Back to Journals » Psychology Research and Behavior Management » Volume 17
An Exploration of Depression and Aggression Among Patients with Schizophrenia in China Rural Community
Authors Zhang S, Ouyang X, Yang K, Shen Y, Zheng S, Wang R ![]() , Sheng X, Ge M, Yang M, Zhou X
, Sheng X, Ge M, Yang M, Zhou X ![]()
Received 11 December 2023
Accepted for publication 21 March 2024
Published 20 April 2024 Volume 2024:17 Pages 1717—1726
DOI https://doi.org/10.2147/PRBM.S453891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Shaofei Zhang,1– 3,* Xu Ouyang,1– 3,* Kefei Yang,2,3,* Yunyun Shen,2,3 Siyuan Zheng,1– 3 Ruoqi Wang,1– 3 Xuanlian Sheng,1– 3 Menglin Ge,1– 3 Meng Yang,1– 3 Xiaoqin Zhou1,2
1School of Mental Health and Psychological Sciences, Anhui Medical University, Hefei City, People’s Republic of China; 2Second Affiliated Hospital of Anhui Medical University, Hefei City, People’s Republic of China; 3Chaohu Hospital of Anhui Medical University, Hefei City, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaoqin Zhou, Second Affiliated Hospital of Anhui Medical University, Hefei City, People’s Republic of China, Tel +8613865913378, Email [email protected]
Purpose: In schizophrenia, aggressive conduct is frequent. And depressed mood can also contribute to the occurrence of aggressive behaviors. The aim of this study was to investigate the risk factors for the occurrence of aggression in stable schizophrenia patients in rural China, mainly to investigate the role of depressed mood in the occurrence of aggression in schizophrenia patients.
Patients and Methods: This is a cross-sectional study conducted in the townships surrounding Chaohu City, Anhui Province, China. Patients’ depressive mood was evaluated using the PHQ-9 (The 9-item Patient Health Questionnaire). Patients’ aggressiveness was evaluated using the Modified Overt Aggression Scale (MOAS). A score of ≥ 4 was used as a threshold and divided into aggressive and non-aggressive groups.
Results: This study comprised a total of 821 schizophrenia patients. Among them, the prevalence of having aggressive behavior was 18.8%. After correcting for confounders, logistic regression analysis showed that low education level (OR=0.470, 95% CI 0.254– 0.870; p=0.016), living with family (OR=0.383, 95% CI 0.174– 0.845; p=0.017) depressed mood (OR=1.147, 95% CI 1.112– 1.184; p< 0.001) was significantly associated with the risk of aggressive behavior in patients with schizophrenia. Multivariate linear regression indicated that higher levels of aggression were linked with lower levels of education and higher depressive mood.
Conclusion: This study suggests that aggression is more common in patients with stable schizophrenia, and lower levels of education and higher levels of depression are associated risk factors for its occurrence. Living alone may be helpful in reducing the likelihood of aggression.
Keywords: schizophrenia depression aggression Chinese
Introduction
With a slightly less than 1% lifetime prevalence, schizophrenia is a chronic and complicated mental condition with a heterogeneous genetic and neurobiological foundation that impacts the early stages of brain development.1 However, the incidence varies by region, with the number of schizophrenics in China being higher in rural than in cities.2 According to a recent study, rural China had a 0.37% prevalence of schizophrenia in 1990, 0.43% in 2000, and 0.50% in 2010.3 Moreover, patients living in rural areas have lower treatment compliance than urban patients, which makes the psychiatric symptoms of rural patients more significant as well4.
On the other hand, schizophrenic symptoms are diverse, and among the many symptoms, some patients present with aggressive behavior, which can manifest as agitation, impaired impulse control, and decreased social sensitivity. A recent meta-analysis involving 15 studies with 4855 patients showed that the prevalence of schizophrenia combined with aggressive behavior was about 33.3%.5 The prevalence of violent conduct among hospitalized patients ranged from 15.3% to 53.2%, according to another meta-analysis that included 19 studies and 3941 patients.6 Schizophrenia individuals with aggressive behaviors exhibit both physical and verbal violence, and these behaviors not only have an impact on the treatment of their illness, but their family members may also be subjected to varying degrees of aggression. A survey of patients’ family members showed that about 77.4% of relatives suffered from varying degrees of verbal and physical aggression, and about the average respondent reported potentially significant levels of PTSD.7 In order to enable early intervention, the study of factors influencing the propensity for violence in schizophrenia patients can offer a clinical basis for anticipating aggression. Currently, several studies addressing factors influencing aggression in schizophrenia patients have found that the occurrence of aggression is mostly associated with substance use8, previous history of violence9, early age of onset, male, poor economic status10, presence of physical illness and severe positive symptoms11 involuntary hospitalization12 etc.
People with schizophrenia often have depressive symptoms, which can appear at nearly any stage of the disease13. Additionally, there is a link between depressive symptoms and aggressive conduct, with one study demonstrating that depressive symptoms can predict violent behavior in teenagers14 Another investigation into adolescent offenders revealed that those who experienced depressed symptoms also displayed higher levels of violence.15 Adults with major depressive disorder are estimated to have a prevalence of 58.7% of any aggressive outbursts, and depressed symptoms have a positive correlation with aggression.16,17 Aggression, however, has also been demonstrated to be connected with characteristics other than depressive symptoms rather than depression per se18,19.
