")
Back to Journals » International Journal of General Medicine » Volume 16
Age- and Gender-Specific Diagnostic Value of the Albumin-to-Creatinine Ratio for the Early Screening of Chronic Kidney Disease Among Middle-Aged and Elderly Males in Southeast China
Authors Zheng X, Liu D, Zhu J, Lu L, Yang J
Received 6 May 2023
Accepted for publication 5 July 2023
Published 13 July 2023 Volume 2023:16 Pages 3033—3042
DOI https://doi.org/10.2147/IJGM.S419100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiang Zheng,* Dan Liu,* Jing Zhu, Li Lu, Jianshu Yang
Department of Health Management Center, the First Affiliated Hospital of Soochow University, Suzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jianshu Yang, Department of Health Management Center, the First Affiliated Hospital of Soochow University, No. 899, Pinghai Road, Gusu District, Suzhou, 215006, People’s Republic of China, Email [email protected]
Objective: To evaluate the potential diagnostic value of the albumin-to-creatinine ratio (ACR) in screening for early kidney injury in a physically examined population from Southeast China.
Methods: A total of 13,250 candidates were selected. Urinary ACR values < 30, 30– 300, and > 300 mg/g were utilized as positive cut-off points to denote normal proteinuria, microalbuminuria, and macroalbuminuria, respectively.
Results: Age, systolic blood pressure, diastolic blood pressure, body mass index, waistline, fasting blood glucose, glycated hemoglobin, triglycerides, and high-density lipoprotein cholesterol were significantly different among the three groups. eGFR was negatively correlated with the levels of sCr, BUN, and UA in the microalbuminuria and macroalbuminuria groups. Furthermore, there was a significant difference in CKD stage between the normal and abnormal urine ACR groups. Meanwhile, for the 20– 40 years patients, the eGFR, sCr and BUN showed no significant difference between microalbuminuria group compared with the normal proteinuria group; in contrast, for the 41– 60 years and > 61 years patients, eGFR, sCr, BUN and UA were all markedly increase in microalbuminuria and macroalbuminuria group in comparison with the normal proteinuria group. Finally, for the 41– 60 males, only eGFR significantly decreased in microalbuminuria group compared with the normal proteinuria group, while for the 41– 60 females, only UA showed no significant difference between microalbuminuria group and normal proteinuria group. On the other hand, for the > 61 males, eGFR, sCr and BUN all significantly changed between microalbuminuria group and normal proteinuria group, while for the > 61 females, eGFR, sCr and BUN all showed no significant difference between microalbuminuria group and normal proteinuria group, as well as microalbuminuria group and macroalbuminuria group.
Conclusion: We proposed using the urinary ACR for the screening of physically examined patients, especially among the elderly males. This approach would assist in the early diagnosis and treatment of renal damage.
Keywords: albumin-to-creatinine ratio, microalbuminuria, kidney injury, physical examination population, screening
Introduction
In recent years, the incidence of various cardiovascular, cerebrovascular, metabolic, and other chronic diseases has increased due to aging and the modern lifestyle. This has also led to an increase in the incidence of various secondary chronic kidney diseases (CKDs). According to epidemiological studies, the prevalence of CKD in China and worldwide is approximately 10.8% and 14.3%, respectively.1,2 Owing to differences in dietary habits and lifestyle, the incidence of CKD in Southeast China (the most economically developed area in China) may differ from that recorded in other parts of the country.3,4 Because of its high prevalence, long disease course, high cost of treatment, and poor prognosis, CKD has become a serious public health problem. At the onset stage, CKD may be insidious, and patients with early-stage CKD often do not experience any symptoms.5,6 Hence, the early detection of renal damage has become an important goal in the field of physical examination. Prompt diagnosis would assist in avoiding the progression of disease in patients undergoing health examination.
