Back to Journals » International Journal of General Medicine » Volume 17
Aldehyde Dehydrogenase 2 rs671 G/A and a/A Genotypes are Associated with the Risk of Acute Myocardial Infarction
Authors Li Y, Zhong W, Liu Z, Huang C, Peng J, Li H
Received 26 April 2024
Accepted for publication 10 August 2024
Published 19 August 2024 Volume 2024:17 Pages 3591—3600
DOI https://doi.org/10.2147/IJGM.S475756
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Youqian Li,1,2 Wei Zhong,1,2 Zhidong Liu,1,2 Changjing Huang,1,2 Junyin Peng,1,2 Hanlin Li1,2
1Center for Cardiovascular Diseases, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China; 2Guangdong Provincial Engineering and Technology Research Center for Molecular Diagnostics of Cardiovascular Diseases, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China
Correspondence: Youqian Li, Center for Cardiovascular Diseases, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, No. 63 Huangtang Road, Meijiang District, Meizhou, People’s Republic of China, Email [email protected]
Background: Aldehyde dehydrogenase 2 (ALDH2) is a key catalytic enzyme involved in the aldehyde metabolism that plays an important role in the occurrence and development of acute myocardial infarction (AMI). However, the relationship of ALDH2 polymorphism and susceptibility to AMI may differ among different regions and populations, and it has not yet been reported in Hakka population. The purpose of the present study was to investigate it in this population.
Methods: Four hundred and nineteen AMI patients and 636 individuals without AMI were included in the present study. The ALDH2 rs671 polymorphism was genotyped using polymerase chain reaction (PCR)-microarray. Differences in ALDH2 rs671 genotypes and alleles between patients and controls were compared, and the relationship between ALDH2 rs671 genotypes and AMI risk was analyzed.
Results: Patients with AMI had a lower frequency of ALDH2 rs671 G/G genotype (43.2% vs 52.7%, p=0.003), and a higher G/A genotype (45.6% vs 38.5%, p=0.025) than controls. And AMI patients had a lower frequency of ALDH2 rs671 G allele (66.0% vs 71.9%), and a higher A allele (34.0% vs 28.1%) (p=0.004) than controls. Logistic regression analysis showed that overweight (body mass index (BMI)≥ 24.0 kg/m2 vs BMI 18.5– 23.9 kg/m2: odds ratio (OR) 2.046, 95% confidence interval (CI): 1.520– 2.754, p< 0.001), history of hypertension (yes vs no: OR 3.464, 95% CI: 2.515– 4.770, p< 0.001), ALDH2 rs671 G/A genotype (G/A vs G/G: OR 1.476, 95% CI: 1.102– 1.976, p=0.009), and A/A genotype (A/A vs G/G: OR 1.656, 95% CI: 1.027– 2.668, p=0.038) maybe the independent risk factors for AMI.
Conclusion: Overweight (BMI≥ 24.0 kg/m2), a history of hypertension, and ALDH2 rs671 G/A or A/A genotypes increased the risk of developing AMI in Hakka population.
Keywords: aldehyde dehydrogenase 2, acute myocardial infarction, polymorphism, Hakka
Introduction
Coronary artery disease (CAD) is a heart disease caused by myocardial ischemia or necrosis due to stenosis, blockage and spasm of the coronary artery atherosclerosis.1,2 Acute myocardial infarction (AMI) is a severe form of CAD, caused by the rupture of coronary atherosclerotic plaques, the acute occlusion of the coronary artery leading to interruption of blood flow, and the myocardial necrosis caused by severe and persistent ischemia and hypoxia.3,4 AMI is an important disease burden worldwide, with a high fatality rate,5,6 there are approximately 290 million cardiovascular patients and 2.5 million have AMI in China.7,8 It is of great significance to identify individuals susceptible to AMI.
The pathological basis of AMI is atherosclerosis. At present, atherosclerosis is regarded as a chronic inflammatory disease characterized by a sequence of immune responses, and inflammation plays an important role in the occurrence and development of atherosclerotic lesions.9 The formation of atherosclerotic plaque is characterized by lipid accumulation, local vascular inflammation, proliferation of smooth muscle cells (SMCs), apoptosis, and fibrillation, which is mainly the activation of inflammatory cells and a series of chronic inflammatory reactions triggered by endothelial cell injury.10 The anti-inflammatory treatment of AMI is also receiving more research and attention.11 Some indicators that can reflect the systemic or local inflammation level have potential value in the diagnosis and prognosis assessment of AMI, such as neutrophil-to-lymphocyte ratio (NLR),12 blood cell ratios associated with immune cells,13 fibrinogen albumin ratio (FAR),14 and C-reactive protein (CRP).15
The body will produce a large number of reactive oxygen species (ROS) under stress, which intensifies the peroxidation of mitochondrial polyunsaturated fatty acids, and produces toxic aldehydes.16 Aldehyde dehydrogenase can metabolize toxic aldehydes into low-toxicity carboxylic acids, thus reducing the damage caused by aldehyde overload on the mitochondria,17,18 such as aldehyde dehydrogenase 2 (ALDH2).19 Previous studies have shown that ALDH2 is associated with secondary liver injury, Alzheimer’s disease, pulmonary hypertension, and some cancers.19–22 The relationship between ALDH2 and atherosclerosis, hypertension, and cardiac insufficiency has been reported.23,24 ALDH2 activity is influenced by ALDH2 single nucleotide polymorphism (SNP) rs671 (G>A, Glu504Lys) variants.25,26 Based on the SNP rs671, the population is composed of three genotypes: wild-type ALDH2*1/*1 (G/G), heterozygous type ALDH2*1/*2 (G/A), and homozygous mutant ALDH2*2/*2 (A/A). The Glu504Lys polymorphism can cause ALDH2 enzyme activity to drop to 30–50% of normal.27,28
Several studies found that ALDH2 variant was associated AMI.29–31 The susceptibility to AMI may differ among different regions and populations. The Hakka people are an ethnic group formed by the integration of the people from the central plains of China with different ethnic groups during the southward migration, and Meizhou city is one of the main gathering places of Hakka people.32 The relationship between ALDH2 gene polymorphisms and the risk of AMI in this region has not yet been reported. The purpose of the present study was to analyze the relationship in this population.
