Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 12
Alternative Method for Full Oral Rehabilitation in Patients with Pycnodysostosis Syndrome: A Case Report
Authors Costa MM, Pennisi PRC ![]() , Oliveira ACZM
, Oliveira ACZM ![]() , Oliveira JEC, Oliveira GV
, Oliveira JEC, Oliveira GV ![]() , Moffa EB
, Moffa EB ![]() , Paranhos LR
, Paranhos LR
Received 29 January 2020
Accepted for publication 17 March 2020
Published 15 April 2020 Volume 2020:12 Pages 131—139
DOI https://doi.org/10.2147/CCIDE.S247614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Márcio Magno Costa,1 Pedro Rogério Camargos Pennisi,1 Andréa Cristina Zacarias Martins de Oliveira,2 João Edson Carmo de Oliveira,1 Gustavo Vilela Oliveira,3 Eduardo Buozi Moffa,4 Luiz Renato Paranhos1
1Federal University of Uberlândia, School of Dentistry, Uberlândia, MG, Brazil; 2Private Clinic, Uberlândia, Brazil; 3Federal University of Uberlândia, School of Mechanical Engineering, Uberlândia, MG, Brazil; 4University Center - UNIFAE, School of Dentistry, São João da Boa Vista, SP, Brazil
Correspondence: Luiz Renato Paranhos
Federal University of Uberlândia, Uberlândia, MG, Brazil
Tel +55 34 32258145
Email [email protected]
Abstract: Pycnodysostosis (PYCD) is a rare autosomal recessive skeletal dysplasia arising from a change in the production of the cathepsin K enzyme and it is also known as Maroteaux-Lamy Syndrome. The main changes in the buccal and maxillofacial region are modifications of the facial bones (leading to the loss of the mandibular angle due to micrognathia), deep palate, premature and/or delayed tooth eruption, hypopneumatization of the maxillary sinuses, chin hypoplasia, hypercementosis, enamel hypoplasia, hyperdontia, incomplete dentin calcification, root hypoplasia, pulp chamber obliteration, and increased free functional space. This paper aims to report a case of a patient with PYCD, in which are highlighted the oral manifestations of this syndrome and present an option of oral rehabilitative treatment through a removable overdenture made on natural tooth of the patient. The technique of dental coating through overdenture is a simple, viable and conservative alternative for oral rehabilitation of patients with large maxillomandibular discrepancies, as in cases of pycnodysostosis, especially in the presence of increased free space – characteristic of patients with this syndrome. The result was quite satisfactory both aesthetically and functionally and provided a better life quality for the patient.
Keywords: malocclusion, pycnodysostosis, oral rehabilitation
Introduction
Pycnodysostosis (PYCD), also known as Maroteaux-Lamy Syndrome, was described for the first time by Maroteaux and Lamy, in 1962.1 It is a congenital malformation of the hard tissues, rare and with autosomal recessive inheritance, arising from a defect in the gene encoding of the cathepsin K enzyme,2 in addition the gene responsible for the disease is located in the chromosome 1q21.3 Genetic and biochemical procedures have been used to achieve a more specific diagnostic in the field of the bone dysplasia’s, however, the clinical and radiological features still are considered the main bases of the diagnostic. The inaccuracy in the diagnosis may underestimate the prevalence of the disease and osteoporosis is one of the confounding factors.4
The prevalence of PYCD is 1.7/1,000,000 and the disease can reach both genders without distinction, being reported parental consanguinity in approximately 30% cases.5–9 The most common clinical and radiographic manifestations in PYCD includes low height10 and narrowing of the medullary cavity of the long bones associated with other anomalies, which is related to the increase of the bone density and fragility.11 In regard to the craniofacial changes it is common to find late eruption of permanent molars, arched and narrow palate,11 change of the format and positioning of the teeth, such as: malformation, malocclusion and dental crowding,11 in addition to presence of micrognathia, bone fragility, with the possibility of pathological bone fractures and, yet, frontal bossae, exophthalmos and bluish sclerotics.10 The described orofacial changes increase the morbidity of the disease.12 Osteomyelitis is the greater complication arising from oral problems, being common in adults with PYCD, but unusual in children.13
The presence of facial changes such as anterior teeth deformations, bone changes in the facial development, among others, cause an aesthetic impact that has been a direct impact in the life quality of the patient.14 It is well known that changes of any kind in format, color and function can be direct predisposing situations for bullying in people’s lives.15 The changes caused by the syndrome impact negatively in the patient wellbeing.16
The approach for treatment of PYCD is, especially, focused on symptoms, with emphasis on prevention of fractures. Rigorous daily oral cleanliness and antibiotic prophylaxis in extraction cases are the procedures recommended to prevent osteomyelitis.5 The literature is scarce regarding to the oral rehabilitation treatment. Osteogenic distraction has been reported as a possible way to correct the maxillo-mandibular discrepancies presented by patients with the syndrome.17 As the presence of orofacial alterations in the patients with PYCD brings functional and aesthetic disorders due to the inadequate dental positioning and discrepancy between the dental arches, this case report presents an innovative treatment through a removable overdenture made on remaining teeth to provide an appropriate support to the oral structures and a favorable dental occlusion in a patient with PYCD.
