")
Back to Journals » International Journal of Women's Health » Volume 14
An Investigation of Depressive Symptoms in Patients with Congenital Cervical and Vaginal Aplasia: A Cross-Sectional Study
Authors Liu X, Ding J, Li Y, Hua K , Zhang X
Received 30 July 2022
Accepted for publication 4 November 2022
Published 17 November 2022 Volume 2022:14 Pages 1621—1627
DOI https://doi.org/10.2147/IJWH.S384339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Xiaotong Liu,* Jingxin Ding,* Yuqi Li, Keqin Hua, Xuyin Zhang
Department of Gynecology, Obstetrics and Gynecology, Hospital of Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuyin Zhang; Keqin Hua, Department of Gynecology, Obstetrics and Gynecology Hospital of Fudan University, 128 Shen yang Road, Shanghai, 200090, People’s Republic of China, Tel +86 17355381668 ; +86 19512268803, Email [email protected]; [email protected]
Purpose: Congenital cervical and vaginal aplasia is a rare condition that has a great impact on patients physically and psychologically. The present study was designed to assess depressive symptoms related to congenital cervical vaginal aplasia and provide a scientific basis for formulating psychological intervention measures.
Patients and Methods: This was a cross-sectional study of forty-six patients who were diagnosed with congenital cervical and vaginal aplasia and underwent cervicovaginal reconstruction surgery between January 2018 and December 2020. Patients were required to complete a demographic questionnaire, the Patient Health Questionnaire-9 (PHQ-9), the Generalized Anxiety Disorder-7 (GAD-7), and the Symptom Checklist-90 (SCL-90). When patients had sexual activity, their sexual function was evaluated by the Female Sexual Function Index (FSFI) questionnaire. The main outcome was the depressive symptoms screened by PHQ-9, and the factors affecting depressive symptoms were analyzed. Quantitative and categorical variables were compared using Student’s t-test and chi-squared test, respectively.
Results: Of all patients diagnosed with congenital cervical and vaginal aplasia, 58.7% (27/46) presented moderate to severe depressive symptoms. Some factors were related to the patient’s depressive symptoms, such as age, parental attitudes, family disharmony, being teased by peers, sexual dysfunction, fertility anxiety, and feeling uncomfortable while wearing the vaginal mold.
Conclusion: Half of patients with congenital cervical and vaginal aplasia have depressive symptoms. These findings stress that psychotherapy should be regarded as an independent treatment for patients with congenital cervical and vaginal aplasia.
Keywords: cervicovaginal reconstruction, depression, female genital tract malformation, psychotherapy, PHQ-9
Introduction
Müllerian agenesis has a reported incidence of 1 per every 4000–10,000 women. Among the affected patients, 2–7% have a normal functioning endometrial cavity in the uterus. So, congenital cervical and vaginal aplasia in the presence of a functioning uterus with endometrial cavity is an extremely rare Müllerian anomaly, which is associated with an obstructive phenomenon after menarche that leads to cyclic abdominal pain and pelvic masses.1 Most patients are diagnosed in adolescence, a sensitive age. This disease is frequently managed surgically.2 Hysterectomy can avoid re-obstruction. In recent years, advances in reconstructive techniques have allowed some patients to preserve fertility.3
Research on the relationship between psychology and disease has gradually increased, pointing out that a good psychological state plays a positive role in disease recovery.4,5 However, clinicians usually pay attention to patients’ physical symptoms and ignore the manifestations of psychological disorders, resulting in some patients suffering from psychological problems, which affects the effectiveness of treatment.
