Back to Journals » ImmunoTargets and Therapy » Volume 14
Advancing Adjuvant Immunotherapy in Hepatocellular Carcinoma: A Comprehensive Review
Authors Akabane M, Chatzipanagiotou OP, Imaoka Y, Schenk A, Pawlik TM ![]()
Received 17 March 2025
Accepted for publication 16 June 2025
Published 25 June 2025 Volume 2025:14 Pages 631—654
DOI https://doi.org/10.2147/ITT.S528709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Miho Akabane,1 Odysseas P Chatzipanagiotou,1 Yuki Imaoka,2 Austin Schenk,1 Timothy M Pawlik1
1Department of Surgery, The Ohio State University Wexner Medical Center and James Comprehensive Cancer Center, Columbus, OH, USA; 2Division of Abdominal Transplant, Department of Surgery, Stanford University, Stanford, CA, USA
Correspondence: Timothy M Pawlik, Department of Surgery, The Ohio State University Wexner Medical Center and James Comprehensive Cancer Center, 395 W. 12th Avenue, Suite 670, Columbus, OH, 43210, USA, Tel +1614-293-8701, Fax +1614-293-4063, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) remains a leading cause of cancer-related mortality globally, with high rates of recurrence even after curative-intent treatments such as hepatectomy and liver transplantation (LT). In recent years, immune checkpoint inhibitors (ICIs) have transformed the therapeutic landscape for HCC, demonstrating significant efficacy among advanced-stage tumors through combination regimens, such as anti-programmed cell death ligand-1 (PD-L1)/PD-1 inhibitors with anti-vascular endothelial growth factor agents. Recent advances have highlighted the potential of ICIs as adjuvant therapy to improve recurrence-free survival among high-risk patients post-resection. However, challenges such as low immunogenicity, the immunosuppressive tumor microenvironment, and immune resistance remain substantial barriers to the broader success of ICIs. In the context of LT, the use of ICIs is further complicated by the concurrent need for immunosuppressive agents, which can exacerbate the risk of recurrence. Emerging strategies focusing on the optimization of the timing of ICI therapy and the utilization of novel biomarkers are being explored to mitigate graft rejection while maintaining antitumor efficacy. Additionally, immune-cell-based therapies based on chimeric antigen receptor-T and natural killer (NK) cells, adoptive cell transfer, and liver-resident NK cell approaches are also being investigated for their potential to reduce recurrence and improve survival outcomes. This review focuses on the current landscape of adjuvant immunotherapy and immune-cell therapy in the postoperative management of HCC, highlighting ongoing clinical trials, therapeutic potential, and associated risks. With continued advancements in immunotherapeutic strategies and personalized approaches, these therapies hold the promise of transforming outcomes for patients undergoing curative resection or LT.
Keywords: hepatocellular carcinoma, hepatectomy, liver transplantation, immune checkpoint inhibitors, adjuvant immunotherapy, immune-cell therapy
Introduction
Hepatocellular carcinoma (HCC) is one of the fastest-growing causes of cancer-related mortality worldwide.1,2 Curative treatments such as hepatectomy and liver transplantation (LT) are viable options for patients in the early stages of the disease. However, approximately 50–60% of patients with HCC eventually require systemic therapy due to disease progression.3 Radical surgical resection is not a feasible option for many patients with advanced HCC, thus leaving systemic therapies as first-line treatment. Despite achieving a median overall survival (OS) of 11–14 months,3–5 these therapies often fail to effectively control tumor progression or prevent recurrence. Recent advancements in immuno-oncology have introduced immune checkpoint inhibitors (ICIs), which have transformed the management of many malignancies, including HCC.6–8 Remarkable efficacy has been demonstrated by combination regimens, such as anti-programmed cell death ligand-1 (PD-L1) or PD-1 inhibitors with anti-cytotoxic T-lymphocyte antigen 4 (CTLA-4) monoclonal antibodies and anti-vascular endothelial growth factor (VEGF) agents like bevacizumab. This approach has extended median survival to approximately 19 months in some cases, offering new hope to patients with advanced HCC.9–12 Clinical trials have consistently demonstrated the superior efficacy of combination ICI therapies compared to tyrosine kinase inhibitors alone.13 In HCC management, neoadjuvant downstaging therapies, including immunotherapy, have shown potential in converting previously unresectable diseases into resectable Similarly, the use of ICIs as bridging therapy during LT waitlisting has been proposed to reduce waitlist mortality. Moreover, adjuvant immunotherapy has been gaining recognition for its potential to prevent both postoperative recurrence and de novo malignancies following resection or LT. Clinical trials investigating neoadjuvant and adjuvant immunotherapies for HCC have been reporting encouraging outcomes. Of note, the IMbrave050 trial initially suggested that adjuvant therapy with atezolizumab and bevacizumab might improve recurrence-free survival (RFS) over active surveillance among patients at high risk of HCC recurrence.14,15 However, updated data presented at ESMO 2024 showed that this difference in RFS was not statistically significant, prompting a re-evaluation of the clinical utility of this regimen in the adjuvant setting. These findings underscore the need for further studies to identify which patient subsets may benefit most from adjuvant immunotherapy.14,15 In this context, a recent study published in Nature Communications16 demonstrated that perioperative administration of immunotherapy—specifically combining neoadjuvant and adjuvant approaches—can significantly enhance anti-tumor immune responses in early-stage HCC, further supporting the rationale for immunotherapy in the curative setting.
Importantly, the prevalence and incidence of HCC vary significantly according to the etiology of chronic liver disease. Viral hepatitis B and C are the most common underlying causes of HCC, particularly in cirrhotic livers, whereas autoimmune liver diseases such as autoimmune hepatitis and primary biliary cholangitis are associated with a much lower incidence of HCC, even in the presence of cirrhosis.17 This epidemiological distinction underscores the relevance of immune microenvironment differences and may impact response to immunotherapy.17
Despite the progress, several challenges limit the efficacy of ICIs in the management of HCC. The response rate to ICI monotherapy is under 20%, primarily due to the complex immunosuppressive tumor microenvironment (TME) and the heterogeneous pathogenesis of HCC.18 Although combination therapies have demonstrated better response rates of 30–36%, the development of immune resistance is common and presents a significant hurdle.19,20 Factors contributing to resistance include impaired antigen presentation, abnormal activation of immunosuppressive cells, and dysfunctional anti-tumor immune cells within the TME.20 Moreover, tumor heterogeneity, lack of tumor antigen expression, and gut microbiota dysregulation further exacerbate immune resistance.20 Importantly, ICIs carry a risk of severe immune-related adverse events (irAEs) leading to life-threatening complications in up to 10% of patients.21 This concern is particularly relevant among LT recipients, since the use of immunosuppressive agents is required to prevent graft rejection, but simultaneously increases susceptibility to infections, tumor recurrence, and de novo malignancies.22–24 Even though ICIs are largely excluded from clinical trials involving immunocompromised or transplanted patients due to concerns about graft rejection, emerging reports have started to explore their feasibility and safety in pre- and post-LT settings; however, evidence remains sparse and controversial.
Beyond ICIs, alternative immunotherapies, including T-cell and natural killer (NK) cell therapies, have also been under investigation. These therapies aim to enhance anti-tumor immunity, potentially reducing postoperative recurrence and preventing de novo malignancies.25 If proven safe and effective, these strategies could significantly improve outcomes for patients with HCC undergoing resection or LT. This review focuses on the current landscape of adjuvant immunotherapy and immuno-cell therapy during the postoperative management of HCC, highlighting ongoing clinical trials, therapeutic potential, and associated risks (Figure 1).
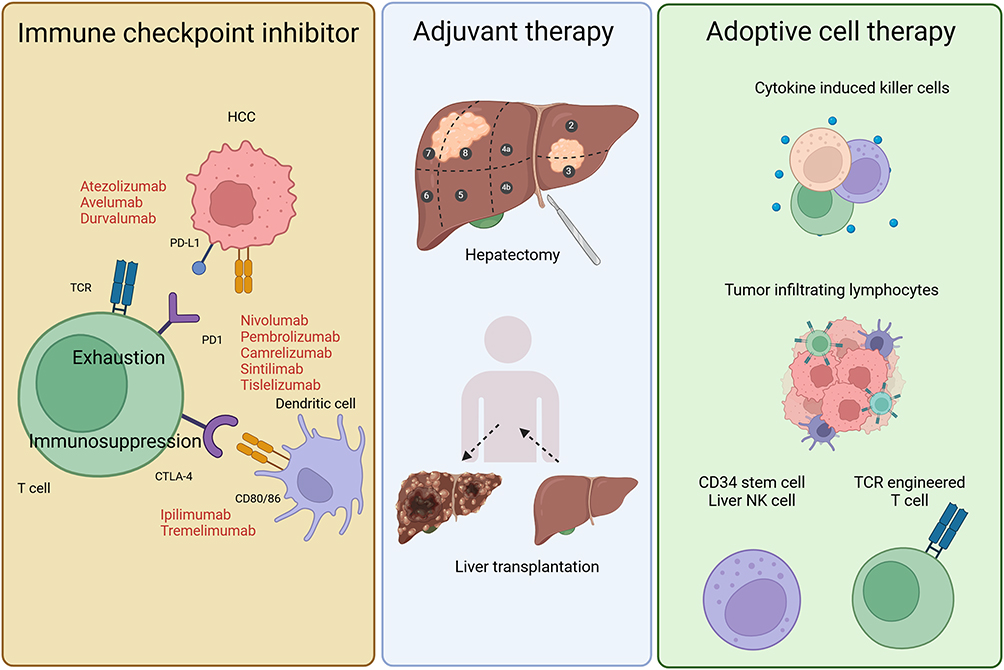 |
Figure 1 Schematic overview of adjuvant immunotherapy and adoptive immune-cell therapy in the postoperative management of hepatocellular carcinoma (HCC). This illustration summarizes the major immunotherapeutic strategies following hepatectomy or liver transplantation for HCC. Left panel (Immune checkpoint inhibitors): Immune checkpoint blockade restores T cell antitumor function by targeting PD-1/PD-L1 and CTLA-4 pathways. Agents shown include PD-1 inhibitors (nivolumab, pembrolizumab, camrelizumab, sintilimab, tislelizumab), PD-L1 inhibitors (atezolizumab, avelumab, durvalumab), and CTLA-4 inhibitors (ipilimumab, tremelimumab). These therapies aim to overcome T cell exhaustion and immunosuppression within the tumor microenvironment. Middle panel (Adjuvant therapy): Curative treatments such as hepatic resection and liver transplantation are represented. Adjuvant immunotherapies, including ICIs, are being explored to reduce recurrence after these interventions. Right panel (Adoptive cell therapy): Various immune-cell-based strategies are depicted, including cytokine-induced killer cells, tumor-infiltrating lymphocytes, CD34 stem cell-derived liver NK cells, and genetically engineered TCR T cells. These approaches aim to enhance antitumor immunity and prevent recurrence following surgery or transplantation. |
Overview of Immunotherapy for HCC
Cancer immunosurveillance is a complex and dynamic process wherein malignant cells are detected and eliminated through the coordinated activity of innate and adaptive immune responses. This process is profoundly influenced by the TME, which plays a pivotal role in shaping immune interactions. In the liver, the immunological landscape is predominantly characterized by immunosuppressive cells and signals, creating a tolerogenic microenvironment that facilitates immune evasion.26,27 Key cellular players moderating immune suppression within the TME of HCC include regulatory T cells (Tregs), Kupffer cells (liver-resident macrophages), monocyte-derived macrophages, and myeloid-derived suppressor cells (MDSCs).26 These cells collectively impair effective antitumor immunity by suppressing innate and adaptive immune responses. Dysfunctional dendritic cells and regulatory B cells further contribute to this immunosuppressive milieu, impeding robust immune activation.28,29
Tumor-associated macrophages (TAMs), which comprise a significant portion of macrophages in the HCC TME, are central to immune evasion and tumor progression. These cells exert their effects through multiple mechanisms, including the secretion of immunosuppressive cytokines, expression of PD-L1, recruitment of Tregs and Th17 cells, promotion of angiogenesis, and downregulation of pro-inflammatory cytokines.30 High TAM density has been correlated with poor prognosis among patients with HCC.31 Neutrophils also play a role in tumor progression, likely by fostering an immunosuppressive environment, enhancing tumor cell survival, remodeling the extracellular matrix, and promoting angiogenesis.32 Additionally, the liver harbors a significant population of MDSCs producing factors that inhibit T-cell activation. Patients with HCC often exhibit elevated levels of circulating MDSCs and Tregs compared to healthy individuals, further contributing to systemic immune suppression.33 Regulatory dendritic cells, through the production of IL-10, exacerbate this immunosuppressive state.28 Interestingly, B cells have a dual role in HCC immunobiology by promoting tumor development under certain conditions, while also supporting antitumor immunity via the production of tumor-targeting antibodies and activating T cells that potentially enhance response to immunotherapy.29
Importantly, angiogenesis is now recognized as a key element not only in supporting tumor vascularization but also in promoting immune evasion through modulation of the TME. Pro-angiogenic factors such as VEGF contribute to T cell dysfunction, exclusion from the tumor bed, and impaired dendritic cell maturation. These insights provide a strong mechanistic rationale for combining anti-angiogenic agents, such as tyrosine kinase inhibitors, with ICIs, as demonstrated by the clinical success of regimens like atezolizumab plus bevacizumab. This combination enhances antitumor efficacy by concurrently inhibiting angiogenesis and restoring antitumor immune responses.34 Moreover, some tyrosine kinase inhibitors, such as regorafenib, exert direct immunomodulatory effects. Regorafenib has been shown to reduce the infiltration of TAMs, suppress angiogenesis, and shift macrophage polarization from the pro-tumor M2 phenotype to the antitumor M1 phenotype, thereby further remodeling the TME to enhance immune-mediated tumor control.35 Recent profiling studies indicate that the neo-angiogenic vasculature in HCC is closely linked to an immunosuppressive milieu; regorafenib can normalize aberrant vessels, dampen macrophage-mediated suppression, and recruit effector T cells, thereby providing a clear rationale for combining this TKI with PD-1/PD-L1 blockade.
