Back to Journals » Journal of Pain Research » Volume 15
Adverse Effects Associated with Patient-Controlled Analgesia with Ketamine Combined with Opioids and Ketamine Infusion with PCA Bolus in Postoperative Spine Patients: A Retrospective Review
Authors Pouldar TM, Maher DP, Betz AW, Wiegers JJ, Friedman JA, Zaidi SS, Rejali A, Tran HP, Yumul R, Louy C
Received 17 January 2022
Accepted for publication 5 August 2022
Published 10 October 2022 Volume 2022:15 Pages 3127—3135
DOI https://doi.org/10.2147/JPR.S358770
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Ellen Soffin
Tiffany M Pouldar,1 Dermot P Maher,2 Alexander W Betz,1 Jeffrey J Wiegers,1 Jeremy A Friedman,1 Sameer S Zaidi,1 Ali Rejali,3 Hai P Tran,3 Roya Yumul,1,4 Charles Louy1
1Department of Anesthesiology, Cedars-Sinai Medical Center, Los Angeles, CA, 90048, USA; 2Department of Anesthesiology and Critical Care Medicine, Pain Medicine Division, Johns Hopkins Hospital, Baltimore, MD, 21205, USA; 3Department of Pharmacy, Cedars-Sinai Medical Center, Los Angeles, CA, 90048, USA; 4Department of Anesthesiology, David Geffen School of Medicine-UCLA, Los Angeles, CA, 90095, USA
Correspondence: Charles Louy, Department of Anesthesiology, Cedars-Sinai Medical Center, 8700 Beverly Blvd #8211, Los Angeles, CA, 90048, USA, Tel +1 310-423-5841, Email [email protected]
Objective: There has been increasing use of ketamine at subanesthetic doses as an adjunct to opioids in perioperative pain management. There are several known adverse drug effects (ADEs) associated with ketamine. However, the incidence of ADEs with ketamine infusions with patient-controlled analgesia (PCA) boluses compared with combined opioid and ketamine PCAs is not well described. The objectives of this study were to compare the incidence and type of ADEs in postoperative spine surgery patients on ketamine infusions with as-needed PCA boluses to patients on combined opioid and ketamine PCAs.
Methods: The medical records of patients who underwent spine surgery between March 2016 and March 2020 who were postoperatively treated with a ketamine infusion and as-needed PCA boluses and parenteral opioids or treated with a combined opioid and ketamine PCA were reviewed. Perioperative information including patient characteristics and preoperative morphine equivalent daily dose (MEDD) were collected. Patient charts were reviewed for ADEs including psychological and neurological side effects, nausea, and new-onset tachycardia.
Results: A total of 315 patients met the inclusion criteria and were included in the final analysis. Of these patients, 121 experienced at least one ADE (38%). Sixteen of the 68 ketamine infusion with PCA bolus patients (24%), 77 of the 203 hydromorphone and ketamine patients (38%), and 28 of the 44 morphine and ketamine patients (64%) experienced an ADE [p< 0.01]. In patients with preoperative MEDD ≤ 90, nausea was the only ADE that differed significantly among the three groups.
Conclusion: This retrospective analysis suggests that postoperative spine patients treated with a ketamine infusion with as-needed PCA boluses and parenteral opioids were associated with fewer ADEs when compared to an intravenous combined opioid and ketamine PCA. In patients with preoperative MEDD ≤ 90, nausea with and without emesis was the only ADE that showed statistically significant difference amongst the three groups.
Keywords: ketamine, opioid, patient-controlled analgesia, adverse drug effects, postoperative, retrospective
Introduction
Ketamine is a phencyclidine derivative that antagonizes the N-methyl-D-aspartate (NMDA) receptor and has additional pharmacological effects at multiple other receptors. It was first clinically used as an anesthetic in humans as early as 1964 and FDA approved in 1970.1 Recently, there has been increasing use of ketamine at subanesthetic doses as an adjunct in both acute and chronic pain management, as it may reduce opioid requirements.2,3 Subanesthetic intraoperative ketamine infusions may be considered for opioid-dependent or opioid-tolerant patients, especially patients undergoing highly stimulating or painful surgery.4 Complementary usage of ketamine in the perioperative period is associated with reduced postoperative opioid consumption for up to 6 weeks following spine surgery.5–7
Ketamine may lead to a number of adverse drug effects (ADEs) including hallucinations, dizziness, delirium, visual disturbances, tachycardia, hypertension, and nausea.7 Intraoperative ketamine, when used in combination with opioids as part of a multimodal anesthetic, has been shown to reduce the risk of postoperative opioid-related adverse effects, including decreased postoperative nausea and vomiting.8–10
Despite ketamine’s ability to reduce opioid consumption, there is conflicting data on the incidence of postoperative ADEs associated with ketamine. Furthermore, there are few studies addressing ketamine patient-controlled analgesia (PCA) dosages or infusion dosages that can lead to ketamine-induced ADEs.11,12 Recent guidelines have even recommended intraoperative ketamine infusions for complex spine surgeries, but not for the immediate postoperative period.13
Even with increasing use of ketamine, there are limited studies directly comparing the incidence of ADEs in ketamine infusions with as-needed PCA boluses and combined opioid and ketamine PCAs in postoperative spine patients. The objective of this study is to compare the incidence and type of ADEs in postoperative spine surgery patients on ketamine infusions with PCA bolus to patients on combined opioid and ketamine PCAs. We want to determine whether patients on postoperative ketamine infusions with PCA bolus experience lower incidence rates of ADEs when compared to patients placed on combined hydromorphone and ketamine PCAs as well as combined morphine and ketamine PCAs.
