Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
An Effect of Chronic Negative Stress on Hippocampal Structures and Functional Connectivity in Patients with Depressive Disorder
Authors Zhang L, Zhang Y, Guo W, Ma Q, Zhang F, Li K, Yi Q
Received 23 February 2024
Accepted for publication 3 May 2024
Published 14 May 2024 Volume 2024:20 Pages 1011—1024
DOI https://doi.org/10.2147/NDT.S460429
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Lili Zhang,1– 3 Yunshu Zhang,2,3 Wentao Guo,2,3 Qi Ma,1,4 Feng Zhang,2,3 Keqing Li,2,3 Qizhong Yi1,4
1The First Affiliated Hospital of Xinjiang Medical University, Urumqi, People’s Republic of China; 2Hebei Provincial Mental Health Center, Baoding, Hebei Province, People’s Republic of China; 3Hebei Key Laboratory of Major Mental and Behavioural Disorders, Baoding, Hebei Province, People’s Republic of China; 4Xinjiang Clinical Research Center for Mental (Psychological) Disorder, Urumqi, People’s Republic of China
Correspondence: Qizhong Yi, The First Affiliated Hospital of Xinjiang Medical University, No. 137, Liyushan Road, Urumqi, 830054, People’s Republic of China, Tel +86 13079911689, Email [email protected] Keqing Li, Hebei Provincial Mental Health Center, No. 572, Dongfeng East Road, Baoding City, Hebei Province, 071000, People’s Republic of China, Tel +86 13703288007, Email [email protected]
Purpose: Depressive disorder is a mental health disorder with complicated etiopathogenesis. Environmental stress and neurodevelopment combined with other factors contribute to the occurrence of depression. Especially for the depressive disorder with chronic negative stress, it has characteristics of recurrence and poor curative effect because of unclear mechanism. Here, we investigated the hippocampal structures and functional connectivity (FC) according to resting-state functional magnetic resonance imaging in patients with depression who underwent chronic negative stress.
Patients and Methods: A total of 65 patients with depression (34 underwent chronic negative stress and 31 non-underwent chronic negative stress) and 30 healthy controls who did not undergo chronic negative stress were included in the study. The volumes of hippocampal subfields, seed-based FCs between hippocampus and the whole brain voxels, and ROI-wise-based FC between hippocampal subfields were compared among the three groups.
Results: In the patients with depression who underwent chronic negative stress, the volumes of right_GC-ML-DG-head, right_CA4-head and right_CA3-head increased, FCs between Temporal_Mid_R, Precuneus_R, Frontal_Sup_R, Temporal_Sup_R, Angular_L, Frontal_Inf_Tri_R, Supp_Motor_Area_R, Precentral_L and hippocampus increased, and FCs between parasubiculum and CA3, and presubiculum and CA1 decreased. When compared to the patients who did not undergo chronic negative stress, the patients who underwent chronic negative stress had larger volumes of right_GC-ML-DG-head and right_CA3-head, higher FCs between Frontal_Sup_R, Frontal_Inf_Tri_R and hippocampus, and lower FCs between presubiculum and CA1.
Conclusion: The depression underwent chronic negative stress may experience disrupted hippocampal structures and functional connectivity. It may be one of potential depressive disorder subtypes.
Keywords: depressive disorder, chronic stress, hippocampus, functional connectivity
A Letter to the Editor has been published for this article.
Introduction
Major depressive disorder (MDD) is a common psychiatric disorder with persistent depressed mood, anhedonia, or hopelessness. MDD is often associated with impaired social function and even leads to suicide in severe cases.1 Depression is the main cause of mental health related disease burden and disability internationally. In 2019, MDD affected 280 million people globally.2
The antidepressant medication treatment is the main therapy for treating depression, but the remission rate is barely satisfactory, especially when the patients are only treated with drugs. Only 1/3 of patients respond to the antidepressant medication, and often suffer from side effects, such as nausea, vomiting, sleep interruption, sedation, sexual dysfunction and weight gain induced by drugs. In addition, nearly 15–30% of patients may develop into treatment-resistant depression.3–5
The risk factors, including genetic, immune, and environmental factors, for the onset of depressive disorder are comprehensive, and life events have been found to be important causes for depression.6 Studies showed that prolonged exposure to stress increased vulnerability to depression and other mood disorders, and led to memory disorder, cognitive disorder and even changes of the brain structure.7 Life events affect the onset and symptoms of depressive disorder, and also prognosis and recurrence.8 The positive correlation was found between negative life events and severity of depression.9 A study examined five stress exposures on depression in 878 Afro-Caribbean women and found chronic stress was associated with increased risk for both recent (past week) and more distal (past-year and lifetime) major depressive episodes.10 In a 10-year cohort study, negative life events was one of the predictors for vulnerable and chronic high-risk groups with depressive and posttraumatic stress disorder symptoms, which were more likely to experience poor quality of life in adulthood.11 The research on first-episode MDD showed cumulative effects of adverse childhood experiences and negative life events were associated with suicidal behaviors, cognitive impairment and phenome features.12 So the chronic negative stress may have strong effects on the clinical features of major depressive disorder. The MDD with chronic negative stress may be worth researching and using rather than the binary diagnosis of MDD based on the DSM-5 or ICD. However, objective evidence are still lacking to prove the differences between MDD with and without chronic negative stress.
Hippocampus may participate in cognitive and emotional regulation, and the current view is that the dorsal hippocampus is implicated in memory as well as cognition, and ventral hippocampus mediates the mood.13 In addition, recent studies focused more on the changes of hippocampal subfields. A study extracted 12 hippocampal subfield volumes per hemisphere in 4174 participants, and showed larger right hippocampal fissure was associated with depressive symptoms, and larger bilateral hippocampal fissure, larger right molecular layer and smaller right cornu ammonis (CA)3 were associated with chronic depressive symptoms.14 Except for hippocampal and the subfields volumes, recent studies also investigated the hippocampal functional abnormalities in MDD. According to seed-based analysis, weaker connectivity of the right hippocampal subregion to the temporal cortex (extending to the insula) and basal ganglia, enhanced connectivity of the right subiculum to the bilateral lingual gyrus were exhibited, and FC between the right CA1 and right fusiform, between the right hippocampal amygdala transition area and the bilateral basal ganglia, were negatively related with depression severity;15 decreased FC between right hippocampus and bilateral medial superior frontal gyrus in MDD group.16 According to ROI-wise-based analysis, the hippocampus-right angular gyrus FC had the highest predictive strength for the clinical remission induced by Ketamine in major depression.17 The brain image evidence supported hippocampal structural and functional connectivity participated in the depressive disorder.
