Back to Journals » Drug Design, Development and Therapy » Volume 20
Advancing Daptomycin Precision Dosing Through Evaluation of Published Population Pharmacokinetic Models and Development of a Dosing Tool
Authors Xie X, Qian C, Luque S, Liu L, Chen J, Mendoza CC ![]() , Sorli L, Yuan H, Ma C, Ren L, Xu N, Ju G, Zhu X, Liu X
, Sorli L, Yuan H, Ma C, Ren L, Xu N, Ju G, Zhu X, Liu X ![]()
Received 15 November 2025
Accepted for publication 17 March 2026
Published 27 March 2026 Volume 2026:20 581874
DOI https://doi.org/10.2147/DDDT.S581874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Xi Xie,1,* Cheng Qian,2,* Sonia Luque,3– 5 Li Liu,6 Jiayu Chen,2 Carla Comajuan Mendoza,3,4 Luisa Sorli,3,4 Huamin Yuan,1 Chen Ma,2 Lin Ren,7 Nuo Xu,2 Gehang Ju,8,9 Xiao Zhu,2 Xin Liu2
1Department of Clinical Laboratory, Hunan Prevention and Treatment Institute for Occupational Diseases, Affiliated Prevention and Treatment Institute for Occupational Diseases of University of South China, Changsha, People’s Republic of China; 2Department of Clinical Pharmacy and Pharmacy Administration, School of Pharmaceutical Sciences, Fudan University, Shanghai, People’s Republic of China; 3Infectious Pathology and Antimicrobials Research Group (IPAR), Institute Hospital Del Mar d’Investigacions Mèdiques (IMIM), Barcelona, Spain; 4Pharmacy Department, Hospital del Mar, Barcelona, Spain; 5CIBER of Infectious Diseases (CIBERINFEC CB21/13/0002), Institute of Health Carlos III, Madrid, Spain; 6The Second People’s Hospital of Hunan Province (Brain Hospital of Hunan Province), Changsha, People’s Republic of China; 7Department of Pharmacy, The First Affiliated Hospital of Soochow University, Soochow, People’s Republic of China; 8Institute of Big Data, Central South University, Changsha, People’s Republic of China; 9Hunan Key Laboratory for Bioanalysis of Complex Matrix Samples, Changsha Duxact Biotech Co., Ltd, Changsha, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiao Zhu; Xin Liu, Department of Clinical Pharmacy and Pharmacy Administration, School of Pharmaceutical Sciences, Fudan University, Shanghai, 201203, People’s Republic of China, Email [email protected]; [email protected]
Background: Daptomycin is an important antibiotic against multidrug-resistant Gram-positive infections, but its wide interindividual variability and narrow therapeutic window pose challenges for optimal dosing. Population pharmacokinetic (PopPK) models provide a quantitative framework for precision dosing, yet a systematic evaluation of existing models and their clinical application method remains lacking.
Methods: Model structures, demographic characteristics, and covariate effects were systematically summarized from previously published papers. Predictive performance was compared through simulations in virtual populations with varying renal function. Monte Carlo simulations were performed to evaluate the probability of target attainment (PTA; AUC24h/MIC ≥ 666) and the probability of toxicity (Cmin ≥ 24.3 mg/L). Furthermore, an open-access precision dosing tool was developed based on maximum a posteriori Bayesian estimation using representative model structure and parameters.
Results: Eighteen PopPK studies were included in this analysis. Renal function was the most frequently identified covariate influencing clearance. Model comparisons revealed variability in predicting exposure and PTA. Simulations indicated that patients with impaired renal function face a higher risk of exceeding the toxicity threshold, even at moderate doses. The developed Shiny-based tool enables real-time estimation of AUC and Cmin, integration of therapeutic drug monitoring data, and individualized dose adjustment.
Conclusion: This study provides a comprehensive evaluation of daptomycin PopPK models and translates these findings into a practical precision dosing tool. This work enhances understanding of interindividual variability of daptomycin and offers clinicians a scientifically grounded resource to optimize daptomycin therapy in diverse patient populations.
Keywords: population pharmacokinetic, precision dosing, daptomycin, renal impairment
Introduction
Gram-positive bacteria remain major pathogens responsible for severe infections,1 and the escalating prevalence of antimicrobial resistance has emerged as a critical global health concern, driving both morbidity and healthcare costs. Daptomycin, a cyclic lipopeptide antibiotic, exhibits potent activity against multidrug-resistant Gram-positive organisms, particularly methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Enterococcus (VRE).2,3 Pharmacokinetically, daptomycin shows extensive plasma protein binding (90–93%), a small volume of distribution (about 0.1 L/kg), and predominant renal elimination, with nearly 50% of the dose excreted unchanged in urine.4 Owing to these properties and its rapid and potent concentration-dependent bactericidal activity, daptomycin has been approved for indications such as bacteriaemia, complicated soft tissue infections,5 with commonly recommended doses ranging from 4 to 12 mg/kg. However, this broad dosing range creates clinical uncertainty.6 It may compromise both efficacy and safety, especially in vulnerable patients such as those with renal impairment.7 Thus, the need for precision dosing has become increasingly urgent.
Optimizing daptomycin therapy requires quantitative approaches rather than empirical decision-making. Daptomycin is a concentration-dependent bactericidal agent, with efficacy best correlated to an exposure target of AUC24h/MIC ≥666.8,9 In contrast, toxicity is linked to elevated trough concentrations (Cmin>24.3 mg/L),10 which predispose patients to dose-limiting myopathy. Although therapeutic drug monitoring (TDM) has been recommended for improving the treatment outcomes,11 its practical use is somehow restricted, as it requires multiple steady-state samples, delays timely adjustment, and relies heavily on expert interpretation.12 These limitations hinder real-time dose optimization in daily practice. Previous studies have proposed several strategies to optimize precision dosing of daptomycin, as target exposure attainment has not been consistently achieved. These include TDM-guided dose adjustment, Bayesian forecasting tools such as BestDose13 and Tucuxi14 for individual PK parameter estimation, and nomogram-based dosing strategies have been proposed for specific clinical settings, such as vancomycin-resistant enterococcal infections.15 However, to date, no dedicated pharmacometric platform has been established to comprehensively support model-informed precision dosing of daptomycin.
Model-informed precision dosing (MIPD) has therefore emerged as a promising strategy for individualized pharmacotherapy.12,16 By combining drug concentration data with patient-specific covariates, MIPD allows proactive and adaptive dose optimization, even before treatment initiation.17,18 Population pharmacokinetics (PopPK), as the foundation of MIPD, serve as the key strategy for individualized dosing through informing remedial dosing strategies,19 optimal sampling design,20 and clinical decision-support tools.21 Although several PopPK models of daptomycin have been published, systematic evaluation of their predictive performance and clinical utility remains limited.
The present study was designed to address this gap. Specifically, we (i) systematically reviewed published PopPK models of daptomycin, (ii) compared their predictive performance, and (iii) identified covariates contributing to interindividual variability. Furthermore, we developed an open-access maximum a posteriori (MAP) Bayesian estimator based on the PopPK repository. Together, these efforts aim to advance the clinical application of MIPD and facilitate precision dosing of daptomycin.
Methods
Search Strategy and Data Extraction
A systematic literature search was conducted in PubMed, Web of Science, and Embase to identify daptomycin PopPK models published up to 6 May 2025, following the PRISMA reporting guidelines. The search was restricted to parametric PopPK models to ensure consistency with the study objectives, including structural model comparison, interindividual variability assessment, covariate extraction, and evaluation of model-informed precision dosing trends. The nonlinear mixed-effects framework provides standardized reporting of fixed and random effects, enabling direct cross-study comparison.22 The search terms and selection criteria were presented in the Supplemental Materials 1.
Two authors independently extracted the following information from eligible articles: (1) baseline data: first author, year of publication, population Characteristics (including number of subjects, participant characteristics country, age, sex, weight, etc).; (2) study characteristics: sampling schedule, administration protocol, sample number, analysis method, etc.; (3) PopPK characteristics: model parameters, modeling software/algorithm, covariates, covariate selection criteria, inter-individual variability (IIV), and residual unexplained variability (RUV). (4) model application.
