")
Back to Journals » Infection and Drug Resistance » Volume 16
Adverse Events and Drug Resistance in Critically Ill Patients Treated with Colistimethate Sodium: A Review of the Literature
Authors Ahumada Topete VH , de Dios Sanchez KJ, Casas Aparicio GA, Hernandez Silva G, Lopez Vejar CE, Torres Espíndola LM , Aquino-Galvez A , Rodriguez Ganen O , Castillejos Lopez MDJ
Received 3 December 2022
Accepted for publication 11 February 2023
Published 10 March 2023 Volume 2023:16 Pages 1357—1366
DOI https://doi.org/10.2147/IDR.S398930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Victor Hugo Ahumada Topete,1,* Kevin Jesus de Dios Sanchez,1,* Gustavo Alejandro Casas Aparicio,2 Graciela Hernandez Silva,2 Cesar Emmanuel Lopez Vejar,1 Luz Maria Torres Espíndola,3 Arnoldo Aquino-Galvez,4 Odalis Rodriguez Ganen,5 Manuel de Jesus Castillejos Lopez1
1Hospital Epidemiology and Infectology Unit, National Institute of Respiratory Diseases Ismael Cosío Villegas, Mexico City, Mexico; 2Department of Infectious Disease Research, National Institute of Respiratory Diseases Ismael Cosío Villegas, Mexico City, Mexico; 3Laboratory of Pharmacology, National Institute of Pediatrics, Mexico City, Mexico; 4Molecular Biology Laboratory, National Institute of Respiratory Diseases Ismael Cosío Villegas, Mexico City, Mexico; 5Department of Hospital Pharmacy, National Institute of Respiratory Diseases Ismael Cosío Villegas, Mexico City, Mexico
*These authors contributed equally to this work
Correspondence: Manuel de Jesus Castillejos Lopez; Arnoldo Aquino Galvez, Email [email protected]; [email protected]
Abstract: The adverse events related to sodium colistimethate have had variability regarding the prevalence of nephrotoxicity, neurotoxicity, and less frequent respiratory depression. In recent years, its use has been relevant due to the increase of multidrug-resistant bacteria since it is considered the last-line drug, being its main adverse event and reason for discrepancies between authors’ nephrotoxicity. The indiscriminate use of antibiotic therapy has generated multiple mechanisms of resistance, the most common being related to Colistin, the bactericidal escape effect. Based on the search criteria, no randomized clinical trials were identified showing safety and efficacy with the use of Colistin, inferring that the application of the appropriate dose is governed by expert opinion and retrospective and prospective observational studies, which confounding factors such as the severity of the patient and the predisposition to develop acute renal failure are constant. In this review, we focus on identifying the mechanism of nephrotoxicity and bacterial resistance, where much remains to be known.
Keywords: colistin, colistimethate, nephrotoxicity, neurotoxicity, resistance mechanism, multidrug-resistant gram-negative bacteria, risk factors, high doses, toxicity
Introduction
Polymyxins were described in 19471,2 in isolates of Bacillus Polymyxa, subspecies coelestinus koyama.1,3 Sodium colistimethate (CMS) was discontinued in the 1980s due to adverse events such as nephrotoxicity and neurotoxicity, and the marketing of new drugs with a higher safety profile. The lack of efficacy of the new drugs and the indiscriminate use of antibiotics made it an ideal environment for developing multidrug-resistant gram-negative bacilli (BGN-MDR), making their reintroduction feasible two decades later.2,4
These drugs are cyclic polypeptides whose primary mechanism alters the permeability of the lipopolysaccharide wall of gram-negative bacteria. In the literature, alternative mechanisms are described as the vesicle–vesicle contact route causing exchange and loss of phospholipids and the route of death by hydroxyl radical, given by the reaction of Fenton (hydrogen peroxide oxidizes ferrous iron in serum iron). This reaction generates oxidative damage leading to cell death.4,5 Its antimicrobial spectrum comprises; A cinetobacter baumannii, Pseudomonas aeruginosa, and K. pneumoniae, having no activity against gram-positive bacteria since it does not bind favorably to lipoteichoic acid.6 Its use should be reserved as a last-line drug when you have an infection with the bacteria mentioned above and under certain conditions as empirical treatment.7
We investigate the landscape of nephrotoxicity in the last decade and describe the various resistance mechanisms reported. Until now, it has been considered the last available antibiotic therapy against multi-resistant bacteria. However, during the COVID-19 pandemic, the use of colistin increased due to a lack of evidence of a standardized treatment, resulting in greater antibiotic resistance. Starting from this point, this review will allow more information about renal deterioration and resistance mechanisms associated with this drug in multiple studies.8
In one of the largest cohorts conducted before the period of his detention by Koch9 in 1970, evaluated 317 patients using CMS, 63 (20.1%) developed acute kidney injury, while the development of neurological symptoms was in 23 (7.2%) of 317, being one of the Falagas hypotheses10 that the increase in nephrotoxicity at that time was due to the use of CMS in intramuscular forms intravenously, as well as the development of adverse events that are currently infrequent, described in Figure 1. 27
 |
Figure 1 Adverse events related to colistin. Created with BioRender.com. |
Resistance is one of the biggest concerns worldwide due to the lack of new drugs with equal or greater efficacy and fewer adverse events. The primary mechanism of resistance is the modification of 4-amino-4-deoxy-L-arabinose (L-Ara4N).11
The warnings of the Institute of Clinical and Laboratory Standards (CLSI) issued in the manual M100 version 32 concern limited clinical efficacy according to clinical data, pharmacokinetics, and pharmacodynamics (PK/PD), promulgating intermediate cohort point (<2 mg/dl) and resistant (>4 mg/dl).12 To reduce the prevalence of nephrotoxicity, an adjustment of CMS to renal dose, proposed by the International Colistin Consensus, was made,13,14 which to this day are still the guidelines used; however, the different clinical contexts, such as the patient in critical condition, mean that the doses proposed by the consensus do not reach the expected therapeutic efficacy.