Adult hippocampal neurogenesis in human brain was demonstrated, and the environmental components, such as stress and life events, have significant impacts on adult hippocampal neurogenesis.18 That becomes the research focus in the depression underwent stress, and also provided the new strategy for exploring the pathogenesis.19–21 Chronic unpredictable restraint stress over 4 weeks for rat decreased total hippocampal volume, reflecting loss of volume in dorsal and ventral hippocampus,22 reduced the length and volume of myelinated fibers in CA1 region and DG, and the rats showed depressive-like behaviors.23 Volumetric analysis of the brain that underwent neonatal maternal separation in adult mice revealed that the left hippocampus was smaller, and the neuronal integrity of right hippocampus reduced.24 In the chronic restraint stress-induced depression model, the volume of the hippocampal hilus decreased significantly.25 In major depressive disorder patients, the whole brain analysis identified reduced hippocampal gray matter volume was a common feature of major depressive disorder patients, and the left hippocampal gray matter volume was also associated with stressful life events.26,27 Another study investigated the differences of hippocampal subfield volumes using 7-Tesla MRI, and analyzed the association between life-stressor and hippocampal subfield volumes, found right-hemisphere CA2/3 subfield volume reduced in MDD patients, and left CA1, left CA4/DG, right subiculum total, left hippocampus total, and right hippocampus total were negatively associated with life-stressor checklist scores.28
In summary, the evidence above suggests hypotheses that depressive disorder underwent chronic negative stress, especially the life stress, may be one potential subtype of MDD, and hippocampus may participate in the the pathogenic process of depression in those who underwent chronic stress. However, there is little research evidence now to support this hypotheses in these patients, and the role of hippocampus is worth further discussion. In this study, patients with depression who underwent chronic stress were included, the features of structural, seed-based and ROI-wise-based functional connectivity of hippocampus and subfields were analyzed and screened.
Materials and Methods
Participants
Patients
Sixty-five first-onset patients with major depressive disorder were recruited from Hebei Provincial Mental Health Center of China during January, 2021 and October, 2022. The age of patients ranged from 18 to 45. The patients were right-handed and diagnosed using Diagnostic and Statistical Manual of Mental Disorders 5th edition by psychiatrists and met the criteria for major depressive disorder. The clinical symptoms were assessed using 17-item Hamilton Depression Rating Scale (HAMD-17), and the total score was ≥17. All the patients never had manic or manic symptoms episode history. The patients were never treated with antidepressant therapy, hormones, antibiotics, or other drugs that affect the secretion and metabolism of immune and neurotransmitters before included in the study. All participants submitted written informed consent before conducting the study. Patients with other psychiatric disorders, serious neurological or medical disorders, receiving MECT or rTMS treatment, and MRI scan contraindication were excluded.
Health Controls
Thirty health controls were right handed and recruited from the community. The age, gender and education level were matched with patients. All the controls were screened to ensure the lifetime absence of psychiatric illness. The scores of HAMD-17 for controls were <7. All of them submitted written informed consent. The controls with positive family history were excluded, and other exclusion criteria were the same with patients.
Chronic Negative Stress Evaluation
We evaluated the chronic negative stress with Life Events Scale (LES).29 It is a self reporting scale, with good reliability and validity, widely used in China. The LES measures the numbers and sensory stress of stressful life events the subjects have been exposed to. There are 48 items in the scale, including 3 dimensions. The subjects need to recall the life events occurred within at least one year, evaluate the nature (positive or negative) of the events, as well as the impact extent and duration on mental state. The impact extent is divided into 5 levels which ranges from 0 to 4 points. The duration ranges from 1 to 4 (1=within 3 months, 2= within 6 months, 3= within one year, 4=more than one year). The greater mental stress is indicated by higher scores of LES. Based on previous research, the negative life events have greater impact on physical and mental health, and the effects of the positive life events needs to be studied. The evidence also supported chronic stress may increase the risk of depression.30–33
Taking into account the feature of LES and the study evidence, the study focused on the effects of chronic negative life events. To assess the presence of chronic negative life stress, it should meet the standards as following: the participants reported more than one negative life stress, impact extent reached moderate and above (score≥2);33 and the duration lasted more than 1 year (score=4).34 The participants who could not meet the standards above simultaneously were regarded as not having undergone chronic negative life stress.
fMRI Data Acquisition and Processing
fMRI data were collected by a 3.0T GE Signa scanner. The imaging sessions included structural T1 and a resting condition FC.
The structural T1 images were acquired with the following parameters: repetition time (TR)=6.7ms, echo time (TE)=2.7ms, flip angle(FA)=15°, field of view (FOV)=256mm×256mm, matrix=256×256, slice thickness=1mm, slices=200. The structural T1 images were conducted with FreeSurfer 7.3.2. FS 6.0 version, which was employed to perform the hippocampal subfields.35 The volumes of the subfields, including parasubiculum, presubiculum, subiculum, cornu ammonis (CA1, CA3 and CA4), GC-ML-DG, molecular layer, HATA, fimbria, hippocampal fissure, hippocampal tail and whole hippocampus, were returned.
The resting-state functional images were acquired using the following parameters: TR=2000ms, TE=30ms, FA=90°, FOV=220mm×220mm, matrix=64×64, slice thickness=3mm, slices=35. The functional images data was conducted using the SPM12 software. The first five volumes were discarded. Scans with head motion of more than 3mm in the x, y, or z direction or 3° of any angular motion were excluded. The remaining images were normalized to a standard Montreal Neurological Institute (MNI) template, resampled into 3mm×3mm×3mm voxel size, smoothed with 6mm×6mm×6mm full-width-at-half-maximum Gaussian kernel. Multiple regression models were employed to remove the effects of confounding factors, including white matter signals, cerebrospinal fluid signals, and 24 motion parameters. Finally, the images were temporally band-pass filtered at the range of 0.01Hz-0.08Hz.
Functional Connectivity (FC) Analysis
For seed-based FC analysis, the bilateral hippocampus regions defined from Anatomical Automatic Labeling (AAL) atlas were selected as seeds. The correlation analysis was conducted between the seed regions and the whole brain voxels, and then the resulting r values were converted according to Fisher’s r-to-z transformation. For ROI-wise-based FC analysis, the average time series across all voxels of each hippocampal subregion was computed as a reference time course separately for each subject, and then the correlation coefficients were converted according to Fisher’s r-to-z transformation.
Statistical Analysis
SPSS 22.0 software was used to analyze the demographic and clinical variable. The fMRI data were analyzed mainly on the Matlab and GraphPad Prism platform. ANCOVA was performed to access differences in volumes for hippocampal subfields among the patients with depression who underwent chronic stress, the patients with depression who did not undergo chronic stress and health controls while adjusting for the effects of age, gender and educational level. The findings were considered significant at P <0.05, and then the significant results were analyzed with Fisher’s LSD. Age, gender and education were modeled as covariates of no interests, and ANOVA was employed to compare the differences of seed-based FC among 3 groups, significant clusters were identified by using a Gaussian random field cluster level threshold of P < 0.05 which corresponded to a voxel P < 0.001 at corrected level with FWE, and the significant results were corrected using Bonferroni’s multiple comparisons test. The values of ROI-wise-based FC were also compared among groups by ANOVA and results were considered significant at corrected P < 0.05 (using Bonferroni’s multiple comparisons test).
Results
Demographic and Clinical Characteristics
34 patients with depression who underwent chronic negative stress, 31 patients with depression who did not undergo chronic negative stress and 30 health controls were included in the study.
The age range for the subjects was 18–45. There were no significant differences in regard to age (F=0.06, P=0.94), gender (χ2=0.66, P=0.72), educational level (χ2=8.03, P=0.09), occupational status (χ2=4.33, P=0.12), marital status (χ2=2.79, P=0.59), residence (χ2=2.50, P=0.29), smoking history (χ2=0.35, P=0.84), and alcohol use (χ2=0.78, P=0.68) among the participants. The parenting-pattern (χ2=22.17, P=0.001) were significantly different among the 3 groups. Amid the depressive patients, coddling parenting, authoritative parenting and neglecting parenting patterns were more common than controls. The demographic data were presented in Table 1.