Currently, the estimated glomerular filtration rate (eGFR) based on serum creatinine (sCr) values is the most widely used index for the diagnosis and staging of CKD in clinical practice. However, the use of the eGFR for the assessment of early renal impairment is characterized by some limitations.7 In elderly patients, there is a decrease in muscle mass due to reduced activity and changes in diet (eg, a long-term vegetarian diet). Consequently, the sCr levels may not reflect changes that appear early in the course of kidney injury,8,9 thus leading to a decrease in the sensitivity of the eGFR. Proteinuria is the most commonly observed clinical manifestation during the development and progression of CKD. At present, clinical testing for urinary protein generally involves a qualitative or quantitative approach. Qualitative tests are influenced by numerous factors (eg, diet, position, and exercise) and cannot accurately reflect the total amount of urinary protein. Therefore, this approach may only serve as a primary screening test for urinary protein examination.10 The 24-h urine protein quantitative test is the refined standard for detecting total urinary protein. Nevertheless, the assay is complex and unsuitable for large-scale screening targeting early renal impairment in the field of physical examination.
In recent studies, it has been reported that the albumin-to-creatinine ratio (ACR) can reflect the degree of early microangiopathy in the kidneys; this assay is sensitive, rapid, and convenient. Moreover, the results of several other studies11,12 have demonstrated a significant correlation between the ACR and 24-h urine protein levels. Therefore, in the present study, we aimed to determine the clinical value of the ACR in the screening for early renal impairment in a physically examined population from Southeast China. The objective was to establish a foundation for improving the early diagnosis and treatment of CKD.
Subjects and Methods
Study Subjects
A total of 13,250 patients who underwent health examination at the Health Management Center of the First Affiliated Hospital of Soochow University (Suzhou, China) from March 2021 to December 2021 were selected. Patients with incomplete clinical data or examination items were excluded from the analysis. The exclusion criteria also included the presence of connective tissue disorders, pregnancy, and low body weight. The final 12,163 examinees were included in this study [7455 males (61.3%), 4708 females (38.7%), aged 22–94 years, with an average age of (47.6 ± 12.3) years]. This study was approved by the Institutional Review Board of the First Affiliated Hospital of Soochow University. Written informed consent was provided prior to the study. The current study complies with the Declaration of Helsinki.
Methods
All subjects were examined after fasting for 10 h. The medical history (Table S1) and clinical physical examination data were collected, including the name, sex, age, height, weight, body mass index, waistline, blood pressure, total cholesterol, triglycerides, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, fasting blood glucose, sCr, and other biochemical indicators.
Morning urine was collected for examination, before taking urine, the candidate should wipe the area around the urethral opening to avoid contamination. When collecting urine, first urinate a small portion and then collect mid-section urine for detection with more accurate results. Immune scatter turbidimetry was used to determine the levels of urinary microalbumin and creatinine. Albumin and creatinine have been measured using Cobas c502 module® (Roche, Mannheim, USA). Urine albumin was examined by immunoturbidimetric assay, and urine creatinine (mg/dL) was measured based on kinetic Jaffe method. Urinary ACR values <30, 30–300, and >300 mg/g were utilized as positive cut-off points to denote normal proteinuria, microalbuminuria, and macroalbuminuria, respectively. The eGFR was calculated using the CKD-EPI equation.13 CKD staging was performed according to the eGFR (ie, ≥90, 60–89, 30–59, 15–29, and <15 mL/min/1.73 m2 for stages 1–5, respectively).
Statistical Methods
The SPSS version 22.0 statistical software (IBM Corp., Armonk, NY, USA) was used for data analysis. Measurement data were expressed as the mean ± standard deviation. Comparisons among multiple groups were performed through one-way analysis of variance (ANOVA) using the ANOVA test for equality of variances. For homogeneous variances, statistical values were based on the results of one-way ANOVA; the least significant difference method was used for pairwise comparisons. For heterogenous variances, statistical values were based on the results of Welch’s ANOVA; the Games–Howell test was used for pairwise comparisons. Count data were described using rate (%) or the constituent ratio. Comparisons between groups were performed using the chi-squared test or Fisher’s exact probability test. Correlation analysis was performed using Pearson’s correlation coefficient. P-values <0.05 denoted statistically significant differences.
