Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Afebrile Presentation in COPD Patients with Influenza A: A Risk Factor for Prolonged Viral Shedding
Authors Fan Y, Fan J, Ma L ![]() , Wu C, Wang L, Chen H, Chen Y
, Wu C, Wang L, Chen H, Chen Y
Received 31 August 2025
Accepted for publication 3 March 2026
Published 11 March 2026 Volume 2026:21 559844
DOI https://doi.org/10.2147/COPD.S559844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jill Ohar
Yuchen Fan, Junlin Fan, Li Ma, Chunxia Wu, Lu Wang, Hong Chen, Yajuan Chen
Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chongqing Medical University, Chongqing, 400016, People’s Republic of China
Correspondence: Yajuan Chen, Department of Respiratory and Critical Care Medicine, The First Affiliated Hospital of Chongqing Medical University, No. 1 Youyi Road, Yuzhong District, Chongqing, 400016, People’s Republic of China, Email [email protected]
Purpose: To investigate the risk factors for prolonged viral shedding in influenza A patients treated with oseltamivir and analyze fever patterns in chronic obstructive pulmonary disease (COPD) patients.
Patients and Methods: This retrospective study analyzed 309 hospitalized patients with RT-PCR-confirmed influenza A at a multi-campus tertiary medical center from 2022 to 2025. Influenza A virus retesting was performed on day 6 of antiviral treatment to assess viral clearance. Multivariate logistic regression was used to identify risk factors for prolonged viral shedding. ROC curve analysis evaluated the predictive value of absolute lymphocyte count (ALC). Subgroup analyses compared fever patterns in COPD and non-COPD patients using the Mann–Whitney U and chi-square (χ2) tests.
Results: Overall, 309 influenza A inpatients were included. Six independent risk factors for prolonged viral shedding were identified: older age (95% CI 1.01– 1.05), lymphopenia (95% CI 0.09– 0.38), cerebrovascular disorders (95% CI 1.64– 16.08), immunosuppressants (95% CI 1.05– 3.36), delayed antiviral treatment (95% CI 4.13– 15.27), and fungal coinfection (95% CI 1.25– 4.69). Notably, 63.7% of the COPD patients were afebrile, compared to 23.6% of non-COPD patients (p < 0.05). In the COPD group, prolonged shedders had higher odds of afebrile status (95% CI 1.39– 12.59), lower ALC (95% CI 0.01– 0.17) and delayed oseltamivir initiation (95% CI 1.65– 13.28) than nonprolonged shedders. The ALC demonstrated good predictive accuracy for prolonged viral shedding (AUC 0.75 overall; AUC 0.77 for the COPD group).
Conclusion: Early antiviral therapy and targeted management for high-risk groups (especially COPD patients) are valuable. Afebrile presentations in COPD patients highlight the importance of routine influenza testing during exacerbations.
Keywords: prolonged viral shedding, oseltamivir, afebrile, absolute lymphocyte count
Introduction
Influenza is a highly contagious respiratory viral disease that poses a significant risk to global health and a considerable disease burden on human health and economic development. The World Health Organization estimates that three to five million individuals develop severe influenza each year globally and that 290,000 to 650,000 adults die from influenza-related causes.1
Importantly, China faces unique epidemiological challenges: southern China reported an unusually high number of influenza cases in the summer of 2022,2 and the 2023–2024 influenza season was characterized by delayed onset and high epidemic intensity.3 These region-specific trends, combined with China’s large elderly population and high prevalence of chronic comorbidities (eg, chronic obstructive pulmonary disease [COPD]), highlight the need for targeted research in Chinese clinical settings. While oseltamivir is widely used for hospitalized adults with severe influenza in China, data on viral shedding dynamics and clinical outcomes in this specific population remain scarce-particularly compared to studies from Western countries.4 This gap is critical, as genetic variations in influenza strains, differences in healthcare access, and population-specific comorbidity profiles may lead to distinct disease trajectories and treatment responses.
Influenza A virus, with its unique antigenic drift and shift properties, retains substantial pandemic potential.5 While most influenza cases are mild and self-limiting, severe and life-threatening outcomes are disproportionately common among the elderly and individuals with chronic conditions6,7-groups that are highly represented in Chinese hospitals. Importantly, our clinical observations reveal a key phenotypic difference in COPD patients coinfected with influenza A: a subset of these patients lack fever, a hallmark symptom traditionally relied upon for influenza diagnosis.8 This atypical presentation is particularly relevant in China, where COPD has a high prevalence,9 and influenza-related AECOPD (acute exacerbation of COPD) constitutes a major cause of hospitalization and mortality. Given the paucity of data on afebrile influenza in Chinese COPD patients and its potential to delay diagnosis and treatment, investigating this population fills a critical gap in both local and global literature.
Notably, the Expert Consensus on the Acute Exacerbation of Chronic Obstructive Pulmonary Disease in China10 stipulates that empirical antiviral therapy targeting influenza viruses is not recommended for patients with acute exacerbation of COPD (AECOPD). Antiviral intervention may be considered exclusively for high-risk AECOPD patients who present with classic influenza symptoms (eg, fever, myalgia, malaise, and respiratory tract infection), have symptom duration of fewer than 48 hours, and are evaluated during a documented influenza outbreak. This clinical guideline is predicated on the presence of typical influenza manifestations, yet it fails to account for the atypical, afebrile presentation of influenza coinfection in a subset of COPD patients – a oversight that may contribute to delayed antiviral treatment initiation and suboptimal clinical outcomes.
This study aimed to investigate the factors associated with prolonged viral shedding among inpatients with influenza A who were treated with oseltamivir and analyze fever patterns in the COPD group.