Materials and Methods
Study Participants
As a case-control study, this study included 1055 individuals who received medical treatment or physical examination in Meizhou People’s Hospital, Guangdong Province from December 2019 to July 2023 as the study objects, including 419 patients with AMI as the study group and 636 individuals who underwent physical examination as the control group. According to the Fourth Universal Definition of Myocardial Infarction,33 the diagnostic criteria for AMI were revised to include: increased markers of acute myocardial injury, at least once above the 99th percentile of the upper limit of normal, accompanied by at least one of the following indicators: (1) symptoms of acute myocardial ischemia; (2) new ischemic electrocardiogram changes; (3) new pathological Q wave; (4) imaging evidence of loss of viable myocardium or segmental wall motion abnormalities; or (5) coronary angiography confirmed the presence of coronary thrombosis.
Inclusion criteria for the disease group were as follows: (1) 18 years of age and older; (2) patients diagnosed with AMI; and (3) complete medical records. Controls met the following criteria: (1) age ≥18 years old; (2) absence of a CAD diagnosis; and (3) complete examination and laboratory testing information. Exclusion criteria were as follows: (1) combined with suspected or confirmed other cardiomyopathy, such as dilated cardiomyopathy, myocardial amyloidosis, and hypertrophic obstructive cardiomyopathy; (2) other malignant or severe diseases; and (3) pregnancy or tumor.
This study was performed in accordance with the ethical standards of the Declaration of Helsinki and approved by the Human Ethics Committee of Meizhou People’s Hospital. Sample size calculation was performed using Clinical Research Sample Size Calculator (CRESS version 1.3): odds ratio was set at 1.4, ALDH2 variant allele frequency was 28% in Hakka population,34 statistical power was 90%, type I error rate (α) at 0.05, two-sided significance tests, resulting in a sample of 278 patients with AMI and 278 controls.
Data Collection
Information such as age, sex, body mass index (BMI), history of smoking, history of alcohol consumption, history of diabetes mellitus, and history of hypertension was collected from the patient’s medical record information system. BMI was divided into three subgroups based on the Chinese criteria:35,36 <18.5 kg/m2, 18.5–23.9 kg/m2, and ≥24.0 kg/m2. Early morning fasting blood collection and serum separation. Criteria for the diagnosis of hypertension:37 systolic ≥140mmHg and/or diastolic ≥90 mmHg from 2 blood pressure measurements taken on different days without antihypertensive medication. Diagnostic criteria for diabetes mellitus:38 have symptoms of diabetes and plasma glucose ≥11.1mmol/L at any one time, fasting plasma glucose (FPG)≥7.0mmol/L, or 2h 75-g oral glucose tolerance test (OGTT) ≥11.1mmol/L.
The lipid levels in the serum samples were assessed using an automated biochemical analysis system (Olympus AU5400 system, Tokyo, Japan). Serum lipid levels included total cholesterol (TC), triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), Apolipoprotein A1 (Apo-A1), and Apolipoprotein B (ApoB).
DNA Isolation and ALDH2 Genotyping
Genomic DNA was extracted from venous blood collected from EDTA anticoagulant collection vessels using a blood DNA isolation kit (Qiagen GmbH, Germany). DNA quality and concentration were assessed using a Nano-Drop 2000™ spectrophotometer (ThermoFisher Scientific, Waltham, MA, USA). ALDH2 genotype was detected using ALDH2 Gene Detection Kit based on polymerase chain reaction (PCR)-gene chip method (BaiO Technology Co, Ltd., Shanghai, China). Details about ALDH2 polymorphism detection have been reported in previous articles from our hospital.39,40
Statistical Analysis
All statistical analyses were performed using SPSS statistical software (version 26.0; IBM Inc., USA). Continuous variables were expressed as means ± standard deviations and were compared using either Student’s t-test or the Mann–Whitney U-test. The comparison of the genotype composition ratio and allele frequency between the two groups were analyzed using Chi-square test. Logistic regression analysis was used to examine the relationship between ALDH2 polymorphism and AMI. p<0.05 was considered to represent statistical significance.
Results
Characteristics of Subjects
Of the 1055 subjects included in this study, 797 (75.5%) were male and 258 (24.5%) were female. There were 146 cases (13.8%) with BMI <18.5 kg/m2 and 317 cases (30.0%) with BMI≥24.0 kg/m2. A total of 273 cases (25.9%) patients had a history of smoking, 94 cases (8.9%) had a history of alcohol consumption, 268 cases (25.4%) had hypertension, and 180 cases (17.1%) had diabetes mellitus. The study included 419 patients with AMI and 636 controls. The proportion of overweight subjects in the patient group was higher than that in the control group (185 (44.2%) cases with ≥24.0 kg/m2 vs 132 (20.8%) controls with ≥24.0 kg/m2), the difference in BMI distribution among the groups was statistically significant (p<0.001). The proportions of history of alcohol consumption, hypertension, and diabetes mellitus in AMI patients and controls were 4.1%, 41.8%, 22.7%, and 12.1%, 14.6%, 13.4% respectively, with the difference being statistically significant (all p<0.001). The differences in TC, TG, HDL-C, LDL-C, Apo-A1, and Apo-B levels between groups were statistically significant (all p<0.001) (Table 1).
