Back to Journals » Infection and Drug Resistance » Volume 13
Altered Brain Function in Young HIV Patients with Syphilis Infection: A Voxel-Wise Degree Centrality Analysis
Authors Zhang XD, Liu GX, Wang XY, Huang XJ, Li JL, Li RL, Li HJ
Received 16 October 2019
Accepted for publication 25 February 2020
Published 11 March 2020 Volume 2020:13 Pages 823—833
DOI https://doi.org/10.2147/IDR.S234913
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Xiao-Dong Zhang,1,2 Guang-Xue Liu,3 Xiao-Yue Wang,2 Xiao-Jie Huang,4 Jing-Li Li,1 Rui-Li Li,2 Hong-Jun Li2
1Department of Radiology, Tianjin First Central Hospital, Tianjin 300192, People’s Republic of China; 2Department of Radiology, Beijing Youan Hospital, Capital Medical University, Beijing 100069, People’s Republic of China; 3Department of Natural Medicines, School of Pharmaceutical Sciences, Peking University Health Science Center, Beijing 100191, People’s Republic of China; 4Center for Infectious Diseases, Beijing Youan Hospital, Capital Medical University, Beijing 100069, People’s Republic of China
Correspondence: Rui-Li Li; Hong-Jun Li
Department of Radiology, Beijing Youan Hospital, Capital Medical University, No. 8, Xi Tou Tiao, Youanmen Wai, Fengtai District, Beijing 100069, People’s Republic of China
Tel +86 010 83997337
Fax +86 010 63051182
Email [email protected]; [email protected]
Objective: This study assessed the possible effect of syphilis co-infection in the brain function in young HIV patients by using voxel-wise degree centrality (DC) analysis.
Methods: Forty-four syphilis-co-infected HIV patients (HIV+/syphilis+), 45 HIV patients without syphilis history (HIV+/syphilis-) and 43 matched healthy controls (HC) underwent resting-state fMRI examinations. Laboratory tests and a battery of neuropsychological tests were performed before each MRI examination. One-way ANOVA was used to compare the differences of DC among the three groups. The correlations between MRI metrics and laboratory/neuropsychological tests in each patient’s group were performed by Pearson correlation analysis.
Results: Compared with HIV+/syphilis-, worse performance in complex motor skills was found in HIV+/syphilis+. Compared with HC, HIV+/syphilis+ and HIV+/syphilis- groups showed attenuated DC in the right orbital frontal cortex and increased DC in the left parietal/temporal cortex. Besides, we also found increased DC in the left inferior frontal cortex and bilateral posterior cingulated cortex/precuneus in HIV+/syphilis+ compared with HC. Moreover, compared with HIV+/syphilis-, HIV+/syphilis+ displayed decreased DC in the left middle occipital cortex. Additionally, in HIV+/syphilis+ group, the mean z value of DC was correlated to the CD4+ cell counts and the learning and delayed recall score.
Conclusion: Syphilis co-infection might be related to more brain functional reorganization in young HIV patients which could be reflected by DC value.
Keywords: syphilis, HIV, functional connectivity, fMRI, brain
Introduction
The reemerging syphilis in high-risk HIV infected individuals became more prominent in recent years, especially in homosexual men, despite the overall prevalence of syphilis remarkably decreased due to widespread use of penicillin.1 Treponema pallidum, the responsible organism for syphilis is highly neuroinvasive2 and could invade the CNS at the primary stage of infection.3,4 Central nervous system (CNS) invasions of Treponema pallidum can be related to meningeal, vascular or parenchymal sites.1 If the immune system is not able to eliminate the infection in time, progression to neurosyphilis might happen, which is more common in the context of HIV infection, due to the compromised immune system.5
The HIV and syphilis co-infection increase the incidence of neurological complications.6 Commonly, both HIV and syphilis infection could cause cognitive impairment. HIV-associated neurocognitive disorder (HAND) is one of the most important comorbidities in HIV patients, and it is related with impaired attention, information processing speed, motor speed, memory, executive function, and decision-making.7–10 Based on the clinical manifestation, HAND could be categorized into asymptomatic neurocognitive impairment (ANI), mild neurocognitive disorder (MND) and even dementia.7 However, the underlying neural mechanism of HAND has not been fully elucidated. Chronic inflammation often related to monocytes and macrophages appears to be the most widely hold mechanism of HAND.8 In terms of syphilis infection in CNS, neurosyphilis with or without overt neuropsychiatric symptoms is more common in HIV-infected patients.1 Moreover, syphilis co-infection history could deteriorate the cognitive impairment in HIV patients. Wallace et al found that the impaired cognitive function in HIV patients could be worsened with a syphilis co-infection history.13 More recently, Marra et al14 claimed that HIV-infected patients with past syphilis performed worse on a comprehensive neuropsychological test battery than HIV-infected patients who had never had syphilis. These studies raised the supposition that syphilis co-infection might cause worse brain damages in HIV positive patients.
The mechanism of syphilis infection on cognitive impairment in patients with HIV is not well understood and remains a matter of debate. One of the vital hypotheses of the mechanism of HAND is persistent CNS inflammation, and it was supposed that the co-infection of syphilis and HIV might act in a synergistic way on the cognitive decline.1 A most recent study found that the syphilis infection could augment HIV-associated CNS inflammation by testing the cerebral spinal fluid.2 However, this finding could not explain the cognitive impairment in HIV patients with syphilis co-infection. Thus, alternative biomarkers from neuroimaging tools might be useful in assessing the underlying mechanism of brain impairment in patients with HIV and syphilis infection.
To date, it is well known that MR imaging is a sensitive and noninvasive method that could reflect the subtle brain changes of HAND even on effective treatment.8 Generally, HIV-positive patients could suffer decreased brain volume, more white matter hyperintensities loads, disturbed white matter microstructure integrity, decreased cerebral perfusion, and compromised functional connectivity.11 Among the multimodal MR methods, the blood oxygenation level-dependent (BOLD) resting-state functional MRI (rs-fMRI), without the presence of any cognitive tasks or stimulation, has been increasingly used in investigating the alteration of brain spontaneous activity in HIV. At present, the majority of rs-fMRI studies on HIV are related to functional connectivity and brain network. Studies found compromised functional connectivity mainly involved fronto-striatal network, parietal cortex, occipital cortex, and the cerebellum.12 Nevertheless, whether there is any additional effect of syphilis co-infection on the brain function in HIV patients remains unknown.
Most recently, graph theory-based topological analysis has been applied in assessing the brain functional and structural organization in HIV patients. The topological changes in HIV patients might be induced by underlying synaptodendritic damage caused by neuro-inflammation.15–17 Notably, one prior study has indicated that centrality could be associated with HAND.15 According to graph theory, centrality is defined to describe nodes as central or more crucial in a brain network. As far as we know, these previous functional connectivity methods based on graph theory mentioned above relied remarkably on preselected seed regions or atlases. However, the selection of the seed locations is arbitrary to some extent. In order to avoid potential selection bias, voxel-wise and data-driven method is needed. Besides, as far as we know, no graph theory-based functional connectivity analysis had been used in assessing the possible effect of syphilis co-infection on the brain function in young HIV patients.