The majority of recent research on violence in schizophrenia patients has only examined inpatients and disregarded patients treated at home. Additionally, research on the connection between violent conduct and negative mood in schizophrenia patients is scarce. In order to ease the clinical application of early intervention, we comprehensively investigate in this work how violent behavior of schizophrenia patients treated at home is influenced by depressed mood.
Materials and Method
Participants
This is a cross-sectional study conducted around Chaohu City, Anhui Province, China from September to October 2022. The study population consisted of patients with severe mental disorders in the surrounding townships of Chaohu City, Anhui Province. Chinese Han patients who met the following criteria were recruited for this study: (1) Met the DSM-5 diagnostic criteria for schizophrenia. (2) Aged between 18 and 75 years old. (3) Less than 50% change in dose of any major psychotropic medication in the past three months. Exclude patients based on the following criteria: (1) Have other neurological or psychiatric disorders. (2) Age <18 years or >75 years. (3) Pregnancy or lactation. (4) History of psychoactive substance abuse.
Through a self-designed questionnaire, personal information including age, gender, BMI, education level, and marital status was gathered. Total duration of illness, age at onset, physical co-morbidities, and depression scores of patients with schizophrenia were collected through clinical interviews. This cross-sectional study enrolled 1205 individuals with schizophrenia, of whom 821 cases met the inclusion criteria. This investigation was approved by the Ethics Committee of Chaohu Hospital of Anhui Medical University(KYXM-202212-013). All patients signed an informed consent form before the survey to ensure that their privacy would not be disclosed.
Measures
Moas
We used the Modified Overt Aggression Scale (MOAS) to assess aggression. The scale contains four subscales: verbal aggression, property aggression, self-aggression, and aggression toward others. Each individual’s score on each subscale ranged from 0 (no aggression) to 4 (highest score), based on the descriptions of the patient and his or her family. The subscale scores were also weighted to calculate the total MOAS score: verbal aggression score multiplied by 1; aggressive property score multiplied by 2; self-aggression score multiplied by 3; and aggression toward others score multiplied by 4. The sum of these weighted scores was the total MOAS score.20 Based on the MOAS total score, patients were divided into two groups: a total score ≥4 for the aggression group and a total score <4 for the non-aggression group.
Phq-9
Patients’ depressed mood was assessed using the 9-item Patient Health Questionnaire (PHQ-9), which includes nine questions diminished interest, depressed mood, feelings of fatigue, eating disorders, difficulty concentrating, feelings of low self-esteem, excessive or lackluster behavior, sleep disturbances, and suicidal ideation. Responses range from 0 (not at all) to 3 (almost every day) and from 0 to 27, with higher scores indicating higher depressed mood. Studies have shown that the internal consistency and test retest reliability of the PHQ-9 is excellent21.
Statistical Analysis
The Kolmogorov–Smirnov test was utilized to determine whether the data distribution was normal. Normal continuous data are described by mean ± standard deviation (SD) and were tested using the t-test. The Mann–Whitney U-test was used to evaluate non-normal continuous data, and the median (interquartile spacing) was used to describe the data. Categorical variables were described by numbers and percentages and analyzed using the χ2 test. Analysis of risk factors influencing aggressive behavior in schizophrenia patients using binary logistic regression was conducted. The correlation between the sample’s characteristics and its aggression ratings was evaluated using Spearman correlation analysis or the U-test. After adjustment for confounders, Variables that might be connected to aggressive behavior were found using multiple linear regression analysis. Statistical tests were two-sided, with P < 0.05 considered significant. All data were analyzed using SPSS version 24.0 software (SPSS Inc., Chicago, IL).
Results
For this study, the sum of 821 people with schizophrenia were included, with an 18.8% prevalence of aggressive behavior and a mean age of 49.08 years (SD=11.971). The participants’ demographic data and other details are shown in Table 1. The mean BMI of the patients was 25.026 (SD=4.309), with a slightly higher proportion of female patients (52.0%) than male (48.0%) and 701 patients (85.4%) had no religious affiliation. In addition, we saw that 84.5% of patients only had a junior high school education, 81.7% had no family history of mental illness, 90.6% lived with their families, 54.0% were married, 62.7% had no other comorbid physical illnesses, 79.4% had no smoking behavior, 91.4% had no alcohol abuse. 65.2% had no Physical exercise behavior, 81.4% of patients were unemployed, and 52.7% of patients had an average monthly family income between 500 and 2000 RMB.
