")
Back to Journals » Journal of Pain Research » Volume 14
An Italian Expert Consensus on the Use of Opioids for the Management of Chronic Non-Oncological Pain in Clinical Practice: Focus on Buprenorphine.
Authors Mattia C , Luongo L, Innamorato M , Melis L , Sofia M, Zappi L, Puntillo F
Received 15 April 2021
Accepted for publication 30 July 2021
Published 11 October 2021 Volume 2021:14 Pages 3193—3206
DOI https://doi.org/10.2147/JPR.S314206
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Consalvo Mattia,1,2 Livio Luongo,3,4 Massimo Innamorato,5 Luca Melis,6 Michele Sofia,7 Lucia Zappi,8 Filomena Puntillo9,10
1Department of Medical and Surgical Sciences and Biotechnologies, Faculty of Pharmacy and Medicine, “Sapienza” University of Rome, Rome, Italy; 2Anesthesia, Intensive Care and Pain Unit, ICOT-Polo Pontino, Latina, Italy; 3Department of Experimental Medicine, Division of Pharmacology, University of Campania “L. Vanvitelli”, Naples, Italy; 4NEUROMED, Pozzilli, Italy; 5Pain Therapy Unit, AUSL Romagna, S.M.Croci Hospital Ravenna, Ravenna, Italy; 6Poliste, Cagliari, Italy; 7Department of Palliative Care and Pain Therapy, ASST Rodhense, Garbagnate Milanese, Itlay; 8UOC Antalgic Therapy, Emergency and Acceptance Department, San Martino Polyclinic Hospital, Genoa, Italy; 9Department of Interdisciplinary Medicine, “Aldo Moro” University of Bari, Bari, 70124, Italy; 10Anesthesia, Intensive Care and Pain Unit, Policlinico Hospital of Bari, Bari, 70124, Italy
Correspondence: Consalvo Mattia
Department of Medical and Surgical Science, University Sapienza, Corso della Repubblica, 79, Latina, 04100, Italy
Tel +39 0773 6511
Email [email protected]
Purpose: The aim of the present work was to evaluate the knowledge and prescriptive habits of clinicians involved in the management of chronic non cancer pain (CNCP), with a special focus on the use of opioids.
Methods: A Delphi method was used. A Board of specialists elaborated and discussed a series of statements, based on available literature and personal clinical expertise, about particularly controversial topics on pain pathophysiology and treatment. A Panel of experts in the field of pain management, selected by the Board, was invited to vote the proposed statements, indicating the level of agreement on a 5-point Likert scale (1: strongly disagree; 2: disagree; 3: partially agree; 4: agree; 5: strongly agree). The threshold for consensus was set at minimum 66.6% of the number of respondents with a level of agreement ≥ 4 (Agree or Strongly agree).
Results: The Board included 5 pain therapists, 1 pharmacologist and 1 methodology expert and drew up a total of 36 statements (for a total of 40 requested answers)”. A total of 100 clinicians were included in the Expert Panel. Respondents were 89 (89%). Consensus was achieved for 32 out of 40 answers. Most of the lack of consensus was recorded for statements regarding opioids use, and resulted from a low level of agreement (3 on the Likert scale), suggesting a neutral position deriving from a lack of knowledge rather than a strong contrary opinion.
Conclusion: Most of the proposed items reached consensus, suggesting a generally homogeneous approach to CNCP management. However, the lack of consensus recorded for several items regarding opioid use confirms the need to fill important gaps in the knowledge of available agents. A clear explanation of the peculiar pharmacological properties of drugs associated with potential clinical advantages (such as buprenorphine) will help optimize pain treatment in both primary care and hospital settings and improving pain control in CNCP patients.
Keywords: pain, chronic, non-oncological, strong opioids, buprenorphine, Delphi survey
Introduction
Chronic pain is defined as pain that persists or recurs for more than 3 months.1 Although it commonly presents itself as a manifestation of an injury or a disease, it should be considered as a separate condition rather than an accompanying symptom of other conditions.2 Chronic pain is associated with functional impairment and decreased quality of life, making treatment imperative for patient well-being.3 Targeted and appropriate prevention and management strategies need to take into proper account the physical aspects of pain, as well as its psychological, socio-demographic, and lifestyle determinants.2,4
Epidemiology of Chronic Pain
It is estimated that 50 million adults in the United States experience chronic pain, which in 19.6 million subjects it has a high impact on daily life or work activities.3
Chronic pain affects about 20% of the European population. In terms of the prevalence of chronic pain, Italy ranks third in Europe, with about 26% of the population who has used drugs to treat chronic pain at least once in their lifetime.5
Since CNCP prevalence increases with age, it is likely to rise markedly in the near future, given the aging population in many developed nations in North America, Europe, and Asia.6
The financial cost to society is huge, currently estimated at more than 200 billion Euros per annum in Europe and $150 billion per annum in the US.7
While important advances in the understanding of pain mechanisms have increased potential therapeutic options, management of chronic pain remains generally unsatisfactory; two-thirds of patients report dissatisfaction with current treatments and most of them complain about chronic pain persisting for many years.7
Achieving adequate pain relief through new therapeutic strategies is therefore important for achieving control of symptoms and improving quality of life in patients with chronic pain.3
The Role of Opioids in the Management of Chronic Pain
Chronic pain treatment typically involves Schedule II full μ-opioid receptor agonists;3 however, different approaches to the management of cancer and non-cancer chronic pain have been observed in clinical practice. Whereas there is widespread consensus worldwide for the use of opioids in the management of pain associated with advanced-stage cancer, where the benefit of pain relief fully justifies the risks of long-term opioid therapy, the use of opioids in CNCP is still controversial.5
Nevertheless, in Europe, an increase in strong opioid prescriptions has also occurred, with most prescriptions being for CNCP. In the UK, it has been estimated that nearly one million people are using some form of opioid; in France prescription opioid use between 2004 and 2017 at least doubled.8
In Italy, an almost four-fold increase in opioid prescriptions has been documented between 2007 and 2015, potentially correlated to the observed reduction in the prescription of NSAIDs.5
The most impactful consequences of long-term opioid treatment are the development of tolerance, physical and mental addiction and the potential risk of incurring a substance use disorder (SUD). In the United States of America, where more than 3% of the adult population receives chronic opioid therapy, there is a real epidemic linked to the misuse of opioid drugs prescribed for non-cancer pain control. The phenomenon affects almost all age groups, and the highest mortality rate, in both sexes, is seen in the 45–54-year age range.5
The risk of opioid addiction makes the treatment of chronic pain quite challenging for both patients and physicians, while adhering to state-mandated regulations and preventing misuse. Potentially safer yet equally effective therapeutic strategies are needed.3
A possible successful approach may be the use of strong opioids at low doses, to be preferred to weak opioids at high doses: in fact, the development of opioid dependence disorders is less likely in patients who are prescribed strong opioids in the longer term. This may suggest a mediatory role of pseudoaddiction, whereby patients receiving inadequate analgesia (weak opioids prescribed over short-term periods) exhibit addiction-like behavior in an effort to achieve successful pain management.9
New evidence suggest that long-term side effects of strong opioids can differ according to their pharmacodynamic profile (above all the degree of mu-opioid receptor stimulation), their daily dose, route of administration (oral vs transdermal) and formulation (long-acting vs short acting).10
Among strong opioids, buprenorphine, a partial mu-opioid agonist which has been in clinical use for over 25 years as parenteral, sublingual, and transdermal formulations, presents peculiar pharmacological characteristics, which make it a valid therapeutic option for the management of CNCP. Unlike full mu-opioid agonists, buprenorphine shows a ceiling effect on those receptors not directly involved in pain transmission such as at the rewarding areas, which may limit the abuse potential and may result in a wider safety margin.11 In addition, buprenorphine also shows a partial agonist profile for stimulating of mu-opioid receptors in respiratory centers thus reducing the risk of respiratory depression.12,13