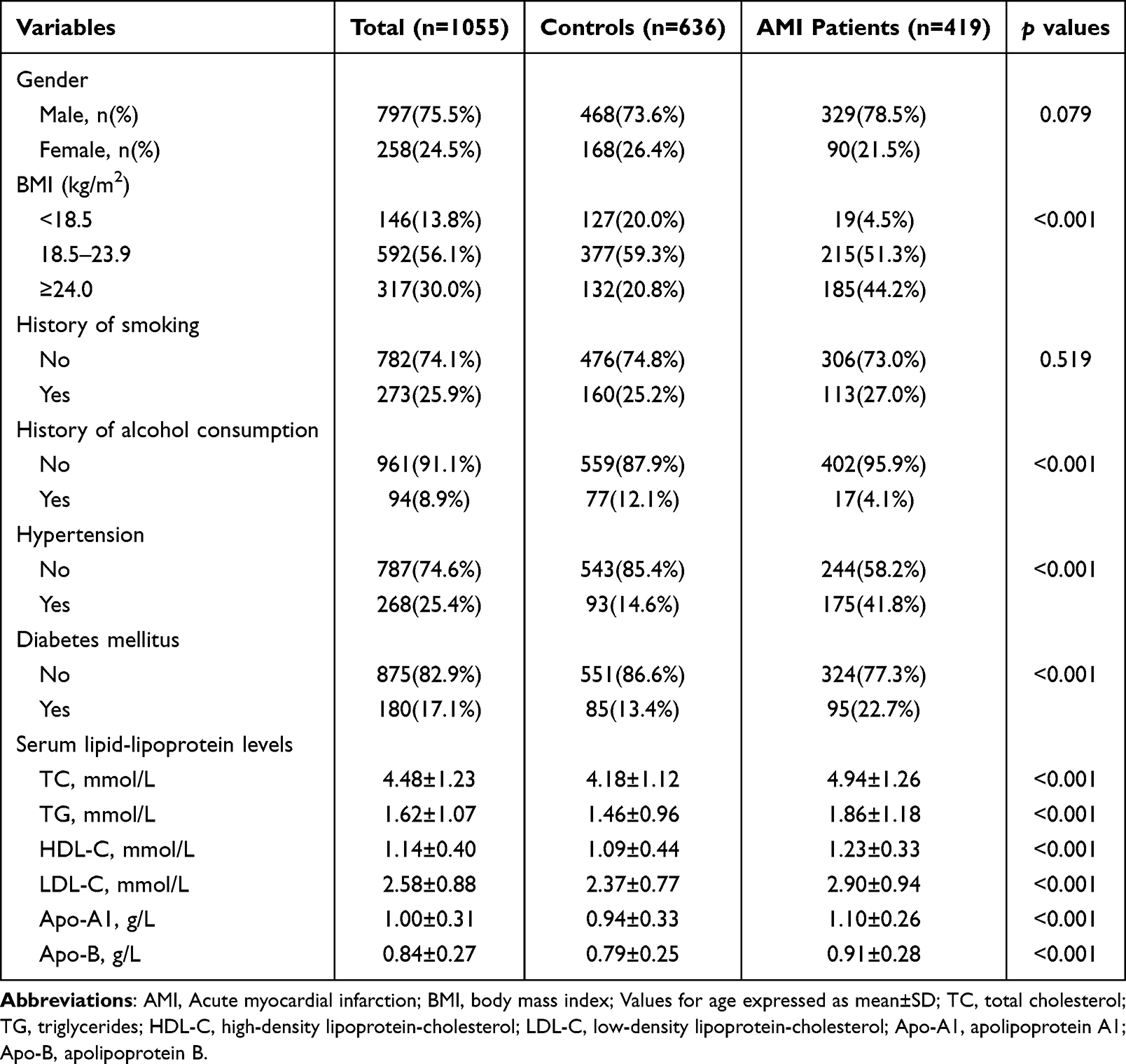 |
Table 1 Clinical Characteristics of the Subjects of This Study |
Distribution of the ALDH2 Genotypes and Alleles Between AMI Patients and Controls
The ALDH2 rs671 genotypes in the AMI patients (χ2=0.102, p=0.750), and controls (χ2=1.344, p=0.246) conformed to the Hardy-Weinberg equilibrium, respectively. A comparison of the frequencies of ALDH2 genotypes between the two groups showed that AMI patients had a lower frequency of ALDH2 rs671 G/G genotype (43.2% vs 52.7%, p=0.003) and a higher frequency of ALDH2 rs671 G/A genotype (45.6% vs 38.5%, p=0.025). There was no statistically significant difference in ALDH2 rs671 A/A genotype (11.2% vs 8.8%, p=0.205) between the two groups. A comparison of allele frequencies showed that AMI patients had a lower frequency of ALDH2 rs671 G allele (66.0% vs 71.9%) and a higher A allele (34.0% vs 28.1%) (p=0.004) than controls (Table 2).
 |
Table 2 Distribution Frequencies of ALDH2 rs671 Genotype and Allele in AMI Patients and Controls |
Clinical Characteristics and Serum Lipid-Lipoprotein Levels of Subjects Stratified by ALDH2 rs671 Genotypes
There was a statistically significant difference in the proportion of patients with a history of alcohol consumption among the ALDH2 rs671 G/G, G/A, and A/A genotypes (p<0.001). The individuals with A/A genotype had lower TG levels (1.34±0.82 mmol/L vs 1.68±1.09 mmol/L and 1.61±1.08 mmol/L, p<0.001) than individuals with G/G genotype and G/A genotype, respectively. There were no statistically significant differences in the BMI distribution, history of smoking, and levels of other serum lipid lipoproteins among ALDH2 rs671 G/G, G/A, and A/A genotype groups (all p>0.05) (Table 3).