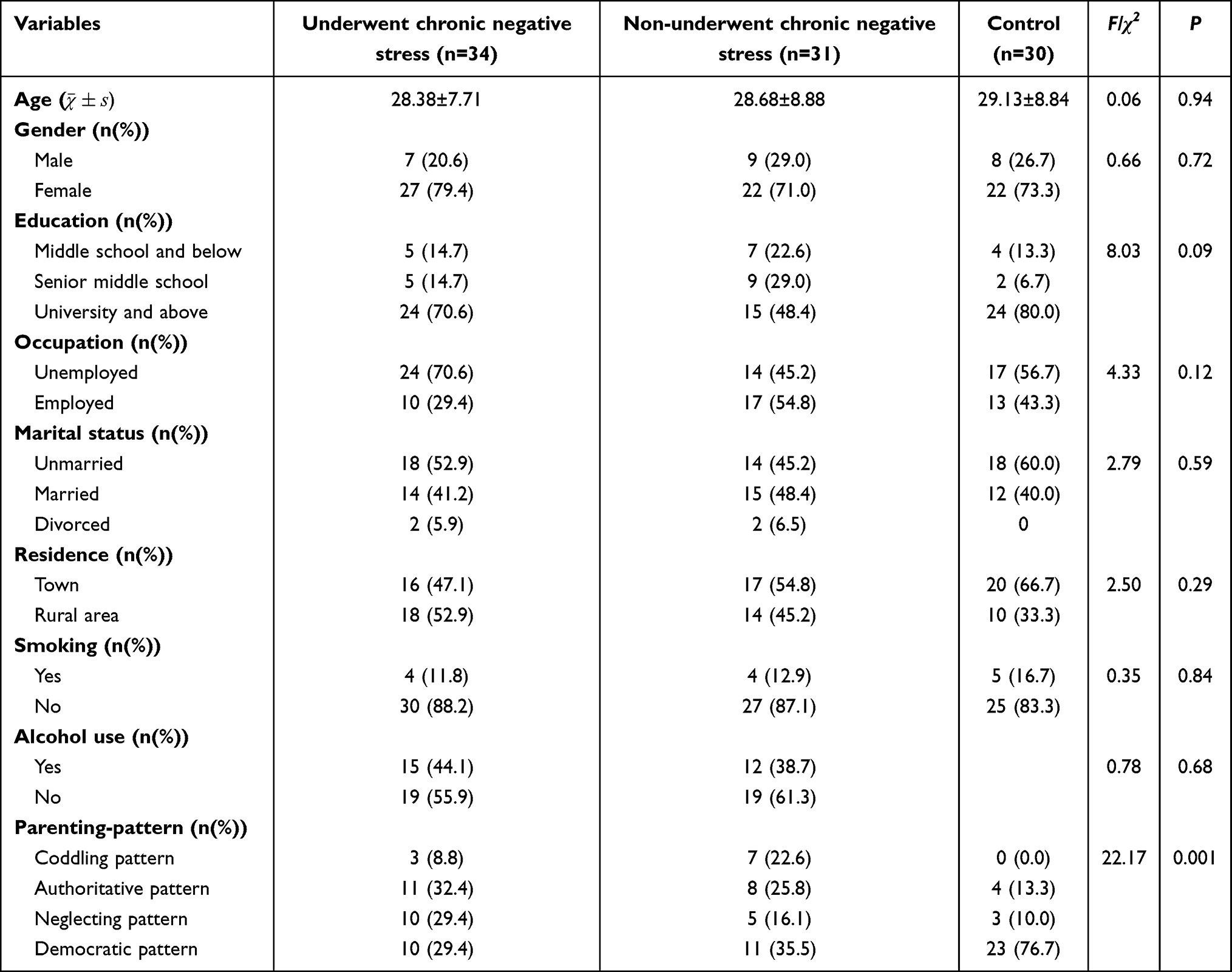 |
Table 1 Comparison of Demographic Data Among the Patients with Depression Who Underwent Chronic Negative Stress, the Patients with Depression Who Did Not Undergo Chronic Negative Stress and Health Controls |
All the patients had no somatic diseases nor positive family history of mental illness. The results for comparing the clinical features showed longer course (Z=−2.58, P=0.01), higher LES scores (t=2.48, P=0.02) in the patients with depression who underwent chronic negative stress. There was no significant difference in HAMD-17 scores (t=0.74, P=0.46), suicide behavior (χ2=1.88, P=0.17) or psychotic symptoms (χ2=1.15, P=0.28) between the two groups. The clinical data were showed in Table 2.
 |
Table 2 Comparison of Clinical Data Between the Patients with Depression Who Underwent Chronic Stress and the Patients with Depression Who Did Not Undergo Chronic Stress |
Hippocampal Subfields Analysis
Due to poor quality image, 1 participant was excluded in patients with depression who did not undergo chronic negative stress group. Thus, 94 subjects were included for hippocampal subfields analysis.
The volumes of right_GC-ML-DG-head (F=3.27, P=0.04), right_CA4-head (F=3.17, P=0.047) and right_CA3-head (F=4.16, P=0.02) showed significant differences among the 3 groups (Table 3). According to Fisher’s LSD analysis, the results supported that the volume of right_GC-ML-DG-head increased in the patients with depression who underwent chronic negative stress compared with the patients who did not undergo chronic negative stress (P=0.03) and controls (P=0.03); the volume of right_CA4-head are higher in the patients with depression who underwent chronic negative stress than controls (P=0.02); and the right_CA3-head increased in the patients with depression who underwent chronic negative stress compared with the patients who did not undergo chronic negative stress (P=0.02) and controls (P=0.01) (Figure 1A–C.).