The lack of precise data on the prevalence of AKI due to the use of colistin in the last decade and of randomized clinical trials on the efficacy of Colistimethate sodium in critically ill patients also allows knowing the incidence of adverse events found today generated the need for a comprehensive review to obtain updated information on the use of colistin; therefore, the main objective of this review is to present a comprehensive and up-to-date overview of adverse events and resistance to the use of colistin in critically ill patients.
Materials and Methods
We searched for original articles, and reviewed articles in PubMed, Google Scholar, and Cochrane Library between Mar 15, 2022, and Jun 20, 2022, with a temporality from 2006 to 2022, in English or Spanish. The following search terms were used: “Colistin”, “colistimethate”, “nephrotoxicity”, ‘neurotoxicity’, “resistance mechanism”, “Multidrug-resistant gram-negative bacteria”, “Risk Factors” “Toxicity”, “High doses”. Recommendations of the prism group were followed in terms of identification, detection, eligibility, and inclusion criteria. The authors evaluated the titles and abstracts of the studies according to the objective of the work. The inclusion criteria for the studies were:
- Prevalence of nephrotoxicity.
- Adverse events and mechanisms of nephrotoxicity.
- Mechanism of resistance from in vitro studies.
- Colistimethate mechanism of action.
Results
We identified 120 articles, of which 51 were eliminated for not meeting the inclusion criteria described above; of the 69, 14 were used for collecting prevalence with temporality from 2010 to 2022, and the rest were used for describing adverse events and resistance mechanisms (Figure 2). Acute kidney injury due to Colistin, resistance mechanisms, and exceptional adverse events such as neurotoxicity were identified in the included studies (Figure 1). According to the GRADE guide15 Assessing the evidence quality was low because they had an observational design.
 |
Figure 2 The article search and selection flowchart is summarized. |
Prevalence and Incidence of Adverse Events
In 2020, Rosas et al16 was the first study to mention the incidence of nephrotoxicity, which included 90 patients with a mean duration of treatment of 8.3 days and an incidence of 1.73 cases/100 days of treatment. Emphasizing that nephrotoxicity was transient and not an established lesion. Currently, in 2021 the meta-analysis conducted by Khalid Eljaaly et al.17 Despite using established doses, they conclude that despite being a last-line drug, having some alternative would be more favorable to prevent the development of nephrotoxicity (Table 1). Martínez y cols18 in 2014, in 2014, analyzed the prevalence of nephrotoxicity in critical patients, using RIFLE, concluding that critical patients may be more susceptible to nephrotoxicity,19 contrasting with studies where the prevalence of kidney injury was lower in critically ill patients.20,29,31
 |
Table 1 Compilation of Nephrotoxicity Prevalence |
In Mexico, Meraz Muñoz20 in 2018, a retrospective cohort study of patients with MDR infection treated with CMS over four days evaluated whether the effect of AKI induced by CMS could have permanent damage at the renal level. Finding that of 29 patients who had colistin-associated AKI, after six months, 22 (75%) progressed to CKD (Grade 3). Concluding that acute kidney injury associated with Colistin had an increased risk of developing chronic kidney disease in 6 months.
Nephrotoxicity Criteria
According to the Kidney Disease guidelines: Improving Global Outcomes (KDIGO), 1) increase in serum creatinine by ≥0.3 mg/dl within 48 hours, 2) increase in serum creatinine to ≥1.5 times baseline, which is known or assumed to have occurred within the previous seven days, and 3) urine volume <0,5 mL/kg/h during >6 h.21,22,69
Molecular Nephrotoxicity Hypothesis
Suzuki23 He described the first experimental evidence where CMS exerts its nephrotoxic effect by accumulating in proximal tubule cells. Determining that these cells reabsorb CMS by binding to megalin, a 600 kDa glycoprotein expressed in the apical membrane of the proximal tubule. Biological models showed a reduction in renal accumulation and a simultaneous increase in urinary excretion of Colistin when administered with a megalin-releasing agent (maleic acid) and megalin ligands (cytochrome c and FRALB). Yoshihisa Hori and Nobumasa Aoki, by cilastatin, suppressed megalin-mediated tubular reabsorption, thereby decreasing the nephrotoxic effect.24,25
Nezu and Tamai et al.26 Investigated that the mutation in the SLC22A5 gene located on chromosome 5q31.1 causes a systemic deficiency of carnitine, showing that a single intraperitoneal administration of Colistin did not produce signs of renal damage (Figure 1).27
Mohammad Tabish28 described one of the less common causes found in the literature as acquired Bartter syndrome induced by Colistin, using three days of standard therapy in the patient, a 46-year-old man, which remitted upon discontinuation of the drug.
