")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Advancing Virtual at-Home Care for Community Health Center Patients Using Patient Self-Care Tools, Technology, and Education
Authors Modica C , Lewis JH, Bay RC
Received 10 October 2023
Accepted for publication 22 January 2024
Published 2 February 2024 Volume 2024:17 Pages 521—531
DOI https://doi.org/10.2147/JMDH.S443973
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Cheryl Modica,1 Joy H Lewis,2 R Curtis Bay3
1National Association of Community Health Centers, Bethesda, MD, USA; 2Department of Medicine and Public Health, A.T. Still University, School of Osteopathic Medicine, Mesa, AZ, USA; 3Department of Interdisciplinary Health Sciences, Arizona School of Health Sciences, A.T. Still University, Mesa, AZ, USA
Correspondence: Cheryl Modica, National Association of Community Health Centers, Inc, 7501 Wisconsin Avenue, Suite 1100W, Bethesda, MD, 20814, USA, Tel +1 301 310 2250, Email [email protected]
Introduction: Health centers are community-based, patient directed primary care providers that offer accessible, high-quality primary care within medically underserved communities. Screening for cancer and managing complex chronic conditions such as diabetes, hypertension, obesity, and depression are vital services for the vulnerable populations seen by community health centers. Delivering care for complex chronic conditions and preventive services using virtual models that integrate self-care tools and technology is an important approach to increasing access for hard-to-reach patients served by health centers.
Objective: This study aimed to explore the use of a virtual care model, applied using a systems approach and patient-driven tools and technology, on the performance of clinical and patient experience measures.
Methods: A virtual care model, applied using a systems approach offered by the Value Transformation Framework (VTF), was combined with self-care tools and technology in twenty health centers across 17 states to drive improvement efforts. Changes in clinical measures and patient experience were compared.
Results: A total of 385 patients were enrolled and 270 (70.1%) completed a baseline visit and at least four virtual visits during the six-month intervention period. Statistically significant improvements were seen in measures for HbA1c, systolic and diastolic blood pressure, and bodyweight. Among the 270 who completed the baseline and at least 4 virtual visits, the percentage up-to-date for colorectal cancer screening increased from 113/270 (41.9%) to 169/270 (62.6%) after six months, p< 0.001, a 20.7% increase. Patients completing the baseline visit and at least 4 virtual visits reported a 10.7% decrease in depression and increased satisfaction with virtual care visits compared to in-person visits (p< 0.001).
Conclusion: Health centers applying the Value Transformation Framework’s organizing framework to the use of virtual care models together with patient self-care tools, technology, and education, had improvements in measures for chronic and preventive conditions and patient experience.
Plain Language Summary: The Value Transformation Framework (VTF) was designed by the lead author to serve as an organizing framework for health center systems change and advancement toward the Quintuple Aim: improved health outcomes, improved patient experiences, improved staff experiences, reduced costs, and equity. When applied in the health care setting, the VTF translates research, evidence-based solutions, and promising practices into clear and practical steps that health centers can use to achieve value-driven care. In this paper, the authors report on results from a study where the VTF’s organizing approach was combined with evidence-based virtual care models supported by patient self-care tools, technology, and education with improvements seen in measures for colorectal cancer screening, hypertension control, diabetes control, weight, patient reported depression, and patient experience. The action steps taken by health centers participating in this quality improvement project can be replicated by other health centers.
The impact of colon cancer, hypertension, diabetes, obesity, and depression, particularly among health center patients, is substantial. Identifying strategies to change health center systems in ways that improve performance is critically important. The authors demonstrated that implementing the VTF can provide health centers with a practical and actionable approach to health center systems change to achieve significant improvements in clinical measurements, patient-reported depression, and patient experience with care.
Keywords: vulnerable populations, colorectal cancer screening, hemoglobin A1c, obesity, depression, patient experience
A Letter to the Editor has been published for this article.
A Response to Letter by Prof. Dr. Masriadi has been published for this article.
Introduction
Many primary care services do not require an in-person visit. Care, services, and referrals can often be completed by telephone or other remote methods. The COVID-19 pandemic, combined with rapid advances in technology, drove creative technological innovations in health care delivery.
Within the United States (US) there is a network of nearly 1400 health centers with over 14,000 delivery sites where primary care services are provided to more than 30 million patients, many of whom are uninsured, living below the poverty line, or experiencing other challenges in accessing care.1 This network of safety-net primary care providers is hereafter referred to as “health centers”. Health centers are community-based health care providers that offer primary care to medically underserved populations regardless of their ability to pay. They are funded, in part, through the Health Resources and Services Administration (HRSA) Health Center Program.