Case Report
Ethics Approval and Consent to Participate
This case was conducted according to the Helsinki Statement, and the patient provided informed written consent prior to all interventions according to the requirements of the intuitional review board of the Faculty of Dentistry, Federal University of Uberlândia. Informed written consent for publication was obtained from the patient.
The case report was prepared according to the CARE guidelines.18
Patient Information
Male patient, 30 years, went to a clinic school for dental treatment. During the anamnesis, it was found that he was a patient with PYCD. The diagnosis of PYCD was made in 2003 by a multi-professional team composed by orthopedist, endocrinologist and geneticist. The patient did not undergo genetic tests. As for family history, two other cousins have the same syndrome.
The main concerns of the patient in the moment of the first attendance was the the difficulty to chew and the aesthetic aspect. He claims that his social and family life was relatively normal.
Clinical Findings
The clinical and radiological frame was characteristic. In the physical examination, it was possible to note low height (Figure 1), hooked nose, prominent, exophthalmos and loss of the vertical dimension. The phalanges of the altered hands (Figure 2A) characterize the syndrome, the same way as changes in long bones (Figure 2B). The X-rays confirm the characteristics of mandibular hypoplasia with loss of mandible angle (Figure 3), abnormal dentition and craniofacial disproportion (Figure 4). In the intraoral clinical examination, it was detected an absence of occlusal stability (Figure 5), increase of the free functional space, inadequate dental positioning, atypical and arched palate with fibrous tissue development typical of the syndrome. In Table 1, the brief of the patient’s clinical characteristics can be noted.
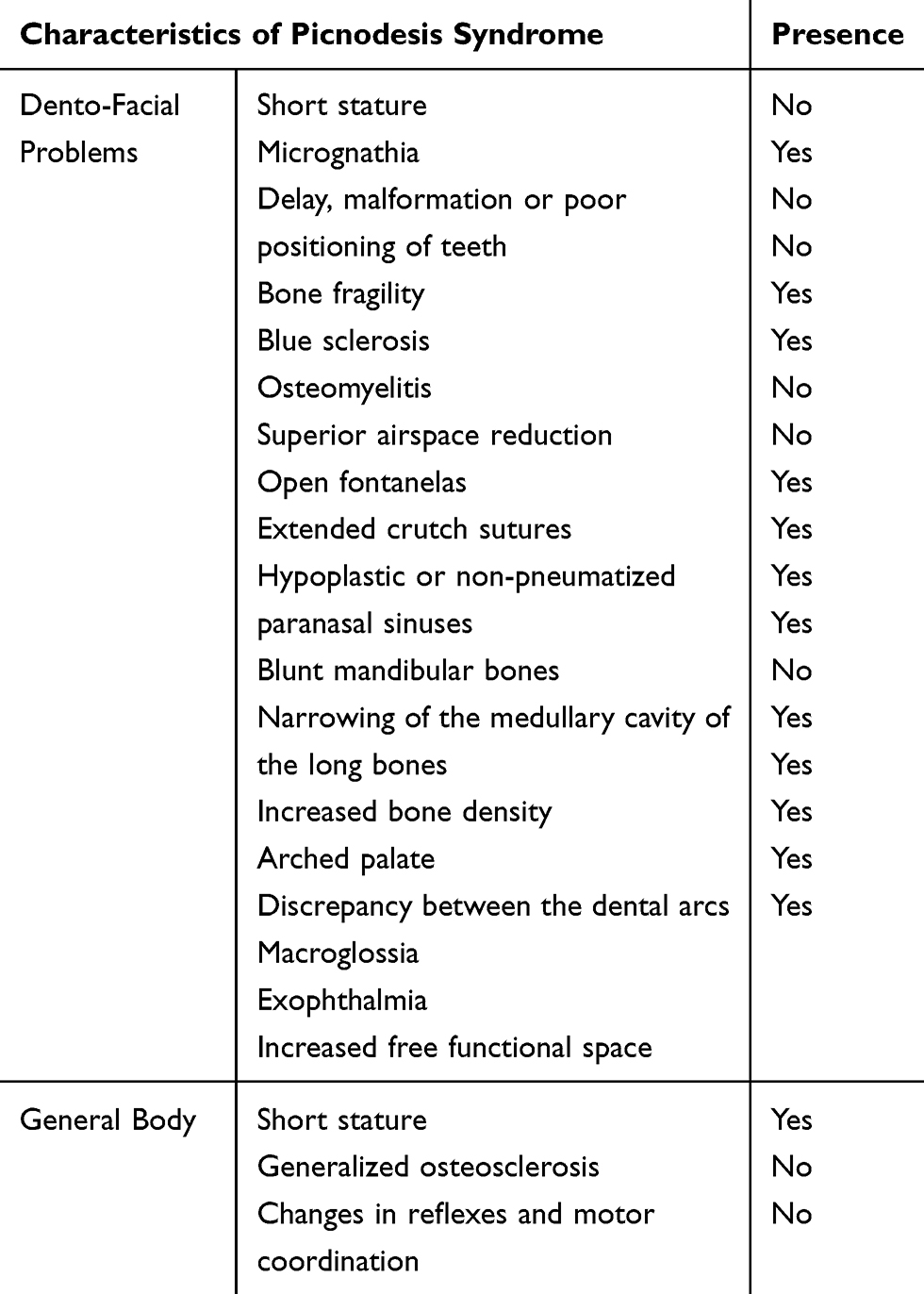 |
Table 1 Physical Characteristics Related to Pyicnodysostosis Syndrome, Described in the Literature. The Table Demonstrates the Presence or Absence of Such Characteristics in the Reported Individual |
 |
Figure 1 Body aspect (A), frontal aspect (B) and lateral aspect (C) of the patient. |
 |
Figure 2 Radiological aspects of patient’s hand (A) and humerus and radius (B). |
 |
Figure 3 Initial panoramic radiograph. |
 |
Figure 4 Initial lateral cephalogram. |
 |
Figure 5 Initial intraoral photographs. (A) Right side view; (B) front view; (C) left side view. |
In the maxillary dental arch, the remaining teeth were preserved, requiring only non-surgical periodontal treatment. In the mandibular dental arch, the remaining teeth were crowded, with inclinations and rotations, but without mobility or probing depth to justify their extractions. (Figure 6).