Methods
The Cedars-Sinai Medical Center Institutional Review Board approved this study protocol without a requirement for written patient consent. The study was consistent with the standards set by the Declaration of Helsinki. A retrospective analysis was performed on consecutive patients between the ages of 18 and 79 who underwent elective or urgent, but not emergent, single and multi-level spine surgery at one urban, hybrid academic/private institution in Los Angeles, California, between March 2016 and March 2020. Patients underwent cervical, thoracic, lumbar, and sacral anterior fusions, posterior fusions, laminectomies, foraminotomies, microdiscectomies, and corpectomies. Patients received either a postoperative ketamine infusion with PCA bolus, combined hydromorphone and ketamine PCA, or combined morphine and ketamine PCA.
Exclusion criteria included age less than 18 years, patients who received opioid-alone PCAs, oral or intranasal ketamine, and patients treated with regional anesthesia. Both Intensive Care Unit (ICU) and non-ICU patients were included. Patients who received intraoperative ketamine for induction and analgesia were included in the study if they were also treated postoperatively with a ketamine infusion with PCA bolus, hydromorphone and ketamine PCA, or morphine and ketamine PCA. The main outcome investigated was the number and type of ADEs experienced by patients in the three groups. Information was obtained from hospital progress notes in a unified electronic medical record (EMR). Patients were first grouped by the type of PCA used postoperatively and then dichotomized into those that experienced a particular ADE and those that did not.
Patient characteristics including age, gender, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, and preoperative morphine equivalent daily dose (MEDD) were recorded. It was noted whether patients were diagnosed with chronic pain prior to their surgery. Patients were identified as having chronic pain if they experienced pain lasting more than 6 months prior to surgery.14 The average daily amount of preoperative opioids that each patient was prescribed, as indicated in their medical records, were converted into the equianalgesic dose of oral morphine.15 Similarly, intraoperative opioid and ketamine use were both recorded. Patients who required a rapid response team (RRT) assessment for imminent clinical deterioration while on a PCA were also identified.
The decision to begin a postoperative PCA was made at the discretion of the inpatient pain service (IPS), comprised of nurse practitioners and attending pain physicians, in consultation with the primary surgical team. The IPS team was trained in the management of ketamine infusions with PCA bolus as well as combined opioid and ketamine PCAs, including detection of ADEs. Patients were treated with a ketamine infusion with PCA bolus at 0.06 mg/kg/hr with a 0.1 mg/hr demand dose bolus, a combined hydromorphone 1 mg/mL and ketamine 1 mg/mL PCA, or combined morphine 1 mg/mL and ketamine 1 mg/mL PCA. Demand doses and lockout intervals for the combined opioid and ketamine PCAs varied at the discretion of the IPS team and were recorded. Patients in the ketamine infusion with PCA bolus group were continued on their home oral opioid regimen with additional as-needed oral and intravenous opioids available to supplement the ketamine infusion and PCA.
All patients were extubated in the operating room and admitted to the postoperative neurosurgical floor or the neurosurgical intensive care unit following surgery. The IPS team managed and followed patients daily while using a postoperative infusion or PCA, including weekends and holidays. The PCA was generally started within 4 hours following surgery, but could be started as late as 24 hours postoperatively. Duration of PCA in days was recorded for each patient. ADEs were managed with benzodiazepines, clonidine, and ondansetron when appropriate. Patient infusions and PCAs could be discontinued at any time following initiation. Patient’s EMR daily progress notes written by the IPS team, surgical team, and registered nurses were assessed for specific ADEs. Patients were examined for psychological ADEs including visual hallucinations, auditory hallucinations, paranoid ideas, anxious feelings, inability to control thoughts, derealization in time and space, increased awareness of sound and color, out-of-body experiences, and euphoria while on a PCA. Similarly, neurological ADEs experienced by patients, including dizziness, sedation, blurred vision, vertigo, nystagmus, nightmares, vivid dreams, impaired motor function, and memory deficits while on a PCA, were documented. The EMR was also reviewed for documented nausea with or without vomiting while being treated with a PCA, heart rate immediately prior to initiation of PCA and maximum heart rate during PCA treatment. Tachycardia was defined as a heart rate greater than or equal to 100 beats per minute. Patients with new-onset tachycardia while on a PCA were counted. Lastly, length of hospitalization in days was documented.