Materials and Methods
Study Design
This study included a total of 468 RT‒PCR-confirmed influenza A cases collected between 2022 and 2025. All cases were sourced from the three campuses of the First Affiliated Hospital of Chongqing Medical University, located in Jiulongpo District (Yuanjiagang Campus), Yuzhong District (Jingwei Campus), and Yubei District (Jinshan Campus). This medical institution is a 4616-bed primary and tertiary university-affiliated hospital in Chongqing, China. The study was approved by the Institutional Research Ethics Committee of the First Affiliated Hospital of Chongqing Medical University (No. 2025–283-01). This retrospective study employed anonymized medical records and data obtained from routine clinical care. The Institutional Ethics Committee waived the requirement for written informed consent, citing the retrospective design of the study. All procedures performed in this study were in compliance with the Declaration of Helsinki.
Participants
Inclusion Criteria
Adults over 18 years of age who presented with severe respiratory symptoms requiring hospitalization and who tested positive for influenza virus via a PCR assay initiated oseltamivir treatment.
Exclusion Criteria
- Patients who passed away during hospitalization or whose duration of hospitalization was less than 6 days
- Individuals receiving additional antiviral medications specific to influenza A (eg, zanamivir, peramivir, or baloxavir marboxil) alongside oseltamivir during the inpatient period
- Patients with incomplete virological monitoring due to failure to undergo protocol-specific influenza A nucleic acid testing within 6 days following the initiation of antiviral treatment
- Patients with coinfection with influenza A virus and other respiratory viruses (eg, influenza B virus, SARS-CoV-2, respiratory syncytial virus, or other coronaviruses).
- Patients with hematological diseases or those who have undergone recent chemotherapy that influence lymphocyte counts.
Study Definitions
We collected baseline data from patients upon admission, including ALC, respiratory symptoms, comorbidities, and the initiation time of antiviral treatment. The initial PCR test is conducted based on clinical suspicion of Influenza A, either upon admission or during the hospital stay. The World Health Organization (WHO) recommended a standard five-day treatment course of oseltamivir for influenza; Therefore, we will perform a PCR retest on Day 6, which corresponds to the day following the completion of a five-day course of oseltamivir treatment. Delayed antiviral therapy was considered when the duration of illness onset exceeded 48 hours. We defined prolonged shedders as patients who still required hospitalization and had a positive PCR assay on day 6 of treatment. Immunosuppression was defined as a condition in which an individual had been treated with systemic glucocorticoids, cyclophosphamide, methotrexate, or other immunosuppressive agents. The primary outcome was factors associated with prolonged influenza A virus shedding. We also investigated fever status and its associated influencing factors in patients with chronic obstructive pulmonary disease (COPD) following infection, with influenza A as the secondary outcome.
Sample Processing and Influenza A (H1N1) Virus Detection
The PCR assay was performed on day 6. If a repeat PCR assay was negative or if the patient was discharged, no further tests were performed. Triple swabs were drawn from the patients’ throat and both nostrils and put into sterile viral transport media. The tube was immediately sent to the laboratory or refrigerated at 4°C until it was transported to the laboratory. Influenza A (H1N1) virus was detected by real-time RT‒PCR, following the WHO protocol, in a Stratagene MX3000 thermocycler.
Statistical Analysis
Continuous variables are expressed as medians and interquartile ranges (M [Q1, Q3]) for nonnormally distributed data, with group comparisons conducted via the Mann‒Whitney U-test. Categorical variables are presented as frequencies (n) and percentages (%) and were analyzed by Pearson’s chi-square test, continuity-corrected chi-square test, or Fisher’s exact test as appropriate, whereas the Cochran‒Armitage trend test was used for ordered categorical variables. Univariate and multivariate logistic regression analyses were performed to identify influencing factors, with the results reported as odds ratios (ORs) and 95% confidence intervals (95% CIs), and model fit was assessed via the Hosmer‒Lemeshow test. The predictive value of the absolute lymphocyte count (ALC) for the rate of prolonged viral shedding in influenza A patients was evaluated through receiver operating characteristic (ROC) curve analysis, and the area under the curve (AUC) with 95% CI, optimal cutoff value (determined by the Youden index), sensitivity, specificity, and predictive values were calculated. All tests were two-tailed, with p < 0.05 considered statistically significant, and Bonferroni correction was applied for multiple comparisons when appropriate. Data quality was verified through normality (Shapiro‒Wilk test) and homogeneity of variance (Levene’s test) assessments prior to analysis. Statistical analyses were performed via SPSS version 26.0.
Results
Patient Characteristics and Clinical Features in the Prolonged Shedder Group and Nonprolonged Shedder Group
Between June 2022 and February 2025, we screened 468 patients diagnosed with influenza A. A total of 159 patients were excluded. The reasons for exclusion were: 42 patients did not receive oseltamivir monotherapy per protocol (including those who either did not receive oseltamivir at all or received oseltamivir in combination with other influenza antiviral agents). Eighty-four patients failed to complete the nucleic acid test within the prescribed time. Thirty-three patients were diagnosed with influenza A virus coinfection involving other respiratory viruses.