Although the liver’s TME is predominantly immunosuppressive, the presence of specific immune cells capable of eliminating cancer cells may counterbalance this effect.32,36 Key players in antitumor immunity include CD8+ T cells and both liver-resident and infiltrating NK cells.26 These cells facilitate adaptive immune responses by targeting a broad spectrum of tumor antigens, such as tumor-associated antigens (TAA) and neoantigens, which are tumor-specific antigens (TSA) that arise from genomic alterations, abnormal RNA splicing, post-translational modifications, or integrated viral elements.
Among certain malignancies, a high tumor mutational burden (TMB) has been correlated with improved responses to ICIs.37 However, this association appears less clear in HCC. Specifically, in the IMbrave 150 trial, which demonstrated a survival benefit of atezolizumab combined with bevacizumab over sorafenib as a first-line treatment for unresectable HCC, TMB showed no significant correlation with overall response rate or survival.38 The TMB distribution in HCC was narrow, with a low median of 4.4 mutations per megabase (mut/Mb). Although a small subset of HCCs with high TMB (>10 mut/Mb) might derive greater benefit from ICIs, this has not yet been definitively established.39,40 Unlike other malignancies, HCCs typically exhibit low TMB, while even high TMB does not necessarily translate to increased immune cell infiltration,39,40 potentially due to deficiencies in antigen-presentation pathways within HCC.40,41 Copy number alterations, which frequently occur in HCC, lead to the loss of genes critical for effective antigen presentation, thereby shaping the immunosuppressive nature of the TME.40 Additionally, cancer cell-intrinsic signaling pathways have demonstrated a significant role in modulating the immune microenvironment. For instance, activation of WNT–β-catenin signaling in murine models of HCC suppressed dendritic cell recruitment and impaired NK cell recognition, thus facilitating immune evasion.42 Transforming growth factor-β (TGF-β) signaling contributed to an immunosuppressive “cancer field effect” by further inhibiting antitumor immunity.43 Moreover, MYC overexpression enhanced PD-L1 expression, while TP53 mutations drove the recruitment of immunosuppressive cell populations.44 Interestingly, mutations in epigenetic regulators, which increased TMB, were paradoxically associated with reduced interferon-γ (IFN-γ) signaling, underscoring the complex interplay between genetic alterations and immune suppression in HCC.45,46
HCCs can be broadly classified as inflamed or non-inflamed based on the characteristics of their immune microenvironment. Inflamed tumors, accounting for approximately 30% of cases, are defined by robust immune cell infiltration and immune activity. These tumors exhibit increased expression of immune checkpoints, such as PD-1 and PD-L1, activation of IFN signaling pathways, and relatively low levels of large chromosomal alterations.39,40,47 On the basis of mRNA-based gene expression profiles, inflamed HCCs can be further categorized into immune-active, immune-like, and immune-exhausted subtypes.39,47 Immune-active HCCs are characterized by heightened cytolytic activity and strong activation of IFN signaling, reflecting an active immune response. Immune-like tumors also demonstrate IFN signaling but are frequently associated with CTNNB1 mutations, suggesting a unique interplay between immune activation and oncogenic signaling. Conversely, immune-exhausted tumors display features of T cell exhaustion and are marked by the activation of TGF-β signaling pathways.39,47 Patients with inflamed HCCs generally have better prognoses and are more likely to benefit from ICIs due to the presence of responsive immune cells.39,41,47 Several gene expression signatures capturing the inflamed components of the TME have been linked to favorable responses to ICIs.38,41,47–49 On the other hand, non-inflamed HCCs are associated with minimal immune cell infiltration and low immune activity in the TME.39,47 These tumors exhibit T cell exclusion and are classified into two subtypes: immune-intermediate tumors, which often harbor TP53 mutations and exhibit high chromosomal instability, and immune-excluded tumors, characterized by CTNNB1 mutations and activation of the canonical WNT signaling pathway.39,47 Patients with non-inflamed HCCs typically have limited responses to immunotherapy, demonstrating the challenges that immune evasion poses for these tumors.41,50
Immune cells express ligand-receptor checkpoints that regulate their activity, either enhancing or inhibiting effector functions. These checkpoints play a crucial role in modulating the duration and intensity of immune responses while minimizing collateral tissue damage. Stimulatory immune checkpoints, such as CD28, GITR, and OX40, promote T cell activation and proliferation, whereas inhibitory checkpoints, including PD-1, CTLA-4, LAG3, TIGIT, and TIM3, suppress immune activity to prevent overactivation.26 In the context of HCC, immunotherapy predominantly focuses on restoring antitumor immunity through ICIs, which are monoclonal antibodies targeting inhibitory checkpoints or their ligands.26 As such, the adjuvant combination of atezolizumab and bevacizumab has demonstrated efficacy in improving RFS in patients at high risk of recurrence following curative resection or local ablation.14
In HCC, immunotherapy is categorized into neoadjuvant and adjuvant approaches.51 Neoadjuvant therapies, such as bridging and downstaging strategies, have distinct objectives. In LT, bridging therapy aims to stabilize disease and reduce the risk of dropout among patients that have already met the Milan criteria, while downstaging therapies seek to decrease tumor burden, enabling patients initially outside the Milan criteria to become eligible for LT. Within this framework, neoadjuvant ICIs have emerged as a promising option, offering the potential to improve patient outcomes.52 On the other hand, adjuvant therapies focus on preventing disease recurrence following curative treatments such as hepatic resection or local ablation. Despite advancements in HCC management, the majority of patients experience recurrence or metastasis within five years of curative intervention, underscoring the critical need for effective systemic therapies in the adjuvant setting.53,54 Towards addressing this unmet need, ICIs have shown increasing promise in preventing or delaying HCC recurrence, with a growing body of evidence supporting their efficacy.26 In addition to ICIs, immune-cell-based therapies have garnered significant interest in recent years. These therapies, which include adoptive T-cell transfer and NK cell-based approaches, hold potential for clinical application. Building on these developments, the subsequent sections of this review will examine the current status of adjuvant immunotherapy and immune-cell therapy in HCC, focusing on their applications in resection and LT, with a particular emphasis on recent clinical trials.
The Role of ICIs in Adjuvant Immunotherapy After Resection for HCC
Surgical resection is widely recognized as the treatment of choice among patients with early-stage HCC who qualify as suitable candidates. For patients with early-stage disease who are not eligible for resection, LT serves as an alternative option.1,15 Despite its curative intent, surgical resection is associated with a high risk of disease recurrence, ranging from 50% to 70% within five years. The first 12 months post-resection represent the period of highest recurrence risk.55 Early recurrence often manifests as either extrahepatic or intrahepatic metastases located far from the resection margin, believed to originate from occult micrometastases that were present at the time of surgery.56,57 Tumor characteristics such as size, number, vascular invasion, grade of differentiation, and α-fetoprotein have been associated with early recurrence.58 On the contrary, late recurrence occurring more than 12 months after resection has been typically attributed to new primary tumors (de novo HCCs), potentially influenced by the underlying liver disease. Risk factors for late recurrence include patient demographics, the etiology of the underlying liver disease, and the presence of cirrhosis.59 The substantial risk of recurrence underscores the critical need for effective perioperative adjuvant therapies to reduce tumor recurrence and metastasis while improving long-term survival.
Adjuvant therapies offer several advantages compared to neoadjuvant approaches. The utilization of postoperative pathology and molecular classification can facilitate more precise patient selection and individualized treatment plans without delaying surgery. The primary candidates for adjuvant therapy are patients who have undergone surgical resection but remain at high risk for recurrence and metastasis based on tumor pathology and clinical factors. Of note, adjuvant ICIs have emerged as a promising approach to address this unmet need, based on their ability to restore and enhance antitumor immunity, thus offering potential benefits towards targeting residual microscopic disease and preventing early recurrence. In the near future, the utilization of ICIs in the postoperative setting is expected to play a pivotal role in reshaping HCC management and establishing a pathway toward improved outcomes for patients following surgical resection.