Studies demonstrate that health centers deliver care that meets or exceeds national practice standards at lower costs.2,3 Health centers are estimated to save the US health care system $24 billion annually.2 The Community Health Center Program has its roots in President Lyndon B. Johnson’s war on poverty and today continues to serve low income, uninsured, and underinsured populations with attention to social drivers of health and equity.
In 2022, approximately 28% of health center patients had hypertension and 16% of all health center patients were individuals with diabetes.1 During that same period, the prevalence of obesity and depression among health center patients was 27% and 9%, respectively.1 Managing chronic conditions and addressing preventive screenings is critical to improved health outcomes for health center patients.
The use of telehealth to provide care and services has increased for a host of reasons, including interest in the potential to improve access, enhance efficiency, and reduce cost. The term “telehealth” describes any service that allows patients to access care from a provider remotely.4 Remote patient monitoring is an approach to telehealth in which patients self-measure health data and report the data from a non-clinical setting (often their homes) to their healthcare provider.4 Remote patient monitoring is particularly well suited for screening programs and for the management of chronic conditions such as diabetes and hypertension because it can reduce the cost and burden of in-person clinic visits.5–8
Research is emerging that suggests telephone and video visits may be a preferred method of health care delivery for some patients and may have a significant effect on advancing health care in the future.9,10 Patients report being satisfied with the use of telemedicine and remote home monitoring for the management of chronic conditions.5,9,11,12
Colorectal cancer screening (CRCS) and follow-up care for diabetes and hypertension are three areas of clinical care that could dramatically benefit from the rapid advance in telehealth and virtual care. In 2020, 40.1% of health center patients had up-to date CRCS compared to 69.7% of the general population.1,13 CRCS can be conducted remotely by mail using fecal tests, and studies have found that sending tests by mail increases uptake of CRCS.14–16 One study of at-home CRCS implementation in health centers in Kentucky found increased provider willingness to utilize at-home CRCS due to disruptions to normal care caused by the COVID-19 pandemic.17
While many patients prefer telehealth for its convenience, reduced travel time, reduced wait time, and lower cost,18 telehealth may not be warranted in all situations. Limitations or patient concerns regarding telephone and/or virtual (video) visits have been reported.19,20 Despite the growing literature on the pros and cons of the use of telehealth in health care, little of this research explores the use of telehealth and remote patient monitoring in underserved populations.11
This study sought to explore the use of virtual care delivery models, using the VTF systems approach model, and self-care tools, technology, and patient education. The goal was to evaluate changes in clinical measures (colorectal cancer screening, diabetes control, hypertension control, depression, and weight) and patient experience. While the project was conceived prior to the COVID-19 pandemic, it was implemented during the height of the public health emergency. The timing was fortuitous in that health centers, along with other health care organizations around the globe, were looking to quickly adopt new virtual models of care and new and expanded uses of technology. This was a time when many patients chose to stay home rather than seek in-person health care and access to food, exercise, or other factors supporting healthy lifestyles became more challenging. This was a period of unprecedented expansion in technology, not only in health care but in all aspects of life, work, and play.
Value Transformation Framework (VTF)
This project was guided by a whole-person, systems approach to change. A systems approach allows for engagement by staff at all levels of the organization, directing change in multiple parts of the overall health center system at the same time. The Value Transformation Framework (VTF), designed by the lead author, is an organizing framework for making changes and improvements across a system. It focuses on fifteen areas of change organized into three main domains: infrastructure, care delivery, and people systems. By working across multiple areas within a health system at the same time, changes can take place that drive improved health center performance and achievement of the Quintuple Aim: improved health outcomes, improved patient experiences, improved staff experiences, reduced costs, and equity [Figure 1].21–25 The VTF has been shown to be an effective framework to guide health center systems change.21–23,25
 |
Figure 1 Value Transformation Framework (VTF). |
This paper discusses how the VTF’s organizing framework guided a virtual care model that, when combined with patient self-care tools, technology, and education, delivered evidence-based care and saw improvements to measures of clinical performance and patient experience in the health center setting.
Methods
Study Design
This study was conducted in a cohort of twenty US health centers from September 2020 to June 2021. The study combined (1) a systems approach to change using the VTF; (2) new virtual care models; and (3) patient self-care tools, technology, and education referred to as “Patient Care Kits” to support evidenced-based interventions and tracking of clinical measures. The results from the new virtual care model were investigated to determine if improvements in performance of clinical and patient experience measures could be observed. These measures included CRCS, hypertension control, diabetes control, depression screening, weight, and patient experience.
