additional maternal and neonatal characteristics are presented in Table 1.
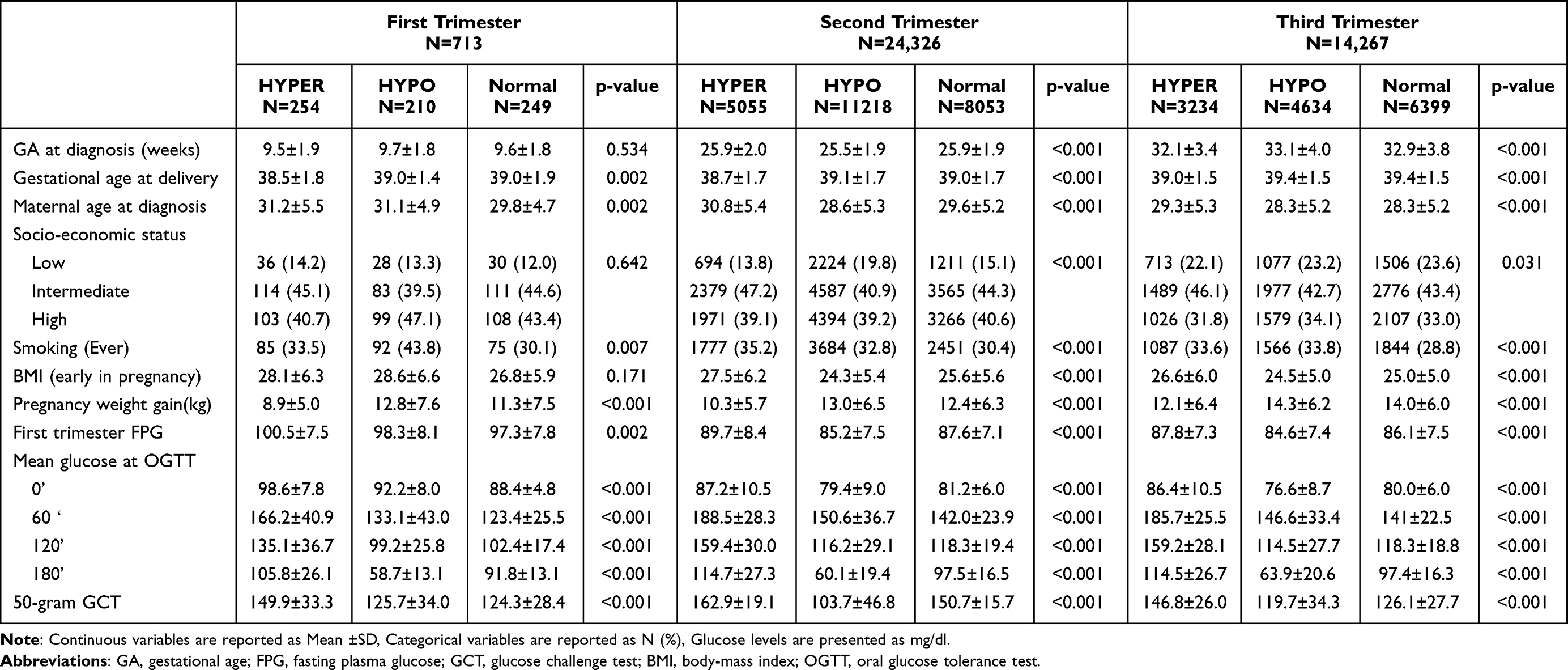 |
Table 1 Population Characteristics |
Outcome Data
Overall, 8543 patients had hyperglycemia, 16,062 had hypoglycemia and 14,701 were normoglycemic.
Main Results
When comparing patients with hyperglycemia to normoglycemia in the second trimester, the likelihood of SGA <10 centile was 1.2 (95% CI 1.1–1.4), and the likelihood of SGA <1 centile was 3.5 (95% CI 1.6–7.8). This difference was not apparent in the third trimester.
When comparing patients with hypoglycemia to normoglycemia, the likelihood of SGA <10 centile was 1.2 (95% CI 1.1–1.4) in both the second and the third trimester, and the likelihood of SGA <1 centile was 2.5 (1.1–5.3) in the third trimester only. (Table 2). Neonatal follow-up during the first year of life after maternal hyperglycemia, hypoglycemia and normoglycemia is presented in Supplementary Table 2 per trimester of diagnosis.