In recent years, ICIs such as anti-PD-1, anti-PD-L1, and anti-CTLA-4 antibodies have revolutionized the treatment landscape for various cancers, including HCC.11,60–62 These biologic agents enhance antitumor immunity by promoting T cell activation and enabling the immune system to effectively target and eliminate tumor cells. Ongoing clinical trials evaluating adjuvant ICIs in this population are summarized in Table 1. Importantly, early-phase studies are underway to explore novel perioperative strategies. The PRIME-HCC Phase Ib trial (NCT03682276) is evaluating the safety and tolerability of nivolumab/ipilimumab in the perioperative setting, whereas a Phase II trial (NCT03222076) is assessing the efficacy of combined perioperative nivolumab/ipilimumab versus nivolumab monotherapy.63,64 The NIVOLVE trial, a phase II multicenter study, assessed the safety and efficacy of adjuvant nivolumab in patients undergoing surgical resection or radiofrequency ablation.65 The trial reported a 1-year RFS rate of 78.6% and a median RFS of 26.3 months. Additionally, exploratory analyses identified factors such as copy number gains in WNT/β-catenin-related genes, activation of the WNT/β-catenin pathway, increased Foxp3+ cells, and low CD8+ tumor-infiltrating lymphocytes as potential markers of recurrence after adjuvant nivolumab. Several Phase III trials are investigating other ICI regimens in the adjuvant setting. These include CheckMate 9DX (adjuvant nivolumab; NCT03383458), IMbrave050 (atezolizumab plus bevacizumab; NCT04102098), KEYNOTE-937 (pembrolizumab; NCT03867084), and EMERALD-2 (durvalumab with or without bevacizumab; NCT03847428).66,67
 |
Table 1 Summary of Clinical Trials on Adjuvant Immunotherapy for Liver Resection Among Patients with Hepatocellular Carcinoma |
Notably, the global, open-label phase III IMbrave050 trial evaluated whether adjuvant therapy with atezolizumab plus bevacizumab could improve RFS compared with active surveillance in patients at high risk of recurrence after resection or local ablation.14 While initial analyses suggested a potential benefit, updated results presented at ESMO 2024 indicated that the combination did not achieve a statistically significant improvement in RFS. The trial enrolled 668 patients randomized 1:1 to either the intervention or surveillance arm. Although a previously reported hazard ratio (HR) for RFS favored the intervention group (HR 0.72, 95% CI 0.56–0.93), the updated analysis failed to confirm statistical significance, prompting a reassessment of the clinical utility of this adjuvant regimen. Treatment-related AEs occurred in 41% of patients in the intervention group compared with 13% in the surveillance group, with most events being manageable. The most common immune-related AEs included hepatitis (32% vs 15%), rash (20% vs 2%), and hypothyroidism (20% vs <1%), primarily of grade 1–2 severity.14 These findings highlight the need for refined patient selection and biomarker-based stratification to enhance the effectiveness of adjuvant immunotherapy in HCC.
Despite advancements in immunotherapy, the response rate of HCC to ICIs remains below 20%, largely due to the low immunogenicity of HCC tumors.68 The limited efficacy of ICIs is often attributed to the scarcity of tumor-infiltrating lymphocytes (TILs) in HCC, as tumors with fewer TILs—often referred to as “cold tumors”—are less responsive to immunotherapy. Although global efforts have been made to convert immunologically cold tumors into hot tumors with enhanced immune infiltration, effective strategies for HCC remain elusive.69 Peptide vaccination therapy, which aims to induce tumor antigen-specific T cells, represents one promising avenue.70 Recent studies have demonstrated the efficacy of combining hLAG-3-Ig, a fusion protein of human lymphocyte activation gene 3 (LAG-3) and immunoglobulin G1 (IgG1) Fc, with poly-ICLC, a synthetic double-stranded RNA adjuvant.71 This combination enhances immune activation by blocking inhibitory LAG-3 signaling in T cells, while simultaneously stimulating dendritic cells and monocytes via interaction with major histocompatibility complex class II molecules.72–74 Poly-ICLC further amplifies immune responses by binding to Toll-like receptor 3 and other pattern recognition receptors, inducing type I interferons and IL-12 production, and enhancing dendritic cell cross-priming.75–77 Building on these principles, a novel therapeutic vaccine was developed by combining heat shock protein 70 (HSP70) and glypican-3 (GPC3)-derived peptides with multi-human leukocyte antigen (HLA)-binding capabilities and adjuvants like poly-ICLC.78 A Phase I trial (YNP01, jRCTs061180058) involving patients with advanced gastrointestinal cancers demonstrated its safety and robust induction of peptide-specific T-cell production.79 Immunohistochemical analysis in the trial revealed HSP70 and GPC3 expression in 71% of 112 HCC cases, with at least one of these antigens expressed in 87% of tumors. Notably, three out of four enrollees with stage IVB HCC survived for over two years, qualifying as the only long-term survivors. These promising data have prompted a phase I trial (YCP02) to evaluate the vaccine’s safety as perioperative immunotherapy for resectable HCC.
Moreover, certain clinical trials have explored PD-L1 expression as a predictive marker for immunotherapy response. Elevated PD-L1 levels have been associated with poor prognosis among patients with advanced HCC.19,80,81 The ORIENT-32 trial demonstrated that sintilimab combined with IBI305 significantly improved OS and RFS compared with sorafenib in patients with unresectable, HBV-related HCC.82 Similarly, early studies on tislelizumab reported non-inferior OS compared with sorafenib, a higher objective response rate, and a more durable response, despite sorafenib showing slightly longer RFS.83 However, inter-institutional variability in PD-L1 assessment methods has led to inconsistent findings, highlighting the need for standardized techniques to measure PD-L1 expression. Additionally, understanding the temporal dynamics of PD-L1 expression and determining whether it should be measured in tumor or stromal tissues present ongoing critical challenges.84
Given the heterogeneity of HCC, tailored combination therapies are becoming essential. A meta-analysis by Li et al demonstrated that external beam radiotherapy (EBRT) combined with sorafenib improved outcomes in unresectable HCC.85 Another multicenter study by Su et al suggested that EBRT outperforms transcatheter arterial chemoembolization for HCC tumors ≥5 cm.86 Li et al also reported significant benefits when combining PD-1 inhibitors with transcatheter arterial chemoembolization.87 These findings highlight the evolving role of combination therapies in extending patient survival. Biomarkers such as alkaline phosphatase, albumin-bilirubin score, and aspartate-aminotransferase-to-platelet ratio index are emerging as useful tools for predicting prognosis and assessing treatment response.88–90 Future research is likely to focus on refining immunotherapy combinations and identifying reliable biomarkers to guide personalized treatment strategies.91,92
The Role of ICIs in Adjuvant Immunotherapy After Liver Transplantation for HCC
LT is a cornerstone treatment for HCC among patients who meet stringent selection criteria, such as the Milan Criteria. However, its widespread application is limited by donor scarcity and the significant risk of post-LT tumor recurrence, which occurs in approximately 8% to 20% of cases despite careful candidate selection.93–95 Post-LT recurrence is associated with a poor prognosis, and therapeutic options for these patients remain limited.96,97 To optimize the use of scarce donor resources, minimizing post-LT recurrence and mortality is critical. Achieving this goal necessitates precise donor-recipient matching and ongoing refinement of LT selection criteria, a topic that has been actively debated for over a decade.96,98,99
The use of ICIs in the LT setting presents unique challenges compared to ICI use in HCC resection. Unlike resection, LT patients are immunocompromised due to the use of immunosuppressive agents, especially in the critical early post-LT period. This immunosuppressive state is thought to contribute significantly to HCC recurrence, with two primary mechanisms proposed to explain how immunosuppression drives recurrence.22 The first mechanism suggests that undetectable micrometastases, present outside the liver at the time of LT, may proliferate under the influence of immunosuppressive therapy. The second posits that circulating tumor cells (CTCs) from the primary tumor can engraft in various tissues, including the allograft liver, lymph nodes, lungs, or bones.100–102 During the early post-LT period, when immunosuppression is at its peak, these cancer cells are more likely to evade immune surveillance and establish metastases. Efforts to reduce HCC recurrence post-LT have included strategies to minimize the use of immunosuppressive agents.103–106 Tacrolimus (FK506), one of the most commonly used immunosuppressive agents, has been implicated in promoting HCC cell migration and proliferation through pathways such as Rho/ROCK and Ras signaling.107–110 Additionally, CTCs may escape immune detection by expressing molecules like PD-L1, CD44, and CD47, which facilitate immune evasion.111–113 These findings suggest that modifications to immunosuppressive regimens could reduce recurrence risk to levels observed in non-transplant patients with HCC. Despite these insights, the optimal immunosuppressive protocol post-LT remains uncertain. While some centers have explored reducing exposure to calcineurin inhibitors or incorporating mammalian targets of rapamycin inhibitors to balance graft protection and tumor recurrence prevention, no consensus has been reached.24 Further translational and clinical studies are needed to develop evidence-based regimens that balance graft protection with recurrence prevention.
Emerging evidence highlights the potential of ICIs for managing HCC recurrence after LT. Patterns of recurrence indicate that approximately 11% and 56% of patients experience intrahepatic and extrahepatic recurrence, respectively, while 33% present with both.114–130 Standard immunosuppression protocols vary across centers but typically include high-dose corticosteroids immediately after liver reperfusion to broadly suppress the immune response. These steroids induce T-cell apoptosis and halt T-cell proliferation, serving as the primary treatment for severe irAEs associated with ICIs. Calcineurin inhibitors suppress T-cell activation and cytokine production, while mycophenolate inhibits T and B lymphocyte proliferation by depleting guanosine nucleotides. In recent years, there has been a growing trend towards minimizing or even eliminating steroid use following LT, a shift that has been generally associated with improved patient outcomes. Variability in early steroid use may partially explain differences in the incidence of early graft rejection reported among patients receiving ICIs prior to LT. In addition to steroids, T-cell-depleting agents, such as anti-thymocyte globulin, have been employed as part of immunosuppressive induction protocols to significantly reduce T-cell counts. While this strategy may lower the risk of ICI-related rejection, it comes with potential drawbacks. The depletion of T cells can trigger the homeostatic proliferation of surviving lymphocytes, which may generate memory T cells and complicate long-term graft tolerance.131
The timing of ICI therapy post-LT has emerged as a crucial factor influencing both rejection risk and therapeutic outcomes. Recent studies have shed light on the relationship between the interval from LT to ICI initiation and patient response.13 Shorter intervals between LT and the start of ICI therapy have been associated with a heightened risk of rejection.13 Conversely, a longer LT-to-ICI interval has been linked to improved therapeutic responses, as reflected in higher disease control rates. One study reported that the median interval from LT to ICI initiation was six years in patients who responded to ICIs, compared to three years in non-responders.13 As the post-LT period progresses, immunosuppression is typically tapered to reduce the risk of long-term complications. This reduction allows for the development of a more immune-tolerant graft environment. In patients with older grafts, the immune system may become less focused on rejecting the transplanted organ and more capable of mounting an effective antitumor response.13 These findings highlight the importance of individualized timing when considering ICI therapy in LT recipients to maximize efficacy while minimizing rejection risk.
The integration of molecularly targeted therapies with immunotherapy has become a cornerstone in the management of advanced HCC. Regulatory bodies, including the FDA, have approved the combination of the PD-L1 inhibitor atezolizumab with the VEGF inhibitor bevacizumab as a first-line systemic therapy for advanced HCC. This regimen, now recommended by the National Comprehensive Cancer Network guidelines, has replaced previous standards such as sorafenib and lenvatinib.132 Emerging evidence suggests that other combinations of targeted and immune-based therapies may further enhance treatment outcomes. The pairing of lenvatinib with pembrolizumab has shown significantly higher response rates compared to pembrolizumab monotherapy, although this benefit is accompanied by an increased incidence of toxicities.18 Tyrosine kinase inhibitors such as sorafenib, regorafenib, and lenvatinib not only target VEGFR signaling but also exhibit immune-modulating properties that complement immunotherapy.133 Sorafenib has been shown to enhance antitumor immune responses by promoting CD4+ and CD8+ T-cell activation and infiltration while suppressing Tregs.134,135 These immune-enhancing effects position tyrosine kinase inhibitors as valuable partners in combination therapies. The potential for synergistic effects between tyrosine kinase inhibitors and ICIs has been highlighted in specific clinical scenarios. A case study described the treatment of a patient with HCC who developed metastatic lung lesions following LT. Initially treated with sorafenib monotherapy, the patient’s disease progressed after one year. However, the subsequent addition of pembrolizumab resulted in a complete response, with no evidence of allograft rejection.121 This case underscores the potential of combining tyrosine kinase inhibitors with PD-1 inhibitors to achieve superior antitumor effects, even in complex post-LT settings where monotherapy has limited efficacy.