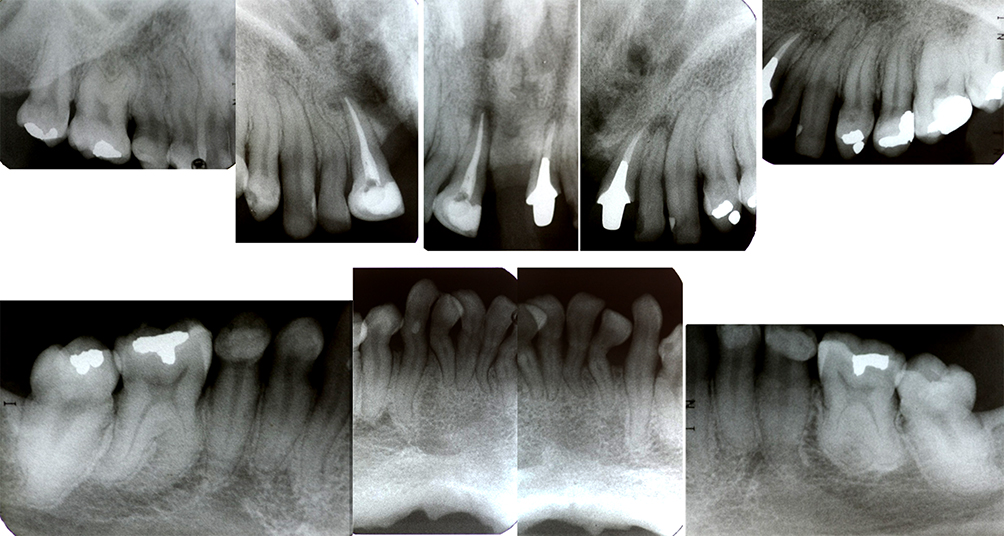 |
Figure 6 Full-mouth periapical X-ray. |
Timeline
Previously, the patient had already undergone by orthodontic treatment and has been submitted to a surgical maxillary expansion, where was not achieved the occlusal stability. With the previous treatment, it was also not possible to decrease the mandibular maxillary discrepancies.
In March 2008, it was made the first prosthesis on teeth present. In 2017, it was made the second prosthesis to the patient, also overdenture, however with the use of additional retention O-ring.
Therapeutic Intervention
The initial treatment proposed was non-surgical periodontal. To decrease the maxillary and mandible discrepancies and adjust the occlusion, a superior removable full overdenture was made over the remaining teeth. In the lower teeth, it was made a selective wear and later was made a reanatomization with composite resin.
Initially, an irreversible hydrocolloid impression was made to obtain the study casts (Figure 7A) and, these were duly assembled in semi-adjustable articulator. The analysis of the casts assembled in a vertical occlusion dimension previously restored through phonetic and metric tests19 allowed the planning of a full removable overdenture with dental cover, from verification of the interocclusal spaces obtained (Figure 7B and C).
 |
Figure 7 Initial impressions with a custom tray (A). Base plaque and wax guide plane performed over the patient teeth (B). Maxillomandibular records (C). |
About the superior study cast, after to make the delimitation of the basal area and to do the relief in wax, it was made the individual tray that allowed the production of the secondary or functional impression, using a polyether-based elastomer (Impregum® Soft, 3M ESPE AG/ESPE Platz, Seefeld, Germany).
After obtaining the superior test base, reanatomizations were performed on the lower teeth, mimicking the aesthetic and conventional standard desired by the patient (Figure 8). Subsequently, the maxillomandibular record was made, in which was obtained the correct vertical occlusal dimension (by the metric and phonetic method), appropriate support for the lip and cheek, reconstituting the facial physiognomy and harmony.
 |
Figure 8 Reanatomization of lower incisors with composite resin. (A) Isolation with a rubber dam; (B) details of the isolation; (C) clinical aspects after the reanatomization. |
The maxillomandibular record enabled to assemble the working models in a semi-adjustable articulator and the assembly the artificial teeth that were selected for the patient. After their assembly, these were tried and adjusted to establish the most satisfactory occlusion possible and a pleasant aesthetic.
When finished the processing of the prosthesis base, this was installed and adjusted and the recommendations on oral hygiene were very emphasized since the teeth covered by the prosthesis would be more prone to the development of caries and periodontal disease. Posterior controls were made until the prosthesis was properly adapted to the oral structures. Immediately after the subsequent controls, the patient underwent surgeries for nasal correction and rhinoplasty and otoplasty for improvement of the facial aesthetics. In the Figure 9, it is possible to note a clinical perspective after prosthesis installation.
 |
Figure 9 Final aspect of the first denture place over the teeth. (A) Right side view; (B) front view; (C) left side view. |
The patient returned annually for controls and maintenance. Eight years after installation, the denture was replaced due to aesthetic deficiencies and even retention and stability associated with the long period of use.
