")
Back to Journals » Journal of Pain Research » Volume 16
Age and Gender, but Not Pain are Associated with Pressure Pain Thresholds in Patients with Temporomandibular Disorders: A Cross-Sectional Study
Authors Zheng Y , Zhu R, Xiao C , Cheng Q, Long Y , Zhou X, Zhang S, Wang J, Xiong X
Received 26 March 2023
Accepted for publication 20 June 2023
Published 28 June 2023 Volume 2023:16 Pages 2205—2216
DOI https://doi.org/10.2147/JPR.S414276
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr David Keith
Yunhao Zheng,1 Rui Zhu,2 Chuqiao Xiao,3 Qiaoyu Cheng,3 Yifei Long,3 Xueman Zhou,3 Shilong Zhang,4 Jun Wang,3 Xin Xiong1,3
1Department of Temporomandibular Joint, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China; 2Department of Prosthodontics, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China; 3Department of Orthodontics, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China; 4Department of Orthodontics, School and Hospital of Stomatology, Hebei Medical University & Hebei Key Laboratory of Stomatology, Shijiazhuang, People’s Republic of China
Correspondence: Xin Xiong, National Clinical Research Center for Oral Diseases, State Key Laboratory of Oral Diseases, Department of Temporomandibular Joint, West China Hospital of Stomatology, Sichuan University, Chengdu, People’s Republic of China, Tel/Fax +86-28-85503898, Email [email protected]
Purpose: This study aims to explore the association of pressure pain thresholds (PPTs) with age, gender, and pain in patients with temporomandibular disorders (TMD).
Patients and Methods: A total of 301 TMD patients (248 female and 53 male) were recruited and classified into the high and low age groups according to their median age of 26 years. Patients’ demographics, pain-related variables, TMD-related variables, and PPTs of both left and right temporomandibular joints (TMJs), masseter, and temporalis were collected.
Results: Pain duration and visual analog scale of pain (VAS) showed no significant correlations with PPTs (P> 0.05). Multiple linear regression analysis revealed a significant positive association of PPTs of all six sites with males (β=0.41– 0.72 kg·cm− 2, 95% CI (0.19– 0.38, 0.74– 0.99), P< 0.001), as well as with the high age group [β=0.28– 0.36 kg·cm− 2, 95% CI (0.07– 0.20, 0.47– 0.53), P< 0.020]. Furthermore, PPTs of the left TMJ showed a significant negative association with left pain-related TMD (PT) [β=− 0.21 kg·cm− 2, 95% CI (− 0.38, − 0.04), P=0.026], but PPTs of the remaining sites did not show a significant association with PT (P> 0.05). Stratified analysis showed that PPTs in females were associated with the high age group [β=0.25– 0.37 kg·cm− 2, 95% CI (0.04– 0.20, 0.45– 0.56), P< 0.020] and that PPT of the left TMJ was associated with left PT [β=− 0.21 kg·cm− 2, 95% CI (− 0.39, − 0.03), P=0.043]. The remaining PPTs did not show a significant association with PT (P> 0.05). In males, PPTs did not show significant correlations with age, PT and VAS (P> 0.05).
Conclusion: PPTs in the orofacial region are associated with gender and age in TMD patients. Pain duration and intensity show no significant correlations with PPTs in TMD patients. Researchers and dentists should take age and gender into account when using PPTs as auxiliary diagnostic indicators for PT.
Keywords: pain sensitivity, temporomandibular disorders, pressure pain threshold, age, gender
Corrigendum for this paper has been published.
Introduction
Temporomandibular disorders (TMDs) are a family of complicated disorders in the musculoskeletal system involving the temporomandibular joints (TMJs), the masticatory muscles, and their associated tissues.1 TMD is the second most common musculoskeletal disorder that causes pain and disability.2,3 Generally, the prevalence of TMD is considered to be 5% to 12% in adults,4,5 while in children it ranges from 22% to 47% in different countries.6 According to Diagnostic Criteria for Temporomandibular Disorders (DC/TMD), TMD can be classified into two groups: pain-related TMD (PT), which includes myalgia, arthralgia, and headache attributed to TMD; and intra-articular TMD (IT) which includes disc displacement, degenerative joint disease, and subluxation.4 The etiologies of TMD are complex and associated with biological, environmental, psychological, social, and cognitive factors.7 Common treatments for TMD include self-management, physical therapy, use of nonsteroidal anti-inflammatory drugs, and psychological interventions.8 In recent years, some emerging therapies such as low-level laser therapy, extracorporeal shockwave therapy and oxygen-ozone therapy have been reported as promising new treatments for TMD.9,10 TMD patients may present overlapping symptoms with other chronic pain conditions, including headache, fibromyalgia, and neurological conditions, probably through the phenomenon of central sensitization (mainly allodynia and hyperalgesia).11–13 The influence of various symptoms of TMD has been widely investigated and proven to be associated with psychological disorders, systemic disorders and overlapping pain conditions.7,8,11–15
As one of the most common symptoms of TMD, pain in the maxillofacial region, especially chronic pain persisting for a long time, was associated with negative emotions of the patients such as depression, stress, anxiety, and stigma as well as increased pain sensitivity.7,14,15 The increased pain sensitivity caused by TMD has been related to the genetic factors and psychological disorders mentioned above and may be the result of an abnormal response of the central nervous system to nociceptive information induced by physical or emotional stress.16,17 Pain sensitivity varies among populations of different ages and genders and is usually measured by pressure pain thresholds (PPTs) which refers to the minimum amount of pressure necessary to induce pain using non-invasive pressure algometers.18 Usually, increased pain sensitivity measured by PPTs is observed in chronic diseases among which females are lower than males.15,19
The orofacial pain prospective evaluation and risk assessment (OPPERA) baseline case-control study and others have shown that patients experiencing PT are more sensitive to experimental pain even in the non-symptomatic region.17,20–22 The recent longitudinal studies further explored the causal association between pain sensitivity and clinical pain and showed that PPTs could fluctuate with the development of TMD. Reduced PPTs on the first-onset TMD could rebound to some extent when effective treatment was applied for TMD recovery, although premorbid PPTs could barely predict the incidence of TMD.23–25 Although the association of PPTs between TMD and TMD-free subjects has been broadly investigated, the association of PPTs with pain only among TMD subjects remains unclear and deserves further studying.