Neurotoxicity
So far, there is no precise neurotoxicity mechanism, and there are only a few reports of neurological damage in patients treated with this drug.10,29 Nevertheless, Jeong ES et al30 and collaborators agreed with Falagas et al10 theory, where before stopping the drug, there was no pre-established dose. Intramuscular doses were used in intravenous forms, having this longer half-life and higher concentration in cerebrospinal fluid (CSF). Due to intrathecal administration, when plasma concentrations exceed the dose of 10 mg/day or greater than 20 mg/day, the generation of chemical meningitis is observed with a prevalence of 10 to 20%, developing meningismus, fever, altered mental status, increased leukocyte count and decreased glucose levels in the CSF (liquefied pleocytosis).31,32
Resistance Mechanism
The resistance mechanisms in Gram-negative are complex and only fully understood now.33 The most accepted theory is the bactericidal effect’s escape by reducing the outer membrane’s negative charge, which hinders binding to Colistin.11 The molecular mechanism that is described by replacing the phosphate groups of lipid A by the cationic remains of 4-amino-4 deoxy-L-arabinose (L-Ara4N) or phosphoethanolamine (PEtN), mutations in the regulatory systems PhoPQ and PmrAB can lead to increased positive regulation, which is accompanied by the addition of more cationic residues to LPS, decreasing the membrane load, and therefore avoiding colistin action.34
The regulations of enzymes are in charge of the system operate pmrCAB encoding three functional proteins 1) pEtN phosphotransferase Pmrc (eptA) having as function the cationic addition to lipid A. 2) Regulator of response PmrA (BasS) function: once activated, allows the activation of the operon pmrCAB, operon pmrHFIJKLM and the gene pmrE, these last two responsible for the synthesis of L-Ara4N and its binding to lipid A. 3) protein kinase sensor PmrB Function:
Activates PmrA through phosphorylation. PhoP (PhoQ), PmrA (PmrB) sensor kinases detect a reduction in the magnesium and calcium contents of the cell envelope, in addition to the presence of Colistin, so the presence of expression of these.35,36
PhoQ and PmrB drive phosphorylation of response regulators (PhoP and PmrA), enhancing the binding of these regulators to the promoters of regulated genes, generating transcription of several genes, including PmrD, its stabilized product PmrA in its phosphorylated state, allowing the generation of L-Ara4N (Table 2).11,36
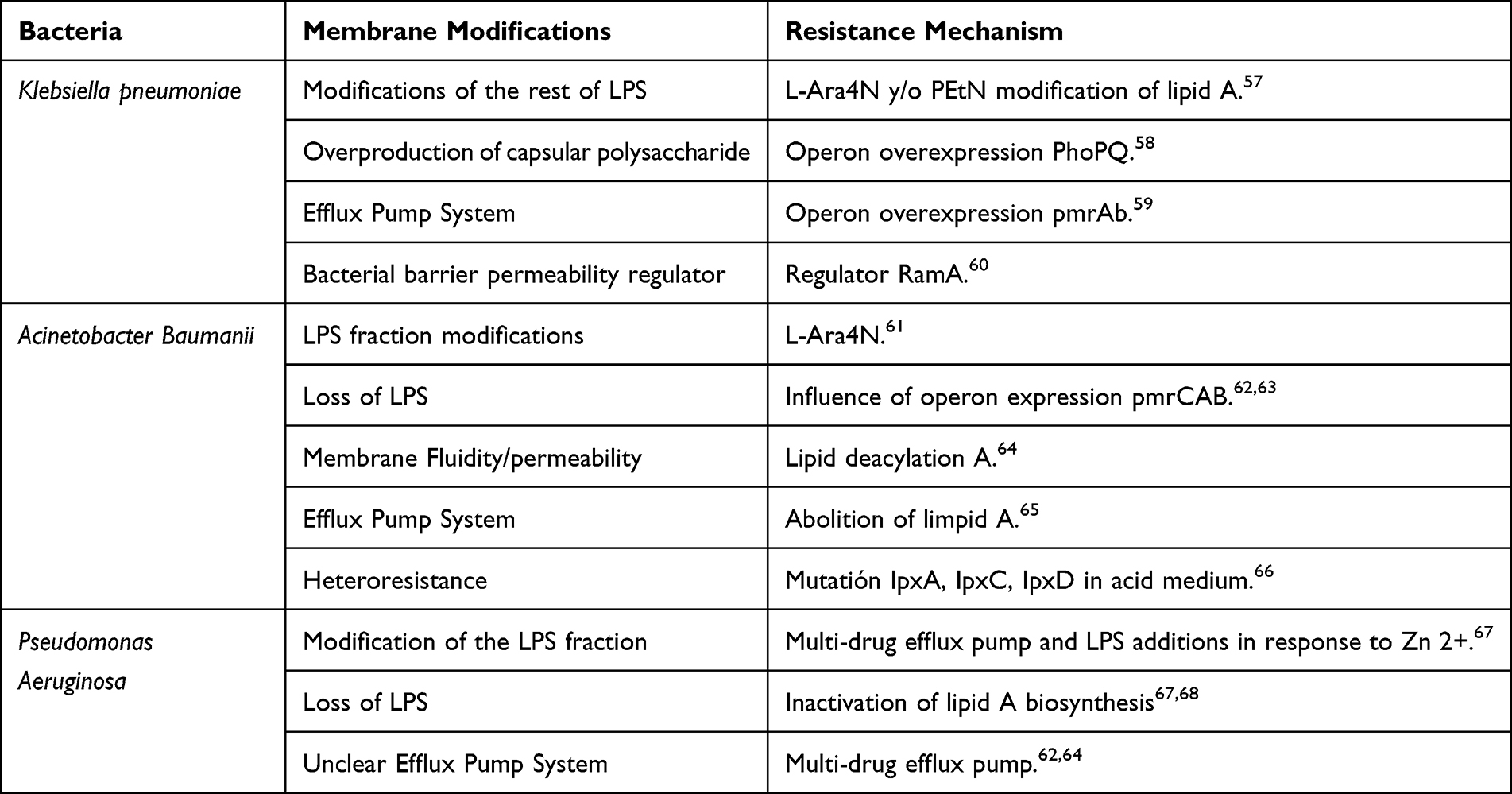 |
Table 2 Compilation of Resistance Mechanisms |
Other Adverse Events
Nephrotoxicity, neurotoxicity, lung damage, dermatological lesion are the main adverse events reported (Figure 1). At the pulmonary level, the administration of colistin for nebulization can cause different degrees of hyperreactivity, such as dry cough or bronchoconstriction. While at the dermatological level, there have been cases of rashes, rash, pruritus, urticaria or fever (Figure 1). 4
Discussion
His literature review focused on determining the prevalence of the last twelve years of CMS and the development of nephrotoxicity, as well as describing the various mechanisms of resistance to this drug, the latter being one of the leading public health problems worldwide.
