")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Age of Diagnosis and Demographic Factors Associated with Autism Spectrum Disorders in Chinese Children: A Multi-Center Survey
Authors Long D , Yang T, Chen J, Dai Y, Chen L, Jia F, Wu L, Hao Y , Li L, Zhang J, Ke X, Yi M, Hong Q, Chen J, Fang S, Wang Y, Wang Q, Jin C, Li T
Received 15 May 2022
Accepted for publication 28 October 2022
Published 30 December 2022 Volume 2022:18 Pages 3055—3065
DOI https://doi.org/10.2147/NDT.S374840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yuping Ning
Dan Long,1 Ting Yang,1 Jie Chen,1 Ying Dai,1 Li Chen,1 Feiyong Jia,2 Lijie Wu,3 Yan Hao,4 Ling Li,5 Jie Zhang,6 Xiaoyan Ke,7 Mingji Yi,8 Qi Hong,9 Jinjin Chen,10 Shuanfeng Fang,11 Yichao Wang,12 Qi Wang,13 Chunhua Jin,14 Tingyu Li1
1Chongqing Key Laboratory of Child Nutrition and Health, Ministry of Education Key Laboratory of Child Development and Disorders, National Clinical Research Center of Child Health and Disorders, Children’s Hospital of Chongqing Medical University, Chongqing, People’s Republic of China; 2Department of Developmental and Behavioral Pediatrics, The First Hospital of Jilin University, Changchun, People’s Republic of China; 3Research Center for Child Development and Behavior, Harbin Medical University, Harbin, People’s Republic of China; 4Department of Pediatrics, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 5Department of Children Rehabilitation, Hainan Women and Children’s Medical Center, Haikou, People’s Republic of China; 6Children Health Care Center, Xi’an Children’s Hospital, Xi’an, People’s Republic of China; 7The Affiliated Brain Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 8Department of Child Health Care, The Affiliated Hospital of Qingdao University, Qingdao, People’s Republic of China; 9Maternal and Child Health Hospital of Baoan, Shenzhen, People’s Republic of China; 10Department of Child Health Care, Shanghai Children’s Hospital, Shanghai, People’s Republic of China; 11Department of Child Health Care, Children’s Hospital Affiliated of Zhengzhou University, Zhengzhou, People’s Republic of China; 12National Health Commission Key Laboratory of Birth Defect for Research and Prevention, Hunan Provincial Maternal and Child Health Hospital, Changsha, People’s Republic of China; 13Deyang Maternal and Child Health Hospital, Deyang, People’s Republic of China; 14Department of Children Health Care, Capital Institute of Pediatrics, Beijing, People’s Republic of China
Correspondence: Tingyu Li, Children’s Hospital of Chongqing Medical University, Chongqing, 400014, People’s Republic of China, Tel +86 23 63630913, Fax +86 23 63622754, Email [email protected]
Purpose: The present study investigated the age of diagnosis, treatment and demographic factors of Chinese children with autism spectrum disorders (ASD), to provide a scientific basis for the early detection, diagnosis, and intervention of ASD.
Patients and Methods: A total of 1500 ASD children aged 2– 7 years old from 13 cities in China were administered questionnaires to examine their diagnosis, treatment, and basic family information. The Childhood Autism Rating Scale (CARS) was used to measure the symptoms and severity of ASD children, and the Children Neuropsychological and Behavior Scale-Revision 2016 (CNBS-R2016) was utilized to measure neurodevelopmental levels of ASD children.
Results: We found that for children with ASD, the median (p25, p75) age for the initial detection of social behavioral developmental delay was 24 (18, 30) months, while the age for the initial diagnosis was 29 (24, 36) months and the age for the beginning of intervention was 33 (27, 42) months. Multiple linear regression (MLR) analysis suggested that in children with ASD whose parents were divorced, separated, or widowed, or whose mothers were engaged in physical work, the initial detection of social behavioral developmental delay happened later. For the children with ASD who lived in urban areas, had higher levels of ASD symptom severity or whose parents were not divorced or separated, the age for the initial diagnosis was earlier. For the children with ASD who lived in urban areas or whose mothers had received higher level of education, the earlier age for the beginning of intervention was observed, while for those with ASD whose mothers were engaged in physical work, the age for the beginning of training was later.
Conclusion: It is recommended to actively carry out health education of ASD and strengthen the support for ASD families to enhance their rehabilitation level.
Keywords: autism spectrum disorders, children, age, influencing factors, multicenter
Introduction
Autism spectrum disorders (ASD) are a group of neurodevelopmental disorders characterized by social communication disorders, repetitive stereotyped sensory-motor behavior and narrow interests, starting from early infancy.1 Since the first case of ASD was reported by an American pediatric psychiatrist Kanner in 1943, the prevalence of ASD has followed an increasing trend annually around the world. In the latest report by the US Centers for Disease Control and Prevention, it has been estimated that 23.0 per 1000 children aged 8 years suffer from ASD, which corresponds to 1 in 44 children.2 In China, the number of the children with ASD has been dramatically increasing, and although the prevalence was 0.7% in 2020,3 it is estimated to increase to 1% of the whole population (13 million people).4 ASD has become a life-long disease that may impact an individual’s quality of life and well-being. At present, one of the most important findings in the clinical study of ASD suggests that the earlier the diagnosis and the intervention result in a better relief of the core symptoms of ASD and consequently improved life quality.5 However, the delay in the detection of ASD symptoms and the diagnosis means that affected children are more prone to miss opportunities for timely interventions during periods of optimal neuroplasticity.6 Due to culture, geography and medical resources constraints, few epidemiological studies have been conducted on the age of diagnosis and treatment of ASD children in China. Therefore, we conducted the first large-sample, multi-center study aimed at investigating the age of diagnosis and treatment of children with ASD in China. We also analyzed demographic factors that influenced the age of diagnosis and treatment, to provide a reference for the early detection, early diagnosis, and early intervention in ASD.