Therefore, according to previous studies, it can be assumed that TMD patients with painful TMD have higher pain sensitivity and lower PPTs than those without pain. It could also be hypothesized that females have lower PPTs than males. Our research aimed to investigate the relationship between PPTs and age, gender, and pain, including pain intensity and pain duration in patients with TMD.
Materials and Methods
Subjects and TMD Diagnosis
This observational cross-sectional study was performed at the Department of Temporomandibular Joint, West China Hospital of Stomatology, Sichuan University, from July 2022 to December 2022. The Ethics Committee of West China Hospital of Stomatology of Sichuan University (Ethics number: 2022-212) approved the study, and the Declaration of Helsinki was followed during the study.
Patients with TMD were enrolled in this study prospectively when they were seeking care in the hospital and all the patients and legal guardians of underage patients provided informed consent. The inclusion criteria included: (a) patients diagnosed with TMD; (b) clinical data of patients was complete. The exclusion criteria included: (a) presence of TMJ trauma or operations; (b) presence of analgesics use in the last 3 months, for example, nonsteroidal anti-inflammatory drugs (NSAIDs); (c) cognitive impairment and/or illiteracy; (d) presence of facial skin disease; (e) ongoing dental pain, neuralgia, and sinusitis. Patients participating in this study were classified into the high and the low age groups according to the median age.
All the patients were examined by two experienced TMD specialists and the diagnoses were established based on the DC/TMD.4 Two diagnoses were made by the same specialist at different times, and the intra- and inter-examiner reliability of the diagnoses were tested using the kappa coefficient (intra-examiner: kappa = 0.93 and 0.91; inter-examiner: kappa = 0.87). In the case of different diagnoses, a consensus diagnosis after discussion was adopted.
In this study, according to DC/TMD, PT included myalgia, arthralgia, and headache attributed to TMD. Patients classified as non-PT were those with TMD but without a PT diagnosis, ie, patients whose diagnosis included only disc displacement, degenerative joint disease, and subluxation.
Data Collection and Measurements
Data collection and measurements were performed on the same day after the patient was diagnosed with TMD. Data included demographics, medical histories, the visual analogue scale of pain (VAS), maximal interincisal opening (MIO), palpation examination, and PPTs. PPTs were measured last, after all other measurements were completed.
Demographics and Medical Histories
Demographics included the age and gender of the patients. Medical histories involved pain duration, systemic diseases, and parafunctional habits. Pain duration was further classified as no pain, acute pain (≤3 months), and chronic pain (>3 months). Systemic diseases include cardiovascular diseases (eg hypertension, coronary artery disease, etc.), endocrine diseases (eg diabetes, hyperthyroidism, etc.), autoimmune diseases (eg systemic lupus erythematosus, rheumatoid arthritis, etc.), psychiatric comorbidities, other chronic pain conditions etc. Parafunctional habits referred to poor habits associated with TMD, such as unilateral chewing, biting hard foods, etc.26
PPTs
PPTs are the minimal pressure (force) that induces pain.27 PPTs were measured using a manual Wagner-type algometer (FPIX25, Wagner instruments) with a rubber round probe with a surface area of 1 cm2.28 PPTs of both left and right TMJ, masseter, and temporalis were evaluated. The investigator places the pain meter probe vertically at the assessed spot, continuously and steadily increasing the pressure at a constant rate of 1 kg·cm−2 per second. The patients were asked to raise their hands at the exact moment they felt pain. Measurements were repeated three times and the average of the three algometer readings would be recorded as the corresponding PPTs.27
VAS
The VAS was applied to measure the intensity of pain in the TMJ and associated orofacial muscles at the time of the patient’s visit, which ranged from 0 (no pain at all) to 10 (the most intense pain imaginable).
MIO
The overbite and the distance between the incisive margins of the maxillary and mandibular central incisors during assisted maximum mouth opening was measured using a millimeter ruler while the subject was in an upright position. The sum of the two measurements was recorded as MIO.
Palpation
Palpation was employed to identify both TMJ noises and pain in the masticatory muscles and TMJ. TMJ noises were divided into clicking and crepitus sounds, according to DC/TMD. Pain reported by patients at the location of palpation was recorded. Examination was performed on both bilateral TMJs and masticatory muscles.