PopPK Models Predictive Performance Comparison
A total of 1000 virtual subjects were generated and stratified by renal function into four groups using rxode2 (version 4.0.3) package in R (version 4.5.1): normal renal function, mild renal impairment, moderate renal impairment, and severe renal impairment. Each virtual subject was assigned a standard age of 70 years and a body weight of 70 kg, reflecting the typical characteristics reported in most identified PopPK studies. Published PopPK models were then applied to simulate concentration–time profiles in these populations. A daily intravenous infusion of 6 mg/kg (infusion duration 1 h) was administered for 5 consecutive days to ensure steady state. Following the final dose, concentrations were sampled over a 24-hour period, and a non-compartment analysis was conducted to calculate the AUC and Cmin of different model prediction. All simulations were conducted using the rxode2 package in R.
Effect of Covariates on Clearance Variation
Clearance (CL) is a key determinant of individualized daptomycin dosing. To assess the influence of different covariates, we constructed a forest plot comparing their effects on CL. A covariate was considered clinically significant if the resulting change in CL exceeded 80–125%. For comparability, all continuous covariates were standardized to the same range. For renal function, different indicators such as CLcr and eGFRcys were used across studies. To ensure consistency, renal function was categorized into four groups: normal, mild, moderate, and severe. Body weight was classified according to previous studies21,23–25into three groups: low (30–59 kg), medium (60–100 kg), and high (>100 kg). Age was divided into three categories based on World Health Organization standards. Binary covariates, such as methadone23 co-administration, which was reported as a significant covariate that influence daptomycin CL, were coded such that the control group without methadone co-administartion was assigned as (COVi = 0), and the test group with methadone co-administration was assigned as (COVi = 1):

Accordingly, the range of individual clearance (CLi) is [CLcommon, CLcommon + CLdiff] when CLdiff > 0, and [CLcommon + CLdiff, CLcommon] when CLdiff < 0. The final impact of each covariate on CL was quantified using equation 2.

Monte Carlo Simulation for the Probability of Target Attainment
After the PopPK model repository of daptomycin was established, Monte Carlo simulations (n = 1000) were conducted for populations with different level of renal function (normal, mild, moderate, severe). Daptomycin was assumed to be administered via a 30-minute intravenous infusion under five common dosage regimens: 4, 6, 8, 10, and 12 mg/kg/d. For each regimen, the total area under the concentration-time curve at the steady state (AUC24h,ss) was calculated. Eight MIC values were considered: 0.25, 0.5, 1, 2, 4, and 8 mg/L, with MIC = 1 mg/L established as the threshold for daptomycin to cover most target strains under the current dosage regimens. The pharmacodynamic target was defined as AUC24h/MIC ≥ 666.9,26 The probability of target attainment (PTA) was then computed to evaluate the likelihood of achieving this target across renal function groups, dosing regimens, and MIC values. Toxicity risk was also assessed. Since a trough concentration (Cmin) ≥ 24.3 mg/L has been associated with a 50% probability of creatine phosphokinase elevation,10 we simulated the probability of Cmin ≥ 24.3 mg/L at 24 hours for each scenario. Optimal dosing was defined as regimens achieving PTA ≥ 90% for the PK/PD target, while maintaining the probability of Cmin ≥ 24.3 mg/L at ≤ 20%.27
Precision Dosing Tool Development
In clinical practice, clinicians often need to assess both AUC and Cmin to determine whether patients achieve adequate exposure and to evaluate the risk of toxicity. To support this process, we developed an AUC calculation tool based on maximum a posteriori Bayesian estimation (MAP-BE). The tool could integrate TDM data with population pharmacokinetic models and was implemented using R Shiny (version 1.11.1) and the mapbayr package (version 0.10.0).
Results
Overview of Included PopPK Studies for Daptomycin
Study Identification and Characteristic
A total of 592 records were retrieved through a comprehensive search strategy: 274 from PubMed, 93 from Embase, and 225 from Web of Science. After applying the eligibility criteria, 33 full-text articles were reviewed in detail. Among these, two studies were excluded because they used a nonparametric modeling approach. Four study was based solely on in vitro data and adopted model structures from previous work. Seven studies did not report PopPK parameters, and five studies only performed simulations without parameter estimation. Ultimately, 15 studies met the inclusion criteria and were incorporated into the present analysis. The study selection workflow is summarized in Figure 1.
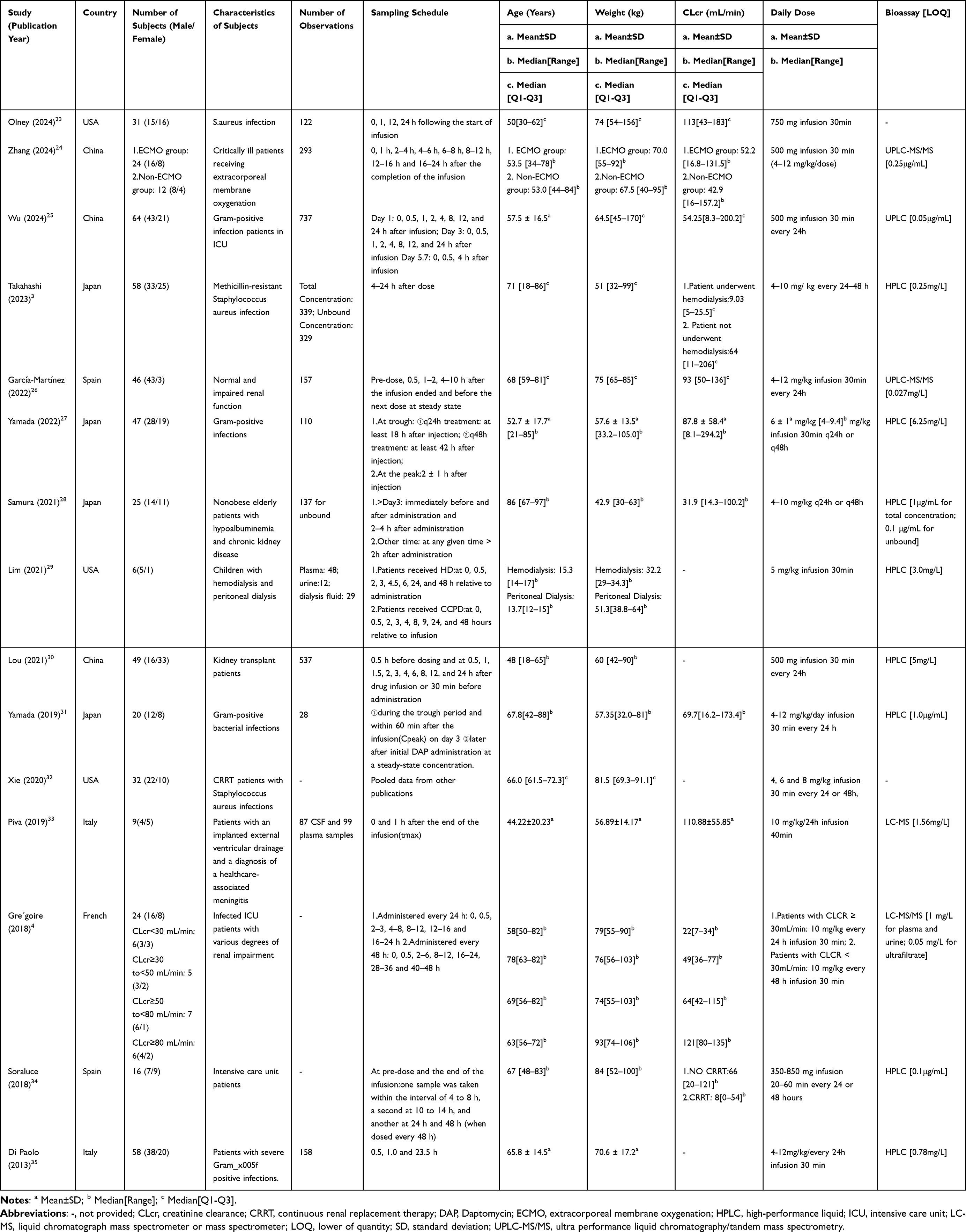 |
Table 1 Characteristics of Included Population Pharmacokinetic Studies |
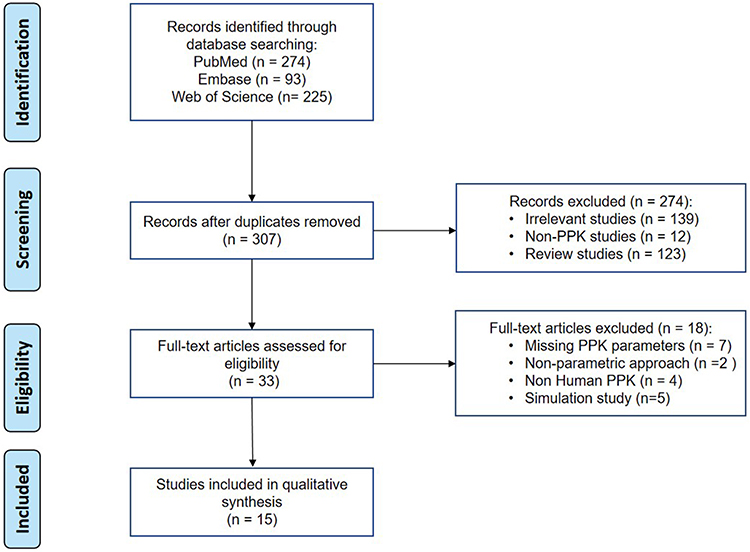 |
Figure 1 PRISMA flow diagram illustrating the study selection process for parametric population pharmacokinetic models of daptomycin. |
Study Characteristics
The demographic characteristics of all included studies are summarized in Table 1. The studies were published between 2013 and 2024 and involved populations from China, the United States of America (USA), Japan, Spain, Italy, and France. Of the 15 included studies, 14 were conducted in adult patients.3,4,23–28,30–35 Only one study involved pediatric participants receiving dialysis.29 Most adult studies focused on elderly patients with renal impairment, notably, one study extended its investigation to individuals with normal renal function.26 Regarding modeling software, the majority of studies used NONMEM.3,4,24–27,30–35 Two studies adopted Phoenix NLME,28,29 and one used Monolix.23 In terms of structural models, 10 studies employed a two-compartment model to describe daptomycin pharmacokinetics,3,4,24–30,32 while 5 studies applied a one-compartment model.23,31,33–35 Internal validation was commonly performed using goodness-of-fit (GOF) plots, visual predictive checks (VPC), and bootstrap. Two studies also incorporated normalized prediction distribution errors (NPDE). However, none of the included models underwent external validation. The detailed model characteristics and pharmacokinetic parameters are summarized in Table 2.