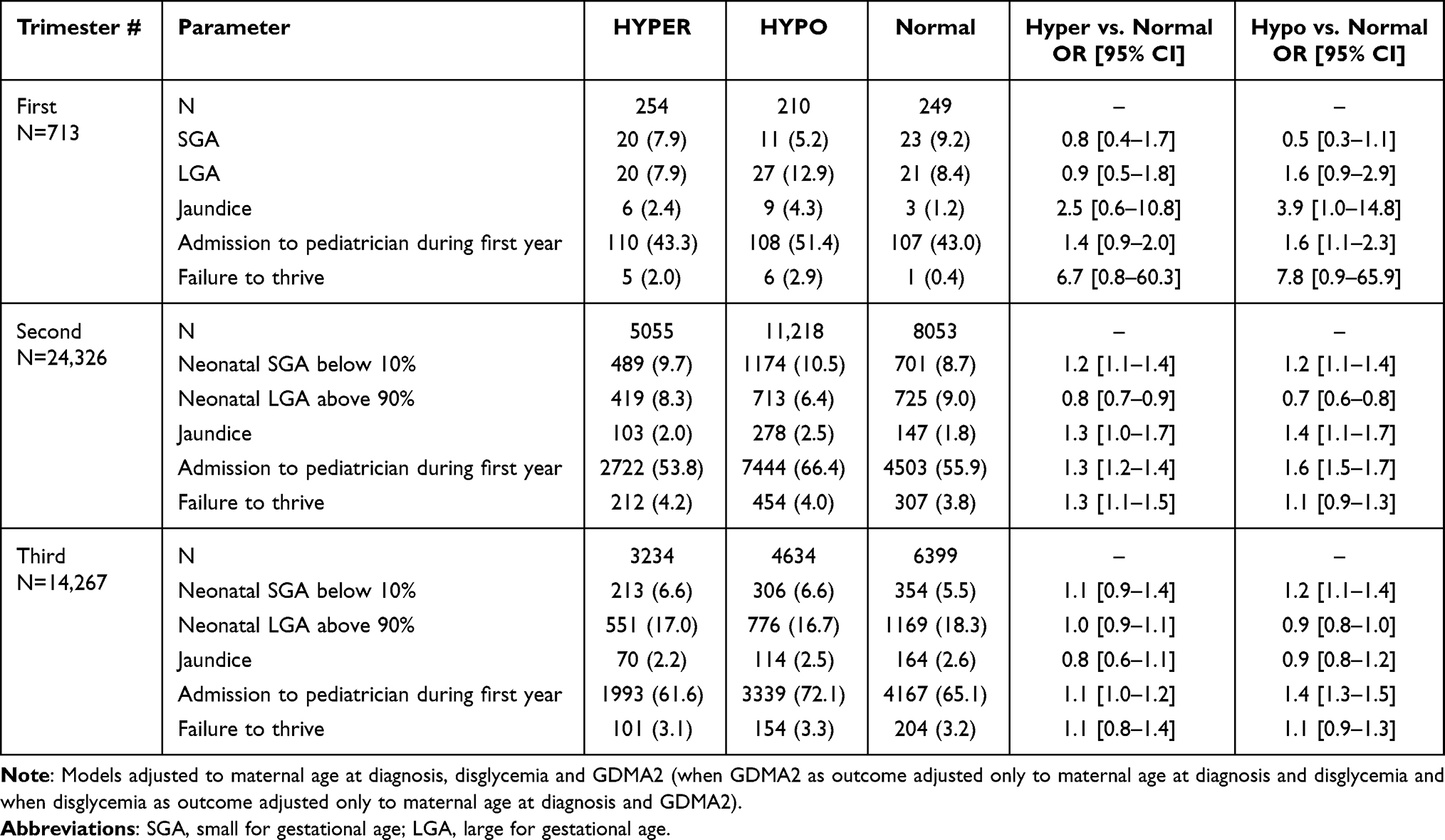 |
Table 2 Neonatal Outcomes |
Compared to individuals with normoglycemia the likelihood of hypertensive disorder was increased in both hyper- and hypoglycemia. However, the number of patients in each group was very small. Compared to individuals with normoglycemia, individuals with hypoglycemia were less likely than individuals with hyperglycemia to be diagnosed with DM later in life. Compared to individuals with normoglycemia, the likelihood of diagnosis of dysglycemia during pregnancy (had ICD code for gestational diabetes