To avoid the potential seed-selection bias in previous functional connectivity analysis, we utilized the degree centrality (DC) to study the functional alteration in HIV patients with syphilis co-infection. DC is a reliable and frequently used graph-theory-based method with moderate to high test–retest reliability for describing the functional connectivity of neural network.18 Voxel-wised DC analysis could calculate the density of functional connectivity of each voxel in the whole-brain network without any prior hypotheses. As such, for the first time, we implemented DC to assess the likely underlying mechanism of brain damage in patients with early HIV and syphilis co-infection.
Subjects and Methods
Subjects
This study was approved by the institutional review board of Beijing Youan Hospital, Capital Medical University, Beijing, China, and was conducted in accordance with the Declaration of Helsinki. Written informed consents were gained from all the subjects. This study was a cross-sectional study. We prospectively designed the MRI examination with careful inclusion and exclusion criteria. However, we retrospectively collected the laboratory and clinical data from the medical records. Forty-four consecutive patients with HIV co-infected by syphilis (HIV+/syphilis+) (female\male=1\43; age: 32.11 ± 6.96 years) and 45 patients with HIV without syphilis co-infection history (HIV+/syphilis-) (female\male=3\42; age: 31.23±6.21 years) were enrolled from infectious disease outpatient clinic of Beijing Youan Hospital, Capital Medical University. The HIV+ patients were diagnosed by testing plasma HIV RNA or by positive HIV enzyme-linked immunoassay. Given that the high risk of co-morbidity of HIV and syphilis, laboratory tests for syphilis infection were also performed in each patient with a high risk of HIV infection. The syphilis infection was diagnosed by T pallidum particle agglutination (TP-PA). And the Rapid Plasma Reagin (RPR) was performed for assessing the current syphilis infection status and evaluating response to therapy. All the patents with syphilis co-infection were administered with penicillin at diagnosis. Besides, before each MRI examination, plasma CD4+ cell count, CD4+/CD8+ ratio and HIV viral load were tested. History of syphilis infection diagnosis and treatment, estimated HIV infection duration and the HIV therapy history were acquired from medical history records. Moreover, a comprehensive battery of neuropsychological tests was performed prior to MR examination.
For HIV+/syphilis+, the inclusion criteria were as follows: (1) patients infected by both HIV and syphilis; (2) age range from 18 to 50 years old; (3) right-handed. In order to reduce the heterogeneity between subjects and to avoid the FC difference from handedness, we only recruited right-hander in our study. Exclusion criteria included: (1) illiterate people, (2) obvious brain diseases according to conventional MR imaging such as trauma, tumor and stroke, (3) neurodegenerative diseases or psychiatric illness, (4) any substance use disorder according to the Diagnostic Statistical Manual-5th edition. The neuroimaging methods have revealed the structural and functional impairment in patients with substance use disorder. Thus, it is necessary to rule out substance use disorder in order to exclude those patients with a pathological condition potentially confounding. (5) anxiety or depressive symptoms, (6) head motion greater than 1.0° or 1.0 mm during MR examination, (7) HCV co-infection.
For HIV+/syphilis-, the inclusion criteria were as follows: (1) patients infected with HIV and without any syphilis infection history (a combination of TPPA-/RPR-); (2) age range from 18 to 50 years old; (3) right-handed. The exclusion criteria for HIV+/syphilis- were identical to those for HIV+/syphilis+.
Besides, forty-three age, gender, and education matched healthy controls (HC) without any HIV or syphilis infection (female\male=4\39; age, 33.09 ± 6.27 years) were enrolled from the local community. The inclusion criteria for HC were 18 to 50 years old and right-handed. The exclusion criteria for HC group were the same as applied in HIV+ patients.
Neuropsychologic Tests
A battery of neuropsychological tests (related to six cognitive domains including verbal fluency, executive function, speed of information processing, fine motor, attention/working memory, and learning/delayed recall)19 were conducted in all HIV patients (please see the details in Supplementary Table 1). The activity of daily living scale was used as a questionnaire to assess changes in everyday functioning.20 The raw scores for each test were converted to T scores and adjusted for age, gender, and education level. Averaged T score was calculated for the cognitive domain with multiple cognitive tests. According to Frascati criteria,19 41% (18/44) and 36% (16/45) patients were diagnosed as ANI in HIV+/syphilis+ and HIV+/syphilis- groups, respectively. No MND and dementia were diagnosed in all the HIV patients. Thus, the rest patients were diagnosed as non-HAND in the two groups of patients with less than 2 cognitive domain impairments.19
MRI Data Acquisition
MRI data sets were acquired on a 3.0-Tesla MR scanner (Tim-Trio, Siemens Medical Solutions, Erlangen, Germany) with a 32-channel phased-array head coil. All subjects were required to stay awake and still with eye closed, and not to think about anything particular. Rs-fMRI data were gained using a gradient echo sequence: TR/TE:2000/30, FOV: 224 × 224 mm, matrix: 64 × 64, section thickness: 3.5 mm, flip angle: 90°, and voxel size: 3.5 × 3.5 × 4.2mm3. Each brain volume included 33 consecutive axial slices and each run contained 240 volumes. In addition, the conventional T1 weighted MRI (TR/TE=250/2.46) and T2 weighted sequences (TR/TE =2500/200) were also performed. And these images were interpreted by two neuroradiologists (X.D.Z and R.L.L with 9 and 12 years of experience of neuroradiology) in consensus to exclude obvious brain abnormalities, such as stroke and tumor.
Functional MRI Data Preprocessing
Resting-state functional MRI data were preprocessed in a standard manner by using Statistical Parametric Mapping (SPM8, http://www.fil.ion.ucl.ac.uk/spm). Firstly, the first 10 time points of each subject were discarded accounting for the signal equilibrium and adaptation of the subject. After that, for the rest 230 time points, slice timing, correction of head movement and spatial normalization to the Montreal Neurological Institute (MNI) EPI template with a resampled voxel size of 3×3×3 mm3 were performed. Subjects were ruled out with head movement more than 1 mm translation in any axis or 1°angular rotation in any axis during fMRI scanning. After that, the data were detrended to remove the linear trend of time courses and band-pass filtered (temporal band-pass filtering was 0.01–0.08 Hz) voxel by voxel to reduce the effects of low-frequency drift and high-frequency respiratory and cardiac noise. Finally, white matter signal and cerebral-spinal fluid signal were regressed out as covariates.
