Back to Journals » International Journal of General Medicine » Volume 16
Aftereffects in Epigenetic Age Related to Cognitive Decline and Inflammatory Markers in Healthcare Personnel with Post-COVID-19: A Cross-Sectional Study
Authors Nolasco-Rosales GA ![]() , Alonso-García CY, Hernández-Martínez DG, Villar-Soto M, Martínez-Magaña JJ, Genis-Mendoza AD, González-Castro TB
, Alonso-García CY, Hernández-Martínez DG, Villar-Soto M, Martínez-Magaña JJ, Genis-Mendoza AD, González-Castro TB ![]() , Tovilla-Zarate CA
, Tovilla-Zarate CA ![]() , Guzmán-Priego CG
, Guzmán-Priego CG ![]() , Martínez-López MC, Nicolini H
, Martínez-López MC, Nicolini H ![]() , Juárez-Rojop IE
, Juárez-Rojop IE ![]()
Received 1 July 2023
Accepted for publication 16 October 2023
Published 31 October 2023 Volume 2023:16 Pages 4953—4964
DOI https://doi.org/10.2147/IJGM.S426249
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Germán Alberto Nolasco-Rosales,1,* Cecilia Yazmin Alonso-García,1,* David Gustavo Hernández-Martínez,1 Mario Villar-Soto,2 José J Martínez-Magaña,3 Alma Delia Genis-Mendoza,4 Thelma Beatriz González-Castro,5 Carlos Alfonso Tovilla-Zarate,6 Crystell Guadalupe Guzmán-Priego,1 Mirian Carolina Martínez-López,1 Humberto Nicolini,7 Isela Esther Juárez-Rojop1
1División Académica de Ciencias de la Salud, Universidad Juarez Autónoma de Tabasco, Villahermosa, Tabasco, México; 2Hospital Regional de Alta Especialidad de Salud Mental, Villahermosa, Tabasco, México; 3Department of Psychiatry, Yale University School of Medicine, New Haven, CT, USA; 4Hospital Psiquiátrico Infantil “Dr. Juan N. Navarro”, Ciudad de México, México; 5División Académica Multidisciplinaria de Jalpa de Méndez, Universidad Juarez Autónoma de Tabasco, Jalpa de Méndez, Tabasco, México; 6División Académica Multidisciplinaria de Comalcalco, Universidad Juarez Autónoma de Tabasco, Comalcalco, Tabasco, México; 7Departamento de Genética Psiquiátrica, Instituto Nacional de Medicina Genómica (INMEGEN), Ciudad de México, México
*These authors contributed equally to this work
Correspondence: Isela Esther Juárez-Rojop, División Académica de Ciencias de la Salud, Universidad Juarez Autónoma de Tabasco, Av. Gregorio Méndez 2838-A, Col. Tamulté, Villahermosa, 86100, México, Email [email protected] Humberto Nicolini, Instituto Nacional de Medicina Genómica (INMEGEN), Ciudad de México, 86100, México, Email [email protected]
Purpose: Epigenetic age and inflammatory markers have been proposed as indicators of severity and mortality in patients with COVID-19. Furthermore, they have been associated with the occurrence of neurological symptoms, psychiatric manifestations, and cognitive impairment. Therefore, we aimed to explore the possible associations between epigenetic age, neuropsychiatric manifestations and inflammatory markers (neutrophil-lymphocyte ratio [NLR], platelet-lymphocyte ratio [PLR], monocyte-lymphocyte ratio [MLR], and systemic immune-inflammation index [SII]) in healthcare personnel with post-COVID condition.
Patients and Methods: We applied the Montreal Cognitive Assessment (MoCA) and Mini-Mental State Examination (MMSE) tests to 51 Mexican healthcare workers with post-COVID-19 condition; we also estimated their epigenetic age using the PhenoAge calculator.
Results: The participants had a post-COVID condition that lasted a median of 14 months (range: 1– 20). High NLR (> 1.73) had association with mild cognitive impairment by MMSE (p=0.013). Likewise, high MLR (> 0.24) were associated with language domain in MOCA (p=0.046). Low PLR (< 103.9) was also related to delayed recall in MOCA (p=0.040). Regarding comorbidities, hypertension was associated with SII (p=0.007), overweight with PLR (p=0.047) and alcoholism was associated with MLR (p=0.043). Interestingly, we observed associations of low PLR (< 103.9) and low SII (< 1.35) levels with increased duration of post-COVID condition (p=0.027, p=0.031). Likewise, increases in PhenoAge were associated with high levels of SII (OR=1.11, p=0.049), PLR (OR=1.12, p=0.035) and MLR (OR=1.12, p=0.030).
Conclusion: We observed neurocognitive changes related to inflammatory markers and increases in epigenetic age in healthcare personnel with post-COVID-19 condition. Future research is required to assess mental and physical health in individuals with post-COVID-19 symptoms.