in their medical chart) was also lower in individuals with hypoglycemia versus hyperglycemia. Although many hypoglycemic patients received treatment with glucose lowering agents (GDMA2), the adjusted likelihood of such treatment was lower in individuals with hypoglycemia versus hyperglycemia when compared to normoglycemia. (Table 3)
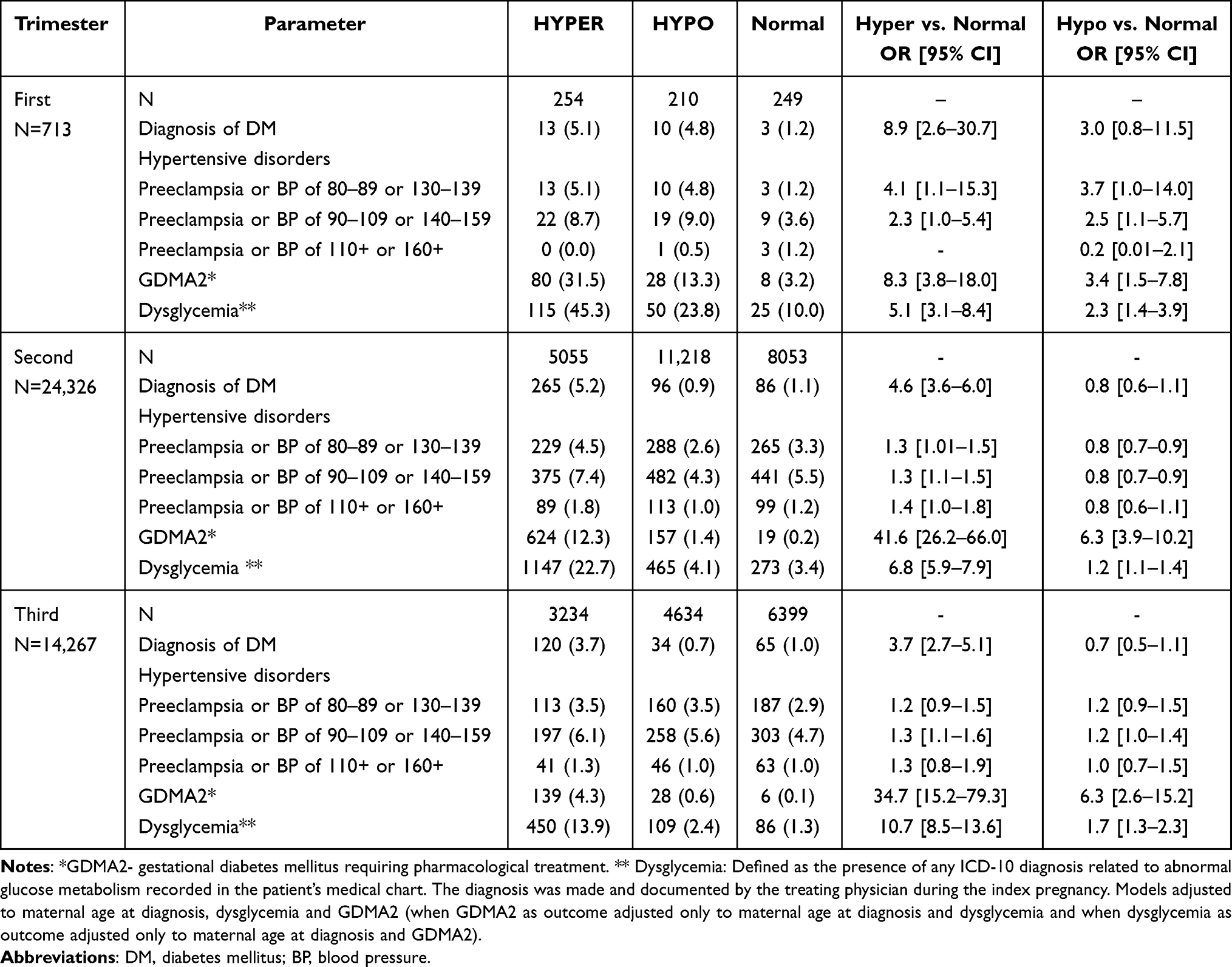 |
Table 3 Maternal Outcomes |
Utilization of obstetric services among patients with hyperglycemia, hypoglycemia and normoglycemia per trimester of diagnosis is presented in Supplementary Table 3.