Methods
Participants
This study is a part of the China Multi-Center Preschool Autism Project (CMPAP, Registration No. CHCTR2000031194),7 and incorporated data from 1500 children aged 2–7 years old diagnosed with ASD from 13 cities in China to investigate the early occurrence of ASD. The study was carried out between May 2018 and December 2019 and received approval from the Medical Ethics Committee of Children’s Hospital of Chongqing Medical University. It is very difficult to conduct stratified random sampling or cluster sampling because the diagnostic and therapeutic capacity of ASD varies throughout China. However, the diagnostic and therapeutic capacity of the CMPAP members Subspecialty Group of Developmental and Behavioral Pediatrics, the Society of Pediatrics, and the Chinese Medical Association is outstanding. Thanks to the locations of these institutions, which are in the major Chinese regions, the results of the study can better reflect the early occurrence of ASD children in China. Therefore, all participants were selected from 13 cities in the north (Heilongjiang, Qingdao and Changchun), east (Shanghai and Nanjing), west (Chongqing, Deyang and Xi’an), south (Shenzhen, Hainan and Hunan), and central area (Wuhan and Zhengzhou) of China. The inclusion criteria were as follows: children with ASD from sub-center outpatient clinics and local special education organizations; Based on the standard for autism formulated by Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5), those children were diagnosed by a child psychologist and a developmental-behavioral pediatrician with substantial experience in local hospitals. Due to various factors, some children with ASD only attended once and some twice. The exclusion criteria involved (1) children with brain injury, (2) those with severe somatic disorders or sensory disturbances (blind or deaf), (3) those with other independent neurodevelopmental disorders or neurological disorders, (4) those with other acute or chronic diseases. The parents of the children involved in this study all provided written informed consent.
Sample Size
The sample size calculation used the formula of infinite populations under simple random sampling:

The previous investigation of our research group showed that the average age for the initial diagnosis of ASD children was 30.2 months, and the standard deviation sigma was 13.7 months. Set alpha was 0.05, and delta was 1 month. The required sample size is 721 through calculation.
Questionnaires and Scales
The “questionnaires for basic situation of ASD children” was conducted by referring to ASD questionnaire at home and abroad. This was also combined with knowledge of the specific situation of ASD children in China. The questionnaires included the medical history and socio-economic and demographic information which were collected and completed by family members of ASD children with the assistance of well-trained professional investigators.
The CARS is a scale used to measure the symptoms and severity of children with ASD, which was compiled by E. Schopler in 1980 to be utilized for the early diagnosis of ASD; it has shown good reliability and validity.8,9 The scale consist of 15 items and was administered by professionals. The items were graded into 4 classes. Patients with a total score of 30–36 points and at least 5 items <3 points were enrolled in the mild-to-moderate group, and those with a total score of >36 points and at least 5 items >3 points were assigned to the severe group.
The CNBS-R2016 is a diagnostic assessment tool used to measure neurodevelopmental levels of children with ASD. It firstly researched and developed independently in China was revised by the Capital Institute of Pediatrics in 2016, and achieved better reliability and validity. The Cronbach’s alpha coefficient is 0.90 in Chinese version.10,11 The CNBS-R2016 was used to evaluate the degree of development of 5 major areas of behavior, including gross motor, fine motor, adaptive behavior, language and personal-social behavior. These were evaluated and graded into 5 classes by professionals. The test results represented the development quotient (DQ) with children scoring <70 points being regarded as presenting developmental delay (DD).
Quality Control
Before administering the questionnaires, investigators were trained to ensure homogeneity in the administration of the survey. Furthermore, the respondents were selected strictly according to the inclusion and exclusion criteria to ensure the accuracy of the information acquired by the questionnaires. The data were entered via independent double entry to ensure the accuracy and completeness of data.
Statistical Analysis
The data were logged into Excel 2016 software and analyzed using SPSS 26.0 software. The Kolmogorov–Smirnov goodness-of-fit test was used to test the distribution of each dataset for normality. Categorical variables were described as N (%). Continuous variables were described as median (p25, p75). The Wilcoxon and Kruskal–Wallis rank sum tests were used to analyze differences between groups. Multiple linear regression (MLR) was used to analyze socio-economic and demographic factors as well as the diagnosis and treatment situation influencing the age of diagnosis and treatment of ASD. P < 0.05 is considered to be statistically significant in this study.
Results
Basic Situation
Among the 1500 children with ASD, 1228 (81.9%) cases were male; with the male-to-female ratio being 4.5:1. The average age of the investigated children was (50.63±15.99) months. The median age for the initial detection of social behavioral developmental delay was 24 (18, 30) months, and the cases aged less than or equal to 24 months accounted for 56.1%. The median age for the initial diagnosis was 29 (24, 36) months, and the cases aged less than or equal to 36 months accounted for 76.3%. The median age for the beginning of intervention was 33 (27, 42) months, and the cases aged less than or equal to 36 months accounted for 61.7%. Children with a 0–3 months of interval time between initial diagnosis and intervention accounted for 40.3% (527/1308); those with an interval time of 4–6 months accounted for 20.3% (265/1308); those with an interval time of 7–12 months for 14.8% (193/1308); those with an interval time of 13–24 months for 14.1% (184/1308) and finally, those with an interval time of more than 24 months for 10.6% (139/1308).
Correlations Between the Age of Diagnosis and Treatment of ASD and Socio-Economic and Demographic Factors
For the children with ASD who lived in urban areas, the age for initial diagnosis and the beginning of intervention was earlier (P < 0.05). For the children with ASD whose parents were not divorced or separated, an earlier age for the initial detection of social behavioral developmental delay and initial diagnosis was found (P < 0.05). For the children with ASD whose parents received higher level of education, an earlier age for the beginning of intervention was observed (P < 0.05), while for children with ASD whose mothers were engaged in physical work, the age for the initial detection of social behavioral developmental delay and the beginning of intervention was later (P < 0.05) (see Table 1).