Study Participants
Participating health centers were recruited through an open application process to health centers nationally. Any health center or health center look-alike (organizations who meet federal health center requirements but do not receive federal award funding) who operated a care management program was eligible to apply. Selecting health centers with existing care management programs allowed for a quick program start-up and brought consistency across health centers through already sufficient staffing and workflows to support the engagement and follow-up of patients with multiple chronic conditions. A total of seventy interested health centers applied. Based on available project resources, twenty health centers were selected for participation. Selection was conducted by an internal NACHC review panel based on the following criteria: the health center’s proposed strategy to design a new care delivery model with virtual care processes and patient self-care tools and technology that would be integrated with the health center’s current workflow and model of care, a demonstrated risk stratification process, the strength of the proposed strategy to distribute self-care tools and technology to patients, and the current and proposed strategies to engage patients in the use of self-care tools, technology, and virtual visits.
Patient recruitment was conducted by health center staff using a purposive sampling approach, through the deliberate selection of participants based on inclusion criteria. The goal was to recruit 20 participants per health center and enroll 400 patients in the overall program. To be eligible for participation in the study, participants had to be 50–75 years old with two or more chronic conditions, including diabetes.
Ethical Considerations
This project was submitted to the AT Still University (ATSU Arizona) Institutional Review Board (IRB) which deemed it to be a quality improvement project and classified it as “non-jurisdiction”. The IRB application number was 220–238.
Study Setting
The 20 selected health centers represented 17 states. The state and regional primary care associations (PCAs) and health center controlled networks (HCCNs) that offer technical assistance, training, and other technology and operational support to health centers in their state or network, were invited to join program calls and activities.
Intervention
This project, titled “Leading Change: Transforming At-Home Care” (or “Leading Change”), provided guidance and coaching to implement new virtual models of care, which included assistance in developing workflows, materials to support staff training, and patient instructional and educational materials. The project provided one “Patient Care Kit” (Kit) for each patient enrolled in the virtual care program. The Kits provided participating patients with a uniform set of tools, technology, and educational materials. Kit tools included a home CRCS (stool) test and home blood sugar (A1c) test. Technology included a blood pressure monitor, thermometer, and digital scale. In addition, each Kit included patient educational and instructional materials (available in five languages), and logs and recording tools. Instructions and recording logs were also provided to health center staff. The target patient population for the project was individuals 50–75 years of age with two or more chronic conditions, one of which was diabetes.
The project was implemented over a ten-month period which included a six-month intervention window that incorporated monthly patient-care team exchanges and virtual care visits. During the intervention period, the twenty health centers deployed new models of care that delivered monthly virtual care services. Live touchpoints were added if/when deemed necessary by the patient, care team, or provider.
Following the selection of participating health centers in September 2020, NACHC held an orientation call to welcome the cohort to the project and acquaint them with project expectations and timelines. Each health center identified a staff member to serve as project lead and point of contact with the NACHC team. Participating health centers were guided in project start-up activities including strategies for leadership engagement, communicating the initiative to staff within the health center, preparing the health center to receive Patient Care Kits, and identifying eligible patients. A virtual project launch meeting was held in October of 2020 during which the Principal Investigator (PI) presented the project plan, improvement approach using the VTF, and reporting requirements. Following orientation and launch calls, the NACHC team held monthly project calls that included all participating health centers. These calls provided training and technical assistance, troubleshooting, sharing of best practices, and peer exchange. In addition to monthly project calls, each participant health center was paired with a NACHC coach who provided additional one-on-one guidance and support throughout the project. A one-on-one coaching call was held with each site approximately half-way through the intervention period with additional calls taking place as needed.
NACHC’s project team guided care team leads at each health center through a four-step transformation process over the course of the ten-month Leading Change project. These steps included:
- Step 1: Lay the Groundwork
- Step 2: Launch
- Step 3: Implement
- Step 4: Project Close
Step 1 Lay the Groundwork
Health centers assessed organizational readiness for systems change using a VTF Assessment tool. This tool, developed as a companion to the VTF,24 measures health center readiness and progress in fifteen areas of health systems change that correspond with the VTF. During this phase, health centers also defined project goals and created workflows to implement the improvement intervention. The intervention consisted of:
- Monthly virtual care visits for six months
- Depression screening using the PHQ-2 at baseline and last virtual visit26
- Social risk assessment using questions from the NACHC PRAPARE® tool27
- Patient experience survey at baseline and last virtual visit
- Live touchpoints as determined by the patient, care team, or provider
- Provision of patient self-care tools and technology, referred to as a “Patient Care Kit”
- Patient education and instruction in preventive health screening and use of the tools in the Kit
Step 2 Launch
Health centers distributed Patient Care Kits and conducted an initial “baseline” health care visit with patients. Baseline visits were conducted in-person at the health center or at the patient’s home, with a few performed virtually as requested by the patient. Participating health centers collected a uniform set of data at the baseline visit including clinical, social risk (using a subset of NACHC’s PRAPARE® tool), depression screening (PHQ-2), and patient experience measures. These same measurements were collected again at 6 months, the close of the intervention period. Patients were also provided instructions and training regarding how to use the tools and technology and how to report measurements over the course of the program.