Discussion
Principal Findings
In this observational study of nearly 40,000 pregnant individuals who underwent either a GCT or an OGTT, the likelihood of SGA neonates was higher among those with hypoglycemia than those with normoglycemia. This association was most pronounced in the second and third trimesters of pregnancy. However, neonatal follow-up revealed no clinically significant differences in the studied variables within the first year of life.
Regarding maternal outcomes, the prevalence of hypertensive disorders was slightly higher in individuals with either hyperglycemia or hypoglycemia versus normoglycemia, although the difference appeared negligible. As expected, individuals in hyperglycemia group had a higher prevalence of GDMA2, more individuals were diagnosed with dysglycemia during pregnancy (presence of ICD-10 diagnosis related to abnormal glucose metabolism recorded in the patient’s medical chart by the treating physician during the index pregnancy) and more individuals were diagnosed with DM later in life, across all three trimesters. Interestingly, individuals with hypoglycemia also had a higher prevalence of GDMA2 and dysglycemia, albeit a similar prevalence of DM later in life, compared to individuals with normoglycemia. Due to the retrospective design of the study, the exact mechanism underlying this relationship remains unclear, but it is possible that patients with hypoglycemia underwent self-glucose monitoring more frequently, ultimately revealing previously undiagnosed diabetes requiring medical intervention. This finding supports the hypothesis that hypoglycemia following a glucose challenge may be an unrecognized marker of diabetes. Nevertheless, individuals with hypoglycemia versus hyperglycemia were less likely to be diagnosed with DM later in life. Additionally, while individuals with hyperglycemia had more frequent obstetric visits, those with hypoglycemia did not differ significantly in their visit frequency compared to normoglycemic individuals.
Results in Context of What is Known
Our study is unique in that it included a somewhat larger cohort than the largest study to date.16 Of previous studies evaluating hypoglycemia and pregnancy outcomes, two were conducted at the UK,10,17 one in China,18 one in the US16 and one in Israel.8 Four studies included data from a single medical center8,10,16,17 but only one included community-level data such as ours.18 Although two reports described maternal outcomes,16,17 these included pregnancy-related outcomes only, like hypertensive disorders, mode of delivery, postpartum hemorrhage and diagnosis of GDM. In the current study, we also examined the rate of diagnosis of DM later in life.
Our study included only individuals with a live birth as did prior studies.10,16–18 Our findings that hypoglycemia is associated with SGA were similar to several previous studies.10,16,18 Raviv et al found that the rate of SGA was similar once adjusted to maternal age, BMI, nulliparity, and any hypertensive disorder. However, they also stated that “it would be hard to ignore the differences in birthweight trends”.8
We found no clinically significant difference between hyperglycemic, hypoglycemic and normoglycemic individuals in either age or the rate of hypertensive disorders and therefore did not adjust for these variables, and the paucity of data regarding BMI in our database did not enable adjustment for this variable. Furthermore, our study population also differed from that of Raviv et al in maternal age (lower percent of individuals >35 years) and rate of nulliparity (100% vs. 30%).
Contrary to most prior studies,10,16,17 we limited the upper age of the included population to 50 years. Leng et al18 included only individuals aged less than 39 years Our study included only individuals in their first pregnancy whereas the rest included both nulliparous and multiparous individuals.10,16–18 Across all studies, including ours, the criteria for inclusion in terms of glucose testing that were used for diagnosis and the cutoffs used for classification of abnormality were inconsistent. For example, Ding et al used a cutoff of 82 mg/dl to define hypoglycemia during 50 g GCT,16 Nayak et al10 used 88.5 mg/dl, while we defined hypoglycemia less than 70 mg/dl on either 50 g GCT or 100OGTT.