A total of 309 participants were enrolled in the study; the median age was 69 years, and 223 (72.2%) were males. Among these, 171 (55%) were prolonged shedders, and the others were nonprolonged shedders (45%) (Table 1). Subjects in the prolonged shedder group were compared with those in the non-prolonged shedder group (Table 1). Univariate analysis revealed factors associated with age, ALC, delayed antiviral therapy, rates of cobacterial and co-fungal infections, mechanical ventilation, sex, smoking history, fever symptoms, chronic comorbidities (COPD, cardiovascular disease, neurologic disorder, diabetes), and immunosuppression. After adjusting for potential confounders, prolonged viral shedding was significantly associated with several risk factors. Positive associations (OR > 1) were observed for older age (OR 1.027, 95% CI 1.007–1.047; p = 0.007), the presence of neurological disorders (OR 5.141, 95% CI 1.640–16.115; p = 0.005), immunosuppression (OR 1.875, 95% CI 1.047–3.360; p = 0.035), delayed initiation of antiviral therapy (OR 7.932, 95% CI 4.123–15.260; p < 0.001), and co-fungal infection (OR 2.425, 95% CI 1.252–4.697; p = 0.009). In contrast, a higher ALC demonstrated a strong negative association (OR 0.187, 95% CI 0.093–0.377; p < 0.001), suggesting its protective effect against prolonged viral shedding.
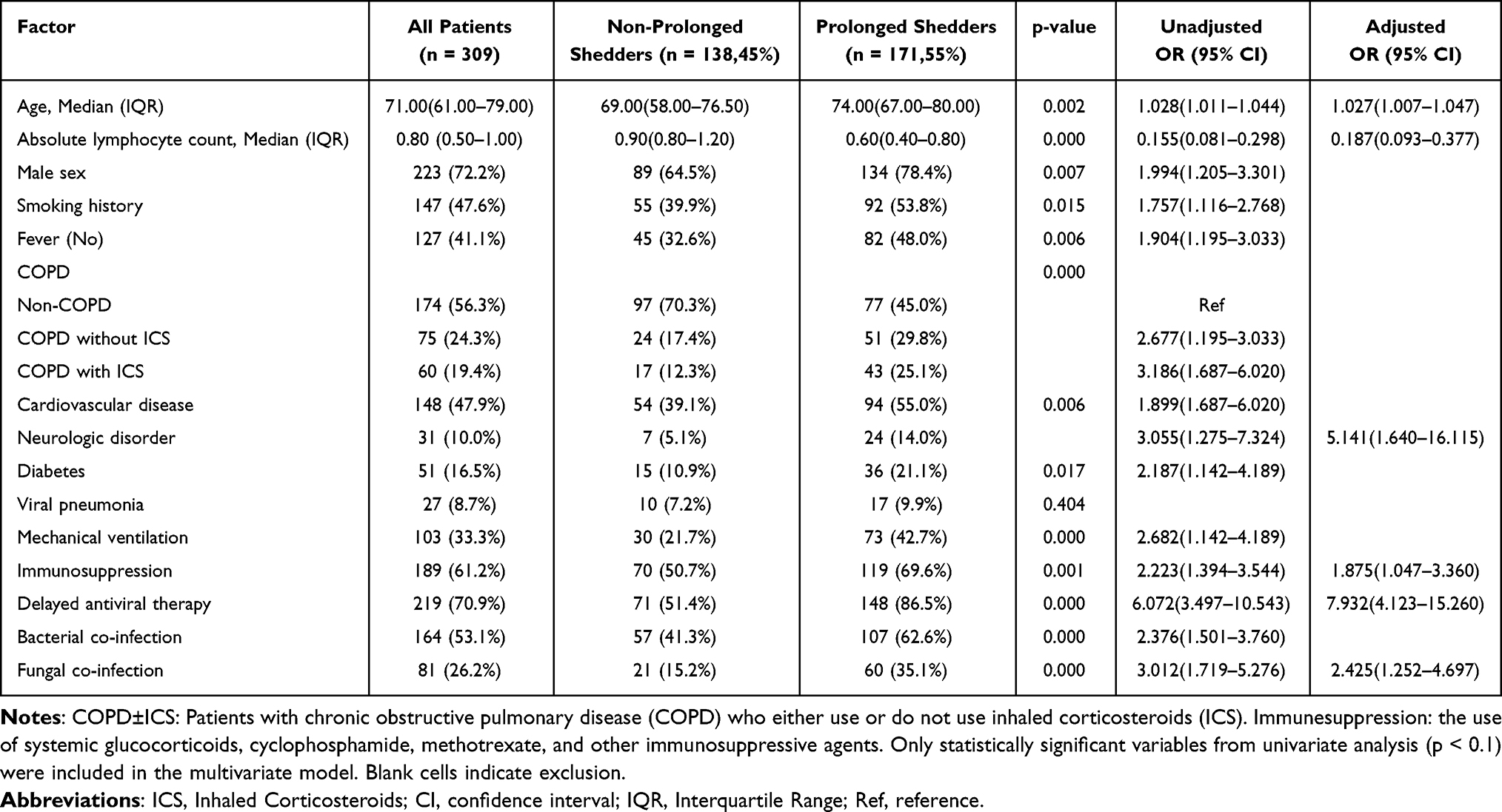 |
Table 1 Factors Associated with Prolonged Shedding of the Influenza A Virus in All Patients |
Fever Status and Its Associated Influencing Factors in Patients with COPD Following Infection with Influenza A
In the COPD group (n = 135), 63.7% of patients (n = 86) remained afebrile, whereas in the non-COPD group (n = 174), only 23.6% of patients (n = 41) presented no fever (OR = 0.12 95% CI [0.06–0.23], p < 0.001). Consistent trends were observed in both the subgroup analysis excluding ICS users (OR = 0.18, 95% CI [0.09–0.36], p < 0.001) and in the propensity score-matched (PSM) cohort (OR = 0.20, 95% CI [0.08–0.53], p = 0.001). These findings demonstrate that the proportion of afebrile patients in the COPD group was significantly greater than that in the non-COPD group (Table S1).