Given the higher preoperative MEDD in the combined opioid PCA groups, we conducted a sub-analysis of 189 patients with preoperative MEDD less than or equal to 90. The CDC recommends that prescribers should not increase opioid dosages to greater than 90 MEDD/day unless necessary and with careful justification.15 This sub-analysis may help determine if the three treatment modalities maintain differences in postoperative ADEs among patients with similar preoperative MEDD. Similarly, a sub-analysis of patients who experienced any ADE except for new-onset tachycardia was performed to draw a more meaningful comparison with existing literature.
Statistical Analyses
For continuous variables of sufficient homoscedasticity, a one-way analysis of variance was used to compare differences between the three analgesic groups. When significant differences were detected, a Tukey–Kramer test was performed for post hoc pairwise comparison. Equality of variance was assessed using Levene’s test. For continuous variables which violated the equality of variance assumption, Welch’s one-way ANOVA was substituted for the traditional one-way ANOVA and the Games–Howell test was used for post hoc pairwise comparison. For the sole ordinal variable, ASA Status, the Kruskal–Wallis H-test was used. For all other categorical variables, either Pearson’s chi-squared test or Fisher’s exact test was used. When significant differences were detected, a post hoc pairwise comparison was performed with Bonferroni adjusted p-values. Among outcome variables, a Bonferroni correction was also included. Finally, a binary logistic regression was performed to assess the risk of an ADE for each analgesic group. Independent variables were selected either due to clinical relevance or a significant difference between analgesic groups. Dependent variables included the dichotomous composite, Any ADE, and Nausea with or without emesis. Associations with P<0.05 were considered statistically significant. All analyses were conducted using R statistical software, version 4.2.0.
Results
A total of 1630 medical records were reviewed. A total of 315 patients were included in the analysis based on the study criteria. A total of 1315 patients were excluded as these patients did not meet inclusion criteria. Of the patients included in the analysis, 68 were treated with a ketamine infusion with PCA bolus, 203 with hydromorphone and ketamine, and 44 with morphine and ketamine. No patient experienced respiratory or cardiac arrest while on a PCA. No patient required the use of naloxone. No differences were found among the three groups with respect to gender, BMI, ASA status, chronic pain diagnosis, and prior spine surgery (Table 1). In total, 176 females and 139 males were included in the study. The average preoperative MEDD is 61 in the ketamine infusion with PCA bolus group (group 1), 102 in the hydromorphone and ketamine group (group 2), and 113 in the morphine and ketamine group (group 3) [p=0.02], the post hoc pairwise comparisons between group 2 and group 1, as well as between group 3 and group 1 being both significant.