Functional Connectivity Density Mapping
Voxel-wise DC value was computed in every voxel by using DPABI (Yan, C.G., Wang, X.D., Zuo, X.N., Zang, Y.F., 2016. DPABI: Data Processing & Analysis for (Resting-State) Brain Imaging. Neuroinformatics 14, 339–351). In a brain network, the time course of each voxel in the network was correlated to time course of every other voxel, generating an n×n matrix of Pearson’s correlation coefficients, where n is the dimension of the whole-brain mask. DC of a given voxel is referred to the total number of edges connected to it from the remaining voxels in the whole brain.18 The DC of each voxel in this brain network was generated one by one without any exception resulting in the whole-brain DC mapping. The computation of DC of each voxel (i) with all other voxels (j) was coming from the following formula.18

The DC value was standardized by being converted to Z scores. Thus, all DC map across subjects could be further averaged and compared. In addition, the Z score transformation abided by the following equation.

The  represented the mean degree throughout all the voxels of the whole brain, while σD was the standard deviation. Before the statistical analysis, the images were smoothed with 8 mm3 full-width-at-half-maximum (FWHM) Gaussian kernel.
represented the mean degree throughout all the voxels of the whole brain, while σD was the standard deviation. Before the statistical analysis, the images were smoothed with 8 mm3 full-width-at-half-maximum (FWHM) Gaussian kernel.
Statistical Analysis
The clinical and neuropsychological data were compared by using SPSS 20.0 (IBM Inc. Armonk, NY). Difference of gender among the three groups was compared with χ2 test. The rest of the variables were tested for normal distribution by using the Kolmogorov–Smirnov test. Variables with normal distribution were displayed as mean ± standard deviation and analyzed by two-sample t-test or one-way analysis of variance. Variables with non-normal distribution were displayed as median and inter-quartile range and further tested by Mann–Whitney U-test or Kruskal–Wallis Test. The level of statistical significance was set as p< 0.05.
Rs-fMRI data were analysed by using SPM8 (The FIL Methods Group, London, England). Between-group comparison was performed by using one-way analysis of variance with sex, age and education level as covariates among the three groups. Post hoc analysis was further performed for pair-wise group comparisons. We utilized a whole-brain grey mask for the F-test and post hoc tests in ANOVA. Multiple comparison correction was performed with AFNI’s 3dClustSim by using mixed autocorrelation function (ACF)21 (significance level: voxel p = 0.005, α = 0.05 with 5000 Monte Carlo simulations).
To assess the correlations of DC value in brain regions with a significant difference in the HIV+/syphilis+ and HIV+/syphilis- groups to clinical and neuropyschometric data (T scores), Pearson correlation was performed by using SPSS 20.0 (P < 0.05).
Results
Demographic, Clinical and Neuropsychological Data
Clinical and neuropsychological data for the HIV+/syphilis+, HIV+/syphilis-, and HC were exhibited in Table 1. No significant differences in gender, age, and education level among the three groups were found (all P > 0.05). There were no statistical differences in HIV infection duration, CD4+ cell count, and CD4+/CD8+ ratio (all P > 0.05) as well. In our study, in fact, there were three kind patients in the 44 patients of HIV+/syphilis+ group. A. RPR+ with presence of ulcerative lesions who were diagnosed as primary syphilis (13/44); B. RPR+ without presence of ulcerative lesions (17/44); C. RPR- with a history of syphilis diagnosed as primary syphilis within 2 years (14/44). All of the HIV+/syphilis+ patients had a history of syphilis infection with TPPA+/RPR+ within 2 years. Thus, all of them were not new infections. Of note, all the male patients with HIV infection in this study were men who have sex with men. They took more risk of being infected by syphilis and a higher risk of syphilis relapse. The range of RPR titre at the time of MRI examination was from negative to 1:256. Penicillin was administrated in all the patents with syphilis co-infection at diagnosis. The combination antiretroviral therapy (cART) was given in 82% (36/44) and 82% (37/45) patients of HIV+/syphilis+ and HIV+/syphilis- groups, respectively. Since no HIV+/syphilis+ individuals got obvious neuropsychological manifestations, most of them refused to receive any lumbar puncture; thus, the neurosyphilis cannot be diagnosed based on CSF variables.
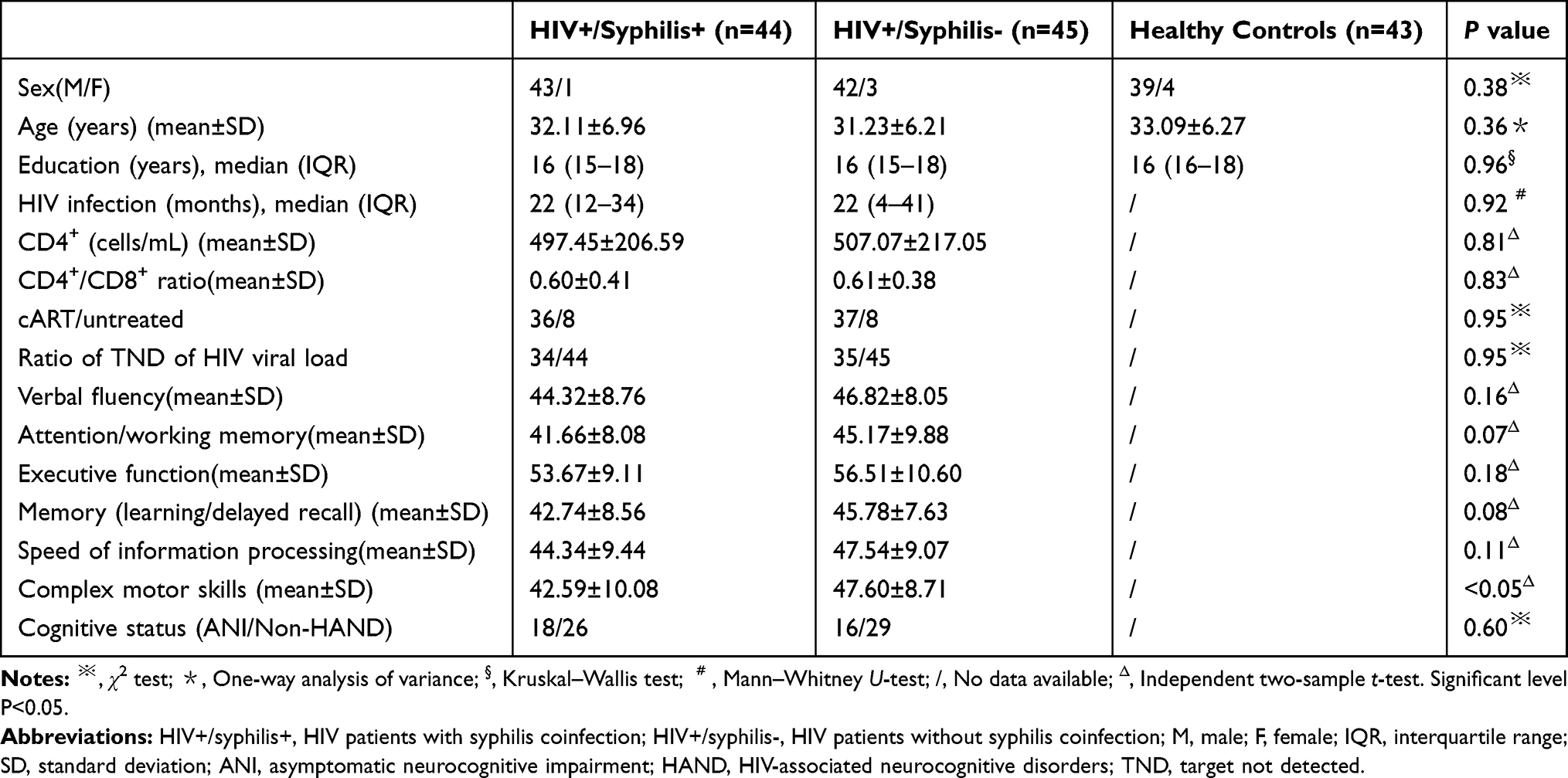 |
Table 1 Demographic, Clinical and Neruopsychological Data of the Three Groups |
Of note, we found a significant lower score in the cognitive domain of fine motor (P < 0.05) in HIV+/syphilis+ group. With regard to the rest of the cognitive domains, a trend of lower cognitive scores in the syphilis co-infection group was found (all P > 0.05). No MND and dementia were diagnosed in all the HIV patients. In addition, the cognitive status (ANI/non-HAND) between the two HIV+ groups showed no significant difference (P > 0.05).