Congenital cervical and vaginal aplasia have a great impact on patients, including the periodic severe abdominal pain before the operation, the continuous placement of vaginal mold after the operation, and the difficulty in getting pregnant, which may cause depressive symptoms.6–8 As the location of this disease is private, patients may be shy to express it. After diagnosis, patients might feel anxiety about their female identity. Other congenital genital malformations, such as the psychological problems of MRKH patients, have been studied. Tsarna reported that MRKH patients were associated with a higher prevalence of anxiety and depression symptoms. Zhu reported that three-quarters of MRKH patients showed depressive symptoms, and one-third of these individuals were even at risk for depressive disorders. Therefore, depressive symptom screening in MRKH patients is of great importance.9,10 We believe that patients with congenital cervical and vaginal aplasia have more serious problems than those with MRKH, such as cyclic abdominal pain and endometriosis. If patients have depression and other psychological problems, it may affect the postoperative management. For example, patients may not be able to wear vaginal molds on time or take oral contraceptives on time to prevent the recurrence of endometriosis. Therefore, it is essential to understand the depressive symptoms of patients while treating cervical and vaginal aplasia to improve the treatment outcome. There was no study on the psychological states of patients with congenital cervical and vaginal aplasia until now. Hence, to fill this gap in the current literature, the present study was designed to assess depressive symptoms related to congenital cervical and vaginal aplasia, identify factors associated with depressive symptoms, and provide a scientific basis for psychotherapy.
Materials and Methods
Participants
Our cross-sectional study was conducted from March 1 to April 1, 2022, among patients who were diagnosed with congenital cervical and vaginal aplasia and underwent cervicovaginal reconstruction surgery between January 2018 and December 2020 at the Obstetrics and Gynecology Hospital of Fudan University. Inclusion criteria were: without psychiatric disorders, and voluntary participation.
Measurement
Demographic information gathered from patients and their families included: age, duration of cyclic abdominal pain before surgery, level of maternal and paternal education, family stress, family attitudes, and family harmony. They were also questioned as to whether they were being mocked or not, their state of sexual life, level of fertility anxiety, and whether they experienced discomfort while wearing the vaginal mold.
The depressive symptoms of the patients were evaluated by the Patient Health Questionnaire-9 (PHQ-9), which is a widely used tool for screening depressive symptoms with comparable sensitivity and specificity.11,12 This is a self-reported measure of depression consisting of nine items. Patients were asked to complete the items on a scale of 0 to 3. The score is divided into five categories: no (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20 or above). The test for depressive symptoms was based on a cut-off score of 10.11,13
In addition to assessing depression symptoms, other measures were also collected for further investigations: (1) Generalized Anxiety Disorder-7 (GAD-7) was used to assess the common anxiety symptoms of the participants, which has great reliability and validity.14,15 It is a seven-item self-administered questionnaire, each item on a scale of 0 to 3. The scores of 0–4, 5–9, 10–14, and 15–21 represent no, mild, moderate, and severe anxiety symptom levels, respectively.15 The sensitivity for diagnosing anxiety disorders (cut point 10 or above) was 89%, and the specificity was 82%.16 Therefore, a cut-off score of 10 or above was used to test for anxiety disorders. (2) The psychological health of the patients was assessed by the Symptom Checklist-90 (SCL-90).17 The SCL-90 has 90 items. Ten factors reflect the psychological symptoms in ten aspects, including somatization, obsessive-compulsive disorder, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, psychoticism, and additional items. The SCL-90 uses a 5-point scale from 1 (Not at All) to 5 (Extremely). The higher the score, the worse the psychological state. If the total score exceeds 160 points, the number of positive items (score two or above) exceeds 43, or any factor score is greater than two, these indicate that the psychological symptoms are positive.18 (3) When patients had sexual activity, the sexual function of the patients was evaluated by the Female Sexual Function Index (FSFI) questionnaire, which contains nineteen self-reported questions.19 The total score ranges from 2.0 to 36.0. The greater the score, the better the result. Based on investigation research of Chinese women, total scores less than 23.45 were defined as sexual dysfunction.20
Statistical Analysis
Statistical analysis was performed using SPSS version 25.0. All continuous data are expressed as mean ± standard deviation (SD). The Student’s t-test was used to compare differences between quantitative variables. The chi-squared test was used to evaluate the correlation between depressive symptoms and independent variables. P < 0.05 indicated significance for all tests.
Ethics Approval and Informed Consent
The questionnaire and methodology for this study were approved by the Institutional Review Board of the Obstetrics and Gynecology Hospital of Fudan University (Ethics approval number: 2022–47, 28th of February 2022). All methods in this study were carried out in accordance with the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study. Parent/legal guardian informed consent was obtained for the research participants under the age of 18 years.