Buprenorphine is suitable for use in multiple patient populations: it can be used in patients with a dual diagnosis of chronic pain and opioid use disorder, those requiring concomitant medications (as fewer interactions may occur with other drugs), those with renal impairment, in the elderly and in patients with cardiovascular comorbidities, as no clinically significant prolongation in the QT interval is observed at the therapeutic dose of 10 mcg/h.14 At supratherapeutic doses of 40 and 80 mcg/h, BTDS treatment can produce prolongation of QT interval but not large enough to be considered associated with proarrhythmic effects.15 Additional benefits of the drug include the absence of immunosuppressive action and negative impact on the hypothalamic-pituitary-adrenal pathway, and the ability to reduce anxiety and depression.3
Buprenorphine is an effective analgesic with similar or even better tolerability compared with other opioids, which can play an important role, at low doses, in the treatment of chronic pain as the preferential first-line opioid in clinical practice.16
The Role of Primary Care in the Management of Chronic Pain
Chronic pain is one of the most common reasons adults seek medical care.3 In most countries, the majority of patients who experience chronic pain (20% of the general population) are managed in primary care by general practitioners (GPs), while only 0.5–2% are ever referred to secondary care for pain management. Consultations on pain account for 22% of all primary care consultations: patients affected by chronic pain visit their GPs twice as often as patients without chronic pain.17
Primary care management should incorporate both pharmacological and non-pharmacological approaches, including psychotherapy, self-management, physiotherapy, peripheral nervous system stimulation, complementary therapies and comprehensive pain-management programs.18
Complete awareness of available analgesic agents and adequate knowledge of their efficacy and safety profiles are crucial for their proper inclusion into a successful management strategy of CNCP.
Aim
The purpose of the present work was to evaluate the knowledge and prescriptive habits of pain specialists and other clinicians involved in the management of CNCP, with a special focus on the use of opioids in clinical practice.
Methods
This research was exempt from review or approval by an institutional review board or ethics committee because no patients or clinical data were included in this research. Delphi method was used to reach the above-mentioned aim.19 It represents an indirect, anonymous, iterative process aimed at achieving consensus among experts on specific topics, especially regarding disease management and drug therapy.
A Board of specialists was appointed as a scientific committee; in charge of designing and supervising the study. The Board included 5 pain therapists, 1 pharmacologist, all with extensive clinical and scientific expertise in the field of pain management and research, and 1 methodology expert.
A Panel of 100 experts in the field of pain management was thereafter selected by the Board, on the basis of their skills in research and/or clinical experience.
No strict criteria for engagement of panel experts were used, being the community of pain therapists in Italy small enough for the Board to scout practitioners who distinguished themselves amongst their clinical or academic institutions. The members of the Board could therefore compose a list of 101 panel members, indeed big enough to include most relevant differences in terms of clinical background and geographical area, and thus limit possible selection bias with its width. Still, the panel remains a convenience sample.
The Board drafted and discussed a series of statements, based on available literature and personal clinical expertise, about specific topics on pain pathophysiology and treatment, which are particularly controversial within the scientific and/or clinical community.
The statements were divided into four main categories:
a. general concepts
b. non-opioid therapy
c. opioid therapy
d. interventional therapy
In the preparation phase of the first round of questionnaire submission, each member of the Board, according to their specific area of expertise, was assigned a sub-topic and requested to draft candidate statements related to it, together with linked literature references. Approximately 50 candidate statements were thus produced and submitted to the Scientific Chair of the Board, who jointly examined them together with the senior methodology expert, in order to check what evidences could support the statement and, at the same time, the absence from the statement of possible clues that might bias responses by the panel.
Candidate statements were assembled in the draft questionnaire; then, a second review was carried out, aimed at minimizing redundancies and assuring consistent wording across statements. An external expert was also involved in this phase, who provided the Board with feedbacks on the adequateness of wording. The expert, whose role of beta-tester could have brought him to biased insights on the proposed statements, was not involved in any further phase of the research, in order to avoid data pollution.
The resulting questionnaire was made available to the Panel using a dedicated online platform. An encoded key was issued to each of the panelists, so that they could login to the platform with no disclosure of their identities that were only known to a third-party agency which never communicated any related information to the Board. Clinicians were then invited to indicate their level of agreement on the proposed statements on a 5-point Likert scale (1: strongly disagree; 2: disagree; 3: partially agree; 4: agree; 5: strongly agree). In addition to the questionnaire, the invitation sent to the panelists also included a link to an online thesaurus with operational definitions of key points elaborated by the statements, named WikiDDOL which was specifically drawn up by the Board in order to provide panelists with a source of disambiguation in meanings of key words and to better understand the meaning of the statements and definitions used in them. However, the definitions in WikiDDOL were written in a way to avoid influencing the panelists’ attitudes when answering.
Before starting the analysis, the threshold for consensus was set at minimum 66.6% of the number of respondents with a level of agreement ≥4 (Agree or Strongly agree), considered by the Board as fit to establish a “strong consensus”. Only levels 4 and 5 of agreement were therefore considered as consensus in the analysis of the results.
A first round of Delphi was then launched, allocating 12 calendar days for panelists to answer. The deadline was later postponed by 3 more calendar days, and a reminder was sent to the panel, also in order to solicitate those who had not answered yet. Eighty-four panelists, out of the 100 that were invited, answered the first round of Delphi. Data were analyzed and presented to the board, both with a full table (including statistics for all statements) and with explanatory graphs for each statement.
The analysis of preliminary data enabled board members to highlight statements whose result was not clear or not consistent with other statements. In a plenary session, the board thus reviewed the Delphi questionnaire rephrasing the statements that supposedly introduced a bias by means of ambiguous wording: Two statements were found to contain two separate sentences, and were thus split into sub-sentences in order to make them clearer. In 2 cases, the statement was considered unfit to be clarified as is, and again sub-sentences were used to provide panelists with detailed sub-topics to express their agreement on.
The reviewed questionnaire was then approved as ready to be launched for the second round, and implemented on the online platform. This time, 14 calendar days were allocated for answering and the deadline was then postponed by 2 more calendar days. Eighty-nine panelists, out of the total 100 that were invited, answered the second round of Delphi. Again, data was analyzed and presented to the board, with both a full table and explanatory graphs. In addition, a comparison chart was produced, with a cross check between answers in first and second round. In the overall process, the matching procedure was carried out by means of an encoded referencing number for each panelist, always preserving complete anonymity and data safety.
Due to the restrictions imposed by the current pandemic situation, all activities were done virtually, which in some instances limited the opportunities for discussion and sharing of opinions/expertise.