Inter-Group Comparisons of DC
The DC differences among HIV+/syphilis+, HIV+/syphilis- and HC and the pair-wise post hoc results are exhibited in Figure 1 and Table 2. F-test of ANOVA showed DC differences located in the right orbital frontal cortex, left lateral occipital cortex, left inferior frontal cortex (oper/Tri), bilateral posterior cingulated cortex/precuneus and left inferior parietal lobule. Pair-wise inter-group comparisons were further conducted. Compared with HC, HIV+/syphilis+ and HIV+/syphilis- groups showed decreased DC in the right orbital frontal cortex and increased DC in the left inferior parietal cortex. Apart from that, we also found increased DC in the left inferior frontal cortex (oper/Tri) and bilateral posterior cingulated cortex/precuneus in HIV+/syphilis+ compared with HC. Moreover, compared with HIV+/syphilis-, HIV+/syphilis+ displayed decreased DC in the left middle occipital cortex. (P<0.005, cluster number = 249, α = 0.05, corrected). The mean z values of DC of brain regions with statistical significance were extracted and displayed by bar graph at the group level (Supplementary Figure 1).
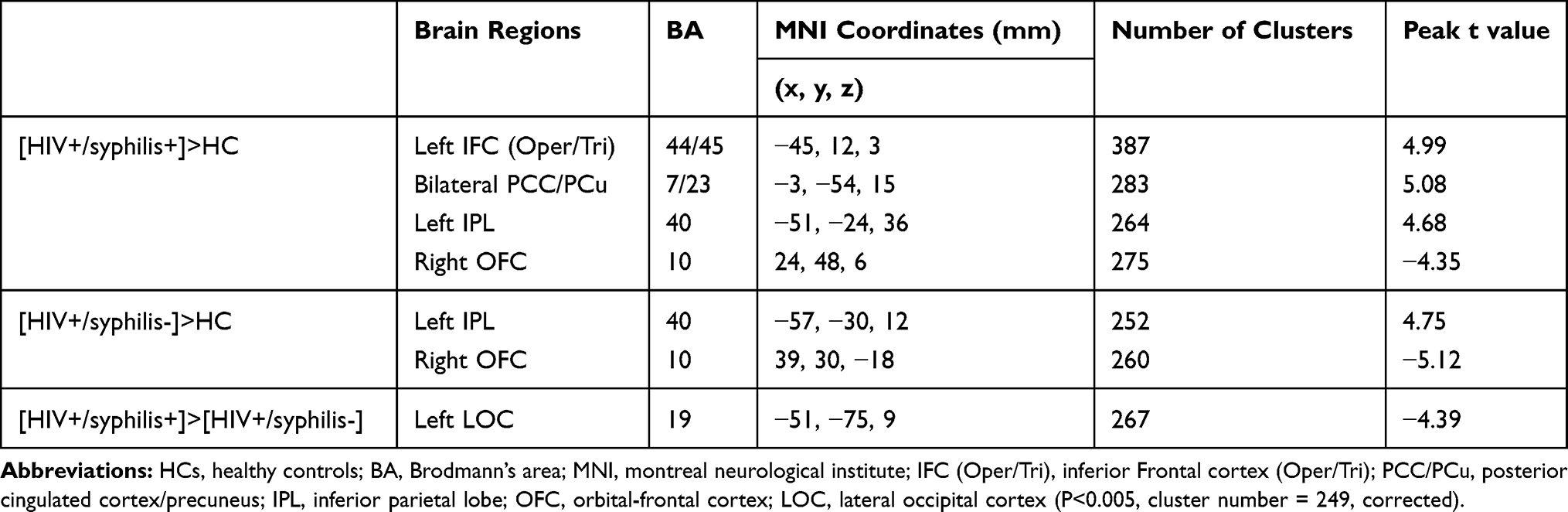 |
Table 2 Brain Regions with DC Differences Among the Three Groups |
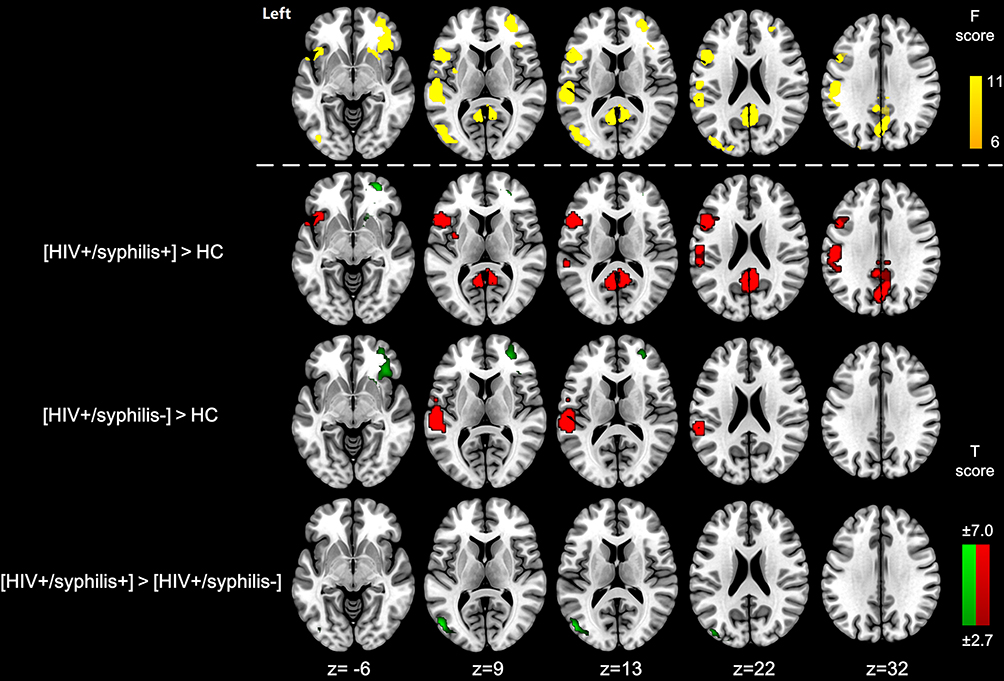 |
Figure 1 DC differences among HIV+/syphilis+, HIV+/syphilis- and HC groups. Notes: F-test of ANOVA showed DC differences mainly located in bilateral frontal cortex, left occipital cortex, and bilateral inferior parietal lobule (yellow). HIV+/syphilis+ showed decreased DC in the right frontal cortex and increased DC in the bilateral inferior parietal cortex and left occipital cortex. HIV+/syphilis- showed decreased DC in the right frontal cortex and increased DC in the left inferior parietal cortex. Compared with HIV+/syphilis-, HIV+/syphilis+ displayed decreased DC in the left occipital cortex. (P<0.005, cluster number = 249, α = 0.05, corrected). Increased DC was shown in red, while decreased DC was shown in green.Abbreviations: ANOVA, analysis of variance; DC, functional connectivity density; HIV+/syphilis+, HIV patients with syphilis coinfection; HIV+/syphilis-, HIV patients without syphilis coinfection; HC, healthy controls. |
Correlation Analysis
In HIV+/syphilis+ group, we found that the mean z value of DC in the right orbital frontal cortex was positively correlated to the CD4+ cell counts (r = 0.366, P = 0.014) (Figure 2A). In addition, the mean z value of DC in the left inferior parietal lobe was negatively correlated to the executive function score (r = −0.314, P = 0.038) (Figure 2B). Nevertheless, no significant correlations were found in any clinical and neuropyschometric data (all P>0.05, Pearson correlation).