Results
Participants’ General Characteristics
Forty-six patients with a mean age of 18.83 ± 2.91 years were enrolled in our study. The demographic characteristics of the patients are shown in Table 1. All patients experienced relief of abdominal pain and resumed menstruation. The duration of cyclic abdominal pain before surgery was 13.13 ± 5.48 months. Eight patients (17.39%) had severe family stress. Thirty-one patients (67.39%) had a harmonious family, and twenty-eight patients (60.87%) declared that their family showed love and care for them. Eleven patients (23.91%) admitted that they had been teased by peers about having long-term cyclic abdominal pain. Eighteen patients (39.13%) had a sexual partner. Eleven patients (23.91%), twenty-two patients (47.83%), and thirteen patients (28.26%) felt mild, moderate, and severe discomfort while wearing the vaginal mold, respectively. Half of them (47.83%) had moderate fertility anxiety, and fifteen (32.61%) had severe fertility anxiety.
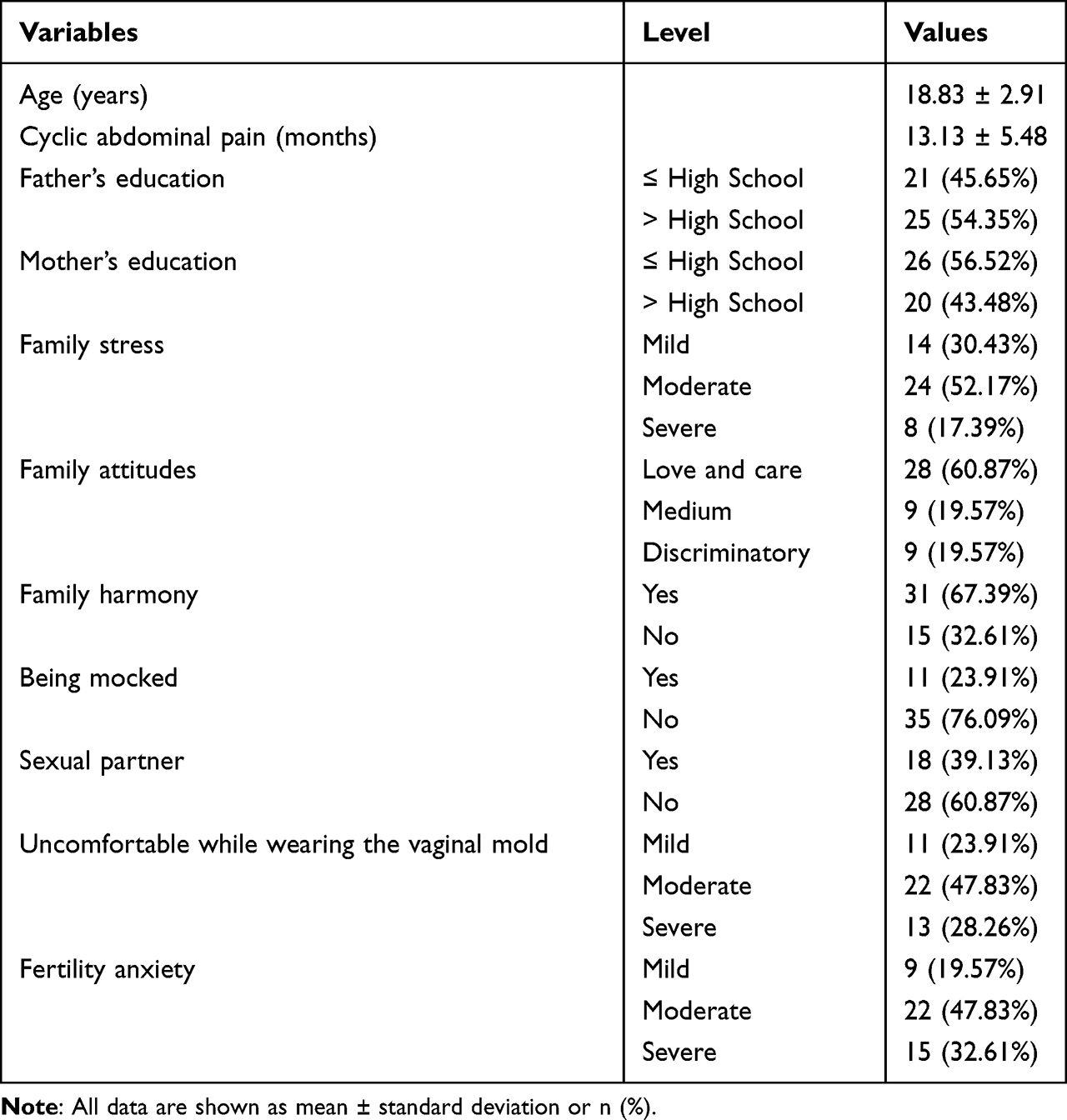 |
Table 1 Demographic Features of the Patients with Congenital Cervical and Vaginal Aplasia (N=46) |
Factors Associated with Depressive Symptoms
Among all patients, 28.26% (13/46) had no depressive symptoms, 13.04% (6/46) had mild symptoms, 28.26% (13/46) had moderate symptoms, 19.57% (9/46) had moderately severe symptoms, and 10.87% (5/46) had severe symptoms. Twenty-seven patients (58.7%) were assigned to the depression group based on their score of PHQ-9.
The results of the univariable analysis are listed in Table 2. The t-test results showed that the age of patients in the depression group was significantly higher (P < 0.001). The depression group tended to have longer cyclic abdominal pain (14.37 ± 5.14 vs 11.37 ± 5.61 months), but the difference was of no statistical significance. The chi-square statistics suggested that depressive symptoms were significantly associated with patients with low levels of maternal and paternal education (P < 0.05). In contrast to the non-depressive group, more patients in the depressive group had disharmonious families (P < 0.05), and their families discriminated against them (P < 0.05). Patients who had been teased by peers were more likely to have depressive symptoms (P < 0.05). Severe discomfort patients felt while wearing the vaginal mold