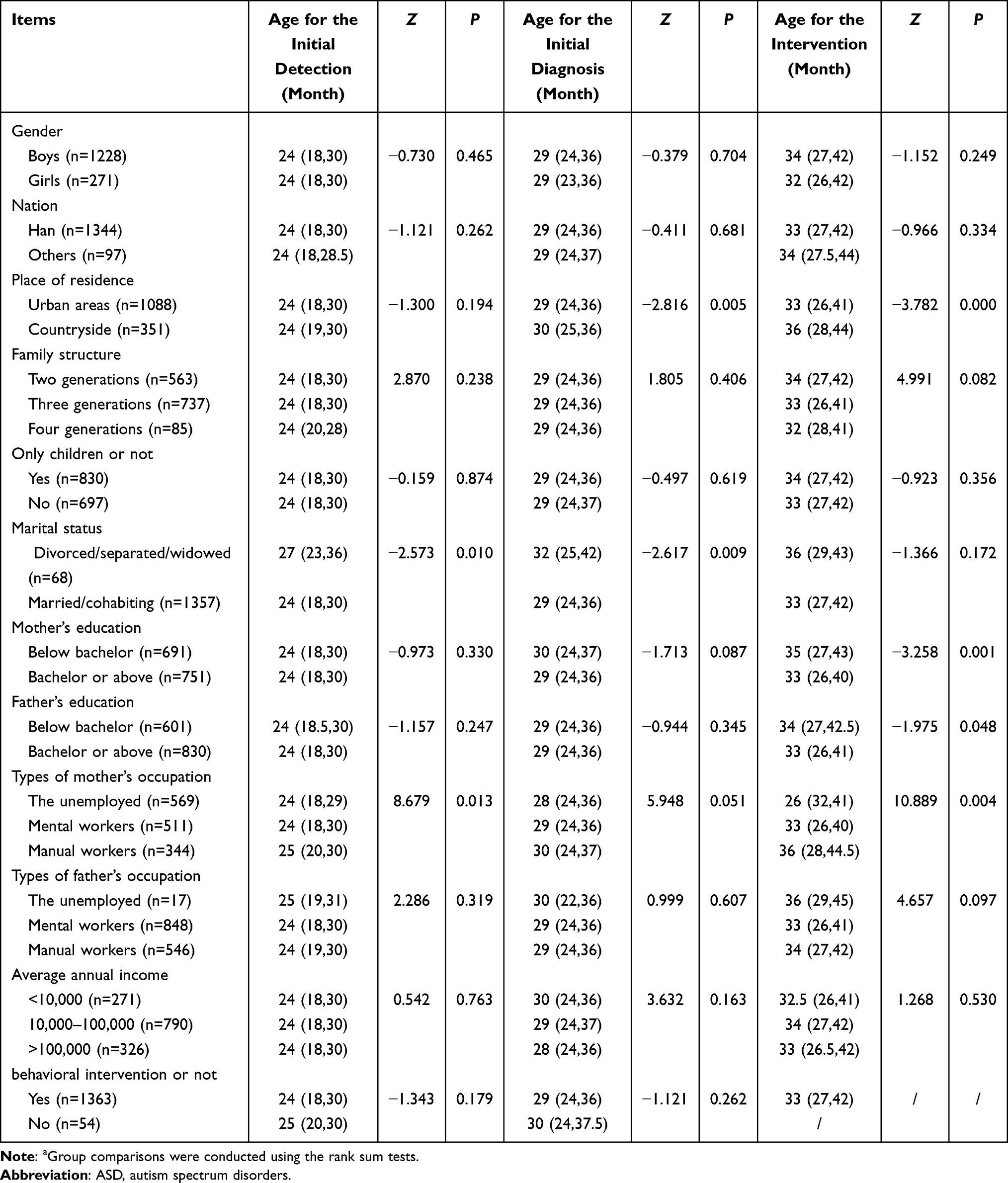 |
Table 1 Analysis of Socio-Economic and Demographic Factors Affecting the Age of ASD Diagnosis and Treatment [M(p25, p75)]a |
Correlations Between the Age of Diagnosis and Treatment of ASD and Disease Severity and Diagnosis
According to the grading results of CARS, ASD children were divided into two groups: the mild-to-moderate group and the severe group. There were no significant differences in the age for the initial detection of social behavioral developmental delay and for the beginning of intervention between the two groups (P > 0.05). However, the age for the initial diagnosis in the severe group was earlier than that in the mild-to-moderate group (P < 0.05) (see Table 2).
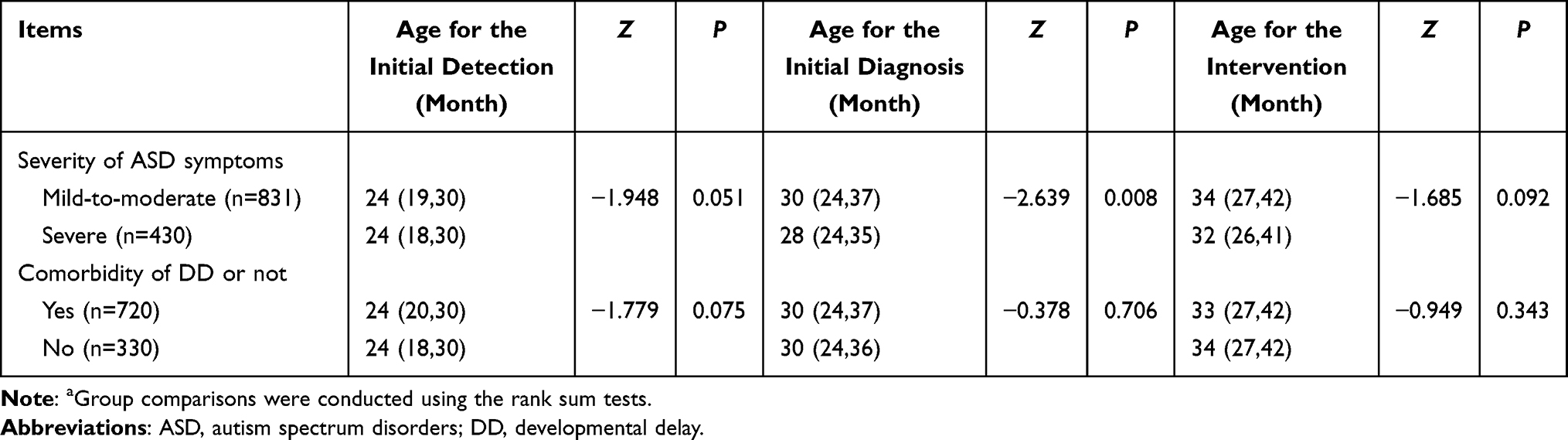 |
Table 2 Relationship Between Age at Diagnosis and Treatment of ASD and Autism Symptom Severity and Diagnosis [M (p25, p75)]a |
According to the grading results of CNBS, ASD children were divided into two groups: the ASD + DD group and the ASD group. Differences between the two groups in the time interval between initial diagnosis and intervention were statistically significant (P < 0.05) (see Table 3).