We further investigated the potential factors associated with the absence of fever in patients with COPD who were infected with influenza A (Table 2). Compared with the fever group, the nonfever group was significantly younger (73.5 vs 78.0 years, p = 0.001) and had a higher ALC (0.75 vs 0.60, p = 0.019) and proportion of inhaled corticosteroid (ICS) use (51.2% vs 32.7%, p = 0.037).
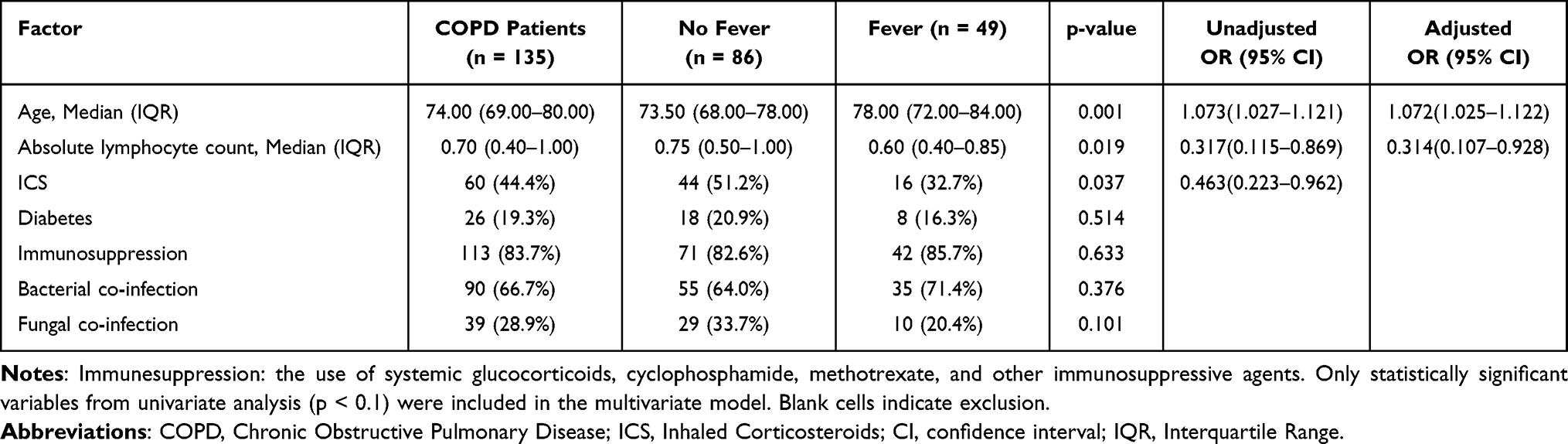 |
Table 2 Factors Contributing to Fever in Patients with COPD |
With fever as the dependent variable, factors that exhibited significant differences in the univariate analysis, namely, age, ALC, and the use of ICS, were included in the multivariate logistic regression analysis. The results indicated that age (OR 1.072; 95% CI 1.025–1.122; p = 0.002) and ALC (OR 0.314; 95% CI 0.107–0.928; p = 0.036) were significant influencing factors for fever (Table 2). The above results suggested that in the COPD population, older age and lower lymphocyte counts were associated with an increased rate of fever.
Analysis of Factors Affecting the Duration of Viral Shedding in COPD Patients
A greater proportion of patients in the nonfever group than in the fever group exhibited prolonged viral shedding (63.7% vs 36.3%, p = 0.000). Consequently, the COPD cohort was further stratified into nonprolonged shedder and prolonged shedder subgroups.
Chi-square tests and Fisher’s exact probability tests revealed significant differences between the prolonged shedder subgroup and the nonprolonged shedder subgroup in terms of fever (p = 0.006), ALC (p = 0.000) and delayed antiviral therapy (p = 0.000). In contrast, no significant differences were noted in the use of ICSs or immunosuppressants (p > 0.05) (Table 3).
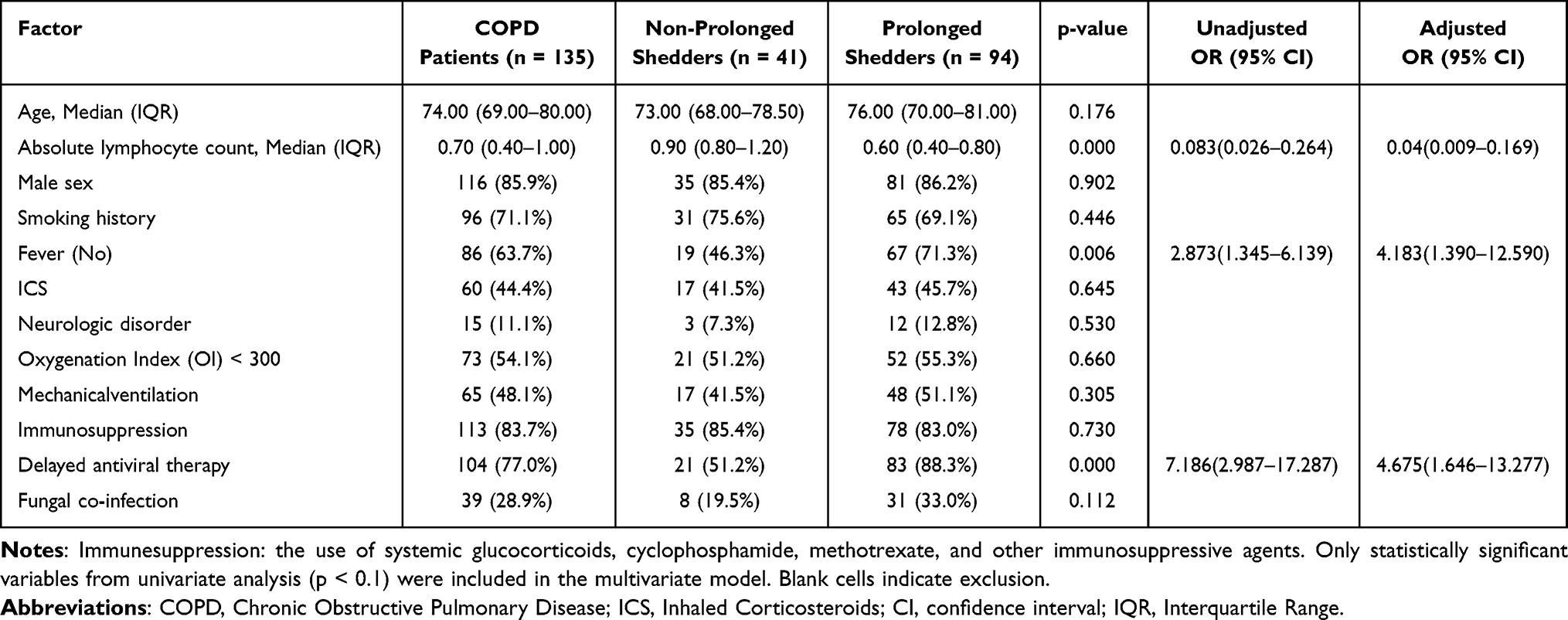 |
Table 3 Factors Associated with Prolonged Shedding of the Influenza A Virus in COPD Group |