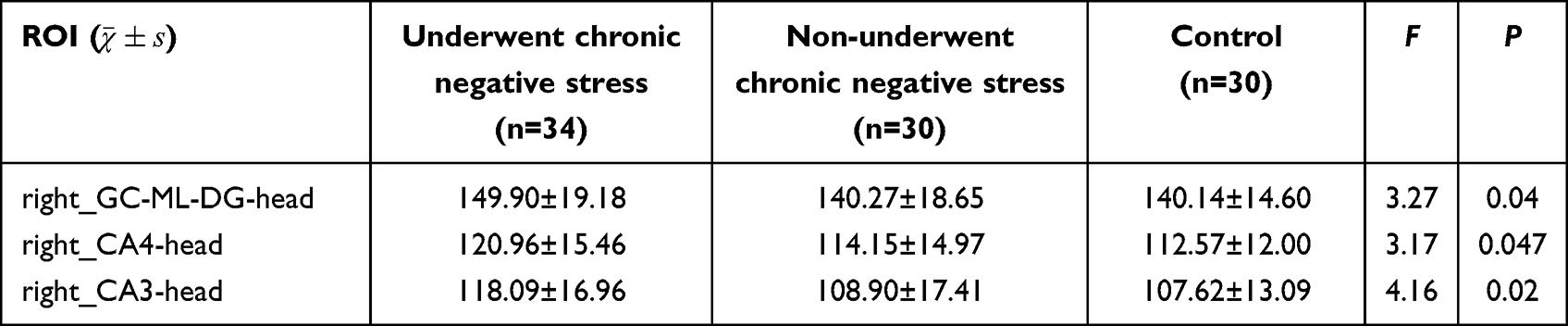 |
Table 3 Comparison of Hippocampal Subfields Volumes Among the Patients with Depression Who Underwent Chronic Negative Stress, the Patients with Depression Who Did Not Undergo Chronic Negative Stress and Health Controls |
 |
Figure 1 Comparison of hippocampal subfields volumes among the 3 groups. (A) The difference of volumes for right_GC-ML-DG-head; (B) The difference of volumes for right_CA4-head; (C) The difference of volumes for right_CA3-head. D1: Patients with depression who underwent chronic negative stress, D2: Patients with depression did not undergo chronic negative stress, HC: Health controls. *P<0.05. |
Functional Connectivity Results
ANOVA results of seed-based FC analysis revealed the significant differences for FCs between Temporal_Mid_R, Precuneus_R, Frontal_Sup_R, Temporal_Sup_R, Angular_L, Frontal_Inf_Tri_R, Supp_Motor_Area_R, Precentral_L and bilateral hippocampus. There were no regions with decreased FC (Table 4, Figure 2). Bonferroni’s multiple comparisons test showed increased FC between Frontal_Sup_R and hippocampus (P<0.001), as well as increased FC between Frontal_Inf_Tri_R and hippocampus (P=0.013) in the patients with depression who underwent chronic negative stress compared to patients with depression who did not undergo chronic negative stress (Figure 3A–H.).
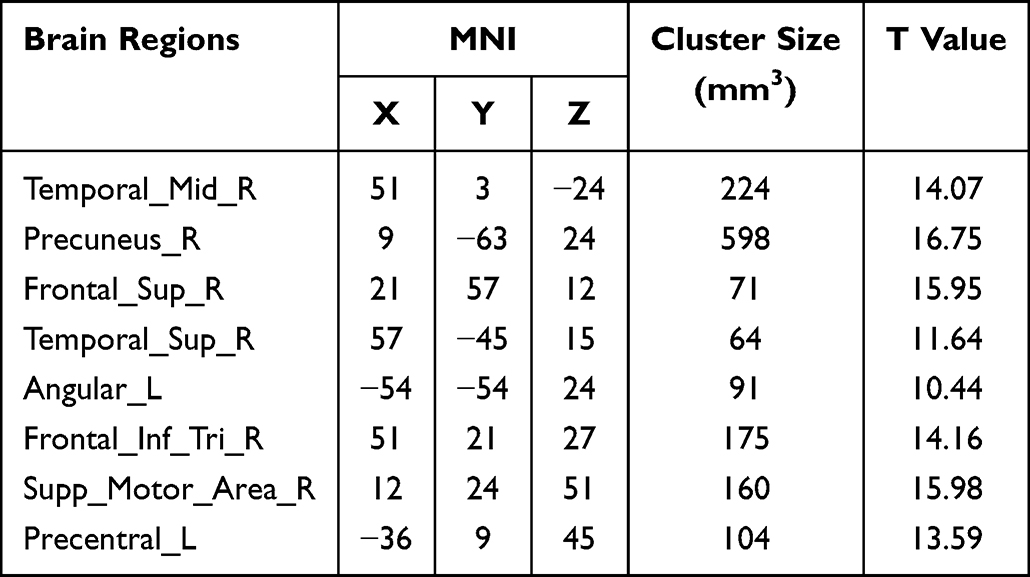 |
Table 4 The Differences of Seed-Based FCs Between Hippocampus and Whole Brain Among the Patients with Depression Who Underwent Chronic Negative Stress, the Patients with Depression Did Not Undergo Chronic Negative Stress and Health Controls |
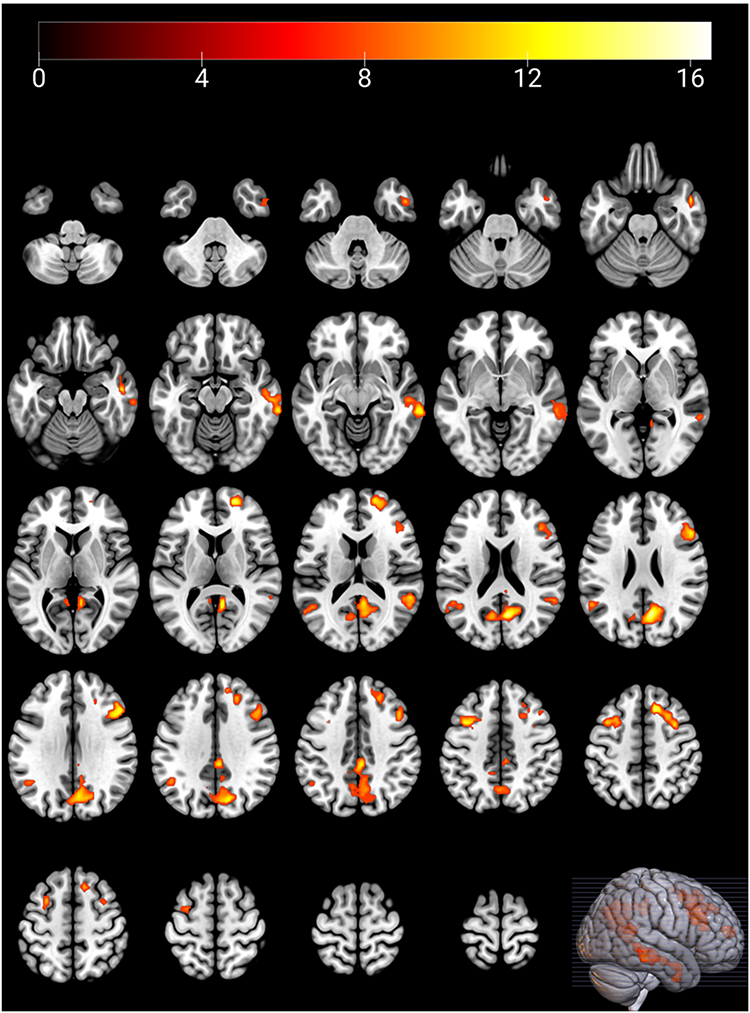 |
Figure 2 Significantly different brain regions of seed-based functional connectivity between hippocampus and whole brain among the three groups. zFCs increased between hippocampus and the brain regions marked with color, and there were no regions with reduced FC. After FWE correction, the voxel P<0.001 and cluster P<0.05. |
 |
Figure 3 Significantly different brain regions of seed-based functional connectivity between hippocampus and whole brain among the 3 groups. (A) The difference of zFC between Temporal_Mid_R and bilateral hippocampus; (B) The difference of zFC between Precuneus_R and bilateral hippocampus; (C) The difference of zFC between Frontal_Sup_R and bilateral hippocampus; (D) The difference of zFC between Temporal_Sup_R and bilateral hippocampus; (E) The difference of zFC between Angular_L and bilateral hippocampus; (F) The difference of zFC between Frontal_Inf_Tri_R and bilateral hippocampus; (G) The difference of zFC between Supp_Motor_Area_R and bilateral hippocampus; (H) The difference of zFC between Precentral_L and bilateral hippocampus. D1: Patients with depression who underwent chronic negative stress, D2: Patients with depression did not undergo chronic negative stress, HC: Health controls. *: P<0.05, **: P<0.01, ***: P<0.001, ****: P<0.001. |
The ROI-wise FC analysis showed significant differences for FCs from parasubiculum to CA3 (F=3.58, P=0.03), as well as presubiculum to CA1 (F=5.74, P=0.005) among the 3 groups (Figure 4.). After Bonferroni’s multiple comparisons test, the parasubiculum showed decreased FC with CA3 (P=0.03) in the patients with depression who underwent chronic negative stress compared to controls, and presubiculum showed lower FC with CA1 (P=0.003) in the patients with depression who underwent chronic negative stress than the patients with depression who did not undergo chronic negative stress (Figure 5A and B).