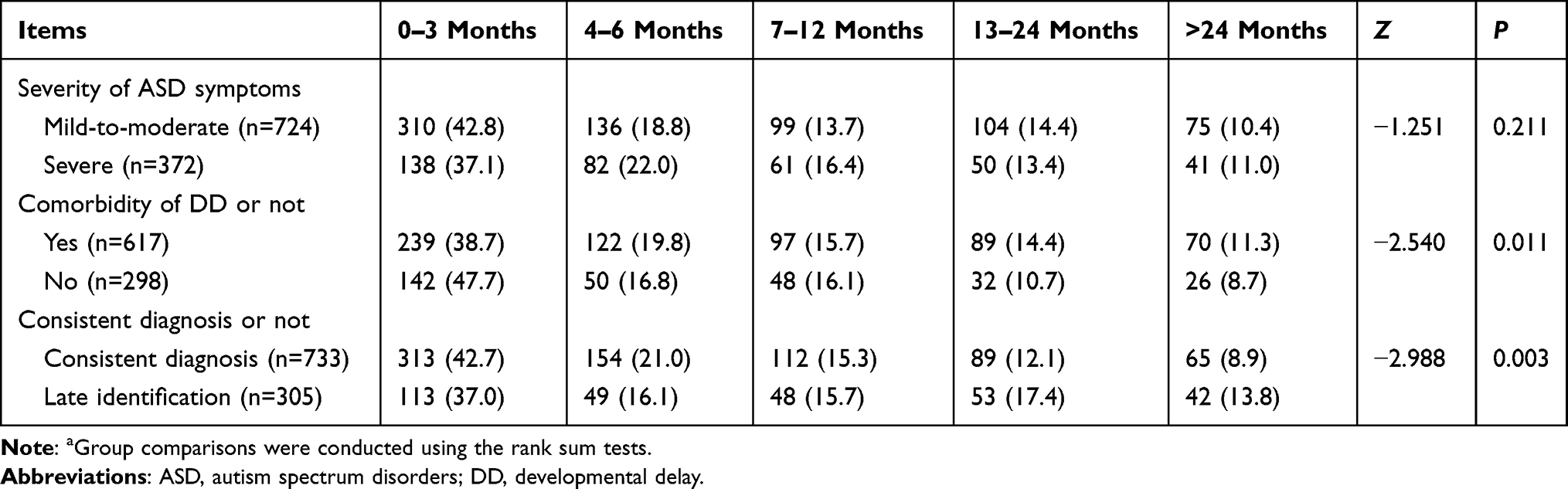 |
Table 3 Analysis of the Diagnostic Factors Influencing the Interval Between Diagnosis and Treatment of ASD [n, (%)]a |
If children were diagnosed with ASD both at the first and second visit, the results were considered as “consistent diagnosis”. Conversely, if cases were diagnosed with another condition at the first visit and with ASD at the second visit, the results were considered as “late identification”. Children who only attended once were excluded. Among 1038 children with ASD, cases with consistent diagnosis accounted for 70.6%, and cases with late identification for 29.4%. Differences between the two groups in the interval time between initial diagnosis and intervention were statistically significant (P < 0.05) (see Table 3).
Multivariate Analysis of Factors Influencing the Age of Diagnosis and Treatment of ASD
Based on previous research reports and clinical theories,12,13 it is considered that whether ASD children are only children may be related to their age of diagnosis and treatment. Thus, eight factors could potentially influence the age of diagnosis and treatment of ASD including living places, only children vs siblings, parental marital status, education background, mothers’ occupation, severity of ASD symptoms and comorbidity of developmental disorders were further analyzed by MLR.
The results revealed that later age for the initial detection of social behavioral developmental delay was found for the children with ASD whose parents were divorced, separated, or widowed, or whose mothers were engaged in physical work (see Table 4). For the children with ASD who lived in urban areas, with higher levels of ASD symptom severity or whose parents were not divorced or separated, the age for the initial diagnosis was earlier (see Table 5). For the children with ASD who lived in urban areas or whose mothers received higher level of education, an earlier age for the beginning of intervention was observed, while for those with ASD whose mothers were engaged in physical work, the age for the beginning of intervention was later (see Table 6).
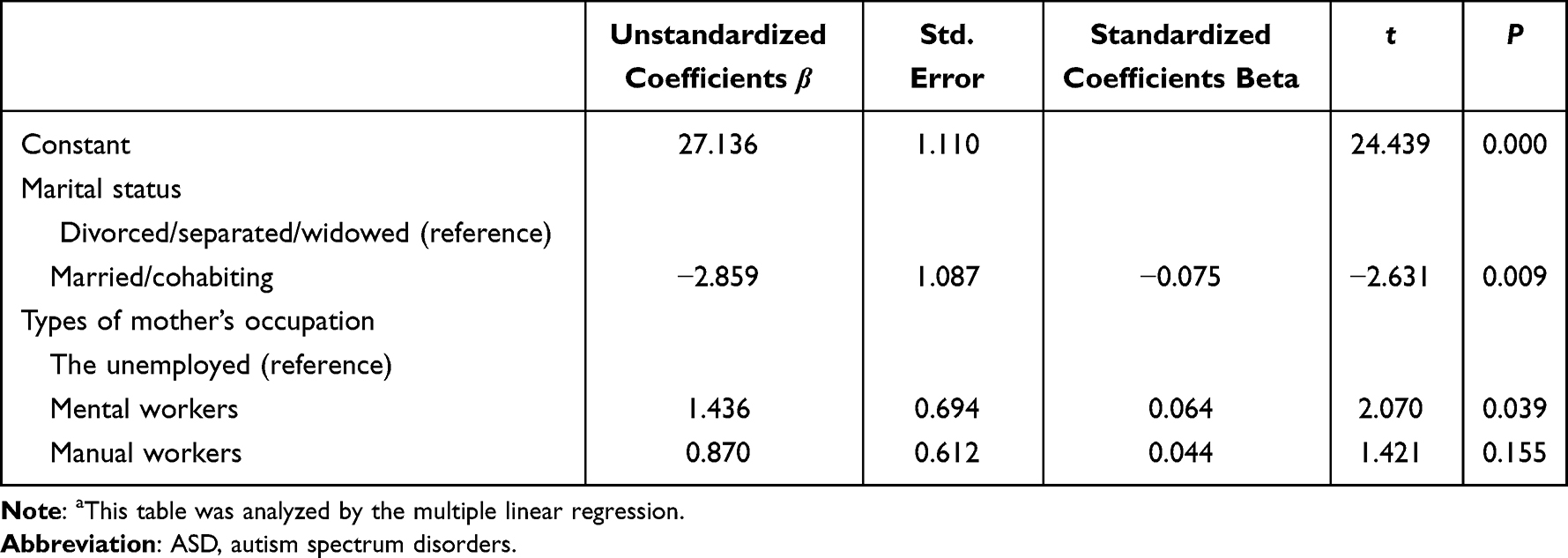 |
Table 4 A Multiple Linear Regression Analysis of Influencing Factors of Age at First Found Social Backwardness in ASDa |
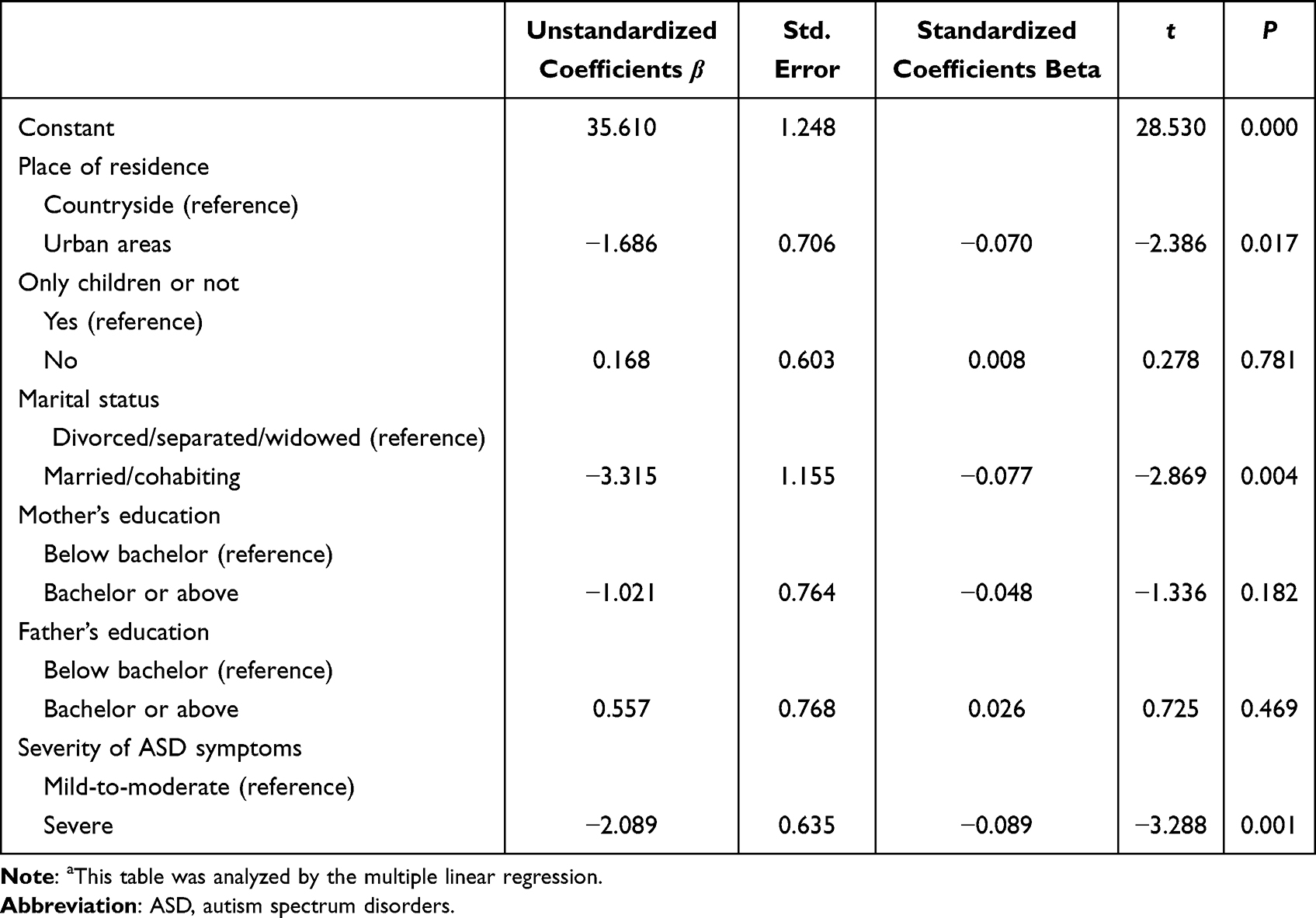 |
Table 5 A Multiple Linear Regression Analysis of Influencing Factors of Age at the First Diagnosis of ASDa |
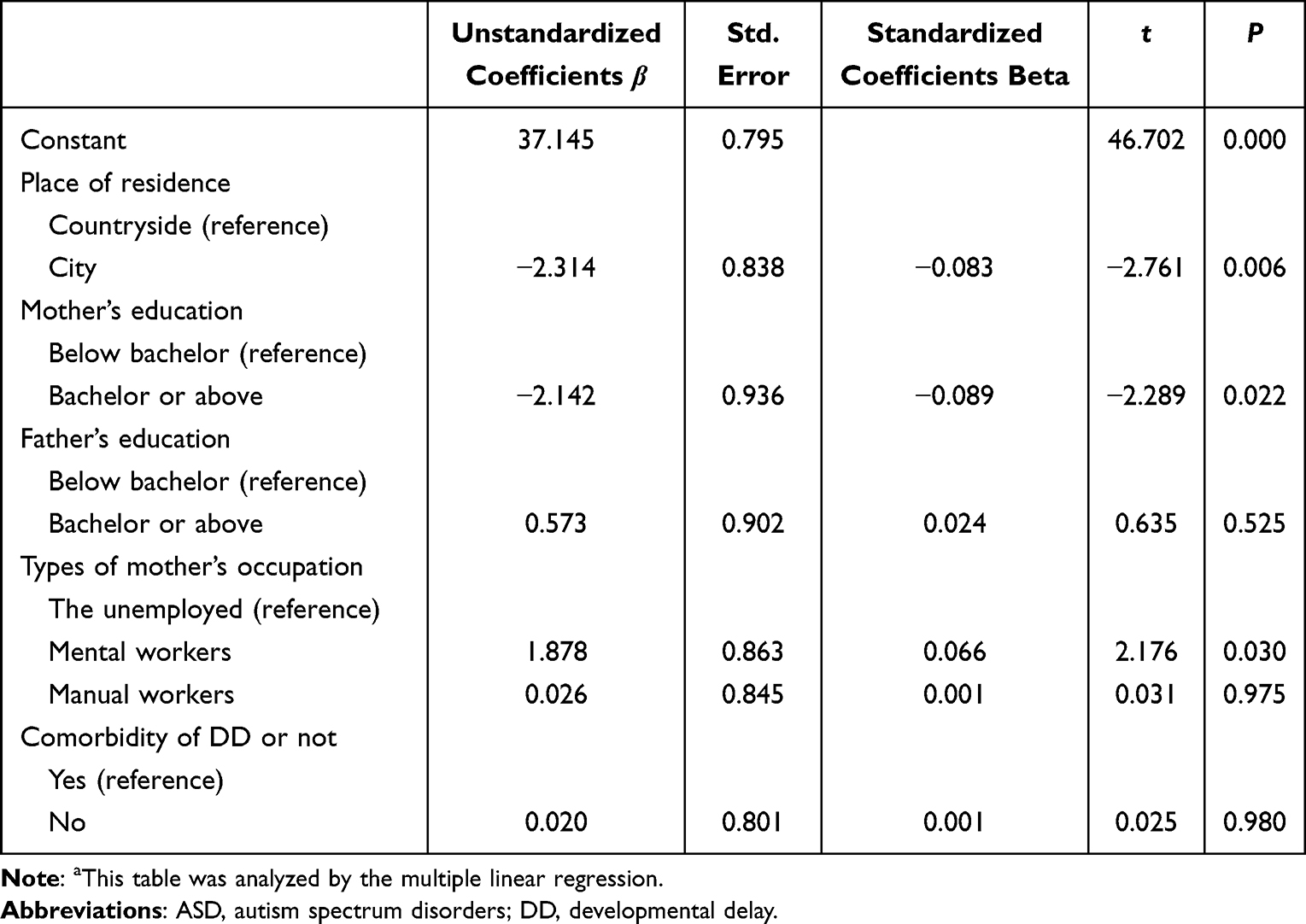 |
Table 6 A Multiple Linear Regression Analysis of Influencing Factors of Age at Initial Intervention of ASDa |
Discussion
The main purposes of this study were to investigate the age of diagnosis and treatment of children with ASD in China and analyze demographic factors, which can provide a reference for the early detection, diagnosis, and intervention of ASD.
Basic Situation of ASD Children