Results
Abnormal ACR Rate
A total of 12,163 subjects (mean age: 47.6 ± 12.3; range: 22–94 years), comprising 7455 males (61.3%) and 4708 females (38.7%) (male-to-female ratio: 1.58:1), were included in this study. Of those, 533 (4.4%) subjects (367 [4.9%] males and 166 [3.5%] females) had an abnormal ACR. The difference noted between males and females with an abnormal ACR was statistically significant (P < 0.001) (Table 1).
 |
Table 1 Comparison of the Abnormal Rate of ACR in Different Genders (%) |
Clinical Characteristics Among Groups with Different Urinary ACR Values
As shown in Table 2, age, systolic blood pressure, diastolic blood pressure, body mass index, waistline, fasting blood glucose, glycated hemoglobin, triglycerides, and high-density lipoprotein cholesterol were significantly different among the three groups (P < 0.05). In contrast, there were no statistically significant differences in low-density lipoprotein cholesterol and total cholesterol between the three groups (P > 0.05).
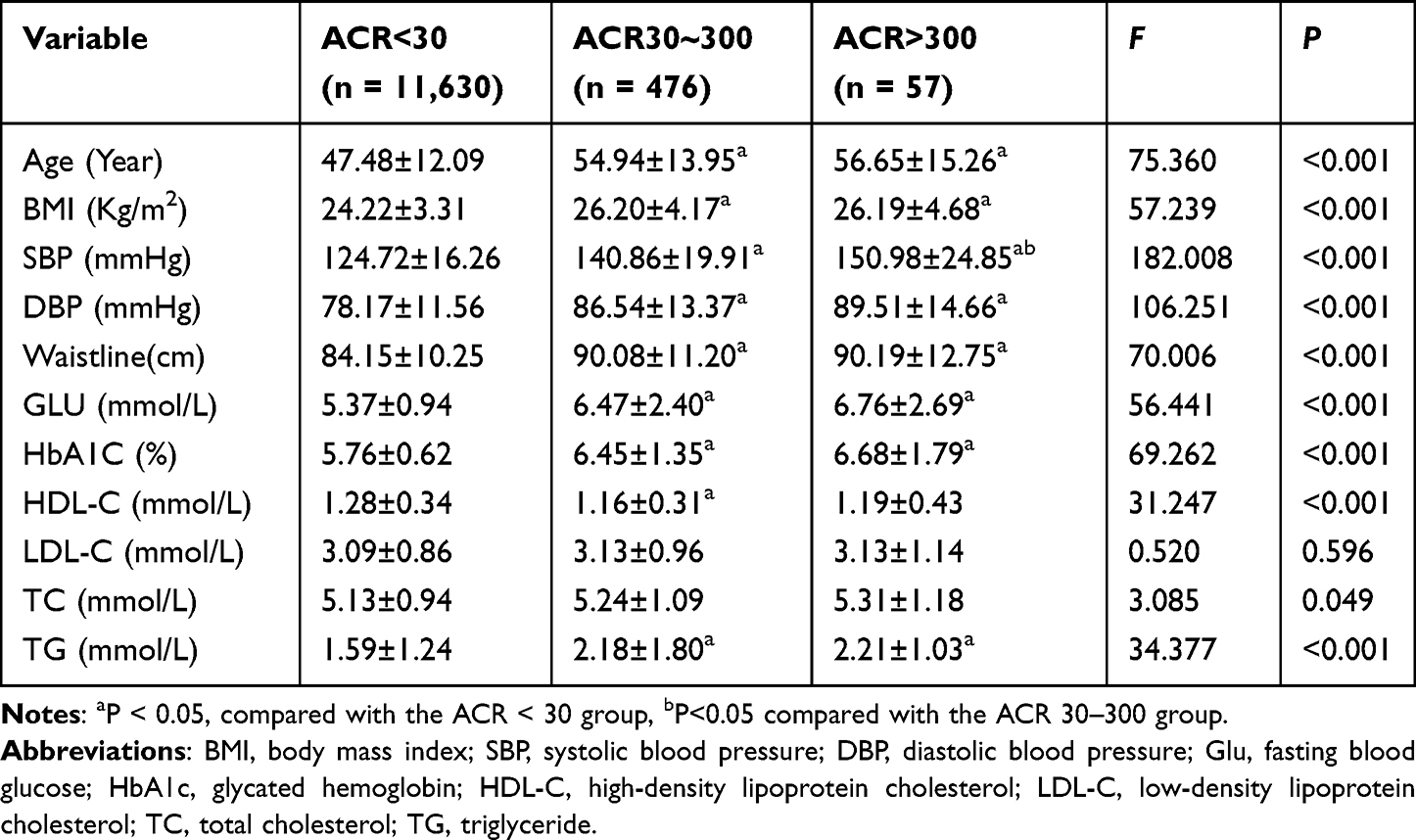 |
Table 2 Differences in Relevant Indexes Between Different Groups of Urinary ACR Levels |
Comparison of CKD-Related Indices Among Groups with Different Urinary ACR
As shown in Figure 1, the eGFR was significantly decreased in the microalbuminuria group compared with the normal proteinuria group (p < 0.01). Moreover, the eGFR was markedly reduced in the macroalbuminuria group versus the microalbuminuria group. In contrast, the levels of sCr, blood urea nitrogen (BUN), and uric acid (UA) were increased in the microalbuminuria group compared with the normal proteinuria group (P < 0.001). Also, the levels of these indices were markedly increased in the macroalbuminuria group versus the microalbuminuria group (p < 0.05).