Statistical Analysis
Cohen’s f2 with a medium effect size (0.15) was used to determine the sample size at α = 0.05 and power = 0.95, and 128 was the minimum acceptable sample size. The Shapiro–Wilk test was employed to test the normality of the variables, the Wilcoxon rank sum test was used to test for differences between non-normal variables, and the Fisher exact test was used to test for differences in categorical variables. Spearman correlation coefficients adjusted with Benjamini-Hochberg method were calculated for the initial exploration of the relationship between the variables while hierarchical clustering was performed at the same time. Simple linear regression models were employed for preliminary variable selection (P < 0.1), and eventually, the variable set was checked and determined based on expert knowledge. Multiple linear regression models were utilized to investigate the relationship between PPTs and covariates, as well as to adjust for possible confounders. Stratified analysis was employed to adjust for the gender and to investigate the factors associated with PPTs in male and female patients. The Benjamini-Hochberg method was used in the multiple linear regression to adjust the p-values. Variance inflation factors (VIFs) were used to test for the presence of multicollinearity in the model. Restricted cubic splines were used to fit nonlinear relationships.
All statistical analyses were performed using R, version 4.2.1 (R Core Team 2022). The significance level α was set to 0.05.
Results
Demographics
A total of 301 subjects with TMD (248 female and 53 male patients with a median age of 26 years) were enrolled in this study (Figure 1). Table 1 shows the characteristics of the TMD patients under study at baseline. MIO and PPTs at all sites were significantly higher in male TMD patients than in female TMD patients (P < 0.001). The remaining variables were not significantly different (P > 0.05). Among the 301 subjects (Table 2), 209 patients had PT (69.4%), while 92 patients had non-PT (30.6%). Patients with PT had significantly higher age, VAS, and pain duration compared to those with non-PT (P < 0.05). Conversely, patients with PT had significantly lower MIO and proportion of clicking sounds than patients with non-PT (P < 0.05). The PPT of TMJ was significantly lower in patients with PT compared to those with non-PT (P < 0.05), while no significant difference was observed in the PPT of masseter and temporalis (P > 0.05).
 |
Table 1 Baseline Characteristics of the TMD Patients Under Study |
 |
Table 2 Demographic and Clinical Characteristics of Patients with Non-PT and PT |
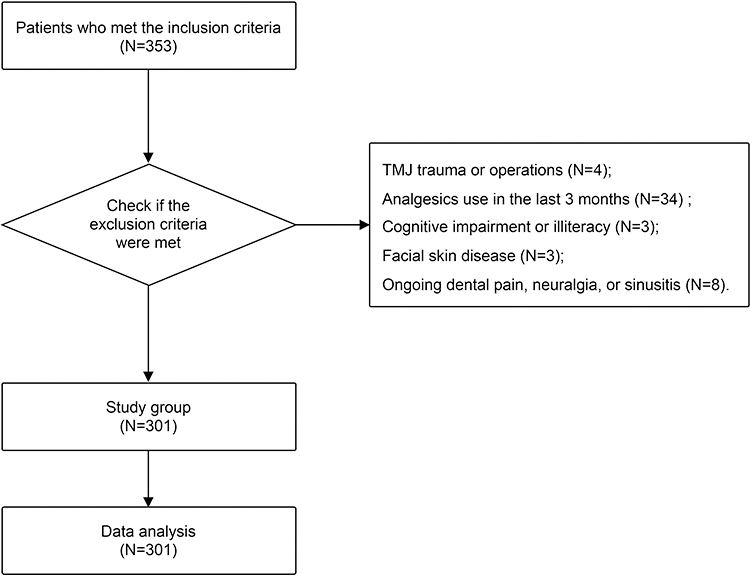 |
Figure 1 The flowchart of the study. |
Spearman Correlation Analysis and Hierarchical Clustering
Spearman correlation coefficients adjusted with Benjamini-Hochberg method (Supplementary Figure 1, Supplementary Materials) showed significant positive correlations for the six PPTs (P < 0.001), and significant positive correlations between age and PPTs (P < 0.01), gender (male), and PPTs (P < 0.001). Left PPTs showed a significant negative correlation with the left PT (P < 0.01) but not with the right PT (P > 0.05). In contrast, neither right PPTs nor left PPTs showed a significant correlation with the right PT (P > 0.05). The left palpation pain showed a negative correlation with the left PPTs of TMJ (P < 0.05). Except for the above variables, the correlations between the remaining variables and PPTs were not significant (P > 0.05).
Simple Linear Regressions and Variable Selection
Simple linear regression models between PPTs and variables (Table 3) indicated that all six PPTs were significantly associated with gender (P < 0.001) and age (P < 0.05). The left PPT was significantly associated with the left PT (P < 0.05), whereas the right PPT did not show a significant correlation with the right PT (P > 0.05). The PPT of the right temporalis was significantly correlated with the right palpation pain (P < 0.05). Moreover, the correlation between the six PPTs was statistically significant (P < 0.001).