 |
Table 1 Patient Characteristics in the Ketamine Infusion with PCA Bolus Group, Combined Hydromorphone and Ketamine PCA Group, and Combined Morphine and Ketamine PCA Group (N=315) |
The majority of patients in each group underwent multi-level spine surgery (Table 2). Eighty-two percent of ketamine infusion with PCA bolus patients, 45% of hydromorphone and ketamine, and 61% of morphine and ketamine patients received ketamine intraoperatively [p<0.01] (significant differences between the ketamine infusion with PCA bolus group and combined hydromorphone and ketamine group by post-hoc analysis). Only two patients received intraoperative ketamine infusions. Patients in the ketamine infusion with PCA bolus cohort received less intraoperative opioids when compared to the hydromorphone and ketamine PCA group as well as the morphine and ketamine PCA group [p=0.05].
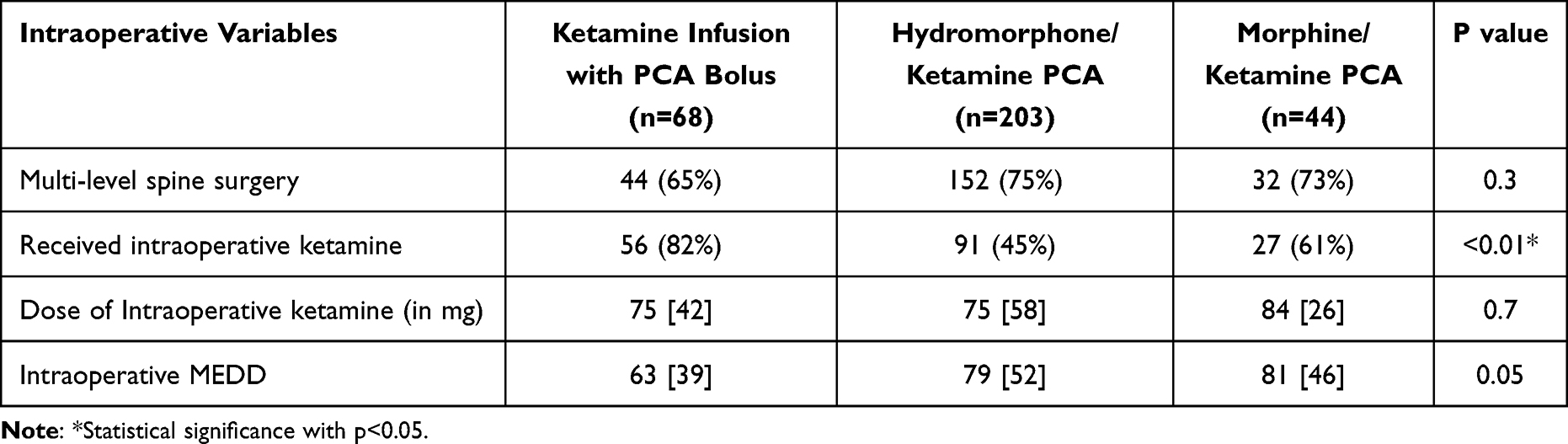 |
Table 2 Intraoperative Variables in the Ketamine Infusion with PCA Bolus Group, Combined Hydromorphone and Ketamine PCA Group, and Combined Morphine and Ketamine PCA Group (N=315) |
In total, 121 of 315 patients experienced at least one ADE (Table 3). Sixteen of the 68 ketamine infusion with PCA bolus patients (24%), 77 of the 203 combined hydromorphone and ketamine PCA patients (38%), and 28 of the 44 combined morphine and ketamine PCA patients (64%) experienced an ADE [p<0.01]; the proportions are significantly different between the combined morphine and ketamine PCA group compared to the ketamine infusion with PCA bolus group. The most common ADE was new-onset tachycardia (22%) followed by nausea (13%). Two of the 68 patients on ketamine infusions with PCA bolus (group 1) (3%), 11 of the 203 patients on combined hydromorphone and ketamine PCAs (group 2) (5%), and 9 of the 44 patients on combined morphine and ketamine PCAs (group 3) (21%) experienced psychological ADEs [p<0.01]; proportions differ significantly between group 1 and group 3, and between group 2 and group 3. Eight of the 315 patients required benzodiazepine treatment and two of these patients were continued on their home benzodiazepines. Two of the 315 patients required clonidine.
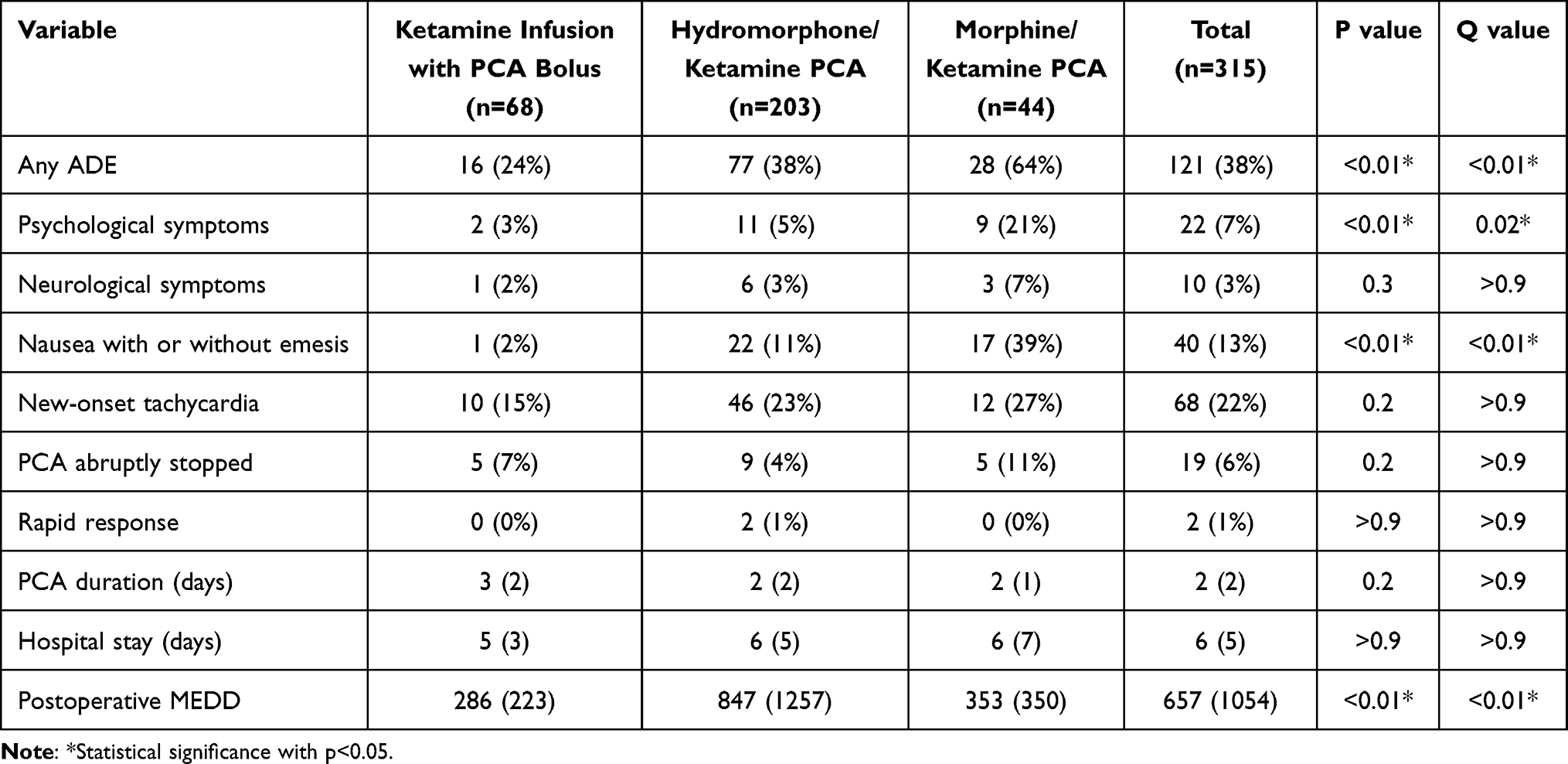 |
Table 3 Incidence of ADEs and Other Variables in the Ketamine Infusion with PCA Bolus Group, Combined Hydromorphone and Ketamine PCA Group, and Combined Morphine and Ketamine PCA Group (N=315) |
Amongst the three groups, 297 out of 315 patients were taken off their PCA once their pain was controlled and transitioned to oral medications for discharge home. Only 19 patients had ADEs that necessitated discontinuation of the PCA. Postoperative MEDD was the lowest in the ketamine infusion with PCA bolus group compared to the combined opioid and ketamine groups [p<0.01].