 |
Figure 1 CKD related indexes eGFR (A), sCr (B), BUN (C), UA (D) among ACR < 30, ACR 30–300 and ACR >300 groups. *p<0.05, ***p<0.001. Abbreviations: eGFR, glomerular filtration rate; sCr, creatinine; BUN, blood urea nitrogen; UA, uric acid. |
Correlation Between eGFR and CKD-Related Indices
As shown in Figure 2, the eGFR was negatively correlated with sCr, BUN, and UA in the microalbuminuria group (Figure 2A) and macroalbuminuria group (Figure 2B).
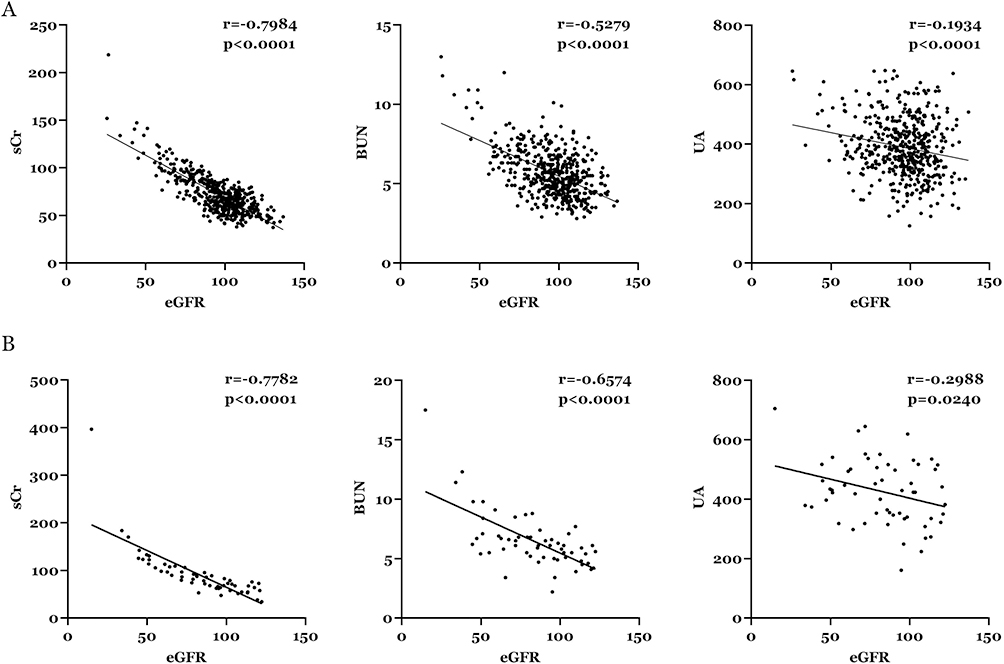 |
Figure 2 Correlation between eGFR and CKD related indexes in the microalbuminuria group (A) and macroalbuminuria group (B). Abbreviations: eGFR, glomerular filtration rate; sCr, creatinine; BUN, blood urea nitrogen; UA, uric acid. |
CKD Staging According to the Urinary ACR
As shown in Table 3, in the group with a normal urine ACR, 86% of the subjects had stage 1 CKD (86.0%), followed by 13.6% and 0.4% who had stage 2 and 3 disease, respectively. In the group with an abnormal urinary ACR, 67.1% of subjects had stage 1 CKD, while the remaining 32.9% had stage 2–5 disease. Analysis according to each stage of CKD revealed statistically significant differences between the two groups (P < 0.05).
