")
Back to Journals » Journal of Pain Research » Volume 15
An International Survey on the Practice of Lumbar Radiofrequency Ablation for Management of Zygapophyseal (Facet)-Mediated Low Back Pain
Authors Abd-Elsayed A, Azeem N , Chopra P, D'Souza RS , Sayed D , Deer T
Received 17 December 2021
Accepted for publication 6 April 2022
Published 14 April 2022 Volume 2022:15 Pages 1083—1090
DOI https://doi.org/10.2147/JPR.S354506
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Krishnan Chakravarthy
Alaa Abd-Elsayed,1 Nomen Azeem,2 Pooja Chopra,3 Ryan S D’Souza,4 Dawood Sayed,5 Timothy Deer6
1Department of Anesthesiology, University of Wisconsin, Madison, WI, USA; 2Florida Spine & Pain Specialists, Tampa, FL, USA; 3Bux Pain Management, Danville, KY, USA; 4Department of Anesthesiology and Perioperative Medicine, Mayo Clinic Hospital, Rochester, MN, USA; 5Department of Pain Medicine, University of Kansas Medical Center, Kansas City, KS, USA; 6The Spine and Nerve Centers, Charleston, WV, USA
Correspondence: Alaa Abd-Elsayed, Department of Anesthesiology University of Wisconsin Madison, WI, USA, Email [email protected]
Objective: The objective of this study was to survey current clinical practice related to lumbar radiofrequency (RFA) for the treatment of zygapophyseal (facet)-mediated low back pain.
Methods: Survey questions regarding the clinical practice of lumbar RFA were created and piloted by the American Society of Pain and Neuroscience (ASPN) leadership. After revision for clarity, health-care professionals worldwide who hold membership status within the ASPN Society and who offer lumbar RFA in their clinical practice were recruited to participate in this online survey. All responses were tabulated and summarized descriptively.
Results: A total of 329 participants responded in the survey. Most participants specialized in anesthesiology (68.4%) and physical medicine and rehabilitation (21.8%) and had been practicing pain management for more than five years (70.5%). Of physician respondents, 27.5% did not complete an Accreditation Council for Graduate Medical Education (ACGME)-accredited pain medicine fellowship and 16.5% were not board-certified in pain medicine. The majority of providers (69.7%) reported that they perform two diagnostic medial branch blocks prior to proceeding with lumbar RFA. Bupivacaine 0.5% was the most common medication utilized for both the first (37.4%) and second (37.1%) diagnostic blocks. There were 32.6% of total respondents who reported not utilizing contrast dye when performing diagnostic blocks. The vast majority of providers (91.4%) reported using conventional RFA for lumbar medial branch neurotomy.
Conclusion: This survey study provides a summary of the application of lumbar RFA for the treatment of axial low back pain in the real-world setting. We highlight a significant portion of providers who perform lumbar RFA yet do not have pain fellowship training at an ACGME-accredited institution or do not maintain current pain medicine board certification. We also report deviations from standard practice, specifically the type of local anesthetic used for comparative diagnostic blocks and the omission of contrast injection during diagnostic blocks.
Keywords: radiofrequency ablation, low back pain, medial branch block, survey, clinical practice
Introduction
Chronic low back pain is the leading cause of disability in the United States.1 Approximately 15–45% of chronic low back pain is due to facet joint arthropathy.2 Facet-mediated pain is typically related to osteoarthritis with nociception originating in the synovial membrane, hyaline cartilage, bone, or fibrous capsule of the facet joint.3,4 Due to the anatomic considerations and the overall size of the facet joints, there are minimally invasive and effective long-term treatment options for lumbar facet-mediated low back pain. Nociceptive sensation in the facet joints is carried by afferent fibers in the medial branch nerves of the lumbar dorsal rami (MBN). Thus, lesioning of the MBN by radiofrequency ablation (RFA) is commonly used as a treatment for facet-mediated low back pain.5
The use of RFA for the treatment of chronic pain was first described in 1931 when Kirschner described treatment of trigeminal neuralgia through radiofrequency to the gasserian ganglion.6 The first described application of RFA for lumbar spine facetogenic pain occurred in 1975 by Shealy.6 This led to a number of other physicians describing the use of RFA for the treatment of low back pain between 1976 and 1980.7–10 Over the 1990s and into the 2000s the RFA techniques were refined. Today, in many centers around the world, RFA is a very common long-term treatment of axial, mechanical, and facet-mediated low back pain.11 Furthermore, with advancements in technology, there are several modalities of RFA including traditional RFA, cooled RFA, pulsed RFA, and bipolar RFA, all of which have unique characteristics with advantages and disadvantages.5,12,13
Despite the significant accumulation of evidence highlighting the efficacy of RFA for treatment of low back pain and the significant evolution of multiple modalities of RFA in clinical practice, there has been limited efforts to assess clinical practice variations in the United States and worldwide. The purpose of this clinical survey is to evaluate provider-related factors, procedural-related factors, and variation in clinical practice among pain provides worldwide that utilize lumbar RFA for treatment of chronic low back pain.