Results
The Board of specialists elaborated a total of 36 statements: four items (number 6, number 20, number 33 and number 36) included two possible options requiring a separate evaluation (for a total of 40 requested answers).
A total of 100 clinicians were included in the Expert Panel and invited to vote on the proposed items. Respondents were 84 (84%) and 89 (89%) in the first and second round, respectively.
Consensus was achieved for 29 out of 36 and 32 out of 40 items in the first and second round, respectively.
Table 1 shows the list of statements. The number next to the statement indicates the order in which they are presented during the two Delphi rounds.
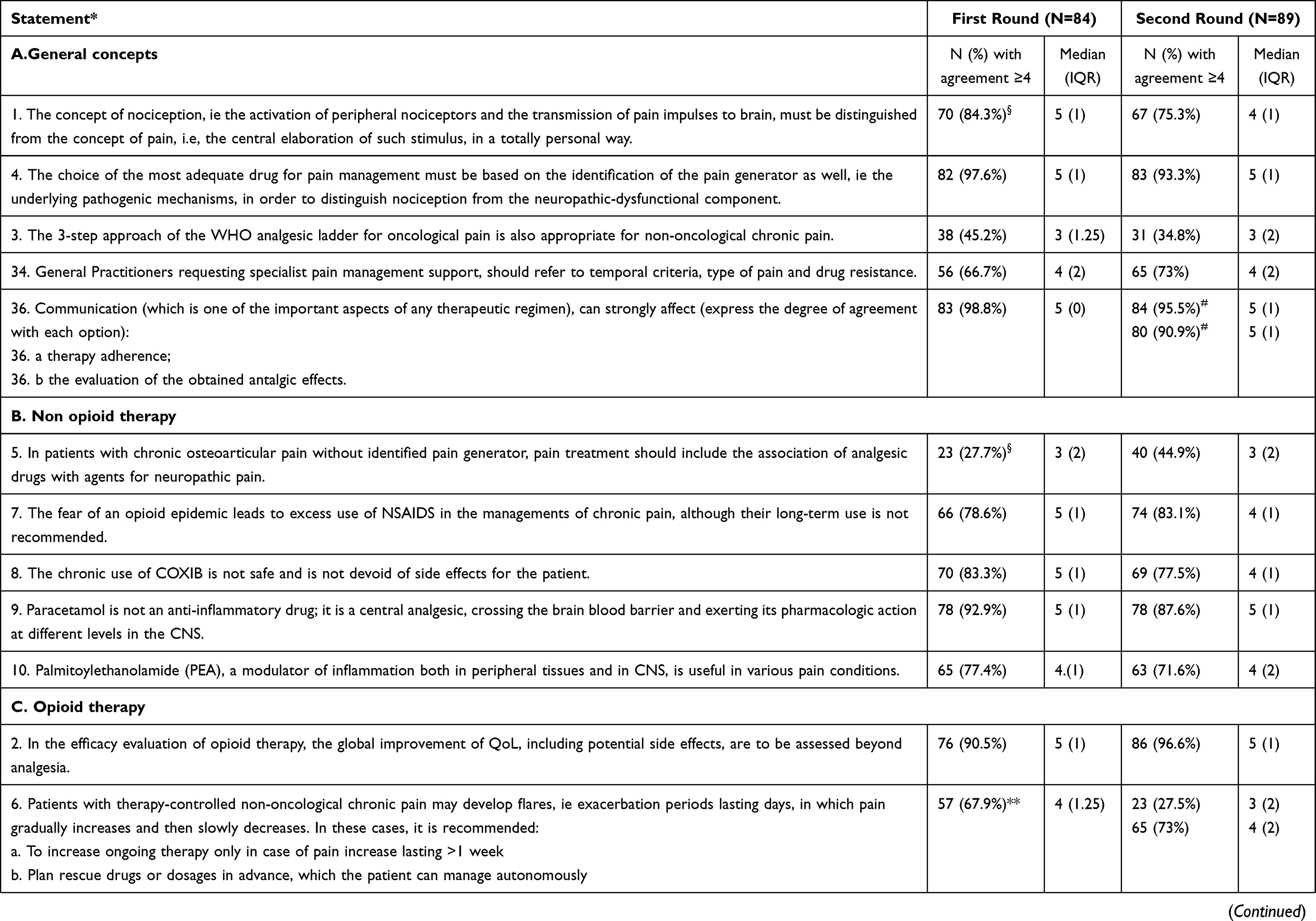 | 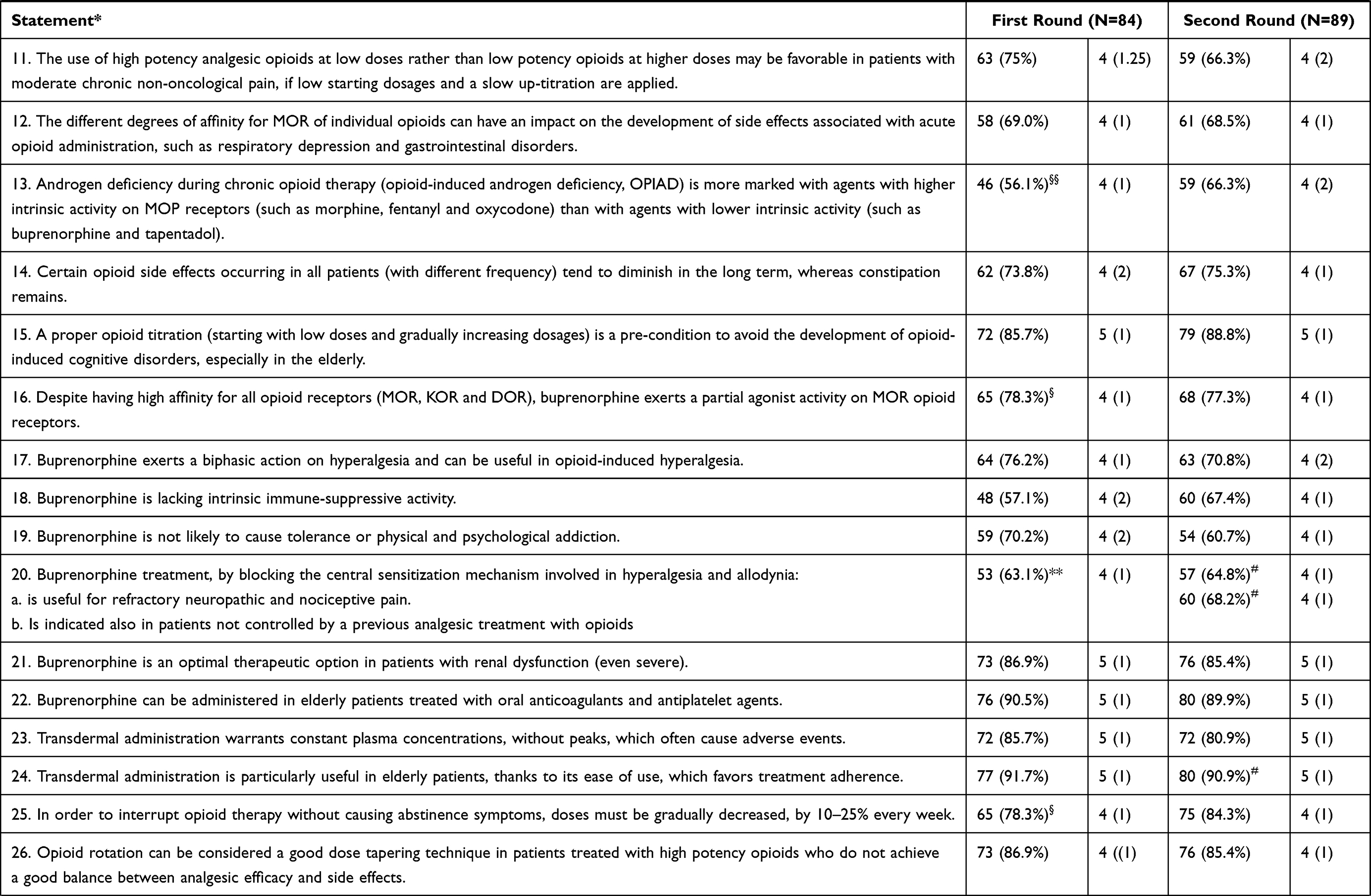 | 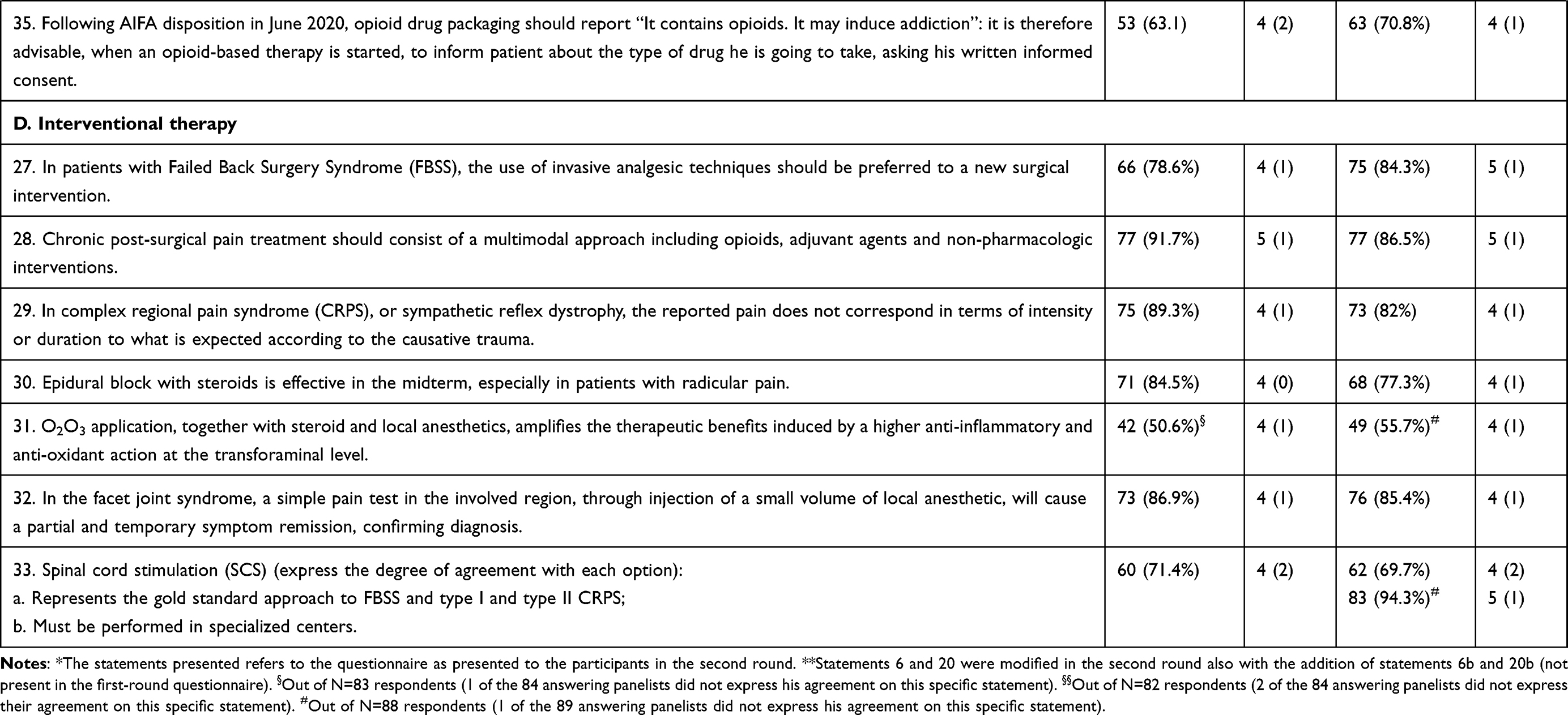 |
Table 1 List of Statements with the Respective Level of Consensus Reached During the First and Second Round |
For each statement, the number and percentage of respondents, as well as median and interquartile range of the agreement level are reported. The statements presented in the tables refer to the questionnaire as presented to the participants in the second round.
Discussion
Most of the proposed statements reached consensus either in the first or second round of the Delphi survey, suggesting a generally homogeneous approach to CNCP management among involved clinicians. However, the lack of consensus recorded for most items regarding opioid use confirms the need to fill important gaps in the knowledge of available agents and in the implementation of successful strategies.
Notably, most of the lack of consensus derived from participants expressing a low level of agreement (3 on the Likert scale), suggesting a neutral position derived from a lack of knowledge or direct experience rather than a strong contrary opinion.