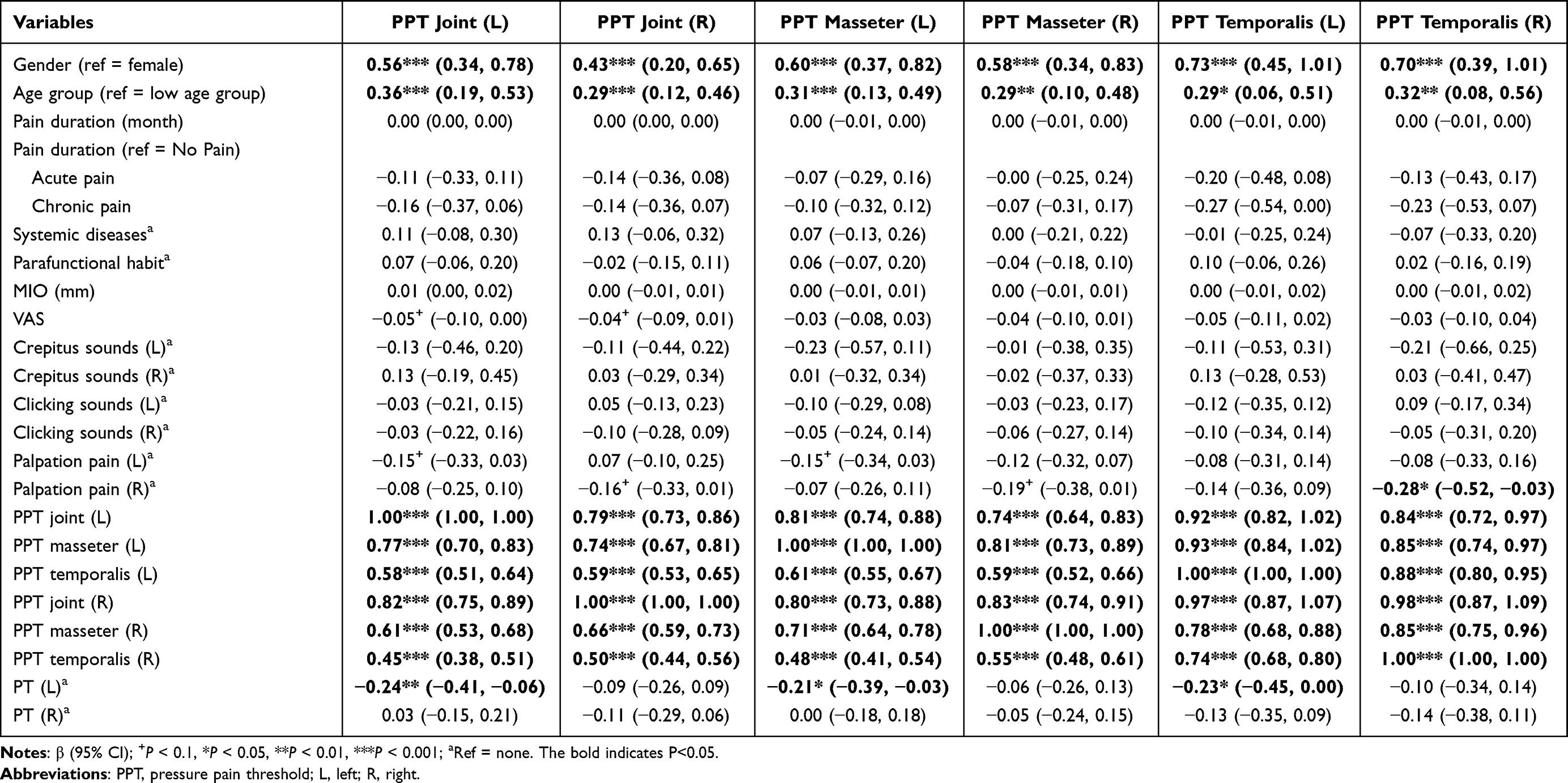 |
Table 3 Crude Association Between PPTs and Variables |
The age group, gender, VAS, palpation pain, and PT were initially included in the variable set for multiple regressions according to the criterion of P < 0.1 in the simple linear regressions (Table 3).
Multiple Linear Regressions
The results of the multiple linear regression analysis (Table 4) showed a significant positive association of PPT of all six sites with males (0.41–0.72 kg·cm−2, P < 0.001), as well as with the high age group (0.28–0.36 kg·cm−2, P < 0.020). In addition, PPTs of the left TMJ showed a significant negative association with left PT [−0.21 kg·cm−2, 95% CI (−0.38, −0.04), P = 0.026], but the PPTs of the remaining sites did not show a significant correlation with PT (P > 0.05). Besides, PPTs showed no significant association with VAS (P > 0.05).
 |
Table 4 β-Coefficients in Multiple Linear Regression Models of TMD Patients |
In female TMD patients, multiple linear regression analysis (Table 5) showed that female TMD patients in the high age group had an average increase in PPTs of 0.25 kg·cm−2 to 0.37 kg·cm−2 compared to the low age group (P < 0.05). The effects of the presence of left and right PT of the patients and the VAS on the PPTs were not statistically significant, but the presence of left PT was significantly related to the lower PPT of the left TMJ [−0.21 kg·cm−2, 95% CI (−0.39, −0.03), P = 0.043].