Methods
This survey study was approved by the University of Wisconsin Institutional Review Board. Firstly, a structured survey was designed to obtain information on practices related to lumbar RFA for treatment of low back pain. Specific questionnaire items are presented in Supplemental Table 1. The survey was first piloted among various executive members of the American Society of Pain and Neuroscience (ASPN) and was revised to enhance clarity. After approval by executive members, the survey was then distributed to all members who are part of the ASPN Society.
Participants were informed about the purpose of the survey. While each participant was not required to provide signed consent by the institutional review board, completion of the survey was an indication of willingness to participate and implied consent. The authors did not set a threshold over the short study period but were anticipating around 200 completed surveys to be considered a robust and representative assessment of pain physicians from one national society.
The surveys were distributed via an e-mail link to members’ registered e-mail address. Instructions were also included in the survey requesting responses from only providers who offered lumbar RFA to patients for treatment of low back pain. If the survey was not completed within two weeks, the co-authors provided a reminder e-mail. The survey questions were multiple-choice items and appeared consecutively on the webpage. The item choices were categorical in nature. The survey responses were tabulated and descriptive statistics were performed to summarize results, specifically with total number and percentages for categorical outcomes.
Results
The survey was distributed to all members of the ASPN Society (4,594 members) and a total of 329 providers who offer lumbar RFA responded. Of these providers who responded to the survey, 252 (76.6%) of providers identified as male, 73 (22.2%) identified as female, and 4 responders (1.2%) preferred not to specify their gender. While the survey respondents consisted of a wide range of provider types, including attending physicians, physicians in training, nurse practitioners, and physician assistants, the majority were attending physicians, comprising 92% of respondents (Table 1). Of the physicians who responded, their primary specialities consisted primarily of anesthesiology, followed by physical medicine and rehabilitation, neurology, psychiatry, and others such as neurosurgery. Two-hundred-fifty-five respondents (77.5%) reported greater than 80% of their practice is dedicated to pain medicine. Furthermore, 253 providers (77%) stated that they were board certified in pain medicine and 221 physicians (67.6%) graduated from an ACGME accredited pain fellowship program (Table 1). The majority (121 responders) ranged from being 31 to 40 years of age. There were 67 providers ranging from ages 51 to 60 (20.4%), 42 ranging from ages 61 to 70 (12.8%), 6 ranging under 30 years of age (1.8%), and 5 ranging from ages 71 to 80 (1.5%). Of these survey participants, 273 (83.0%) resided in the United States while 56 (17.0%) resided from other countries (Supplemental Table 2).
 |
Table 1 Provider-Related Survey Items |
Regarding procedural-related factors, a total of 317 physicians (96.3%) reported that they performed this procedure. Two-hundred-twenty-eight providers (69.7%) stated that they performed two diagnostic medial branch blocks prior to proceeding with lumbar RFA. While bupivacaine 0.5% was the most common medication utilized for the first and second diagnostic blocks, there were other medication formulations that were also commonly utilized as outlined in Table 2. One-hundred-eighty-four respondents (56.6%) reported that they use contrast dye during diagnostic blocks, whereas 106 providers (32.6%) reportedly do not utilize contrast dye when performing these diagnostic blocks.