A detailed discussion of the most relevant statements is reported below:
-The fear of an opioid epidemic leads to an excess use of NSAIDS in the managements of chronic pain, although their long-term use is not recommended (statement 7).
Comments: Consensus was fully achieved for this statement in both the first (78.76%, median 5) and second (83.1%, median 4) round, suggesting a general agreement about the fact that the use of NSAIDs is often excessive and inappropriate, despite the recommendations by current guidelines to avoid their long-term use. NSAIDs are associated with 30% of hospital admissions for preventable adverse drug reactions.19 Data from multiple placebo-controlled trials and meta-analyses studies highlight the adverse effects of NSAIDs in terms of gastrointestinal, cardiovascular, hepatic, renal, cerebral and pulmonary complications. The action of NSAIDs on major organs including stomach, small intestine, heart, liver, kidney, respiratory tract and brain is mainly mediated through PGHS-dependent prostanoid modulation and alteration of mitochondrial functional integrity, leading to mitochondrial oxidative stress generation, depolarization of mitochondrial transmembrane potential and consequent cell death.19
Inappropriate use of NSAIDS is particularly frequent in elderly people: a large population-based study conducted in Southern Italy recently demonstrated that 36.6% of elderly patients were incident NSAID users, and 9.2% were prescribed ketorolac/indomethacin, which should be avoided in elderly subjects. Furthermore, at least half of all elderly people with chronic kidney disease or congestive heart failure were prescribed NSAIDs, though these drugs should be avoided.20
The 3-step approach of the WHO analgesic ladder for oncological pain is appropriate also for non-oncological chronic pain (Statement 3).