For the construction of the new denture, we decided to increase its retention and stability through O-ring attachments positioned on the first molars bilaterally and between the two upper central incisors. We have flatted the vestibular of the anterior and posterior upper teeth, to reduce the need for internal PT relief and improving its insertion axis. In this way, the risk of tipping occurred in the first license with its daily use was reduced. For this, metal crowns were made on teeth 16, 26 and metalloceramics were made on teeth 11 and 12. The male components of the O-rings were positioned on the molar crowns (Figure 10), as well as between the crowns of the elements 11 and 12, which were splinted. In the base of the prosthesis were placed the female components of the O-rings.
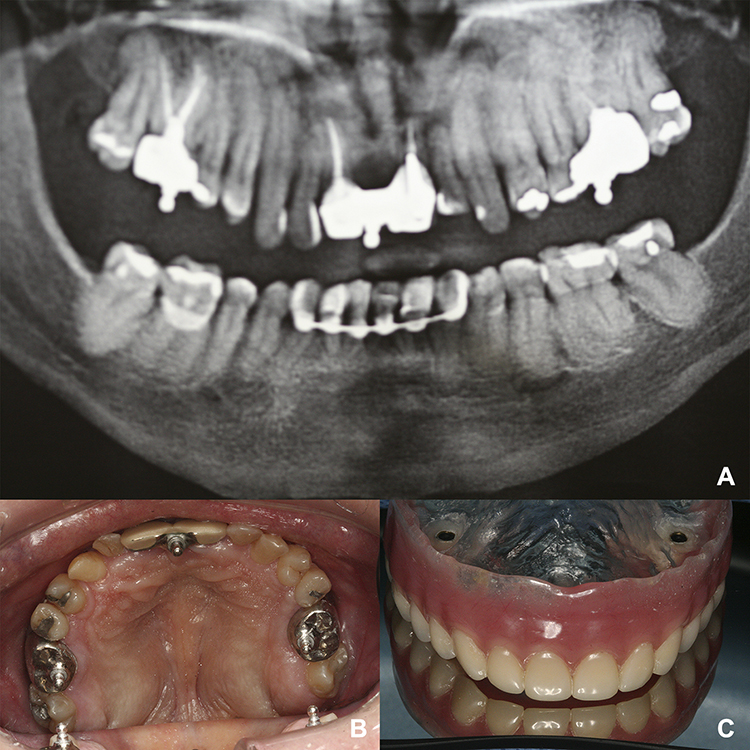 |
Figure 10 Panoramic radiograph after the O-rings installation (A). Occlusal view of the tree O-rings installed (B). Inner surface of the denture with the attachments placed on position (C). |
The clinical and laboratory sequence of construction of the new prosthesis was basically the same used for the construction of the first prosthesis, described previously. However, the use of the attachments provided a very significant improvement in the retention and stability of the new complete upper denture, providing more comfort and confidence for the patient. After the installation, all controls were made until the patient was fully comfortable with the denture (Figure 11). As the lower anterior teeth had short and anatomically irregular roots, they were splinted to ensure longer longevity. The results were quite satisfactory both functionally as aesthetically (Figure 12).
 |
Figure 11 Frontal and lateral aspects of the patient before (A and B) and after (C and D) the rehabilitation procedure. |
 |
Figure 12 Final aspect of the patient with an improvement of esthetic appearance achieved with minimally invasive prosthetic approach. |
Follow-Up and Outcomes
After 10 years of use of the overdentures, the remaining structures are preserved, and the prosthesis is in excellent conservation condition.
In the last follow-up the patient told about how the treatment change his life:
The corrective treatment was a divider in my life, I can say that it was transformative. There was a considerable gain in self-esteem and a huge change in the functional aspect.