While maintaining immunological tolerance is essential to prevent allograft rejection, ICIs activate cellular immunity, potentially disrupting this delicate balance. This activation can lead to T-cell-mediated rejection, making ICIs traditionally contraindicated among LT recipients.136 Preclinical models have highlighted the risks associated with ICIs in LT. In animal studies, blockade of the PD-1/PD-L1 pathway or the use of PD-L1 knockout liver allografts resulted in acute rejection characterized by increased T-cell infiltration, hemorrhage, and necrosis.137 Similarly, inhibition of CTLA-4 exacerbated lymphocyte infiltration and enhanced cytotoxic T lymphocyte and NK cell activity, thereby increasing the likelihood of rejection.138 As such, the role of ICIs in the setting of managing de novo or recurrent tumors in LT recipients is an area of active investigation.139,140
Specifically, the development of de novo malignancies following LT represents a significant long-term concern for recipients. Data from the United States Scientific Registry of Transplant Recipients, encompassing over 108,000 LT recipients between 1987 and 2015, estimated the cumulative incidence of de novo extrahepatic cancers to be approximately 1.3% within the first year and up to 18.8% at 20 years post-LT.141 Of note, compared to HCC recurrence, de novo cancers typically have a longer latency period before onset.142 Common de novo malignancies in LT recipients include non-Hodgkin’s lymphoma, keratinocyte skin cancers (basal cell carcinoma and squamous cell carcinoma), cervical cancer, and head and neck cancers. Preventative strategies such as careful immunosuppression management, regular cancer screenings (eg, dermatologic evaluations and Pap smears), and minimizing sun exposure are recommended to facilitate early detection and intervention.143,144 Emerging evidence suggests differential responses to ICIs between de novo malignancies and recurrent HCC in LT recipients. A systematic review reported better disease control rates for de novo malignancies treated with ICIs compared to recurrent HCC.13 However, graft rejection rates in the de novo cancer group (21.4%) were similar to those observed in patients with post-LT HCC recurrence. These findings highlight that further studies are needed to refine the use of ICIs in this population and manage the associated risks effectively.142
Off-label use of ICIs in LT recipients has yielded insights into their safety and efficacy. Histological analysis of PD-L1 expression has been proposed as a potential biomarker for rejection risk, with some studies reporting higher rejection rates in PD-L1-positive cases. However, PD-L1 staining alone is not yet a reliable predictor of rejection or therapeutic response.13,125,145 For example, one case study detailed a patient with recurrent HCC post-LT who was treated with atezolizumab and bevacizumab. Despite negative PD-L1 staining on a pre-treatment biopsy, the patient tolerated two cycles of therapy before experiencing tumor progression.125 Such examples underscore the need for further research to clarify the role of ICIs in LT recipients, including the timing of therapy, the utility of biopsy-based biomarkers, and the most effective methods for assessing treatment response.
Numerous clinical trials are currently investigating the role of ICIs in managing HCC recurrence following LT. A summary of these ongoing studies is presented in Table 2. Trials such as NCT03966209 and NCT04564313 are evaluating the safety and efficacy of ICIs in this challenging clinical setting. ICIs, particularly in combination with other treatments, have shown superior OS compared to tyrosine kinase inhibitors, solidifying their status as first-line therapeutic options for advanced HCC. Tyrosine kinase inhibitors exert their antitumor effects by inhibiting tyrosine kinase receptors, thereby blocking downstream signaling pathways, promoting apoptosis, and exerting anti-angiogenic effects within the TME.146 Sorafenib, a small molecule tyrosine kinase receptor, was the first treatment for advanced HCC to gain FDA approval, following the results of the landmark SHARP trial in 2008.147 Cabozantinib, another tyrosine kinase receptor, has since been approved as a second-line therapy for advanced HCC.148 Emerging combination therapies are also showing promise in intermediate-stage HCC. The phase III Emerald-1 trial demonstrated that combining durvalumab, bevacizumab, and transarterial chemoembolization significantly improved objective response rates and RFS compared to transarterial chemoembolization alone.149 These findings suggest that integrating ICIs with locoregional treatments may offer a superior strategy for managing intermediate-stage HCC. Additionally, small-scale clinical trials have reported positive outcomes for ICI-based therapies in early-stage resectable HCC.64,150,151 These studies reflect the expanding application of ICIs across the HCC treatment spectrum, from early-stage surgical candidates to advanced and post-transplant cases.
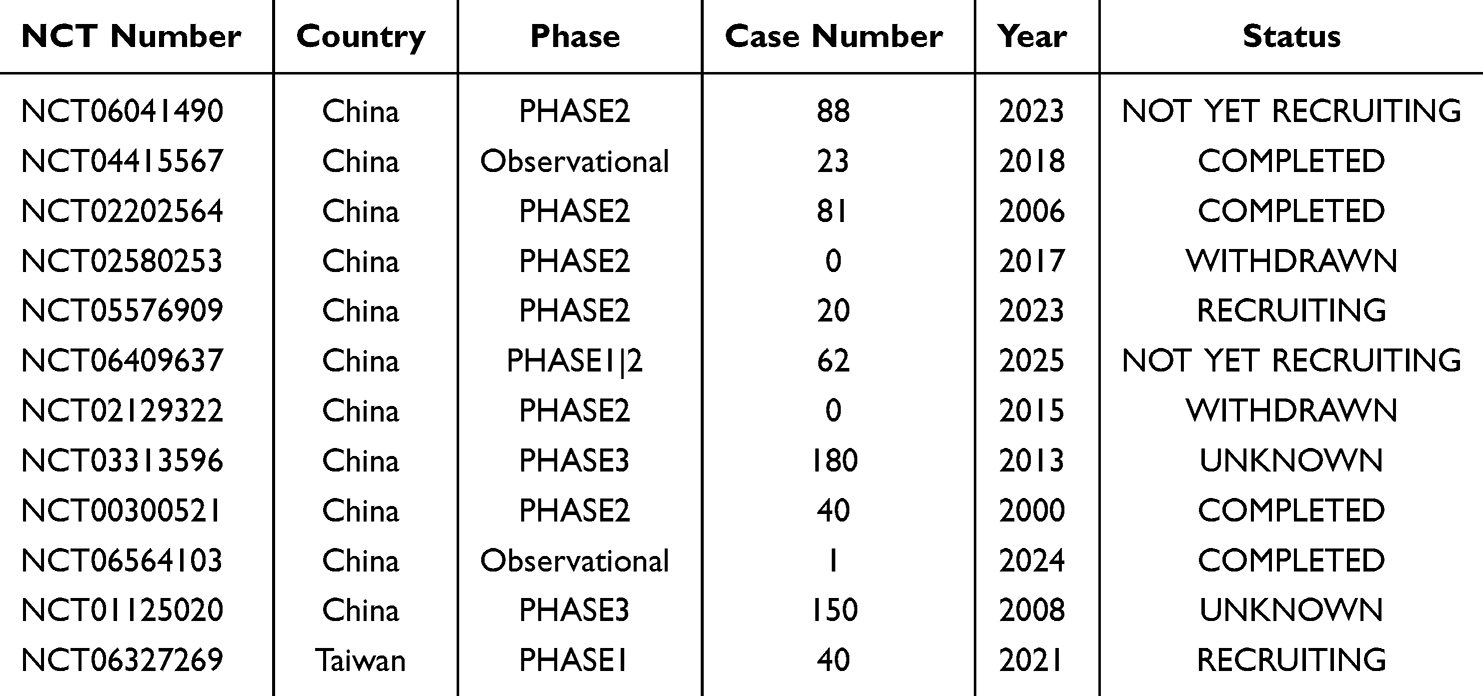 |
Table 2 Summary of Clinical Trials on Adjuvant Immunotherapy for Liver Transplantation Among Patients with Hepatocellular Carcinoma |
Recommendations for addressing graft rejection in LT recipients treated with ICIs are largely derived from protocols developed for managing ICI-induced liver toxicity in native livers.152 Recent studies emphasize the importance of liver biopsy in patients presenting with grade 2 or higher liver toxicity—defined by alanine aminotransferase or aspartate aminotransferase levels exceeding three times the upper limit of normal, or bilirubin levels exceeding 1.5 times the upper limit of normal.153 Biopsy not only confirms and grades histological rejection but also excludes alternative causes of liver injury. For cases of mild rejection, oral prednisone at 0.5–1.0 mg/kg/day is typically recommended. In moderate to severe rejection, intravenous methylprednisolone at 1–2 mg/kg/day is the preferred treatment. Corticosteroid therapy resolves liver toxicity within 5–9 weeks, correlating with the terminal half-life of most ICIs, which ranges from 15 to 27 days.154,155 Patients who do not respond to corticosteroids may require additional immunosuppressive therapies, including mycophenolate mofetil, cyclosporine, tacrolimus, anti-thymocyte globulin, or targeted agents such as tocilizumab (an IL-6 receptor antagonist) and infliximab, while plasmapheresis may also be considered in refractory cases.152 Of note, salvage re-LT may be an option in situations of irreversible allograft failure, provided the underlying malignancy does not contraindicate LT.
Emerging data indicate that anti-PD-1 therapies may elicit stronger rejection responses compared to other ICIs.156,157 This observation has led some experts to suggest anti-CTLA-4 therapies as a safer alternative for patients where preserving graft function is paramount. Preliminary studies suggest that anti-PD-1 and anti-CTLA-4 therapies may exhibit synergistic effects, with combination treatments occasionally demonstrating superior efficacy compared to monotherapy.158–160 However, combining these therapies did not appear to confer a significant survival benefit over monotherapy in other reports and was associated with increased risks of toxic side effects, making concurrent or sequential use less favorable.161,162 While anti-PD-1/PD-L1 agents have demonstrated slightly better efficacy in some studies compared to anti-CTLA-4 therapies, the difference was not statistically significant.163 Thus, the increased toxicity associated with combination regimens necessitates careful consideration, and conflicting results regarding overall survival benefits underscore the need for further investigation. The mechanisms underlying the PD-1 and CTLA-4 pathways exhibit both similarities and differences.164,165 The PD-1 pathway primarily regulates effector T cell activity in peripheral tissues and tumors by inhibiting the interaction between PD-1 and PD-L1, thereby enhancing antitumor immune responses.166–168 In contrast, the CTLA-4 pathway acts during the initial T cell activation phase, where CTLA-4 competes with CD28 for binding to CD80/CD86, dampening T cell activation. Anti-CTLA-4 therapies block this inhibitory interaction, thereby facilitating CD28-mediated activation.169,170 Both pathways are also highly expressed in Tregs, which enhance their immunosuppressive functions via increased Foxp3 expression.60,171–173 There are notable intersections between the PD-1 and CTLA-4 pathways. Both therapies elevate IL-2 levels, thus activating donor-specific T cells, enhancing cytotoxic activity, and reducing apoptosis from allogeneic reactivity.164 Additionally, these agents induce phosphorylation within the T cell receptor signaling pathway, which suppresses downstream activation signals and prevents excessive T cell activation.174 Both pathways also modulate immune responses through Tregs, contributing to their overlapping mechanisms of action. Further research is needed to elucidate the interplay between these pathways, optimize graft rejection management, and balance tumor immunity with graft tolerance in LT recipients, particularly in light of these sometimes conflicting findings regarding combination therapy.
The relationship between irAEs and post-LT outcomes is a crucial consideration in patient management.175–193 The efficacy of ICIs is tempered by irAEs, which affect up to 70% of patients and result from the restoration of antitumor immunity, often disrupting self-tolerance.194 Of note, liver injury is among the most common irAEs, occurring in approximately one out of four patients. This condition is typically managed with corticosteroids as first-line therapy, and additional immunosuppressive drugs are used for more severe or refractory cases.195 Recently, ICI-induced cholangitis has emerged as a notable irAE. While most irAEs occur within the initial months of therapy, late-onset toxicities—sometimes arising after discontinuation of ICIs—have also been documented. Management strategies for irAEs generally involve pausing or permanently stopping ICI therapy and administering steroids for grade 2 or higher toxicities. Prompt recognition and treatment of irAEs are essential for the optimization of outcomes among LT recipients receiving ICIs.