 |
Table 3 Clinical Characteristics and Serum Lipid-Lipoprotein Levels of Subjects Stratified by ALDH2 rs671 Genotypes |
Logistic Regression Analysis of Risk Factors Associated with AMI
Univariate logistic regression showed that overweight (BMI≥24.0 kg/m2 vs BMI 18.5–23.9 kg/m2: odds ratio (OR) 2.458, 95% confidence interval (CI): 1.859–3.249, p<0.001), history of hypertension (yes vs no: OR 4.188, 95% CI: 3.123–5.615, p<0.001), history of diabetes mellitus (yes vs no: OR 1.901, 95% CI: 1.376–2.626, p<0.001), ALDH2 rs671 G/A genotype (G/A vs G/G: OR 1.443, 95% CI: 1.111–1.874, p=0.006), A/A genotype (A/A vs G/G: OR 1.553, 95% CI: 1.013–2.383, p=0.044) maybe the risk factors of AMI. And history of alcoholism (yes vs no: OR 0.307, 95% CI: 0.179–0.527, p<0.001) was a protective factor for AMI. Multivariate logistic regression showed that overweight (BMI≥24.0 kg/m2 vs BMI 18.5–23.9 kg/m2: OR 2.046, 95% CI: 1.520–2.754, p<0.001), history of hypertension (yes vs no: OR 3.464, 95% CI: 2.515–4.770, p<0.001), ALDH2 rs671 G/A genotype (G/A vs G/G: OR 1.476, 95% CI: 1.102–1.976, p=0.009), A/A genotype (A/A vs G/G: OR 1.656, 95% CI: 1.027–2.668, p=0.038) maybe the independent risk factors for AMI, and history of alcoholism (yes vs no: OR 0.277, 95% CI: 0.150–0.512, p<0.001) was a protective factor (Table 4).
 |
Table 4 Logistic Regression Analysis of Risk Factors for AMI |
Discussion
The pathological features of AMI include myocardial hypertrophy, decreased myocardial contractile function, myocardial fibrosis, and cardiomyocyte apoptosis.41,42 ROS produced by cells can cause membrane lipid peroxidation by attacking polyunsaturated fatty acids to produce the acetaldehyde derivative, 4-hydroxynonenal (4-HNE). 4-HNE is a strong electrophilic agent that causes apoptosis or necrosis by absorbing intracellular proteins, binding glutathione, and inhibiting the phosphorylation activity of sodium-potassium-ATPase.43 ALDH2 is an important aldehyde oxidase in the mitochondria.44 ALDH2 plays an important role in the formation of foam cells, which are involved in the occurrence and development of atherosclerosis via the 4-HNE/PPARγ/CD36 pathway.45 In addition, ALDH2 is involved in the migration of coronary endothelial cells,46 endoplasmic reticulum stress and smooth muscle cell apoptosis.47 These biological processes may be the mechanisms by which ALDH2 plays an important role in the occurrence and development of AMI.
Regard to ALDH2, a meta-analysis suggested that the A allele of the ALDH2 rs671 polymorphism may increase the risk of CAD and AMI.48–50 Jiang et al found that ALDH2 variant may be an independent risk factor for AMI.29 ALDH2 rs671 A allele is prevalent among Japanese patients with acute ST-segment elevation myocardial infarction (STEMI) patients.30 ALDH2 rs671 A allele additively increases the risk of AMI in the Japanese population.31 Zhu et al found that ALDH2 GA and AA genotypes were independent risk factors for myocardial infarction.51 ALDH2 rs671 A/A genotype is a risk factor for myocardial infarction in Japanese men.52 ALDH2 rs671 G/A and A/A genotypes were independent risk factors for myocardial infarction in elderly Korean men.53 In this study, ALDH2 rs671 G/A and A/A genotypes were independent risk factors for AMI. Our results are consistent with these findings.
In this study, individuals with A/A genotype had lower TG levels than those with G/G genotype and G/A genotype, respectively. A genome-wide association study (GWAS) showed that ALDH2 rs671 was associated with TG levels.54 Han et al found that individuals with ALDH2 G/G genotype had higher lipid levels and a higher proportion of TC disorders.55 In Japanese males, the ALDH2 rs671 variant was associated with lower HDL-C levels,56 another study from Japan showed that individuals carried ALDH2 G/G genotype had high TG levels.57 A recent meta-analysis showed that the rs671 A allele was associated with higher levels of LDL-C and lower TG and HDL-C.58 The relationship between ALDH2 polymorphism and blood lipid may be related to the process of ALDH2 participating in the metabolism of lipid aldehydes generated by lipid peroxidation to carboxylic acids. However, more researches are needed to uncover the exact mechanism.
Obesity can lead to the development of cardiovascular disease and can also directly contribute to the development of cardiovascular risk factors, including dyslipidemia, type 2 diabetes, hypertension, and atrial fibrillation.59–62 Most studies have linked obesity and being overweight to poor outcomes and the risk of death from cardiovascular disease.60,63,64 However, AMI patients with a low BMI have a worse clinical prognosis than obese patients.65 It has been suggested that underweight is also associated with a high risk of cardiac death after AMI.66 Of course, there was a contrary finding: overweight or obesity was a protective factor for AMI short- and long-term risks of death.67 Overweight (BMI 25–30 kg/m2) and obesity (BMI >30 kg/m2) status are independent risk factors for early onset of AMI.68 Obesity increased the risk of AMI in patients aged <45 years old.69 In this study, being overweight (BMI≥24.0 kg/m2) may be an independent risk factor for AMI.
Canto JG et al found that a history of hypertension is the most common manifestation in patients with myocardial infarction.70 A history of hypertension is a common risk factor for AMI.71 According to a clinical study, hypertension, smoking, diabetes, and obesity were the leading risk factors for heart attacks worldwide.72 In a study from South Korea, age, history of hypertension, diabetes, and smoking were found to be risk factors for AMI in a rural population.73 Smoking, hypertension, and obesity increased the risk of heart attack in patients aged <45 years.69 In a Chilean population study, smoking, increased ApoB/ApoAl ratio, and hypertension were found to be risk factors for AMI.74 Hypertension, smoking, and diabetes are closely associated with the occurrence of early-onset myocardial infarction.75 In the Bangladeshi population, a history of hypertension was a risk factor for AMI in the elderly population; however, there were no similar results in the younger population.76
In addition, most of the individuals with a history of alcohol consumption included in this study had mild to moderate alcohol consumption, and the results showed a history of alcoholism was a protective factor. Several studies found that light to moderate alcohol consumption was beneficial to reduce the incidence of cardiovascular and cerebrovascular diseases. A clinical study (INTERHEART) showed that regular moderate alcohol consumption was associated with a reduced incidence of AMI.72 A longitudinal study of 11,711 men with hypertension found that one standard unit of alcohol per day reduced the risk of AMI by 30%.77 Its cardiovascular protection mechanism may be related to the increase of level of serum HDL-C, the increase of fibrinolytic activity, the decrease of platelet aggregation, and the enhancement of insulin sensitivity.78,79 More clinical and basic researches are needed to uncover the relationship between the type of alcohol consumed and daily alcohol intake and cardiovascular risk.