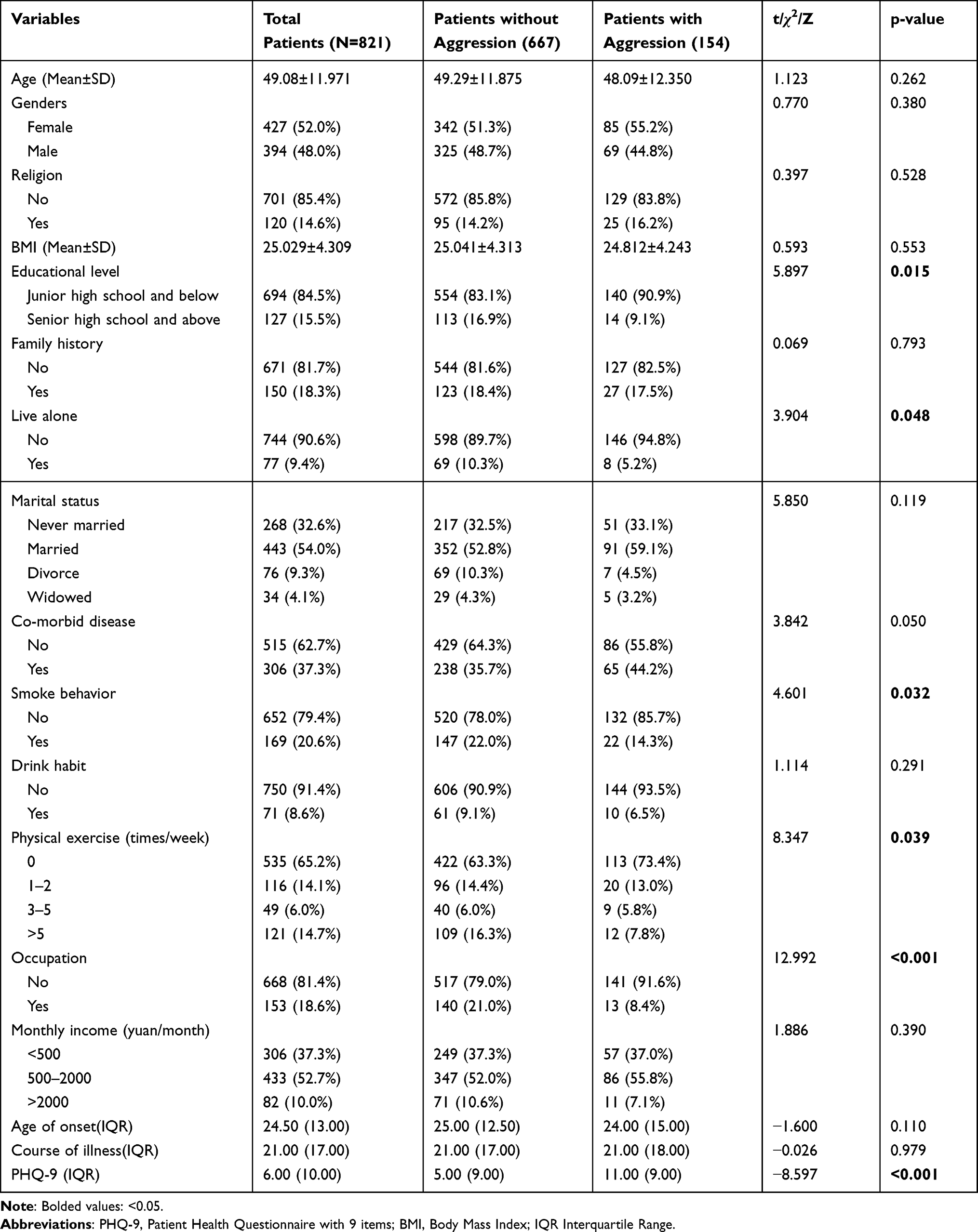 |
Table 1 Demographic Characteristics and PHQ-9 Scores of Patients with Schizophrenia with and without Aggressive Behavior |
As shown in Table 1, patients in the assault group had a lower level of education compared to the non-assault group (F=5.897, p=0.015). There were statistically significant differences in the form of residence (F=3.904, p=0.048), smoking behavior (F=4.601, p=0.032), and physical activity (F=8.347, p=0.039) between the two groups. Additionally, the percentage of unemployed individuals in the attack group was considerably higher than that in the non-assault group (91.6% vs 79.0%, p<0.001). In comparison to the non-assault group, the assault group’s PHQ-9 ratings were considerably higher (F=−8.597, p<0.001).
As shown in Table 2, a multifactorial logistic regression equation was constructed by including education level, whether living alone, smoking behavior, physical activity status, work, and PHQ-9 score. The results found that the effects of education level on aggression in schizophrenia patients were statistically significant (OR=0.470, 95% CI 0.254–0.870), whether or not living alone on aggression in schizophrenia patients were statistically significant (OR=0.383, 95% CI 0.174–0.845), depressive mood on aggression in schizophrenia patients was statistically significant (OR=1.147, 95% CI 1.112–1.184).
