")
Back to Journals » International Journal of General Medicine » Volume 16
Age and Sex Differences in LDL Cholesterol Distribution in Adults in Malaysia: A Cross-Sectional Study (2010–2021)
Authors Chalitsios CV , Akyea RK , Abdul-Hamid H, Leonardi-Bee J, Kanchau JD, Kamal A, Mohamed-Yassin MS , Baharudin N, Ramli AS , Qureshi N
Received 26 May 2023
Accepted for publication 27 September 2023
Published 12 December 2023 Volume 2023:16 Pages 5885—5888
DOI https://doi.org/10.2147/IJGM.S423091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Christos V Chalitsios,1,* Ralph K Akyea,2,* Hasidah Abdul-Hamid,2,3 Jo Leonardi-Bee,1,4 Johanes D Kanchau,5 Aisyah Kamal,5 Mohamed-Syarif Mohamed-Yassin,3 Noorhida Baharudin,3,5 Anis Safura Ramli,3,5 Nadeem Qureshi2
1Nottingham Centre for Epidemiology and Public Health, Lifespan and Population Health Unit, School of Medicine, University of Nottingham, Nottingham, UK; 2PRISM Research Group, Centre for Academic Primary Care, Lifespan and Population Health Unit, School of Medicine, University of Nottingham, Nottingham, UK; 3Department of Primary Care Medicine, Faculty of Medicine, Universiti Teknologi MARA, Sungai Buloh, Selangor, Malaysia; 4Centre for Evidence-Based Medicine, Faculty of Medicine and Health Sciences, University of Nottingham, Nottingham, UK; 5Institute of Pathology, Laboratory and Forensic Medicine (I‑PPerForM), Universiti Teknologi MARA, Sungai Buloh, Selangor, Malaysia
*These authors contributed equally to this work
Correspondence: Nadeem Qureshi, Centre for Academic Primary Care, School of Medicine, University of Nottingham, Nottingham, UK, Email [email protected]
Introduction
Cardiovascular disease (CVD) is the leading cause of death worldwide. Hypercholesterolaemia, especially higher low-density lipoprotein cholesterol (LDL-c), has been recognised as one of the major key risk factors for CVD.1 Lipid-lowering treatments, such as statins, have been shown to impact both primary and secondary cardiovascular prevention.2
In Europe and America, the prevalence of hypercholesterolaemia in adults was 53.7% and 47.7%, respectively, with a lower prevalence in Southeast Asia (30.3%) and Africa (23.1%).3 In Malaysia, there is an increasing trend in the prevalence of hypercholesterolaemia, with a recent prospective study of 11,288 adults reporting a prevalence of 64.0% (95% confidence interval (CI) 63.0–65.0%) and 56.7% (95% CI 55.7–57.7%) for elevated total cholesterol (ie, > 5.2 mmol/L) and elevated LDL-c (ie, > 3.4 mmol/L), respectively.4
Establishing the mean LDL-c for each age range in the population is vital for preventive and management strategies for hypercholesterolaemia. In Europe and North America, the mean LDL-c is well established,5,6 however; the mean LDL-c level among the primary care population in Malaysia is not well established.
This study, therefore, aimed to describe the mean LDL-c levels in the Malaysian primary care adult population and additionally describe the age and sex differences in the mean LDL-c levels.
Materials and Methods
A cross-sectional study was conducted in 11 out of the 21 Ministry of Health primary care clinics in Selangor, Putrajaya and Kuala Lumpur in Malaysia. Of the 11 primary care clinics involved in this study, 6 were in Selangor, and the remaining 5 were in Kuala Lumpur and Putrajaya. Demographic data (age and gender) and LDL-c readings from 2010 to 2021 were electronically extracted from the electronic medical record (EMR). Adult patients aged ≥18 years old with LDL-c results recorded in the EMR system were included in this study. Patients with missing information on age and/or sex were excluded. The study setting and population have been previously described in detail.7
Descriptive analyses were conducted to describe the mean LDL-c levels overall and by sex stratified by 10-year age band. Baseline characteristics were presented as frequencies with percentages, means with standard deviation (SD) or medians with interquartile ranges. Analyses were performed using R statistical software (version 4.0.5).