The present study showed that overweight individuals, a history of hypertension, and ALDH2 rs671 G/A or A/A genotypes had an increased risk of developing AMI. This study had some limitations. First, the subjects included in this case-control study were all patients who visited the hospital or individuals who underwent physical examination; therefore, the selection of the population may be biased. Second, the study did not consider other possible influencing factors (such as diet, sleep quality, and physical activity). Third, because of the insufficient number of cases included in the present study, patients with AMI were not classified (such as ST‐segment elevation myocardial infarction (STEMI), and non‐ST‐segment elevation myocardial infarction (NSTEMI)) in this study, but this is one of the things we are working on.
Conclusion
In summary, overweight individuals (BMI≥24.0 kg/m2), those with a history of hypertension, and ALDH2 rs671 G/A or A/A genotypes had an increased risk of developing AMI. Revealing the characteristics and risks of AMI is of great significance for its prevention and treatment.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval
As this study was a retrospective study, it was not possible for all participants to return to the hospital to sign informed consent. All participants were informed on the study procedures and goals and the informed consent from all the participants was obtained in verbal form through the telephone communication, which was approved by the Ethics Committee of the Meizhou People’s Hospital. The study was performed under the guidance of the Declaration of Helsinki and approved by the Ethics Committee of Medicine, Meizhou People’s Hospital (Clearance No.: 2021-A-60).
Acknowledgments
The authors thank their colleagues, who were not listed in the authorship of the Center for Cardiovascular Diseases, Meizhou People’s Hospital, for their helpful comments on this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program of Meizhou (Grant No.: 2019B0202001).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Shaya GE, Leucker TM, Jones SR, Martin SS, Toth PP. Coronary heart disease risk: low-density lipoprotein and beyond. Trends Cardiovasc Med. 2022;32(4):181–194. doi:10.1016/j.tcm.2021.04.002
2. Stone PH, Libby P, Boden WE. Fundamental pathobiology of coronary atherosclerosis and clinical implications for chronic ischemic heart disease management-the plaque hypothesis: a narrative review. JAMA Cardiol. 2023;8(2):192–201. doi:10.1001/jamacardio.2022.3926
3. Reed GW, Rossi JE, Cannon CP. Acute myocardial infarction. Lancet. 2017;389(10065):197–210. doi:10.1016/S0140-6736(16)30677-8
4. Panhwar MS, Reed GW, Jain V, et al. Impella in acute myocardial infarction complicated by cardiogenic shock: history and current controversies. J Invasive Cardiol. 2022;34(10):E709–e719. PMID: 36001457.
5. Safiri S, Karamzad N, Singh K, et al. Burden of ischemic heart disease and its attributable risk factors in 204 countries and territories, 1990–2019. Eur J Prev Cardiol. 2022;29(2):420–431. doi:10.1093/eurjpc/zwab213
6. Mechanic OJ, Gavin M, Grossman SA. Acute Myocardial Infarction. In: StatPearls. StatPearls Publishing LLC; 2024. PMID: 29083808.
7. Cai M, Liu E, Bai P, et al. The chasm in percutaneous coronary intervention and in-hospital mortality rates among acute myocardial infarction patients in rural and urban hospitals in China: a mediation analysis. Int J Public Health. 2022;67:1604846. doi:10.3389/ijph.2022.1604846
8. Wu M, Wang W, Zhang X, Li J. The prevalence of acute stress disorder after acute myocardial infarction and its psychosocial risk factors among young and middle-aged patients. Sci Rep. 2022;12(1):7675. doi:10.1038/s41598-022-11855-9
9. Ridker PM. Residual inflammatory risk: addressing the obverse side of the atherosclerosis prevention coin. Eur Heart J. 2016;37(22):1720–1722. doi:10.1093/eurheartj/ehw024
10. Singh RB, Mengi SA, Xu YJ, Arneja AS, Dhalla NS. Pathogenesis of atherosclerosis: a multifactorial process. Exp Clin Cardiol. 2002;7(1):40–53. PMID: 19644578.
11. Matter MA, Paneni F, Libby P. Inflammation in acute myocardial infarction: the good, the bad and the ugly. Eur Heart J. 2024;45(2):89–103. doi:10.1093/eurheartj/ehad486
12. Sharma DJ, Nath HJ, Batta A, Goala AK. Neutrophil-to-Lymphocyte Ratio (NLR) useful as a cost-effective preliminary prognostic marker in ST-elevation myocardial infarction (STEMI): an observational study from a tertiary care hospital in northeast India. Cureus. 2023;15(3):e36885. doi:10.7759/cureus.36885
13. Jercălău CE, Andrei CL, Darabont RO, et al. Blood cell ratios unveiled: predictive markers of myocardial infarction prognosis. Healthcare. 2024;12(8):824. doi:10.3390/healthcare12080824
14. Makkar K, Sharma YP, Batta A, Hatwal J, Panda PK. Role of fibrinogen, albumin and fibrinogen to albumin ratio in determining angiographic severity and outcomes in acute coronary syndrome. World J Cardiol. 2023;15(1):13–22. doi:10.4330/wjc.v15.i1.13
15. Gupta L, Thomas J, Ravichandran R, Singh M, Nag A, Panjiyar BK. Inflammation in cardiovascular disease: a comprehensive review of biomarkers and therapeutic targets. Cureus. 2023;15(9):e45483. doi:10.7759/cureus.45483
16. Zhai X, Zhang Z, Liu W, et al. Protective effect of ALDH2 against cyclophosphamide-induced acute hepatotoxicity via attenuating oxidative stress and reactive aldehydes. Biochem Biophys Res Commun. 2018;499(1):93–98. doi:10.1016/j.bbrc.2018.03.041
17. Duan Y, Gao Y, Zhang J, et al. Mitochondrial aldehyde dehydrogenase 2 protects gastric mucosa cells against DNA damage caused by oxidative stress. Free Radic Biol Med. 2016;93:165–176. doi:10.1016/j.freeradbiomed.2016.02.001
18. Gao Y, Xu Y, Hua S, Zhou S, Wang K. ALDH2 attenuates Dox-induced cardiotoxicity by inhibiting cardiac apoptosis and oxidative stress. Int J Clin Exp Med. 2015;8(5):6794–6803. PMID: 26221217.