Comments: Complete disagreement with this statement was achieved both in the first (45.2%, median 3) and second (34.8%, median 3) round, confirming the need to identify treatment strategy alternatives to the WHO analgesic ladder, which better meet the pathophysiological mechanisms and clinical manifestations of CNCP.
The WHO analgesic ladder, proposed by the World Health Organization (WHO) in 1986, is a strategy developed following the recommendations of an international group of experts to provide adequate pain relief for cancer patients. Such strategy has undergone several modifications over the years and is currently applied for managing cancer pain, as well as non-cancer painful conditions associated with degenerative disorders, musculoskeletal diseases, neuropathic pain disorders, and other types of chronic pathologies.21
The advantage of the analgesic ladder is its ease of use, even by non-pain medicine experts. However, one important limitation of the WHO pain ladder derives from the role attributed to NSAIDs as first step drugs, which could lead to a false belief that this represents the most secure treatment, favoring its long-term use. In fact, long-term use of NSAIDs combined with opioids for the treatment of moderate pain (second step) can lead to much more serious side effects than those described for opioids.21
Moreover, since the original issue of the WHO 3 step analgesic ladder in 1986, notions about neurobiology of pain have changed considerably, leading to a greater recognition of the various types of pain (eg, nociceptive, neuropathic or nociplastic), and of the complexity of pain pathogenesis: as a consequence, a number of new pain management strategies have emerged.22 For instance, the International Association For The Study Of Pain (IASP) suggested adopting a therapeutic approach more focused on the type of pain and on the mechanism of action of the drugs used to treat it. Therefore, the use of steroids or NSAIDs is more appropriate for chronic nociceptive pain with an inflammatory basis, whereas opioids or non-opioids analgesics are recommended for low-inflammatory nociceptive pain, and antidepressants or anticonvulsants may be useful for neuropathic pain, as well as specific drugs for certain rheumatologic conditions.23
The use of the three-step ladder in CNCP very likely contributed to opioid analgesic overuse and escalation, responsible for the so-called “opioid crisis” in the United States, where approximately 130 persons die each day from opioid overdoses, with 68% of the drug overdose deaths in 2017 involving an opioid medication.22 Nowadays experts in pain medicine find the original analgesic ladder inappropriate for successful pain management, as it only concentrates on the physical aspect of pain.21 It is now necessary to incorporate both multimodal and multidisciplinary approaches into the WHO Three-step ladder, in particular for the management of CNCP. As a chronic condition involving physiological, social, and subjective aspects, CNCP should not be treated with pharmacological agents alone. Therefore, a revised analgesic ladder has been recently proposed, including integrative therapies at each step of the original WHO pain ladder.22 There have been other proposed suggestions in an attempt to offer a more precise methodology: Cuomo et al proposed the so-called “multimodal trolley approach,” which gives importance to the physical, psychological, and emotional causes of pain.24
In patients with chronic osteoarticular pain without identified pain generator, pain treatment should include the association of analgesic drugs with agents for neuropathic pain (statement 5).
Comments: Wide disagreement with this statement was recorded in both the first (27.7%, median 3) and second (44.9%, median 3) round, suggesting a lack of consensus on the use of the association of analgesics with drugs for neuropathic pain, despite the available experimental evidence supporting the involvement of central sensitization in both chronic and neuropathic pain. Osteoarthritis (OA) is a debilitating chronic condition, whose pathology includes cartilage erosion, joint remodeling and joint inflammation.25 Joint pain associated with OA has a strong mechanical component, triggered by specific activities and relieved by rest. The pain becomes more constant over time, and neuropathic traits can be present in the advanced disease.26 Since different pathogenic mechanisms (inflammatory, nociceptive, neuropathic) are involved in generating osteoarticular pain,27 the use of multiple drugs with different mechanisms of action is required to achieve pain control. A better knowledge of the pathophysiology of pain and a higher awareness of the available therapeutic strategies are essential prerequisites for a more homogeneous approach to osteoarticular pain in clinical practice.
Patients with therapy-controlled non-oncological chronic pain may develop flares, ie, exacerbation periods lasting days, in which pain gradually increases and then slowly decreases. In these cases, it is recommended: a. to increase ongoing therapy only in case of pain increase lasting >1 week; b. to plan rescue drugs or dosages in advance, which the patient can manage autonomously (statement 6).
Comments: A complete lack of consensus (27.4%, median 3) was recorded for the first option given for this item, which is consistent with the strong consensus (73%) obtained for the second option. This reflects a homogeneous approach to the management of flares in patients with CNCP, consisting in the planning of doses and timing of available rescue medications in advance, which the patient can use autonomously. Dosage increase of ongoing therapy is not considered a proper solution for pain exacerbations, which generally require a more specific intervention on the different components of pain.28
The use of high potency analgesic opioids at low doses rather than low potency opioids at higher doses may be favorable in patients with moderate chronic non-oncological pain, if low starting dosages and a slow up-titration are applied (statement 11).
Comments: Consensus reached in the first round was not fully confirmed in the second round (66.3%, median 4) with only 9 participants expressing disagreement. This suggests that the approach to moderate CNCP with strong opioids is still not completely shared by pain therapists.
In 2012, the European Association of Palliative Care revised the second step of WHO ladder and recommended to include strong opioids at low doses in it. Low doses were identified as <20 mg per day for oxycodone, <30 mg per day for morphine and <4 mg/day for hydromorphone.29 At that time, no other strong opioids were available at low doses while now we have low dose formulations of 25 mg tapentadol tablets, 12mcg/h fentanyl patch and 5–7, 5-10-15-20 mcg/h buprenorphine patch. In wikiDDOL, these informations are included.
The preferential use of strong opioids, which is generally accepted for cancer pain, is still not unanimously implemented in the management of CNCP. A recently published Italian Delphi Survey on the rational use of analgesics in patients with cancer pain confirmed the consensus among pain specialists on the use of strong opioids, at low doses, to provide an adequate pain control in oncological patients with mild or moderate pain not controlled with NSAIDs.30 CDC guidelines31 and ASIPP recommendations32 support the use of short acting low-potency opioids such as tramadol and codeine (also associated with acetaminophen) for management of acute to moderate pain and for exacerbation of chronic pain. However, short acting formulations are associated with wider fluctuations of plasma concentrations, which may induce tolerance and addiction.33 In this respect, variability in opioid dosage may be a risk factor for opioid overdose, suggesting that practitioners should seek to minimize dose variability when managing long-term opioid therapy.34 Moreover, prescription of strong, rather than weak opioids was associated with a significantly lower incidence of opioid dependence or abuse, suggesting that the use of low-dose high potency opioids should be preferred to high-dose low-potency agents.10
Strong opioids, unlike weak opioids, can significantly differ from each other in terms of both pharmacodynamic and pharmacokinetic and this can affect their analgesia and side effects profiles. Indeed, when choosing a strong opioid for long-term pain relief, many considerations about opioids and patient characteristics need to be made. Among potent opioids, buprenorphine has a unique pharmacology, allowing important therapeutic applications as an analgesic of low abuse potential. Buprenorphine binds to all three major opioid receptors (mu, kappa, delta), and also binds to the orphan-like receptor, the receptor for orphanin FQ/nociceptin, with lower affinity. Its action as a partial agonist at traditional mu receptors potentially contributes to its ceiling effect on respiratory depression, whereas its effect as an inverse agonist at the kappa receptor is possibly responsible for its anti-hyperalgesic activity, less sedation and dysphoria. Moreover, its action as an antagonist at delta receptors is possibly responsible for its antidepressant activity. Finally, its affinity for a recently discovered structurally distinct subtype of mu receptor involved in analgesia truly distinguishes buprenorphine from other analgesics.35
Buprenorphine is increasingly recognized as an effective analgesic with an improved therapeutic index relative to certain potent opioids. Advantages of buprenorphine include a ceiling on the euphoriant effects and on respiratory depression, but not on analgesia at doses up to 32 mg/day, less physical dependence, absence of risk hypogonadism risk and of immunosuppressant effect.35
Despite being classified as a partial agonist, buprenorphine produces analgesia with only 5–10% of receptors occupied; because buprenorphine has a high affinity and long-lasting binding to mu receptors, it would seem rational that it would produce subadditive analgesia when combined with other opioids.35 Moreover, animal studies revealed that the effect of buprenorphine is antagonized by intrathecal but not intracerebroventricular injection of naloxone. These data suggest an additional supraspinal component insensitive to naloxone, Pertussis toxin (PTX) and nociceptin/orphanin-FQ in the supraspinal analgesic effect of buprenorphine. In addition, a possible involvement of Gz protein and protein Ser/Thr phosphatase has been suggested, giving further insight into the mechanism of action of buprenorphine.36
The different degrees of affinity for MOR of individual opioids can have an impact on the development of side effects associated with acute opioid administration, such as respiratory depression and gastrointestinal disorders (statement 12).