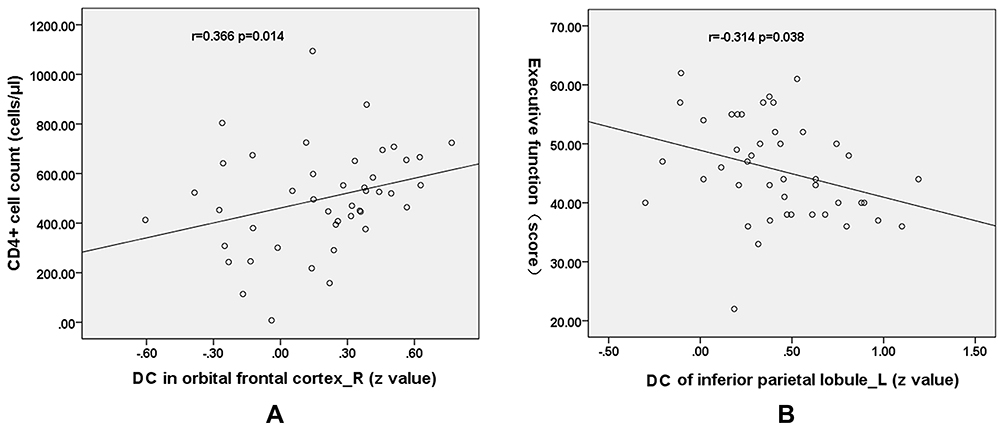 |
Figure 2 Pearson correlation between DC values and clinical variables and cognitive metrics in HIV+/cART+. Notes: The mean z value of DC in the right orbital-frontal cortex was positively correlated to the CD4+ cell counts (r = 0.366, P = 0.014) (A). The mean z value of DC in the left inferior parietal lobe was negatively correlated to the executive function score (r = −0.314, P = 0.038) (B). |
Discussion
HIV and syphilis affect similar patient groups, and the co-infection is common and dangerous combination at present.6 Especially, resurgent syphilis has been found to occur predominantly in high-risk HIV groups, which has renewed great interest in this issue. Syphilis co-infection history could deteriorate the cognitive impairment in HIV patients.13,14 We assessed the effect of syphilis co-infection on the resting-state brain function in young HIV patients by using DC analysis. In this study, we found a significant lower score in the cognitive domain of fine motor in HIV+/syphilis+ group. Compared with HC, HIV+/syphilis+ and HIV+/syphilis- groups showed decreased DC in the right orbital frontal cortex and increased DC in the left inferior parietal lobule. Besides, DC elevated in the left inferior frontal cortex and bilateral posterior cingulated cortex/precuneus in HIV+/syphilis+ compared with HC. Moreover, compared with HIV+/syphilis-, HIV+/syphilis+ displayed decreased DC in the left middle occipital cortex. Additionally, in HIV+/syphilis+ group, the mean z value of DC was correlated to the CD4+ cell counts and the executive function score.
The close interaction between syphilis and HIV on CNS involvement is complicated and not fully understood.2 Cognitive impairment might be the least likely to respond to antibiotic treatment in syphilis CNS infection.6,22 Despite the timely prescribing of penicillin, concerns have been raised in terms of the adequate penicillin concentrations in CSF and the antibiotic resistance of Treponema pallidum.22 Moreover, the extension of syphilis infection to the CNS could emerge in any stage of syphilis infection.23 Neuroinflammatory was considered to be responsible for cognitive disturbances in HIV positive individuals.24 Both syphilis and HIV could contribute to meningitis and neural inflammation of the host, which might mutually augment the CNS impairment.1 In addition to syphilis co-infection, some other chronic co-infections, such as, hepatitis C virus25 or toxoplasmosis,26 may worsen cognition impairment in HIV. Thus, it is plausible that additive or synergistic effect on cognitive malfunction might be induced by syphilis co-infection in HIV patients, even in the early stage of syphilis.
Nevertheless, to date, investigations leave not fully uncovered the role of syphilis co-infection on cognitive impairment in HIV individuals. A greater level of neurocognitive impairment was reported in HIV patients with syphilis co-infection history.13 More recently, it was claimed that HIV-infected patients with past syphilis performed worse on a comprehensive neuropsychological test battery than HIV-infected patients who never had syphilis,14 even in HIV infected subjects on stable cART. Moreover, a most recent prospective study found no difference of mental alternation scores between neurosyphilis and uncomplicated syphilis, but did claim higher level of CNS inflammatory markers was linked to the cognitive impairment in neurosyphilis in the setting of HIV infection, which stressed the significance of CNS inflammation underlying the cognitive impairment out of HIV and syphilis co-infection.2 However, this study did not address whether syphilis co-infection without neurosyphilis could contribute to cognitive impairment in HIV.2 Therefore, alternative neuroimaging biomarkers might be useful in assessing the underlying mechanism of brain impairment in patients with HIV and syphilis infection. In this study, we found a significant lower score in the cognitive domain of fine motor (P < 0.05) and a trend of lower cognitive scores in the HIV+/syphilis+ group. These lower scores of cognitive test without statistical significance might be attributed to effective therapy in our patient groups. With the advent of advanced MRI methods, additional biomarkers might be found in detecting the neural traits underlying cognitive impairment in HIV patients with syphilis history, in addition to neuropsychological tests and CNS inflammatory biomarkers.