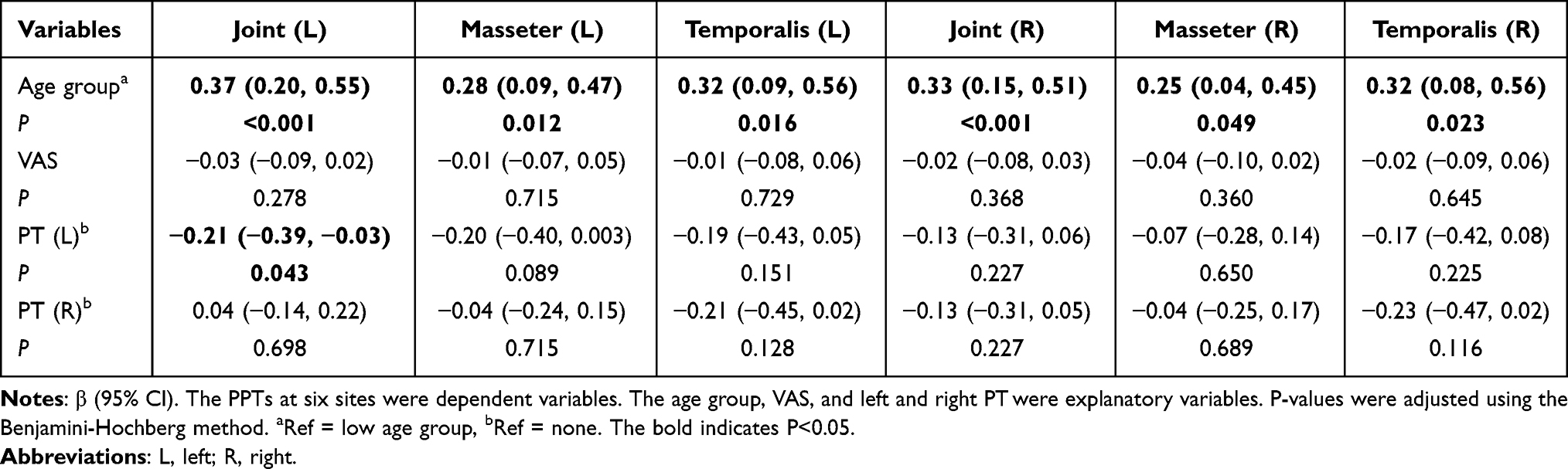 |
Table 5 β-Coefficients in Multiple Linear Regression Models of Female TMD Patients |
In male TMD patients (Table 6), no variable showed a significant association with PPTs.
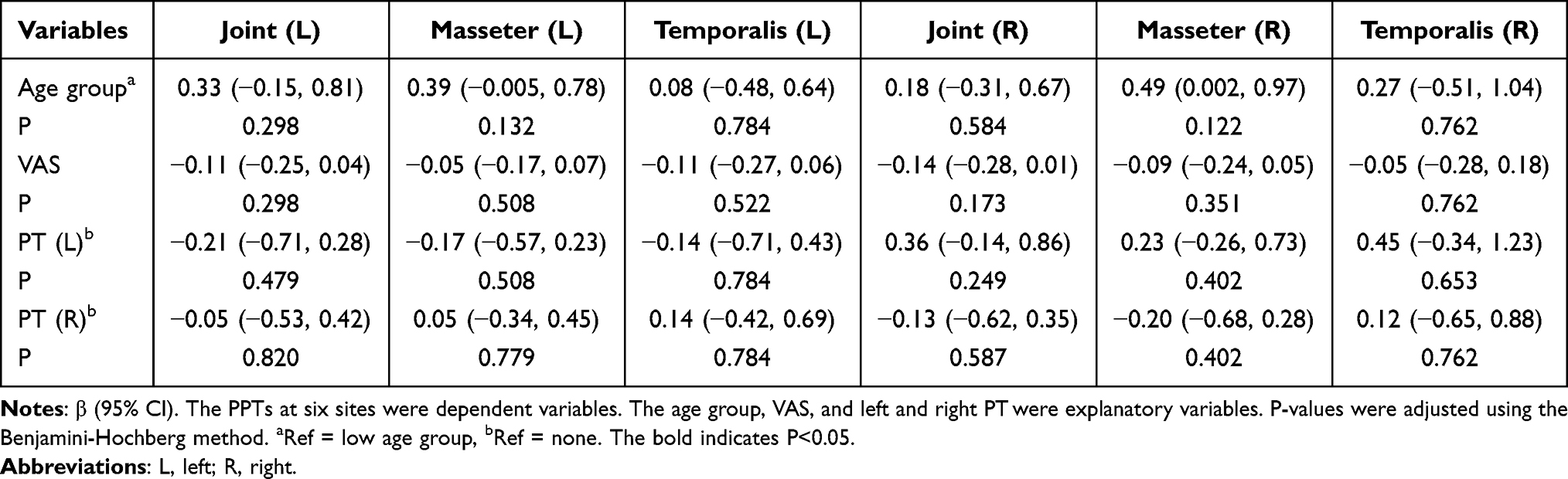 |
Table 6 β-Coefficients in Multiple Linear Regression Models of Male TMD Patients |
The VIFs were calculated to test for the presence of multicollinearity in the models, and the results showed no significant multicollinearity in all models (Supplementary Table 1). Restricted cubic splines (Figure 2) show the shapes of the associations between age and PPTs in TMD patients.