Step 3 Implement
After the baseline visit, health centers conducted at least monthly video visits and/or checks-in for the duration of the project. Additional virtual and/or in-person contact occurred if requested by the patient, care team, or provider. Health centers implemented workflows and processes to support virtual check-ins and patients’ use of self-care tools and technology during the 6-month implementation phase. Throughout the project period, health center staff had access to a NACHC-managed online platform that served as a central repository of project information, educational tools, and resources. To support the diverse populations served by the 20 participating organizations, patient educational materials were translated into Spanish, Karen, Lao, and Vietnamese. Educational and instructional materials were also provided to staff.
Step 4 Project Close
Health centers completed a final project-related patient visit at the close of the six-month intervention window to gather final measurements, including post-data for clinical measures, social risk, depression screening, and patient experience.
Data Collection
Health centers collected patient data using their routine primary care practices and then reported de-identified clinical, social risk, and patient experience data to NACHC monthly. No patient-identifying or personal information was transmitted to the NACHC team, thus there was no risk that private medical information could be linked directly to an individual person. While health centers report Uniform Data Systems (UDS) metrics annually as part of federally required reporting to the Health Resources and Services Administration (HRSA),1 health centers participating in this project tracked data monthly. To ensure that data were valid, the project team provided coaching and support in the collection and reporting of measures.
Analysis
Summary statistics including means (standard deviations) and counts (percentages) were calculated, as appropriate. Dependent-samples t-tests were used to evaluate change in clinical measurements and ratings of care received from baseline to six months. McNemar paired-sample proportions tests were used to evaluate changes in categorical data. An alpha of 0.05 was used as the criterion for statistical significance. SPSS ver. 28 (IBM Corp., Armonk NY) was used for statistical analysis.