The sub-analysis of 189 patients with preoperative MEDD less than or equal to 90 displayed an average preoperative MEDD of 31 in the ketamine infusion with PCA bolus group (n=50), 34 in the hydromorphone and ketamine group (n=116), and 35 in the morphine and ketamine group (n=23). A statistically significant difference persisted with regards to nausea with or without emesis, with one patient in the ketamine infusion with PCA bolus group (2%), 16 patients in the combined hydromorphone and ketamine group (14%), and 11 patients in the combined morphine and ketamine group (48%) [p<0.01]. In the MEDD ≤ 90 patient population, nausea with or without emesis was the only significant ADE.
Among the patient population, 174 patients received intraoperative ketamine while 141 did not. When comparing the three PCA groups in patients who received intraoperative ketamine, persistent statistical differences existed with respect to any ADE: 12 patients in the ketamine infusion with PCA bolus group (21%), 36 in the hydromorphone ketamine PCA group (40%), and 16 in the morphine ketamine PCA group (59%) [p<0.03]. Similarly, a statistical significance persisted for nausea with or without emesis, with a total of zero of 56 patients in the ketamine infusion with PCA bolus group (0%), seven out of 91 in the hydromorphone and ketamine group (8%), and nine out of 27 in the morphine ketamine group (33%) [p<0.01]. The incidence of new-onset tachycardia across the three groups remained non-significant [p=0.5]. A repeat sub-analysis of the 141 patients who did not receive intraoperative ketamine yielded similar levels of significance for incidence of any ADE [p=0.03], nausea with or without vomiting [p<0.01], and new-onset tachycardia [p=0.4]. Lastly, intraoperative opioid usage was not associated with postoperative ADEs [p=0.4].
With regards to any ADE when excluding new-onset tachycardia, 22% of the patients experienced an ADE and a statistically significant difference persisted amongst the three groups. Eight patients in the ketamine infusion with PCA bolus group (12%), 41 patients in the combined hydromorphone and ketamine group (20%), and 21 patients in the combined morphine and ketamine group (48%) experienced an ADE [p<0.01].
Discussion
Postoperative spine surgery patients treated with a ketamine infusion with PCA bolus and parenteral opioids experienced less ADEs compared to patients who received hydromorphone and ketamine as well as morphine and ketamine PCAs. There are statistically fewer incidences of psychological symptoms and nausea in the ketamine infusion with PCA bolus group compared to the combined opioid and ketamine groups. There are no differences between the groups with respect to neurological ADEs or new-onset tachycardia. These results suggest that postoperative spine surgery patients treated with a multimodal approach consisting of a ketamine infusion with PCA bolus and as-needed parenteral opioids were associated with a lower incidence of ADEs when compared to hydromorphone and ketamine as well as morphine and ketamine PCA treatment.
A possible explanation for the higher incidence of ADEs in the combined opioid and ketamine PCA group is that they did not have a basal rate infusion in comparison to the ketamine infusion with PCA group, which provided a steady-state blood concentration of ketamine, possibly allowing for less opioid consumption. The opioid containing PCAs demand dosing allowed for pulsatile boluses of both opioid and ketamine, which may be responsible for an ADE. Serum ketamine and opioid levels were not measured as part of routine care and were not included in this analysis. Additionally, the ketamine infusion with PCA bolus group had access to as-needed oral and intravenous opioids to supplement the PCA. However, these patients had lower postoperative MEDD dosages compared to the combined opioid and ketamine PCA groups. Thus, the higher incidence of ADEs in the combined groups may be secondary to the opioids, not ketamine.