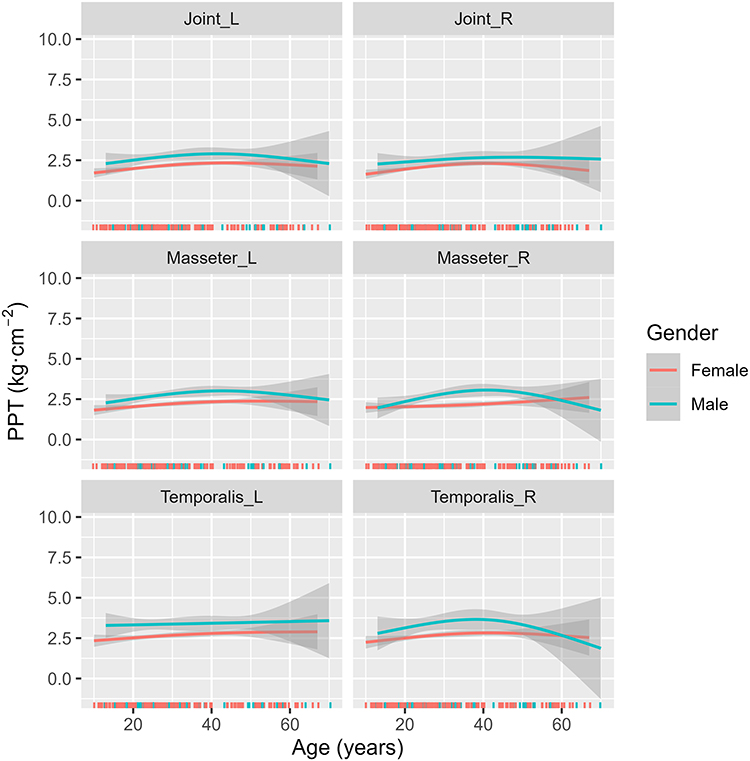 |
Figure 2 Restricted cubic spline approach to explore the shapes of the associations between age and PPTs in TMD patients. The bands show 95% confidence intervals. Abbreviations: L, left; R, Right; PPT, pressure pain threshold. |
Discussion
In the present study, we comprehensively collected the PPTs of almost entire TMD-related sites including both left and right TMJ, masseter, and temporalis, and pain-related indicators like pain intensity and pain duration. To our surprise, instead of pain, we found that age and gender were the main factors influencing PPTs in patients with TMD. Specifically, females had statistically lower PPTs than males among TMD patients, and age was the main factor influencing PPTs of all six sites in females. Thus, our first hypothesis was rejected but our second hypothesis was validated.
Consistent with previous studies,15,19 we found that the PPTs of all six sites tested in TMD patients were significantly higher in males than in females, indicating that females suffered from significantly increased pain sensitivity than males. The sexual differences in pain sensitivity can be interpreted in terms of hormonal factors and societal gender roles.15 Pain sensitivity has been proven affected by testosterone and estrogen. It is reported that testosterone could reduce chronic pain and is related to a higher pain tolerance while estrogen is associated with a lower tolerance to pain.29–31 The mechanism of testosterone remains unclear, but the role of estrogen in pain has been widely studied. Specifically, estrogen can affect both the central and peripheral nervous systems, modulating pain and its perception by modifying pain-related neurotransmitters such as serotonin.32 As for the discrepancies in societal gender roles, in a number of cultures around the world, masculinity is linked to high pain tolerance, while femininity is connected to high pain sensitivity.33
Apart from the differences of PPTs caused by gender, we also found that there existed gender differences in the influential factors of PPTs. For females, we found that age was the main factor influencing PPTs of all six sites during TMD in which the elders had significantly higher PPTs than the younger. It indicated that the PPTs increased with age even in pathological conditions, which was consistent with the findings in healthy populations.34 Furthermore, an interesting finding was observed among female subjects in our study. Although PPTs were negatively associated with PT, the significant correlations were only observed between PPT of left TMJ and left PT. This might be associated with personal habits such as right-side chewing preference and dextromanuality. As for males, the significant association between PPTs and PT was not observed. In addition, no significant association of age with PPTs was found in male patients. This may be partly attributed to fewer male patients in our sample, as the prevalence of TMD is lower in males than in females.8
Although this finding was unexpected, a similar trend has been observed in previous studies. Knuutila et al observed significant negative correlations between myalgia and arthralgia subgroups and PPTs in female TMD patients, but not in male TMD patients, in a 46–47-year-old Northern Finland population.15
Studies have proven that the PPTs will decrease significantly compared to themselves when individuals get TMD, especially PT.24 An intriguing and surprising finding in our study was that pain including pain intensity and pain duration was not associated with PPTs in both female and male patients with TMD, indicating that PPTs could not be further influenced by pain during TMD. Previous studies based on OPPERA data have shown that patients with TMD experience a decrease in PPT some time after the onset of symptoms, compared to their PPT when they did not have TMD (median of 17 months ago).24 However, the previous study was not able to determine whether the decline in PPT occurred before or after the onset of TMD. According to our study, no association of PPTs with pain duration was observed in patients diagnosed with PT. This implies that the decline in PPT may occur only before the onset of TMD rather than after it. This inference needs to be verified by further well-designed longitudinal studies (Supplementary Figure 2). Consistent with our results, other studies had the same finding that there was no correlation between PPTs and VAS in patients with TMD.35 The results were also found in chronic tension-type headache patients. Neither the intensity nor the duration of the headache was found to be associated with a decrease in PPTs.36
Restricted cubic splines indicated that the assumption of linearity between age and PPTs in TMD patients was reasonable because there existed linear relationships within the 95% confidence interval. In addition, the fit results of the restricted cubic spline implied that PPTs may increase and then decrease with age. However, the large 95% confidence interval in the tail of the splines suggested that this trend may not be robust due to a lack of sufficient samples of female TMD patients over 40 years of age.