In the present survey, as has been shown in similar studies in China and foreign countries, male children were about 4.5 times more likely to be diagnosed with ASD than female children.14,15 The reason for the gender differences among children with ASD remains unclear and is currently considered to be related to sex-linked genes, sex hormone levels and maternal environment during pregnancy.16 A recent study on 1410 ASD children aged 4 years and above from 18 European countries showed that (controlling for language ability), female children are diagnosed later than male children.17 However, in the present survey, no correlation between gender factors and age of diagnosis and treatment of ASD was found, and this is consistent with conclusions made in most previous studies.12,18,19 The above different results may be related to differences in the sample age, sample size and regions, and therefore, the influence of gender on the age of diagnosis and treatment of ASD should be further investigated in the future.
Detection of Social Behavioral Developmental Delay of ASD Children
In recent years, the results of studies from China and other countries have indicated that in about 70% of children later diagnosed with ASD the initial symptoms occurred before 24 months of age. These symptoms mainly include social communication disorders (ie, ignoring people and refusing to speak or to make eye contact).20,21 In this survey, the age for the initial detection of social behavioral developmental delay of ASD children was ranged between 18 and 30 months. More specifically, 56% of the children were detected at less than or equal to 24 months of age. However, in children with ASD whose parents were divorced, separated, or widowed, or whose mothers were engaged in physical work, the age for the initial detection of social behavioral developmental delay was later. The reason may be that those parents paid less attention to the early development of children with ASD due to inharmonious family relationships and that might have driven the later age for the initial detection of social behavioral developmental delay. Given that the particular roles of mothers and fathers in the child-rearing process are shaped by the traditional Chinese culture, there are significant gender differences in how they perceive child-rearing pressures.22 Usually, mothers play the main role in child-rearing23 and if mothers are engaged in the physical work, not only will the opportunities for emotional exchanges and positive interaction with children be relatively reduced, but also the initial symptom may be easily ignored due to their poor recognition of signs suggestive of ASD. Consequently, this may result in the later age for the initial detection of social behavioral developmental delay. Hence, it is recommended that a favorable and harmonious family atmosphere, increased parents-child activities, and attention to the early development of children must be fostered.
Initial Diagnosis of ASD Children