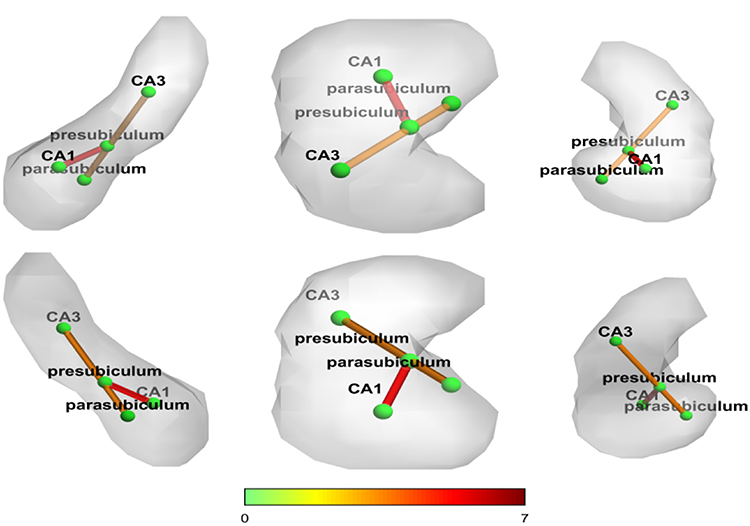 |
Figure 4 Significantly different functional connectivity analysis of hippocampal subfields among the 3 groups. Statistically significant zFCs between hippocampal subregions marked with color. |
 |
Figure 5 Significantly different functional connectivity among hippocampal subfields among the 3 groups. (A) The difference of zFC between parasubiculum and CA3; (B) The difference of zFC between presubiculum and CA1. D1: Patients with depression who underwent chronic negative stress, D2: Patients with depression did not undergo chronic negative stress, HC: Health controls. *: P<0.05, **: P<0.01. |
Discussion
This study investigated the changes of hippocampal structure and functional connectivity in the patients with depression who underwent chronic negative stress. Compared with the depressive patients who did not undergo chronic negative stress and controls, the volumes of right_GC-ML-DG-head, right_CA4-head and the right_CA3-head increased in the patients with depression who underwent chronic negative stress, FCs between Frontal_Sup_R, Frontal_Inf_Tri_R and bilateral hippocampus increased, and FCs between parasubiculum and CA3, and presubiculum and CA1 decreased in the patients with depression who underwent chronic stress. The study results presents the characteristic changes of hippocampus exist in depressive disorder with chronic negative stress, which may be the potential subtype of MDD.
Considering the demographic and clinical characteristics of the depressive disorders, we analyzed the features in the depressive patients who underwent chronic negative stress. Our findings suggested that the parenting-pattern may be related to the onset of depression. Coddling parenting, authoritative parenting and neglecting parenting were more common in the depressive patients, and democratic pattern was more common in health controls. Previous studies also supported our findings, showing that stressful life events and maladaptive parenting patterns were correlated with depression.36,37 But we failed to find the differences for the parenting-pattern between the patients who underwent chronic negative stress and those who did not. There were also a lack of positive evidence in the two groups. The scores of LES are higher in patients with depression who underwent chronic negative stress, indicating that these patients experienced more mental pressure. The study also showed longer illness course in depression with chronic negative stress. Sanwald S et al provided evidence that life stress was negatively associated with the age of depression onset, and positively associated with primary emotions,38 which also partly supported the results of the study. A previous study of Goldstein BL et al predicted higher depression symptoms in patients with higher levels of stressful life events,39 but our study did not find significant differences in scores of HAMD-17 between patients who underwent chronic negative stress and those who did not. Because of the smaller sample size, we were not able to classify the severity levels in patients according to the scores of HAMD-17 and clarify the relationship between chronic negative stress and depressive symptoms. The review reported that exposure to traumatic events might develop post traumatic neuropsychiatric sequelae, such as posttraumatic stress, major depression, and increased suicidal risk.40 However, this research could not find significant differences of suicide behavior between depressive patients who underwent chronic negative stress and those who did not. The relationship among chronic negative stress, depression and suicide may be complex, and the factors including stress types, depressive symptoms and severity may affect the final outcomes, therefore, all the variables need to be discussed in future studies.
Hippocampus as a core region was studied in depressive disorder. An article in 2020 targeted on hippocampal volume changes reviewed 39 studies, 11 of which investigated hippocampal substructures. The results showed the left and right hippocampi were, respectively, 92% and 91.3% of the volume found in controls.41 But these results did not show in other studies, neither did they find the hippocampal volume changes in depressive patients compared to controls.42,43 It prompted that inconsistent conclusions might be related to the characteristics of subjects, such as depressive subtypes, exposing stress, therapy, severity level and so on. On the other hand, the volume changes may happen more in hippocampal subfields than in the whole hippocampus. In this study, the confounding factors were controlled as much as possible and focused more on the volume changes of hippocampal subfields. The volumes of right_GC-ML-DG-head, right_CA4-head and right_CA3-head increased in patients with depression who underwent chronic negative stress compared to the controls. The volumes of right_GC-ML-DG-head and right_CA3-head in the patients with depression who underwent chronic negative stress increased compared to those who did not. Above results suggest that whether one undergoes chronic negative stress or not may potentially be depressive disorder subtypes. A study in 2019 also found that early stress exposure increased the volumes of hippocampus, in particular within the CA and DG;44 and another study showed a trend for higher total hippocampal volume in subjects who experienced stressful life events, yet a trend for lower total hippocampal volume in those who reported childhood maltreatment.45 These reports exposed the effects of stress on hippocampal volume which also was expounded in our study, but effects may differ according to varied stress types. The chronic negative stress was focused in our study, and may have the trend for a higher hippocampal subfields volumes rather than the total hippocampus. But it is necessary to clarify that increased hippocampal subfields volume does not mean the enhanced hippocampal function. Instead, it may cause functional problems, such as displayed inflammatory cell infiltration, swelling, vacuolar degeneration and necrosis and shrinkage of the neurons in hippocampus.46,47
Stress may affect brain functional connectivity.48 In healthy people, the left hippocampal connectivity with inferior parietal lobe was significantly correlated with chronic stress.49 Chronic restraint stress (CRS) depression model in rats showed hyperconnectivity in right retrosplenial cortex, visual cortex, and inferior colliculus and in bilateral thalamus, superior colliculus, dentate gyrus, and CA3.50 These revealed that chronic stress may have effects on functional connectivity in hippocampus and other brain regions. Recent studies also focused on the relationship between stress and hippocampal functional connectivity in depressive patients. One study assessed 34 first-episode, drug-naïve MDD patients with childhood trauma questionnaires and calculated the functional connectivity for ten hippocampal subregions, and found that functional connectivity alterations of CA1 were related to childhood trauma among the 34 patients.51 Another study investigated the mediating role of hippocampal connectivity in early-life socioeconomic deprivation and symptoms of depression and anxiety in the participants aged 23–24. It reported negative relationship between early-life socioeconomic deprivation and depressive symptoms, and global connectivity of the right hippocampus.52 In adolescents with MDD, connectivity between left hippocampus and bilateral orbital frontal cortex and right inferior temporal gyrus decreased, connectivity between left hippocampus and bilateral orbital frontal cortex was negatively correlated with the conflict scores of the Family Environment Scale, and it demonstrated that family environment contributed to MDD through hippocampal connectivity.53 Hendrix CL et al exposed the relationship between stress and hippocampus prior to birth, completing a fetal resting-state functional