Results
A total of 385 patients were enrolled in the project. All patients received a Patient Care Kit, educational material, and instruction in how to use Kit tools and technology. The majority, 270 (70.1%), of the patients who completed a baseline visit and received a Kit and instruction also completed at least four virtual visits. See Table 1.
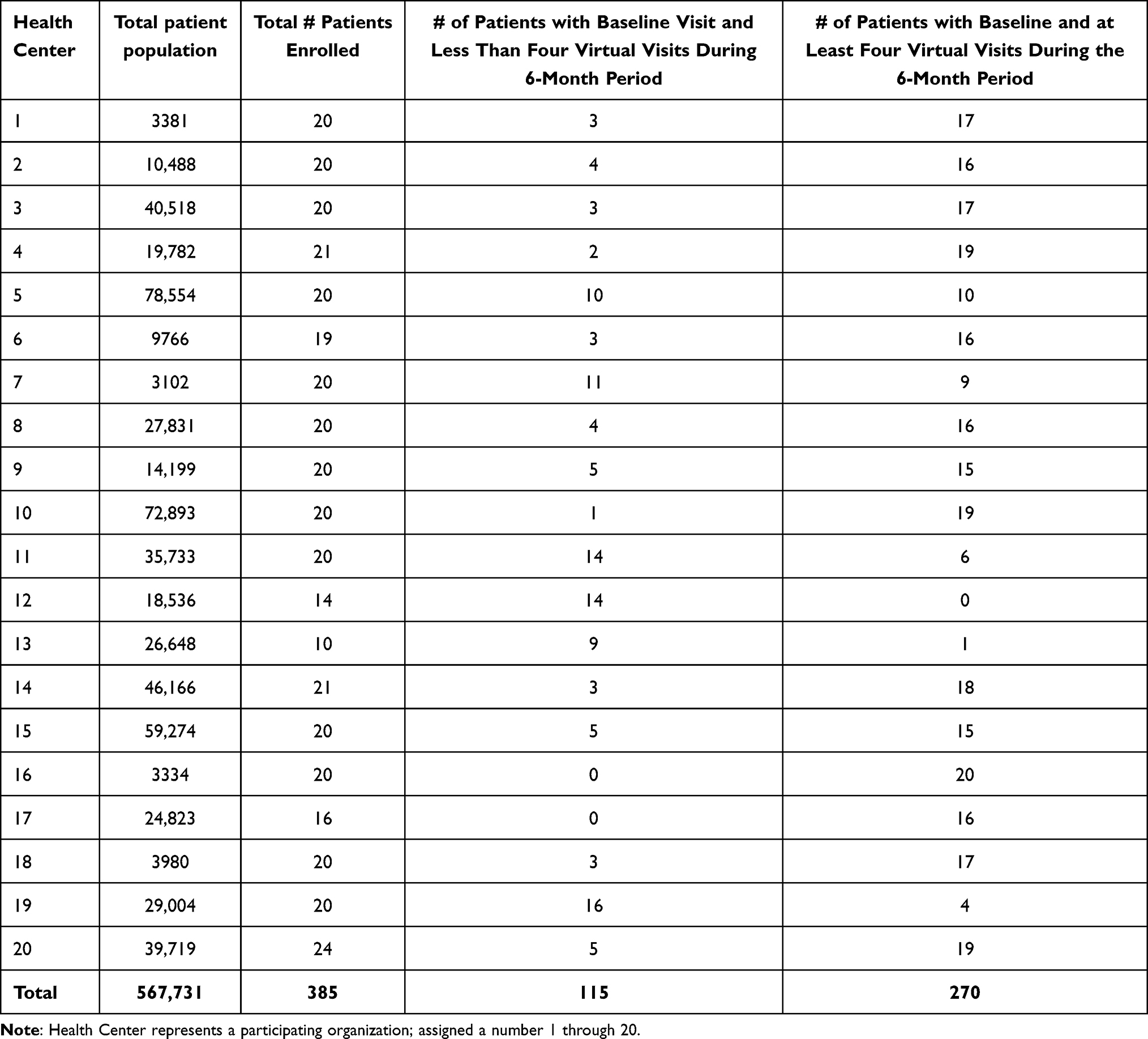 |
Table 1 Patient Participation, by Health Center |
Project participants (Table 2) included a higher percentage of uninsured (22%) as compared to the national health center average (12%).
 |
Table 2 Participant Insurance Status |
Table 3 highlights the higher proportion of White, and Non-Hispanic or Latino/a participants in the patient cohort as compared to the national average.
 |
Table 3 Participant Race/Ethnicity (% of Total Patients Rounded to the Nearest Integer) |
There were statistically significant improvements in measures for HbA1c, systolic and diastolic blood pressure, and bodyweight among the participants over the six-month intervention period. Mean changes in HbA1c of −0.63 (p<0.001), systolic blood pressure of −3.68 (p=0.002); diastolic blood pressure of −2.28 (p=0.002); and weight of −2.50 (p=0.003) for patients remaining in the study for the full six months are noted in Table 4.
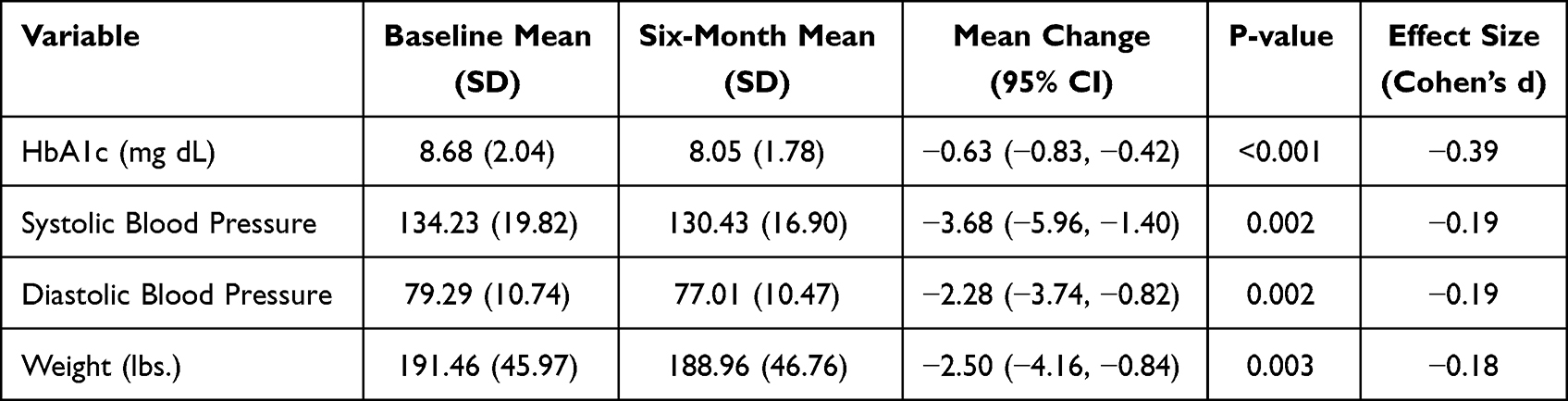 |
Table 4 Changes in Clinical Indicators During the Intervention |
Table 5 highlights CRCS levels among all patients and those who completed the baseline visit and at least 4 virtual care visits. Among all patients enrolled, 148/385 (38.4%) had up-to-date CRCS at baseline per HRSA UDS guidelines.1 At six months, 190/385 (49.4) had appropriate CRCS, p=0.003. Among the 270 who completed the baseline and at least 4 virtual care visits, the percentage up-to-date for CRCS increased from 113/270 (41.9%) at initiation of the study to 169/270 (62.6%) at six months, p=<0.001, a 20.7% increase in CRCS. Eighteen (18) of the 20 participating health centers achieved a higher rate of CRCS for patients in their study population than was reported in their 2020 UDS data.