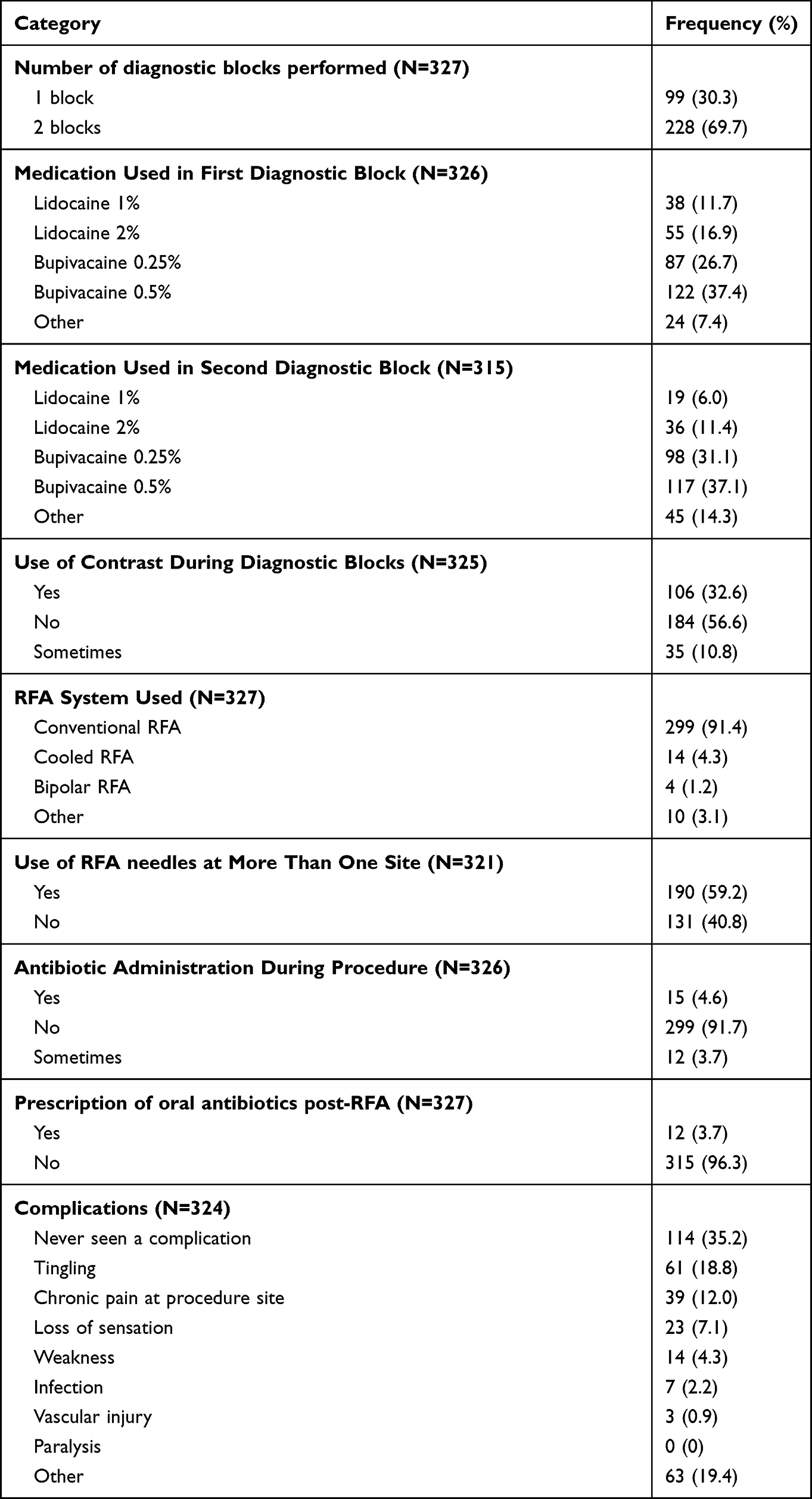 |
Table 2 Procedural-Related Survey Items |
The vast majority of providers (299 respondents, 91.4%) reported using conventional RFA as opposed to other systems such as cooled RFA, or pulsed RFA, or bipolar RFA for lumbar medial branch neurotomy. One-hundred-ninety respondents (59.1%) stated that they used their RFA needles at more than one site. When specifically asked about antibiotic administration with these procedures, the majority of respondents do not provide antibiotics after performing either blocks or RFA (Table 2). In regards to complications, 35.2% of respondents stated that they have not seen any complications associated with diagnostic blocks or RFA, but of the complications, tingling (18.8%) and chronic procedural site pain (12.0%) was the most prevalent.
Discussion
In this survey study evaluating practice patterns of 329 pain providers, we provide a “snapshot” of how the application of RFA for the treatment of axial low back pain is utilized and practiced in the real-world setting. We highlight that a high proportion of non-pain-fellowship trained and non-pain board-certified providers offered RFA; a high proportion of male respondents were represented; there is highly variable practice of type of local anesthetic injectate used for diagnostic medial branch blocks; that the majority of clinicians performed two separate diagnostic medial branch blocks; and that the majority of respondents deviated from recommended practice of including contrast injection during diagnostic blocks.