Keywords: post-COVID-19, cognitive manifestation, inflammatory markers, epigenetic age
Introduction
Aging is a biological process that has been related to disease and mortality, which is reflected in molecular characteristics, epigenetic modifications, and telomere wear and tear.1 However, individuals with the same chronological age exhibit differences in their underlying biological aging process that could reflect different susceptibilities to age-related diseases.2 The biological differences between individuals can be expressed via epigenetic age, an estimation of age in years resulting from a mathematical algorithm based on the DNA methylation.3 Although DNA methylation is the primary method for estimating epigenetic age, clinical biomarkers (biochemical parameters and blood cell count) can be used as a surrogate measure,2 by using a calculator for epigenetic age. The Horvath-Levine PhenoAge Calculation combines the results of 9 blood parameters and uses the Horvath-Levine Blood Component PhenoAge Equation; its results correlate strongly with age in every tissue and cell tested.2,4 The epigenetic age could be altered due to viral infections and DNA methylation, which has been shown to correlate with the aging process and can be used to estimate epigenetic aging in tissues.1 Similarly, several studies have shown increased epigenetic ages in COVID-19 survivors;5,6 these changes due to SARS-CoV2 could be short-lasting or permanent. Therefore, there should be a post-COVID-19 monitoring of survivors.6
Evidence indicates that COVID-19 is associated with neurologic symptoms, acute and chronic psychiatric manifestations, as well as cognitive impairment.7–9 COVID-19 induces persistent symptoms after the acute phase such as muscle pain and weakness, headache, sleep disturbances, palpitations, sleep problems, anxiety, low-grade fever, and physical and mental fatigue.7–9 Importantly, cognitive impairment is observed as one of the consequences in patients with COVID who developed mild symptoms.10–13 It has been reported that 48 to 56% of individuals who presented COVID-19, have a cognitive decline afterwards, particularly after a severe infection by SARS-CoV-2.14,15
On the other hand, several studies have shown that a disruption of immune and inflammatory responses caused by SARS-CoV-2 infection can lead to long-term disorders.16 In this sense, inflammatory markers such as the systemic immune-inflammation index (SII), neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR) and monocyte-lymphocyte ratio (MLR) have been prognostic biomarkers in tumors, cardiovascular diseases, and COVID-19.17,18 Recently, the “post-COVID-19 condition” is considered when after three months of having the SARS-CoV2 infection, the individual has persistent symptoms for at least two months, and no alternative diagnosis has been made.8,19 Additionally, high levels of inflammatory markers have been observed in individuals with post-COVID-19 symptoms, indicating that there is a relationship between immunity and post-COVID condition.16
Evidence that individuals have post-COVID condition is increasing every day. However, to the best of our knowledge, there is a paucity of studies relating phenotypic age, inflammatory markers and cognitive characteristics in healthcare workers with post-COVID-19 condition. In this study, our aim was to explore the possible associations between neurocognitive manifestations, inflammatory markers and epigenetic age, in Mexican healthcare workers who present post-COVID-19 condition.
Materials and Methods
Participants
This is a descriptive and cross-sectional study. We recruited 51 healthcare workers with a previous diagnosis of COVID-19 who work at the Mental Health Regional High Specialty Hospital in Tabasco, Mexico; the data collection was from August to December 2021. We included healthcare personnel (physicians, nurses, chemists, and pharmacists) of 18–60 years of age, who had been diagnosed with a positive PCR test for SARS-CoV-2 and recovered from COVID-19 at least four weeks before the evaluation. The participants were diagnosed between March 2020 and October 2021 (range: 1–20 months post-COVID-19). Exclusion criteria were recent infection with SARS-CoV-2 confirmed by PCR test, diagnosis of chronical or recent acute infectious diseases, clinical history off autoimmune diseases or cancer, history of a mental health disorder, and previous diagnosis of neurocognitive impairment. A psychiatrist evaluated the mental health and neurocognitive impairment history of the participants.
Study Design
We interviewed the participants and gathered information about their medical history, sociodemographic data, symptoms of acute COVID-19 disease, and anthropometric measurements. We conducted face-to-face surveys to 51 healthcare workers: the Mini-Mental State Examination (MMSE) and Montreal Cognitive Assessment (MoCA) neurocognitive scales.20,21 We employed the Spanish version of the MoCA test, a validated scale for the Mexican population.22 MoCA scores ≥26 indicate normal cognitive functioning, while lower scores indicate a mild neurocognitive impairment; 1 point is added to patients with ≤12 years of schooling. The MMSE scale used was a validated version for the Mexican population.23 MMSE is associated with the identification of moderate to severe cognitive impairment; it has a maximum score of 30, scores >24 points are normal, and ≤24 is neurocognitive impairment moderate to severe. Both the MoCA and the MMSE were obtained from the guidelines of the National Institute of Geriatrics in Mexico (INGer).24
Epigenetic Age and Inflammatory Markers
From each participant, venous blood samples were taken in tubes with and without EDTA to determinate the inflammatory markers and epigenetic age. The hemogram test was determined with CELL-DYN Ruby (Abbott). Data from the hemogram was used to calculate SII, NLR, PLR, and MLR using the following formulas: NLR= neutrophils count/lymphocytes count, PLR= platelets count/lymphocytes count, MLR= monocytes count/lymphocytes count, and SII index= (platelets count × neutrophils count)/lymphocytes count. We divided all inflammatory markers into low, medium, and high categories using tertiles: <3.16x103, 3.16–4.74×103 and >4.743 x103 for SII, <1.35, 1.35–1.73 and >1.73 for NLR, <103.9, 103.9–134.8 and >134.8 for PLR, and <0.1860, 0.1860–0.2487 and >0.2487 for MLR, respectively. Stratifying the inflammatory ratios in tertiles is commonly used in literature.25,26
We determined albumin (g/L), alkaline phosphatase (U/L), creatinine (µmol/L), fasting glucose (mmol/L), C-Reactive Protein (mg/L), using the Cm250 (Wiener Lab ®). These biochemical parameters were required to calculate the phenotypic age. We utilized the Horvarth-Levine PhenoAge Calculator to estimate phenotypic age, DNA methylation, Δ age (Phenotypic age - Chronological age), and 10-year mortality.4
Statistical Analysis
We expressed numerical variables as mean ± standard deviation for variables with normal distribution, and median (interquartile range [IQR]) for variables with non-normal distribution. Categorical data was expressed as frequencies and percentages (%). We used the Shapiro–Wilk test to assess normality in our variables. To compare inflammatory markers tertiles, we used the Chi-squared test for categorical variables and ANOVA test for numerical data. Later, we performed ordinal logistic regression analysis for SII, NLR, PLR, and MLR; all models included the duration (in months) that the post-COVID-19 condition lasted, MMSE total score, PhenoAge, and associated features as cofounding variables. Ordinal logistic regression results were expressed as odds ratio and 95% CI for the highest tertile of inflammatory markers. Comparisons of the PhenoAge estimations and the neurocognitive scores were made using ANOVA test and Kruskal–Wallis test. The effect size was estimated using Cramér’s V (V), Cohen’s D (d), Eta-squared (η2), Cliff’s delta (δ) and ranked Eta-squared (η2H) (for Chi-squared, t-Student, ANOVA, Mann–Whitney U and Kruskal–Wallis tests, respectively). A p-value <0.050 was considered significant for all the analyses. Shapiro–Wilk, Chi-squared, t-Student, ANOVA, Mann–Whitney U, and Kruskal–Wallis tests were made with SPSS v. 26. The effect size and logistic regression analyses were performed with R v.4.2. Word cloud of comorbidities was performed with the wordcloud package for R. Density plots and bump charts were performed with ggplot2, ggbump, and patchwork packages for R.