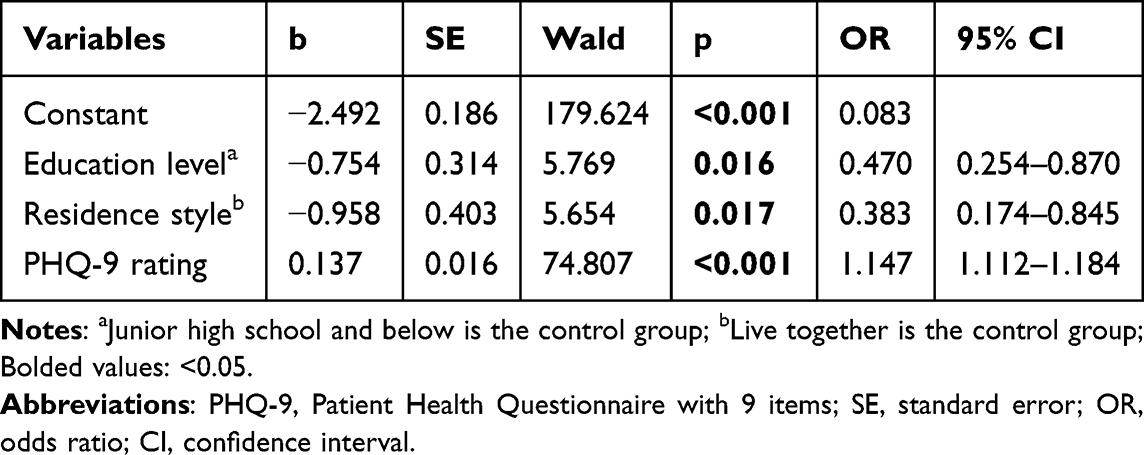 |
Table 2 Logistic Regression of Factors Associated with Aggression in Patients with Schizophrenia |
In a univariate analysis, Table 3 demonstrates that poorer literacy (p=0.028), less physical activity (p=0.005), unemployment (p=0.001), younger age at disease debut (p=0.010), and higher melancholy mood (p<0.001) were linked with higher levels of aggression. Higher levels of violence remained correlated with lower literacy (p=0.017) and higher depressive symptoms (p<0.001) in multivariate analysis.
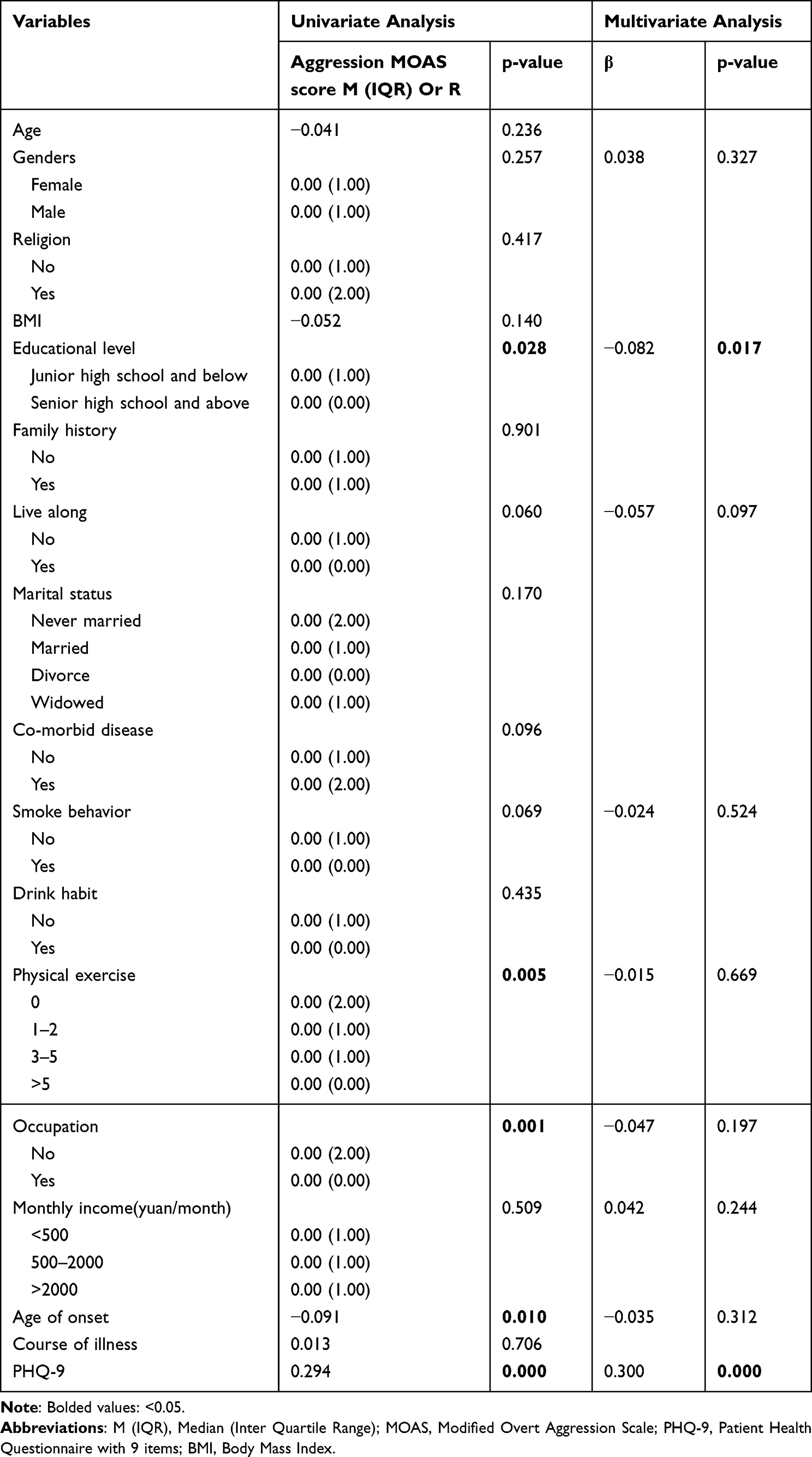 |
Table 3 Clinical and Sociodemographic Traits That Correlate with the Intensity of the Violence |
Discussion
This is the first study to look at the link between depressed mood and aggressive behaviors in schizophrenia patients. Patients in the aggressive group had lower rates of smoking and living alone, higher percentages of unemployment, lower levels of education, and lower exercise practices as compared to the non-aggressive group. Depression, education level, and resident style were found to be significantly linked with aggressive behavior in schizophrenia patients using logistic regression analysis. Multiple linear regression showed that higher levels of aggression were associated with lower levels of education and higher depressive mood.