Comments: Consensus was achieved on this statement both in the first (69.0%, median 4) and second (68.5%) round, suggesting a general agreement of clinicians on the risks associated with acute opioids administration. However, the kinetic and dynamic profile of different opioids is associated to different side effects, as well as different degrees of compliance by the patients. It is conceivable that opioids such as buprenorphine, which show a ceiling effect on MOR expressed in the bulb, exert less side effects related to the respiratory center regulation.13,15
Androgen deficiency during chronic opioid therapy (opioid-induced androgen deficiency, OPIAD) is more marked with agents with higher intrinsic activity on MOP receptors (such as morphine, fentanyl and oxycodone) than with agents with lower intrinsic activity (such as buprenorphine and tapentadol) (statement 13).
Comments: A consensus was not reached in both the first (56.1%) and second (66.3%) round. This suggests that the assumption that opioid side effects mainly depend on the degree of activity on the mu receptor (ie, mu-load) is not completely shared among pain therapists. Many clinicians think that other factors are also involved like opioid daily dose and formulation.
The use of opioids in patients with CNCP can be associated with opioid-induced androgen deficiency (OPIAD) in men, deriving from the opioid-induced suppression of gonadotropin-releasing and luteinizing hormones and subsequent impairment of testosterone levels. Besides having a significant negative impact on sexual function, mood, bone density and body composition, OPIAD can also interfere with pain control and lead to hyperalgesia, worsening sexual dysfunction and mood impairment and resulting in poor quality of life.37–40
Unlike morphine, buprenorphine has only limited endocrine effects and can be used for months without inducing hypogonadism.40 In comparative studies in patients with OPIAD and sexual dysfunction, buprenorphine caused less marked reduction of testosterone levels and a lower incidence of sexual dysfunction, compared with methadone.41 Physicians should therefore prefer opioids with a lower MOP affinity when prescribing opioid therapy: the evaluation of serum testosterone levels should be considered in chronic opioid male users and the decision to initiate testosterone treatment should be based on the clinical profile of individuals, in consultation with the patient.37
The higher the daily opioid dose, the higher the risk for OPIAD development:39 patients treated with opioid doses >60 mg of morphine equivalents per day (MED) and particularly those treated with doses >100 mg of MED are at risk of and must therefore be carefully monitored for the development of hypogonadism. In this respect, low-dose transdermal buprenorphine formulations may be advantageous over other opioids.37
Buprenorphine is lacking intrinsic immune-suppressive activity (statement 18) and is not likely to cause tolerance or physical and psychological addiction (statement 19).
Comments: The lack of a full consensus about these sentences, in both rounds, reveals the need of better knowledge of buprenorphine. Indeed, unlike morphine and fentanyl, buprenorphine does not impact the immune system and its slow-release formulations (such as the transdermal ones) are associated with lower risk of abuse, tolerance and addiction.35,42
Transdermal buprenorphine has demonstrated good overall efficacy and tolerability in clinical studies in patients with CNCP, such as musculoskeletal pain associated with osteoarthritis and low back pain, among others. Transdermal buprenorphine is a versatile analgesic that has been shown to offer effective pain relief in a variety of different patient populations and cancer as well as non-cancer pain syndromes.42
In addition to providing effective analgesia, transdermal buprenorphine may be beneficial for functional improvement in patients with CNCP, improving the ability of treated patients to perform daily life activities. Transdermal buprenorphine may also be combined with other agents for multi-mechanistic pain syndromes.42
Moreover, buprenorphine, due to its pharmacodynamic profile, owns a reduced tolerance since it behaves similarly to those new opioids that have been defined as “biased” agonists such as oliceridine. These “biased” profile is due to the reduced capability of the drug in recruiting downstream signaling β-arrestin 2.43 An important difference is that oliceridine shows a similar withdrawal syndrome when injected with the naloxone, confirming the hypothesis that the β-arrestin 2 pathway is critical in tolerance but not in the addiction,44,45 while buprenorphine is characterized by a lower risk of abuse and, more importantly, it has been properly used in detoxification protocols of opioid abuse.46
Buprenorphine treatment, by blocking the central sensitization mechanism involved in hyperalgesia and allodynia: a. is useful for refractory neuropathic and nociceptive pain; b. Is indicated also in patients not controlled by a previous analgesic treatment with opioids (statement 20).
Comments: Although full consensus (64.8%, median 4) was not recorded for the first option given for this item, consensus (68.2%, median 4) was obtained for the second option: the high median value (4) observed for both items suggests a somewhat high awareness of buprenorphine’s role in the management of CNCP, also in patients not responding to previous opioid therapies. The lack of consensus about its use for refractory neuropathic and nociceptive pain despite the available evidence,47,48 probably reflects the need of combination therapy for this kind of pain. Treatment of neuropathic pain is indeed multimodal since the cellular and molecular mechanisms at the basis of tactile allodynia are still poorly understood. Spinal microglia cells have a role in the pathogenesis of neuropathic pain of peripheral and central origin. Microglia cells proliferate and corroborate the neural sensitization by releasing pro-inflammatory factors.49 It has been suggested that the opioid-induced abnormal hyperalgesia could be due to their effect on microglia cells, particularly by the stimulation of the Toll Like receptor 4 (TLR4) on these cells.50,51
About the statements regarding interventional therapy, a large consensus was reached about the midterm efficacy of epidural steroids for radicular pain and the long-term results of Spinal Cord Stimulation for the treatment of Complex regional Pain Syndromes and Failed Back Pain Syndromes (statements 30, 33), according to the latest evidence in the literature.52–54
Instead, no consensus was reached on the utility of adding O2O3 to steroids and local anestethics at the transforaminal level (statement 31).