Data on real-world practices may prove useful to the novice clinician or trainee who has recently been trained in performing RFA for low back pain and would like to further advance learning based on the practice patterns of other clinicians. Conversely, even to the experienced and seasoned clinician, this study may inform what the current overall practice patterns are like in the field of pain medicine and may inspire new changes to their current practice. From a research perspective, this may also motivate future research efforts to investigate the association between positive analgesic outcomes and variable factors such as provider-related variables (eg, current board certification in pain medicine, full-time equivalents contributed to pain medicine job, etc.), number of diagnostic blocks, type of RFA, utilization of contrast during diagnostic blocks, and many other variables.2
The survey provided insight on several provider-related factors. There was a large proportion of providers who did not complete an ACGME-accredited pain medicine fellowship (27.52%) and did not obtain board certification in pain medicine (16.46%). This is concerning because this may highlight that providers, who may have not received the appropriate training or may not have the necessary qualifications, are offering this procedure to patients. Without adherence to maintenance of certification standards, it is also possible that these providers may not adhere to the standard of care when offering RFA for treatment of pain. State medical boards should enforce stricter surveillance of non-board certified physicians offering specialized procedures to monitor for safe practice and appropriate adherence to guidelines. However, the authors do acknowledge that certain specialties such as interventional radiology may be well-qualified to offer fluoroscopic-guided spinal injections, although there were no providers from interventional radiology represented in this survey. In this survey, providers from anesthesiology (68.40%), physical medicine and rehabilitation (21.78%), and neurology (2.15%) comprised most of the respondents. There was also a preponderance of male respondents in the survey, which is expected as there are several prior studies highlighting that male health-care providers and male leaders tend to comprise the vast majority in the pain medicine field.14–16
Selection of patients for RFA is important. The majority of providers (69.72%) offered two diagnostic trial blocks prior to RFA. It is well known that diagnostic medial branch blocks are associated with a high false-positive rate.17 Thus, the conservative approach would be to offer dual diagnostic medial branch blocks which are associated with a higher subsequent success rate for RFA.17 This may also be a requirement for many insurance companies. However, per the consensus practice guidelines by a multispecialty and international working group, the committee recommended a single diagnostic trial block. Prior guidelines by the Spine Intervention Society18 and the American Society of Interventional Pain Physicians19 have advocated for two diagnostic nerve blocks before proceeding with RFA. The rationale for performing dual blinded comparative local anesthetic blocks (two local anesthetics with different duration of action on two separate occasions) is to reduce the placebo effect. However, other factors may also account for false-positive blocks such as leakage of injectate to other adjacent pain-generating areas (eg, epidural space, myofascial pain), use of significant superficial local anesthetic infiltration, administration of sedative or other analgesic agents, and patients not performing normal activities after the injection.17
Another important variable that impacts patient selection is the type of local anesthetic used for diagnostic medial branch blocks. Most respondents used 0.25% of 0.5% bupivacaine for both the first and second diagnostic medial branch blocks. This would suggest provider preference for a longer-acting local anesthetic (bupivacaine) that provides analgesia for an additional few hours compared to lidocaine injection. However, there may be improved diagnostic utility by offering double comparative diagnostic blocks that involve two separate blocks with lidocaine and bupivacaine.17
The majority of respondents also indicated preference for various practices that may have implications for procedural efficiency and cost savings. For instance, 56.62% of providers reported that they do not use contrast when performing diagnostic medial branch blocks and 10.77% only use contrast sometimes. While this may be associated with lower cost and decreased procedural duration, it is not consistent with standard practice and current guidelines. Injection of a small amount of contrast (0.1–0.3 mL) helps to exclude vascular uptake and decreases the chance of injection into inappropriate locations (eg, neuraxial space).20 Per guidelines from the American Society of Regional Anesthesia and Pain Medicine and the Spine Intervention Society, it is recommended to check for intravascular needle placement by aspiration and visualization of contrast spread in real-time fluoroscopy in order to detect intravascular update and ensure adequacy of injectate spread.17 It is likely that proceduralists who do not utilize contrast to limit vascular spread are instead performing needle aspiration to check for intravascular placement. However, studies have demonstrated that while aspirating for blood prior to injection has a high specificity for intravascular needle placement (95% confidence interval: 95.6–98.4%), this technique carries a low sensitivity (95% confidence interval: 29.2–53.7%) which makes it a poor screening tool.21