 |
Table 3 Differences in CKD Stages Between Different Urinary ACR Groups |
Comparison of CKD-Related Indices Among Groups with Different Urinary ACR at Different Ages
Furthermore, CKD-related indices among groups with different urinary ACR at different ages were compared. As shown in Figure 3A, for the 20–40 group, the eGFR, sCr and BUN showed no significant difference between microalbuminuria group compared with the normal proteinuria group (p > 0.05), while UA markedly increased in microalbuminuria group (P < 0.001). In contrast, for the 41–60 group and >61 group, eGFR, sCr, BUN and UA were all markedly increase in microalbuminuria group (p < 0.05) and macroalbuminuria group (p < 0.05) in comparison with the normal proteinuria group (Figure 3B and C).
 |
Figure 3 Comparison of CKD-related indices among groups with different urinary ACR at 20–40 years (A), 41–60 years (B) and >61 years (C). *p<0.05, **p<0.01, ***p<0.001. Abbreviations: eGFR, glomerular filtration rate; sCr, creatinine; BUN, blood urea nitrogen; UA, uric acid; NS, not significant. |
Comparison of CKD-Related Indices Among 41–60 and >61 Groups with Different Urinary ACR and Genders
Next, CKD-related indices among groups with different urinary ACR in 41–60 and >61 groups with different genders were compared. As shown in Figure 4A, for the 41–60 male group, the eGFR significantly decreased in microalbuminuria group compared with the normal proteinuria group (p < 0.01), while sCr, BUN and UA showed no significant difference (p > 0.05); meanwhile, eGFR, sCr, BUN and UA showed significant difference between microalbuminuria group and macroalbuminuria group (p < 0.05). In Figure 4B, for the 41–60 female group, eGFR, sCr and BUN showed no significant difference between microalbuminuria group and normal proteinuria group (p > 0.05); on the other hand, eGFR and sCr markedly changed in microalbuminuria group compared with macroalbuminuria group (p < 0.05), while BUN and UA showed no significant difference (p > 0.05).
 |
Figure 4 Comparison of CKD-related indices among males (A) and females (B) with different urinary ACR at 41–60. *p<0.05, **p<0.01, ***p<0.001. Abbreviations: eGFR, glomerular filtration rate; sCr, creatinine; BUN, blood urea nitrogen; UA, uric acid; NS, not significant. |
For the >61 males, eGFR, sCr and BUN all significantly changed between microalbuminuria group and normal proteinuria group (p < 0.05) (Figure 5A); and for the >61 females, eGFR, sCr and BUN all showed no significant difference between microalbuminuria group and normal proteinuria group (p > 0.05), as well as microalbuminuria group and macroalbuminuria group (p > 0.05) (Figure 5B).