Logistic regression analysis corroborated the aforementioned findings. In the COPD group, prolonged shedders presented significantly greater odds of afebrile status (OR 4.183; 95% CI 1.390–12.590; p = 0.011), lower ALC (OR 0.040; 95% CI 0.009–0.169; p = 0.000), and delayed initiation of oseltamivir therapy (OR 4.675; 95% CI 1.646–13.277; p = 0.004) than nonprolonged shedders did (Table 3).
Optimal Cutoff Values for the ALC and ROC Curve Analysis
ROC curve analyses were performed to assess the predictive performance of ALC for prolonged viral shedding in influenza A patients, with the corresponding results summarized in Figure 1 and Table S2. Among all participants included in the study, the AUC for ALC was 0.751 (95% CI: 0.697–0.805), with an optimal cutoff value of 0.725 × 109/L, achieving a sensitivity of 69.0% and a specificity of 76.8%. Subgroup analysis for COPD patients revealed that the AUC for ALC was 0.771 (95% CI: 0.688–0.854), with an optimal cutoff value of 0.750 × 109/L, achieving a sensitivity of 71.3% and a specificity of 78.0%. In both the overall sample and the COPD subgroup, the ALC demonstrated predictive value for prolonged viral shedding.
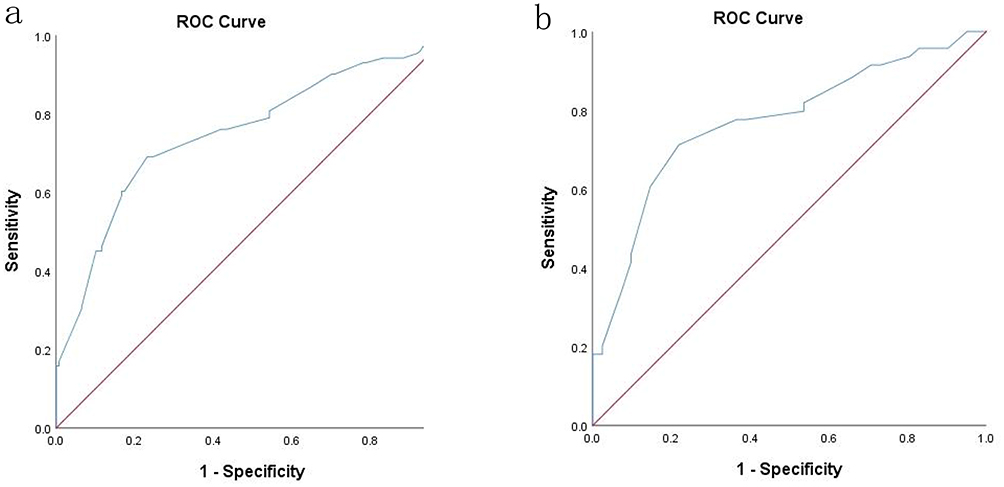 |
Figure 1 Receiver operating characteristic (ROC) analysis of ALC in predicting the prolonged viral A shedding. (a) For the overall participants. Area under ROC curve = 0.751. (b) For the COPD group. Area under ROC curve = 0.771. |
Discussion
In this retrospective cohort study, we performed serial PCR assays of respiratory samples obtained from inpatients with influenza A who were treated with oseltamivir at 5-day intervals. Old age, low ALC, cerebrovascular disorders, the use of immunosuppressants, delayed initiation of antiviral treatment, and co-fungal infections are independently associated with prolonged duration of viral shedding (>5 days).