Ethical Considerations
We followed the Official Mexican Standard NOM-012-SSA3-2012 guidelines and the ethical principles of the Declaration of Helsinki to perform this research. Additionally, this study was approved by the ethics committee of the Mental Health Hospital “Villahermosa” in Mexico (HRAESM/DG/UEI/467/2021). The participants received verbal and written information about the objectives of this study. Every person participated voluntarily without receiving any remuneration and signed an informed consent.
Results
Sociodemographic and Clinical Characteristics of Healthcare Personnel with Post-COVID-19 Condition
This study included 51 healthcare workers (29 females and 22 males); their mean age was 40.57 (10.96) years. We also evaluated variables such as schooling (16.32 [4.08] years) and Body Mass Index (29.72 [6.52]). We observed that 92.15% (n=47) of participants had mild symptoms of COVID-19 and required home treatment in social isolation, and only 1.96% (n=1) were treated in hospital. The duration of the post-COVID condition showed a median of 14 (4.5–16.5) months. According to the MoCA test, we identified 76.47% (n=47) healthcare personnel with mild cognitive impairment. Nonetheless, the MMSE showed that 7.84% (n=4) of healthcare workers had scores indicating mild neurocognitive impairment. (Table 1)
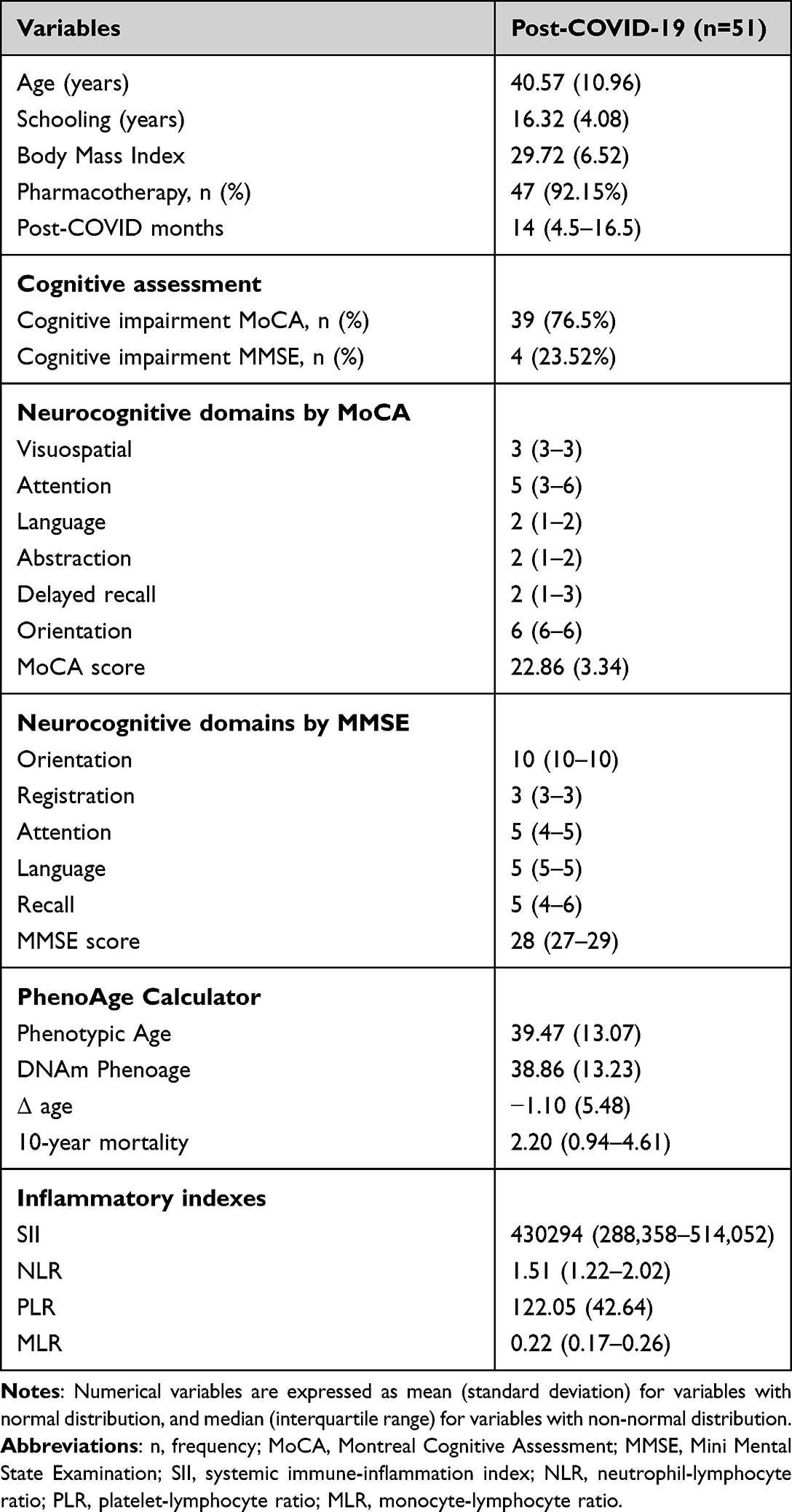 |
Table 1 Sociodemographic, Clinical Characteristics and Cognitive Assessment in Post-COVID-19 Mexican Healthcare Personnel |
Inflammatory Ratios in Post-COVID-19 Healthcare Personnel
A high NLR was associated with mild cognitive impairment measured by MMSE (p=0.013, V=0.36); nonetheless, we did not observe an association with MoCA. Figure 1A shows the proportion of patients with and without cognitive impairment among inflammatory marker tertiles.
 |
Figure 1 Associations between inflammatory markers’ tertiles, cognitive and epigenetic age features. Notes: (A–E) Cognitive domains and inflammatory markers’ distributions. (F–J) PhenoAge features and inflammatory markers’ distributions. All features were significant in Chi-square and ANOVA test (p<0.05). |
Cognitive domains showed different associations. Figure 1B–E shows the association between the inflammatory markers tertiles and the cognitive domains scores. The language domain in MoCA was associated with medium NLR and high MLR (respectively: p=0.022, η2H=0.12; p=0.047, η2H=0.12); likewise, low PLR levels were associated with a delayed recall in MoCA (p=0.040, η2H=0.09). In addition, high MLR levels were significant in language score measured by MMSE (p=0.046, η2H=0.02).