The densely connected nodes of the brain network characterized by fast inter-brain connection with minimal energy cost are thought to be the network hubs.18 DC analysis could be used to assess the distribution of hubs in order to make a better understanding of the brain network organization in an energy-efficient way. Further, various neuropsychiatric diseases have been related to abnormal configuration of DC distribution.27–29 Importantly, compared with previous studies on HAND based on graph theory analysis by simplifying the brain network into 90 regions,13,14 DC analysis is a data-driven method without the constrain of specific seeds and allows for whole-brain topological analysis voxel by voxel. Furthermore, centrality is considered as a vital topological metric related to HAND.30 Whereby, the DC method was employed in this current study. So far as we know, no study was conducted using DC to assess the potential additive effect of syphilis co-infection on cognitive impairment in HIV patients.
Compared with HC, both HIV positive groups showed decreased DC in the right orbital-frontal cortex. HIV has been shown to invade the brain causing irreversible damage to synaptic connections, which can gradually lead to neuronal dysfunction. The human orbitofrontal cortex was a vital component of prefrontal cortex, which was related to convergence of sensory information, learning, and decision-making.31 Ketzler et al found loss of neurons of orbital-frontal cortex in brains with AIDS.32 Thompson et al33 found cortical thinning in frontal polar cortex in AIDS patients. Further, Ernst et al34 claimed that mild HIV brain injury is associated with increased glial activation in the frontal white matter and deep gray matter without major involvement of neuronal abnormalities. Moreover, Sailasuta et al reported the concentration of brain glutamate neurotransmitter was reduced in the frontal white matter region in HIV-seropositive patients with or without highly active retroviral therapy.35 Recent functional connectivity study indicated decreased bilateral connectivity between the precuneus and prefrontal cortex in HIV patients with HAND compared with those without HAND.36 In our recent study, we found decreased DC in the right orbital-frontal cortex, which indicated that this region got less connected in a functionally reorganized brain of HIV patients compared with HIV-negative HC. Nonetheless, to date, the exact role of prefrontal cortex and its subdivisions, such as orbital-frontal part, in the pathophysiological mechanism of HAND has not been fully understood. Besides, in HIV+/syphilis+ group, we found that the mean z value of DC in the right orbital-frontal cortex was positively correlated to the CD4+ cell counts. CD4+ cell counts could reflect the immune status of AIDS, and could predict the neurocognitive functional compromise in HIV infection.37 In terms of structural MRI, Thompson et al33 reported that thinner frontopolar cortex correlated with immune system deterioration measured by CD4+ lymphocytes in HIV patients. Currently, we only found the correlation between DC in orbital-frontal cortex and CD4+ cell counts in HIV+/syphilis+ group, rather than HIV+/syphilis- group. Two possible reasons might be responsible for it. Firstly, our patients with HIV were in quite early-stage infection. Secondly, the syphilis co-infection might cause additive or synergistic impairment with HIV on the brain function.
In addition, increased DC in the left inferior parietal lobule was found in both HIV+ groups, and negatively correlated to executive function. Inferior parietal lobule was located in the posterior part of the parietal cortex and adjacent to the occipital cortex. Inferior parietal lobule was reciprocally connected with various cortical and subcortical brain regions and served as a site of integrating nearly all aspects of mental function.38 Lines of evidence indicated that Inferior parietal lobule played a vital role in structural and functional reorganization in HIV-infected patients. Shin et al found cortical thinning in the left inferior parietal lobule and many other frontal-parietal cortices in HAND.39 Li et al also found reduced gray matter in inferior parietal lobule in HIV vertically infected adolescents.40 Wang et al found reduced coactivation in left inferior parietal cortex in HIV by using independent component analysis.41 In our study, increased DC of the left inferior parietal lobule gave further insights into functional reorganization of the brain affected by HIV infection from the perspective of graph theory.
Notably, we found more extended brain regions of DC alteration between HIV+/syphilis+ and HC. Apart from the altered DC in the brain regions mentioned above in both patient groups compared with HC, we also found that the DC values increased in the left inferior frontal lobe and bilateral posterior cingulated cortex/precuneus in HIV+/syphilis+ compared with HC. Inferior frontal lobe was a vital site in the structural and functional cerebral alteration related to HIV infection. Decreased gray matter of the Inferior frontal lobe was reported in HIV patients.42 Convergent evidence from functional MRI studies indicated greater functional activation within the left inferior frontal lobe in HIV patients.43 After effective antiviral therapy, the decreased striato-inferior frontal functional connectivity could be reversed to some extent.44 In addition, the posterior cingulated cortex/precuneus was another important brain site correlated with the HIV infection. Posterior cingulated cortex/precuneus was a vital part of default mode network of the brain, which was frequently involved in HIV patients.45 Cohen et al claimed that activation of the posterior cingulate cortex during rest was related to Hopkins Verbal Learning Test-2 learning in HIV patients, which was not found in HIV-negative controls.17 Recently, Zhuang et al found decreased functional connectivity between posterior cingulate cortex and left inferior parietal cortex in HIV positive patients without white matter fractional anisotropy alteration in this tract.46 These additional brain regions with increased DC found in HIV+/syphilis+ group might indicate that syphilis infection resulted in a synergetic effect with HIV infection on the brain functional remodeling. However, these changes were not found in the HIV+/syphilis- group, which might be due to the early stage of HIV infection in our patient cohort.
Moreover, compared with HIV+/syphilis-, HIV+/syphilis+ displayed decreased DC in the left middle occipital cortex, which might be specifically attributed to syphilis infection. In recent years, with the advent of multimodal MRI, many evidence from neuroimaging, especially from multimodal MRI, indicate that the occipital cortex does get involved in neuropsychological impairment of HIV patients. Many studies claimed decreased occipital gray matter,47 occipital cortex thinning33 and increased MD in fronto-occipital fasciculus42 in HIV patients. For instance, Küper et al found lower CD4 cell count correlated with a decrease of occipital gray matter in early HIV patients by using VBM.47 Thompson et al found that the thinning of the cerebral cortex visualized in HIV/AIDS was linked to CD4+ T lymphocyte decline.33 Most recently, DTI study by using TBSS found increased MD in fronto-occipital fasciculus in HIV patients from Beijing Youan Hospital of Capital Medical University. Evidence from rs-fMRI studies in early HIV-infected individuals indicated decreased functional connectivity in occipital cortex.41,48 Wang et al found decreased functional connectivity in lateral occipital cortex in patients within 1 year of HIV infection.41 Moreover, Egbert et al reported that occipital lobe was affected by HIV more profoundly than other brain networks even years after infection.48 Besides, Ances et al demonstrated significant reductions in cerebral blood flow in both visual cortex and lenticular nuclei in recent HIV-infected individuals by using arterial spin labeling MRI.49 Küper et al speculated that the occipital cortex may be especially vulnerable to HIV mediated neurotoxicity when the immune system deteriorates.47 However, no DC difference in occipital cortex was found in both HIV+ groups compared with healthy controls with possible explanation related to the early stage of HIV infection in this cohort.