Although ASD can be diagnosed at very early stages when children are 18 months,5 the ages for ASD diagnosis in most developed countries are later than that. From 2004 to 2014, the age for diagnosis of the British children with ASD was 55 months; in the past decade, this figure has not yet been reduced, indicating that the rate of early identification has remained stagnant.18 In two national surveys in the USA (2017), it was reported that most children’s ASD diagnoses were confirmed after the age of 3 and that between 1/3 and 1/2 were confirmed after 6 years old. Furthermore, those with mild ASD were diagnosed between the age of 5.6 and 8.6 years old while severe ASD cases were confirmed at preschool age (3.7–4.5 years old).24 In the latest meta-analysis, it was shown that around the world, the average age for ASD diagnosis is 60.48 months; 43.18 months among children less than 10 years old.25 In this survey, the age for the initial diagnosis of the children with ASD was between 24 and 36 months, similar to the previous survey results in China,12,13 indicating that although the initial research on ASD is late in China, the positive popularization spread of information in recent years has contributed to the recent achievements in the clinical practice of ASD.
Recently, multiple studies have confirmed that individuals, families and society are related to the early diagnosis of ASD, but most results are controversial or have not been further discussed yet.25 The present study found that for the children with ASD whose parents were not divorced or separated, the age for the initial diagnosis was earlier. A possible interpretation of these results could be that parents were in stable relationships and paid more attention to children’s abnormal features, making it easier for them to detect ASD symptoms at an earlier stage and be treated in time. This study also revealed that the median age for the ASD diagnosis in the mild-to-moderate group was 30 (24, 37) months compared to that of the severe group which was 28 (24, 35) months. Overall, consistent with the results of previous studies,17,26,27 greater the ASD symptom severity is associated with the earlier the age for the initial diagnosis. The reason may be that abnormal behaviors occur earlier in children with higher levels of ASD symptom severity, and therefore, the differences with other typically developing children of similar ages are more marked and easily noticed by parents, thus promoting active intervention and early diagnosis. Some children with mild-to-moderate ASD are allowed to go to school because of no significant differences with other typically developing children of similar age, which leads to delayed diagnosis. The present study revealed that the age for the initial diagnosis of ASD in children who lived in urban areas was earlier compared to children who lived in rural areas. The reason may be that compared with rural areas, children in urban areas have better access to medical resources. Furthermore, this may be also related to the parents’ socio-economic status, consistent with results from other studies in China and foreign countries.12,27,28 Therefore, the promotion of education about ASD should be strengthened to improve parental awareness and attention to the early signs of ASD. Meanwhile, aspects such as team building and professional training for domestic pediatricians should be enhanced and the development of all children should be monitored so that ASD can be identified at the earlier stages to ensure that key treatment opportunities are not delayed.