Results
A total of 139,702 participants were included in the analysis. The number of study participants from each primary care clinic varied, ranging from 6189 (4.4%) to 19,781 (14.2%). The mean age was 58.4 ± 14.2 (range, 18 to 108) years old, with the majority of participants being women (54.4%) (Table 1). The mean (SD) LDL-c level of the overall population was 3.5 (1.10) mmol/l. The mean LDL-c levels ranged from 3.0 to 3.7 mmol/L and 3.2 to 3.8 mmol/L in men and women, respectively (Figure 1). Women aged 50 to 59 years had the highest overall mean LDL-c level (3.8 mmol/L), while the highest mean LDL-c in men (3.7 mmol/L) was in those aged 30 to 49 years. Men had higher LDL-c levels compared to women between 18 to 39 years old; however, this was reversed after the age of 50 years old.
 |
Table 1 Baseline Characteristics of the Study Population |
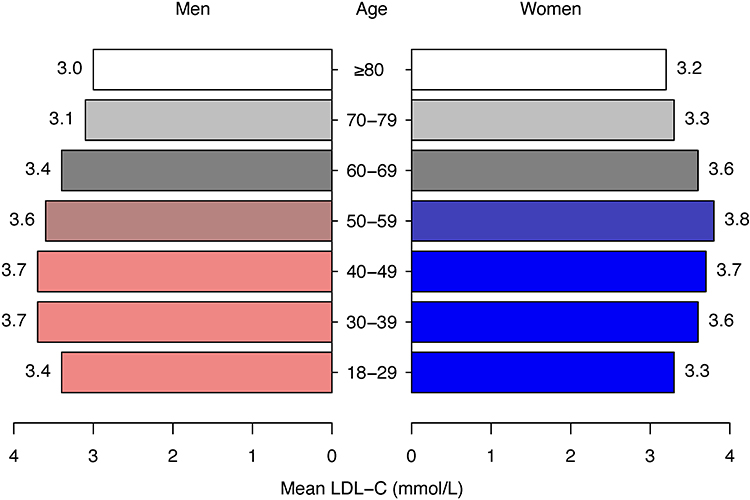 |
Figure 1 Mean LDL-c (mmol/L) stratified by 10-year age bands and sex. |
Discussion
This study using electronic medical records from 11 primary care clinics in Malaysia found that the highest mean LDL-c levels were in individuals aged 30 to 59 years old. Additionally, we observed sex and age-related variations in LDL-c levels. Men had higher LDL-c levels compared to women between the ages of 18 to 39 years old. However, this pattern was reversed after the age of 50 years, with women having higher LDL-c levels. Furthermore, we found a consistent decline in LDL-c measurements after the age of 60 years in our study population.
Relationship with Other Literature
Our findings align with previous research, particularly a prospective study of 11,288 Malaysian adults, which reported similar mean LDL-c levels across the various age groups. The highest mean LDL-c level reported in this Malaysian study was 3.79 (± 1.14) mmol/L among individuals aged 50 to 60 years old.4 Furthermore, our finding of higher LDL-c in women aged 51 to 60 years old is consistent with previous literature, and this phenomenon may be partially explained by hormonal changes associated with menopause.8 The population-based Malaysian Cohort Study of 106,527 recruited individuals reported a 44.9% prevalence of hypercholesterolaemia with similar mean LDL-c levels across the various age-sex groups.9
Strengths and Limitations
This study has several strengths. It is the first study in Malaysia reporting on mean LDL-c levels using primary care EMR data. The primary strength of this study is the inclusion of a large sample size.
However, some limitations should be mentioned. The LDL-c testing was not part of a general screening programme but following consultation in primary care clinics. In younger individuals, cholesterol testing/assessment may be initiated due to existing cardiovascular risk factors (such as a family history of cardiovascular diseases or raised LDL-c). The data was not nationally representative as the selection of the clinics was purposely undertaken for the FAMCAT study,7 and involved three out of 14 states and federal territories in Malaysia. Additionally, only data on age and sex were extracted from the EMR for this study, it was therefore impossible to assess the relationship between age and/or sex and LDL-c levels, adjusting for other confounding variables such as dietary habits, physical activity, and medication use, which are known to impact LDL-c levels.10 Given these limitations, the interpretation and generalisation of the results to the broader Malaysian population should be made with caution.
Clinical Implications
Our study findings have significant clinical implications for the management of cardiovascular health in Malaysia. Firstly, the age-specific variations in LDL-c levels underscore the importance of tailoring screening and intervention strategies to different age groups. For instance, healthcare professionals could closely monitor LDL-c levels in individuals aged 30 to 59, as they exhibited the highest mean LDL-c levels. Additionally, the reversal of sex-related LDL-c differences after age 50 suggests that post-menopausal women may require closer attention regarding their cardiovascular risk factors, including LDL-c levels. Furthermore, the declining trend in LDL-c levels after the age of 60 raises questions about the potential benefits of adjusting cholesterol-lowering interventions in older individuals. Future research should investigate whether the age-related decrease in LDL-c levels in this population is associated with improved cardiovascular outcomes or if additional factors play a role.