Determining which LT recipients can safely receive ICIs is an area of growing interest, with efforts focused on balancing immunological risks and oncological benefits. One potential approach involves using PD-L1 expression levels in transplanted livers as a biomarker for safety, as suggested by retrospective analyses and small prospective studies. While promising, the clinical utility of PD-L1 as a predictive tool remains inconclusive and requires further validation. Recent work has introduced a comprehensive framework for guiding ICI administration in LT recipients.153 This model incorporates a detailed evaluation of immunological risk factors, including the time elapsed since LT, patient demographics such as age and sex, the underlying etiology of liver disease, the presence of donor-specific antigens, prior episodes of graft rejection, baseline transaminase levels, and the extent of liver fibrosis. Oncological benefits are assessed by considering tumor stage, survival improvements, and quality-of-life enhancements demonstrated in randomized controlled trials, alongside the patient’s overall performance status and comorbidities. Based on these parameters, patients are stratified into categories to recommend the optimal course of treatment. While ICIs may be cautiously prescribed in some cases with rigorous monitoring, they may be strongly discouraged or replaced with alternative therapies in others, depending on the risk-benefit profile.153 The therapeutic potential of ICIs in this population is supported by pooled analyses, which report a disease control rate of 44.2% among LT recipients treated with these therapies. Patients who responded to ICIs exhibited significantly longer OS, with a median of 26.4 months compared to 3.4 months for non-responders.13 Despite these encouraging outcomes, the evidence remains insufficient to draw definitive conclusions due to limitations such as small sample sizes and heterogeneity in study designs. To establish ICIs as a viable therapeutic option for LT recipients, further research is essential. Large, well-controlled studies are needed to confirm safety and efficacy, as well as to refine and standardize clinical guidelines.
Adjuvant Immuno-Cell Therapy After Resection for HCC
Adoptive cell therapy (ACT) represents an innovative and potent approach to cancer treatment, aiming to enhance the antitumor capabilities of immune cells. This therapeutic modality involves the ex vivo process of sensitizing and expanding lymphocytes, either autologous or allogeneic, before reinfusing them into the patient.196 This represents a highly personalized cancer therapy, since the effector cells in ACT predominantly originate from the patient’s immune system. The primary strategies employed in ACT include T cells expressing chimeric antigen receptors (CAR), T cells engineered with tumor-specific T cell receptors (TCR), cytokine-induced killer (CIK) cells, TILs, lymphokine-activated killer (LAK) cells, and NK cells.196,197 Although ACT has primarily been applied to hematologic malignancies, its success has encouraged researchers to explore its applicability in solid tumors, including HCC.198 In the context of HCC, ACT is predominantly used for advanced or unresectable cases, while its use as an adjuvant therapy to prevent postoperative recurrence remains limited. Table 3 summarizes clinical trials, as reported on clinicaltrials.gov, investigating the role of ACT as an adjuvant therapy for HCC, and highlights these developments.
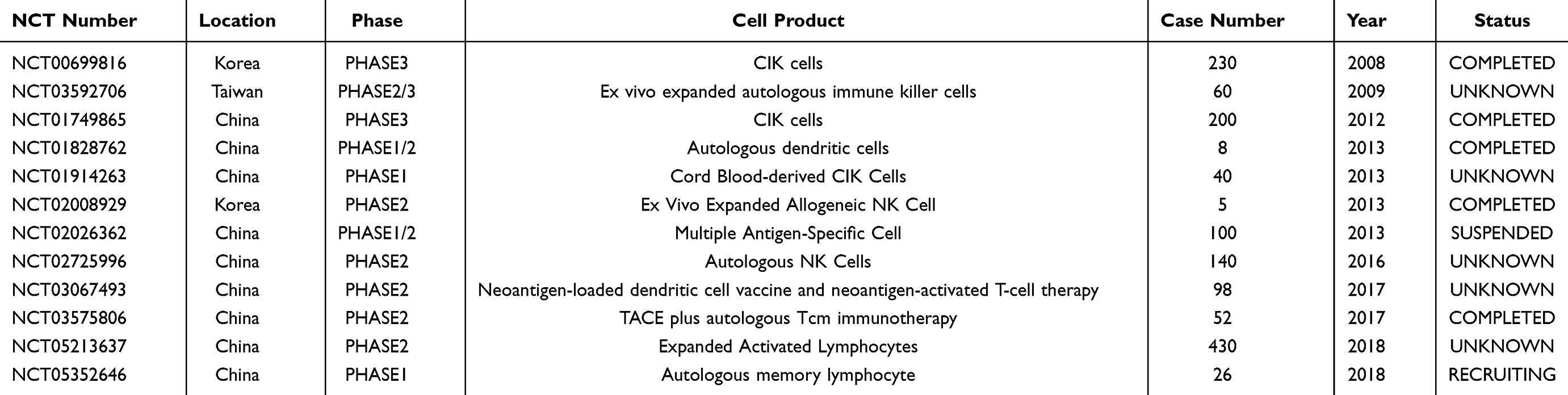 |
Table 3 Summary of Clinical Trials on Adjuvant Immuno-Cell Therapy for Liver Resection Among Patients with Hepatocellular Carcinoma |
Among ACT modalities that do not involve genetic modification, CIK cells, TILs, and NK cells are noteworthy. CIK cells, which are CD3+CD56+ NK-like T cells, exhibit non-MHC-restricted cytotoxicity and proliferation capabilities. TILs, on the other hand, consist of polyclonal tumor-targeting T cells expanded ex vivo for use as autologous therapy. NK cell therapies are divided into several groups based on whether they were derived from peripheral blood, tissue-resident cells, apheresis-derived products, or umbilical cord blood. Recent advances in genetic engineering technologies have enabled the modification of immune cells with synthetic receptors, such as CAR-T and TCR-T, thereby enhancing the visibility of TAAs and TSAs. The antigens targeted by ACT for HCC are categorized into three main groups: TAAs (eg, AFP and GPC-3), virus-derived cancer antigens (eg, HBV and HCV), and cancer-testis antigens (eg, NY-ESO-1 and MAGE).197
For the generation of CIK cells, IL-2, IFN-α, and anti-CD3 monoclonal antibodies are utilized to stimulate peripheral blood mononuclear cells (PBMCs) under laboratory conditions.199 CIK cells predominantly comprise NK cells, NKT cells, and cytotoxic T lymphocytes (CTLs). Through adhesion molecules, CIK cells can recognize tumor cells independently of MHC and lyse them. Takayama et al conducted a clinical trial involving 150 postoperative HCC patients and reported an 18% reduction in recurrence rates in the treatment group compared to the control group, with no significant AEs observed.200 A multicenter, randomized, non-blinded phase III trial assessed the efficacy and safety of adjuvant immunotherapy with activated CIK cells among 230 patients who underwent curative therapies for HCC, such as surgical resection, radiofrequency ablation, or percutaneous ethanol injection. While the incidence of severe AEs did not significantly differ between groups (7.8% vs 3.5%; P=0.15), adjuvant therapy with activated CIK cells improved RFS and OS rates.201 On the contrary, a single-institution, randomized, non-blinded phase III trial involving 200 patients who underwent curative resection failed to demonstrate improvements in disease-free survival or OS.202 While the utility of CIK therapy continues to be investigated across various HCC treatment settings, its potential remains promising.203–210
TILs represent a component of the host immune response against tumors and comprise T cells, Tregs, NK cells, and B cells.211 TILs are harvested from surgically resected tumor tissues and demonstrate superior antitumor efficacy compared to drugs targeting specific antigens or mutations, as they can detect multiple antigens. A phase I clinical trial involving 17 patients who underwent hepatectomy for primary HCC confirmed the safety of TIL therapy.212 Similar to other solid tumors, immune infiltration significantly impacts postoperative survival in HCC, warranting further clinical trials to validate its potential.213
CAR-T therapy, a focus of current ACT research, involves genetically engineering T cells to recognize specific TAAs, representing a novel immunotherapeutic approach against cancer.214 Although CAR-T therapy as an adjuvant treatment for postoperative HCC has not yet progressed to clinical trials, preclinical studies and clinical trials have identified potential target antigens, such as mucin-1, GPC-3, AFP, NKG2D ligands, and c-MET.214 However, the migration of CAR-T cells to tumor sites is critical for achieving cytolytic effects.215 This remains a challenge as T cells lack chemokine receptors,216 and the dense fibrotic structure of HCC tissues reduces chemokine expression, significantly impairing the ability of CAR-T cells to infiltrate tumors.217,218 The technology used to produce CAR-T cells can also generate CAR-NK cells. Compared to CAR-T cells, CAR-NK cells have a shorter lifespan, potentially reducing the risks of autoimmunity and tumorigenicity.219 While CAR-NK cells have been investigated in clinical trials for leukemia, lymphoma, and some solid tumors, no trials have yet evaluated their efficacy in treating HCC.
A phase I trial is currently underway investigating the infusion of peripheral blood CD34+ stem cell-derived NK cells in patients with high-risk recurrent HCC following curative hepatectomy.220 NK cell-based therapies can be categorized into approaches utilizing primary peripheral blood NK cells, apheresis-derived products, or umbilical cord blood. Peripheral blood NK cells are readily accessible and widely used but are less amenable to functional enhancement due to their mature state and short lifespan. Furthermore, NK cell activity in patients with cirrhosis or HCC is already depleted, making them less favorable for therapeutic use.221–223 In contrast, methods producing NK cells from hematopoietic stem cells via apheresis are unaffected by the underlying disease and yield NK cells with promising activity. In cases where alternative sources are used, graft-versus-host disease poses a significant risk, necessitating the removal of T cells to prevent rapid elimination of infused NK cells.224
In summary, ACT has demonstrated significant potential in cancer therapy, and ongoing advancements continue to broaden its applicability, particularly in solid tumors such as HCC. Future research efforts should aim to overcome existing challenges and establish safer, more effective treatment modalities.
Adjuvant Immuno-Cell Therapy After Liver Transplantation for HCC
ACT among LT recipients requires careful consideration due to the unique immunological environment post-transplantation. Of note, the immunosuppression necessary to prevent graft rejection by suppressing adaptive immunity paradoxically increases the risk of tumor recurrence. To address this issue, studies have investigated the potential use of CAR T-cell immunotherapy targeting TAAs, demonstrating potent antitumor effects. Nevertheless, the occurrence of severe AEs, such as neurotoxicity and cytokine release syndrome (CRS), has limited its application in LT settings.225,226 On the other hand, the feasibility of hepatitis B virus-specific T-cell receptor (HBV-TCR) engineered T-cell therapy for recurrent HCC post-transplantation has been reported, with Phase I clinical trials confirming its safety.114,227 Notably, no participants in these trials exhibited CRS or neurotoxicity. Unlike CAR-T cell therapy, CAR-NK cell therapy has been associated with a minimal risk of neurotoxicity and CRS, making it a more viable option for LT patients.228 However, clinical trials for CAR-NK therapy in this context have not yet been conducted.