Martinez et al18 found that the prevalence of nephrotoxicity with the use of CMS from 2010 to 2022 ranged (from 15.1% to 68.5%), of which the highest percentage is represented in critical patients; in this type of patents; the authors described that the predisposition to acute kidney injury is due to the use of invasive mechanical ventilation, polypharmacy, hydro electrolytic alterations, acid-base state, the latter being a component of the hypothesis of Falagas et al10 ten where he relates a state of acidosis with a decrease in bactericidal activity, not being able to reach the minimum inhibitory concentration (MIC) <2 this,12 given the neutral pH characteristics of the lipopolysaccharide2,3,10 However, up to now, there is no evidence of this deregulatory mechanism.
The sars-cov2 pandemic had a significant increase in patients in critical condition, so the use of CMS increased considerably due to the irrational use of antibiotics and the latent generation of multidrug-resistant bacteria, this added to the various variables existing in each patient, such as race, age, sex, state of severity, biochemical alterations (hypoalbuminemia), sepsis, septic shock,18,19,21,45 which may contribute to an increase in the nephrotoxic potential of CMS,21,22 since it has been described that they predispose to the risk of acute kidney injury, so that, currently, the assessment of these variables could decrease the incidence of acute kidney injury.
One of the theories of nephrotoxicity generation proposed by Rosas et al16 agrees with retrospective and prospective studies,17,18,20,21 in those patients in which the use of loading doses and duration of treatment, not schematized, generates the development of acute renal injury due to the effect of accumulated dose, so the acceptable use to reach a minimum inhibitory concentration (MIC) requires knowledge beyond the stipulated guidelines. The expertise and individualization of the patient are fundamental tools to have the desired therapeutic effect.
In the retrospective cohort of Katip et al,37 396 patients with infections caused by E. coli and Klebsiella pneumoniae were studied to evaluate the mortality by dose load of colistin. Compared to the carbapenem group, nephrotoxicity induced by colistin was reported at 48.2%; this group had more significant mortality at 30 days, greater clinical failure, and bacteriological failure. Meanwhile, what was studied by Katip et al,38 in the retrospective cohort of 365 patients, who evaluated the clinical efficacy and nephrotoxicity of colistin alone versus colistin with vancomycin, found that the colistin alone developed nephrotoxicity in 49.24% and 48, 96% with colistin and vancomycin. However, the results did not show significant differences in the clinical, microbiological, and nephrotoxicity response between more vancomycin vs colistin groups. Katip et al39 conducted a retrospective cohort study at Chiang Mai University Hospital, where they studied a total of 383 patients to evaluate 30-day survival, as well as determining nephrotoxicity in critically ill patients who received a No-loading dose (LOD) versus LD of CMS for the treatment of carbapenem-resistant A.baumannii (CRAB) infection, resulting in 1.70 times greater survival than those who did not use loading doses.
Meanwhile, the nephrotoxicity of colistin with a loading dose was 56.76%, while using colistin without a loading dose generated 32.26% of nephrotoxicity. The loading dose mechanism was the main factor in the generation of nephrotoxicity.
The future projection for the early detection of nephrotoxicity is the biomarkers of renal damage, as described by some authors,40–44 determine that Cystatin C (Cys C) is the biomarker of choice over NGAL and α-1-microglobulin for the early detection of AKI. In addition, mathematical models have been described; one of them is Phe, which has a high percentage of specificity, another is the CART analysis with high sensitivity, and these could be applied during treatment with CMS, so we can establish that these would allow the development of preventive measures.