Patients on postoperative ketamine infusions with PCA boluses as well as combined opioid and ketamine PCAs do not require Intensive Care Unit (ICU) or Progressive Care Unit (PCU) nursing in our institution. They can be placed on the hospital floor without special monitoring. This has been in practice at our institution since 2015 and continues to occur in 2022. Not every patient can receive a postoperative ketamine infusion with PCA bolus or combined opioid and ketamine PCA. Patients with elevated intracranial pressure, intraocular pressure, and uncontrolled hypertension were not started on ketamine infusions with PCA bolus or combined opioid and ketamine PCAs.
The incidence of ADEs in the presented data is greater when compared to the existing literature.
Some studies have shown that there is no associated increase in neurologic or psychiatric ADEs with the use of a single dose or intravenous infusions of low-dose ketamine.7 Other studies have reported that intravenous infusions of ketamine increased psychiatric effects when compared to a placebo group.16 For example, the PODCAST trial demonstrated that a single subanesthetic dose of ketamine led to postoperative hallucinations and nightmares, but did not lead to delirium following major surgery.17 There exists literature describing the effect of adding ketamine to opioids for the treatment of acute and acute-on-chronic pain.18–20
One study that analyzed patients receiving morphine and ketamine PCAs found that 6.2% had vivid dreams and/or hallucinations and 23.5% experienced nausea, compared to 21% and 37% in the presented data, respectively.21 Although our study similarly focuses on medications administered through PCAs, it differs as the previous study included perioperative patients undergoing many surgeries, rather than being limited to spine surgery patients. Additionally, the prior study did not screen for psychological symptoms beyond hallucinations.
In our study, patients treated with a ketamine infusion with PCA bolus were placed on a subanesthetic dose of 0.06 mg/kg/hr and demand dose of 0.1 mg/hr, which is lower compared to doses reported in the literature.7 For instance, the addition of an intraoperative and postoperative ketamine infusion at 0.12 mg/kg/hr for 24 hours did not lead to side effects including headache, hallucinations, and excessive sedation.22 This dose is within the current guidelines for use of adjunct ketamine infusions (up to 1 mg/kg/hr) for perioperative analgesia.4
Schwenk conducted a retrospective, observational study analyzing ADEs associated with ketamine alone infusions as high as 20 mg/hr in 321 postoperative spine surgery patients, and found that 31.8% of the patients exhibited at least one ADE, the most common being central nervous system excitation.11 Similarly, Stoker performed a retrospective review of 95 patients who received subanesthetic dosed ketamine infusions and found that 29.5% of the patients experienced at least one ADE, the most common being hallucinations and dysphoria at 14.8%.23 This is in contrast to the presented data, which found that 38% of the patients displayed at least one ADE, the most predominant being new-onset tachycardia. When removing new-onset tachycardia as an ADE, 22% of the patients displayed at least one ADE, lower than the presented rates in Stoker and Schwenk. Our data also showed 13% of all patients and only 2% of those who received a ketamine infusion with PCA bolus experienced nausea comparable to the 2.8% incidence described by Schwenk. In our study, the hydromorphone and ketamine PCA group as well as the morphine and ketamine PCA group account for our higher percentage of ADEs. This plausibly explains our overall higher occurrence of ADEs in comparison to the Schwenk and Stoker studies (Table 4). Additionally, the presented study includes broader psychological and neurological ADEs as well as new-onset tachycardia.
 |
Table 4 Comparison of Incidence of Ketamine ADEs Among Retrospective and Meta-Analysis of Prospective Studies |
Conversely, Rasmussen retrospectively studied 50 patients on both medical and surgical units who received continuous intravenous ketamine infusions for management of pain or sedation.24 They noted that 22% of the patients experienced short-lived psychological symptoms compared to 7% of the patients in the presented data. The side effects in Rasmussen’s analysis include agitation, confusion, and hallucinations that occurred during or shortly after starting the infusion. Their patients were treated with 0.01 to 1.64 mg/kg/hr, with an average rate of 0.19 mg/kg/hr. The infusion rates between patients who responded poorly to ketamine and those who did not were not different (p = 0.53).24 However, similar to Schwenk and Stoker’s studies, Rasmussen’s study only focused on continuous intravenous ketamine infusions and did not include patients on combined intravenous hydromorphone and ketamine as well as morphine and ketamine PCAs.
There exists no statistical significance between our three groups with respect to new-onset tachycardia. This is potentially because postoperative patients may experience increases in baseline heart rate secondary to inadequate pain control or post-surgical complications such as bleeding, infection, or sepsis. Intramuscular ketamine (4 mg/kg) or intravenous ketamine (1 mg/kg) may cause a transient increase in heart rate when treating agitation in the emergency room.25 This may be secondary to a reduction in vagal efferent activity and increased sympathetic activity.26 Despite this evidence, there is limited literature commenting on the effect of ketamine infusions and PCAs on heart rate.