Autologous CIK cell therapy has demonstrated significant improvements in RFS and OS among HCC patients following curative treatment.201,229 The main advantage of CIK cells is that they can be administered multiple times after surgery. Based on this approach, a phase I/II trial is currently underway to evaluate the application of these techniques as adjuvant therapy after LT for HCC (NCT03983967). At present, this group’s research is the most advanced and is closest to clinical application. A search of the ClinicalTrials.gov clinical trial registry revealed that there are currently seven clinical trials underway or completed in the United States and East Asia related to cell therapy for HCC after LT. (Table 4)
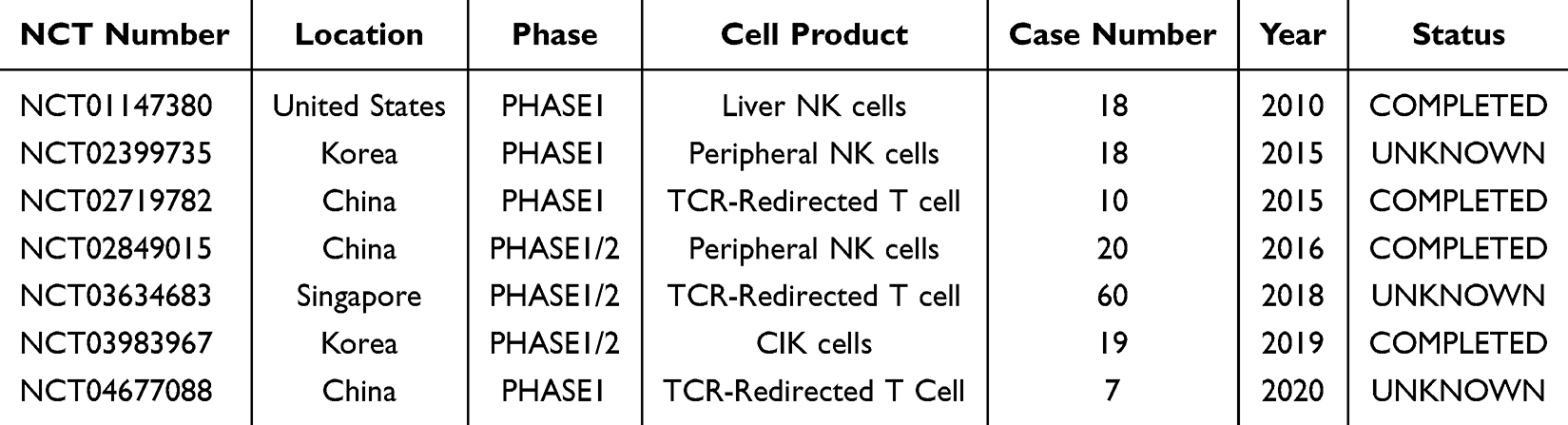 |
Table 4 Summary of Clinical Trials on Adjuvant Immuno-Cell Therapy for Liver Transplantation Among Patients with Hepatocellular Carcinoma |
Importantly, in organ transplantation, immunosuppressive therapy primarily targets the adaptive immune system, specifically T and B lymphocytes, while relatively sparing the innate immune system, including NK cells. Consequently, NK cells serve as a crucial defense mechanism after LT, protecting recipients from infections and potential malignancies.230,231 Researchers in Japan and the United States have been conducting clinical trials to evaluate the potential of NK cell-based therapies in preventing HCC recurrence post-LT.25,232 Notably, these trials have reported no severe AEs such as acute rejection or graft-versus-host disease (GVHD), which were initially concerns associated with cell-based therapies. Furthermore, complication rates were comparable between high-dose and low-dose groups, demonstrating the safety of adoptive liver NK cell therapy.
These research groups have employed a distinctive approach, focusing on liver-resident NK cells rather than peripheral blood-derived NK cells. The greatest advantage lies in the fact that liver perfusate, which was previously discarded at LT, contains an abundant source of liver-derived lymphocytes. This eliminates concerns regarding material supply shortages, making it a highly sustainable resource for therapeutic applications. Liver-resident NK cells exhibit superior antitumor activity against HCC cells, primarily through the tumor necrosis factor-related apoptosis-inducing ligand (TRAIL) receptor pathway, conferring higher antitumor efficacy compared to peripheral NK cells.233–235 The expression of TRAIL and the NK activation receptor NK group 2 member D (NKG2D) has been correlated with the cytotoxicity of liver NK cells against tumor cell lines.236 Interestingly, an exploratory study involving 77 Japanese patients with HCC post-LT evaluated the impact of donor-derived NK cells on recurrence prevention. The findings revealed significantly improved outcomes in patients with mismatched NK cell genotypes, particularly those involving specific interactions between killer immunoglobulin-like receptors (KIR) and human leukocyte antigens. These results highlight the potential of donor liver-derived NK cell-based immunotherapy for achieving favorable outcomes in such patients.237
Globally, early-phase clinical trials utilizing donor-derived liver NK cells, HBV-TCR-engineered T-cells, and CIK cells have shown promising results regarding safety and efficacy in preventing recurrence. Advances in molecular engineering are expected to further drive the development of TCR-T, CAR-T, and CAR-NK therapies, particularly in addressing the unique immunological challenges of HCC patients post-LT. These advancements aim to reduce toxicity and enhance the antitumor cytotoxicity while expanding clinical applicability in this LT patient population for HCC.
Conclusion
In conclusion, advances in immunotherapy have ushered in a new era of potential breakthroughs in the postoperative management of HCC. Both ICIs and immune-cell therapies have demonstrated promising roles in reducing recurrence and improving survival among patients undergoing resection or LT. However, significant challenges remain, including the low immunogenicity of HCC, the immunosuppressive TME, and the complexities of balancing graft tolerance with antitumor immunity in LT recipients. Emerging strategies, such as tailored combination therapies, ACT, and innovative approaches like liver-resident NK cell-based therapies, are expanding the horizon of clinical applicability. Continued efforts to refine immunotherapeutic regimens, identify predictive biomarkers, and enhance safety profiles are critical for translating these advancements into durable clinical benefits. Equally important will be future studies focused on the characterization and validation of prognostic biomarkers that can guide risk stratification and enable truly personalized immunotherapeutic strategies tailored to the heterogeneity of HCC. As ongoing and future clinical trials address these challenges, the integration of immunotherapy into standard treatment paradigms holds immense promise for transforming outcomes in HCC.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors declared that there are no conflicts of interest.
References
1. Galle PR, Forner A, Llovet JM, et al. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2018;69:182–236.
2. Akabane M, Kawashima J, Woldesenbet S, et al. Analyzing the interaction between time to surgery and tumor burden score in hepatocellular carcinoma. J Gastrointest Surg. 2024;29(2):101903. doi:10.1016/j.gassur.2024.101903
3. Fu Y, Guo X, Sun L, et al. Exploring the role of the immune microenvironment in hepatocellular carcinoma: implications for immunotherapy and drug resistance. Elife. 2024;13:e95009.
4. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
5. Jackson R, Psarelli -E-E, Berhane S, Khan H, Johnson P. Impact of viral status on survival in patients receiving sorafenib for advanced hepatocellular cancer: a meta-analysis of randomized phase III trials. J Clin Oncol. 2017;35(6):622–628. doi:10.1200/JCO.2016.69.5197
6. Teixeira Farinha H, Digklia A, Schizas D, Demartines N, Schäfer M, Mantziari S. Immunotherapy for esophageal cancer: state-of-the art in 2021. Cancers. 2022;14(3):554. doi:10.3390/cancers14030554
7. Mamdani H, Matosevic S, Khalid AB, Durm G, Jalal SI. Immunotherapy in lung cancer: current landscape and future directions. Front Immunol. 2022;13:823618. doi:10.3389/fimmu.2022.823618
8. Kole C, Charalampakis N, Tsakatikas S, et al. Immunotherapy for gastric cancer: a 2021 update. Immunotherapy. 2022;14(1):41–64. doi:10.2217/imt-2021-0103
9. Llovet JM, De Baere T, Kulik L, et al. Locoregional therapies in the era of molecular and immune treatments for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(5):293–313. doi:10.1038/s41575-020-00395-0
10. Qin S, Bi F, Gu S, et al. Donafenib versus sorafenib in first-line treatment of unresectable or metastatic hepatocellular carcinoma: a randomized, open-label, parallel-controlled Phase II-III trial. J Clin Oncol. 2021;39(27):3002–3011. doi:10.1200/JCO.21.00163
11. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. New England J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
12. Llovet JM, Montal R, Sia D, Finn RS. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 2018;15(10):599–616. doi:10.1038/s41571-018-0073-4
13. Kayali S, Pasta A, Plaz Torres MC, et al. Immune checkpoint inhibitors in malignancies after liver transplantation: a systematic review and pooled analysis. Liver Int. 2023;43(1):8–17. doi:10.1111/liv.15419
14. Qin S, Chen M, Cheng A-L, et al. Atezolizumab plus bevacizumab versus active surveillance in patients with resected or ablated high-risk hepatocellular carcinoma (IMbrave050): a randomised, open-label, multicentre, phase 3 trial. The Lancet. 2023;402(10415):1835–1847. doi:10.1016/S0140-6736(23)01796-8
15. Singal AG, Llovet JM, Yarchoan M, et al. AASLD practice guidance on prevention, diagnosis, and treatment of hepatocellular carcinoma. Hepatology. 2023;78(6):1922–1965. doi:10.1097/HEP.0000000000000466
16. Li Z, Liu J, Zhang B, et al. Neoadjuvant tislelizumab plus stereotactic body radiotherapy and adjuvant tislelizumab in early-stage resectable hepatocellular carcinoma: the Notable-HCC phase 1b trial. Nat Commun. 2024;15(1):3260. doi:10.1038/s41467-024-47420-3
17. Granito A, Muratori L, Lalanne C, et al. Hepatocellular carcinoma in viral and autoimmune liver diseases: role of CD4+ CD25+ Foxp3+ regulatory T cells in the immune microenvironment. World J Gastroenterol. 2021;27(22):2994–3009. doi:10.3748/wjg.v27.i22.2994
18. Finn RS, Ikeda M, Zhu AX, et al. Phase Ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. J Clin Oncol. 2020;38(26):2960–2970. doi:10.1200/JCO.20.00808
19. Yau T, Kang Y-K, Kim T-Y, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the CheckMate 040 randomized clinical trial. JAMA Oncol. 2020; 6:e204564–e.
20. Wang Z, Wang Y, Gao P, Ding J. Immune checkpoint inhibitor resistance in hepatocellular carcinoma. Cancer Lett. 2023;555:216038. doi:10.1016/j.canlet.2022.216038
21. Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. New England J Med. 2018;378(2):158–168. doi:10.1056/NEJMra1703481
22. Kojima L, Akabane M, Murray M, et al. Reappraisal of tacrolimus levels post liver transplant for hepatocellular carcinoma: a multicenter study toward personalized immunosuppression regimen. Liver Transpl. 2024;31(3):344–354. doi:10.1097/LVT.0000000000000459
23. Euvrard S, Kanitakis J, Claudy A. Skin cancers after organ transplantation. New England J Med. 2003;348(17):1681–1691. doi:10.1056/NEJMra022137
24. Lai Q, Iesari S, Finkenstedt A, et al. Hepatocellular carcinoma recurrence after acute liver allograft rejection treatment: a multicenter European experience. Hepatobiliary Pancreat Dis Int. 2019;18(6):517–524. doi:10.1016/j.hbpd.2019.05.006
25. Ohira M, Hotta R, Tanaka Y, et al. Pilot study to determine the safety and feasibility of deceased donor liver natural killer cell infusion to liver transplant recipients with hepatocellular carcinoma. Cancer Immunol Immunotherap. 2022;1:1–11.