One of the world health problems is the emergence of multidrug-resistant gram-negative bacteria, the main ones being: Pseudomonas aeruginosa, Acinetobacter baumannii, and Klebsiella pneumoniae.38
The lack of new antibiotics to combat these pathogens makes using CMS more frequent. Even with the existence of the dosage recommended by the International Colistin Committee,12 the bactericidal effect has a narrow therapeutic margin that is often related to the prescription of lower doses, thus predisposing to trigger one of its primary mechanisms such as “bactericidal escape” which through the reduction of negative charge and L-Ara4N modification generates resistance,45 other mechanisms that are described less frequently are lipid A deacylation, permeability and loss of lipopolysaccharide,54–57 which are also triggered by under-therapeutic exposure.
Currently, Xu et al46 observed the natural resistance to Colistin by eptA genes of Neisseria meningitidis, describing the beginning of knowledge on new forms of resistance, being the main public health problem for being the last pharmacological line, physicians and pharmacists must evaluate the determination of the therapeutic efficacy of colistin since it has a narrow therapeutic margin. Mainly based on its pharmacodynamic profile since nephrotoxicity and resistance is concentration dependent. Therefore, the ratio between the area under the curve and the MIC (AUC/MIC ratio) is the best PK-PD parameter to reflect the efficacy profile of colistin. In most hospitals in Latin America, therapeutic efficacy monitoring is evaluated by taking periodic cultures or reducing the number of leukocytes. Starting from this point, it can be just as cost-effective as the AUC/MIC ratio for decision-making. Giving guidelines that colistin should not be prescribed in monotherapy, given the high rate of in vitro resistance of multiple genes, including the mrc-1 gene.54,55
These data provide evidence to recommend combining colistin plus carbapenems since they have been associated with less nephrotoxicity. In addition, they reach the appropriate minimum inhibitory concentration, thus avoiding further therapeutic failure and antibiotic resistance.37–39
Meraz et al20 carried out a study in Mexico, proving the irreversible damage caused by CMS, in which they found that up to 75% of the patients evolved to chronic renal disease within six months.
However, they do not describe whether there was any association with sepsis, which is always a distracting factor in various studies and can bias the validity of the data obtained.
In this sense, this finding contributes to some theories generating uncertainty about the progression of chronic kidney disease. Clinical verification is required in these cases of irreversible damage.
We acknowledge the limitations of our review. One of the main points was the loss of homogenization of the various study cohorts due to the variation in the characteristics of the patients on therapy and the frequent presentation of sepsis, knowing that it is a factor that by itself can cause nephrotoxicity.
Conclusion
The frequency of adverse events, and mainly nephrotoxicity associated with Colistin, has a wide range of predisposing variables, including population conditions, patient severity, sepsis, mechanical ventilation, age, and other factors. However, its molecular mechanism still needs to be well defined.
The frequency of adverse events, and mainly nephrotoxicity associated with Colistin, has a wide range of predisposing variables, including population conditions, patient severity, sepsis, mechanical ventilation, age, and other factors. However, its molecular mechanism still needs to be well defined.
So far, its efficacy rate ranges from 50 to 79.1%, this being the primary justification of most authors for its use. Still, the very narrow therapeutic margin makes the possibility of nephrotoxicity a latent adverse effect and underestimating the dosage to prevent it may be the trigger effect to unleash resistance. The lack of a randomized clinical trial is the paradigm for the safe use of the drug.
Acknowledgments
National Institute of Respiratory Diseases (INER), RED MEDICI (Network of Medicine for Education, Development, and Scientific Research of Iztacala), Olmeca University.
Disclosure
Victor Hugo Ahumada Topete and Kevin Jesus de Dios Sanchez are co-first authors for this study. The authors declare that they have no conflict of interest in this work.
References
1. Vargas L. Estudio prospectivo del uso de colistina en el Servicio de Cuidados Intensivos del Hospital Nacional Edgardo Rebagliati Martins. Univ Nacional de San marcos. 2018;2(1):235–270.
2. Storm DR, Rosenthal KS, Swanson PE. Polymyxin and Related Peptide Antibiotics. Annu Rev Biochem. 1977;46(1):723–763. doi:10.1146/annurev.bi.46.070177.003451
3. Coscia L, Causa P, Giuliani E, Nunziata A. Pharmacological properties of new neuroleptic compounds. Arzneimittelforschung. 1975;25(9):1436–1442.