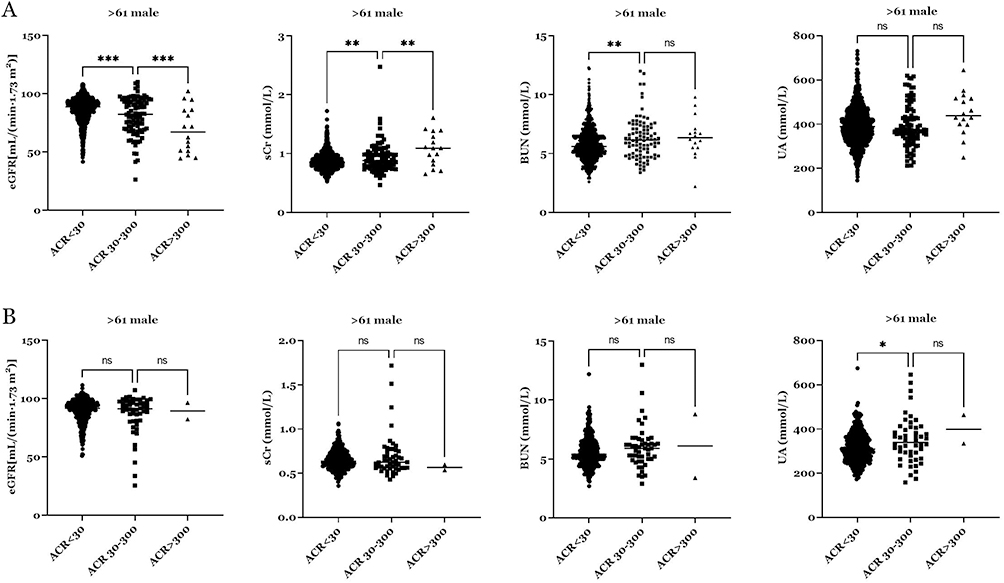 |
Figure 5 Comparison of CKD-related indices among males (A) and females (B) with different urinary ACR at >61. *p<0.05, **p<0.01, ***p<0.001. Abbreviations: eGFR, glomerular filtration rate; sCr, creatinine; BUN, blood urea nitrogen; UA, uric acid; NS, not significant. |
Discussion
Among the subjects included in this study, the detection rate of an abnormal urinary ACR was 4.4%. The results of previous studies demonstrated that the positive rate of urinary ACR in the Chinese population ranged from 4.1% to 20.8%. Also, Zhang et al2 reported that the positive rate of urinary ACR in the general population of China was 9.4%. Therefore, the rate noted in this study is lower than that recorded in general screening. This difference may be attributed to the lack of medication history for the population examined in this study. The possibility of false negative results regarding the urinary protein/creatinine ratio due to the use of various medications cannot be excluded.3 Moreover, the present findings suggested that males are associated with a higher rate of abnormal ACR than females in Southeast China. We hypothesize that this difference may be caused by the higher proportion of males who adopt unfavorable lifestyle habits (ie, drinking and smoking), thus leading to a higher incidence of metabolic diseases, such as hypertension, diabetes, obesity, and hyperuricemia. Consequently, males are at a higher risk for early renal damage than females. However, further studies involving larger populations are warranted to verify these findings.
We also confirmed that age, hypertension, diabetes mellitus, overweight, abdominal obesity, hyperlipidemia, and hyperuricemia are risk factors for early renal injury in patients from Southeast China. The degree of renal injury was also gradually aggravated with advancing age, as well as increases in blood pressure, blood glucose, weight, waist circumference, lipid profile, and UA levels. A possible reason for this observation may be that insulin resistance leads to an increased glomerular filtration rate, dysfunction of renal vascular endothelial cells and other effects. This process can result in the appearance of urinary microalbumin, while the simultaneous emergence of renal injury can further aggravate the underlying disease through different pathways. Consequently, numerous serious complications (eg, glucose and lipid metabolism disorders, hypertension, and atherosclerosis) may occur in these patients.14
An increased ACR is a risk factor for different diseases. For example, an increased ratio has been associated with stroke and homocysteine among hypertensive Asian patients.15 Moreover, the serum ACR is negatively correlated with the short-term clinical outcome of patients with myocardial infarction.16 Furthermore, the results of a recent study indicated that the ACR may predict changes in ambulatory blood pressure in normotensive individuals.17 According to Jia et al,18 hypertension and glucose metabolism disorders are important factors affecting the ACR positive rate; this rate is significantly elevated in response to an increase in those risk factors. The US Kidney Disease Outcomes Quality Initiative guidelines19 recommend the random calculation of the urine ACR for the measurement of total urinary protein. This indicator reflects dehydration and other conditions that cause changes in urinary concentrations. Moreover, it is a simpler and more convenient method than 24-h urine protein quantitative assays, and provides accurate results. In the present study, the levels of sCr, BUN, and UA were markedly increased in the high-ACR group compared with the low-ACR group, particularly among subjects with an ACR >300 mg/g.