26. Llovet JM, Castet F, Heikenwalder M, et al. Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol. 2022;19(3):151–172. doi:10.1038/s41571-021-00573-2
27. Ringelhan M, Pfister D, O’Connor T, Pikarsky E, Heikenwalder M. The immunology of hepatocellular carcinoma. Nat Immunol. 2018;19(3):222–232. doi:10.1038/s41590-018-0044-z
28. Han Y, Chen Z, Yang Y, et al. Human CD14+ CTLA‐4+ regulatory dendritic cells suppress T‐cell response by cytotoxic T‐lymphocyte antigen‐4‐dependent IL‐10 and indoleamine‐2, 3‐dioxygenase production in hepatocellular carcinoma. Hepatology. 2014;59(2):567–579. doi:10.1002/hep.26694
29. Finkin S, Yuan D, Stein I, et al. Ectopic lymphoid structures function as microniches for tumor progenitor cells in hepatocellular carcinoma. Nat Immunol. 2015;16(12):1235–1244. doi:10.1038/ni.3290
30. Zheng C, Zheng L, Yoo J-K, et al. Landscape of infiltrating T cells in liver cancer revealed by single-cell sequencing. Cell. 2017;169(7):1342–56.e16. doi:10.1016/j.cell.2017.05.035
31. Zhang Q, He Y, Luo N, et al. Landscape and dynamics of single immune cells in hepatocellular carcinoma. Cell. 2019;179(4):829–45.e20. doi:10.1016/j.cell.2019.10.003
32. Geh D, Leslie J, Rumney R, Reeves HL, Bird TG, Mann DA. Neutrophils as potential therapeutic targets in hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2022;19(4):257–273. doi:10.1038/s41575-021-00568-5
33. Hoechst B, Ormandy LA, Ballmaier M, et al. A new population of myeloid-derived suppressor cells in hepatocellular carcinoma patients induces CD4+ CD25+ Foxp3+ T cells. Gastroenterology. 2008;135(1):234–243. doi:10.1053/j.gastro.2008.03.020
34. Stefanini B, Ielasi L, Chen R, et al. TKIs in combination with immunotherapy for hepatocellular carcinoma. Expert Rev Anticancer Ther. 2023;23(3):279–291. doi:10.1080/14737140.2023.2181162
35. Granito A, Forgione A, Marinelli S, et al. Experience with regorafenib in the treatment of hepatocellular carcinoma. Therap Adv Gastroenterol. 2021;14:17562848211016959. doi:10.1177/17562848211016959
36. Ramadori P, Kam S, Heikenwalder M. T cells: friends and foes in NASH pathogenesis and hepatocarcinogenesis. Hepatology. 2022;75(4):1038–1049. doi:10.1002/hep.32336
37. Samstein RM, Lee C-H, Shoushtari AN, et al. Tumor mutational load predicts survival after immunotherapy across multiple cancer types. Na Gene. 2019;51(2):202–206. doi:10.1038/s41588-018-0312-8
38. Zhu AX, Abbas AR, de Galarreta MR, et al. Molecular correlates of clinical response and resistance to atezolizumab in combination with bevacizumab in advanced hepatocellular carcinoma. Nat Med. 2022;28(8):1599–1611. doi:10.1038/s41591-022-01868-2
39. Sia D, Jiao Y, Martinez-Quetglas I, et al. Identification of an immune-specific class of hepatocellular carcinoma, based on molecular features. Gastroenterology. 2017;153(3):812–826. doi:10.1053/j.gastro.2017.06.007
40. Bassaganyas L, Pinyol R, Esteban-Fabró R, et al. Copy-number alteration burden differentially impacts immune profiles and molecular features of hepatocellular carcinoma. Clin Cancer Res. 2020;26(23):6350–6361. doi:10.1158/1078-0432.CCR-20-1497
41. Haber PK, Castet F, Torres-Martin M, et al. Molecular markers of response to anti-PD1 therapy in advanced hepatocellular carcinoma. Gastroenterology. 2023;164(1):72–88.e18. doi:10.1053/j.gastro.2022.09.005
42. de Galarreta M R, Bresnahan E, Molina-Sánchez P, et al. β-catenin activation promotes immune escape and resistance to anti–PD-1 therapy in hepatocellular carcinoma. Cancer Discovery. 2019;9(8):1124–1141. doi:10.1158/2159-8290.CD-19-0074
43. Moeini A, Torrecilla S, Tovar V, et al. An immune gene expression signature associated with development of human hepatocellular carcinoma identifies mice that respond to chemopreventive agents. Gastroenterology. 2019;157(5):1383–97.e11. doi:10.1053/j.gastro.2019.07.028
44. Xu Y, Poggio M, Jin HY, et al. Translation control of the immune checkpoint in cancer and its therapeutic targeting. Nat Med. 2019;25(2):301–311. doi:10.1038/s41591-018-0321-2
45. Shen J, Ju Z, Zhao W, et al. ARID1A deficiency promotes mutability and potentiates therapeutic antitumor immunity unleashed by immune checkpoint blockade. Nat Med. 2018;24(5):556–562. doi:10.1038/s41591-018-0012-z
46. Li J, Wang W, Zhang Y, et al. Epigenetic driver mutations in ARID1A shape cancer immune phenotype and immunotherapy. J Clin Invest. 2020;130(5):2712–2726. doi:10.1172/JCI134402
47. Montironi C, Castet F, Haber PK, et al. Inflamed and non-inflamed classes of HCC: a revised immunogenomic classification. Gut. 2023;72(1):129–140. doi:10.1136/gutjnl-2021-325918
48. Sangro B, Melero I, Wadhawan S, et al. Association of inflammatory biomarkers with clinical outcomes in nivolumab-treated patients with advanced hepatocellular carcinoma. J Hepatol. 2020;73(6):1460–1469. doi:10.1016/j.jhep.2020.07.026
49. Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a multicentre, open-label, Phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837–1846. doi:10.1016/S0140-6736(16)00587-0
50. Pinyol R, Sia D, Llovet JM. Immune exclusion-Wnt/CTNNB1 class predicts resistance to immunotherapies in HCC. Clin Cancer Res. 2019;25(7):2021–2023. doi:10.1158/1078-0432.CCR-18-3778
51. Llovet JM, Pinyol R, Yarchoan M, et al. Adjuvant and neoadjuvant immunotherapies in hepatocellular carcinoma. Nat Rev Clin Oncol. 2024;21(4):294–311. doi:10.1038/s41571-024-00868-0
52. Xin H, Zhang C, Ding Z, Zhang M, Ding G, Li N. TACE plus PD-1 inhibitor (Camrelizumab) treatment for bridging to tumor resection in HCC. Clin Res Hepatol Gastroenterol. 2022;46(1):101777. doi:10.1016/j.clinre.2021.101777
53. Yegin EG, Oymaci E, Karatay E, Coker A. Progress in surgical and nonsurgical approaches for hepatocellular carcinoma treatment. Hepatob Pancrea Dis Inter. 2016;15(3):234–256. doi:10.1016/S1499-3872(16)60097-8
54. Craig AJ, Von Felden J, Garcia-Lezana T, Sarcognato S, Villanueva A. Tumour evolution in hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2020;17(3):139–152. doi:10.1038/s41575-019-0229-4
55. Tabrizian P, Jibara G, Shrager B, Schwartz M, Roayaie S. Recurrence of hepatocellular cancer after resection: patterns, treatments, and prognosis. Ann Surg. 2015;261(5):947–955. doi:10.1097/SLA.0000000000000710
56. Chen R, Hou B, Zhou Y, et al. Recurrence after percutaneous radiofrequency ablation of hepatocellular carcinoma: analysis of the pattern and risk factors. Front Oncol. 2023;13:1018715. doi:10.3389/fonc.2023.1018715
57. Vibert E, Schwartz M, Olthoff KM. Advances in resection and transplantation for hepatocellular carcinoma. J Hepatol. 2020;72(2):262–276. doi:10.1016/j.jhep.2019.11.017
58. Zhu Y, Gu L, Chen T, Zheng G, Ye C, Jia W. Factors influencing early recurrence of hepatocellular carcinoma after curative resection. J Inter Med Res. 2020;48(8):0300060520945552. doi:10.1177/0300060520945552
59. Xu X-F, Xing H, Han J, et al. Risk factors, patterns, and outcomes of late recurrence after liver resection for hepatocellular carcinoma: a multicenter study from China. JAMA Surg. 2019;154(3):209–217. doi:10.1001/jamasurg.2018.4334
60. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12(4):252–264. doi:10.1038/nrc3239
61. Sharma P, Allison JP. The future of immune checkpoint therapy. Science. 2015;348(6230):56–61. doi:10.1126/science.aaa8172
62. Faivre S, Rimassa L, Finn RS. Molecular therapies for HCC: looking outside the box. J Hepatol. 2020;72(2):342–352. doi:10.1016/j.jhep.2019.09.010
63. Pinato DJ, Cortellini A, Sukumaran A, et al. PRIME-HCC: phase Ib study of neoadjuvant ipilimumab and nivolumab prior to liver resection for hepatocellular carcinoma. BMC Cancer. 2021;21(1):301. doi:10.1186/s12885-021-08033-x
64. Kaseb AO, Hasanov E, Cao HST, et al. Perioperative nivolumab monotherapy versus nivolumab plus ipilimumab in resectable hepatocellular carcinoma: a randomised, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):208–218. doi:10.1016/S2468-1253(21)00427-1
65. Dickson NR, Beauchamp KD, Perry TS, et al. Real-world use and clinical impact of electronic patient-reported outcomes (ePROs) in patients with solid tumors treated with immuno-oncology (IO) therapy. J Clin Oncol. 2022;40(28_suppl):416. doi:10.1200/JCO.2022.40.28_suppl.416
66. Hack SP, Spahn J, Chen M, et al. IMbrave 050: a Phase III trial of atezolizumab plus bevacizumab in high-risk hepatocellular carcinoma after curative resection or ablation. Future Oncol. 2020;16(15):975–989. doi:10.2217/fon-2020-0162
67. Jimenez Exposito MJ, Akce M, Alvarez JLM, et al. CA209-9DX: Phase III, randomized, double-blind study of adjuvant nivolumab vs placebo for patients with hepatocellular carcinoma (HCC) at high risk of recurrence after curative resection or ablation. Ann Oncol. 2018;29:ix65.