4. Medina J. Actualización acerca de colistina (polimixina E): aspectos clínicos, PK/PD y equivalencias. Revista Médica del Uruguay. 2017. doi:10.29193/RMU.33.3.5
5. Hancock R. The bacterial outer membrane as a drug barrier. Trends Microbiol. 1997;5(1):37–42. doi:10.1016/S0966-842X(97)81773-8
6. Alavi M, Antonic V, Stojadinovic A, Zhang B, Mina Izadjoo M. Pseudomonas aeruginosa induces pigment production and enhances virulence in a white phenotypic variant of Staphylococcus aureus. Infection and Drug Resistance. 2013;175. doi:10.2147/IDR.S49039
7. Mlynarcik P, Kolar M. Molecular mechanisms of polymyxin resistance and detection of mcr genes. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 2019;163(1):28–38. doi:10.5507/bp.2018.070
8. Plachouras D, Karvanen M, Friberg LE, et al. Population Pharmacokinetic Analysis of Colistin Methanesulfonate and Colistin after Intravenous Administration in Critically Ill Patients with Infections Caused by Gram-Negative Bacteria. Antimicrob Agents Chemother. 2009;53(8):3430–3436. doi:10.1128/AAC.01361-08
9. Koch-Weser J. Adverse Effects of Sodium Colistimethate: manifestations and Specific Reaction Rates During 317 Courses of Therapy. Ann Intern Med. 1970;72(6):857. doi:10.7326/0003-4819-72-6-857
10. Falagas ME, Kasiakou SK. Toxicity of polymyxins: a systematic review of the evidence from old and recent studies. Crit Care. 2006;10(1):R27. doi:10.1186/cc3995
11. El-Sayed Ahmed MAEG, Zhong LL, Shen C, Yang Y, Doi Y, Tian GB. Colistin and its role in the Era of antibiotic resistance: an extended review (2000–2019). Em Microbes Infections. 2020;9(1):868–885. doi:10.1080/22221751.2020.1754133
12. Tsuji BT, Pogue JM, Zavascki AP, et al. International Consensus Guidelines for the Optimal Use of the Polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39(1):10–39. doi:10.1002/phar.2209
13. Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006;34(6):1589–1596. doi:10.1097/01.CCM.0000217961.75225.E9
14. Agarossi A, Pintaudi G. Antimicrobials and Progression to Septic Shock in Severe Sepsis Patients: is Delay the Only Thing That Matters? Crit Care Med. 2017;45(9):e988–e989. doi:10.1097/CCM.0000000000002521
15. Guyatt GH, Oxman AD, Montori V, et al. GRADE guidelines: 5. Rating the quality of evidence--publication bias. J Clin Epidemiol. 2011;64(12):1277–1282. doi:10.1016/j.jclinepi.2011.01.011
16. Rosas Espinoza C, Caro Teller JM. Incidencia de nefrotoxicidad inducida por colistina intravenosa en pacientes hospitalizados [Incidence of intravenous colistin nephrotoxicity in hospitalized patients]. Rev Esp Quimioter. 2021;34(1):12–17. doi:10.37201/req/082.2020
17. Eljaaly K, Bidell MR, Gandhi RG, et al. Colistin Nephrotoxicity: meta-Analysis of Randomized Controlled Trials. Open Forum Infectious Dis. 2021;8(2):ofab026. doi:10.1093/ofid/ofab026
18. Martínez J, Loiácono F, Alemano G, Ríos F, Aguilar L, Cestari J. Insuficiencia renal aguda asociada al tratamiento con colistín en Unidad de Cuidados Intensivos. Rev Nefrol Dial Traspl. 2014;34(3):108–111.
19. Dalfino L, Puntillo F, Mosca A, et al. High-dose, extended-interval colistin administration in critically ill patients: is this the right dosing strategy? A preliminary study. Clin Infect Dis. 2012;54(12):1720–1726. doi:10.1093/cid/cis286
20. Meraz-Muñoz A, Gomez-Ruiz I, Correa-Rotter R, Ramirez-Sandoval JC. Chronic kidney disease after acute kidney injury associated with intravenous colistin use in survivors of severe infections: a comparative cohort study. J Crit Care. 2018;44:244–248. doi:10.1016/j.jcrc.2017.11.022
21. Mercado MG, Smith DK, Guard EL. Acute Kidney Injury: diagnosis and Management. Am Fam Physician. 2019;100(11):687–694.
22. Levey AS, James MT. Acute Kidney Injury. Ann Intern Med. 2017;167(9):ITC66–ITC80. doi:10.7326/AITC201711070
23. Suzuki T, Yamaguchi H, Ogura J, Kobayashi M, Yamada T, Iseki K. Megalin contributes to kidney accumulation and nephrotoxicity of colistin. Antimicrob Agents Chemother. 2013;57(12):6319–6324. doi:10.1128/AAC.00254-13
24. Hori Y, Aoki N, Kuwahara S, et al. Megalin Blockade with Cilastatin Suppresses Drug-Induced Nephrotoxicity. J Am Soc Nephrol. 2017;28(6):1783–1791. doi:10.1681/ASN.2016060606
25. Hori Y. Correction: megalin Blockade with Cilastatin Suppresses Drug-Induced Nephrotoxicity. J Am Soc Nephrol. 2022;33(4):872. doi:10.1681/ASN.2022010083
26. Nezu J, Tamai I, Oku A, et al. Primary systemic carnitine deficiency is caused by mutations in a gene encoding sodium ion-dependent carnitine transporter. Nat Genet. 1999;21(1):91–94. doi:10.1038/5030