tended to have a significant influence on psychological health (P < 0.05). Eight patients had sexual dysfunction, and all of them presented with depressive symptoms. The chi-square test showed that the depressive symptoms were significantly different among the varying degrees of fertility anxiety. Patients with severe fertility anxiety suffered from more depressive symptoms than patients with moderate and mild fertility anxiety (P < 0.05). Anxiety symptoms (measured by GAD-7) and bad psychological states (measured by SCL-90) were more prevalent in the depressive groups (P < 0.05).
 |
Table 2 Analysis of Variables Associated with Depressive Symptoms |
Discussion
Research on the relationship between psychology and diseases has gradually increased. It has been suggested that patients’ negative emotions are an important factor in the recovery of the disease.4 Congenital cervical and vaginal aplasia is a rare disease affecting the normal function of reproduction and the psychological states of patients. Many researchers have reported that depressive symptoms result in high suicide risk.21 Therefore, psychological intervention and guidance are also necessary. As far as we know, this study is the first to investigate patients with congenital cervical vaginal aplasia in terms of depressive symptoms.
It is difficult to implement diagnostic examinations for depressive symptoms for each patient in medical settings. Therefore, assessing depressive symptoms with a simple tool is of great importance. To assess depressive symptoms related to congenital cervical and vaginal aplasia and provide a scientific basis for psychotherapy, this study used the PHQ-9 to assess the depressive symptoms of patients and analyze the associated factors.
This study showed that half of the patients with congenital cervical and vaginal aplasia had depressive symptoms, 58.7% had anxiety symptoms, and 63.0% had psychological problems. Anxiety symptoms and worse psychological states were more prevalent in the depressive groups. It has been reported that depressive symptoms and anxiety symptoms commonly coexist, which is consistent with our findings.22 Therefore, coexisting anxiety symptoms and other psychological problems remind clinicians that it is important for patients with this disease to receive a thorough psychological assessment.