Aggressive behaviors are more common among the many symptoms of schizophrenia in patients. The prevalence of aggression in schizophrenia patients varies significantly around the world, ranging from 4.6% to 69.6%.5 Another large-scale study conducted in Norway found that 15.2% of schizophrenia outpatients were at risk for aggression.22 According to our findings, the prevalence of aggression in ambulatory patients was 18.8%. This result is consistent with previous studies. Several theories have attempted to explain why patients with schizophrenia are at higher risk of aggression, and for now, there are fewer studies on the neurobiology of this risk, but a number of candidate genes have been studied, the most studied being the catechol- o -methyltransferase (COMT) gene on chromosome 22.23 According to a new meta-analysis of Val158Met COMT, men with schizophrenia who carry the COMT gene’s low activity Met variant have a little higher risk of behaving violently.24 Other research, focused on female patients with schizophrenia, raises the possibility that various bodily metabolic markers may be connected to the development of violence. Herceg et al pointed out that in female schizophrenia patients, lowered HDL cholesterol levels have been associated with aggression.25 Another study showed that higher prolactin was significantly associated with aggression in female schizophrenia patients.26
Persons with schizophrenia frequently experience depressive mood, and a meta-analysis including 9879 persons with schizophrenia indicated that the frequency of co-morbid depression in schizophrenia was about 28.6%.27 Depression combined with aggression is also more common in adults. A recent longitudinal study of the entire Swedish population found that those with depression had a risk of aggression that was around three times higher than that of the general population and twice as high as that of their non-depressed siblings.28 The most common form of aggression is self-aggression, which has been shown to mediate the relationship between depression and externalizing aggression.29 Numerous research have proven that there is a strong link between depression and the emergence of violent conduct,30,31 however, it is unclear how the two are related causally. According to our research, having a high level of depression increases the likelihood that aggressive conduct would occur. Kofler et al found that a model in which early depressive symptoms predicted changes in maladaptive behaviors was more consistent with the data than a model in which maladaptive behaviors predicted depressive symptoms,32 which is consistent with our findings. But research has also shown that frequent violence contributes to depressed symptoms.33 These findings can be attributed to variations in the survey population and methodology.
In addition, we found that low education levels and living alone were also associated with aggressive behavior. Among them, low education level was a risk factor, while living alone was a protective factor. A previous study reported that schizophrenia patients who live alone lead to poor treatment adherence and high risk of relapse.34 And since several previous studies have shown that the increase in aggression in psychiatric patients is directly proportional to the severity of their psychiatric symptoms,11,35 it would seem that psychiatric patients living alone are seemingly more likely to engage in aggressive behavior, which seems to contradict our findings. However, Swanson et al found that patients who lived with their family were more likely to act aggressively.36 Living alone is a protective factor against agitation, according to results of another observational study from China.37 There are several possible reasons for this. Firstly, because schizophrenia itself can lead to poorer social interactions, and because people with schizophrenia themselves carry a higher degree of stigma than other illnesses,38 which can lead to social withdrawal. Therefore, the aggressive behavior of psychiatric patients living at home mostly occurs with their caregiving relatives, and studies have shown that more than half of the caregiving relatives report that they have had to deal with conflicts,39,40 both verbal and physical, and even more than one-fifth of the relatives said that they feared for their lives as a result.7 In contrast, psychiatric patients living alone do not have caregivers. Second, psychiatric patients who are able to live alone at home are themselves less symptomatic and less likely to engage in aggressive behavior. This is because in China, serious assaults and injuries can result in forced hospitalization by local authorities or other relatives, whereas this survey was conducted on homebound patients only. Third, some patients’ family members may interfere with the patient’s treatment, and there is evidence that some patients’ family members may object to drug treatment.41 On the other hand, it has also been shown that patients with low levels of education are more likely to be aggressive than those with high levels of education,42,43 and the lower the level of education, the greater the likelihood of physical aggressiveness.44,45 Higher education, according to Harris and Kelly, can help people become less aggressive because it teaches them to think critically and restrains their emotional outbursts.45 A study from Europe involving more than 27,000 adolescents suggests that aggression is strongly and negatively correlated with academic performance, and that part of these associations is explained by common genetic effects.46 Additionally, it has been suggested that low levels of educational correspond to worse cognitive functioning, and that cognitive impairment is connected to aggressive and violent conduct in schizophrenia patients.43 Because cognitive rehabilitation therapy may be beneficial for cognitive impairment.47
In previous research, male gender and young age at first were determined to be risk factors for aggression in schizophrenia patients,48 but in our study, our researchers did not discover a relationship between gender and aggression in patients with schizophrenia. The results of numerous studies on gender as a potential risk factor for aggressive behavior in people with schizophrenia vary. In a retrospective study, Vevera et al found that male and female aggressiveness prevalence rates were, respectively, 41.8% and 32.7% overall.49 In contrast, in a large state psychiatric hospital in the United States, the rates of violent behavior during acute admission were 57.6% and 24.5% for women and men, respectively.50 According to many studies, there is a variable relationship between gender and aggression in schizophrenia patients, which may be influenced by the local demographics of the survey area.10
It is crucial to note, however, that the current study had several limitations. First, because the study was cross-sectional, the interpretation of the causal association between aggression and risk variables in stable schizophrenics is limited. Therefore, to confirm the causal association, future research may concentrate on longitudinal investigations. Second, because our sample consisted of patients treated at home, the results may not be applicable to inpatients with schizophrenia. Third, this study was done only in the townships around Chaohu, which may not be representative for patients in other regions of China. Fourth, because only rural schizophrenia patients were examined in this article, the findings may not be generalizable to patients in the cities settings.