27. Events adverse related to colistin, de BioRender.com; 2022. https://app.biorender.com/biorender-templates.
28. Tabish M, Mahendran M, Ray A, Vikram NK. Colistin-induced acquired Bartter-like syndrome: an unusual cause of the meltdown. BMJ Case Rep. 2020;13(2):e232630. doi:10.1136/bcr-2019-232630
29. Jiménez-Mejías ME, Pichardo-Guerrero C, Márquez-Rivas FJ, Martín-Lozano D, Prados T, Pachón J. Cerebrospinal fluid penetration and pharmacokinetic/pharmacodynamic parameters of intravenously administered colistin in a case of multidrug-resistant Acinetobacter baumannii meningitis. Eur J Clin Microbiol Infect Dis. 2002;21(3):212–214. doi:10.1007/s10096-001-0680-2
30. Jeong ES, Kim G, Moon KS, et al. Characterization of urinary metabolites as biomarkers of colistin-induced nephrotoxicity in rats by a liquid chromatography/mass spectrometry-based metabolomics approach. Toxicol Lett. 2016;248:52–60. doi:10.1016/j.toxlet.2016.02.018
31. Fotakopoulos G, Makris D, Chatzi M, Tsimitrea E, Zakynthinos E, Fountas K. Outcomes in meningitis/ventriculitis treated with intravenous or intraventricular plus intravenous colistin. Acta Neurochir. 2016;158(3):603–610. doi:10.1007/s00701-016-2702-y
32. De Bonis P, Lofrese G, Scoppettuolo G, et al. Intraventricular versus intravenous colistin for the treatment of extensively drug resistant Acinetobacter baumannii meningitis. Eur J Neurol. 2016;23(1):68–75. doi:10.1111/ene.12789
33. Sherry N, Howden B. Emerging Gram negative resistance to last-line antimicrobial agents fosfomycin, colistin and ceftazidime-avibactam - epidemiology, laboratory detection, and treatment implications. Expert Rev Anti Infect Ther. 2018;16(4):289–306. doi:10.1080/14787210.2018.1453807
34. Feng Y. Transferability of MCR-1/2 Polymyxin Resistance: complex Dissemination and Genetic Mechanism. ACS Infect Dis. 2018;4(3):291–300. doi:10.1021/acsinfecdis.7b00201
35. Srinivas P, Rivard K. Polymyxin Resistance in Gram-negative Pathogens. Curr Infect Dis Rep. 2017;19(11):38. doi:10.1007/s11908-017-0596-3
36. Son SJ, Huang R, Squire CJ, Leung IKH. MCR-1: a promising target for structure-based design of inhibitors to tackle polymyxin resistance. Drug Discov Today. 2019;24(1):206–216. doi:10.1016/j.drudis.2018.07.004
37. Katip W, Yoodee J, Uitrakul S, et al. Efficacy of loading dose colistin versus carbapenems for treatment of extended spectrum beta lactamase producing Enterobacteriaceae. Sci Rep. 2021;11:18. doi:10.1038/s41598-020-78098-4
38. Katip W, Oberdorfer P. Clinical Efficacy and Nephrotoxicity of Colistin Alone versus Colistin Plus Vancomycin in Critically Ill Patients Infected with Carbapenem-Resistant Acinetobacter baumannii: a Propensity Score-Matched Analysis. Pharmaceutics. 2021;13(2):162. doi:10.3390/pharmaceutics13020162
39. Katip W, Uitrakul S, Oberdorfer P. Clinical Efficacy and Nephrotoxicity of the Loading Dose Colistin for the Treatment of Carbapenem-Resistant Acinetobacter baumannii in Critically Ill Patients. Pharmaceutics. 2022;14(1):31. doi:10.3390/pharmaceutics14010031
40. Arias IM, Pobes A, Baños M, Cistatina C. Nuevo marcador de función renal [Cystatin C. New marker of renal function]. Nefrologia. 2005;25(3):217–220.
41. Hoek FJ, Kemperman FA, Krediet RT. A comparison between cystatin C, plasma creatinine, and the Cockcroft and Gault formula for the estimation of glomerular filtration rate. Nephrol Dial Transplant. 2003;18(10):2024–2031. doi:10.1093/ndt/gfg349
42. Oyabu C, Hayashi N, Sugiyama D, et al. Rinsho Byori. Rinsho Byori. The Japanese Journal of Clinical Pathology. 2006;54(12):1204–1208.