The most common comorbidities presented in this population were overweight and obesity (n = 22, 43.14%), hypertension (n = 11, 21.57%), alcoholism (n = 7, 13.73%), and diabetes (n = 4, 7.84%). The analysis of inflammatory markers indicated that high levels of SII were associated with hypertension (p=0.007, V=0.40) (Supplementary Figure S1A). Overweight (BMI 25–29.9) had significant association with high PLR (p=0.047, V=0.29). Notably, individuals with overweight in our sample had higher mean NLR, MLR and SII compared with obesity and normal weight; nonetheless, we found not significant differences. Also, alcoholism was associated with medium MLR levels (p=0.043, V=0.29). Regarding pharmacotherapy, we found that medium MLR values were associated with the use of hydroxychloroquine for COVID-19 acute treatment (p=0.041, V=0.29). Overall, the most frequent post COVID-19 symptoms were dysgeusia (n = 41, 80.39%), anosmia (n = 39, 76.47%), and headaches (n = 36, 70.59%). Some symptoms were associated with different levels of NLR: high NLR levels were associated with sudden onset (p=0.005, V=0.40), rhinorrhea (p=0.005, V=0.41) and abdominal pain (p=0.025, V=0.33), while low levels of NLR were associated with arthralgia (p=0.048, V=0.29). (Supplementary Figure S1B–S1H). Interestingly, we observed associations of low PLR and SII levels with longer duration (in months) of the post-COVID-19 condition (respectively: p=0.027, η2=0.14; p=0.031, η2=0.13). (Supplementary Figure S1I–S1J)
Epigenetic Age in Healthcare Personnel with Post-COVID-19 Condition
We observed a slightly higher chronologic age (40.55 [11.0]) than the phenotypic age (39.38 [13.12]) and DNAm PhenoAge (38.78 [13.28]) in healthcare workers with post-COVID-19 condition. The mean Δ age was −0.62 (5.55), and the mortality for 10 years was 3.16 (3.17). Notably, we found associations between high SII levels and higher phenotypic age, as well as DNAm PhenoAge (respectively: p=0.048, η2=0.12; p=0.038, η2=0.13); while high NLR was associated with DNAm PhenoAge (p=0.049 η2=0.12). Likewise, high SII levels increased the 10-year mortality (p = 0.044, η2H=0.12) (Figure 1F–J).
Logistic Regression: Epigenetic Age and Inflammatory Markers
The duration (in months) of post-COVID-19 condition showed strong associations with decreased levels of SII (OR=0.87, 95% CI: 0.78–0.96, p=0.008), NLR (OR=0.85, 95% CI: 0.75–0.96, p=0.008) and PLR (OR=0.86, 95% CI: 0.77–0.96, p=0.005). Regarding cognitive impairment, increases in MMSE total score resulted in higher PLR (OR=1.19, 95% CI: 1.00–1.42, p=0.046). Remarkably, arthralgia reduced NLR (OR=0.19, 95% CI: 0.05–0.83, p=0.028). On the other hand, rhinorrhea (OR=5.46, 95% CI: 1.11–26.82, p=0.037) and abdominal pain (OR=29.76, 95% CI: 2.23–396.23, p=0.010) increased risk for high NLR. In comorbidities, hypertension was associated with high SII (OR=10.34, 95% CI: 1.49–72.02, p=0.018). Interestingly, one-year increases in PhenoAge were associated with high levels of SII (OR=1.11, 95% CI: 1.00–1.23, p=0.049), PLR (OR=1.12, 95% CI: 1.01–1.25, p=0.035) and MLR (OR=1.12, 95% CI: 1.01–1.24, p=0.030).
Epigenetic Age and Neurocognitive Domains
We associated the neurocognitive scores with the PhenoAge estimations. Interestingly, we found that lower delayed recall scores (MoCA) were related to older phenotypic age, DNAm Phenoage, and chronological age (p<0.005, η2=0.33 in all tests); also, higher 10-year mortality showed lesser scores in this domain (p=0.004, η2H=0.27) (Table 2). In addition, healthcare personnel with mild cognitive impairment by MoCA scores had higher phenotypic age (41.91 [12.91] vs 31.54 [10.51], p=0.014, d=0.84), DNAm PhenoAge (41.45 [12.63] vs 30.45 [11.99], p=0.010, d=0.88), chronological age (42.56 [10.60] vs 34.08 [9.89], p=0.017, d=0.81) and 10-year mortality (2.41 [1.0–5.8] vs 0.95 [0.43–1.38], p=0.011, δ=0.49). We did not find associations between MMSE domains and the PhenoAge estimations.