Since the diagnosis is generally made during adolescence, its psychological impact is significantly greater. In our study, the depressive group tended to have higher ages (20.15 ± 2.28 vs 16.95 ± 2.70 years, P < 0.001). Women aged 20 years begin to confront some pressures, such as having a sexual partner, marriage, and fertility, which are induced by the anomalies of the cervix and vagina. Hence, it is predictable that patients at this age are more prone to having depressive symptoms. This underscores that additional concern should be given to patients at this age.
Congenital cervical and vaginal aplasia is very rare and private. Due to the particularity of this disease, clinicians need to implement health education along with the treatment of this disease. For patients who need oral contraceptives after surgery, the preventive effect of these drugs on endometriosis should be reasonably explained.23 Thirteen patients (28.26%) admitted that they had severe discomfort while wearing the vaginal mold, so patients should be instructed to wear the vaginal mold correctly.24 Relaxation training and attention shifting can be used to reduce the discomfort of the mold wearing process, such as diaphragmatic breathing, listening to songs, and listening to water sounds.25–27 During the treatment process, medical staff should remain friendly and cordial to establish a harmonious doctor-patient relationship.28
The impact of this disease on families is substantial, and family support is the primary source of patient support, which is essential to cope with the emotional consequences.29 We found that greater family cohesion and harmony were positively associated with the psychological health of patients. In some areas with low education in China, traditional thought was strong, and other family numbers discriminated against patients because such patients were female and far from normal in the areas of menstruation and reproduction. Some families who preferred sons to daughters considered them freaks and even abandoned them. Our research also showed that some families discriminated against such patients, and those patients were more likely to have depressive symptoms. Therefore, in our diagnosis and treatment, psychologists, community workers, and gynecologists should care for patients with congenital cervical and vaginal aplasia, pay attention to their mental health, and teach their parents that menstruation and reproduction can recover after active treatment of this disease. Encourage the patients’ families to give more support and encouragement to the patients to enhance their confidence, this is also important in overcoming the disease.
The average cyclic abdominal pain of patients was 13.13 ± 5.48 months before surgery. Eleven patients (23.91%) admitted that they had been teased by peers about having long-term cyclic abdominal pain and could not study or play normally. Furthermore, patients who had been teased were more likely to have depressive symptoms. Therefore, we suggest that diagnosis and treatment be carried out as soon as possible to reduce the impact on the body and psychology of patients.
During the follow-up period, we found that fifteen patients had severe anxiety about fertility, eight patients had sexual dysfunction, and they all had depressive symptoms. It has been reported that there is a bidirectional association between emotional distress and sexual dysfunction and reproduction.30–32 This is consistent with our finding that patients with sexual dysfunction and fertility anxiety were more vulnerable to depressive symptoms. Providing these patients with fertility opportunities might help alleviate their depression. Patients with cervical and vaginal aplasia are more likely to have upper genital tract lesions, which may affect the possibility of natural conception to some extent, so assisted reproductive techniques can be suggested appropriately.8,33,34
One of the limiting factors is that congenital cervical and vaginal aplasia is a rare malformation, so the sample size was small. Another limitation is that the data in this study only reflected the current psychological states of the patients and could not reflect their long-term depressive symptoms. We recommend further prospective studies with large sample sizes to assess the depressive symptoms and identify factors associated with depressive symptoms in congenital cervical and vaginal aplasia.
Conclusions
In conclusion, this study suggests that half of patients with congenital cervical and vaginal aplasia present moderate to severe depressive symptoms. Parental attitudes, being teased by peers, sexual dysfunction, fertility anxiety, and feeling uncomfortable while wearing the vaginal mold were associated with depressive symptoms. These findings confirm the importance of depressive symptoms screening in these patients. To relieve patients from depressive symptoms, psychotherapy should be regarded as an independent treatment for patients with congenital cervical and vaginal aplasia.
Abbreviations
PHQ-9, Patient Health Questionnaire-9; GAD-7, Generalized Anxiety Disorder-7; SCL-90, Symptom Checklist-90; FSFI, Female Sexual Function Index.