MRI scan during second or third trimester of pregnancy for the pregnant mothers, and reported that self-reported distress of the pregnant mother positively correlated with the higher function between the hippocampus and right posterior parietal association cortex.54 These prove that stress events in various stages of development of human,s and the hippocampal functional changes may contribute to the occurrence of depressive disorder. Because few evidences stated the relationship between chronic negative stress and hippocampal function in patients with depression, this study focused on exploring the correlation of chronic negative life events with hippocampal functional connectivity in first-episode depressive patients. Consensus view is that functional connectivity changes between the hippocampus and other brain regions. But the significant features may be different in depressive patients who underwent chronic negative stress. Compared to healthy control, FCs between hippocampus and Temporal_Mid_R, Precuneus_R, Frontal_Sup_R, Temporal_Sup_R, Angular_L, Frontal_Inf_Tri_R, Supp_Motor_Area_R and Precentral_L increased in the depressive patients who underwent chronic negative stress, but increased FCs only occurred between hippocampus and Frontal_Sup_R and Frontal_Inf_Tri_R compared to depressive patients who did not undergo chronic negative stress. These results also support our theory mentioned – whether one undergoes chronic negative stress or not may potentially be different depressive disorder subtypes. Current research also rarely investigates functional connectivity of hippocampal subfields in patients with depression who underwent chronic negative stress. A study showed FC of cornu ammonis 2, 3 and the dentate gyrus with bilateral caudate nucleus and precuneus was increased in chronic stress,55 however there were only college students with moderate stress indicated by Student-Life Stress Inventory, and depressive subjects were not included. For trauma-exposed adults, the FCs between left hippocampal CA1, left DG, and the posterior cingulate cortex presented weaker positive.56 Although there were no consistent results in current studies, it also supported that stress may affect the FC of hippocampal subfields. In our study, we focused more on the impact of chronic negative stress and found that FCs between parasubiculum and CA3, and presubiculum and CA1 decreased in depressive patients who underwent chronic negative stress. Maybe non-homogeneous research subjects, different types of stress, and so on contribute to the inconsistent results, and also may have brought different effects for the hippocampal functional connectivity.
In our study, it found the hippocampal structural and functional differences in depressive patients. Researchers promote both structural and functional change in regional and network plasticity of hippocampus potentially related to depressive disorder and antidepressant response.57 New articles also discussed the relationship between structural and functional connectivity in MDD, and found lower coupling strength between structural and functional connectivity existed in adolescent MDD group,58 and reduced decoupling of rostral anterior cingulate cortex with hippocampus and other extended task-specific regions during task performance in MDD participants.59 So it clarified that both hippocampal structure and functional connectivity, even the coupling relationship between them contributed to the depressive pathogenesis. Meanwhile, the chronic negative stress may participate in the mechanism of the present results. There was a study that found three weeks of chronic restraint stress induced the changes in the density of dendritic spine shape subtypes in both CA1 and CA3 apical dendrites, suggesting a prolonged stressful challenge affected intrahippocampal connectivity.60 Another study in chick’s hippocampal complex indicated the different stressful conditions may have different effects on hippocampus: the neurons undergo structural modifications when the stress achieved to a certain level; and repeated exposure to chronic stress lead to the neuronal structural disruption by retraction in the dendritic and axonal length, and decreasing in dendritic spines induced less synaptic connections.61 So based on this evidence, we could speculate the chronic negative stress may also cause the disruption of microstructure of hippocampus and the subregions which may be the underlying mechanisms for differences of hippocampal volumes and functional connectivity in depressive patients. Certainly, there may be more complex pathologic processes for the depressive patients who underwent chronic negative stress. The research also supported atrophy of neurons and degradation of signal integrity in cortical and hippocampal regions implicated in depression induced by chronic stress related to elevated adrenal glucocorticoids and inflammatory cytokines as well as other factors.62 We only illustrated the depressive disorder underwent chronic negative stress presented the differences in hippocampal volumes and functional connectivity, and prompted it may be the potential subtype in depressive disorder. However, the underlying mechanism needs further exploring from both microscopic and molecular perspectives.
Our study had several limitations. First, it was a cross-sectional study that only presented the relationship among chronic negative stress, hippocampus and depressive disorder, but could not ascertain the causality. Second, because of the difficulty of enrolling subjects, we failed to include the healthy controls who underwent chronic negative stress, and the number of subjects with suicide behaviour, psychotic symptoms, or positive family history was too small, we could not discuss the impact level of chronic negative stress on depression and its clinical features. Third, for the stress types, we focused on the chronic negative stress rather than early life stress, maybe we could explore the characteristic or additive effects of different types of stress next. Fourth, we analyzed the FCs with hippocampus as the seed, maybe we could investigate the FCs changes with other brain regions as seed in larger scale. In addition, a study presented the relationship among depression, lifestyle factors and the brain structures of depressive patients did not change after following up with 9 years,63 which supported the course of the depressive disorder may have no impact on the brain structures to some extent. But it still cannot explain the course or other clinical features have no effects on hippocampal structures and functional connectivity, which remains to be considered in future study.
Conclusion
Our findings offer preliminary evidence for impact of chronic negative stress on the hippocampal structures and functional connectivity in adults with depressive disorder diagnosis.
Ethics Statement
This study had been approved by the Clinical Research Ethics Committee of Hebei Provincial Mental Health Center, China (NO.202213). Informed written consent was obtained from all the participants after detailed understanding of the research. It was compliant with the guidelines outlined in the Declaration of Helsinki.
Acknowledgments
This study was supported by Natural Science Foundation of China (No. 81960258, 2019), Natural Science Foundation of Xinjiang Uygur Autonomous Region (No.2022D01D64) and Excellent Talents Subsidized Project of Hebei Province, China (No.ZF2023219). Authors appreciate Dr. Xiangxin Liu and Dr. Wei Cui for valuable discussion on research protocol and Ms. Yiming Zhao for improving the language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hasin DS, Sarvet AL, Meyers JL, et al. Epidemiology of adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry. 2018;75(4):336–346. doi:10.1001/jamapsychiatry.2017.4602
2. Abbafati C, Abbas KM, Abbasi-Kangevari M, et al.; GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. 2020;396:1204–1222.