Discussion
Pycnodysostosis is a syndrome characterized by severe bone sclerosis,20 cranial suture opening, loss of the mandible angle,21 defects in the phalanges of the hands and feet and a predisposition to the bone fractures due to the deformities in the long bone.22 The patients with PYCD can present systemic23 and visceral manifestations, such as hepatosplenomegaly, anemia and rickets with radiological signs.24 Osteopetrosis should be considered in the differential diagnosis, because in childhood, the classical osteopetrosis is diagnosed by an increase of density in the long bones, progressive anemia, hepatosplenomegaly, and neurological disorders. However, the dysplasia in the distal portions of the phalanges and clavicles is absent.25
In a study24 conducted with 73 cases of pycnodysostosis, the following oral and maxillofacial such as development of facial bone disorders (loss of the mandibular angle), arched atypical palate, delay in tooth eruption, dental malposition and macroglossia were found. In this report, besides the changes described, it was detected ankylosis in the remaining teeth and also with sagittal discrepancy between the maxilla and mandible, with mandibular prognathism.
The treatment of syndromic patients is focused on correction of the symptoms. In 2017, Aghili et al17 described the improvement of facial aesthetic conditions, in their work it was shown the use of osteogenic distraction technique to promote a maxillary advancement, and, thus, improve the lip support, obtaining a more harmonious profile for patient. Despite the aesthetic improvement, the technique did not promote an appropriate relationship between the antagonistic occlusal surfaces. The overdenture technique described in this paper covers both aesthetics as the function, once provided appropriate support to lip and cheek and promotes an occlusal rearrangement, which improves the masticatory efficiency of the patients with this syndrome.
The dental coating with overdenture only was possible due to these patients present an increased big free space.11 In addition, patients rehabilitated in this way should have strict guidelines to prevent problems, such as periodontal disease and caries. These morbidities can arise damaging and reducing the durability of the rehabilitating process.
Restore the aesthetics and function is a key part of the improvement of the patient`s life quality. The current standard of dental aesthetics permeates the good anatomy of the dental elements with size, format and contour. The overdenture rehabilitation re-established the vertical dimension and the superior teeth aesthetics. The reanatomization of the inferior elements contributed to finalize the improvement in the patient’s look. The ability to socialize normally, to eat better,25 and to speak properly represent an incalculable increase in the life quality of the patients with PYCD. Thus, the rehabilitation process was not aimed only to reestablish the occlusion, aesthetics and function of the patient, but to improve his/her life quality.26
Conclusion
The technique of dental coating through overdenture proved to be a simple, viable and conservative alternative for oral rehabilitation of the patient at issue. It can be indicated for patients that present maxillo-mandibular discrepancies, like the patients with Pycnodysostosis, especially due to these patients present free functional space increased. The result was quite satisfactory both aesthetically as functionally.
The indication of the described technique should be conditioned to a strict control of the hygiene by patients, since the natural teeth covered by the prosthesis will be more prone to caries and periodontal diseases.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Marouteaux P, Lamy M. The malady of toulouse-lautrec. JAMA. 1995;191(3):715–717. doi:10.1001/jama.1965.03080090029007
2. Bitu C, Kaupilla J, Teppo S, Vilen S. Expression of cysteine protease cathepsin K by oral tongue SCCs in vivo and in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(4):109–110.
3. Gelb BD, Shi GP, Chapman HA, Desnick RJ. Pycnodysostosis, a lysosomal disease caused by cathepsin K deficiency. Curll Mol Med. 2002;2(5):36–38.
4. Araújo TF. As bases moleculares da picnodisostose e análise das distribuições das mutações no estado do Ceará e em outras regiões do Brasil [Masters Dissertation] [The molecular basis of pycnodysostosis and analysis of the distribution of mutations in the state of Ceará and other regions of Brazil]. Campinas; 2016.
5. Quezado R. Picnodisostose: relato de dois casos [Pycnodysostosis: report of two cases]. Arq Bras Endocrinol Metab. 2003;47(1):95–101. doi:10.1590/S0004-27302003000100015
6. Xue Y, Cai T, Shi S, et al. Clinical and animal research findings in pycnodysostosis and gene mutations of cathepsin K from 1996 to 2011. Orphanet J Rare Diseases. 2011;11(2):6–20.