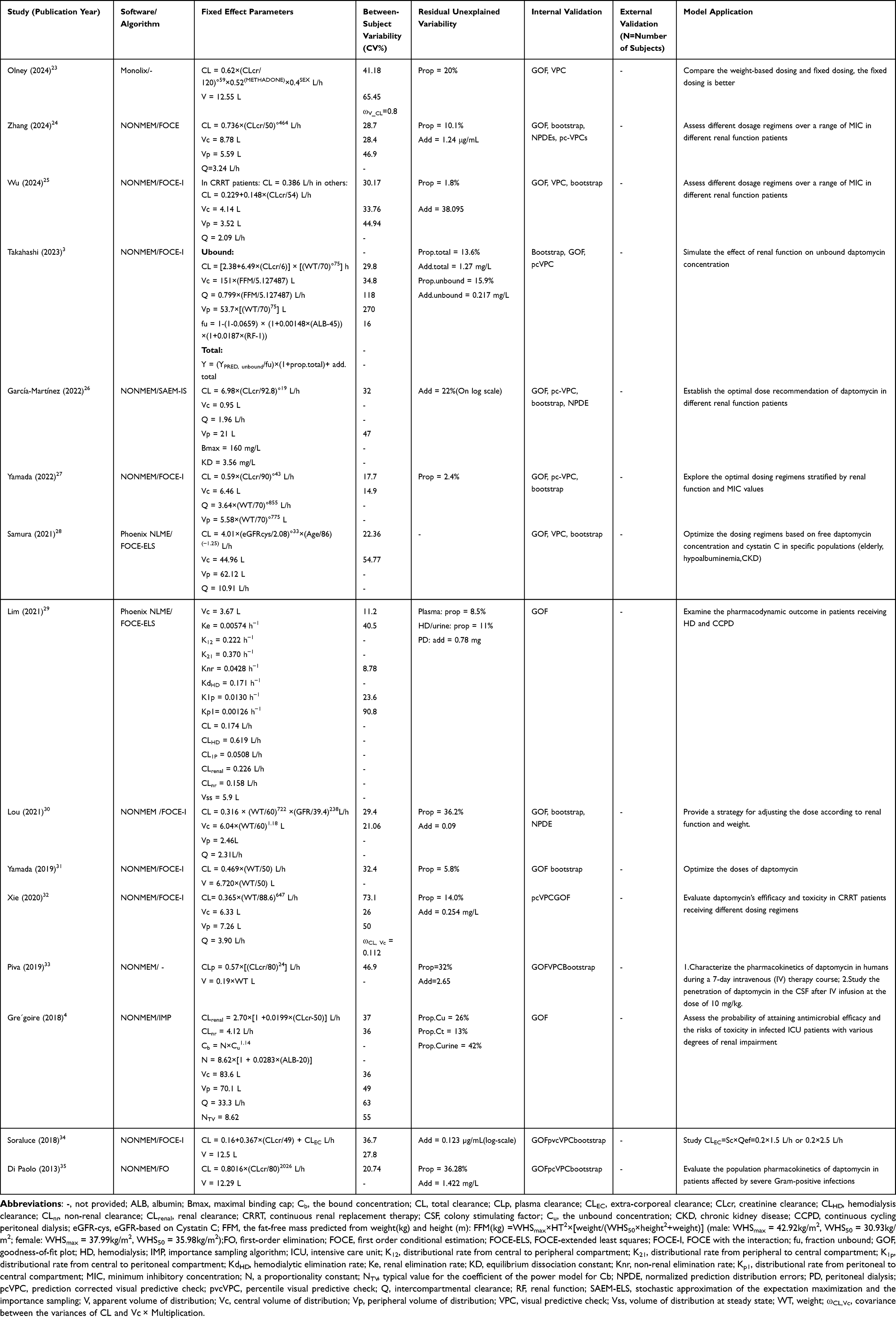 |
Table 2 Model Strategies and Final Pharmacokinetic Parameters of Included Studies |
Application of the PopPK Model Repository
Daptomycin PK Profiles
The steady state concentration–time profiles (assumed steady state is reached by the fifth dose) of daptomycin in populations with different levels of renal function are presented in Figure 2. Across all models, reduced renal function was associated with a marked increase in drug exposure, reflected by higher AUC values. This finding highlights the elevated risk of drug accumulation in patients with impaired renal function and underscores the need for careful dose adjustment to minimize toxicity.