3. Thanacoody HK, Thomas SH. Tricyclic antidepressant poisoning: cardiovascular toxicity. Toxicol Rev. 2005;24(3):205–214. doi:10.2165/00139709-200524030-00013
4. Trivedi MH, Rush AJ, Wisniewski SR, et al.; STAR*D Study Team. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry. 2006;163(1):28–40. doi:10.1176/appi.ajp.163.1.28
5. David DJ, Gourion D. Antidepressant and tolerance: determinants and management of major side effects. Encephale. 2016;42(6):553–561. doi:10.1016/j.encep.2016.05.006
6. Hammen C. Stress and depression. Annu Rev Clin Psychol. 2005;1(1):293–319. doi:10.1146/annurev.clinpsy.1.102803.143938
7. Dai W, Feng K, Sun X, et al. Natural products for the treatment of stress-induced depression: pharmacology, mechanism and traditional use. J Ethnopharmacol. 2022;285:114692. doi:10.1016/j.jep.2021.114692
8. Xiaohua L, Jiang K. The overview for relationship between life stress and depressive disorder. Chin J Behav Med Sci. 2004;13:347–348.
9. Zhang H, Li S, Du Q, et al. Relationships between childhood abuse, personality and stress of life events in Chinese Han depressed people. Chin J Clinicians. 2017;11:535–538.
10. Erving CL. The effect of stress exposure on depressive symptoms and major depressive episode among US Afro-Caribbean women. Soc Psychiatry Psychiatr Epidemiol. 2021;56(12):2227–2238. doi:10.1007/s00127-021-02096-8
11. Chen XY, Wang D, Scherffius A, et al. Comorbid trajectories of posttraumatic stress disorder symptoms and depressive symptoms in a 10-year cohort of Chinese Wenchuan earthquake survivors: course, predictors, and consequences. Psychol Trauma. 2023. doi:10.1037/tra0001619
12. Maes M, Almulla AF. Research and Diagnostic Algorithmic Rules (RADAR) and RADAR plots for the first episode of major depressive disorder: effects of childhood and recent adverse experiences on suicidal behaviors, neurocognition and phenome features. Brain Sci. 2023;13(5):714. doi:10.3390/brainsci13050714
13. Strange BA, Witter MP, Lein ES, et al. Functional organization of the hippocampal longitudinal axis. Nat Rev Neurosci. 2014;15(10):655–669. doi:10.1038/nrn3785
14. Monereo-Sánchez J, Jansen JFA, van Boxtel MPJ, et al. Association of hippocampal subfield volumes with prevalence, course and incidence of depressive symptoms: the Maastricht study. Br J Psychiatry. 2024;224(2):66–73. doi:10.1192/bjp.2023.143
15. Shengli C, Yingli Z, Zheng G, et al. An aberrant hippocampal subregional network, rather than structure, characterizes major depressive disorder. J Affect Disord. 2022;302:123–130. doi:10.1016/j.jad.2022.01.087
16. Fan J, Gao F, Wang X, et al. Right amygdala-right precuneus connectivity is associated with childhood trauma in major depression patients and healthy controls. Soc Cogn Affect Neurosci. 2023;18(1):nsac064. doi:10.1093/scan/nsac064
17. Zhang F, Wang C, Lan X, et al. Ketamine-induced hippocampal functional connectivity alterations associated with clinical remission in major depression. J Affect Disord. 2023;325:534–541. doi:10.1016/j.jad.2023.01.003
18. Kuhn HG, Toda T, Gage FH. Adult hippocampal neurogenesis: a coming-of-age story. J Neurosci. 2018;38(49):10401–10410. doi:10.1523/JNEUROSCI.2144-18.2018
19. Snyder JS, Soumier A, Brewer M, et al. Adult hippocampal neurogenesis buffers stress responses and depressive behaviour. Nature. 2011;476(7361):458–461. doi:10.1038/nature10287
20. Wu Z, Xiao L, Wang H, et al. Neurogenic hypothesis of positive psychology in stress-induced depression: adult hippocampal neurogenesis, neuroinflammation, and stress resilience. Int Immunopharmacol. 2021;97:107653. doi:10.1016/j.intimp.2021.107653
21. Jones KL, Zhou M, Jhaveri DJ. Dissecting the role of adult hippocampal neurogenesis towards resilience versus susceptibility to stress-related mood disorders. NPJ Sci Learn. 2022;7(1):16. doi:10.1038/s41539-022-00133-y
22. Schoenfeld TJ, McCausland HC, Morris HD, et al. Stress and loss of adult neurogenesis differentially reduce hippocampal volume. Biol Psychiatry. 2017;82(12):914–923. doi:10.1016/j.biopsych.2017.05.013
23. Huang CX, Xiao Q, Zhang L, et al. Stress-induced myelin damage in the hippocampal formation in a rat model of depression. J Psychiatr Res. 2022;155:401–409. doi:10.1016/j.jpsychires.2022.09.025
24. Brake AD, Yang X, Lee CY, et al. Reduced hippocampal volume and neurochemical response to adult stress exposure in a female mouse model of urogenital hypersensitivity. Front Pain Res. 2022;3:809944. doi:10.3389/fpain.2022.809944
25. Alemu JL, Elberling F, Azam B, et al. Electroconvulsive treatment prevents chronic restraint stress-induced atrophy of the hippocampal formation-A stereological study. Brain Behav. 2019;9(2):e01195. doi:10.1002/brb3.1195
26. Brosch K, Stein F, Schmitt S, et al. Reduced hippocampal gray matter volume is a common feature of patients with major depression, bipolar disorder, and schizophrenia spectrum disorders. Mol Psychiatry. 2022;27(10):4234–4243. doi:10.1038/s41380-022-01687-4
27. Binnewies J, Nawijn L, Brandmaier AM, et al. Associations of depression and regional brain structure across the adult lifespan: pooled analyses of six population-based and two clinical cohort studies in the European Lifebrain consortium. Neuroimage Clin. 2022;36:103180. doi:10.1016/j.nicl.2022.103180
28. Alper J, Feng R, Verma G, et al. Stress-related reduction of hippocampal subfield volumes in major depressive disorder: a 7-Tesla study. Front Psychiatry. 2023;14:1060770. doi:10.3389/fpsyt.2023.1060770
29. Zhang Y, Yang D. Life events scale. Chin Mental Health J. 1999;(S1):101–108.
30. Li N, Li Y, Wang C, et al. Relationship between chronic stress and neuroimaging and prognosis in patients with depression. J Mol Imaging. 2022;45:599–603.
31. Zeng X, Fu P, Lin X, et al. Effects of 5-hydroxytryptamine, c-Fos protein and chronic psychological stress on negative emotion in individuals from ethnic minority areas. Guang Xi Med J. 2019;41:2426–2429,2439.
32. Yang B, Xiaohong L, Sujian R, et al. Coronary heart disease, depression and chronic stress. J Hubei Univ Chin Med. 2019;21:54–57.
33. Wang C, Xu L, Wang X, et al. Comparative analysis of sleep structure in depression patients with different dimensions of chronic stress. J Neurosci Mental Health. 2022;22:479–486.
34. Li X, Phillips M, Zhang Y. The study on the validity of a suicide-specific life event scale and suicidal behavior. Chin J Nerv Ment Dis. 2008;34:156–160.