Limitations exist in our current study. Firstly, since no HIV+/syphilis+ individuals got obvious neuropsychological manifestations, most of them refused to receive any lumbar puncture, whereby the neurosyphilis cannot be diagnosed based on CSF variables. And therefore, it was not allowed to confirm the proportion of possible neurosyphilis in this cohort. Further studies are warranted to confirm potential cognitive impairment and altered advanced MRI variables in concurrent HIV/syphilis with neurosyphilis and without neurosyphilis. Secondly, all HCs lacked neuropsychological tests, which should be supported in further studies. Thirdly, the relatively high frequency of ANI, and the presence of untreated participants, may contribute to the fMRI abnormalities. Besides, no MND patients were found in our patient cohort, which limited the generalizability of our result. Additionally, we did not further analyze other topological features. More detailed graph theory-based studies on the possible neural influence of syphilis co-infection in HIV were warranted.
Conclusion
HIV+/syphilis+ patients might get more extend frontal and parietal involvement in terms of DC, and decreased DC in the left middle occipital cortex, which indicated that syphilis and HIV co-infection might act synergistically on the brain functional reorganization. However, further researches are needed to confirm this finding.
Abbreviations
DC, degree centrality; MRI, magnetic resonance imaging; HIV, human immunodeficiency virus; HAND, HIV-associated neurocognitive disorders; BOLD, Blood oxygen level-dependent.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (No: 81701679, 81771806, 61936013, 81701984), Peking University Medicine Seed Fund for Interdisciplinary Research (No: BMU2018MX027), Capital medical university research and incubation funding (No: PYZ19162), Beijing Excellent Talent Plan (2018000021469G290, 2018000021213ZK04), National Science and Technology Major Project of China During the 13th Five-year Plan Period (No: 2017ZX10201101), and the Natural Science Foundation of Tianjin (19JCQNJC09800).
Author Contributions
Xiao-Dong Zhang wrote this paper; Guang-Xue Liu, Xiao-Yue Wang, Xiao-Jie Huang and Jing-Li Li participated in the data collection, clinical analysis and the data analysis; Rui-Li Li and Hong-Jun Li designed this study. All authors contributed to data analysis, drafting or revising the article, and gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hobbs E, Vera JH, Marks M, Barritt AW, Ridha BH, Lawrence D. Neurosyphilis in patients with HIV. Pract Neurol. 2018;18:211–218. doi:10.1136/practneurol-2017-001754
2. Ho EL, Maxwell CL, Dunaway SB, et al. Neurosyphilis Increases Human Immunodeficiency Virus (HIV)-associated central nervous system inflammation but does not explain cognitive impairment in hiv-infected individuals with syphilis. Clin Infect Dis. 2017;65:943–948. doi:10.1093/cid/cix473
3. Rolfs RT, Joesoef MR, Hendershot EF, et al. A randomized trial of enhanced therapy for early syphilis in patients with and without human immunodeficiency virus infection. The syphilis and HIV study group. N Engl J Med. 1997;337:307–314. doi:10.1056/NEJM199707313370504
4. Lukehart SA, Hook EW
5. Walter T, Lebouche B, Miailhes P, et al. Symptomatic relapse of neurologic syphilis after benzathine penicillin G therapy for primary or secondary syphilis in HIV-infected patients. Clin Infect Dis. 2006;43:787–790. doi:10.1086/507099
6. Lynn WA, Lightman S. Syphilis and HIV: a dangerous combination. Lancet Infect Dis. 2004;4:456–466. doi:10.1016/S1473-3099(04)01061-8
7. Ellero J, Lubomski M, Brew B. Interventions for neurocognitive dysfunction. Curr HIV/AIDS Rep. 2017;14:8–16. doi:10.1007/s11904-017-0346-z
8. Clifford DB. HIV-associated neurocognitive disorder. Curr Opin Infect Dis. 2017;30:117–122. doi:10.1097/QCO.0000000000000328
9. Ances BM, Hammoud DA. Neuroimaging of HIV-associated neurocognitive disorders (HAND). Curr Opin HIV AIDS. 2014;9:545–551. doi:10.1097/COH.0000000000000112
10. Hakkers CS, Arends JE, Barth RE, Du Plessis S, Hoepelman AI, Vink M. Review of functional MRI in HIV: effects of aging and medication. J Neurovirol. 2017;23:20–32. doi:10.1007/s13365-016-0483-y
11. Cole JH, Caan MWA, Underwood J, et al. No evidence for accelerated aging-related brain pathology in treated human immunodeficiency virus: longitudinal neuroimaging results from the comorbidity in relation to AIDS (COBRA) project. Clin Infect Dis. 2018;66:1899–1909. doi:10.1093/cid/cix1124
12. Wang H, Li R, Zhou Y, et al. Altered cerebro-cerebellum resting-state functional connectivity in HIV-infected male patients. J Neurovirol. 2018;24:587–596. doi:10.1007/s13365-018-0649-x
13. Wallace MR, Heaton RK, McCutchan JA, et al. Neurocognitive impairment in human immunodeficiency virus infection is correlated with sexually transmitted disease history. Sex Transm Dis. 1997;24:398–401. doi:10.1097/00007435-199708000-00003
14. Marra CM, Deutsch R, Collier AC, et al. Neurocognitive impairment in HIV-infected individuals with previous syphilis. Int J STD AIDS. 2013;24:351–355. doi:10.1177/0956462412472827
15. Thomas JB, Brier MR, Ortega M, Benzinger TL, Ances BM. Weighted brain networks in disease: centrality and entropy in human immunodeficiency virus and aging. Neurobiol Aging. 2015;36:401–412. doi:10.1016/j.neurobiolaging
16. Abidin AZ, DSouza AM, Nagarajan MB, et al. Alteration of brain network topology in HIV-associated neurocognitive disorder: a novel functional connectivity perspective. Neuroimage Clin. 2017;17:768–777. doi:10.1016/j.nicl.2017.11.025
17. Ellis R, Langford D, Masliah E. HIV and antiretroviral therapy in the brain: neuronal injury and repair. Nat Rev Neurosci. 2007;8:33–44. doi:10.1038/nrn2040
18. Buckner RL, Sepulcre J, Talukdar T, et al. Cortical hubs revealed by intrinsic functional connectivity: mapping, assessment of stability, and relation to alzheimer’s disease. J Neurosci. 2009;29:1860–1873. doi:10.1523/JNEUROSCI.5062-08.2009
19. Antinori A, Arendt G, Becker JT, et al. Updated research nosology for HIV-associated neurocognitive disorders. Neurology. 2007;69:1789–1799. doi:10.1212/01.WNL.0000287431.88658.8b