 |
Table 2 Associations Between PhenoAge Estimations, Chronological Age, and Delayed Recall Cognitive Domain |
Discussion
Epigenetic Age and Inflammatory Markers in Healthcare Personnel with Post-COVID-19
Data from this research may contribute to understand the post-COVID condition shown by health care workers in relation to epigenetic age, inflammatory markers and cognitive characteristics. For instance, we obtained an association between increased epigenetic age and high SII, NLR, MLR in healthcare workers with post-COVID-19 condition. Literature indicates that methylation derived NLR is a marker of high cardiovascular risk; while high SII and NLR values were found in non-surviving COVID-19 patients.27 Koestler et al have suggested that DNA methylation could be used to estimate NLR and MLR in cancer.28 In our study, the 10-year mortality risk (calculated with PhenoAge) was associated with SII in individuals with post-COVID-19 condition; in this sense, it has been suggested that epigenetic age acceleration and inflammatory markers are associated with the severity of COVID-19.29,30 It is known that epigenetic age in blood reflects both, the chronological age and aspects of the biological age; a higher epigenetic age is associated with a higher mortality and the risk of age-related comorbidities. The epigenetic changes due to COVID-19 include increases in epigenetic age, methylation regulation of Angiotensin Converting Enzyme 2, and immune response genes.31 In this regard, it has been observed that SARS-CoV-2 induces changes in DNA methylation, generating the expression of immune response inhibitor genes; also, individuals with COVID-19 present a downregulation of ACE2, while in individuals with post-COVID-19 condition the expression of ACE2 mRNA is reduced. However, in young individuals with post-COVID-19 condition, an accelerated DeltaAge correlated with lower ACE2 mRNA levels, indicating an adverse effect of DNAmAge on peripheral blood ACE2 density.32
Cao et al suggested that the DNA methylation changes due to SARS-CoV-2 infection may affect the expression of the metabolic process and epigenetic aging due to COVID-19;5 these authors found a reversible influence of epigenetic aging and COVID-19 in some patients with post-COVID-19 condition. Similarly, previous studies have shown that HIV and SARS-CoV-2 infections alter the host cell epigenetic landscape. All these findings suggest that COVID-19 may be involved in the epigenetic clock.1 Nonetheless, some studies have been unsuccessful in associating increased epigenetic age with a higher risk for severe COVID-19.32,33
Neurocognitive Symptoms and Inflammatory Ratios in Post-COVID-19 Healthcare Personnel
We found a neurocognitive decline in healthcare workers with post-COVID-19 condition when assessed with MoCA. Various studies suggest that COVID-19 is associated with neurological, psychiatric manifestations and cognitive impairment.34,35 Bolattürk & Soylu (2022) showed that an early-stage cognitive impairment was detected in 15% of patients with COVID-19 by MMSE, and neurocognitive impairment was detected in 55% of patients by MOCA.36 Other findings have shown some dysfunction of episodic memory, visuospatial domain, slowness for ideation, and alteration of executive functions in patients previously hospitalized for COVID-19.37 Crunffli et al, have reported that 34 to 56% of individuals who recovered from COVID-19 (not hospitalized) presented impaired cognitive function after the diagnosis of COVID-19 (59 days later).38 Interestingly, a study in northern Israel found a characteristic cognitive profile of post-COVID condition related to executive function, language, and attention.13 Cecchetti et al suggested that COVID-19 increases the fragility of brain structures involved in memory processes.39 Other research on post-COVID-19 individuals showed that executive function, language and attention scores were significantly worse than in individuals without post-COVID-19 symptoms.40 In this sense, other findings have shown the dysfunction of episodic memory, visuospatial domain, slowness for ideation and alteration of executive functions in patients previously hospitalized for COVID-19.37
In our study, higher NLR, PLR and MLR were associated with neurocognitive decline (language and delayed recall. Many authors have suggested that inflammation is associated with cognitive dysfunction; in fact, a high NLR has recently been described in mild cognitive impairment. Some studies have shown that NLR is significantly higher in patients with dementia than in controls. Another study reported a correlation between NLR and cognitive decline in individuals with small cerebral blood vessel disease.41–43 High levels of neutrophils characterize chronic inflammation, reflecting the intensity of stress and systemic inflammation (chronic activation of the innate immune system); while a low level of lymphocytes may be indicative of a reduced response to pathogens.44 Maamar et al mentioned that post-COVID-19 condition involve inflammatory mechanisms, immune responses and psychological factors.16 Consistent with our findings, a study showed that high SII was a predictor of developing depression and anxiety in patients with TB.45 In contrast, a reduction in SII observed between admission and discharge may predict the alleviation of depression among survivors of coronavirus disease.5 These findings suggest a consistent association between inflammation and mental disorders.
We found that a longer duration of post-COVID condition (measured in months) was associated with lower SII, NLR, and PLR indices. Previous studies indicate that PLR, NLR and platelets could be efficacious markers of the severity and prognosis of COVID-19.46,47 NLR, MLR, PLR and SII have also been proposed as biomarkers to assess the severity, morbidity, mortality and prognosis of psychiatric and non-psychiatric illnesses.48 Likewise, it has been reported that NLR and other inflammatory markers decrease after a few weeks compared to acute COVID-19 levels49,50 Although SII, NLR and PLR are suggested to predict the risk of severe COVID-19 and mortality, the inflammatory indices could decrease over time in COVID-19 survivors.30,49,51 According to this, individuals with post-COVID condition have shown a relationship between the severity of deterioration and age, where younger patients show impairment in some cognitive domain more frequently than older ones.15,52 Surprisingly though, young people were considered to have better expectations, because a younger age induces a better prognosis in dementia and acquired brain damage. Herrera et al mentions that cognitive difficulties after SARS-Cov2 infection continue for up to two years or more.15 In contrast, patients with a longer evolution time showed better results in verbal learning and visual memory recall.
At the same time, we identified that hypertension was associated with SII in healthcare personnel with post-COVID-19 condition. Other authors found that SII may be a better indicator than NLR and PLR in treatment-naïve hypertensive patients17 and patients with coronary heart disease.53 We also found associations between overweight and PLR. Metabolic syndrome and other comorbidities combined with obesity (eg polycystic ovary syndrome, osteoporosis and cancer) are related with increased levels of inflammatory markers.54–57 Although some studies report that overweight and obesity alone increase the levels of NLR, PLR and SII, these associations are not consistent.58–60 Figure 2 shows the most frequent comorbidities with the largest font, while less frequent comorbidities appear with decreasing font size. Various studies have shown that individuals with comorbidities or chronic diseases are more likely to develop post-COVID-19 condition.19,61 Finally, NLR was associated with rhinorrhea, abdominal pain and arthralgia in our analysis. Maamar et al found differences in inflammatory markers and frequencies of symptoms in mild COVID-19; nonetheless, they reported that high NLR was related to anosmia, ageusia, and fatigue.16
 |
Figure 2 Comorbidities in post-COVID-19 Mexican healthcare workers. Notes: The font size differences indicate changes in frequencies of comorbidities. The most frequent comorbidity, overweight (n=24), is eight times bigger than the least frequent comorbidity, asthma (n=2). |
Some studies indicate that acute viral infection with SARS-CoV-2 alters the inflammatory and immune response, and this could also cause post-COVID 19 condition.16 Proinflammatory factors released by peripheral cells (lymphocytes, monocytes, neutrophils) are known to participate in neuroinflammation by activating astrocytes and microglia and modulating brain areas involved in mood regulation. Proinflammatory factors also decrease the concentration of intracerebral monoamines, trigger neuroendocrine responses, promote excitotoxicity (increased glutamate) and impair brain plasticity.62 Evidence links cortical (frontal, temporal and parietal cortex) and blood brain barrier dysfunction in individuals with post-COVID-19 condition with cognitive impairment. This dysfunction has been suggested to be related to vasculitis, hyperinflammation (cytokines), coagulopathy, and cerebral complications (cerebral hypoperfusion, hypometabolism, and hypoxia) induced by SARS-CoV-2 infection. Altogether, proinflammatory factors can be involved in cognitive impairment in individuals with post-COVID 19 condition.39,63,64
This study has some limitations. We observed a limited participation of healthcare personnel with post-COVID-19 condition; additionally, healthcare personnel showed lack of free time to participate in the study, then, our sample size is small. Another limitation is that possible cofactors could not be considered in our multivariable analysis. We could not establish causal relationships because of the cross-sectional nature of this study. Finally, our results cannot be extrapolated to the Mexican population as they come from one specific sample.