35. Iglesias JE, Augustinack JC, Nguyen K, et al.; Alzheimer’s Disease Neuroimaging Initiative. A computational atlas of the hippocampal formation using ex vivo, ultra-high resolution MRI: application to adaptive segmentation of in vivo MR. Neuroimage. 115;2015:117–137. doi:10.1016/j.neuroimage.2015.04.042
36. Swaab DF, Bao AM. Sex differences in stress-related disorders: major depressive disorder, bipolar disorder, and posttraumatic stress disorder. Handb Clin Neurol. 2020;175:335–358.
37. Wen L, Zhongxiang C, Yu Yunyan X, et al. Correlation between childhood trauma and family rearing patterns in patients with depression. Neural Inj Funct Reconstr. 2022;17:668–671.
38. Sanwald S, Widenhorn-Müller K, Schönfeldt-Lecuona C, et al. Factors related to age at depression onset: the role of SLC6A4 methylation, sex, exposure to stressful life events and personality in a sample of inpatients suffering from major depression. BMC Psychiatry. 2021;21(1):167. doi:10.1186/s12888-021-03166-6
39. Goldstein BL, Kessel EM, Kujawa A, et al. Stressful life events moderate the effect of neural reward responsiveness in childhood on depressive symptoms in adolescence. Psychol Med. 2020;50(9):1548–1555. doi:10.1017/S0033291719001557
40. Linnstaedt SD, Zannas AS, McLean SA, et al. Literature review and methodological considerations for understanding circulating risk biomarkers following trauma exposure. Mol Psychiatry. 2020;25(9):1986–1999. doi:10.1038/s41380-019-0636-5
41. Nolan M, Roman E, Nasa A, et al. Hippocampal and amygdalar volume changes in major depressive disorder: a targeted review and focus on stress. Chronic Stress. 2020;4:2470547020944553. doi:10.1177/2470547020944553
42. Shen X, Reus LM, Cox SR, et al. Subcortical volume and white matter integrity abnormalities in major depressive disorder: findings from UK Biobank imaging data. Sci Rep. 2017;7(1):5547. doi:10.1038/s41598-017-05507-6
43. Ancelin ML, Carrière I, Artero S, et al. Lifetime major depression and grey-matter volume. J Psychiatry Neurosci. 2019;44(1):45–53. doi:10.1503/jpn.180026
44. Mikolas P, Tozzi L, Doolin K, et al. Effects of early life adversity and FKBP5 genotype on hippocampal subfields volume in major depression. J Affect Disord. 2019;252:152–159. doi:10.1016/j.jad.2019.04.054
45. Twait EL, Blom K, Koek HL, et al.; UCC SMART Study Group. Psychosocial factors and hippocampal subfields: the Medea-7T study. Hum Brain Mapp. 2023;44(5):1964–1984. doi:10.1002/hbm.26185
46. Li ZR, Han YS, Liu Z, et al. GR/NF-κB signaling pathway regulates hippocampal inflammatory responses in diabetic rats with chronic unpredictable mild stress. Eur J Pharmacol. 2021;895:173861. doi:10.1016/j.ejphar.2021.173861
47. Zheng X, Cheng Y, Chen Y, et al. Ferulic acid improves depressive-like behavior in prenatally-stressed offspring rats via anti-inflammatory activity and HPA axis. Int J Mol Sci. 2019;20(3):493. doi:10.3390/ijms20030493
48. Saxbe D, Khoddam H, Piero LD, et al. Community violence exposure in early adolescence: longitudinal associations with hippocampal and amygdala volume and resting state connectivity. Dev Sci. 2018;21(6):e12686. doi:10.1111/desc.12686
49. McDermott K, Ren P, Lin F. The mediating role of hippocampal networks on stress regulation in amnestic mild cognitive impairment. Neurobiol Stress. 2019;10:100162. doi:10.1016/j.ynstr.2019.100162
50. Seewoo BJ, Hennessy LA, Feindel KW, et al. Validation of chronic restraint stress model in young adult rats for the study of depression using longitudinal multimodal MR imaging. eNeuro. 2020;7(4):
51. Wu Y, Zheng Y, Li J, et al. Subregion-specific, modality-dependent and timescale- sensitive hippocampal connectivity alterations in patients with first-episode, drug-naïve major depression disorder. J Affect Disord. 2022;305:159–172. doi:10.1016/j.jad.2022.02.052
52. Čermaková P, Andrýsková L, Brázdil M, et al. Socioeconomic deprivation in early life and symptoms of depression and anxiety in young adulthood: mediating role of hippocampal connectivity. Psychol Med. 2022;52(13):2671–2680. doi:10.1017/S0033291720004754
53. Feng R, Bao W, Zhuo L, et al. Family conflict associated with intrinsic hippocampal-OFC connectivity in adolescent depressive disorder. Front Psychiatry. 2022;12:797898. doi:10.3389/fpsyt.2021.797898
54. Hendrix CL, Srinivasan H, Feliciano I, et al. Hippocampal connectivity shows dissociable associations with maternal cortisol and self-reported distress during pregnancy. Life. 2022;12(7):943. doi:10.3390/life12070943
55. Chen J, Wei Z, Han H, et al. An effect of chronic stress on prospective memory via alteration of resting-state hippocampal subregion functional connectivity. Sci Rep. 2019;9(1):19698. doi:10.1038/s41598-019-56111-9
56. Qi R, Luo Y, Zhang L, et al. Decreased functional connectivity of hippocampal subregions and methylation of the NR3C1 gene in Han Chinese adults who lost their only child. Psychol Med. 2021;51(8):1310–1319. doi:10.1017/S0033291720000045
57. Leaver AM, Vasavada M, Kubicki A, et al. Hippocampal subregions and networks linked with antidepressant response to electroconvulsive therapy. Mol Psychiatry. 2021;26(8):4288–4299. doi:10.1038/s41380-020-0666-z
58. Wu B, Zhang X, Xie H, et al. Disrupted structural brain networks and structural-functional decoupling in first-episode drug-naïve adolescent major depressive disorder. J Adolesc Health. 2024;74(5):941–949. PMID:38416102. doi:10.1016/j.jadohealth.2024.01.015
59. Leonards CA, Harrison BJ, Jamieson AJ, et al. Altered task-related decoupling of the rostral anterior cingulate cortex in depression. Neuroimage Clin. 2024;41:103564. doi:10.1016/j.nicl.2024.103564
60. Magariños AM, Li CJ, Gal Toth J, et al. Effect of brain-derived neurotrophic factor haploinsufficiency on stress-induced remodeling of hippocampal neurons. Hippocampus. 2011;21(3):253–264. doi:10.1002/hipo.20744
61. Arya H, Tamta K, Kumar A, et al. Unpredictable chronic mild stress shows neuronal remodeling in multipolar projection neurons of hippocampal complex in postnatal chicks. Anat Sci Int. 2024. PMID:38448780. doi:10.1007/s12565-024-00758-6
62. Duman RS, Sanacora G, Krystal JH. Altered connectivity in depression: GABA and glutamate neurotransmitter deficits and reversal by novel treatments. Neuron. 2019;102(1):75–90. doi:10.1016/j.neuron.2019.03.013
63. Binnewies J, Nawijn L, van Tol MJ, et al. Associations between depression, lifestyle and brain structure: a longitudinal MRI study. Neuroimage. 2021;231:117834. doi:10.1016/j.neuroimage.2021.117834
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.