Data Sharing Statement
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank the staff of the Obstetrics and Gynecology Hospital of Fudan University for their cooperation and support.
Funding
This study was supported by the National Key Research and Development Program of China (Grant No. 2021YFC2701400 and Grant No. 2021YFC2701402).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ludwin A, Pfeifer SM. Reproductive surgery for müllerian anomalies: a review of progress in the last decade. Fertil Steril. 2019;112(3):408–416. doi:10.1016/j.fertnstert.2019.07.005
2. Skinner B, Quint EH. Obstructive reproductive tract anomalies: a review of surgical management. J Minim Invasive Gynecol. 2017;24(6):901–908. doi:10.1016/j.jmig.2017.04.020
3. Mikos T, Gordts S, Grimbizis GF. Current knowledge about the management of congenital cervical malformations: a literature review. Fertil Steril. 2020;113(4):723–732. doi:10.1016/j.fertnstert.2020.02.006
4. Schakel L, Veldhuijzen DS, Crompvoets PI, et al. Effectiveness of stress-reducing interventions on the response to challenges to the immune system: a meta-analytic review. Psychother Psychosom. 2019;88(5):274–286. doi:10.1159/000501645
5. Vase L, Robinson ME, Verne NG, Price DD. Increased placebo analgesia over time in irritable bowel syndrome (IBS) patients is associated with desire and expectation but not endogenous opioid mechanisms. Pain. 2005;115(3):338–347. doi:10.1016/j.pain.2005.03.014
6. Zhang X, Qiu J, Ding Y, Sun L, Hua K. Single port laparoscopy combined with vaginal cervicovaginal reconstruction in a patient with congenital atresia of the cervix. Fertil Steril. 2020;113(3):681–682. doi:10.1016/j.fertnstert.2019.11.011
7. Carson SA, Kallen AN. Diagnosis and management of infertility: a review. JAMA. 2021;326(1):65–76. doi:10.1001/jama.2021.4788
8. Song X, Zhu L, Ding J, Xu T, Lang J. Clinical characteristics of congenital cervical atresia and associated endometriosis among 96 patients. Int J Gynaecol Obstet. 2016;134(3):252–255. doi:10.1016/j.ijgo.2016.02.015
9. Chen N, Song S, Duan Y, et al. Study on depressive symptoms in patients with Mayer-Rokitansky-Küster-Hauser syndrome: an analysis of 141 cases. Orphanet J Rare Dis. 2020;15(1):121. doi:10.1186/s13023-020-01405-9
10. Tsarna E, Eleftheriades A, Eleftheriades M, et al. The impact of Mayer-Rokitansky-Küster-Hauser Syndrome on psychology, quality of life, and sexual life of patients: a systematic review. Children. 2022;9(4):484. doi:10.3390/children9040484
11. Manea L, Gilbody S, McMillan D. A diagnostic meta-analysis of the Patient Health Questionnaire-9 (PHQ-9) algorithm scoring method as a screen for depression. Gen Hosp Psychiatry. 2015;37(1):67–75. doi:10.1016/j.genhosppsych.2014.09.009
12. Wang W, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiatry. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
13. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
14. Kroenke K, Spitzer RL, Williams JB, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007;146(5):317–325. doi:10.7326/0003-4819-146-5-200703060-00004
15. Löwe B, Decker O, Müller S, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008;46(3):266–274. doi:10.1097/MLR.0b013e318160d093
16. Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
17. Derogatis LR, Lipman RS, Covi L. SCL-90: an outpatient psychiatric rating scale--preliminary report. Psychopharmacol Bull. 1973;9(1):13–28.