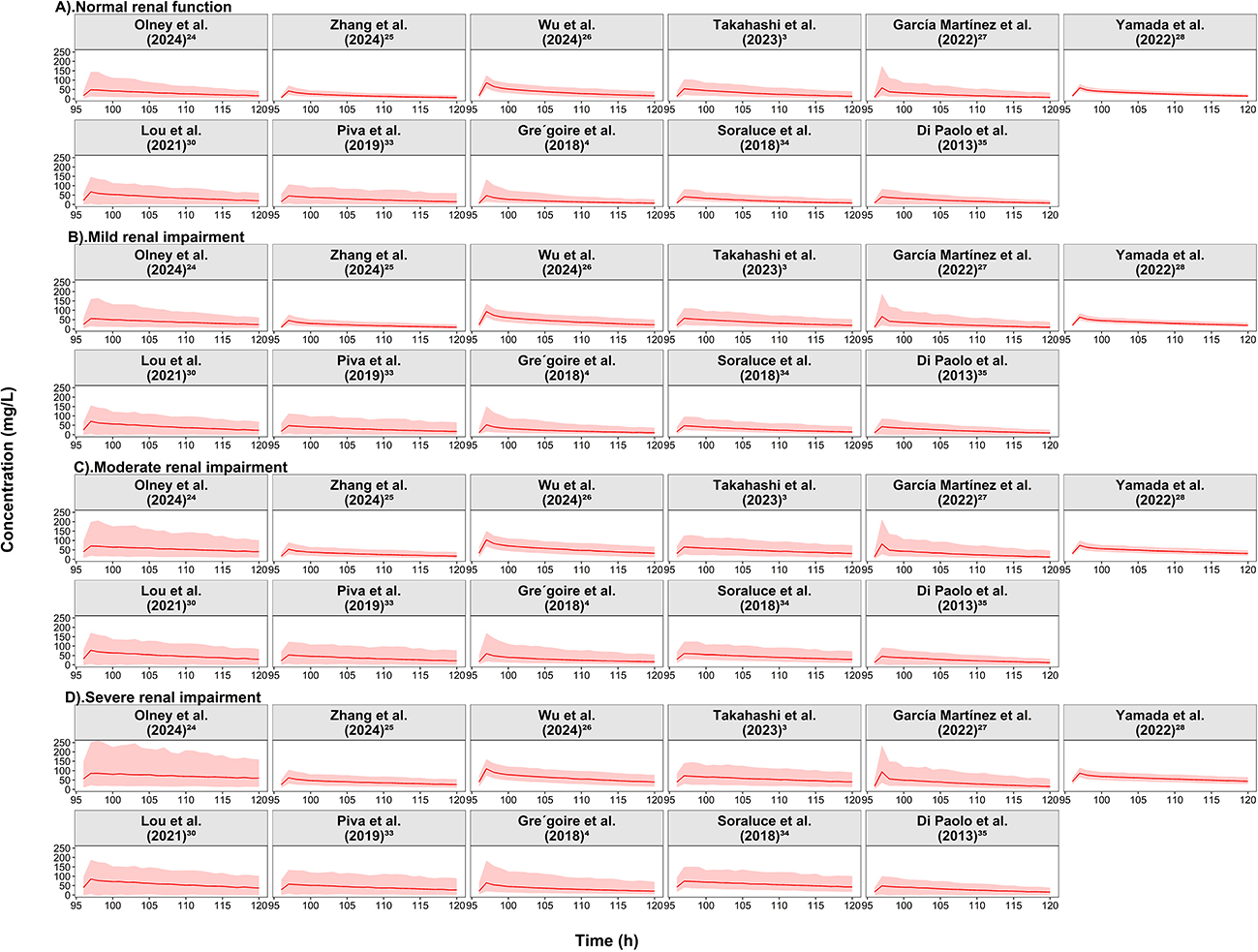 |
Figure 2 Simulated steady-state daptomycin total concentration-time profiles across different renal function subpopulations following intravenous infusion of 6 mg/kg every 24 hours based on retrieved population pharmacokinetic models. Notes: (A) Normal renal function; (B) Mild renal impairment; (C) Moderate renal impairment; (D) Severe renal impairment (renal categories defined according to each original model). The solid line represents the median predicted concentration–time profile, and the shaded area represents the 5th-95th percentile range derived from Monte Carlo simulations. All simulations assumed adult male patients receiving daptomycin monotherapy. Concentrations represent total plasma concentrations. |
In addition to total daptomycin concentrations, four studies3,4,26,28 in the repository developed models describing unbound daptomycin concentrations. Their predictions were also compared (Figure S1). Furthermore, two studies25,34 specifically modeled patients undergoing continuous renal replacement therapy (CRRT). In this subgroup, Soraluce’s34 model predicted exposures that were nearly half of those from Wu’s25 model (Figure S2).
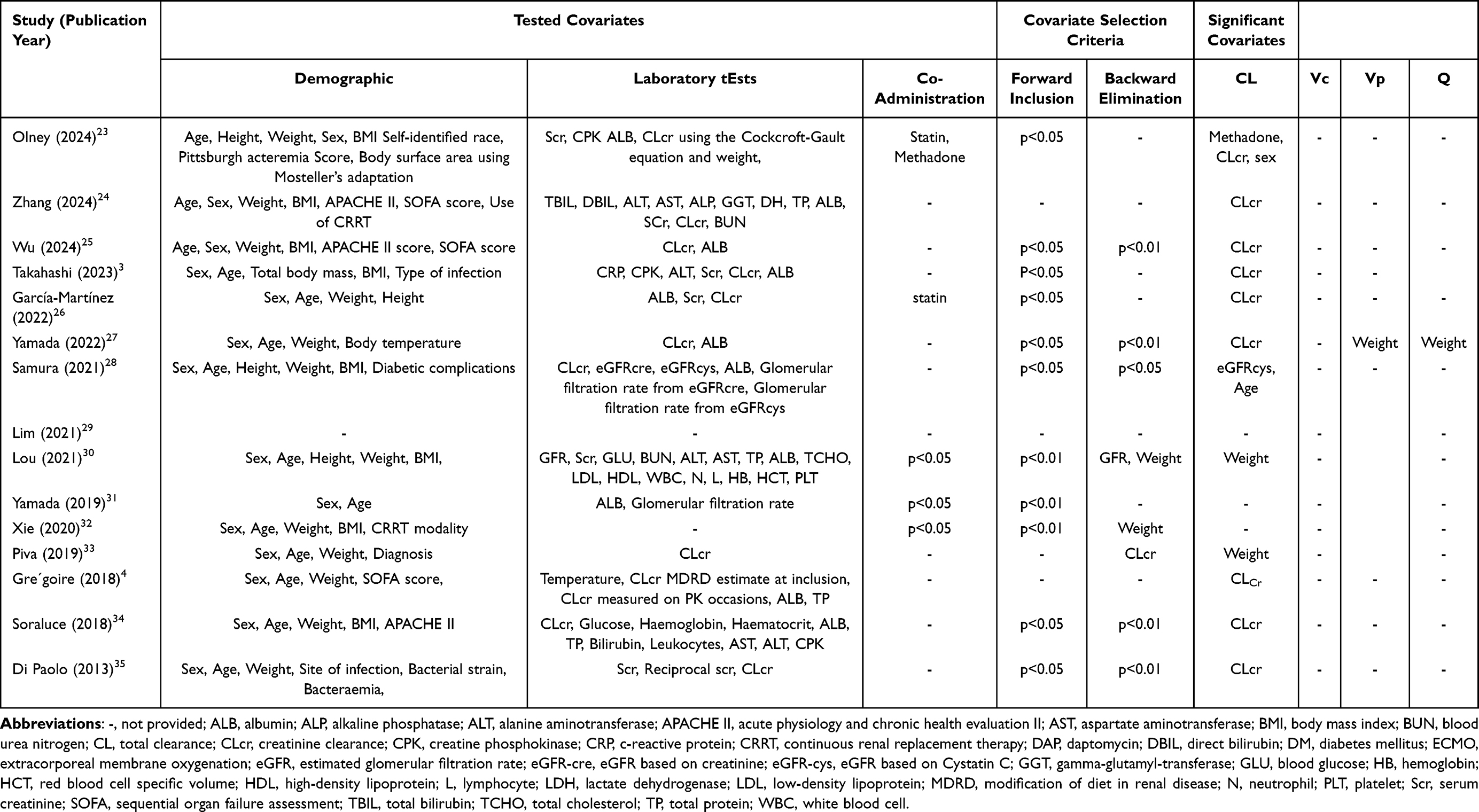 |
Table 3 List of Tested and Significant Covariates in the Model |
Covariate Screening and Covariate Effect
The covariates tested and identified in the PopPK model repository are summarized in Table 3. Renal function and body weight were the most frequently reported covariates influencing daptomycin pharmacokinetics. Renal function (CLcr or eGFRcys) was evaluated in 12 studies (80%),3,4,23–28,30,33–35 and 12 (100%) of these3,4,23–28,30,33–35 identified it as a significant covariate. This confirms that renal function has clinically meaningful effects on clearance, supporting the need for dose adjustments according to renal status. Body weight was identified as a significant covariate in four studies.27,30,32,33 Among these, three studies30,33 reported its impact on the volume of distribution, and two studies23,30 identified an effect on clearance. To further assess the clinical relevance of covariates, a forest plot was generated (Figure 3). The results demonstrated that patients with severe renal impairment differed significantly from those with moderate impairment (reference group). Moreover, even patients with normal or mildly impaired renal function exhibited significant differences in CL compared with the reference group, highlighting the need for dose optimization across renal function categories, rather than only adjusting the dosage for patients with severe renal impairment as indicated on the label.36 The effect of body weight on clearance was more modest. Higher body weight had little influence on clearance, whereas low body weight was associated with reduced clearance. Age showed minimal impact on clearance overall. In addition, Olney’s23 study identified lower clearance in females compared with males, and methadone co-administration significantly reduced daptomycin clearance.