Conclusion
We observed that epigenetic age and 10-year estimated mortality were associated with altered concentrations of inflammatory markers (NLR, PLR, MLR and SII). In addition, inflammatory markers were associated with the duration of post-COVID condition, neurocognitive decline (language and delayed recall) and comorbidities. With all these findings, we suggest that the assessment of epigenetic age, inflammatory markers and neurocognitive scales could help to elucidate the neuropsychiatric sequelae in healthcare personnel with post-COVID-19 condition. Future research is required to evaluate if these alterations are maintained, improved, or worsen over time in post-COVID-19 condition.
Copyright and Licenses
An unauthorized modified version of the Spanish MMSE was used by the study team without permission. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Acknowledgments
The authors thank CONAHCYT for supporting Germán Alberto Nolasco-Rosales with the scholarship No. 813279.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang K, Liu H, Hu Q, et al. Epigenetic regulation of aging: implications for interventions of aging and diseases. Signal Transduct Target Ther. 2022;7(1):374. doi:10.1038/s41392-022-01211-8
2. Levine ME, Lu AT, Quach A, et al. An epigenetic biomarker of aging for lifespan and healthspan. Aging. 2018;10(4):573–591. doi:10.18632/aging.101414
3. Horvath S, Raj K. DNA methylation-based biomarkers and the epigenetic clock theory of ageing. Nat Rev Genet. 2018;19(6):371–384. doi:10.1038/s41576-018-0004-3
4. Zolman O. Horvath-Levine PhenoAge Calculator (defunct). 20one Consulting Ltd; 2023. Available from: https://www.oliverzolman.com/phenoage-calculator.
5. Cao X, Li W, Wang T, et al. Accelerated biological aging in COVID-19 patients. Nat Commun. 2022;13(1):2135. doi:10.1038/s41467-022-29801-8
6. Mongelli A, Barbi V, Gottardi Zamperla M, et al. Evidence for biological age acceleration and telomere shortening in COVID-19 survivors. Int J Mol Sci. 2021;22(11):6151. doi:10.3390/ijms22116151
7. Sivan M, Taylor S. NICE guideline on long covid. BMJ. 2020;371:m4938. doi:10.1136/bmj.m4938
8. Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV. A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis. 2022;22(4):e102–e107. doi:10.1016/S1473-3099(21)00703-9
9. Azcue N, Gómez-Esteban JC, Acera M, et al. Brain fog of post-COVID-19 condition and chronic fatigue syndrome, same medical disorder? J Transl Med. 2022;20(1):569. doi:10.1186/s12967-022-03764-2
10. Tavares-Júnior JWL, de Souza ACC, Borges JWP, et al. COVID-19 associated cognitive impairment: a systematic review. Cortex. 2022;152:77–97. doi:10.1016/j.cortex.2022.04.006
11. Crivelli L, Palmer K, Calandri I, et al. Changes in cognitive functioning after COVID-19: a systematic review and meta-analysis. Alzheimers Dement. 2022;18(5):1047–1066. doi:10.1002/alz.12644
12. Ceban F, Ling S, Lui LMW, et al. Fatigue and cognitive impairment in Post-COVID-19 Syndrome: a systematic review and meta-analysis. Brain Behav Immun. 2022;101:93–135. doi:10.1016/j.bbi.2021.12.020
13. Hadad R, Khoury J, Stanger C, et al. Cognitive dysfunction following COVID-19 infection. J Neurovirol. 2022;28(3):430–437. doi:10.1007/s13365-022-01079-y
14. Miskowiak KW, Bech JL, Henriksen AC, Johnsen S, Podlekareva D, Marner L. Cerebral metabolic rate of glucose and cognitive tests in long COVID patients. Brain Sci. 2023;13(1). doi:10.3390/brainsci13010023
15. Herrera E, Pérez-Sánchez M, San Miguel-Abella R, et al. Cognitive impairment in young adults with post COVID-19 syndrome. Sci Rep. 2023;13(1):6378. doi:10.1038/s41598-023-32939-0
16. Maamar M, Artime A, Pariente E, et al. Post-COVID-19 syndrome, low-grade inflammation and inflammatory markers: a cross-sectional study. Curr Med Res Opin. 2022;38(6):901–909. doi:10.1080/03007995.2022.2042991
17. Saylik F, Sarıkaya R. Can systemic immune-inflammation index detect the presence of exaggerated morning blood pressure surge in newly diagnosed treatment-naive hypertensive patients? Clin Exp Hypertens. 2021;43(8):772–779. doi:10.1080/10641963.2021.1960366
18. Ye Z, Hu T, Wang J, et al. Systemic immune-inflammation index as a potential biomarker of cardiovascular diseases: a systematic review and meta-analysis. Systematic Review. Front Cardiovasc Med. 2022;9. doi:10.3389/fcvm.2022.933913
19. Nalbandian A, Desai AD, Wan EY. Post-COVID-19 Condition. Annu Rev Med. 2023;74(1):55–64. doi:10.1146/annurev-med-043021-030635
20. Tombaugh TN, McDowell I, Kristjansson B, Hubley AM. Mini-Mental State Examination (MMSE) and the Modified MMSE (3MS): a psychometric comparison and normative data. Psychol Assess. 1996;8:48–59. doi:10.1037/1040-3590.8.1.48
21. Nasreddine ZS, Phillips NA, Bédirian V, et al. The Montreal cognitive assessment, MoCA: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
22. Aguilar-Navarro SG, Mimenza-Alvarado AJ, Palacios-García AA, Samudio-Cruz A, Gutiérrez-Gutiérrez LA, Ávila-Funes JA. Validez y confiabilidad del MoCA (Montreal Cognitive Assessment) para el tamizaje del deterioro cognoscitivo en méxico. Revista Colombiana de Psiquiatría. 2018;47(4):237–243. doi:10.1016/j.rcp.2017.05.003
23. Beaman S, Beaman PE, Garcia-Peña C, et al. Validation of a modified version of the mini-mental state examination (MMSE) in Spanish. Aging Neuropsychol Cogn. 2004;11(1):1–11. doi:10.1076/anec.11.1.1.29366
24. Avila-Avila A, Sosa-Tinoco E, Pacheco-Pacheco J, et al. [Guidelines for Comprehensive Geriatric Assessment Instruments].Guía de instrumentos de evaluación geriátrica integral. [National Institute of Geriatrics] Instituto Nacional de Geriatría; 2020. Spanish. Available from: http://www.geriatria.salud.gob.mx/descargas/publicaciones/Guia_InstrumentosGeriatrica_18-02-2020.pdf.