Comments: The lack of consensus for the 31st statement (55.7%, median 4) reflects poor knowledge on the high anti-inflammatory and antioxidant actions of O2O3 but also reflects the paucity of controlled clinical trials on ozone therapy.55,56 However, the potential advantages of different invasive intervention for CNCP call for a wider implementation of such strategies for the optimization of pain control.
Conclusion
Chronic pain is a global epidemic, exacerbated by the risks of harmful use of opioids, diversion, and dependence. Chronic pain patients often have multi-mechanistic pain (eg, nociceptive pain with an additional neuropathic and/or visceral component), which requires a specific and multifaceted approach.
Despite difficulties associated with the current pandemic situation, which imposed all activities to be performed on-line, the results of the present Delphi are very interesting, since they suggest a few gaps in the awareness of the available strategies for CNCP management, reflecting the difficulties often encountered by clinicians in selecting the appropriate treatment and by patients in having their symptomatology completely controlled.
In particular, we focused on Buprenorphine since its unique mechanism of action that we recently conceptualized.57 In particular, this molecule has a very interesting kinetic profile and a poorly understood mechanism of action.
In general, a better knowledge of available agents, with a clear explanation of the specific pharmacological properties and clinical advantages of some drugs such as buprenorphine, together with a better definition of the candidate patients to be treated, will help to optimize pain treatment in both primary care and hospital settings and to improve pain control in CNCP patients.
The main limitation of this study is the presence of a sample selection bias which remains a convenience sample.
Acknowledgments
Project management support was provided by Camilla Ciani, Poliste Srl.
Editorial support was provided by Cristina Germanà, MD, medical writer and Elena Sarugeri, MD, medical writer.
These supports were made possible thanks to an unrestricted grant of Sandoz SpA.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
2. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273–e283. doi:10.1016/j.bja.2019.03.023
3. Pergolizzi JV
4. Hylands-White N, Duarte RV, Raphael JH. An overview of treatment approaches for chronic pain management. Rheumatol Int. 2017;37(1):29–42. doi:10.1007/s00296-016-3481-8
5. Fornasari D, Gerra G, Maione S, et al. Treatment of chronic pain in Italy: therapeutic appropriacy of opioids and fear of addiction: the situation in Italy vs. USA. Pharmaadvances. 2020;1:31–40.
6. Pergolizzi JV
7. van Hecke O, Torrance N, Smith BH. Chronic pain epidemiology and its clinical relevance. Br J Anaesth. 2013;111(1):13–18. doi:10.1093/bja/aet123
8. Guillou-Landreat M, Quinio B, Le Reste JY, et al. Analgesic opioid misuse and opioid use disorder among patients with chronic non-cancer pain and prescribed opioids in a pain centre in France. Int J Environ Res Public Health. 2021;18(4):2097. doi:10.3390/ijerph18042097
9. Higgins C, Smith BH, Matthews K. Incidence of iatrogenic opioid dependence or abuse in patients with pain who were exposed to opioid analgesic therapy: a systematic review and meta-analysis. Br J Anaesth. 2018;120(6):1335–1344. doi:10.1016/j.bja.2018.03.009
10. Davis MP, Mehta Z. Opioids and chronic pain: where is the balance? Curr Oncol Rep. 2016;18(12):71. PMID: 27812860. doi:10.1007/s11912-016-0558-1.
11. Johnson RE, Fudala PJ, Payne R. Buprenorphine: considerations for pain management. J Pain Symptom Manage. 2005;29(3):297–326.
12. Webster LR, Hansen E, Cater J, Smith T. A Phase I placebo-controlled trial comparing the effects of buprenorphine buccal film and oral oxycodone hydrochloride administration on respiratory drive. Adv Ther. 2020;37(11):4685–4696. doi:10.1007/s12325-020-01481-0
13. Pedersen MF, Wróbel TM, Märcher-Rørsted E, et al. Biased agonism of clinically approved μ-opioid receptor agonists and TRV130 is not controlled by binding and signaling kinetics. Neuropharmacology. 2020;166:107718. doi:10.1016/j.neuropharm.2019.107718
14. Behzadi M, Joukar S, Beik A. Opioids and cardiac arrhythmia: a literature review. Med Princ Pract. 2018;27(5):401–414. doi:10.1159/000492616
15. Harris SC, Morganroth J, Ripa SR, Thorn MD, Colucci S. Effects of buprenorphine on QT intervals in healthy subjects: results of 2 randomized positive and placebo-controlled trials. Postgrad Med. 2017;129(1):69–80. doi:10.1080/00325481.2017.1270156
16. Fishman MA, Kim PS. Buprenorphine for chronic pain: a systemic review. Curr Pain Headache Rep. 2018;22(12):83. doi:10.1007/s11916-018-0732-2
17. Mills S, Torrance N, Smith BH. Identification and management of chronic pain in primary care: a review. Curr Psychiatry Rep. 2016;18(2):22. doi:10.1007/s11920-015-0659-9
18. Jones J, Hunter D. Consensus methods for medical and health services research. BMJ. 1995;311:376–380. doi:10.1136/bmj.311.7001.376
19. Bindu S, Mazumder S, Bandyopadhyay U. Non-steroidal anti-inflammatory drugs (NSAIDs) and organ damage: a current perspective. Biochem Pharmacol. 2020;180:114147. doi:10.1016/j.bcp.2020.114147
20. Ingrasciotta Y, Sultana J, Giorgianni F, et al. Analgesic drug use in elderly persons: a population-based study in Southern Italy. PLoS One. 2019;14(9):e0222836. doi:10.1371/journal.pone.0222836
21. Anekar AA, Cascella M. WHO analgesic ladder. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; May 17, 2020. PMID: 32119322.