Conclusions
In conclusion, the current study revealed that 18.8% of stable schizophrenia patients exhibited violent conduct, which indicates that aggressive behavior is relatively common among schizophrenia patients. Furthermore, according to our findings, stable schizophrenics with poor educational levels and depressed mood are more likely to engage in aggressive conduct. Although living alone is a protective factor, this may be related to the selection of the survey population and the fact that people with schizophrenia who live alone are still likely to engage in aggressive behavior. Aggression levels were correlated with education levels and depressive mood. These findings help physicians and families to prevent the onset of schizophrenic aggression early.
Acknowledgments
We thank all participants and researchers for their contribution to the collection and organization of data.
Ethics Approval and Consent to Participate
The survey strictly followed the principles of the Helsinki Declaration and was approved by the Ethics Committee of Chaohu Hospital of Anhui Medical University. Ethics ID:KYXM-202212-013. We informed all respondents and their guardians of the purpose of this study and assured them that their privacy would not be compromised by signing, and all participants and their guardians signed an informed consent form.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Kahn RS, Sommer IE, Murray RM, et al. Schizophrenia. Nat Rev Dis Primers. 2015;1:15067. doi:10.1038/nrdp.2015.67
2. Li N, Chen G, Du W, Song X, Zhang L, Zheng X. Population-level prevalence estimate and characteristics of psychiatric disability among Chinese adults. J Psychiatr Res. 2011;45(11):1530–1534. doi:10.1016/j.jpsychires.2011.07.001
3. Chan KY, Zhao FF, Meng S, et al. Prevalence of schizophrenia in China between 1990 and 2010. J Glob Health. 2015;5(1):010410. doi:10.7189/jogh.05.010410
4. Hou CL, Chen MY, Cai MY, et al. Antipsychotic-free status in community-dwelling patients with schizophrenia in china: comparisons within and between rural and Urban areas. J Clin Psychiatry. 2018;79(3). doi:10.4088/JCP.17m11599
5. Li W, Yang Y, Hong L, et al. Prevalence of aggression in patients with schizophrenia: a systematic review and meta-analysis of observational studies. Asian J Psychiatr. 2020;47:101846. doi:10.1016/j.ajp.2019.101846
6. Zhou JS, Zhong BL, Xiang YT, et al. Prevalence of aggression in hospitalized patients with schizophrenia in China: a meta-analysis. Asia Pac Psychiatry. 2016;8(1):60–69. doi:10.1111/appy.12209
7. Loughland CM, Lawrence G, Allen J, et al. Aggression and trauma experiences among carer-relatives of people with psychosis. Social Psychiatry Psychiatric Epidemiol. 2009;44(12):1031–1040. doi:10.1007/s00127-009-0025-5
8. Fazel S, Gulati G, Linsell L, Geddes JR, Grann M. Schizophrenia and violence: systematic review and meta-analysis. PLoS Med. 2009;6(8):e1000120. doi:10.1371/journal.pmed.1000120
9. Bulgari V, Iozzino L, Ferrari C, et al. Clinical and neuropsychological features of violence in schizophrenia: a prospective cohort study. Schizophr Res. 2017;181:124–130. doi:10.1016/j.schres.2016.10.016
10. Caqueo-Urizar A, Fond G, Urzua A, Boyer L, Williams DR. Violent behavior and aggression in schizophrenia: prevalence and risk factors. A multicentric study from three Latin-America countries. Schizophr Res. 2016;178(1–3):23–28. doi:10.1016/j.schres.2016.09.005
11. Wu Y, Kang R, Yan Y, et al. Epidemiology of schizophrenia and risk factors of schizophrenia-associated aggression from 2011 to 2015. J Int Med Res. 2018;46(10):4039–4049. doi:10.1177/0300060518786634
12. Iozzino L, Ferrari C, Large M, Nielssen O, de Girolamo G. Prevalence and risk factors of violence by psychiatric acute inpatients: a systematic review and meta-analysis. PLoS One. 2015;10(6):e0128536. doi:10.1371/journal.pone.0128536
13. Naguy A. Depression in schizophrenia - A good or bad omen? Asia Pac Psychiatry. 2018;10(2):e12312. doi:10.1111/appy.12312
14. Blitstein JL, Murray DM, Lytle LA, Birnbaum AS, Perry CL. Predictors of violent behavior in an early adolescent cohort: similarities and differences across genders. Health Educ Behav. 2005;32(2):175–194. doi:10.1177/1090198104269516