25. Liu Y, Du X, Chen J, et al. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J Infect. 2020;81(1):e6–e12. doi:10.1016/j.jinf.2020.04.002
26. Regolo M, Vaccaro M, Sorce A, et al. Neutrophil-to-Lymphocyte Ratio (NLR) is a promising predictor of mortality and admission to intensive care unit of COVID-19 patients. J Clin Med. 2022;11(8):2235. doi:10.3390/jcm11082235
27. Ghobadi H, Mohammadshahi J, Javaheri N, Fouladi N, Mirzazadeh Y, Aslani MR. Role of leukocytes and systemic inflammation indexes (NLR, PLR, MLP, dNLR, NLPR, AISI, SIR-I, and SII) on admission predicts in-hospital mortality in non-elderly and elderly COVID-19 patients. Original Research. Front Med. 2022;9. doi:10.3389/fmed.2022.916453
28. Koestler DC, Usset J, Christensen BC, et al. DNA methylation-derived neutrophil-to-lymphocyte ratio: an epigenetic tool to explore cancer inflammation and outcomes. Cancer Epidemiol Biomarkers Prev. 2017;26(3):328–338. doi:10.1158/1055-9965.Epi-16-0461
29. Xu W, Zhang F, Shi Y, Chen Y, Shi B, Yu G. Causal association of epigenetic aging and COVID-19 severity and susceptibility: a bidirectional Mendelian randomization study. Review. Front Med. 2022;9. doi:10.3389/fmed.2022.989950
30. Citu C, Gorun F, Motoc A, et al. The Predictive Role of NLR, d-NLR, MLR, and SIRI in COVID-19 Mortality. Diagnostics. 2022;12(1):122. doi:10.3390/diagnostics12010122
31. Chlamydas S, Papavassiliou AG, Piperi C. Epigenetic mechanisms regulating COVID-19 infection. Epigenetics. 2021;16(3):263–270. doi:10.1080/15592294.2020.1796896
32. Franzen J, Nüchtern S, Tharmapalan V, et al. Epigenetic clocks are not accelerated in COVID-19 patients. Int J Mol Sci. 2021;22(17):9306. doi:10.3390/ijms22179306
33. Xu M, Chen R, Liu L, et al. Systemic immune-inflammation index and incident cardiovascular diseases among middle-aged and elderly Chinese adults: the Dongfeng-Tongji cohort study. Atherosclerosis. 2021;323:20–29. doi:10.1016/j.atherosclerosis.2021.02.012
34. Pilotto A, Cristillo V, Cotti Piccinelli S, et al. Long-term neurological manifestations of COVID-19: prevalence and predictive factors. Neurol Sci. 2021;42(12):4903–4907. doi:10.1007/s10072-021-05586-4
35. de Erausquin GA, Snyder H, Brugha TS, et al. Chronic neuropsychiatric sequelae of SARS-CoV-2: protocol and methods from the Alzheimer’s association global consortium. Alzheimers Dement. 2022;8(1):e12348. doi:10.1002/trc2.12348
36. Bolattürk ÖF, Soylu AC. Evaluation of cognitive, mental, and sleep patterns of post-acute COVID-19 patients and their correlation with thorax CT. Acta Neurol Belg. 2022;123:1089–1093. doi:10.1007/s13760-022-02001-3
37. Hugon J, Msika E-F, Queneau M, Farid K, Paquet C. Long COVID: cognitive complaints (brain fog) and dysfunction of the cingulate cortex. J Neurol. 2022;269(1):44–46. doi:10.1007/s00415-021-10655-x
38. Crunfli F, Carregari VC, Veras FP, et al. Morphological, cellular, and molecular basis of brain infection in COVID-19 patients. Proc Natl Acad Sci USA. 2022;119(35):e2200960119. doi:10.1073/pnas.2200960119
39. Cecchetti G, Agosta F, Canu E, et al. Cognitive, EEG, and MRI features of COVID-19 survivors: a 10-month study. J Neurol. 2022;269(7):3400–3412. doi:10.1007/s00415-022-11047-5
40. Logue JK, Franko NM, McCulloch DJ, et al. Sequelae in adults at 6 months after COVID-19 infection. JAMA Network Open. 2021;4(2):e210830–e210830. doi:10.1001/jamanetworkopen.2021.0830
41. Mazza MG, Palladini M, De Lorenzo R, et al. Persistent psychopathology and neurocognitive impairment in COVID-19 survivors: effect of inflammatory biomarkers at three-month follow-up. Brain Behav Immun. 2021;94:138–147. doi:10.1016/j.bbi.2021.02.021
42. Ganna B, Nils S, Tobias B, et al. Slow but evident recovery from neocortical dysfunction and cognitive impairment in a series of chronic COVID-19 patients. J Nucl Med. 2021;62(7):910. doi:10.2967/jnumed.121.262128
43. Manganotti P, Michelutti M, Furlanis G, Deodato M, Buoite Stella A. Deficient GABABergic and glutamatergic excitability in the motor cortex of patients with long-COVID and cognitive impairment. Clin Neurophysiol. 2023;151:83–91. doi:10.1016/j.clinph.2023.04.010
44. Tondo G, Aprile D, De Marchi F, et al. Investigating the prognostic role of peripheral inflammatory markers in mild cognitive impairment. J Clin Med. 2023;12(13):4298. doi:10.3390/jcm12134298
45. Liu X, Bai X, Ren R, et al. Association between depression or anxiety symptoms and immune-inflammatory characteristics in in-patients with tuberculosis: a cross-sectional study. Orig Res Front Psychiatry. 2022;13:1.