22. Yang J, Bauer BA, Wahner-Roedler DL, Chon TY, Xiao L. The modified WHO analgesic ladder: is it appropriate for chronic non-cancer pain? J Pain Res. 2020;17(13):411–417. doi:10.2147/JPR.S244173
23. Lippe PM, Brock C, David J, Crossno R, Gitlow S. The first national pain medicine summit–final summary report. Pain Med. 2010;11(10):1447–1468. doi:10.1111/j.1526-4637.2010.00961.x
24. Cuomo A, Bimonte S, Forte CA, Botti G, Cascella M. Multimodal approaches and tailored therapies for pain management: the trolley analgesic model. J Pain Res. 2019;12:711–714. doi:10.2147/JPR.S178910
25. Staunton CA, Lewis R, Barrett-Jolley R. Ion channels and osteoarthritic pain: potential for novel analgesics. Curr Pain Headache Rep. 2013;17(12):378. doi:10.1007/s11916-013-0378-z
26. Malfait AM, Schnitzer TJ. Towards a mechanism-based approach to pain management in osteoarthritis. Nat Rev Rheumatol. 2013;9(11):654–664. doi:10.1038/nrrheum.2013.138
27. Fu K, Robbins SR, McDougall JJ. Osteoarthritis: the genesis of pain. Rheumatology. 2018;57(suppl_4):iv43–iv50. doi:10.1093/rheumatology/kex419
28. Chen L, Vo T, Seefeld L, et al. Lack of correlation between opioid dose adjustment and pain score change in a group of chronic pain patients. J Pain. 2013;14(4):384–392. doi:10.1016/j.jpain.2012.12.012
29. Caraceni A, Hanks G, Kaasa S, et al. Use of opioid analgesics in the treatment of cancer pain: evidence-based recommendations from the EAPC. Lancet Oncol. 2012;13:e58–68. doi:10.1016/S1470-2045(12)70040-2
30. Varrassi G, De Conno F, Orsi L, et al. Cancer pain management: an Italian Delphi survey from the Rational Use of Analgesics (RUA) group. J Pain Res. 2020;8(13):979–986. doi:10.2147/JPR.S243222
31. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain – United States, 2016. JAMA. 2016;315:1624–1634. doi:10.1001/jama.2016.1464
32. Manchikanti L, Kaye AM, Knezevic NN, et al. Responsible, safe, and effective prescription of opioids for chronic non-cancer pain: American Society of Interventional Pain Physicians (ASIPP) guidelines. Pain Physician. 2017;20(2S):S3–S92. doi:10.36076/ppj.2017.s92
33. Pedersen L, Borchgrevink PC, Riphagen II, Fredheim OM. Long- or short-acting opioids for chronic non-malignant pain? A qualitative systematic review. Acta Anaesthesiol Scand. 2014;58(4):390–401. doi:10.1111/aas.12279
34. Glanz JM, Binswanger IA, Shetterly SM, Narwaney KJ, Xu S. Association between opioid dose variability and opioid overdose among adults prescribed long-term opioid therapy. JAMA Netw Open. 2019;2(4):e192613. doi:10.1001/jamanetworkopen.2019.2613
35. Davis MP, Pasternak G, Behm B. Treating chronic pain: an overview of clinical studies centered on the buprenorphine option. Drugs. 2018;78(12):1211–1228. doi:10.1007/s40265-018-0953-z
36. Ding Z, Raffa RB. Identification of an additional supraspinal component to the analgesic mechanism of action of buprenorphine. Br J Pharmacol. 2009;157(5):831–843. doi:10.1111/j.1476-5381.2009.00209.x
37. Coluzzi F, Billeci D, Maggi M, Corona G. Testosterone deficiency in non-cancer opioid-treated patients. J Endocrinol Investig. 2018;41:1377–1388. doi:10.1007/s40618-018-0964-3
38. Bawor M, Bami H, Dennis BB, et al. Testosterone suppression in opioid users: a systematic review and meta-analysis. Drug Alcohol Depend. 2015;1(149):1–9. doi:10.1016/j.drugalcdep.2015.01.038
39. Lamprecht A, Sorbello J, Jang C, Torpy DJ, Inder WJ. Secondary adrenal insufficiency and pituitary dysfunction in oral/trans- dermal opioid users with non-cancer pain. Eur J Endocrinol. 2018;179:353–362. doi:10.1530/EJE-18-0530
40. Aloisi AM, Aurilio C, Bachiocco V, et al. Endocrine consequences of opioid therapy. Psychoneuroendocrino. 2009;34(Suppl 1):S162–S168. doi:10.1016/j.psyneuen.2009.05.013
41. Bliesener N, Albrecht S, Schwager A, Weckbecker K, Lichtermann D, Klingmuller D. Plasma testosterone and sexual function in men receiving buprenorphine maintenance for opioid dependence. J Clin Endocrinol Metab. 2005;90:203–206. doi:10.1210/jc.2004-0929
42. Pergolizzi JV
43. Pacifico S, Ferrari F, Albanese V, et al. Biased agonism at nociceptin/orphanin FQ receptors: a structure activity study on N/OFQ (1-13)-NH2. J Med Chem. 2020;63(19):10782–10795. doi:10.1021/acs.jmedchem.9b02057
44. Bohn LM, Gainetdinov RR, Lin FT, Lefkowitz RJ, Caron MG. Mu-opioid receptor desensitization by beta-arrestin-2 determines morphine tolerance but not dependence. Nature. 2000;408(6813):720–723. doi:10.1038/35047086
45. Austin Zamarripa C, Edwards SR, Qureshi HN, Yi JN, Blough BE, Freeman KB. The G-protein biased mu-opioid agonist, TRV130, produces reinforcing and antinociceptive effects that are comparable to oxycodone in rats. Drug Alcohol Depend. 2018;192:158–162. doi:10.1016/j.drugalcdep.2018.08.002
46. Stein M, Herman D, Conti M, Anderson B, Bailey G. Initiating buprenorphine treatment for opioid use disorder during short-term in-patient ‘detoxification’: a randomized clinical trial. Addiction. 2020;115(1):82–94. doi:10.1111/add.14737
47. Likar R. Transdermal buprenorphine in the management of persistent pain - safety aspects. Ther Clin Risk Manag. 2006;2(1):115–125.
48. Simpson RW, Wlodarczyk JH. Transdermal buprenorphine relieves neuropathic pain: a randomized, double-blind, parallel-group, placebo-controlled trial in diabetic peripheral neuropathic pain. Diabetes Care. 2016;39(9):1493–1500. doi:10.2337/dc16-0123
49. Coull JA, Beggs S, Boudreau D, et al. BDNF from microglia causes the shift in neuronal anion gradient underlying neuropathic pain. Nature. 2005;438(7070):1017–1021. doi:10.1038/nature04223
50. Jacobsen JH, Watkins LR, Hutchinson MR. Discovery of a novel site of opioid action at the innate immune pattern-recognition receptor TLR4 and its role in addiction. Int Rev Neurobiol. 2014;118:129–163.
51. Hutchinson MR, Shavit Y, Grace PM, Rice KC, Maier SF, Watkins LR. Exploring the neuroimmunopharmacology of opioids: an integrative review of mechanisms of central immune signaling and their implications for opioid analgesia. Pharmacol Rev. 2011;63(3):772–810. doi:10.1124/pr.110.004135
52. Demartini L, Terranova G, Innamorato MA, et al. Comparison of tonic vs burst spinal cord stimulation during trial period. Neuromodulation. 2019;22(3):327–332. doi:10.1111/ner.12867
53. Isagulyan E, Slavin K, Konovalov N, et al. Spinal cord stimulation in chronic pain: technical advances. Korean J Pain. 2020;33(2):99–107. PMID: 32235010; PMCID: PMC7136296. doi:10.3344/kjp.2020.33.2.99.
54. Heijmans L, Joosten EA. Mechanisms and mode of action of spinal cord stimulation in chronic neuropathic pain. Postgrad Med. 2020;132(sup3):17–21. PMID: 32403963. doi:10.1080/00325481.2020.1769393
55. Özcan Ç, Polat Ö, Çelik H, Uçar BY. The effect of paravertebral ozone injection in the treatment of low back pain. Pain Pract. 2019;19(8):821–825. doi:10.1111/papr.12812.
56. Costa T, Linhares D, Ribeiro da Silva M, Neves N. Ozone therapy for low back pain. A systematic review. Acta Reumatol Port. 2018;43(3):172–181.
57. Infantino R, Mattia C, Locarini P, Pastore AL, Maione S, Luongo L. Buprenorphine: far beyond the “ceiling”. Biomolecules. 2021;11(6):816. doi:10.3390/biom11060816
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.