While conclusions can be drawn from this survey regarding current variation in practice in RFA for low back pain, these results cannot be generalized because of the limitations noted in methodology. Firstly, selection bias is introduced as respondents were invited and chosen only if they were members of the American Society of Pain and Neuroscience (ASPN) and if they were willing to answer internet-based survey questions. A comparison of survey responses with members from other societies (eg, Spine Intervention Society, American Society of Interventional Pain Physicians, American Academy of Pain Medicine) would be of interest and provide information if members from different societies practice differently. This would also be an important indication of the quality of training within a society as certain societies place emphasis and value on evidence-based training. Societies may consider implementing educational initiatives and workshops to educate clinicians about not adhering to guidelines. For instance, as identified in our survey, a high number of proceduralists do not employ contrast injection to assess for vascular uptake during diagnostic medial branch blocks. Societies should emphasize that vascular penetration and injury are possible, with studies citing between 3.7% to upward of 20% incidence of intravascular positioning.17 Educational initiatives should emphasize that vascular penetration is likely to result in a false-negative diagnostic nerve block due to washout of the local anesthetic during medial branch block. A false-negative diagnostic nerve block would prevent the patient from obtaining a radiofrequency ablation, and thus the patient may subsequently be exposed to other invasive interventional procedures that are not targeting facet-mediated pain.
The online survey did not abstract information on non-responders, which would be helpful to know in terms of overall cohort representation. Of the 4,594 members who were invited to complete the survey, a total of 329 providers (7.2%) responded which introduces significant selection bias. Geographical and cultural bias may also affect interpretation of study findings. For instance, while the majority of respondents practiced in the United States (83.0%), about 17.0% of respondents were from other countries (Supplemental Table 2).
Despite these limitations, the survey provides a comprehensive summary of practices that relate to the experience of over 300 providers and serves as a baseline that future studies can compare over time. While the study largely represents providers in the United States, many respondents were also from Europe, South America, and other regions. Future studies should survey a more representative international database that captures worldwide variations in practice. Future studies should also assess the role of demographic and geographical parameters on practice preferences. Finally, reasons for deviating from standard practice such as with omission of contrast injection during diagnostic blocks should be investigated.
Conclusion
This survey study reports practice patterns of RFA for the treatment of axial low back pain among 329 providers. Major findings include that a high proportion of providers who offer lumbar RFA did not undergo pain fellowship training and are not currently board-certified in pain medicine, and there are deviations from standard practice with respect to type of local anesthetic medication and use of contrast during diagnostic blocks.
Funding
There is no funding to report.
Disclosure
A.A. is a consultant of Medtronic and Avanos. T.D. is a consultant to Abbott, Axonics, Flowonix, Saluda Medical, Vertos, SpineThera, Nalu, Medtronic, Nevro, SI Bone, Stimgenics, SPR Therapeutics, Cornerloc, Boston Scientific, and Vertiflex; received research support from Abbott, Vertos, Mainstay Medical, Saluda, SPR Therapeutics, Boston Scientific, and Vertiflex; advisory board for Abbott, Vertos, Flowonix, Nalu, SPR Therapeutics, and Vertiflex; holds equity in Bioness, Vertiflex, Axonic, Vertos, SpineThera, Saluda Medical, Nalu, Cornerloc, and SPR Therapeutics; and patent pending with Abbott. D.S. is a consultant to Abbott, Boston Scientific, Flowonix, Medtronic, Nevro, PainTEQ, SPR Therapeutics, Vertos, and Vertiflex. PC is a speaker for Flowonix. The authors report no other conflicts of interest in this work.