Clinical Implications
In an ideal world, glucose tolerance testing would be conducted in the first trimester of pregnancy. Already at this early stage, more than half of individuals had abnormal glucose values. Individuals with a normal test during first trimester should repeat testing between 24–28 weeks where the highest insulin resistance, while individuals with abnormal glucose, high or low, should be requested to keep a glucose level diary for 1–2 weeks. Those with entirely normal values or sporadic hyperglycemia or hypoglycemia could probably continue intermittent self-glucose monitoring with appropriate lifestyle modification and regular maternal follow up. Those with abnormal values (> 15–20%) despite lifestyle modification, should be referred to maternal fetal medicine specialist clinics to consider further medical treatment. Glucose values should be addressed as a continuum, with pathology being recognized by consistently irregular findings on both sides of the normal spectrum.
Research Implications
Future studies should consider testing the feasibility of such an approach, should include highly granular, prospective data to enable controlling for potential confounders in a sufficiently large sample and should also include more outcome data on patient-centered outcomes.
Strengths and Limitations
Strengths of this study include its large, population-based sample size and the inclusion of long-term maternal outcomes—an aspect rarely addressed in prior work. The exclusive inclusion of primiparous individuals helps control for confounding due to obstetric history. Moreover, the use of real-world data from a national health maintenance organization (HMO) enhances generalizability.
The current study was retrospective, and therefore, despite the large sample size, determines association rather than causation. Although the MHS database covers almost one-third of the population in the country, this sample may still not represent the entire population, nor may it represent pregnant population elsewhere. The need to ensure generalizability requires further research. Our criteria for study inclusion were somewhat different from prior studies. However, the criteria for diagnosis of hypoglycemia during pregnancy are inconsistent across multiple papers. Due to limitations in file linkage, our data does not include in-hospital data such as complications during labor, mode of delivery, Apgar score, umbilical cord pH and neonatal intensive care unit admission.
Conclusion
Maternal hypoglycemia during pregnancy is associated with an increased risk of SGA neonates and may serve as an early marker of underlying glucose dysregulation. Given these findings, repeated glucose monitoring and closer follow-up for individuals with hypoglycemia may be warranted. Several considerations should guide interpretation of these findings. First, given the retrospective observational design, the associations observed cannot establish causality. Prospective validation is also required. Second, the definition of hypoglycemia in pregnancy may need further refinement.
Future studies should include prospective, trimester-specific assessment of glucose dynamics with standardized thresholds, incorporate detailed maternal metabolic phenotyping and nutritional data, and evaluate longer-term maternal and neonatal metabolic implications and outcomes. Such work is needed to inform evidence-based clinical management strategies.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used ChatGPT to enhance language and readability. After using this tool, the authors reviewed and edited the content as needed and takes full responsibility for the final version of the paper.
Data Sharing Statement
The datasets generated and analyzed during the current study are not publicly available due to institutional and national data protection policies but may be made available from the corresponding author on reasonable request and subject to approval by Maccabi Healthcare Services.
Ethics Approval Statement
The study protocol was approved by the Maccabi Healthcare Services Institutional Review Board (0144-22-MHS) and adhered to the Declaration of Helsinki. All data were de-identified prior to analysis.
Patient Consent Statement
As this was a retrospective study using de-identified electronic health records, informed consent was waived by the institutional review board.
Author Contributions
Dr. Inna Bleicher: Conceptualization, Methodology, Investigation, Writing, Original Draft, Writing, Review and Editing. Revital Perlov Gavze: Methodology, Data Curation, Investigation, Supervision, Writing, Review and Editing. Liat Lev Shalem: Methodology, Data Curation, Investigation, Supervision, Writing, Review and Editing. Dr. Rami Sammour: Conceptualization, Methodology, Formal Analysis, Writing, Review and Editing. Prof. Einav Sharon: Writing, Original Draft, Writing, Review and Editing, Visualization. All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This work was supported by Marom, the Maccabi Healthcare Services Research Program, Tel Aviv, Israel.
Disclosure
All authors declare no conflict of interest.