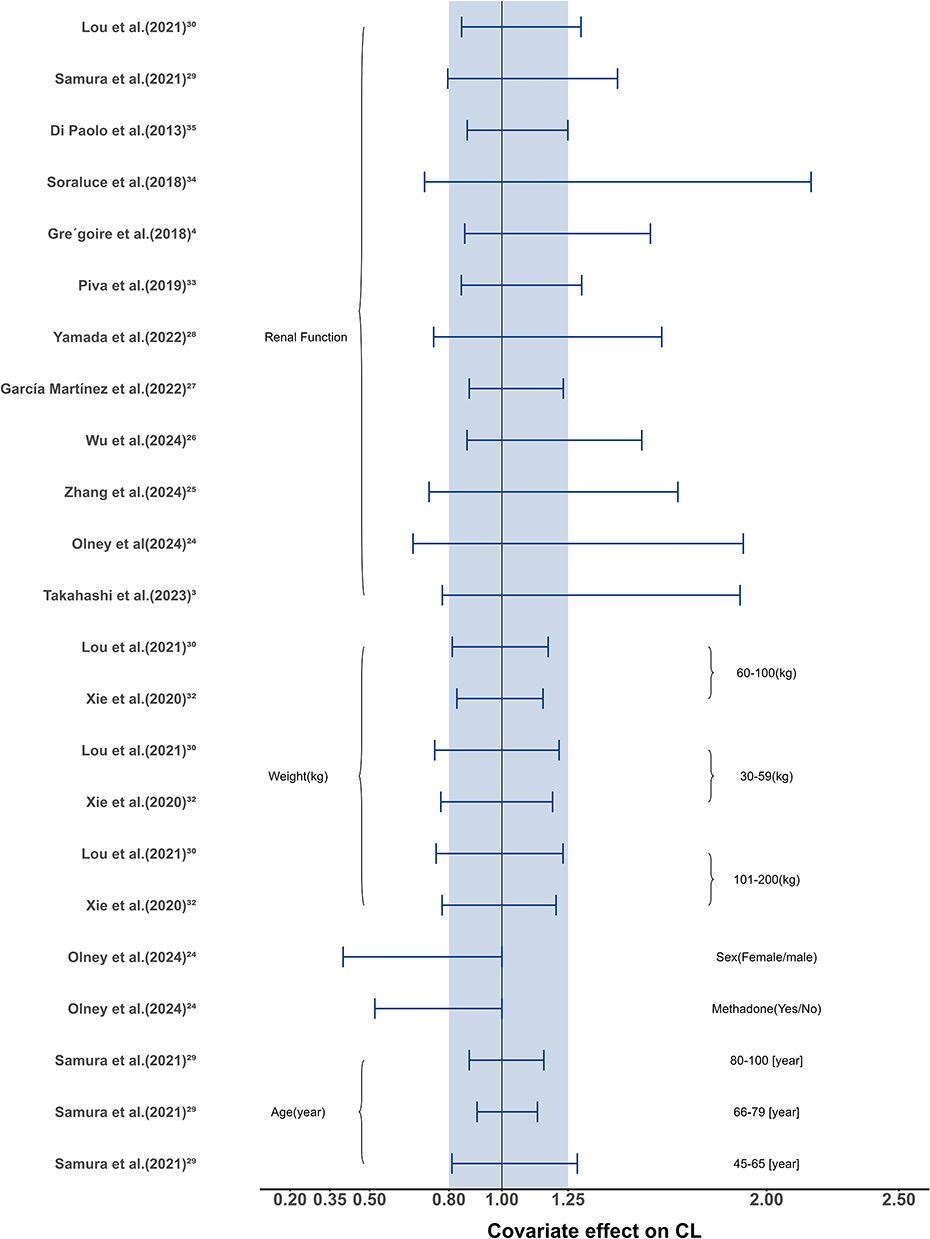 |
Figure 3 Forest plot summarizing the reported covariate effects on daptomycin clearance across included population pharmacokinetic models. Notes: Each horizontal bar represents the fold-change in clearance associated with a specific covariate relative to the reference value reported in the original study. The shaded region (0.8–1.25-fold) indicates the range considered clinically non-significant according to bioequivalence criteria. |
The Probability of Target Attainment
Although PK parameters varied among subpopulations, it was essential to determine whether these differences translated into altered pharmacodynamic outcomes. The results of all PTA simulations are summarized in Figure S3. Using an efficacy target of AUC24h/MIC ≥ 666, the simulations showed that PTA increased as renal function declined, and higher daily doses consistently produced higher PTA values across all populations. At the lowest dose (4 mg/kg), only three studies,25,27,30 predicted that patients with severe renal impairment could achieve the target, whereas patients with better renal function generally failed to reach it. Due to most of the predicted AUC was below the 666 mg*h/L (Figure 4). When the dose was increased to 10 mg/kg, most models predicted that patients with CLcr values between 15 and 60 mL/min achieved the efficacy target (Figures S4–S7).
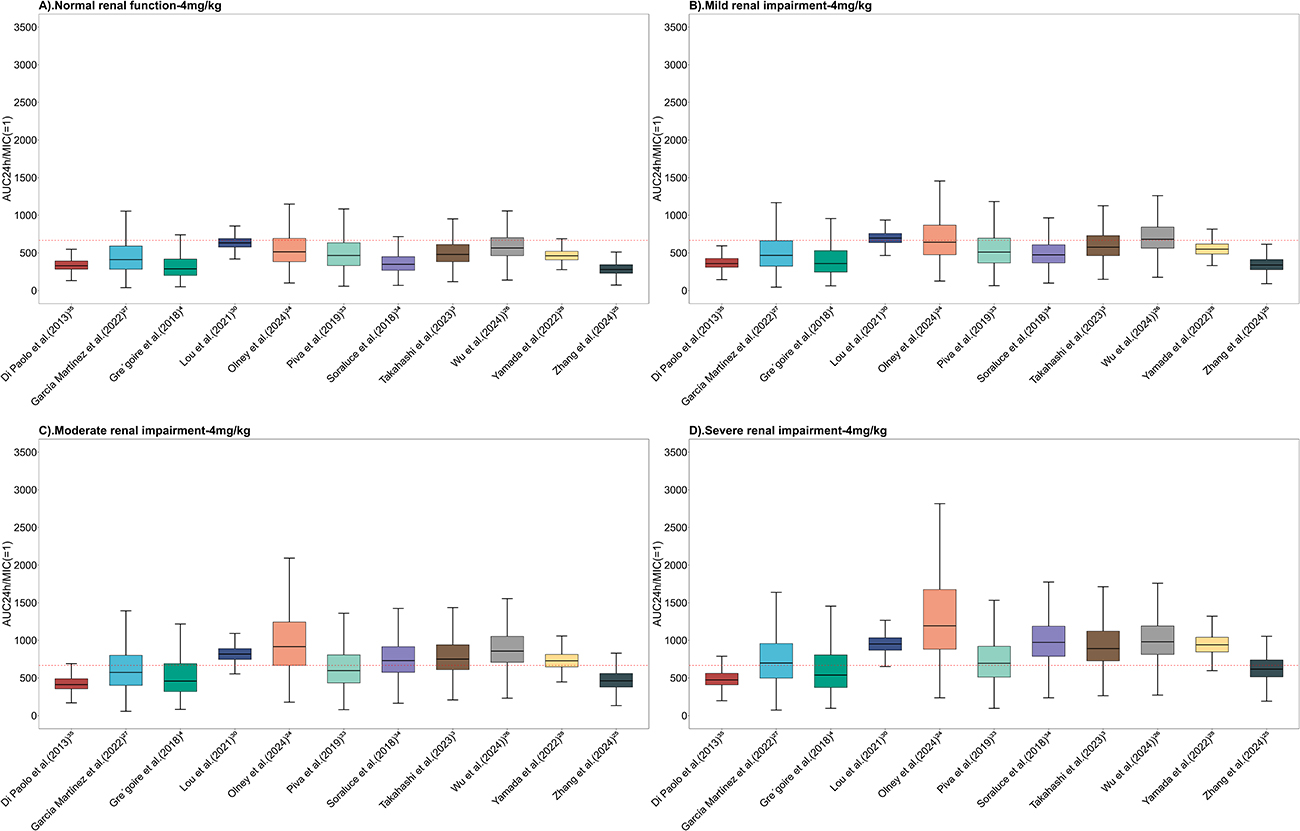 |
Figure 4 Predicted area under the concentration-time curve over 24 hours (AUC0-24h) following a 4 mg/kg intravenous infusion of daptomycin across renal function subpopulations based on retrieved population pharmacokinetic models. Notes: (A) Normal renal function, (B) Mild renal impairment, (C) Moderate renal impairment, (D) Severe renal impairment. The red dashed line represents AUC24h/MIC = 666/1. |
For toxicity assessment, with the toxicity threshold defined as Cmin ≥ 24.3 mg/L, the results are summarized in Figure 5. The probability of exceeding this threshold increased both with worsening renal function and with higher doses. Across most models, patients with severe renal impairment had a three- to fourfold higher risk of exceeding the toxicity threshold compared with those with normal renal function. Even at 4 mg/kg, six studies3,23,25,27,30,34 predicted that more than 20% of patients with severe renal impairment would exceed the safety limit. At 6 mg/kg, 9 out of 11 models3,4,23–25,27,30,33,34 predicted excessive toxicity, indicating that patients with moderate to severe renal impairment should be treated with caution at doses ≥ 6 mg/kg.