15. Kang T, Louden JE, Ricks EP, Jones RL. Aggression, substance use disorder, and presence of a prior suicide attempt among juvenile offenders with subclinical depression. Law Hum Behav. 2015;39(6):593–601. doi:10.1037/lhb0000145
16. Painuly NP, Grover S, Gupta N, Mattoo SK. Prevalence of anger attacks in depressive and anxiety disorders: implications for their construct? Psychiatry Clin Neurosci. 2011;65(2):165–174. doi:10.1111/j.1440-1819.2010.02177.x
17. Liu Q, Cole DA. Aggressive outbursts among adults with major depressive disorder: results from the collaborative psychiatric epidemiological surveys. J Psychiatr Res. 2021;135:325–331. doi:10.1016/j.jpsychires.2021.01.040
18. Ten Have M, de Graaf R, van Weeghel J, van Dorsselaer S. The association between common mental disorders and violence: to what extent is it influenced by prior victimization, negative life events and low levels of social support? Psychol Med. 2014;44(7):1485–1498. doi:10.1017/S0033291713002262
19. Elbogen EB, Johnson SC. The intricate link between violence and mental disorder: results from the national epidemiologic survey on alcohol and related conditions. Arch Gen Psychiatry. 2009;66(2):152–161. doi:10.1001/archgenpsychiatry.2008.537
20. Kay SR, Wolkenfeld F, Murrill LM. Profiles of aggression among psychiatric patients. I. Nature and prevalence. J Nerv Ment Dis. 1988;176(9):539–546. doi:10.1097/00005053-198809000-00007
21. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
22. Ose SO, Lilleeng S, Pettersen I, Ruud T, van Weeghel J. Risk of violence among patients in psychiatric treatment: results from a national census. Nord J Psychiatry. 2017;71(8):551–560. doi:10.1080/08039488.2017.1352024
23. Soyka M. Neurobiology of aggression and violence in schizophrenia. Schizophr Bull. 2011;37(5):913–920. doi:10.1093/schbul/sbr103
24. Singh JP, Volavka J, Czobor P, Van Dorn RA. A meta-analysis of the Val158Met COMT polymorphism and violent behavior in schizophrenia. PLoS One. 2012;7(8):e43423. doi:10.1371/journal.pone.0043423
25. Herceg D, Mimica N, Herceg M, Puljic K. Aggression in women with schizophrenia is associated with lower HDL cholesterol levels. Int J Mol Sci. 2022;23(19). doi:10.3390/ijms231911858
26. Puljic K, Herceg M, Tudor L, Pivac N. The association between prolactin concentration and aggression in female patients with schizophrenia. World J Biol Psychiatry. 2021;22(4):301–309. doi:10.1080/15622975.2020.1795254
27. Li W, Yang Y, An FR, et al. Prevalence of comorbid depression in schizophrenia: a meta-analysis of observational studies. J Affect Disord. 2020;273:524–531. doi:10.1016/j.jad.2020.04.056
28. Fazel S, Wolf A, Chang Z, Larsson H, Goodwin GM, Lichtenstein P. Depression and violence: a Swedish population study. Lancet Psychiatry. 2015;2(3):224–232. doi:10.1016/S2215-0366(14)00128-X
29. Franke I, Shenar R, Nigel S, et al. Selbstaggression als Mediator zwischen Depression und Aggressivität. Psychiatrische Praxis. 2019;46(06):332–337. doi:10.1055/a-0860-4719
30. Coid J, Yang M, Roberts A, et al. Violence and psychiatric morbidity in a national household population--a report from the British household survey. Am J Epidemiol. 2006;164(12):1199–1208. doi:10.1093/aje/kwj339
31. Arseneault L, Moffitt TE, Caspi A, Taylor PJ, Silva PA. Mental disorders and violence in a total birth cohort: results from the Dunedin Study. Arch Gen Psychiatry. 2000;57(10):979–986. doi:10.1001/archpsyc.57.10.979
32. Kofler MJ, McCart MR, Zajac K, Ruggiero KJ, Saunders BE, Kilpatrick DG. Depression and delinquency covariation in an accelerated longitudinal sample of adolescents. J Consult Clin Psychol. 2011;79(4):458–469. doi:10.1037/a0024108
33. Yu R, Aaltonen M, Branje S, et al. Depression and violence in adolescence and young adults: findings from three longitudinal cohorts. J Am Acad Child Adolesc Psychiatry. 2017;56(8):652–8 e1. doi:10.1016/j.jaac.2017.05.016
34. Xiao J, Mi W, Li L, Shi Y, Zhang H. High relapse rate and poor medication adherence in the Chinese population with schizophrenia: results from an observational survey in the People’s Republic of China. Neuropsychiatr Dis Treat. 2015;11:1161–1167. doi:10.2147/NDT.S72367
35. Appelbaum PS, Robbins PC, Monahan J. Violence and delusions: data from the MacArthur violence risk assessment study. Am J Psychiatry. 2000;157(4):566–572. doi:10.1176/appi.ajp.157.4.566