7. Mujawar Q, Naganoor R, Thobbi A, Ukkali S, Malagi N. Pycnodysostosis with unusual findings: a case report. Cases J. 2009;2:6544. doi:10.4076/1757-1626-2-6544
8. Hernández-Alfaro F, Arenaz JB, Serrat MS, Bueno JM. Orthognathic surgery in pycnodysostosis: a case report. Int J Oral Maxillofac Surg. 2011;4(1):110–113. doi:10.1016/j.ijom.2010.07.006
9. Karakurt L, Yilmaz E, Belhan O, Serin E. Pycnodysostosis associated with bilateral congenital pseudoarthrosis of the clavicle. Arch Orthop Trauma Surg. 2003;7(2):125–127. doi:10.1007/s00402-003-0484-1
10. Edelson J, Obad S, Geiger R, On A, Artul H. Pycnodysostosi. Orthopedic aspects with a description of 14 new cases. Clin Orthop Relat Res. 1992;280:263–276.
11. Cui Y. A systematic review of genetic skeletal disorders in chinese biomedical journals between 1978 and 2012. Orphanet J Rare Dis. 2012;22(8):7–55.
12. Stephen T, Robert C, Leslie F. Princípios e Prática de Medicina Oral [Principles and Practice of Oral Medicine].
13. Farias JG. Picnodisostose Associada a Osteomielite da Maxila [Pycnodysostosis Associated with Osteomyelitis of the Maxilla]. Rev Bras CiêncSaúde. 2003;7(2):5.
14. Buss PM. Promoção de saúde e qualidade de vida [Health promotion and quality of life]. Ciência e Saúde Coletiva. 2000;5(1):163–177. doi:10.1590/S1413-81232000000100014
15. Toro GVR, Neves AS, Rezende PCM. Bullying, o exercício da violência no contexto escolar: reflexões sobre um sintoma social [Bullying, the exercise of violence in the school context: reflections on a social symptom]. Pisicologia Teoria e Prática. 2010;12(1):123–137.
16. Neto A, Lopes A. Bullying: comportamento agressivo entre estudantes [Bullying: aggressive behavior among students]. J Pediatr (Rio J). 2005;81(5):164–172. doi:10.2223/JPED.1403
17. Aghili H, Tabataei S, Moghadam M. Clinical radiographic features of pycnodysostosis with emphasis on dentofacial problems. Case Rep Dent. 2017;62:4352485.
18. Gagnier J, Kienle G, Altman D, Moher D, Sox H, Riley D. The CARE guidelines: consensus-based clinical case report guideline development. J Clin Epidemiol. 2014;67(1):38–43. doi:10.1016/j.jclinepi.2013.08.003
19. Igic M. Determination of vertical dimension of occlusion by using the phonetic vowel’O’and’E’. Vojnosanitetski Pregled. 2015;72(2):123–131. doi:10.2298/VSP1502123I
20. Takeuchi K, Tanne K, Fukae S, Sakuda M. Pycnodisostosis: oral and crânio-facial findings of 2 cases. J Osaka Univ Dent School. 1980;20:317–336.
21. Gupta R, Mohan V, Danielson L. Pycnodisostosis. Indian J Radiol. 1988;42:1–13.
22. Koslowski K, Yu S. Pycnodisostosys: a variant form with visceral manifestations. Arch Dis Child. 1972;47(3):804–807. doi:10.1136/adc.47.255.804
23. Santhanakrishnan B, Panneerselvam S, Ramesh S, Panchatcharam M. Pycnodysostosis with visceral manifestation and rickets. Clin Pediatr. 1986;8(2):416–418. doi:10.1177/000992288602500809
24. Sedano H, Gorlin R, Anderson V. Pycnodysostosis: clinical and genetic considerations. Am J Dis Child. 1968;116(7):70–77. doi:10.1001/archpedi.1968.02100020072010
25. Ferreira MC. Cirurgia plástica estética: avaliação dos resultados [Aesthetic plastic surgery: evaluation of results]. Rev Soc Bras Cir Plást. 2000;15(1):61–66.
26. Baxter YO, Ulloa AS. Las Afecciones estéticas: un problema para prevenir [Aesthetic Conditions: a problem for to prevent]. Rev Cubana de Estomatologia. 2001;38(2):83–89.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.