43. Tamba K, Kusano E, Ando Y, Asano Y. Nihon Jinzo Gakkai Shi. Nihon Jinzo Gakkai Shi. 2001;43(8):646–650.
44. Hotta O, Yusa N, Mukaiyama I, Taguma Y. Nihon Jinzo Gakkai Shi. Nihon Jinzo Gakkai Shi. 1999;41(8):797–803.
45. Quiroga C, Nastro M, Di Conza J. Current scenario of plasmid-mediated colistin resistance in Latin America. Revista Argentina de Microbiología. 2019;51(1):93–100. doi:10.1016/j.ram.2018.05.001
46. Xu Y, Wei W, Lei S, Lin J, Srinivas S, Feng Y. An Evolutionarily Conserved Mechanism for Intrinsic and Transferable Polymyxin Resistance. mBio. 2018;9(2):e02317. doi:10.1128/mBio.02317-17
47. Arrayasillapatorn N, Promsen P, Kritmetapak K, Anunnatsiri S, Chotmongkol W. Colistin-Induced Acute Kidney Injury and the Effect on Survival in Patients with Multidrug-Resistant Gram-Negative Infections: significance of Drug Doses Adjusted to Ideal Body Weight. Int J Nephrol. 2021;2021:7795096. doi:10.1155/2021/7795096
48. Abdellatif S, Trifi A, Daly F, Mahjoub K, Nasri R, Ben Lakhal S. Efficacy and toxicity of aerosolised colistin in ventilator-associated pneumonia: a prospective, randomized trial. Ann Intensive Care. 2016;6(1):26. doi:10.1186/s13613-016-0127-7
49. Hartzell JD, Neff R, Ake J, et al. Nephrotoxicity associated with intravenous colistin (colistimethate sodium) treatment at a tertiary care medical center. Clin Infect Dis. 2009;48(12):1724–1728. doi:10.1086/599225
50. Tuon FF, Rigatto MH, Lopes CK, Kamei LK, Rocha JL, Zavascki AP. Risk factors for acute kidney injury in patients treated with polymyxin B or colistin methanesulfonate sodium. Int J Antimicrob Agents. 2014;43(4):349–352. doi:10.1016/j.ijantimicag.2013.12.002
51. Sorlí L, Luque S, Grau S, et al. Trough colistin plasma level is an independent risk factor for nephrotoxicity: a prospective observational cohort study. BMC Infect Dis. 2013;13(1):380. doi:10.1186/1471-2334-13-380
52. Rocco M, Montini L, Alessandri E, et al. Risk factors for acute kidney injury in critically ill patients receiving high intravenous doses of colistin methanesulfonate and/or other nephrotoxic antibiotics: a retrospective cohort study. Crit Care. 2013;17(4):R174. doi:10.1186/cc12853
53. Dalfino L, Puntillo F, Mosca A, et al. High-Dose, Extended-Interval Colistin Administration in Critically Ill Patients: is This the Right Dosing Strategy? A Preliminary Study. Clin Infectious Dis. 2012;54(12):1720–1726. doi:10.1093/cid/cis286
54. Pogue JM, Lee J, Marchaim D, et al. Incidence of and risk factors for colistin-associated nephrotoxicity in a large academic health system. Clin Infect Dis. 2011;53(9):879–884. doi:10.1093/cid/cir611
55. Deryke CA, Crawford AJ, Uddin N, Wallace MR. Colistin dosing and nephrotoxicity in a large community teaching hospital. Antimicrob Agents Chemother. 2010;54(10):4503–4505. doi:10.1128/AAC.01707-09
56. Paul M, Bishara J, Levcovich A, et al. Eficacia y seguridad de la colistina: estudio prospectivo comparativo de cohortes. J Quimioterapia antimicrobiana. 2010;65(5):1019–1027. doi:10.1093/jac/dkq069
57. Kaye KS, Pogue JM, Tran TB, Nation RL, Li J. Agents of Last Resort: polymyxin Resistance. Infect Dis Clin North Am. 2016;30(2):391–414. doi:10.1016/j.idc.2016.02.005
58. Poirel L, Jayol A, Nordmann P. Polymyxins: antibacterial Activity, Susceptibility Testing, and Resistance Mechanisms Encoded by Plasmids or Chromosomes. Clin Microbiol Rev. 2017;30(2):557–596. doi:10.1128/CMR.00064-16
59. Cheng YH, Lin TL, Lin YT, Wang JT. Amino Acid Substitutions of CrrB Responsible for Resistance to Colistin through CrrC in Klebsiella pneumoniae. Antimicrob Agents Chemother. 2016;60(6):3709–3716. doi:10.1128/AAC.00009-16
60. Perez F, El Chakhtoura NG, Yasmin M, Bonomo RA. Polymyxins: to Combine or Not to Combine? Antibiotics. 2019;8(2):38. doi:10.3390/antibiotics8020038
61. Jeannot K, Bolard A, Plésiat P. Resistance to polymyxins in Gram-negative organisms. Int J Antimicrob Agents. 2017;49(5):526–535. doi:10.1016/j.ijantimicag.2016.11.029
62. Lima WG, Alves MC, Cruz WS, Paiva MC. Chromosomally encoded and plasmid-mediated polymyxins resistance in Acinetobacter baumannii: a huge public health threat. Eur J Clin Microbiol Infect Dis. 2018;37(6):1009–1019. doi:10.1007/s10096-018-3223-9
63. Snitkin ES, Zelazny AM, Gupta J, et al. Genomic insights into the fate of colistin resistance and Acinetobacter baumannii during patient treatment. Genome Res. 2013;23(7):1155–1162. doi:10.1101/gr.154328.112
64. Trebosc V, Gartenmann S, Tötzl M, et al. Dissecting Colistin Resistance Mechanisms in Extensively Drug-Resistant Acinetobacter baumannii Clinical Isolates. mBio. 2019;10(4):e01083–19. doi:10.1128/mBio.01083-19
65. Nhu N, Riordan DW, Do HoanNhu T, et al. The induction and identification of novel Colistin resistance mutations in Acinetobacter baumannii and their implications. Sci Rep. 2016;6:28291. doi:10.1038/srep28291.
66. Muller C, Plésiat P, Jeannot K. A two-component regulatory system interconnects resistance to polymyxins, aminoglycosides, fluoroquinolones, and β-lactams in Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2011;55(3):1211–1221. doi:10.1128/AAC.01252-10
67. Miller AK, Brannon MK, Stevens L, et al. PhoQ mutations promote lipid A modification and polymyxin resistance of Pseudomonas aeruginosa found in colistin-treated cystic fibrosis patients. Antimicrob Agents Chemother. 2011;55(12):5761–5769. doi:10.1128/AAC.05391-11
68. Vandeplassche E, Sass A, Lemarcq A, Dandekar AA, Coenye T, Crabbé A. In vitro evolution of Pseudomonas aeruginosa AA2 biofilms in the presence of cystic fibrosis lung microbiome members. Sci Rep. 2019;9(1):12859. doi:10.1038/s41598-019-49371-y
69. Salgado G, Landa M, Masevicius D, et al. Insuficiencia renal aguda según RIFLE y AKIN: estudio multicéntrico. Medicina Intensiva. 2014;38(5):271–277. doi:10.1016/j.medin.2013.04.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.