20. Gandhi NS, Skolasky RL, Peters KB, et al. A comparison of performance-based measures of function in HIV-associated neurocognitive disorders. J Neurovirol. 2011;17:159–165. doi:10.1007/s13365-011-0023-8
21. Cox RW, Chen G, Glen DR, Reynolds RC, Taylor PA. FMRI clustering in AFNI: false-positive rates redux. Brain Connect. 2017;7:152–171. doi:10.1089/brain.2016.0475
22. Moulton CD, Koychev I. The effect of penicillin therapy on cognitive outcomes in neurosyphilis: a systematic review of the literature. Gen Hosp Psychiatry. 2015;37:49–52. doi:10.1016/j.genhosppsych.2014.10.008
23. Beauchemin P, Laforce R
24. Cohen RA, Siegel S, Gullett JM, et al. Neural response to working memory demand predicts neurocognitive deficits in HIV. J Neurovirol. 2018; 24:291–304. doi:10.1007/s13365-017-0607-z
25. Corgiolu S, Barberini L, Suri JS, et al. Resting-state functional connectivity MRI analysis in Human Immunodeficiency virus and hepatitis C virus co-infected subjects. A pilot study. Eur J Radiol. 2018;102:220–227. doi:10.1016/j.ejrad.2018.03.022
26. Bharti AR, McCutchan A, Deutsch R, et al. Latent toxoplasma infection and higher toxoplasma gondii immunoglobulin G levels are associated with worse neurocognitive functioning in HIV-infected adults. Clin Infect Dis. 2016;63:1655–1660. doi:10.1093/cid/ciw655
27. Wang Y, Jiang L, Wang XY, et al. Evidence of altered brain network centrality in patients with diabetic nephropathy and retinopathy: an fMRI study using a voxel-wise degree centrality approach. Ther Adv Endocrinol Metab. 2019;10:2042018819865723. doi:10.1177/2042018819865723
28. Weng Y, Qi R, Liu C, et al. Disrupted functional connectivity density in irritable bowel syndrome patients. Brain Imaging Behav. 2017;1:1812–1822. doi:10.1007/s11682-016-9653-z
29. Qi R, Zhang LJ, Chen HJ, et al. Role of local and distant functional connectivity density in the development of minimal hepatic encephalopathy. Sci Rep. 2015;5:13720. doi:10.1038/srep13720
30. Abidin AZ, D’souza AM, Nagarajan MB, Wismüller A. Investigating changes in brain network properties in HIV-associated neurocognitive disease (HAND) using Mutual Connectivity Analysis (MCA). Proc SPIE Int Soc Opt Eng. 2016;9788:97881W. doi:10.1117/12.2217317
31. Kringelbach ML. The human orbitofrontal cortex: linking reward to hedonic experience. Nat Rev Neurosci. 2005;6:691–702. doi:10.1038/nrn1747
32. Ketzler S, Weis S, Haug H, Budka H. Loss of neurons in the frontal cortex in AIDS brains. Acta Neuropathol. 1990;80:92–94. doi:10.1007/bf00294228
33. Thompson PM, Dutton RA, Hayashi KM, et al. Thinning of the cerebral cortex visualized in HIV/AIDS reflects CD4+ T lymphocyte decline. Proc Natl Acad Sci U S A. 2005;102:15647–15652. doi:10.1073/pnas.0502548102
34. Ernst T, Chang L, Arnold S. Increased glial metabolites predict increased working memory network activation in HIV brain injury. Neuroimage. 2003;19:1686–1693. doi:10.1016/s1053-8119(03)00232-5
35. Sailasuta N, Shriner K, Ross B. Evidence of reduced glutamate in the frontal lobe of HIV-seropositive patients. NMR Biomed. 2009;22:326–331. doi:10.1002/nbm.1329
36. Ann HW, Jun S, Shin NY, et al. Characteristics of resting-state functional connectivity in HIV-associated neurocognitive disorder. PLoS One. 2016;11:e0153493. doi:10.1371/journal.pone.0153493
37. Grauer OM, Reichelt D, Grüneberg U, et al. Neurocognitive decline in HIV patients is associated with ongoing T-cell activation in the cerebrospinal fluid. Ann Clin Transl Neurol. 2015;2:906–919. doi:10.1002/acn3.227
38. Igelström KM, Graziano MSA. The inferior parietal lobule and temporoparietal junction: a network perspective. Neuropsychologia. 2017;105:70–83. doi:10.1016/j.neuropsychologia.2017.01.001
39. Shin NY, Hong J, Choi JY, Lee SK, Lim SM, Yoon U. Retrosplenial cortical thinning as a possible major contributor for cognitive impairment in HIV patients. Eur Radiol. 2017;27:4721–4729. doi:10.1007/s00330-017-4836-6
40. Li J, Gao L, Wen Z, et al. Structural covariance of gray matter volume in HIV vertically infected adolescents. Sci Rep. 2018;8:1182. doi:10.1038/s41598-018-19290-5
41. Wang X, Foryt P, Ochs R, et al. Abnormalities in resting-state functional connectivity in early human immunodeficiency virus infection. Brain Connect. 2011;1:207–217. doi:10.1089/brain.2011.0016
42. Wang B, Liu Z, Liu J, Tang Z, Li H, Tian J. Gray and white matter alterations in early HIV-infected patients: combined voxel-based morphometry and tract-based spatial statistics. J Magn Reson Imaging. 2016;43:1474–1483. doi:10.1002/jmri.25100
43. Plessis SD, Vink M, Joska JA, Koutsilieri E, Stein DJ, Emsley R. HIV infection and the fronto-striatal system: a systematic review and meta-analysis of fMRI studies. AIDS. 2014;28(6):803–811. doi:10.1097/QAD.0000000000000151
44. Ortega M, Brier MR, Ances BM. Effects of HIV and combination antiretroviral therapy on cortico-striatal functional connectivity. AIDS. 2015;29:703–712. doi:10.1097/QAD.0000000000000611
45. Thomas JB, Brier MR, Snyder AZ, Vaida FF, Ances BM. Pathways to neurodegeneration: effects of HIV and aging on resting-state functional connectivity. Neurology. 2013;80:1186–1193. doi:10.1212/WNL.0b013e318288792b
46. Zhuang Y, Qiu X, Wang L, et al. Combination antiretroviral therapy improves cognitive performance and functional connectivity in treatment-naïve HIV-infected individuals. J Neurovirol. 2017;23:704–712. doi:10.1007/s13365-017-0553-9
47. Küper M, Rabe K, Esser S, et al. Structural gray and white matter changes in patients with HIV. J Neurol. 2011;258:1066–1075. doi:10.1007/s00415-010-5883-y
48. Egbert AR, Biswal B, Karunakaran K, et al. Age and HIV effects on resting state of the brain in relationship to neurocognitive functioning. Behav Brain Res. 2018;344:20–27. doi:10.1016/j.bbr.2018.02.007
49. Ances BM, Sisti D, Vaida F, et al. Resting cerebral blood flow: a potential biomarker of the effects of HIV in the brain. Neurology. 2009;73:702–708. doi:10.1212/WNL.0b013e3181b59a97
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.