In this study, unlike some previous studies,27 the effect of comorbidity of other developmental disorders seemed to not influence the age for the initial diagnosis of ASD. This inconsistency may be due to the differences in the sample age, sample size and measurement tools. Therefore, the influence of comorbidity on the age for diagnosis should be further discussed in the future.
Intervention Situation of ASD Children
It is universally acknowledged that early intervention, especially behavioral intervention, can ameliorate core symptoms and whole function of ASD children, overall producing a better long-term prognosis. However, because of the missed diagnosis, delayed diagnosis, complex transfer treatment, living in rural areas, and low socio-economic status of parents of ASD children, the best time for intervention is often missed.13,29–33 This study showed that, the age for the beginning of intervention in children with ASD who lived in urban areas, and whose mothers were not engaged in physical work or had received high education at college-level education and above was earlier. However, it was also found that children without intervention treatment half a year after the initial diagnosis accounted for over 1/3 of all cases, while about 1/4 of the children did not receive intervention treatment even after one year from the initial diagnosis, and were influenced by comorbidity of developmental disorders and the diagnostic stability of ASD. Therefore, delayed intervention treatment is a common problem in Chinese children with ASD and the reasons proposed include: (1) If children with ASD live far away from the special education institutes, the treatment cost is higher and the family burden is heavier and treatment starts later. (2) Because of the little understanding of ASD as a life-long disorder and the influence of the Chinese traditional concept that children who start to speak late will be blessed, some parents believe that as children grow up, the abnormal behaviors will naturally improve and therefore do not seek help. (3) Some parents do not accept the diagnosis and often pursue a second diagnosis in other medical institutions or seek drug treatment, preventing the children from receiving the appropriate intervention timely treatments. (4) Due to insufficient experience in ASD by some pediatricians, ASD diagnosis in children with mild symptoms and normal intelligence may be missed or confused with other developmental disorders. (5) Currently, there is an inadequate supply of proper special education institutes falls short of demand in China, so many children with ASD have to book in advance and wait for a long time before receiving the intervention training. Given the reasons highlighted above, the following suggestions are proposed to promote early intervention in treating ASD children: (1) The promotion and education about ASD need to be improved. Alongside, it is recommended that economic supports and employment opportunities for ASD families should be strengthened by implementing support policies for families of ASD children. (2) The level of knowledge and training of domestic pediatricians in the identification and diagnosis of ASD and common comorbidities should be further improved to reduce the rate of missed diagnosis. (3) More professional special education institutes should be established to improve the system for the diagnosis, treatment, and rehabilitation of ASD, so that children with ASD will be treated effectively at the early stage, thus improving prognosis.
Conclusion
In conclusion, the age of diagnosis and treatment of children with ASD in China is affected by the severity of ASD symptoms and demographic factors, the problems of missed diagnosis, delayed diagnosis and delayed intervention of ASD also exist. Given the great importance of early detection, diagnosis and intervention, the following recommendation are provided to actively carry out promotion and education of ASD; to improve people’s understanding of ASD; to improve diagnosis and identification levels of domestic developmental-behavioral pediatricians for ASD; to perform ASD screening among children with suspected developmental retardation; to strengthen supervision and establishment of rehabilitation facilities and special schools; and to provide economic and employment supports for ASD families to reduce their living burdens.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by the Medical Ethics Committee of Children’s Hospital of Chongqing Medical University. All procedures performed were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The patients/participants provided their written informed consent to participate in this study.
Acknowledgment
We thank all participants who devote their time and excellent cooperation to our study. We also thank EditSprings (https://www.editsprings.com/) for the expert linguistic services provided.
Author Contributions
DL, and TL conceptualized and designed the study. DL, TL, YD, LC, FJ, LW, YH, LL, JZ, XK, MY, QH, JC, SF, YW, QW, and CJ recruited the participants and completed the screening assessments. DL analyzed the data, and wrote the first draft of the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in revising or critically reviewing the article; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (Nos. 81771223, 81770526), the Science and technology major project of Guangdong (2018b03035001), and the Science and technology major project of Guangzhou (202007030002).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Constantino JN, Charman T. Diagnosis of autism spectrum disorder: reconciling the syndrome, its diverse origins, and variation in expression. Lancet Neurol. 2016;15(3):279–291. doi:10.1016/s1474-4422(15)00151-9
2. Maenner M, Shaw K, Bakian A, et al. Prevalence and characteristics of autism spectrum disorder among children aged 8 Years — autism and developmental disabilities monitoring network, 11 Sites, United States, 2018. MMWR Surveill Summ. 2021;70(11):1–16. doi:10.15585/mmwr.ss7011a1
3. Zhou H, Xu X, Yan W, et al. Prevalence of autism spectrum disorder in China: a nationwide multi-center population-based study among children aged 6 to 12 years. Neurosci Bull. 2020;36(9):961–971. doi:10.1007/s12264-020-00530-6
4. Sun X, Allison C, Wei L, et al. Autism prevalence in China is comparable to Western prevalence. Mol Autism. 2019;10:7. doi:10.1186/s13229-018-0246-0