19. Wang W, Wang C, Xu H, Gao Y. Aldehyde dehydrogenase, liver disease and cancer. Int J Biol Sci. 2020;16(6):921–934. doi:10.7150/ijbs.42300
20. Lin CL, Chien RN, Chen LW. The aldehyde dehydrogenase ALDH2*2 allele, associated with alcohol drinking behavior, dates back to prehistoric times. Biomolecules. 2021;11(9):1376. doi:10.3390/biom11091376
21. Seike T, Chen CH, Mochly-Rosen D. Impact of common ALDH2 inactivating mutation and alcohol consumption on Alzheimer’s disease. Front Aging Neurosci. 2023;15:1223977. doi:10.3389/fnagi.2023.1223977
22. Zhao Y, Wang B, Zhang J, et al. ALDH2 (Aldehyde Dehydrogenase 2) protects against hypoxia-induced pulmonary hypertension. Arterioscler Thromb Vasc Biol. 2019;39(11):2303–2319. doi:10.1161/ATVBAHA.119.312946
23. Zhang J, Guo Y, Zhao X. The role of aldehyde dehydrogenase 2 in cardiovascular disease. Nat Rev Cardiol. 2023;20(7):495–509. doi:10.1038/s41569-023-00839-5
24. Maiuolo J, Oppedisano F, Carresi C. The generation of nitric oxide from aldehyde dehydrogenase-2: the role of dietary nitrates and their implication in cardiovascular disease management. Int J Mol Sci. 2022;23(24):15454. doi:10.3390/ijms232415454
25. Yoshida A, Rzhetsky A, Hsu LC, Chang C. Human aldehyde dehydrogenase gene family. Eur J Biochem. 1998;251(3):549–557. doi:10.1046/j.1432-1327.1998.2510549.x
26. Mizoi Y, Yamamoto K, Ueno Y, Fukunaga T, Harada S. Involvement of genetic polymorphism of alcohol and aldehyde dehydrogenases in individual variation of alcohol metabolism. Alcohol Alcohol. 1994;29(6):707–710. PMID: 7695788.
27. Perez-Miller S, Younus H, Vanam R, Chen CH, Mochly-Rosen D, Hurley TD. Alda-1 is an agonist and chemical chaperone for the common human aldehyde dehydrogenase 2 variant. Nat Struct Mol Biol. 2010;17(2):159–164. doi:10.1038/nsmb.1737
28. Chen YC, Peng GS, Tsao TP, Wang MF, Lu RB, Yin SJ. Pharmacokinetic and pharmacodynamic basis for overcoming acetaldehyde-induced adverse reaction in Asian alcoholics, heterozygous for the variant ALDH2*2 gene allele. Pharmacogenet Genomics. 2009;19(8):588–599. doi:10.1097/FPC.0b013e32832ecf2e
29. Jiang Q, Li X, Chen R, Wang C, Liu X, Wang X. Association of functional variant of aldehyde dehydrogenase 2 with acute myocardial infarction of Chinese patients. BMC Cardiovasc Disord. 2022;22(1):303. doi:10.1186/s12872-022-02738-y
30. Mizuno Y, Hokimoto S, Harada E, et al. Variant aldehyde dehydrogenase 2 (ALDH2*2) is a risk factor for coronary spasm and ST-segment elevation myocardial infarction. J Am Heart Assoc. 2016;5(5):e003247. doi:10.1161/JAHA.116.003247
31. Morita K, Miyazaki H, Saruwatari J, et al. Combined effects of current-smoking and the aldehyde dehydrogenase 2*2 allele on the risk of myocardial infarction in Japanese patients. Toxicol Lett. 2015;232(1):221–225. doi:10.1016/j.toxlet.2014.11.014
32. Wang WZ, Wang CY, Cheng YT, et al. Tracing the origins of Hakka and chaoshanese by mitochondrial DNA analysis. Am J Phys Anthropol. 2010;141(1):124–130. doi:10.1002/ajpa.21124
33. Thygesen K, Alpert JS, Jaffe AS, et al. Fourth Universal Definition of Myocardial Infarction (2018). J Am Coll Cardiol. 2018;72(18):2231–2264. doi:10.1016/j.jacc.2018.08.1038
34. Zhong Z, Hou J, Li B, et al. Genetic polymorphisms of the mitochondrial aldehyde dehydrogenase ALDH2 gene in a large ethnic Hakka population in Southern China. Med Sci Monit. 2018;24:2038–2044. doi:10.12659/msm.906606
35. He W, Li Q, Yang M, et al. Lower BMI cutoffs to define overweight and obesity in China. Obesity (Silver Spring). 2015;23(3):684–691. doi:10.1002/oby.20995
36. Tang J, Zhu X, Chen Y, et al. Association of maternal pre-pregnancy low or increased body mass index with adverse pregnancy outcomes. Sci Rep. 2021;11(1):3831. doi:10.1038/s41598-021-82064-z
37. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: executive Summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2018;71(19):2199–2269. doi:10.1016/j.jacc.2017.11.006
38. Zhou M, Astell-Burt T, Bi Y, et al. Geographical variation in diabetes prevalence and detection in China: multilevel spatial analysis of 98,058 adults. Diabetes Care. 2015;38(1):72–81. doi:10.2337/dc14-1100
39. Cai N, Li C, Gu X, et al. ALDH2 rs671 and MTHFR rs1801133 polymorphisms are risk factors for arteriosclerosis in multiple arteries. BMC Cardiovasc Disord. 2023;23(1):319. doi:10.1186/s12872-023-03354-0
40. Wu H, Huang Q, Yu Z, Zhong Z. Association of ALDH2 rs671 and MTHFR rs1801133 polymorphisms with hypertension among Hakka people in Southern China. BMC Cardiovasc Disord. 2022;22(1):128. doi:10.1186/s12872-022-02577-x