More recently, Gil et al published a retrospective case–control study of surgical patients treated with postoperative ketamine infusions that were discontinued secondary to ADEs. One of the statistically significant factors associated with the discontinuation of ketamine infusions was higher postoperative opioid PCA use compared to the control group. This could explain the higher rate of ADEs in our combined opioid and ketamine PCA groups compared to the ketamine infusion with PCA bolus group. It is worth noting that in Gil’s study, only 18.6% of patients with an ADE resulting in discontinuation of ketamine had resolution of the ADEs following cessation of their ketamine infusion. This may infer an association of what may have been thought as ADEs caused by ketamine to be in fact caused by opioid PCAs, consistent with our findings.12
Patients in the ketamine infusion with PCA bolus group, on average, had a lower preoperative MEDD compared to the opioid and ketamine PCA groups, suggesting that opioid dependent or opioid tolerant patients with higher preoperative MEDD were more likely to receive a postoperative combined opioid and ketamine PCA. Moreover, the sub-analysis of patients with preoperative MEDD ≤90 shows that a statistically significant difference persists with regards to nausea with or without emesis; the previously identified differences in psychological ADEs are no longer statistically significant. Of note, the sub-analysis highlights that nausea with or without emesis is the only ADE which differs significantly among the three groups, being the lowest in the ketamine infusion with PCA bolus in patients with preoperative MEDD ≤ 90.
Additionally, when controlling for patients who received intraoperative ketamine, a statistically significant difference persisted with regards to any ADE as well as nausea with or without emesis whereas new-onset tachycardia remained statistically insignificant. Based on this sub-analysis, intraoperative ketamine is not associated with postoperative ADEs. This strengthens the presented results as well as the likelihood that postoperative combined opioid and ketamine PCAs are directly linked to ADEs. Likewise, intraoperative opioid usage is not associated with postoperative ADEs.
This study has several limitations. As with all retrospective studies, only association, not causation, can be determined. There are unequal sample sizes between groups. There is a possibility of incomplete outcome and endpoint data as the main analysis was through retrospective examination via electronic medical record charts. The IPS team did not have a set protocol when evaluating patients; thus, some ADEs may have been missed. Only a small subset of postoperative spine patients were included in this study, thus the results may not be widely generalizable to other surgical or acute pain populations. There may be overlap between the psychological and neurological ADEs, including vivid dreams and nightmares. Additionally, nausea and new-onset tachycardia are known side effects of morphine, making it difficult to establish an association with ketamine versus morphine. Lastly, our institution allows for ketamine infusions with a maximum dose of 0.06 mg/kg/hr, which may limit generalizability to other institutions.
Conclusion
The data suggest that postoperative spine surgery patients receiving ketamine infusions with a PCA bolus and as-needed parenteral opioids had a lower incidence of ADEs when compared to patients receiving combined opioid and ketamine PCAs. Although evidence is currently limited on the benefit of intravenous ketamine infusion with PCA demand bolus as the sole analgesic for perioperative pain, this study supports the use of ketamine infusion with PCA bolus combined with parenteral opioids.4 This study adds to the existing body of literature to continue delineating ketamine’s safety and efficacy profiles in perioperative medicine.
Acknowledgments
The authors would like to thank Keith Siegel, operations analyst at Cedars-Sinai Pain Center, for all the statistical analyses, and Dr Sharon Nessim, DrPH, former staff statistician at Cedars-Sinai Medical Center (Los Angeles, CA, USA) for her review and suggestions regarding the formatting of the results. Collaborators for this study are Sharon Nessim, DrPH, and Keith Siegel.
Funding
No funding was provided for this retrospective analysis.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cohen SP, Bhatia A, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for chronic pain from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):521–546. doi:10.1097/AAP.0000000000000808
2. Gorlin AW, Rosenfeld DM, Ramakrishna H. Intravenous sub-anesthetic ketamine for perioperative analgesia. J Anaesthesiol Clin Pharmacol. 2016;32(2):160–167. doi:10.4103/0970-9185.182085
3. Porter SB, McClain RL, Howe BL, et al. Perioperative ketamine for acute postoperative analgesia: the Mayo Clinic-Florida experience. J Perianesth Nurs. 2015;30(3):189–195. doi:10.1016/j.jopan.2015.01.010
4. Schwenk ES, Viscusi ER, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):456–466. doi:10.1097/AAP.0000000000000806