Therefore, based on our study, it seems that PPTs may not be a meaningful clinical indicator for PT prediction and diagnosis in male patients. However, in female patients, PPTs are promising as an auxiliary diagnostic index of PT, but attention should be paid to the correction of age.
The current study still existed several limitations. Firstly, the sample size of male patients and patients over forty years old should be further increased in future research in order to reduce the size of the confidence interval and improve the power of the test, as well as to explore possible linear relationships or saturation effects between age and PPTs in female patients. Secondly, due to the limitation of clinical data collection, the study lacked a healthy control group, so the information regarding the PPTs baseline was unavailable. Therefore, this study did not compare the difference in PPTs between patients with and without TMD. Third, the current study excluded patients who had used analgesics in the last three months. Although we controlled for pain intensity in the statistical analysis, this could still lead to a potential sample skew toward patients with less severe pain. In addition, our study focused only on populations in southwest China, and further studies are needed to confirm whether there are racial differences in the findings.
Conclusion
PPTs in the orofacial region were associated with gender and age in TMD patients. Moreover, pain duration and pain intensity do not show a significant correlation with PPTs in TMD patients. In female patients with TMD, PPTs were significantly positively associated with age and there was a significant negative association between PPT of the left TMJ and left PT. In male patients, PPTs were not significantly associated with age, and the association of PPTs with PT was also not significant. Researchers and dentists should take age and gender into account when using PPTs as auxiliary diagnostic indicators for PT.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Durham J, Newton-John TRO, Zakrzewska JM. Temporomandibular disorders. BMJ. 2015;350:h1154. doi:10.1136/bmj.h1154
2. Jin LJ, Lamster IB, Greenspan JS, Pitts NB, Scully C, Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral Dis. 2016;22(7):609–619. doi:10.1111/odi.12428
3. Valesan LF, Da-Cas CD, Réus JC, et al. Prevalence of temporomandibular joint disorders: a systematic review and meta-analysis. Clin Oral Invest. 2021;25(2):441–453. doi:10.1007/s00784-020-03710-w
4. Schiffman E, Ohrbach R, Truelove E, et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: recommendations of the international RDC/TMD Consortium Network* and orofacial pain special interest group†. J Oral Facial Pain Headache. 2014;28(1):6–27. doi:10.11607/jop.1151
5. Zhu R, Zheng YH, Zhang ZH, Fan PD, Wang J, Xiong X. Development of a new category system for the profile morphology of temporomandibular disorders patients based on cephalograms using cluster analysis. Front Public Health. 2022;10. doi:10.3389/fpubh.2022.1045815
6. Macrì M, Murmura G, Scarano A, Festa F. Prevalence of temporomandibular disorders and its association with malocclusion in children: a transversal study. Front Public Health. 2022;10:860833. doi:10.3389/fpubh.2022.860833
7. Kmeid E, Nacouzi M, Hallit S, Rohayem Z. Prevalence of temporomandibular joint disorder in the Lebanese population, and its association with depression, anxiety, and stress. Head Face Med. 2020;16(1):19. doi:10.1186/s13005-020-00234-2
8. Committee on Temporomandibular Disorders (TMDs): From Research Discoveries to Clinical Treatment, Board on Health Sciences Policy, Board on Health Care Services, Health and Medicine Division, National Academies of Sciences, Engineering, and Medicine. Temporomandibular disorders. Bond EC, Mackey S, English R, Liverman CT, Yost O, editors. Priorities for Research and Care. National Academies Press; 2020:25652. doi:10.17226/25652
9. de Sire A, Marotta N, Ferrillo M, et al. Oxygen-ozone therapy for reducing pro-inflammatory cytokines serum levels in musculoskeletal and temporomandibular disorders: a comprehensive review. Int J Mol Sci. 2022;23(5):2528. doi:10.3390/ijms23052528
10. Chan NHY, Ip CK, Li DTS, Leung YY. Diagnosis and treatment of myogenous temporomandibular disorders: a clinical update. Diagnostics. 2022;12(12):2914. doi:10.3390/diagnostics12122914
11. Ferrillo M, Migliario M, Marotta N, et al. Temporomandibular disorders and neck pain in primary headache patients: a retrospective machine learning study. Acta Odontol Scand. 2023;81(2):151–157. doi:10.1080/00016357.2022.2105945
12. Minervini G, Mariani P, Fiorillo L, Cervino G, Cicciù M, Laino L. Prevalence of temporomandibular disorders in people with multiple sclerosis: a systematic review and meta-analysis. Cranio. 2022;1–9. doi:10.1080/08869634.2022.2137129
13. Ferrillo M, Giudice A, Marotta N, et al. Pain management and rehabilitation for central sensitization in temporomandibular disorders: a comprehensive review. Int J Mol Sci. 2022;23(20):12164. doi:10.3390/ijms232012164
14. Zhu R, Zhang L, Zheng YH, et al. Association between stigma and pain in patients with temporomandibular disorders. In: Costa ALF, editor. International Journal of Clinical Practice. John Wiley and Sons, Inc.; 2022:1–10. doi:10.1155/2022/2803540
15. Knuutila J, Kivipuro J, Näpänkangas R, et al. Association of temporomandibular disorders with pain sensitivity: a cohort study. Eur J Pain. 2022;26(1):143–153. doi:10.1002/ejp.1844
16. Maixner W, Fillingim RB, Williams DA, Smith SB, Slade GD. Overlapping chronic pain conditions: implications for diagnosis and classification. J Pain. 2016;17(9 Suppl):T93–T107. doi:10.1016/j.jpain.2016.06.002
17. Maixner W, Fillingim R, Booker D, Sigurdsson A. Sensitivity of patients with painful temporomandibular disorders to experimentally evoked pain. Pain. 1995;63(3):341–351. doi:10.1016/0304-3959(95)00068-2
18. Vervullens S, Haenen V, Meert L, et al. Personal influencing factors for pressure pain threshold in healthy people: a systematic review and meta-analysis. Neurosci Biobehav Rev. 2022;139:104727. doi:10.1016/j.neubiorev.2022.104727
19. Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. Br J Anaesth. 2013;111(1):52–58. doi:10.1093/bja/aet127
20. Sarlani E, Grace EG, Reynolds MA, Greenspan JD. Evidence for up-regulated central nociceptive processing in patients with masticatory myofascial pain. J Orofac Pain. 2004;18(1):41–55.