41. Liang B, Zhang XX, Li R, Zhu YC, Tian XJ, Gu N. Guanxin V alleviates acute myocardial infarction by restraining oxidative stress damage, apoptosis, and fibrosis through the TGF-β1 signalling pathway. Phytomedicine. 2022;100:154077. doi:10.1016/j.phymed.2022.154077
42. Tripathi H, Domingues A, Donahue R, et al. Combined transplantation of human MSCs and ECFCs improves cardiac function and decrease cardiomyocyte apoptosis after acute myocardial infarction. Stem Cell Rev Rep. 2023;19(2):573–577. doi:10.1007/s12015-022-10468-z
43. Liu XR, Li T, Cao L, et al. Dexmedetomidine attenuates H2O2-induced neonatal rat cardiomyocytes apoptosis through mitochondria- and ER-medicated oxidative stress pathways. Mol Med Rep. 2018;17(5):7258–7264. doi:10.3892/mmr.2018.8751
44. Ohta S, Ohsawa I. Dysfunction of mitochondria and oxidative stress in the pathogenesis of Alzheimer’s disease: on defects in the cytochrome c oxidase complex and aldehyde detoxification. J Alzheimers Dis. 2006;9(2):155–166. doi:10.3233/jad-2006-9208
45. Wei S, Zhang L, Bailu W, et al. ALDH2 deficiency inhibits Ox-LDL induced foam cell formation via suppressing CD36 expression. Biochem Biophys Res Commun. 2019;512(1):41–48. doi:10.1016/j.bbrc.2019.02.012
46. Roy B, Sundar K, Palaniyandi SS. 4-hydroxy-2-nonenal decreases coronary endothelial cell migration: potentiation by aldehyde dehydrogenase 2 inhibition. Vascul Pharmacol. 2020;131:106762. doi:10.1016/j.vph.2020.106762
47. Yang MY, Wang YB, Han B, et al. Activation of aldehyde dehydrogenase 2 slows down the progression of atherosclerosis via attenuation of ER stress and apoptosis in smooth muscle cells. Acta Pharmacol Sin. 2018;39(1):48–58. doi:10.1038/aps.2017.81
48. Wang Q, Zhou S, Wang L, et al. ALDH2 rs671 Polymorphism and coronary heart disease risk among Asian populations: a meta-analysis and meta-regression. DNA Cell Biol. 2013;32(7):393–399. doi:10.1089/dna.2013.1995
49. Han H, Wang H, Yin Z, Jiang H, Fang M, Han J. Association of genetic polymorphisms in ADH and ALDH2 with risk of coronary artery disease and myocardial infarction: a meta-analysis. Gene. 2013;526(2):134–141. doi:10.1016/j.gene.2013.05.002
50. Gu JY, Li LW. ALDH2 Glu504Lys polymorphism and susceptibility to coronary artery disease and myocardial infarction in East Asians: a meta-analysis. Arch Med Res. 2014;45(1):76–83. doi:10.1016/j.arcmed.2013.10.002
51. Zhu LP, Yin WL, Peng L, et al. Association of aldehyde dehydrogenase 2 gene polymorphism with myocardial infarction. J Inflamm Res. 2021;14:3039–3047. doi:10.2147/JIR.S311885
52. Takagi S, Iwai N, Yamauchi R, et al. Aldehyde dehydrogenase 2 gene is a risk factor for myocardial infarction in Japanese men. Hypertens Res. 2002;25(5):677–681. doi:10.1291/hypres.25.677
53. Jo SA, Kim EK, Park MH, et al. A Glu487Lys polymorphism in the gene for mitochondrial aldehyde dehydrogenase 2 is associated with myocardial infarction in elderly Korean men. Clin Chim Acta. 2007;382(1–2):43–47. doi:10.1016/j.cca.2007.03.016
54. Tan A, Sun J, Xia N, et al. A genome-wide association and gene-environment interaction study for serum triglycerides levels in a healthy Chinese male population. Hum Mol Genet. 2012;21(7):1658–1664. doi:10.1093/hmg/ddr587
55. Han S, Zhao X, Zhang X, Xu Y, Geng J, Wang Y. Acetaldehyde dehydrogenase 2 rs671 polymorphism affects hypertension susceptibility and lipid profiles in a Chinese population. DNA Cell Biol. 2019;38(9):962–968. doi:10.1089/dna.2019.4647
56. Imatoh T, Yengo L, Rocheleau G, et al. ALDH2 Polymorphism rs671, but Not ADH1B Polymorphism rs1229984, Increases Risk for Hypo-HDL-Cholesterolemia in a/a Carriers Compared to the G/G Carriers. Lipids. 2018;53(8):797–807. doi:10.1002/lipd.12087
57. Yokoyama A, Yokoyama T, Matsui T, et al. Alcohol Dehydrogenase-1B (rs1229984) and Aldehyde Dehydrogenase-2 (rs671) genotypes are strong determinants of the serum triglyceride and cholesterol levels of Japanese alcoholic men. PLoS One. 2015;10(8):e0133460. doi:10.1371/journal.pone.0133460
58. Luo Z, Cheng J, Wang Y. Effects of the genetic variants of alcohol-metabolizing enzymes on lipid levels in Asian populations: a systematic review and meta-analysis. Nutr Rev. 2023;81(8):921–938. doi:10.1093/nutrit/nuac100
59. Powell-Wiley TM, Poirier P, Burke LE, et al. Obesity and cardiovascular disease: a scientific statement from the American Heart Association. Circulation. 2021;143(21):e984–e1010. doi:10.1161/CIR.0000000000000973
60. Dikaiou P, Björck L, Adiels M, et al. Obesity, overweight and risk for cardiovascular disease and mortality in young women. Eur J Prev Cardiol. 2021;28(12):1351–1359. doi:10.1177/2047487320908983