Advanced age was identified as an independent risk factor for prolonged viral shedding in our cohort. This observation was consistent with the broader concept of immunosenescence, which in the literature is characterized by a progressive decline in immune function, including diminished T cell-mediated responses.11,12 While our study did not directly assess immune cell function, the association we report aligns with established models of age-related immune dysregulation. These models proposed that such dysregulation may contribute to impaired viral clearance in older adults.13,14
Immunosuppressants, primarily systemic corticosteroids, were associated with prolonged viral shedding in our cohort. Mechanistically, it has been proposed that such agents may delay viral clearance by suppressing inflammatory responses and T-cell function.15,16 However, it remained challenging to distinguish whether the observed delay is directly attributable to the pharmacological effects of the drugs or is instead driven by the severity of the underlying diseases that necessitate such treatment. Therefore, our finding should be interpreted as identifying a high-risk patient phenotype-those requiring systemic immunosuppression-rather than establishing a direct causal role of these agents. This ambiguity mirrored the ongoing debate regarding corticosteroid use in influenza treatment.17–19 While some evidence suggested that low-to-moderate doses may reduce mortality in severe influenza pneumonia, no benefit has been shown in mild cases, and their role remains controversial.20 Notably, inhaled corticosteroids (ICS) were not independently associated with delayed viral clearance in our analysis. Interestingly, prior studies such as that by Luque-Paz et al have reported that ICS use may be linked to higher detection rates of non-influenza respiratory viruses, suggesting a distinct profile of respiratory infection risk.21
Lymphopenia (low ALC) signified more than just low cell counts, it reflected a pervasive immune dysregulation. Central to this was impaired CD4+ T cell function, which undermined the essential help for B cell antibody production, thereby bridging cellular and humoral immune defects.22,23 This nexus helped explain the vulnerability to conditions like hypogammaglobulinemia, which weakened antibody-mediated viral clearance and may foster a vicious cycle of persistent infection and immune exhaustion.24,25 Consequently, the synergy between compromised cellular and humoral immunity appeared fundamental in driving prolonged viral shedding in immunocompromised hosts. This study further demonstrated that the ALC served not only as an independent risk factor but also as a fair predictor of the risk of prolonged viral shedding. When the ALC was markedly reduced (COPD group: <0.75×109/L; overall subjects: <0.725×109/L), such patients should strictly follow the specified nucleic acid retesting schedule. This quantitative threshold for ALC provided a actionable reference for clinical management, enabling targeted monitoring of high-risk patients.
Multivariate regression analysis revealed that, among hospitalized influenza patients overall, fungal co-infection was an independent risk factor associated with prolonged viral shedding. However, this association did not achieve statistical significance in the subgroup of patients with chronic obstructive pulmonary disease (COPD). In the general patient population, the independent association between fungal infection and extended viral shedding suggested potential underlying pathophysiological interactions. A biologically plausible hypothesis was that pulmonary fungal infections-such as invasive pulmonary aspergillosis-may delay viral clearance through active modulation of the host immune response, either directly or indirectly. Specifically, pathogenic fungi such as Aspergillus fumigatus may induce immunosuppression via two key mechanisms. First, direct toxin-mediated suppression: fungal metabolites, including gliotoxin, can impair the function and viability of phagocytic cells (eg, neutrophils and macrophages) and suppress lymphocyte activity, thereby compromising critical effector mechanisms required for viral clearance.26 Second, systemic immune reprogramming: fungal infection can stimulate the bone marrow to generate myeloid-derived suppressor cells (MDSCs), which secrete inhibitory cytokines that suppress T-cell and natural killer (NK) cell proliferation and function, ultimately attenuating adaptive antiviral immunity.27 These mechanisms suggested that fungal infection was not merely a consequence of immune compromise but may also act as an active driver influencing disease progression and viral kinetics through immune modulation. In COPD patients, however, the relationship between fungal infection and prolonged viral shedding may be obscured by pre-existing conditions, including chronic immune-inflammatory dysregulation, structural lung abnormalities, and a higher baseline prevalence of fungal colonization.28,29
Up to 28% of patients with COPD may experience exacerbations attributable to influenza virus infection, and COPD patients are prone to progressing to severe clinical outcomes upon influenza infection.30 Fever is one of the most common and characteristic clinical manifestations of influenza A.8 However, we have observed that some patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD) who presented with aggravated cough and dyspnea but lack fever symptoms may have underlying influenza infections that were easily overlooked by clinicians. The data revealed that the proportion of afebrile patients in the COPD group was 63.7%, which was significantly greater than that in the non-COPD group (23.6%). Ann et al demonstrated that elderly patients may exhibit a diminished thermoregulatory capacity, and a lower proportion of older patients reported fever symptoms. Nevertheless, no significant difference was observed in the mean peak temperature recorded between the older and younger groups.31 It is noteworthy that this study has identified two apparently contradictory associations: in patients with COPD, advanced age and low ALC were associated with an increased likelihood of fever (Table 2), whereas afebrile presentation was independently linked to prolonged viral shedding (Table 3). This “fever paradox” suggested a complex and potentially distinct relationship between fever, immune response, and viral clearance in the context of COPD. We proposed that these associations did not represent opposing ends of a single linear pathway but instead reflected two distinct yet interrelated immunopathological states. In individuals with advanced age and lymphopenia-features commonly associated with immunosenescence-fever may not signify effective antiviral immunity but rather indicated dysregulated immune responses and excessive inflammation, such as that seen in cytokine storm-like phenomena.32,33 Conversely, the absence of fever may reflect impaired or blunted immune activation, resulting in inadequate early viral control and delayed clearance.31,34 Therefore, both presentations-afebrile infection and febrile infection accompanied by severe lymphopenia should be recognized as high-risk clinical phenotypes indicative of compromised viral clearance capacity in COPD patients. This study indicated that the absence of fever, a low absolute lymphocyte count, and delayed antiviral treatment may all be important factors contributing to an increased risk of prolonged duration of viral shedding in patients with COPD. Several studies showed that prolonged viral shedding was associated with longer hospital stay and poorer outcome.32,35 Although To KKW et al noted that prolonged viral shedding during the influenza season was not significantly associated with an extended duration of respiratory symptoms, influenza viruses can be frequently detected in hospitalized patients who do not exhibit typical signs of respiratory tract infections. These patients may serve as a significant source of nosocomial viral transmission.36
The clinical characteristics observed in the patients of this study – including advanced age, multiple comorbidities, and immune dysregulation-reflect a broader population of high-risk individuals in hospital settings. Therefore, during influenza season, for hospitalized patients with similar risk profiles, particularly those with chronic obstructive pulmonary disease (COPD), our study findings supported several key management strategies: (1) influenza testing should be routinely performed even in the absence of typical febrile manifestations; (2) early initiation of empirical antiviral therapy was essential to reduce prolonged viral shedding; and (3) strict infection control measures, including timely isolation, must be implemented to prevent nosocomial transmission.