5. Pendi A, Field R, Farhan SD, Eichler M, Bederman SS. Perioperative ketamine for analgesia in spine surgery: a meta-analysis of randomized controlled trials. Spine. 2018;43(5):E299–E307. doi:10.1097/BRS.0000000000002318
6. Loftus RW, Yeager MP, Clark JA, et al. Intraoperative ketamine reduces perioperative opiate consumption in opiate-dependent patients with chronic back pain undergoing back surgery. Anesthesiology. 2010;113(3):639–646. doi:10.1097/ALN.0b013e3181e90914
7. Jouguelet-Lacoste J, La CL, Schilling D, Chelly JE. The use of intravenous infusion or single dose of low-dose ketamine for postoperative analgesia: a review of the current literature. Pain Med. 2015;16(2):383–403. doi:10.1111/pme.12619
8. Adriaenssens G, Vermeyen KM, Hoffmann VL, Mertens E, Adriaensen HF. Postoperative analgesia with i.v. patient-controlled morphine: effect of adding ketamine. Br J Anaesth. 1999;83(3):393–396. doi:10.1093/bja/83.3.393
9. Wang L, Johnston B, Kaushal A, Cheng D, Zhu F, Martin J. Ketamine added to morphine or hydromorphone patient-controlled analgesia for acute postoperative pain in adults: a systematic review and meta-analysis of randomized trials. Can J Anaesth. 2016;63(3):311–325. doi:10.1007/s12630-015-0551-4
10. Assouline B, Tramer MR, Kreienbuhl L, Elia N. Benefit and harm of adding ketamine to an opioid in a patient-controlled analgesia device for the control of postoperative pain: systematic review and meta-analyses of randomized controlled trials with trial sequential analyses. Pain. 2016;157(12):2854–2864. doi:10.1097/j.pain.0000000000000705
11. Schwenk ES, Goldberg SF, Patel RD, et al. Adverse drug effects and preoperative medication factors related to perioperative low-dose ketamine infusions. Reg Anesth Pain Med. 2016;41(4):482–487. doi:10.1097/AAP.0000000000000416
12. Gil LV, Mazzeffi MA, Cai Y, McLeod WW, Porter SB. Reasons for discontinuation of acute postoperative pain ketamine infusions: a retrospective case-control study. Pain Pract. 2021;21(7):759–765. doi:10.1111/papr.13012
13. Waelkens P, Alsabbagh E, Sauter A, et al. Pain management after complex spine surgery: a systematic review and procedure-specific postoperative pain management recommendations. Eur J Anaesthesiol. 2021;38(9):985–994. doi:10.1097/EJA.0000000000001448
14. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. 2015;156(6):1003–1007. doi:10.1097/j.pain.0000000000000160
15. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain - United States, 2016. MMWR Recomm Rep. 2016;65(1):1–49. doi:10.15585/mmwr.rr6501e1
16. Laskowski K, Stirling A, McKay WP, Lim HJ. A systematic review of intravenous ketamine for postoperative analgesia. Can J Anaesth. 2011;58(10):911–923. doi:10.1007/s12630-011-9560-0
17. Avidan MS, Maybrier HR, Abdallah AB, et al. Intraoperative ketamine for prevention of postoperative delirium or pain after major surgery in older adults: an international, multicentre, double-blind, randomised clinical trial. Lancet. 2017;390(10091):267–275. doi:10.1016/S0140-6736(17)31467-8
18. Michelet P, Guervilly C, Helaine A, et al. Adding ketamine to morphine for patient-controlled analgesia after thoracic surgery: influence on morphine consumption, respiratory function, and nocturnal desaturation. Br J Anaesth. 2007;99(3):396–403. doi:10.1093/bja/aem168
19. Dahi-Taleghani M, Fazli B, Ghasemi M, Vosoughian M, Dabbagh A. Effect of intravenous patient controlled ketamine analgesia on postoperative pain in opium abusers. Anesth Pain Med. 2014;4(1):e14129. doi:10.5812/aapm.14129
20. Nielsen RV, Fomsgaard JS, Siegel H, et al. Intraoperative ketamine reduces immediate postoperative opioid consumption after spinal fusion surgery in chronic pain patients with opioid dependency: a randomized, blinded trial. Pain. 2017;158(3):463–470. doi:10.1097/j.pain.0000000000000782
21. Sveticic G, Eichenberger U, Curatolo M. Safety of mixture of morphine with ketamine for postoperative patient-controlled analgesia: an audit with 1026 patients. Acta Anaesthesiol Scand. 2005;49(6):870–875. doi:10.1111/j.1399-6576.2005.00740.x
22. Subramaniam K, Akhouri V, Glazer PA, et al. Intra- and postoperative very low dose intravenous ketamine infusion does not increase pain relief after major spine surgery in patients with preoperative narcotic analgesic intake. Pain Med. 2011;12(8):1276–1283. doi:10.1111/j.1526-4637.2011.01144.x
23. Stoker AD, Rosenfeld DM, Buras MR, Alvord JM, Gorlin AW. Evaluation of clinical factors associated with adverse drug events in patients receiving sub-anesthetic ketamine infusions. J Pain Res. 2019;12:3413–3421. doi:10.2147/JPR.S217005
24. Rasmussen KG. Psychiatric side effects of ketamine in hospitalized medical patients administered subanesthetic doses for pain control. Acta Neuropsychiatr. 2014;26(4):230–233. doi:10.1017/neu.2013.61
25. Lin J, Figuerado Y, Montgomery A, et al. Efficacy of ketamine for initial control of acute agitation in the emergency department: a randomized study. Am J Emerg Med. 2021;44:306–311. doi:10.1016/j.ajem.2020.04.013
26. Blake DW, Korner PI. Role of baroreceptor reflexes in the hemodynamic and heart rate responses to althesin, ketamine and thiopentone anesthesia. J Auton Nerv Syst. 1981;3(1):55–70. doi:10.1016/0165-1838(81)90030-8
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.