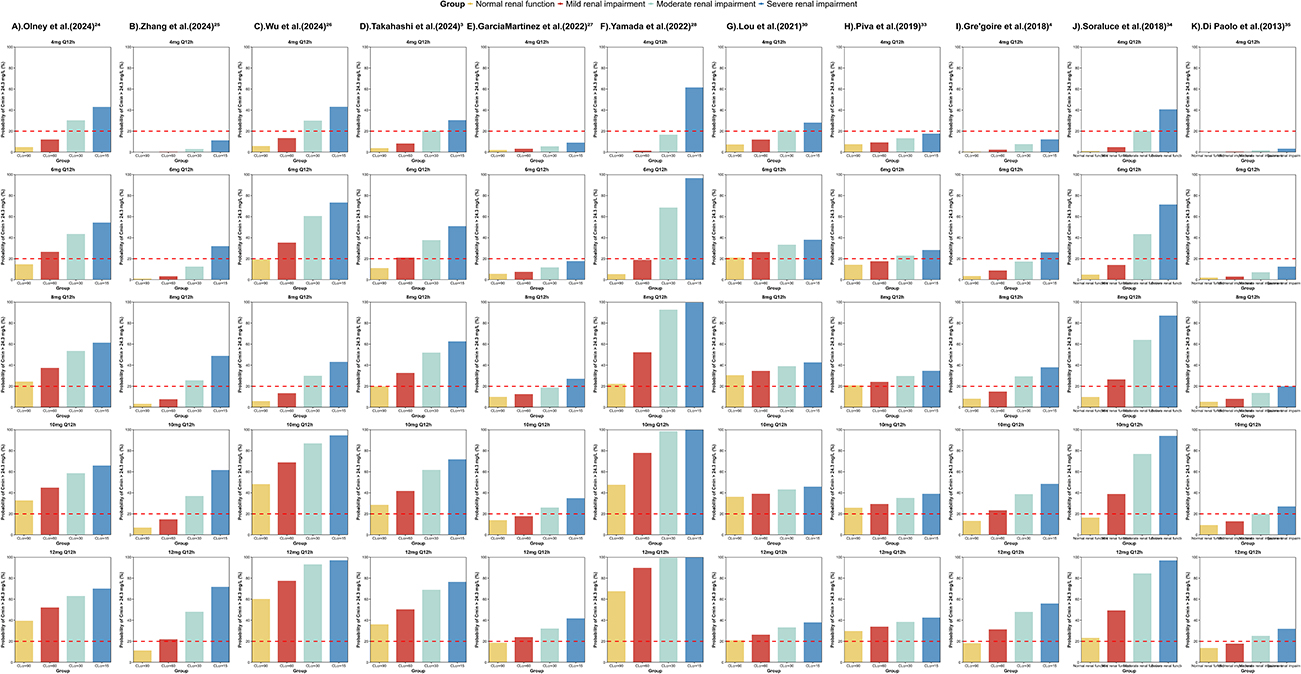 |
Figure 5 Predicted probability of trough concentration exceeding 24.3 mg/L at steady state across different renal function subpopulations for each retrieved population pharmacokinetic model. Notes: (A)–(K) represent different population pharmacokinetic models from different studies used in the simulations. The red dashed line represents the 20% threshold. The yellow column represents the normal renal function, the red column represents the mild renal impairment, the light blue column represents the moderate renal impairment, the blue column represents the severe renal impairment. |
Calculator Based on MAP-BE
With the purpose of transferring the model to clinical bedside, we developed a precision dosing calculator based on the model established by Grégoire4 as an example. The tool estimates AUCinterveal and Cmin following daptomycin administration. Briefly, as it illustrated in Figure 6, to perform these calculations, the calculator requires input of dosing information (eg., dose amount, infusion duration, dosing interval), sampling data (eg., sampling time, observed concentrations), and patient demographics (eg., body weight, serum albumin, creatinine clearance). By entering these parameters, a simulated concentration–time profile is generated for the individual patient, from which AUC and Cmin are calculated for the dosing interval. If the target exposure is not achieved, the “Next Dose Explorer” module provides recommendations for dose adjustment. A demonstration version of this calculator is available online (https://mipdshinyapp.shinyapps.io/Daptomycin/), and a detailed user guide is provided in the Supplementary Materials 2.
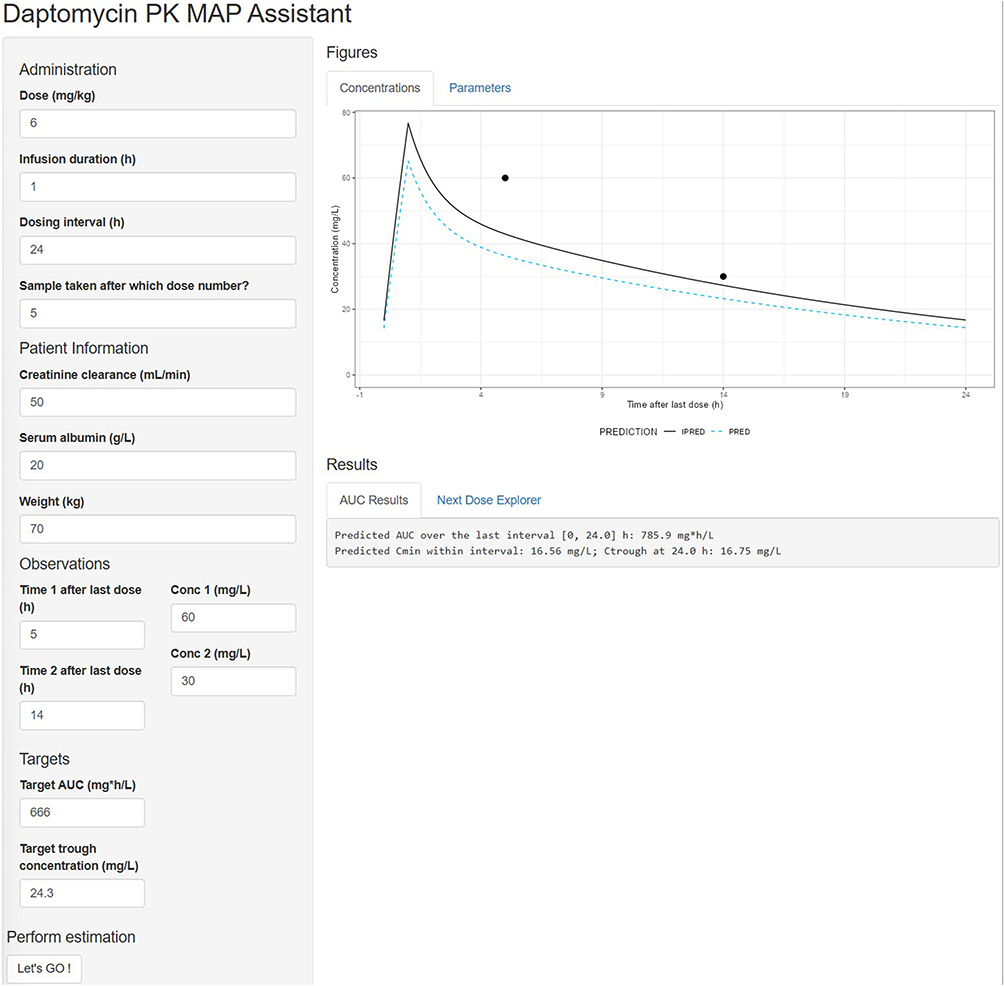 |
Figure 6 Schematic workflow of the Maximum A Posteriori Bayesian estimator assistant developed for individualized daptomycin pharmacokinetic prediction. |
Discussion
To the best of our knowledge, this is the first study to establish a parametric PopPK model repository for daptomycin. By systematically evaluating existing models and integrating their structures, we provide a unified platform to simulate concentration–time profiles, explore covariate effects, and predict probability of target attainment. In addition, we developed a precision dosing tool based on this repository, demonstrating a practical pathway to translate pharmacometrics models into clinical use.