36. Swanson JW, Swartz MS, Van Dorn RA, et al. A national study of violent behavior in persons with schizophrenia. Arch Gen Psychiatry. 2006;63(5):490–499. doi:10.1001/archpsyc.63.5.490
37. Mi W, Zhang S, Liu Q, et al. Prevalence and risk factors of agitation in newly hospitalized schizophrenia patients in China: an observational survey. Psychiatry Res. 2017;253:401–406. doi:10.1016/j.psychres.2017.02.065
38. Zahid A, Best MW. Stigma towards individuals with schizophrenia: examining the effects of negative symptoms and diagnosis awareness on preference for social distance. Psychiatry Res. 2021;297. doi:10.1016/j.psychres.2021.113724
39. Vaddadi KS, Soosai E, Gilleard CJ, Adlard S. Mental illness, physical abuse and burden of care on relatives: a study of acute psychiatric admission patients. Acta Psychiatr Scand. 1997;95(4):313–317. doi:10.1111/j.1600-0447.1997.tb09637.x
40. Lauber C, Eichenberger A, Luginbuhl P, Keller C, Rossler W. Determinants of burden in caregivers of patients with exacerbating schizophrenia. Eur Psychiatry. 2003;18(6):285–289. doi:10.1016/j.eurpsy.2003.06.004
41. Kozuki Y, Schepp KG. Adherence and nonadherence to antipsychotic medications. Issues Ment Health Nurs. 2005;26(4):379–396. doi:10.1080/01612840590922425
42. Sher L, Rutter SB, New AS, Siever LJ, Hazlett EA. Gender differences and similarities in aggression, suicidal behaviour, and psychiatric comorbidity in borderline personality disorder. Acta Psychiatr Scand. 2019;139(2):145–153. doi:10.1111/acps.12981
43. Jeyagurunathan A, Lau JH, Abdin E, et al. Aggression amongst outpatients with schizophrenia and related psychoses in a tertiary mental health institution. Front Psychiatry. 2021;12:777388. doi:10.3389/fpsyt.2021.777388
44. Fond G, Boyer L, Favez M, et al. Medication and aggressiveness in real-world schizophrenia. Results from the FACE-SZ dataset. Psychopharmacology. 2015;233(4):571–578. doi:10.1007/s00213-015-4167-8
45. Harris MB, Knight-Bohnhoff K. Gender and aggression II: personal aggressiveness. Sex Roles. 1996;35(1–2):27–42. doi:10.1007/BF01548173
46. Vuoksimaa E, Rose RJ, Pulkkinen L, et al. Higher aggression is related to poorer academic performance in compulsory education. J Child Psychol Psychiatr. 2021;62(3):327–338. doi:10.1111/jcpp.13273
47. Vita A, Barlati S, Ceraso A, et al. Effectiveness, core elements, and moderators of response of cognitive remediation for schizophrenia: a systematic review and meta-analysis of randomized clinical trials. JAMA Psychiatry. 2021;78(8):848–858. doi:10.1001/jamapsychiatry.2021.0620
48. Dack C, Ross J, Papadopoulos C, Stewart D, Bowers L. A review and meta-analysis of the patient factors associated with psychiatric in-patient aggression. Acta Psychiatr Scand. 2013;127(4):255–268. doi:10.1111/acps.12053
49. Vevera J, Hubbard A, Vesely A, Papezova H. Violent behaviour in schizophrenia. Retrospective study of four independent samples from Prague, 1949 to 2000. Br J Psychiatry. 2005;187:426–430. doi:10.1192/bjp.187.5.426
50. Kraus JE, Sheitman BB. Characteristics of violent behavior in a large state psychiatric hospital. Psychiatr Serv. 2004;55(2):183–185. doi:10.1176/appi.ps.55.2.183
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Minimal Effects of Cariprazine on Prolactin Levels in Bipolar Disorder and Schizophrenia
Culpepper L, Vieta E, Kelly DL, Patel MD, Szatmári B, Hankinson A, Earley WR
Neuropsychiatric Disease and Treatment 2022, 18:995-1011
Published Date: 12 May 2022
Anhedonia in Depression and Schizophrenia: Brain Reward and Aversion Circuits
Liang S, Wu Y, Hanxiaoran L, Greenshaw AJ, Li T
Neuropsychiatric Disease and Treatment 2022, 18:1385-1396
Published Date: 7 July 2022
Factors Affecting Negative Symptoms in Schizophrenia and Their Relationship with Anxiety and Depression
Zeng G, Liang R, Xiao L, Cao W, Zhou W, Wang W, Liu C, Zhou H, Shi X, Chen B, Chen W
Neuropsychiatric Disease and Treatment 2025, 21:229-240
Published Date: 4 February 2025
Oral Health-Related Quality of Life and Depression in Patients with Schizophrenia: The Mediating Roles of Oral Health Literacy and Oral Health-Related Self-Efficacy in a Cross-Sectional Structural Equation Analysis
He X, Huang X, Cai J, Zhou H, Wang Z, Lin Z, He C, Liu L, Xie Z, Liu X, Wei Y, Zeng J, Ye J, Xiao A
Neuropsychiatric Disease and Treatment 2026, 22:613904
Published Date: 8 July 2026