 |
Table 5 Changes in Up-to-Date Colorectal Cancer Screening During the Intervention |
Among all patients, 115 completed the baseline visit but did not have at least four virtual visits. Thirty-five (35) of these 115 patients (30.4%) had appropriate CRCS at baseline. Among the 64 of those 115 patients who were not up-to-date with their CRCS at baseline, 14/64 (21.9%) were brought up-to-date in CRCS during the six-month intervention period of this study.
Counts of virtual visits and dropout rates did not differ significantly across race (African American vs Caucasian), ethnicity (Hispanic vs non-Hispanic), sex of patient, or availability of insurance. Patient age was not associated with the probability of discontinuing virtual visits during the six month intervention window.
Health center staff administered a depression screening tool (PHQ-2) and patient experience survey with project participants at baseline and again at the close of the intervention. Results are shown in Table 6. Among 262 patients who completed the depression screen (PHQ-2) at baseline and at project close, 91 (34.7%) reported being depressed at baseline, and 63 (24.0%) reported being depressed at six months, p<0.001. This represents an 11% decrease in reports of depression during the project period. The patient experience survey included a question that asked patients about their experience with virtual visits relative to in-person visits, with most of the patients having experienced telephone and/or virtual visits with their care team in the months preceding this project due to the pandemic. Mean [SD] responses to the question, “How would you rate the care you receive at virtual visits with your provider as compared to in-person visits in the health center with your provider?” are shown in Table 6 with higher ratings (greater satisfaction) at the final visit (3.95 [1.83]) than baseline (3.43 [0.92]), p<0.001.
 |
Table 6 Changes in Depression and Patient Experience Scores (262 Patients Completed the Depression Screen (PHQ-2) at Baseline and Six Months) |
Discussion
In this project, application of the Value Transformation Framework’s (VTF) organizing approach combined with new models of virtual care and tools and technology offered through Patient Care Kits showed statistically significant improvements across multiple clinical and patient experience measures. Improvements were seen in clinical measures for cancer screening, hypertension control, diabetes control, weight, depression, and patient satisfaction with virtual visits. These improvements were seen despite the short duration of the intervention window and could potentially increase if the intervention were applied over a longer period of time.
The reporting of clinical measures was familiar to health centers and consistent with the methods health centers used for reporting data.1 NACHC provided coaching and support throughout the project. The improvements noted in measurements may be because patients had a high level of engagement and “touch” with their care team during this program, both virtually and in-person. This greater level of communication and follow-up by the care team may have contributed to improved reports of well-being.
Program participants included a higher percentage of uninsured than the national health center average, showing promise for the use of virtual care models with this target population and other traditionally underserved, at-risk patient populations receiving care through community health centers. While the gains in recalcitrant clinical measures are promising, additional interventions and/or additional time may be needed to realize a greater magnitude of change.
These findings support earlier work on the potential impact of the Value Transformation Framework as an organizing approach for improving health outcomes,21–25 in this case focused on a virtual model of care delivery using patient self-care tools, technology, and education. This systems-approach may help advance key Quintuple Aim goals (improved health outcomes, improved patient experiences, improved staff experiences, reduced costs, and equity).28 The improvements noted in clinical measures and patient well-being and experience are encouraging and show promise for spread and scale to other health centers nationally.
Limitations
The patients served by this project had access to technology to support the use of telehealth. We recognize that there are communities where connectivity and access to technology is more limited. The project, however, is unique in that it used a standardized framework for systems change (the VTF) delivered through a structured project implementation approach, while allowing each participant health center to operationalize a virtual care model that fit their organizational culture, quality improvement resources, delivery tactics, and staffing resources. The overall project strategy, therefore, can be replicated.