Renal clearance is the main elimination pathway of daptomycin, with approximately 50% of the administered dose excreted unchanged in urine. Accordingly, the drug label recommends dose adjustment based on creatinine clearance, such as extending the dosing interval when CLcr < 30 mL/min. Consistent with this, our analysis found that 12 of 15 PopPK models identified renal function as a significant covariate for clearance. Among them, Soraluce’s34 model showed the largest variability of CL in different renal function patients, likely because it was developed in a cohort covering a broad range of renal function, and less patients (only 16) involved in the model development. However, Di Paolo35 and García-Martínez’s26 models suggested smaller renal effects on clearance, with the upper and lower bounds fall in the 0.8–1.25 range. This may be attributable to the limited variability in renal function among the patients included in their studies. Using moderate impairment as the reference, we observed clinically significant differences not only between severe and moderate impairment, but also between normal/mild renal impairment function and moderate impairment (Figure 3).
Model performance differed in predicting efficacy. For example, Wu,25 and Yamada’s27 and Lou’s models30 predicted that patients with severe renal impairment could still achieve the efficacy target with 4 mg/kg dosing, whereas other studies did not. This suggests that the standard 4 mg/kg regimen may be inadequate for patients with renal impairment, the higher doses might be required. With respect to safety, the probability of exceeding the Cmin threshold was substantially higher in patients with reduced renal function, indicating an increased risk of toxicity in this group. Previous reports have also suggested that halving the dosing rate in renally impaired patients can lower the incidence of adverse events.4,37 Besides, higher doses were associated with a significantly increased risk of creatine phosphokinase elevation.38 Moreover, genetic polymorphisms may influence daptomycin pharmacokinetics. Romain et al39 reported that the volume of distribution was approximately 25% lower in patients with the homozygous CGC ABCB1 haplotype compared with other genotypes, which may affect target attainment in patients infected with high-MIC pathogens. In addition, Lorena et al40 found that the ABCB1 3435C>T polymorphism influenced daptomycin exposure, with the 3435TT genotype associated with higher AUC0-24h values. Protein binding is another key determinant of daptomycin pharmacokinetics and pharmacodynamics, as only the unbound fraction mediates antibacterial activity. Daptomycin is highly protein bound (90–93%), only four studies3,4,26,28 developed models accounting for bound and unbound drug. Grégoire et al4 measured both plasma and urine samples, finding that the unbound fraction increased as renal function declined. Based on these data, they recommended 10 mg/kg q24h for ICU patients with CLcr ≥ 30 mL/min and q48h for those with CLcr < 30 mL/min. Martínez et al26 also developed a bound/unbound model, but they did not use free concentrations directly, leading to potential structural identifiability issues. For instance, their estimated central compartment volume (0.95 L) was substantially lower than reported in other studies. Special consideration is required for patients receiving CRRT. Xie et al32 developed a PopPK model in this population with Staphylococcus aureus infections. Their simulations indicated that q48h dosing was inadequate, whereas a regimen of 6 mg/kg q24h combined with CRRT doses of 30–35 mL/h/kg provided the best balance of efficacy and safety. These findings align with the drug label, which recommends 6 mg/kg for S. aureus infections and 4 mg/kg for cSSTI.
Body weight and age were less frequently identified as covariates. Only three studies reported significant effects, despite the label recommending weight-based dosing in pediatric and adult populations. This likely reflect the fact that most included studies predominantly enrolled elderly patients (>60 years). The lack of pediatric data highlights an important knowledge gap, particularly regarding precision dosing in children with renal impairment. Further studies are warranted to establish safe and effective regimens in this population.
Moreover, in this study, we further developed a user-friendly interface based on Grégoire’s4 model to support individualized dosing in patients with varying renal function as an example. The tool allows clinicians to integrate TDM data, estimate AUC and Cmin, and explore alternative regimens using MAP Bayesian estimation. It enables real-time PopPK simulations and “what-if” decision-making scenarios. Compared with traditional PopPK model applications, this platform lowers the technical barrier, offering clinicians and pharmacists a practical option to optimize daptomycin therapy at the bedside.
This study has several limitations. First, only English-language publications were included, which may have led to omission of relevant PopPK models published in other languages. Second, due to limited available data, external validation of the published models was not feasible. As a result, only one model was selected as a demonstration for tool development. Future work should conduct external evaluations of existing models and validate the Shiny-based dosing tool in prospective clinical settings.
Conclusion
This study provides a comprehensive evaluation of published PopPK models of daptomycin. By comparing demographic characteristics, structural assumptions, and covariate effects across models, we obtained a clearer understanding of the sources of interindividual variability. In addition, we developed a precision dosing tool based on this model repository. This tool represents a step forward in translating pharmacometric research into clinical practice, providing clinicians with a practical and scientifically grounded resource to support individualized daptomycin therapy.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author (Xin Liu) upon reasonable request.
Funding
This research was funded by the Natural Science Foundation of Hunan Provenience the funding numbers are 2020JJ9029 and 2025JJ80180.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Karaman J. Resistance of Gram-Positive Bacteria to Current Antibacterial Agents and Overcoming Approaches. Molecules. 2020;25(12):2888. doi:10.3390/molecules25122888
2. Aktaş G, Derbentli S, Aktas, & Derbentli. In Vitro Activity of Daptomycin Against VRE and MRSA Strains. Mikrobiyoloji Bulteni. 2014;48(1):123–19.