21. Greenspan JD, Slade GD, Bair E, et al. Pain sensitivity risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case control study. J Pain. 2011;12(11 Suppl):T61–74. doi:10.1016/j.jpain.2011.08.006
22. Garofalo JP, Gatchel RJ, Wesley AL, Ellis E. Predicting chronicity in acute temporomandibular joint disorders using the research diagnostic criteria. J Am Dent Assoc. 1998;129(4):438–447. doi:10.14219/jada.archive.1998.0242
23. Greenspan JD, Slade GD, Bair E, et al. Pain sensitivity and autonomic factors associated with development of TMD: the OPPERA prospective cohort study. J Pain. 2013;14(12):T63–T74.e6. doi:10.1016/j.jpain.2013.06.007
24. Slade GD, Sanders AE, Ohrbach R, et al. Pressure pain thresholds fluctuate with, but do not usefully predict, the clinical course of painful temporomandibular disorder. Pain. 2014;155(10):2134–2143. doi:10.1016/j.pain.2014.08.007
25. La Touche R, Martínez García S, Serrano García B, et al. Effect of manual therapy and therapeutic exercise applied to the cervical region on pain and pressure pain sensitivity in patients with temporomandibular disorders: a systematic review and meta-analysis. Pain Med. 2020;21(10):2373–2384. doi:10.1093/pm/pnaa021
26. Yang W, Xiong X, Wu Y, et al. College students with oral habits exhibit worse psychological status and temporomandibular-related quality of life: a correlational study. Pain Res Manag. 2022;2022:6079241. doi:10.1155/2022/6079241
27. Fischer AA. Pressure algometry over normal muscles. Standard values, validity and reproducibility of pressure threshold. Pain. 1987;30(1):115–126. doi:10.1016/0304-3959(87)90089-3
28. Reeves JL, Jaeger B, Graff-Radford SB. Reliability of the pressure algometer as a measure of myofascial trigger point sensitivity. Pain. 1986;24(3):313–321. doi:10.1016/0304-3959(86)90117-X
29. Borzan J, Fuchs PN. Organizational and activational effects of testosterone on carrageenan-induced inflammatory pain and morphine analgesia. Neuroscience. 2006;143(3):885–893. doi:10.1016/j.neuroscience.2006.08.034
30. Bulls HW, Freeman EL, Anderson AJ, Robbins MT, Ness TJ, Goodin BR. Sex differences in experimental measures of pain sensitivity and endogenous pain inhibition. J Pain Res. 2015;8:311–320. doi:10.2147/JPR.S84607
31. Choi JC, Chung MI, Lee YD. Modulation of pain sensation by stress-related testosterone and cortisol. Anaesthesia. 2012;67(10):1146–1151. doi:10.1111/j.1365-2044.2012.07267.x
32. Paredes S, Cantillo S, Candido KD, Knezevic NN. An association of serotonin with pain disorders and its modulation by estrogens. Int J Mol Sci. 2019;20(22):E5729. doi:10.3390/ijms20225729
33. Defrin R, Shramm L, Eli I. Gender role expectations of pain is associated with pain tolerance limit but not with pain threshold. Pain. 2009;145(1–2):230–236. doi:10.1016/j.pain.2009.06.028
34. Lautenbacher S, Peters JH, Heesen M, Scheel J, Kunz M. Age changes in pain perception: a systematic-review and meta-analysis of age effects on pain and tolerance thresholds. Neurosci Biobehav Rev. 2017;75:104–113. doi:10.1016/j.neubiorev.2017.01.039
35. Sanches ML, Juliano Y, Novo NF, Guimarães AS, Rodrigues Conti PC, Alonso LG. Correlation between pressure pain threshold and pain intensity in patients with temporomandibular disorders who are compliant or non-compliant with conservative treatment. Oral Surg Oral Med Oral Pathol Oral Radiol. 2015;120(4):459–468. doi:10.1016/j.oooo.2015.05.017
36. Fernández-de-las-Peñas C, Cuadrado ML, Arendt-Nielsen L, Ge HY, Pareja JA. Increased pericranial tenderness, decreased pressure pain threshold, and headache clinical parameters in chronic tension-type headache patients. Clin J Pain. 2007;23(4):346–352. doi:10.1097/AJP.0b013e31803b3770
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.