61. Batta A, Hatwal J, Batta A, Verma S, Sharma YP. Atrial fibrillation and coronary artery disease: an integrative review focusing on therapeutic implications of this relationship. World J Cardiol. 2023;15(5):229–243. doi:10.4330/wjc.v15.i5.229
62. Gupta V, Munjal JS, Jhajj P, Jhajj S, Jain R. Obesity and atrial fibrillation: a narrative review. Cureus. 2022;14(11):e31205. doi:10.7759/cureus.31205
63. Wang M, Cao N, Zhou L, Su W, Chen H, Li H. Association of N-terminal pro-B-type natriuretic peptide levels and mortality risk in acute myocardial infarction across body mass index categories: an observational cohort study. Diabetol Metab Syndr. 2023;15(1):192. doi:10.1186/s13098-023-01163-1
64. Patlolla SH, Gurumurthy G, Sundaragiri PR, Cheungpasitporn W, Vallabhajosyula S. Body mass index and in-hospital management and outcomes of acute myocardial infarction. Medicina. 2021;57(9):926. doi:10.3390/medicina57090926
65. Yokoyama H, Tomita H, Honda S, et al. Effect of low body mass index on the clinical outcomes of Japanese patients with acute myocardial infarction - results from the prospective Japan acute myocardial infarction registry (JAMIR). Circ J. 2022;86(4):632–639. doi:10.1253/circj.CJ-21-0705
66. Su W, Wang M, Zhu J, et al. Underweight predicts greater risk of cardiac mortality post acute myocardial infarction. Int Heart J. 2020;61(4):658–664. doi:10.1536/ihj.19-635
67. Yang R, Ma W, Wang ZC, et al. Body mass index linked to short-term and long-term all-cause mortality in patients with acute myocardial infarction. Postgrad Med J. 2022;98(1161):e15. doi:10.1136/postgradmedj-2020-139677
68. Suwaidi JA, Wright RS, Grill JP, et al. Obesity is associated with premature occurrence of acute myocardial infarction. Clin Cardiol. 2001;24(8):542–547. doi:10.1002/clc.4960240804
69. Iftikhar F, Tauqeer S, Farhat S, Orakzai M, Naz R, Rehman A. Common risk factors involved in the development of myocardial infarction in adults younger than 45 years of age. J Ayub Med Coll Abbottabad. 2022;34(4):S995–s999. doi:10.55519/JAMC-04-S4-10236
70. Canto JG, Kiefe CI, Rogers WJ, et al. Atherosclerotic risk factors and their association with hospital mortality among patients with first myocardial infarction (from the National Registry of Myocardial Infarction). Am J Cardiol. 2012;110(9):1256–1261. doi:10.1016/j.amjcard.2012.06.025
71. Pedrinelli R, Ballo P, Fiorentini C, et al. Hypertension and acute myocardial infarction: an overview. J Cardiovasc Med. 2012;13(3):194–202. doi:10.2459/JCM.0b013e3283511ee2
72. Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364(9438):937–952. doi:10.1016/S0140-6736(04)17018-9
73. Lee S, Lee H, Kim HS, Koh SB. Incidence, risk factors, and prediction of myocardial infarction and stroke in farmers: a Korean nationwide population-based study. J Prev Med Public Health. 2020;53(5):313–322. doi:10.3961/jpmph.20.156
74. Lanas F, Potthoff S, Mercadal E, Santibáñez C, Lanas A, Standen D. [Individual and population risk in acute myocardial infarction: the Chilean INTERHEART study]. Rev Med Chil. 2008;136(5):555–560. PMID: 18769801.
75. Wienbergen H, Boakye D. Lifestyle and metabolic risk factors in patients with early-onset myocardial infarction: a case-control study. Eur J Prev Cardiol. 2022;29(16):2076–2087. doi:10.1093/eurjpc/zwac132
76. Alam MM, Rana MS, Hayee S, Mahjabeen F, Tasha T, Shakil SS. Comparison of risk factors between younger and older patients of myocardial infarction among bangladeshi rural people: a hospital based study. Mymensingh Med J. 2023;32(2):567–579. PMID: 37002772.
77. Beulens JW, Rimm EB, Ascherio A, Spiegelman D, Hendriks HF, Mukamal KJ. Alcohol consumption and risk for coronary heart disease among men with hypertension. Ann Intern Med. 2007;146(1):10–19. doi:10.7326/0003-4819-146-1-200701020-00004
78. Tizabi Y, Getachew B, Ferguson CL, et al. Low vs. high alcohol: central benefits vs. Detriments Neurotox Res. 2018;34(4):860–869. doi:10.1007/s12640-017-9859-x
79. Wu X, Pan B, Wang Y, Liu L, Huang X, Tian J. The protective role of low-concentration alcohol in high-fructose induced adverse cardiovascular events in mice. Biochem Biophys Res Commun. 2018;495(1):1403–1410. doi:10.1016/j.bbrc.2017.11.141
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between ALDH2 Polymorphisms and the Risk of Diabetes Mellitus in Hypertensive Patients
Zeng M, Liu Y, Xie Y
International Journal of General Medicine 2023, 16:5719-5727
Published Date: 6 December 2023
Aldehyde dehydrogenase 2 rs671 a/A Genotype is Associated with an Increased Risk of Early Onset Coronary Artery Stenosis
Rao H, Wang X, Luo Y, Liang L, Ye W, Guo X
International Journal of General Medicine 2024, 17:2407-2415
Published Date: 24 May 2024