18. Preti A, Carta MG, Petretto DR. Factor structure models of the SCL-90-R: replicability across community samples of adolescents. Psychiatry Res. 2019;272:491–498. doi:10.1016/j.psychres.2018.12.146
19. Rosen R, Brown C, Heiman J, et al. The Female Sexual Function Index (FSFI): a multidimensional self-report instrument for the assessment of female sexual function. J Sex Marital Ther. 2000;26(2):191–208. doi:10.1080/009262300278597
20. Ma J, Pan L, Lei Y, Zhang A, Kan Y. Prevalence of female sexual dysfunction in urban Chinese women based on cutoff scores of the Chinese version of the female sexual function index: a preliminary study. J Sex Med. 2014;11(4):909–919. doi:10.1111/jsm.12451
21. Wiebenga JX, Eikelenboom M, Heering HD, van Oppen P, Penninx BW. Suicide ideation versus suicide attempt: examining overlapping and differential determinants in a large cohort of patients with depression and/or anxiety. Aust N Z J Psychiatry. 2021;55(2):167–179. doi:10.1177/0004867420951256
22. Liu Q, Wangqing P, Baima Y, et al. Comorbid depressive and anxiety symptoms and their correlates among 93,078 multiethnic adults in Southwest China. Front Public Health. 2021;9:783687. doi:10.3389/fpubh.2021.783687
23. Becker CM, Bokor A, Heikinheimo O, et al.; Members of the Endometriosis Guideline Core Group. ESHRE Endometriosis Guideline Group. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022(2):hoac009. doi:10.1093/hropen/hoac009
24. Adeyemi-Fowode OA, Dietrich JE. Assessing the experience of vaginal dilator use and potential barriers to ongoing use among a focus group of women with Mayer-Rokitansky-Küster-Hauser syndrome. J Pediatr Adolesc Gynecol. 2017;30(4):491–494. doi:10.1016/j.jpag.2017.02.002
25. Shao S, Wang X, Lei X, Hua K, Zhang Y. Psychological intervention in women with Mayer-Rokitansky-Küster-Hauser syndrome after artificial vaginoplasty: a prospective study. Int Urogynecol J. 2022;33(3):723–729. doi:10.1007/s00192-022-05075-y
26. Linnemann A, Kappert MB, Fischer S, Doerr JM, Strahler J, Nater UM. The effects of music listening on pain and stress in the daily life of patients with fibromyalgia syndrome. Front Hum Neurosci. 2015;9:434. doi:10.3389/fnhum.2015.00434
27. Thoma MV, Mewes R, Nater UM. Preliminary evidence: the stress-reducing effect of listening to water sounds depends on somatic complaints: a randomized trial. Medicine. 2018;97(8):e9851. doi:10.1097/MD.0000000000009851
28. Singh M. Communication as a bridge to build a sound doctor-patient/parent relationship. Indian J Pediatr. 2016;83(1):33–37. doi:10.1007/s12098-015-1853-9
29. Shapiro J. Family reactions and coping strategies in response to the physically ill or handicapped child: a review. Soc Sci Med. 1983;17(14):913–931. doi:10.1016/0277-9536(83)90218-6
30. Holt R, Slade P. Living with an incomplete vagina and womb: an interpretative phenomenological analysis of the experience of vaginal agenesis. Psychol Health Med. 2003;8:19–33. doi:10.1080/1354850021000059232
31. Atlantis E, Sullivan T. Bidirectional association between depression and sexual dysfunction: a systematic review and meta-analysis. J Sex Med. 2012;9(6):1497–1507. doi:10.1111/j.1743-6109.2012.02709.x
32. Omani-Samani R, Ghaheri A, Navid B, Sepidarkish M, Maroufizadeh S. Prevalence of generalized anxiety disorder and its related factors among infertile patients in Iran: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1):129. doi:10.1186/s12955-018-0956-1
33. Shen F, Zhang XY, Yin CY, Ding JX, Hua KQ. Comparison of small intestinal submucosa graft with split-thickness skin graft for cervicovaginal reconstruction of congenital vaginal and cervical aplasia. Hum Reprod. 2016;31(11):2499–2505. doi:10.1093/humrep/dew230
34. Mikos T, Lantzanaki M, Anthoulakis C, Grimbizis GF. Functional and reproductive outcomes following surgical management of congenital anomalies of the cervix: a systematic review. J Minim Invasive Gynecol. 2021;28(8):1452–1461.e16. doi:10.1016/j.jmig.2020.10.030
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.