Beyond antiviral therapy, adjunctive treatments such as intravenous immunoglobulin have been explored in severe or immunocompromised influenza cases, particularly when immune impairment is suspected.37,38 However, their role remained supplementary and was not yet established for routine clinical practice. The current study underscored that prompt recognition, timely antiviral treatment, and effective source control remain paramount for this vulnerable inpatient population.
To the best of our knowledge, this was the first study to investigate the factors influencing fever patterns and the prolonged duration of viral shedding in individuals with COPD caused by influenza A. Additionally, few studies have explored viral shedding duration among hospitalized adult patients with influenza A in China. Nevertheless, several limitations should be mentioned. First, owing to the retrospective design of this study, we were unable to fully exclude potential biases. Some data (eg, vaccination records) were incomplete. Second, during the data collection, the specific subtypes of the influenza A virus were not differentiated, and potential confounding factors such as viral mutations were not accounted for.
Conclusion
This study suggested that early antiviral intervention and personalized management strategies for high-risk populations, particularly patients with COPD, are valuable. During the flu season, for patients with COPD who have a normal body temperature but aggravated respiratory symptoms, routine nasopharyngeal swab screening for influenza virus is recommended to prevent missed diagnoses and treatment delays. Empirical antiviral therapy may be initiated prior to the availability of test results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Centers for Disease Control and Prevention. Estimated flu burden. Available from: https://www.cdc.gov/flu/about/burden/index.html.
2. National Health Commission of the People’s Republic of China. Summary of Notifiable Infectious Diseases in China. Beijing: National Health Commission; 2022.
3. Chinese Center for Disease Control and Prevention. Weekly report on influenza surveillance in China (2023-2024 season). Beijing: China CDC; 2024 [Cited June 8 2025]. Available from: https://ivdc.chinacdc.cn/cnic/en/.
4. Wiemken TL, Furmanek SP, Carrico RM, et al. Effectiveness of oseltamivir treatment on clinical failure in hospitalized patients with lower respiratory tract infection. BMC Infect Dis. 2021;21(1):1106. doi:10.1186/s12879-021-06812-2
5. World Health Organization. Fact sheet on influenza (seasonal). Geneva: World Health Organization; [Cited May 30, 2025]. Available from: https://www.who.int/news-room/fact-sheets/detail/influenza-seasonal.
6. Moghadami M. A narrative review of influenza: a seasonal and pandemic disease. Iran J Med Sci. 2017;42(1):2–10. PMID: 28293045.
7. Wong SS, Oshansky CM, Guo X-ZJ, et al. Severe influenza is characterized by prolonged immune activation: results from the SHIVERS cohort study. J Infect Dis. 2018;217(2):245–256. doi:10.1093/infdis/jix571
8. Bautista E, Chotpitayasunondh T, Gao Z, et al. Clinical aspects of pandemic 2009 influenza A (H1N1) virus infection. N Engl J Med. 2010;362(18):1708–1719. doi:10.1056/NEJMra1000449
9. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
10. Medical, Center National Health Commission Emergency, Association Emergency Medical Branch Of Chinese, Branch Chinese Medical Doctor Association Emergency, et al. Expert consensus of Chinese and Western medicine treatment on acute exacerbation of chronic obstructive pulmonary disease in China (2021). Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021; 33(11):1281–1290. doi:10.3760/cma.j.cn121430-20211003-01438
11. Liang Z, Dong X, Zhang Z, et al. Age-related thymic involution: mechanisms and functional impact. Aging Cell. 2022;21(8):e13671. PMID: 35822239; PMCID: PMC9381902. doi:10.1111/acel.13671
12. Rydyznski Moderbacher C, Ramirez SI, Dan JM, et al. Antigen-Specific adaptive immunity to SARS-CoV-2 in acute COVID-19 and associations with age and disease severity. Cell. 2020;183(4):996–1012.e19. doi:10.1016/j.cell.2020.09.038
13. Ueno A, Kawasuji H, Miyajima Y, et al. Prolonged viral clearance of severe acute respiratory syndrome coronavirus 2 in the older aged population. J Infect Chemother. 2021;27(7):1119–1121. PMID: 33781692; PMCID: PMC7951882. doi:10.1016/j.jiac.2021.03.007
14. Lacasse É, Dubuc I, Gudimard L, et al. Delayed viral clearance and altered inflammatory responses affect severity of SARS-CoV-2 infection in aged mice. Immun Ageing. 2025;22(1):11. doi:10.1186/s12979-025-00503-1
15. Kumar D, Sehrawat S. Divergent effects of a transient corticosteroid therapy on virus-specific quiescent and effector CD8+ T cells. Front Immunol. 2019;10:1521. PMID: 31354707; PMCID: PMC6639716. doi:10.3389/fimmu.2019.01521