In conclusion, our study provides valuable insights into the distribution of mean LDL-c levels across different age groups and sex in the Malaysian primary care population. Due to the limitations of our data, further research is warranted to comprehensively understand the complex relationship between age, sex, and LDL-c levels in the Malaysian population. These findings could, however, help in developing tailored strategies for cardiovascular risk assessment and management.
Ethics
The study was approved by the respective research ethics committees in Malaysia, that is, the UiTM Research Ethics Committee [(REC/03/2020) (FB/48)] and the Medical Research Ethics Committee of the Ministry of Health Malaysia [NMRR20-272-52797 (IIR)].
Acknowledgment
Our special thanks to the participants and health care professionals from the 11 participating primary care clinics. ASR and NQ are co-corresponding authors, with ASR representing the Principal Investigator for Malaysia and NQ representing the Principal Investigator for the UK.
Data Sharing Statement
Raw data are kept at the Institute of Pathology, Laboratory and Forensic Medicine (I-PPerForM), Universiti Teknologi MARA, Selangor, Malaysia and encrypted data are kept at the University of Nottingham, United Kingdom in secured databases. Unidentified data will be shared by the corresponding authors upon request after all the results of this study have been published, and the data are subjected to the data protection regulations of Malaysia and the United Kingdom.
Funding
This study was funded by the Newton-Ungku Omar Fund (NUOF): The UK-Malaysia Joint Partnership Call on Non-communicable Diseases – Reducing Premature Coronary Artery Disease by Early Identification of Familial Hypercholesterolaemia. Patient consent was not required to review the routinely collected medical records. Grant references: 100-TNCPI/GOV 16/6/2 (002/2020)-02 and MR/T 017384/1.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pekkanen J, Linn S, Heiss G, et al. Ten-year mortality from cardiovascular disease in relation to cholesterol level among men with and without preexisting cardiovascular disease. J Med. 2010;322(24):1700–1707. doi:10.1056/NEJM199006143222403
2. Akyea RK, Kai J, Qureshi N, Iyen B, Weng SF. Sub-optimal cholesterol response to initiation of statins and future risk of cardiovascular disease. Heart. 2019:heartjnl-2018–314253. doi:10.1136/heartjnl-2018-314253
3. World Health Organization. Global health observatory data repository; 2016. Available from: https://apps.who.int/gho/data/view.main.2467?lang=en.
4. Mohamed-Yassin MS, Baharudin N, Daher AM, et al. High prevalence of dyslipidaemia subtypes and their associated personal and clinical attributes in Malaysian adults: the REDISCOVER study. BMC Cardiovasc Disord. 2021;21(1):1–13. doi:10.1186/S12872-021-01956-0/TABLES/7
5. Pirillo A, Casula M, Olmastroni E, Norata GD, Catapano AL. Global epidemiology of dyslipidaemias. Nat Rev Cardiol. 2021;18(10):689–700. doi:10.1038/s41569-021-00541-4
6. Carroll MD, Kit BK, Lacher DA, Shero ST, Mussolino ME. Trends in lipids and lipoproteins in US adults, 1988–2010. JAMA. 2012;308(15):1545–1554. doi:10.1001/JAMA.2012.13260
7. Ramli AS, Qureshi N, Abdul-Hamid H, et al. Reducing premature coronary artery disease in Malaysia by early identification of familial hypercholesterolemia using the Familial Hypercholesterolemia Case Ascertainment Tool (FAMCAT): protocol for a Mixed Methods Evaluation Study. JMIR Res Protoc. 2023;12:e47911. doi:10.2196/47911
8. Ambikairajah A, Walsh E, Cherbuin N. Lipid profile differences during menopause: a review with meta-analysis. Menopause. 2019;26(11):1327–1333. doi:10.1097/GME.0000000000001403
9. Jamal R, Syed Zakaria SZ, Kamaruddin MA, et al. Cohort profile: the Malaysian Cohort (TMC) project: a prospective study of non-communicable diseases in a multi-ethnic population. Int J Epidemiol. 2015;44(2):423. doi:10.1093/IJE/DYU089
10. Schröder H, Marrugat J, Elosua R, Covas MI. Relationship between body mass index, serum cholesterol, leisure-time physical activity, and diet in a Mediterranean Southern-Europe population. Br J Nutr. 2003;90(2):431–439. doi:10.1079/BJN2003899
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.