5. Hyman SL, Levy SE, Myers SM. Identification, evaluation, and management of children with autism spectrum disorder. Pediatrics. 2020;145:1. doi:10.1542/peds.2019-3447
6. Courchesne E, Pramparo T, Gazestani VH, Lombardo MV, Pierce K, Lewis NE. The ASD living biology: from cell proliferation to clinical phenotype. Mol Psychiatry. 2019;24(1):88–107. doi:10.1038/s41380-018-0056-y
7. Yang T, Zhu J, Li Q, et al. China Multi-Center Preschool Autism Project (CMPAP): design and methodologies to identify clinical symptom features and biomarkers of autism spectrum disorders. Front Psychiatry. 2020;11:613519. doi:10.3389/fpsyt.2020.613519
8. Lu J, Yang Z, Shu M, Su L. Reliability, validity, analysis of children autism rating scale. China J Mod Med. 2004;14(13):119–123. doi:10.3969/j.issn.1005-8982.2004.13.037
9. Lord C, Elsabbagh M, Baird G, Veenstra-Vanderweele J. Autism spectrum disorder. Lancet. 2018;392(10146):508–520. doi:10.1016/s0140-6736(18)31129-2
10. Jin C, Li R, Zhang L, et al. The revision and according validity research of China development scale for children. Chin J Child Health Care. 2014;22(12):1242–1246. doi:10.11852/zgetbjzz2014-22-12-04
11. Li R, Jin C, Zhang L, et al. Psychometric analysis of the “China development scale for children” (aged 4~6 years old). Chin J Child Health Care. 2015;23(9):934–936. doi:10.11852/zgetbjz2015230912
12. Li W, Liu X, Dai Y, Cheng Q. Age of diagnosis of autism spectrum disorder in children and factors influencing the age of diagnosis. Chin J Contemp Pediatr. 2018;20(10):799–803. doi:10.7499/j.issn.1008-8830.2018.10.003
13. Yang T, Zhu J, Guo M, et al. Family related factors in diagnosis and treatment of autism spectrum disorder in Chongqing. J Bio-Education. 2018;6(4):197–201. doi:10.3969/j.issn.2095-4301.2018.04.005
14. Loomes R, Hull L, Mandy WPL. What is the male-to-female ratio in autism spectrum disorder? A systematic review and meta-analysis. J Am Acad Child Adolesc Psychiatry. 2017;56(6):466–474. doi:10.1016/j.jaac.2017.03.013
15. Dai Q, Xu H, Wang H, Zhao Z, Zhang X, Zhou A. Prevalence of autism spectrum disorder in Chinese from 2010 to 2016: a meta-analysis. Chin J Child Health Care. 2017;25(12):1243–1246. doi:10.11852/zgetbjzz2017-25-12-16
16. Schaafsma SM, Pfaff DW. Etiologies underlying sex differences in autism spectrum disorders. Front Neuroendocrinol. 2014;35(3):255–271. doi:10.1016/j.yfrne.2014.03.006
17. Salomone E, Charman T, Mcconachie H, Warreyn P. Child’s verbal ability and gender are associated with age at diagnosis in a sample of young children with ASD in Europe. Child Care Health Dev. 2016;42(1):141–145. doi:10.1111/cch.12261
18. Brett D, Warnell F, McConachie H, Parr JR. Factors affecting age at ASD diagnosis in UK: no evidence that diagnosis age has decreased between 2004 and 2014. J Autism Dev Disord. 2016;46(6):1974–1984. doi:10.1007/s10803-016-2716-6
19. Fountain C, King MD, Bearman PS. Age of diagnosis for autism: individual and community factors across 10 birth cohorts. J Epidemiol Community Health. 2011;65(6):503–510. doi:10.1136/jech.2009.104588
20. He Y, Yang Y, Shao D, et al. Case-control study on clinical features and influencing factors of children with autism spectrum disorders. Chin J Appl Clinl Pediatr. 2017;32(8):607–612. doi:10.3760/cma.j.issn.2095-428X.2017.08.012
21. Parmeggiani A, Corinaldesi A, Posar A. Early features of autism spectrum disorder: a cross-sectional study. Ital J Pediatr. 2019;45(1):144. doi:10.1186/s13052-019-0733-8
22. Hu X, Han ZR, Bai L, Gao MM. The mediating role of parenting stress in the relations between parental emotion regulation and parenting behaviors in Chinese families of children with autism spectrum disorders: a dyadic analysis. J Autism Dev Disord. 2019;49(10):3983–3998. doi:10.1007/s10803-019-04103-z
23. Dardas LA, Ahmad MM. Predictors of quality of life for fathers and mothers of children with autistic disorder. Res Dev Disabil. 2014;35(6):1326–1333. doi:10.1016/j.ridd.2014.03.009
24. Sheldrick RC, Maye MP, Carter AS. Age at first identification of autism spectrum disorder: an analysis of two US surveys. J Am Acad Child Adolesc Psychiatry. 2017;56(4):313–320. doi:10.1016/j.jaac.2017.01.012
25. van ‘t Hof M, Tisseur C, van Berckelear-Onnes I, et al. Age at autism spectrum disorder diagnosis: a systematic review and meta-analysis from 2012 to 2019. Autism. 2020;25(4):862–873. doi:10.1177/1362361320971107
26. Montiel-Nava C, Chacín J, González-ávila Z. Age of diagnosis of autism spectrum disorder in Latino children: the case of Venezuelan children. Autism. 2017;21(5):573–580. doi:10.1177/1362361317701267
27. Mazurek M, Handen B, Wodka E, Nowinski L, Butter E, Engelhardt C. Age at first autism spectrum disorder diagnosis: the role of birth cohort, demographic factors, and clinical features. J Dev Behav Pediatr. 2014;35(9):561–569. doi:10.1097/dbp.0000000000000097
28. Mandell DS, Novak MM, Zubritsky CD. Factors associated with age of diagnosis among children with autism spectrum disorders. Pediatrics. 2005;116(6):1480–1486. doi:10.1542/peds.2005-0185
29. Towle PO, Patrick PA, Ridgard T, Pham S, Marrus J. Is earlier better? The relationship between age when starting early intervention and outcomes for children with autism spectrum disorder: a selective review. Autism Res Treat. 2020;2020:17. doi:10.1155/2020/7605876
30. Darcy-Mahoney A, Minter B, Higgins M, Guo Y, Zauche LH, Hirst J. Maternal and neonatal birth factors affecting the age of ASD diagnosis. Newborn Infant Nurs Rev. 2016;16(4):340–347. doi:10.1053/j.nainr.2016.09.033
31. Aggarwal S, Angus B. Misdiagnosis versus missed diagnosis: diagnosing autism spectrum disorder in adolescents. Australas Psychiatry. 2015;23(2):120–123. doi:10.1177/1039856214568214
32. Dinora P, Bogenschutz M, Lynch K. Factors that may influence parent treatment decision making for young children with autism spectrum disorder. J Soc Work Disabil Rehabil. 2017;16(3–4):377–395. doi:10.1080/1536710X.2017.1392395
33. Elder JH, Brasher S, Alexander B. Identifying the barriers to early diagnosis and treatment in underserved individuals with autism spectrum disorders (ASD) and their families: a qualitative study. Issues Ment Health Nurs. 2016;37(6):412–420. doi:10.3109/01612840.2016.1153174
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.