While 99 patients did not complete at least 4 virtual visits in addition to the baseline visit, approximately half of these patients (49) completed CRCS prior to the end of the study. We do not have information regarding the reasons they ended engagement with the project, but these patients may have felt they received needed care or completed measures for the areas that were the focus of the project. This is an area the authors plan to evaluate in more detail in future work.
Data were self-reported by health centers using methods outlined in the HRSA UDS reporting requirements. The validity of data collected was managed with routine check-ins by the project team regarding health center data collection and validation.
Conclusion
Since the onset of the COVID-19 pandemic, health centers have been shifting to more virtual models of care delivery. The need to improve access, engage patients, and deliver efficient, coordinated, and high-quality care is imperative. Screening for preventive conditions such as colorectal cancer and managing complex and chronic conditions such as diabetes and hypertension, are vital in underserved and vulnerable communities. Virtual health services using self-care tools and technology is an important model to increase access to care for hard-to-reach patients and shows great promise within health centers. Findings from the Leading Change: Delivering At-Home Care initiative demonstrate that when health centers apply a systems approach using the Value Transformation Framework, combined with evidence-based virtual care, patient self-care tools, technology and education, measures of clinical performance and patient experience can improve.
Acknowledgments
The authors thank the following health centers that were supported in this project by the Centers for Disease Control and Prevention (CDC) of US Department of Health and Human Services (HHS) as part of Cooperative Agreement 6 NU380T000223-04-02: Accordia Health (AL), Alliance Community Healthcare (NJ), CareSouth Carolina (SC), East Bay Community Action Program (RI), Kaniksu Community Health (ID), Oak Orchard Health (NY), OneWorld Community Health Center (NE), Shawnee Health Services (IL), The Wright Center for Community Health (PA), and White House Clinics (KY).
The authors thank the following health centers that were supported in this project by the Health Resources and Services Administration of the HHS as part of an award totaling $7,287,500 with 0% funded with non-governmental sources: Charter Oak Health Center (CT), Comprehensive Health Center-Phoenix (AZ), International Community Health Services (WA), Kintegra Health (NC), Lone Star Circle of Care (TX), Native American Health Center (CA), Family Health Matters Community Health Center (CA), Open Door Family Medical Center (NY), Wahiawa Health (HI), and Zufall Health Center (NJ).
Disclosure
Cheryl Modica has a copyright registration for the Value Transformation Framework. Joy H. Lewis and R. Curtis Bay report that they received grants from NACHC during the conduct of this project. The authors report no other conflicts of interest in this work.
References
1. National Health Center Program Uniform Data System (UDS) Awardee Data. Available from: https://data.hrsa.gov/tools/data-reporting/program-data/national.
2. Goldman LE, Chu PW, Tran H, Stafford RS. Community health centers and private practice performance on ambulatory care resources. Am J Prev Med. 2012;43(2):142–149. doi:10.1016/j.amepre.2012.02.033
3. Ku LC, Richard P, Dor A, Tan E, Shin P, Rosenbaum SJ. Using Primary Care to Bend the Curve: Estimating the Impact of a Health Center Expansion on Health Care Costs (Geiger Gibson/RCHN Community Health Foundation Research Collaborative Policy Research Brief No 14). Washington, D.C.: George Washington University, School of Public Health and Health Services, Department of Health Policy; 2009.
4. Telehealth Basics. ATA. Available from: https://www.americantelemed.org/resource/why-telemedicine/.
5. Lee PA, Greenfield G, Pappas Y. The impact of telehealth remote patient monitoring on glycemic control in type 2 diabetes: a systematic review and meta-analysis of systematic reviews of randomized controlled trials. BMC Health Serv Res. 2018;18(1):495. doi:10.1186/s12913-018-3274-8
6. Liu K, Xie Z, Or CK. Effectiveness of mobile app-assisted self-care interventions for improving patient outcomes in type 2 diabetes and/or hypertension: systematic review and meta-analysis of randomized controlled trials. JMIR MHealth UHealth. 2020;8(8):e15779. doi:10.2196/15779
7. Meador M, Hannan J, Roy D, et al. Accelerating use of self-measured blood pressure monitoring (SMBP) through clinical-community care models. J Community Health. 2021;46(1):127–138. doi:10.1007/s10900-020-00858.0
8. Roy D, Meador M, Sasu N, Whelihan K, Lewis JH. Are community health center patients interested in self-measured blood pressure monitoring (SMBP) – and can they do it? Integr Blood Press Control. 2021;14:19–29. doi:10.2147/IBPC.S285007
9. Ebbert JO, Ramar P, Tulledge-Scheitel SM, et al. Patient preferences for telehealth services in a large multispecialty practice. J Telemed Telecare. 2023;29(4):298–303. doi:10.1177/1357633X20980302
10. Doraiswamy S, Abraham A, Mamtani R, Cheema S. Use of telehealth during the COVID-19 pandemic: scoping review. J Med Internet Res. 2020;22(12):e24087. doi:10.2196/24087
11. Sim R, Lee SWH. Patient preference and satisfaction with the use of telemedicine for glycemic control in patients with type 2 diabetes: a review. Patient Prefer Adherence. 2021;15:283–298. doi:10.2147/PPA.S271449
12. Finn MTM, Brown HR, Friedman ER, Kelly AG, Hansen K. Preference for telehealth sustained over three months at an outpatient center for integrative medicine. Glob Adv Health Med. 2021;10:2164956121997361. doi:10.1177/2164956121997361
13. Centers for Disease Control and Prevention (CDC). Behavioral risk factor surveillance system survey data. Atlanta, Georgia: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. Available from: https://www.cdc.gov/brfss/index.html.