46. Shang W, Dong J, Ren Y, et al. The value of clinical parameters in predicting the severity of COVID-19. J Med Virol. 2020;92(10):2188–2192. doi:10.1002/jmv.26031
47. Toori KU, Qureshi MA, Chaudhry A, Safdar MF. Neutrophil to lymphocyte ratio (NLR) in COVID-19: a cheap prognostic marker in a resource constraint setting. Pak J Med Sci. 2021;37(5):1435–1439. doi:10.12669/pjms.37.5.4194
48. Battaglini D, Lopes-Pacheco M, Castro-Faria-Neto HC, Pelosi P, Rocco PRM. Laboratory biomarkers for diagnosis and prognosis in COVID-19. Review. Front Immunol. 2022;13. doi:10.3389/fimmu.2022.857573
49. Alagbe AE, Pedroso GA, de Oliveira BB, et al. Hemograms and serial hemogram-derived ratios in survivors and non-survivors of COVID-19 in Campinas, Brazil. Hematol Transfus Cell Ther. 2022. doi:10.1016/j.htct.2022.11.003
50. Petelina TI, Musikhina NA, Garanina VD, et al. [Characterization of blood biomarkers in prospective follow-up of patients with cardiovascular pathology in combination with type 2 diabetes mellitus after COVID-19 associated pneumonia]. Характеристика биомаркеров крови при проспективном наблюдении пациентов с сердечно-сосудистой патологией в сочетании с сахарным диабетом типа 2, перенесших covid-19 ассоциированную пневмонию. Klin Lab Diagn. 2022;67(10):561–569. Russian. doi:10.51620/0869-2084-2022-67-10-561-569
51. Karaaslan T, Karaaslan E. Predictive value of systemic immune-inflammation index in determining mortality in COVID-19 patients. J Crit Care Med. 2022;8(3):156–164. doi:10.2478/jccm-2022-0013
52. Devita M, Di Rosa E, Iannizzi P, et al. Cognitive and psychological sequelae of COVID-19: age differences in facing the pandemic. Brief research report. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.711461
53. Çırakoğlu ÖF, Yılmaz AS. Systemic immune-inflammation index is associated with increased carotid intima-media thickness in hypertensive patients. Clin Exp Hypertens. 2021;43(6):565–571. doi:10.1080/10641963.2021.1916944
54. Zhang X, Li JH, Zhang Q, et al. Relationship between prognostic nutritional index and mortality in overweight or obese patients with cancer: a multicenter observational study. J Inflamm Res. 2021;14:3921–3932. doi:10.2147/jir.S321724
55. Çakıroğlu Y, Vural F, Vural B. The inflammatory markers in polycystic ovary syndrome: association with obesity and IVF outcomes. J Endocrinol Invest. 2016;39(8):899–907. doi:10.1007/s40618-016-0446-4
56. Y-z N, Z-q Y, Yin H, Shan L-H, Wang J-H, Wu Q-H. Osteosarcopenic obesity and its components—osteoporosis, sarcopenia, and obesity—are associated with blood cell count-derived inflammation indices in older Chinese people. BMC Geriatr. 2022;22(1):532. doi:10.1186/s12877-022-03225-x
57. Nicoară D-M, Munteanu A-I, Scutca A-C, et al. Assessing the relationship between systemic immune-inflammation index and metabolic syndrome in children with obesity. Int J Mol Sci. 2023;24(9):8414. doi:10.3390/ijms24098414
58. Osadnik T, Bujak K, Osadnik K, et al. Novel inflammatory biomarkers may reflect subclinical inflammation in young healthy adults with obesity. Endokrynol Pol. 2019;70(2):135–142. doi:10.5603/EP.a2019.0002
59. Erdal E, Inanir M. Platelet-to-lymphocyte ratio (PLR) and Plateletcrit (PCT) in young patients with morbid obesity. Revista da Associacao Medica Brasileira. 2019;2019:65.
60. J-Y Y, Choi W-J, Lee H-S, Lee J-W. Relationship between inflammatory markers and visceral obesity in obese and overweight Korean adults: an observational study. Medicine. 2019;98:9.
61. Oronsky B, Larson C, Hammond TC, et al. A review of persistent post-COVID syndrome (PPCS). Clin Rev Allergy Immunol. 2023;64(1):66–74. doi:10.1007/s12016-021-08848-3
62. Rhie SJ, Jung E-Y, Shim I. The role of neuroinflammation on pathogenesis of affective disorders. J Exerc Rehabil. 2020;16(1):2–9. doi:10.12965/jer.2040016.008
63. Ajčević M, Iscra K, Furlanis G, et al. Cerebral hypoperfusion in post-COVID-19 cognitively impaired subjects revealed by arterial spin labeling MRI. Sci Rep. 2023;13(1):5808. doi:10.1038/s41598-023-32275-3
64. Bhikram T, Sandor P. Neutrophil-lymphocyte ratios as inflammatory biomarkers in psychiatric patients. Brain Behav Immun. 2022;105:237–246. doi:10.1016/j.bbi.2022.07.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.