The eGFR is a good indicator of glomerular filtration function.20,21 In this study, the eGFR declined with the increasing urinary ACR. Interestingly, the eGFR was negatively correlated with sCr, BUN, and UA in the groups with an ACR of 30–300 and >300 mg/g. These results further confirmed the diagnostic value of ACR for CKD. Moreover, the number of patients with stage ≥2 CKD was significantly higher in the group with an abnormal urinary ACR than in that with a normal urinary ACR. Therefore, the combination of the eGFR and ACR may be helpful for the early detection of CKD.
The correlation between CKD and age has been investigated previously, and it has been widely recognized that the risk of CKD increases with the age.22,23 In the current study, the correlation between age and CKD has been explored. Interestingly, for the patients between 20 and 40 years, most of the CKD related index, ie eGFR, sCr and BUN showed no significant difference between microalbuminuria group compared with the normal proteinuria group, suggesting that for people less than 40 years old, CKD can be unrecognized and ACR may not reflect the severity of the disease; in contrast, for patients over 40 years old, eGFR, sCr, BUN and UA were all markedly increase in microalbuminuria and macroalbuminuria group in comparison with the normal proteinuria group. Taken together, our results suggested that ACR may function as a sensitive bio-marker for the diagnosis of CKD among middle-aged and elderly but not for the young adults.
Both our data and previous results suggested that males are associated with a higher incident rate of ACR than females.24 Therefore, 41–60 and >61 groups were divided into male and female groups, and CKD-related parameters were analyzed. For the 41–60 males, only eGFR significantly decreased in microalbuminuria group compared with the normal proteinuria group, while for the 41–60 females, only showed no significant difference between microalbuminuria group and normal proteinuria group. The above data suggested that ACR is sensitive for both middle-aged males and females. On the other hand, for the >61 males, eGFR, sCr and BUN all significantly changed between microalbuminuria group and normal proteinuria group while for the >61 females, eGFR, sCr and BUN all showed no significant difference between microalbuminuria group and normal proteinuria group, as well as microalbuminuria group and macroalbuminuria group. These results suggested that for the diagnosis of CKD among the elderly, ACR is gender sensitive for males, and ACR may not reflect the severity of the disease among females. However, our results still need to be confirmed with larger population.
The current work has limitations. First, while the current work focuses on ACR, Hb/Hct-related data were not collected. Hb/Hct levels should be investigated in future works, which will enhance the study’s relevance and broaden its scope. Moreover, the elderly females are less likely to effective clean the vulva compared to males and this may affect the level of ACR.
In summary, we investigated the potential diagnostic value of ACR for the early diagnosis of CKD among patients in Southeast China. We found that ACR may function as a sensitive bio-marker for the diagnosis of CKD among middle-aged and elderly but not for the young adults; we also proved that among the elderly, ACR is gender sensitive for males. Our data may assist in the early diagnosis and treatment of renal damage, especially among the elderly males.
Funding
This research was supported by Suzhou Health Management Association Research project (JKGL220104).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ene-Iordache B, Perico N, Bikbov B, et al. Chronic kidney disease and cardiovascular risk in six regions of the world (ISN-KDDC): a cross-sectional study. Lancet Glob Health. 2016;4(5):e307–19.
2. Zhang L, Wang F, Wang L, et al. Prevalence of chronic kidney disease in China: a cross-sectional survey. Lancet. 2012;379(9818):815–822.
3. Song Y, Lobene AJ, Wang Y, Hill Gallant KM. The DASH Diet and Cardiometabolic Health and Chronic Kidney Disease: a Narrative Review of the Evidence in East Asian Countries. Nutrients. 2021;13(3):984.
4. Liu ZH. Nephrology in China. Nat Rev Nephrol. 2013;9(9):523–528.
5. Wang H, Ainiwaer A, Song Y, et al. Perturbed gut microbiome and fecal and serum metabolomes are associated with chronic kidney disease severity. Microbiome. 2023;11(1):3.
6. Navaneethan SD, Zoungas S, Caramori ML, et al. Diabetes Management in Chronic Kidney Disease: synopsis of the KDIGO 2022 Clinical Practice Guideline Update. Ann Intern Med. 2023;176(3):381–387.