14. Kemper KE, Glaze BL, Eastman CL, et al. Effectiveness and cost of multilayered colorectal cancer screening promotion interventions at federally qualified health centers in Washington state. Cancer. 2018;124(21):4121–4129. doi:10.1002/cncr.31693
15. Wolf AMD, Fontham ETH, Church TR, et al. Colorectal cancer screening for average-risk adults: 2018 guideline update from the American Cancer Society. CA Cancer J Clin. 2018;68(4):250–281. doi:10.3322/caac.21457
16. Singal AG, Gupta S, Tiro JA, et al. Outreach invitations for FIT and colonoscopy improve colorectal cancer screening rates: a randomized controlled trial in a safety-net health system. Cancer. 2016;122(3):456–463. doi:10.1002/cncr.29770
17. Kruse-Diehr AJ, Dignan M, Cromo M, et al. Building cancer prevention and control research capacity in rural Appalachian Kentucky primary care clinics during COVID-19: development and adaptation of a multilevel colorectal cancer screening project. J Cancer Educ off J Am Assoc Cancer Educ. 2022;37(5):1407–1413. doi:10.1007/s13187-021-01972-w
18. Rasmussen B, Perry R, Hickey M, et al. Patient preferences using telehealth during the COVID-19 pandemic in four Victorian tertiary hospital services. Intern Med J. 2022;52(5):763–769. doi:10.1111/imj.15726
19. Gordon HS, Solanki P, Bokhour BG, Gopal RK. “I’m not feeling like I’m part of the conversation” patients’ perspectives on communicating in clinical video telehealth visits. J Gen Intern Med. 2020;35(6):1751–1758. doi:10.1007/s11606-020-05673-w
20. Oikonomidi T, Ravaud P, Cosson E, Montori V, Tran VT. Evaluation of patient willingness to adopt remote digital monitoring for diabetes management. JAMA Network Open. 2021;4(1):e2033115. doi:10.1001/jamanetworkopen.2020.33115
21. Modica C, Bay C, Lewis JH, Silva C. Applying the value transformation framework in federally qualified health centers to increase clinical measures performance. J Healthc Qual. 2022;44(4):185–193. doi:10.1097/JHQ.0000000000000340
22. Whelihan K, Modica C, Bay RC, Lewis JH. Patient and staff satisfaction and experience while transforming health center systems. Risk Manag Healthc Policy. 2022;15:2115–2124. doi:10.2147/RMHP.S375983
23. Modica C, Lewis JH, Bay RC. The value transformation framework: applied to diabetes control in federally qualified health centers. J Multidiscip Healthc. 2021;14:3005–3014. doi:10.2147/JMDH.S284885
24. Modica C. The value transformation framework: an approach to value-based care in federally qualified health centers. J Healthc Quality. 2020;42(2):106–112. doi:10.1097/JHQ.0000000000000239
25. Modica C, Lewis JH, Bay C. Colorectal cancer: applying the value transformation framework to increase the percent of patient receiving screening in federally qualified health centers. Prev Med Rep. 2019;15:1–7. doi:10.1016/j.pmedr.2019.100894
26. Kroenke K, Spitzer R, Williams J. The patient health questionnaire-2: validity of a two-item depression screener. Med Care. 2003;41(11):1284–1292. doi:10.1097/01.MLR.0000093487.78664.3C
27. National Association of Community Health Centers (NACHC), and Association of Asian Pacific Community Health Organizations (AAPCHO). PRAPARE® Screening Tool. Available from: https://prapare.org/the-prapare-screening-tool/.
28. Nundy S, Cooper LA, Mate KS. The quintuple AIM for health care improvement: a new imperative to advance health equity. JAMA. 2022;327(6):521–522. doi:10.1001/jama.2021.25181
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.