16. Harrison KS, Cowan SR, Jones C. Murine nasal-associated lymphoid tissue (NALT) harbors human alphaherpesvirus 1 (HSV-1) DNA during latency, and dexamethasone triggers viral replication. J Virol. 2025;99(4):e0225124. PMID: 40135894; PMCID: PMC11998502. doi:10.1128/jvi.02251-24
17. Rodrigo C, Leonardi-Bee J, Nguyen-Van-Tam JS, et al. Effect of corticosteroid therapy on influenza-related mortality: a systematic review and meta-analysis. J Infect Dis. 2015;212(2):183–194. doi:10.1093/infdis/jiu645
18. Chow EJ, Doyle JD, Uyeki TM. Influenza virus-related critical illness: prevention, diagnosis, treatment. Crit Care. 2019;23(1):214. doi:10.1186/s13054-019-2491-9
19. Yamaya M, Kikuchi A, Sugawara M, et al. Anti-inflammatory effects of medications used for viral infection-induced respiratory diseases. Respir Investig. 2023;61(2):270–283. doi:10.1016/j.resinv.2022.11.002
20. Li H, Yang S-G, Gu L, et al.National Influenza A(H1N1)pdm09 Clinical Investigation Group of China. Effect of low-to-moderate-dose corticosteroids on mortality of hospitalized adolescents and adults with influenza A(H1N1)pdm09 viral pneumonia. Influenza Other Respir Viruses. 2017;11(4):345–354. doi:10.1111/irv.12456
21. Luque-Paz D, Tattevin P, Loubet P, et al. Chronic use of inhaled corticosteroids in patients admitted for respiratory virus infections: a 6-year prospective multicenter study. Sci Rep. 2022;12(1):4199. doi:10.1038/s41598-022-08089-0
22. Hofflich B, Lunardhi A, Sunku N, et al. Modeling the viral kinetics of influenza a during infection in humans. In:
23. Cheng Y, Zhao H, Song P, et al. Dynamic changes of lymphocyte counts in adult patients with severe pandemic H1N1 influenza A. J Infect Public Health. 2019;12(6):878–883. doi:10.1016/j.jiph.2019.05.017
24. Denney L, Aitken C, Li CK-F, et al. Reduction of natural killer but not effector CD8 T lymphocytes in three consecutive cases of severe/lethal H1N1/09 influenza A virus infection. PLoS One. 2010;5(5):e10675. doi:10.1371/journal.pone.0010675
25. Uyeki TM, Bernstein HH, Bradley JS, et al. Clinical practice guidelines by the infectious diseases society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenzaa. Clin Infect Dis. 2019;68(6):895–902. doi:10.1093/cid/ciy874
26. van de Veerdonk FL, Carvalho A, Wauters J, et al. Aspergillus fumigatus biology, immunopathogenicity and drug resistance. Nat Rev Microbiol. 2025;23(10):652–666. PMID: 40316713. doi:10.1038/s41579-025-01180-z
27. Kaminski VL, Menezes ALO, de Lima KG, et al. Immunoregulation in fungal infections: a review and update on the critical role of myeloid-derived suppressor cells. J Fungi. 2025;11(7):496. doi:10.3390/jof11070496
28. Xu L, Chen B, Wang F, et al. A higher rate of pulmonary fungal infection in chronic obstructive pulmonary disease patients with influenza in a large tertiary hospital. Respiration. 2019;98(5):391–400. PMID: 31330521. doi:10.1159/000501410
29. Rabe KF, Watz H. Chronic obstructive pulmonary disease. Lancet. 2017;389(10082):1931–1940. PMID: 28513453. doi:10.1016/S0140-6736(17)31222-9
30. Sapey E, Stockley RA. COPD exacerbations. 2: aetiology. Thorax. 2006;61(3):250–258. doi:10.1136/thx.2005.041822
31. Falsey AR, Baran A, Walsh EE. Should clinical case definitions of influenza in hospitalized older adults include fever? Influenza Other Respir Viruses. 2015;9(1):23–29. doi:10.1111/irv.12316
32. To KK, Hung I, Li I, et al. Delayed clearance of viral load and marked cytokine activation in severe cases of pandemic H1N1 2009 influenza virus infection. Clin Infect Dis. 2010;50(6):850–859. doi:10.1086/650581
33. Gu Y, Zuo X, Zhang S, et al. The mechanism behind influenza virus cytokine storm. Viruses. 2021;13(7):1362. doi:10.3390/v13071362
34. Bohmwald K, Gálvez NMS, Ríos M, Kalergis AM. Neurologic alterations due to respiratory virus infections. Front Cell Neurosci. 2018;12:386. PMID: 30416428; PMCID: PMC6212673. doi:10.3389/fncel.2018.00386
35. Lee N, Chan P, Hui D, et al. Viral loads and duration of viral shedding in adult patients hospitalized with influenza. J Infect Dis. 2009;200(4):492–500. doi:10.1086/600383
36. To KK, Chan KH, Ho J, et al. Respiratory virus infection among hospitalized adult patients with or without clinically apparent respiratory infection: a prospective cohort study. Clin Microbiol Infect. 2019;25(12):1539–1545. doi:10.1016/j.cmi.2019.04.012
37. Onodera H, Urayama T, Hirota K, et al. Neutralizing activities against seasonal influenza viruses in human intravenous immunoglobulin. Biologics. 2017;11:23–30. PMID: 28331286; PMCID: PMC5354529. doi:10.2147/BTT.S123831
38. Díez JM, Casals D, Romero C, et al. Medicinal Immunoglobulin G products (2020) show high infectivity neutralizing activity against seasonal influenza virus strains selected for future vaccines (2020-2022). Open Forum Infect Dis. 2022;9(7):ofac216. doi:10.1093/ofid/ofac216.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.