7. George C, Hill J, Nqebelele U, Peer N, Kengne AP. Leveraging the South African Diabetes Prevention Programme to screen for chronic kidney disease: an observational study. BMJ Open. 2023;13(1):e068672.
8. Levey AS, Gansevoort RT, Coresh J, et al. Change in Albuminuria and GFR as End Points for Clinical Trials in Early Stages of CKD: a Scientific Workshop Sponsored by the National Kidney Foundation in Collaboration With the US Food and Drug Administration and European Medicines Agency. Am J Kidney Dis. 2020;75(1):84–104.
9. Floege J, Barbour SJ, Cattran DC, et al. Management and treatment of glomerular diseases (part 1): conclusions from a Kidney Disease: improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019;95(2):268–280.
10. Liao S, Lin D, Feng Q, et al. Lipid Parameters and the Development of Chronic Kidney Disease: a Prospective Cohort Study in Middle-Aged and Elderly Chinese Individuals. Nutrients. 2022;15(1):112.
11. Chang CC, Su MJ, Ho JL, et al. The efficacy of semi-quantitative urine protein-to-creatinine (P/C) ratio for the detection of significant proteinuria in urine specimens in health screening settings. Springerplus. 2016;5(1):1791.
12. Yu G, Cheng J, Li H, Li X, Chen J. Comparison of 24-h Urine Protein, Urine Albumin-to-Creatinine Ratio, and Protein-to-Creatinine Ratio in IgA Nephropathy. Front Med. 2022;9:809245.
13. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimate glomerular filtration rate. Ann Intern Med. 2009;150(9):604–612.
14. Yanai H, Adachi H, Hakoshima M, Katsuyama H. Molecular Biological and Clinical Understanding of the Pathophysiology and Treatments of Hyperuricemia and Its Association with Metabolic Syndrome, Cardiovascular Diseases and Chronic Kidney Disease. Int J Mol Sci. 2021;22(17):9221.
15. Satoh M. Elevated albumin-to-creatinine ratio as a risk factor for stroke and homocysteine as an effect modifier in hypertensive Asian individuals. Hypertens Res. 2022;45(1):170–171.
16. Turkyilmaz E, Ozkalayci F, Birdal O, et al. Serum Albumin to Creatinine Ratio and Short-Term Clinical Outcomes in Patients With ST-Elevation Myocardial Infarction. Angiology. 2022;73(9):809–817.
17. Gerber LM, Schwartz JE, Pickering TG. Albumin-to-creatinine ratio predicts change in ambulatory blood pressure in normotensive persons: a 7.5-year prospective study. Am J Hypertens. 2006;19(2):220–226.
18. Jia W, Gao X, Pang C, et al. Prevalence and risk factors of albuminuria and chronic kidney disease in Chinese population with type 2 diabetes and impaired glucose regulation: shanghai diabetic complications study (SHDCS). Nephrol Dial Transplant. 2009;24(12):3724–3731.
19. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(2 Suppl 1):S1–266.
20. Kuppachi S, Norman SP, Lentine KL, Axelrod DA. Using race to estimate glomerular filtration and its impact in kidney transplantation. Clin Transplant. 2021;35(1):e14136.
21. Husain SA, King KL, Mohan S. Differences between race-based and race-free estimated glomerular filtration rate among living kidney donors. Am J Transplant. 2022;22(5):1504–1505.
22. Liu P, Quinn RR, Lam NN, et al. Accounting for Age in the Definition of Chronic Kidney Disease. JAMA Intern Med. 2021;181(10):1359–1366.
23. Ma Y, Lin J, Xia P, et al. Comparison of the profiles of patients defined by age-adapted and fixed threshold CKD criteria: a nationwide, cross-sectional study. Clin Kidney J. 2022;15(12):2312–2321.
24. Park SI, Kim J, Yu KS, Jang IJ, Lee S. Changes in Cardiac Function After a Single Intravenous Administration of CKD-712 in Healthy Male Volunteers. Clin Drug Investig. 2017;37(4):393–403.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.