References
1. Rj G, Alsweiler J, Ae M, et al. diabetes mellitus: an overview of cochrane reviews (Review). 2020. doi:10.1002/14651858.CD012394.pub3
2. Dudley DJ. Diabetic-associated stillbirth: incidence, pathophysiology, and prevention. Obstet Gynecol Clin North Am. 2007;34(2):293–11. doi:10.1016/J.OGC.2007.03.001
3. Venkatesh KK, Lynch CD, Powe CE, et al. Risk of adverse pregnancy outcomes among pregnant individuals with gestational diabetes by race and ethnicity in the United States, 2014–2020. JAMA. 2022;327(14):1356–1367. doi:10.1001/JAMA.2022.3189
4. Page KA, Romero A, Buchanan TA, Xiang AH. Gestational diabetes mellitus, maternal obesity, and adiposity in offspring. J Pediatr. 2014;164(4):807. doi:10.1016/J.JPEDS.2013.11.063
5. Kramer CK, Campbell S, Retnakaran R. Gestational diabetes and the risk of cardiovascular disease in women: a systematic review and meta-analysis. Diabetologia. 2019;62(6):905–914. doi:10.1007/S00125-019-4840-2/FIGURES/3
6. Waters TP, Kim SY, Werner E, et al. Should women with gestational diabetes be screened at delivery hospitalization for type 2 diabetes? Am J Obstet Gynecol. 2020;222(1):
7. Committee on Practice Bulletins—Obstetrics. Mellitus APBNo 190: GD. ACOG practice bulletin No. 190: gestational diabetes mellitus. Obstet Gynecol. 2018;131(2):e49–e64. doi:10.1097/AOG.0000000000002501
8. Raviv S, Wilkof-Segev R, Maor-Sagie E, et al. Hypoglycemia during the oral glucose tolerance test in pregnancy—maternal characteristics and neonatal outcomes. Int J Gynecol Obstet. 2022;158(3):585–591. doi:10.1002/IJGO.14037
9. Yuen L, Bontempo S, Wong VW, Russell H. Hypoglycaemia on an oral glucose tolerance test in pregnancy - Is it clinically significant? Diabet Res Clin Pract. 2019;147:111–117. doi:10.1016/J.DIABRES.2018.11.018
10. Nayak AU, Vijay AMA, Indusekhar R, Kalidindi S, Katreddy VM, Varadhan L. Association of hypoglycaemia in screening oral glucose tolerance test in pregnancy with low birth weight fetus. World J Diabetes. 2019;10(5):304–310. doi:10.4239/WJD.V10.I5.304
11. Illsley NP, Baumann MU. Human placental glucose transport in fetoplacental growth and metabolism. Biochim Biophys Acta Mol Basis Dis. 2020;1866(2):165359. doi:10.1016/J.BBADIS.2018.12.010
12. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
13. Dollberg S, Haklai Z, Mimouni FB, Gorfein I, Gordon ES. Birthweight standards in the live-born population in Israel. Isr Med Assoc J. 2005;7(5):311–314.
14. ElSayed NA, Aleppo G, Bannuru RR; American Diabetes Association Professional Practice Committee. 2. diagnosis and classification of diabetes: standards of care in Diabetes—2024. Diabetes Care. 2024;47(Suppl 1):S20–S42. doi:10.2337/dc24-S002
15. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Hypertension. 2018;71(6):e13–e115. doi:10.1161/HYP.0000000000000065
16. Ding JJ, Lundsberg LS, Culhane JF, Patridge C, Milley L, Son M. The association between a low 50-gram, 1-hour glucose challenge test value and neonatal morbidity. J Matern Fetal Neonatal Med. 2023;36(2):2245527. doi:10.1080/14767058.2023.2245527
17. Blunt C, Mathew S, Mung SM, Krishnamurthy R, Jude EB. Hypoglycaemia following the 2-hour 75g OGTT in pregnancy - Investigating maternal and foetal outcomes. Diabetes Metab Syndr. 2024;18(3):102977. doi:10.1016/j.dsx.2024.102977
18. Leng J, Hay J, Liu G, et al. Small-for-gestational age and its association with maternal blood glucose, body mass index and stature: a perinatal cohort study among Chinese women. BMJ Open. 2016;6(9):e010984. doi:10.1136/bmjopen-2015-010984
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effects of the Ethanol Extract of Allium Ascalonicum L. in High-Fat-High-Fructose-Induced Insulin Resistance Swiss-Webster Male Mice
Elkanawati RY, Sumiwi SA, Levita J
Journal of Experimental Pharmacology 2025, 17:207-221
Published Date: 16 May 2025