3. Takahashi T, Tsuji Y, Holford N, et al. Population Pharmacokinetic Model for Unbound Concentrations of Daptomycin in Patients with MRSA Including Patients Undergoing Hemodialysis. Eur J Drug Metab Pharmacokinet. 2023;48(2):201–211. doi:10.1007/s13318-023-00820-0
4. Gregoire M, Marchand S, Ferrandière M, et al. Population pharmacokinetics of daptomycin in critically ill patients with various degrees of renal impairment. J Antimicrob Chemother. 2019;74(1):117–125. doi:10.1093/jac/dky374
5. Kosmidis C, Levine DP, Kosmidis, & Levine. Daptomycin: pharmacology and clinical use. Expert Opin Pharmacother. 2010;11(4):615–625. doi:10.1517/14656561003598893
6. Jones J, Jun AH, Michal JL, et al. High-Dose Daptomycin and Clinical Applications. Ann. Pharmacother. 2021;55(11):1363–1378. doi:10.1177/1060028021991943
7. Martins M, Martins JES, Severino P, et al. Physiologically based pharmacokinetic modelling to inform combination dosing regimens of ceftaroline and daptomycin in special populations. Br J Clin Pharmacol. 2023;89(9):2726–2738. doi:10.1111/bcp.15731
8. Canut I, Isla A, Betriu C, et al. Pharmacokinetic-pharmacodynamic evaluation of daptomycin, tigecycline, and linezolid versus vancomycin for the treatment of MRSA infections in four Western European countries. Eur J Clin Microbiol Infect Dis. 2012;31(9):2227–2235. doi:10.1007/s10096-012-1560-7
9. Falcone R, Russo A, Venditti M, et al. Considerations for Higher Doses of Daptomycin in Critically Ill Patients With Methicillin-Resistant Staphylococcus aureus Bacteremia. Clinl Infect Dis. 2013;57(11):1568–1576. doi:10.1093/cid/cit582
10. Bhavnani R, Rubino C, Ambrose P, et al. Daptomycin Exposure and the Probability of Elevations in the Creatine Phosphokinase Level: data from a Randomized Trial of Patients with Bacteremia and Endocarditis. Clinl Infect Dis. 2010;50(12):1568–1574. doi:10.1086/652767
11. Matsumoto S, Samura M, Tashiro S, et al. Target Therapeutic Ranges of Anti-MRSA Drugs, Linezolid, Tedizolid and Daptomycin, and the Necessity of TDM. Biol Pharm Bull. 2022;45(7):824–833. doi:10.1248/bpb.b22-00276
12. Wicha M, Märtson A-G, Nielsen EI, et al. From Therapeutic Drug Monitoring to Model-Informed Precision Dosing for Antibiotic. Clin Pharmacol Ther. 2021;109(4):928–941. doi:10.1002/cpt.2202
13. Heitzmann T, Thoma Y, Bricca R, et al. Implementation and Comparison of Two Pharmacometric Tools for Model-Based Therapeutic Drug Monitoring and Precision Dosing of Daptomycin. Pharmaceutics. 2022;14(1):114. doi:10.3390/pharmaceutics14010114
14. Kantasiripitak VD, Van Daele R, Gijsen M, et al. Software Tools for Model-Informed Precision Dosing: how Well Do They Satisfy the Needs? Front Pharmacol. 2020;11:620. doi:10.3389/fphar.2020.00620
15. Tran P, Palmer HR, Weston J, et al. Evaluation of a daptomycin dose-optimization protocol. Am J Health Syst Pharm. 2012;69(11):979–984. doi:10.2146/ajhp110279
16. Dibbets K, Koldeweij C, Osinga EP, et al. Barriers and Facilitators for Bringing Model-Informed Precision Dosing to the Patient’s Bedside: a Systematic Review. Clin Pharmacol Ther. 2025;117(3):633–645. doi:10.1002/cpt.3510
17. Oda S, Saito H, Jono H, et al. Bayesian prediction-based individualized dosing of anti-methicillin-resistant Staphylococcus aureus treatment: recent advancements and prospects in therapeutic drug monitoring. Pharmacol Ther. 2023;246:108433. doi:10.1016/j.pharmthera.2023.108433
18. Hoffert D, Dia N, Vanuytsel T, et al. Model-Informed Precision Dosing of Tacrolimus: a Systematic Review of Population Pharmacokinetic Models and a Benchmark Study of Software Tools. Clin Pharmacokinet. 2024;63(10):1407–1421. doi:10.1007/s40262-024-01414-y
19. Liu J, Ju G, Yang W, et al. Escitalopram Personalized Dosing: a Population Pharmacokinetics Repository Method. Drug Des Devel Ther. 2023;17:2955–2967. doi:10.2147/dddt.S425654
20. Sturkenboom M, Mulder LW, de Jager A, et al. Pharmacokinetic Modeling and Optimal Sampling Strategies for Therapeutic Drug Monitoring of Rifampin in Patients with Tuberculosis. Antimicrob Agents Chemother. 2015;59(8):4907–4913. doi:10.1128/aac.00756-15
21. Liu L, Li Z-R, Wang C-Y, et al. Handling delayed or missed direct oral anticoagulant doses: model-informed individual remedial dosing. Blood Adv. 2024;8(22):5906–5916. doi:10.1182/bloodadvances.2024013854
22. Goutelle W, Woillard J-B, Buclin T, et al. Parametric and Nonparametric Methods in Population Pharmacokinetics: experts’ Discussion on Use, Strengths, and Limitations. J Clin Pharmacol. 2022;62(2):158–170. doi:10.1002/jcph.1993
23. Olney P, Pai MP, Thomas JK, et al. Fixed dose daptomycin: an opportunity for pharmacokinetic/pharmacodynamic optimization in Staphylococcus aureus infections. Pharmacotherapy. 2024;44(8):615–622. doi:10.1002/phar.4602
24. Zhang L, Li Q-Y, Zhang Y-Q, et al. Population pharmacokinetics of daptomycin in critically ill patients receiving extracorporeal membrane oxygenation. J Antimicrob Chemother. 2024;79(7):1697–1705. doi:10.1093/jac/dkae171
25. Zheng W, Lv Z, Zhao W, et al. Population pharmacokinetics of intravenous daptomycin in critically ill patients: implications for selection of dosage regimens. Front Pharmacol. 2024;15. doi:10.3389/fphar.2024.1378872
26. García-Martínez B-M, Bellés-Medall MD, García-Cremades M, et al. Population Pharmacokinetic/Pharmacodynamic Modelling of Daptomycin for Schedule Optimization in Patients with Renal Impairment. Pharmaceutics. 2022;14(10):2226. doi:10.3390/pharmaceutics14102226
27. Yamada S, Soda M, Nishida R, et al. Simplified daptomycin dosing regimen for adult patients with methicillin-resistant Staphylococcus aureus infections based on population pharmacokinetic analysis. Drug Metab Pharmacokinet. 2022;44:100444. doi:10.1016/j.dmpk.2022.100444
28. Samura T, Takada K, Yamamoto R, et al. Population Pharmacokinetic Analysis and Dosing Optimization Based on Unbound Daptomycin Concentration and Cystatin C in Nonobese Elderly Patients with Hypoalbuminemia and Chronic Kidney Disease. Pharm Res. 2021;38(6):1041–1055. doi:10.1007/s11095-021-03058-0
29. Lim L, Lewis T, Woo S, et al. Daptomycin Pharmacokinetics in Adolescents Undergoing Hemodialysis and Peritoneal Dialysis: a Case Series With Pharmacokinetic Modeling. J Pediatric Pharmacol Therap. 2021;26(2):123–132. doi:10.5863/1551-6776-26.2.123
30. Lou L, Liu Y-X, Wang J, et al. Population pharmacokinetics and individual analysis of daptomycin in kidney transplant recipients. Eur J Pharm Sci. 2021;162:105818. doi:10.1016/j.ejps.2021.105818
31. Yamada O, Ooi Y, Oda K, et al. Observational study to determine the optimal dose of daptomycin based on pharmacokinetic/pharmacodynamic analysis. J Infect Chemother. 2020;26(4):379–384. doi:10.1016/j.jiac.2019.11.002
32. Xie L, Li S, Cheng Z, et al. Population pharmacokinetics and dosing considerations of daptomycin in critically ill patients undergoing continuous renal replacement therapy. J Antimicrob Chemother. 2020;75(6):1559–1566. doi:10.1093/jac/dkaa028
33. Di Paolo P, Di Paolo A, Galeotti L, et al. Daptomycin Plasma and CSF Levels in Patients with Healthcare-Associated Meningitis. Neurocrit Care. 2019;31(1):116–124. doi:10.1007/s12028-018-0657-y
34. Soraluce A-P, Asín-Prieto E, Rodríguez-Gascón A, et al. Population pharmacokinetics of daptomycin in critically ill patients. Int J Antimicrob Agents. 2018;52(2):158–165. doi:10.1016/j.ijantimicag.2018.03.008
35. Paolo D, Tascini, Tascini C, et al. Population pharmacokinetics of daptomycin in patients affected by severe Gram-positive infections. Int J Antimicrob Agents. 2013;42(3):250–255. doi:10.1016/j.ijantimicag.2013.06.006
36. FDA. (2024). DAPTOMYCIN for injection, for intravenous use [FDA Label]. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/208385s005lbl.pdf.
37. Kullar M, McClellan I, Geriak M, et al. Efficacy and Safety of Daptomycin in Patients with Renal Impairment: a Multicenter Retrospective Analysis. Pharmacotherapy. 2014;34(6):582–589. doi:10.1002/phar.1413
38. Bhavnani A, Ambrose PG, Hammel JP, et al. Evaluation of Daptomycin Exposure and Efficacy and Safety Endpoints To Support Risk-versus-Benefit Considerations. Antimicrob Agents Chemother. 2016;60(3):1600–1607. doi:10.1128/aac.02967-15
39. Bricca G, Goutelle S, Roux S, et al. Genetic polymorphisms of ABCB1 (P-glycoprotein) as a covariate influencing daptomycin pharmacokinetics: a population analysis in patients with bone and joint infection. J Antimicrob Chemother. 2019;74(4):1012–1020. doi:10.1093/jac/dky541
40. Baietto D, D’Avolio A, Cusato J, et al. Effect of SNPs in human ABCB1 on daptomycin pharmacokinetics in Caucasian patients. J Antimicrob Chemother. 2015;70(1):307–308. doi:10.1093/jac/dku368
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.