References
1. Mafi JN, McCarthy EP, Davis RB, Landon BE. Worsening trends in the management and treatment of back pain. JAMA Intern Med. 2013;173(17):1573–1581. doi:10.1001/jamainternmed.2013.8992
2. Yadav A, Hagedorn JM, D’Souza RS, Engle AM, Deer TR. Effect of patient characteristics on reported outcomes over 12 months following lumbar radiofrequency ablation: a retrospective review of 500 patients. Pain Pract. 2021;21(2):152–159. doi:10.1111/papr.12938
3. Van Kleef M, Vanelderen P, Cohen SP, Lataster A, Van Zundert J, Mekhail N. Pain originating from the lumbar facet joints. Pain Pract. 2010;10(5):459–469. doi:10.1111/j.1533-2500.2010.00393.x
4. Cohen SP, Raja SN. Pathogenesis, diagnosis, and treatment of lumbar zygapophysial (facet) joint pain. Anesthesiology. 2007;106(3):591–614. doi:10.1097/00000542-200703000-00024
5. ZL M, Marshall B, Walker J, McCarthy R, DR W. Long-term function, pain and medication use outcomes of radiofrequency ablation for lumbar facet syndrome. Int J Anesth Anesth. 2015;2(2). doi:10.23937/2377-4630/2/2/1028
6. Shealy CN. Percutaneous radiofrequency denervation of spinal facets. Treatment for chronic back pain and sciatica. J Neurosurg. 1975;43(4):448–451. doi:10.3171/jns.1975.43.4.0448
7. Pawl RP. Results in the treatment of low back syndrome from sensory neurolysis of the lumbar facets (facet rhizotomy) by thermal coagulation. Proc Inst Med Chic. 1974;30(4):151–152.
8. Banerjee T, Pittman HH. Facet rhizotomy. Another armamentarium for treatment of low backache. N C Med J. 1976;37(7):354–360.
9. Flórez G, Eiras J, Ucar S. Percutaneous rhizotomy of the articular nerve of Luschka for low back and sciatic pain. Acta Neurochir. 1977;Suppl 24(67–71). doi:10.1007/978-3-7091-8482-0_11
10. Schaerer JP. Radiofrequency facet rhizotomy in the treatment of chronic neck and low back pain. Int Surg. 1978;63(6):53–59.
11. Starr JB, Gold L, McCormick Z, Suri P, Friedly J. Trends in lumbar radiofrequency ablation utilization from 2007 to 2016. Spine J. 2019;19(6):1019–1028. doi:10.1016/j.spinee.2019.01.001
12. Leggett LE, Soril LJ, Lorenzetti DL, et al. Radiofrequency ablation for chronic low back pain: a systematic review of randomized controlled trials. Pain Res Manag. 2014;19(5):e146–e153. doi:10.1155/2014/834369
13. Byrd D, Mackey S. Pulsed radiofrequency for chronic pain. Curr Pain Headache Rep. 2008;12(1):37–41. doi:10.1007/s11916-008-0008-3
14. D’Souza RS, Langford B, Moeschler S. Gender representation in fellowship program director positions in ACGME-accredited chronic pain and acute pain fellowship programs. Pain Med. 2021;22:1360–1366. doi:10.1093/pm/pnab041
15. D’Souza R, Langford B, D’Souza S, Rose S, Long T. Characteristics of designated institutional officials and sponsoring institutions of ACGME-accredited training programs. J Grad Med Educ. 2020;13:70–75. doi:10.4300/JGME-D-20-00313.1
16. D’Souza R, King R, Strand N, Barman R, Olatoye O. Sex Disparity Persists in Pain Medicine: A Cross-Sectional Study of Chairpersons Within ACGME-Accredited Chronic Pain Fellowship Programs in the United States. J Educ Perioper Med. 2022;XXIV(1):1-9. Available from https://www.seahq.org/assets/docs/JEPM/volxxiv/VolXXIV_Issue1_D%27Souza.pdf. Accessed April 12, 2022.
17. Cohen SP, Bhaskar A, Bhatia A, et al. Consensus practice guidelines on interventions for lumbar facet joint pain from a multispecialty, international working group. Reg Anesth Pain Med. 2020;45(6):424–467. doi:10.1136/rapm-2019-101243
18. Falco FJ, Manchikanti L, Datta S, et al. An update of the systematic assessment of the diagnostic accuracy of lumbar facet joint nerve blocks. Pain Physician. 2012;15(6):E869–E907. doi:10.36076/ppj.2012/15/E869
19. Bogduk N. International Spine Intervention Society. Lumbar Medial Branch Blocks.
20. Johnson BA, Schellhas KP, Pollei SR. Epidurography and therapeutic epidural injections: technical considerations and experience with 5334 cases. AJNR Am J Neuroradiol. 1999;20(4):697–705.
21. Joo Y, Kim YC, Lee SC, et al. Impact of type of needle on incidence of intravascular injection during diagnostic lumbar medial branch block. Reg Anesth Pain Med. 2016;41(3):392–397. doi:10.1097/AAP.0000000000000381
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.