68. Harding JJ, Nandakumar S, Armenia J, et al. Prospective genotyping of hepatocellular carcinoma: clinical implications of next-generation sequencing for matching patients to targeted and immune therapies. Clin Cancer Res. 2019;25(7):2116–2126. doi:10.1158/1078-0432.CCR-18-2293
69. Galon J, Bruni D. Approaches to treat immune hot, altered and cold tumours with combination immunotherapies. Nat Rev Drug Discov. 2019;18(3):197–218. doi:10.1038/s41573-018-0007-y
70. Hazama S, Tamada K, Yamaguchi Y, Kawakami Y, Nagano H. Current status of immunotherapy against gastrointestinal cancers and its biomarkers: perspective for precision immunotherapy. Ann Gastroenterol Surg. 2018;2(4):289–303. doi:10.1002/ags3.12180
71. Kano Y, Iguchi T, Matsui H, et al. Combined adjuvants of poly(I:C) plus LAG −3-Ig improve antitumor effects of tumor-specific T cells, preventing their exhaustion. Cancer Sci. 2016;107(4):398–406. doi:10.1111/cas.12861
72. Avice MN, Sarfati M, Triebel F, Delespesse G, Demeure CE. Lymphocyte activation gene-3, a MHC class II ligand expressed on activated T cells, stimulates TNF-alpha and IL-12 production by monocytes and dendritic cells. J Immunol. 1999;162(5):2748–2753. doi:10.4049/jimmunol.162.5.2748
73. Casati C, Camisaschi C, Rini F, et al. Soluble human LAG-3 molecule amplifies the in vitro generation of type 1 tumor-specific immunity. Cancer Res. 2006;66(8):4450–4460. doi:10.1158/0008-5472.CAN-05-2728
74. Legat A, Maby-El Hajjami H, Baumgaertner P, et al. Vaccination with LAG-3Ig (IMP321) and peptides induces specific CD4 and CD8 T-cell responses in metastatic melanoma patients--report of a phase I/IIa clinical trial. Clin Cancer Res. 2016;22(6):1330–1340. doi:10.1158/1078-0432.CCR-15-1212
75. Zhu X, Nishimura F, Sasaki K, et al. Toll like receptor-3 ligand poly-ICLC promotes the efficacy of peripheral vaccinations with tumor antigen-derived peptide epitopes in murine CNS tumor models. J Transl Med. 2007;5(1):10. doi:10.1186/1479-5876-5-10
76. Longhi MP, Trumpfheller C, Idoyaga J, et al. Dendritic cells require a systemic type I interferon response to mature and induce CD4+ Th1 immunity with poly IC as adjuvant. J Exp Med. 2009;206(7):1589–1602. doi:10.1084/jem.20090247
77. Ammi R, De Waele J, Willemen Y, et al. Poly(I:C) as cancer vaccine adjuvant: knocking on the door of medical breakthroughs. Pharmacol Ther. 2015;146:120–131. doi:10.1016/j.pharmthera.2014.09.010
78. Matsui H, Hazama S, Tamada K, et al. Identification of a promiscuous epitope peptide derived from HSP70. J Immunother. 2019;42(7):244–250. doi:10.1097/CJI.0000000000000274
79. Nakajima M, Hazama S, Tamada K, et al. A phase I study of multi-HLA-binding peptides derived from heat shock protein 70/glypican-3 and a novel combination adjuvant of hLAG-3Ig and Poly-ICLC for patients with metastatic gastrointestinal cancers: YNP01 trial. Cancer Immunol Immunother. 2020;69(8):1651–1662. doi:10.1007/s00262-020-02518-7
80. Yin S, Chen Z, Chen D, Yan D. Strategies targeting PD-L1 expression and associated opportunities for cancer combination therapy. Theranostics. 2023;13(5):1520–1544. doi:10.7150/thno.80091
81. Zhu AX, Finn RS, Edeline J, et al. Pembrolizumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib (KEYNOTE-224): a non-randomised, open-label phase 2 trial. Lancet Oncol. 2018;19(7):940–952. doi:10.1016/S1470-2045(18)30351-6
82. Ren Z, Xu J, Bai Y, et al. Sintilimab plus a bevacizumab biosimilar (IBI305) versus sorafenib in unresectable hepatocellular carcinoma (ORIENT-32): a randomised, open-label, phase 2-3 study. Lancet Oncol. 2021;22(7):977–990. doi:10.1016/S1470-2045(21)00252-7
83. Qin S, Kudo M, Meyer T, et al. Tislelizumab vs sorafenib as first-line treatment for unresectable hepatocellular carcinoma: a phase 3 randomized clinical trial. JAMA Oncol. 2023;9(12):1651–1659. doi:10.1001/jamaoncol.2023.4003
84. Brunnström H, Johansson A, Westbom-Fremer S, et al. PD-L1 immunohistochemistry in clinical diagnostics of lung cancer: inter-pathologist variability is higher than assay variability. Mod Pathol. 2017;30(10):1411–1421. doi:10.1038/modpathol.2017.59
85. Li H, Wu Z, Chen J, et al. External radiotherapy combined with sorafenib has better efficacy in unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Clin Exp Med. 2023;23(5):1537–1549. doi:10.1007/s10238-022-00972-4
86. Su K, Wang F, Li X, et al. Effect of external beam radiation therapy versus transcatheter arterial chemoembolization for non-diffuse hepatocellular carcinoma (≥ 5 cm): a multicenter experience over a ten-year period. Front Immunol. 2023;14:1265959. doi:10.3389/fimmu.2023.1265959
87. Li H, Su K, Guo L, et al. PD-1 inhibitors combined with antiangiogenic therapy with or without transarterial chemoembolization in the treatment of hepatocellular carcinoma: a propensity matching analysis. J Hepatocell Carcinoma. 2023;10:1257–1266. doi:10.2147/JHC.S415843
88. Li H, Guo L, Su K, et al. Construction and validation of TACE therapeutic efficacy by ALR score and nomogram: a large, multicenter study. J Hepatocell Carcinoma. 2023;10:1009–1017. doi:10.2147/JHC.S414926
89. Su K, Huang W, Li X, et al. Evaluation of lactate dehydrogenase and alkaline phosphatase as predictive biomarkers in the prognosis of hepatocellular carcinoma and development of a new nomogram. J Hepatocell Carcinoma. 2023;10:69–79. doi:10.2147/JHC.S398632
90. Su K, Shen Q, Tong J, et al. Construction and validation of a nomogram for HBV-related hepatocellular carcinoma: a large, multicenter study. Ann Hepatol. 2023;28(4):101109. doi:10.1016/j.aohep.2023.101109
91. Appleman LJ. Multifactorial, biomarker-based predictive models for immunotherapy response enter the arena. J Natl Cancer Inst. 2021;113(1):7–8. doi:10.1093/jnci/djaa077
92. Yi M, Zheng X, Niu M, Zhu S, Ge H, Wu K. Combination strategies with PD-1/PD-L1 blockade: current advances and future directions. Mol Cancer. 2022;21(1):28. doi:10.1186/s12943-021-01489-2
93. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–699. doi:10.1056/NEJM199603143341104
94. Zimmerman MA, Ghobrial RM, Tong MJ, et al. Recurrence of hepatocellular carcinoma following liver transplantation: a review of preoperative and postoperative prognostic indicators. Arch Surg. 2008;143(2):182–188. doi:10.1001/archsurg.2007.39
95. Akabane M, Bekki Y, Imaoka Y, et al. Impact of donor characteristics on hepatocellular carcinoma recurrence after liver transplantation. Br J Surg. 2024;111(4):znae080.
96. Akabane M, Esquivel CO, Kim WR, Sasaki K. The future frontier of liver transplantation exploring young donor allocation strategies for hcc recipients. Transplant Direct. 2024; 10:e1657.
97. Akabane M, Melcher ML, Sasaki K. Debating the indication: re-transplant for patients whose initial transplant indication was hepatocellular carcinoma. HPB. 2023;25(12):1600–1602. doi:10.1016/j.hpb.2023.08.003
98. Wehrle CJ, Kusakabe J, Akabane M, et al. Expanding selection criteria in deceased donor liver transplantation for hepatocellular carcinoma: long-term follow-up of a national registry and 2 transplant centers. Transplantation. 2024;108(12):2386–2395. doi:10.1097/TP.0000000000005097
99. Akabane M, McVey JC, Firl DJ, et al. Continuous risk score predicts waitlist and post-transplant outcomes in hepatocellular carcinoma despite exception changes. Clin Gastroenterol Hepatol. 2024;22(10):2044–2052.e4. doi:10.1016/j.cgh.2024.05.046
100. Moeckli B, Ivanics T, Claasen M, Toso C, Sapisochin G. Recent developments and ongoing trials in transplant oncology. Liver Int. 2020;40(10):2326–2344. doi:10.1111/liv.14621
101. Rodríguez-Perálvarez M, Tsochatzis E, Naveas MC, et al. Reduced exposure to calcineurin inhibitors early after liver transplantation prevents recurrence of hepatocellular carcinoma. J Hepatol. 2013;59(6):1193–1199. doi:10.1016/j.jhep.2013.07.012
102. Zhang Y, Shi ZL, Yang X, Yin ZF. Targeting of circulating hepatocellular carcinoma cells to prevent postoperative recurrence and metastasis. World J Gastroenterol. 2014;20(1):142–147. doi:10.3748/wjg.v20.i1.142
103. Lerut J, Iesari S, Foguenne M, Lai Q. Hepatocellular cancer and recurrence after liver transplantation: what about the impact of immunosuppression? Transl Gastroenterol Hepatol. 2017;2(10):80. doi:10.21037/tgh.2017.09.06
104. Rana A, Ackah RL, Webb GJ, et al. No gains in long-term survival after liver transplantation over the past three decades. Ann Surg. 2019;269(1):20–27. doi:10.1097/SLA.0000000000002650
105. Welker MW, Bechstein WO, Zeuzem S, Trojan J. Recurrent hepatocellular carcinoma after liver transplantation - an emerging clinical challenge. Transpl Int. 2013;26(2):109–118. doi:10.1111/j.1432-2277.2012.01562.x
106. Filgueira NA. Hepatocellular carcinoma recurrence after liver transplantation: risk factors, screening and clinical presentation. World J Hepatol. 2019;11(3):261–272. doi:10.4254/wjh.v11.i3.261
107. Ogawa T, Tashiro H, Miyata Y, et al. Rho-associated kinase inhibitor reduces tumor recurrence after liver transplantation in a rat hepatoma model. Am J Transplant. 2007;7(2):347–355. doi:10.1111/j.1600-6143.2006.01647.x
108. Maluccio M, Sharma V, Lagman M, et al. Tacrolimus enhances transforming growth factor-beta1 expression and promotes tumor progression. Transplantation. 2003;76(3):597–602. doi:10.1097/01.TP.0000081399.75231.3B
109. Hojo M, Morimoto T, Maluccio M, et al. Cyclosporine induces cancer progression by a cell-autonomous mechanism. Nature. 1999;397(6719):530–534. doi:10.1038/17401
110. Datta D, Contreras AG, Basu A, et al. Calcineurin inhibitors activate the proto-oncogene Ras and promote protumorigenic signals in renal cancer cells. Cancer Res. 2009;69(23):8902–8909. doi:10.1158/0008-5472.CAN-09-1404
111. Baccelli I, Schneeweiss A, Riethdorf S, et al. Identification of a population of blood circulating tumor cells from breast cancer patients that initiates metastasis in a xenograft assay. Nat Biotechnol. 2013;31(6):539–544. doi:10.1038/nbt.2576
112. Loreth D, Schuette M, Zinke J, et al. CD74 and CD44 expression on CTCs in cancer patients with brain metastasis. Int J Mol Sci. 2021;23(1):22. doi:10.3390/ijms23010022
113. Szczerba BM, Castro-Giner F, Vetter M, et al. Neutrophils escort circulating tumour cells to enable cell cycle progression. Nature. 2019;566(7745):553–557. doi:10.1038/s41586-019-0915-y
114. Hafezi M, Lin M, Chia A, et al. Immunosuppressive drug‐resistant armored T‐cell receptor T cells for immune therapy of HCC in liver transplant patients. Hepatology. 2021;74(1):200–213. doi:10.1002/hep.31662
115. Qasim W, Brunetto M, Gehring AJ, et al. Immunotherapy of HCC metastases with autologous T cell receptor redirected T cells, targeting HBsAg in a liver transplant patient. J Hepatol. 2015;62(2):486–491. doi:10.1016/j.jhep.2014.10.001
116. Tan AT, Yang N, Krishnamoorthy TL, et al. Use of expression profiles of HBV-DNA integrated into genomes of hepatocellular carcinoma cells to select T cells for immunotherapy. Gastroenterology. 2019;156(6):1862–76.e9. doi:10.1053/j.gastro.2019.01.251
117. Xie S, Wu Z, Zhou L, et al. Iodine-125 seed implantation and allogenic natural killer cell immunotherapy for hepatocellular carcinoma after liver transplantation: a case report. OncoTargets and Therapy. 2018;Volume 11:7345–7352. doi:10.2147/OTT.S166962
118. Amjad W, Kotiah S, Gupta A, Morris M, Liu L, Thuluvath PJ. Successful treatment of disseminated hepatocellular carcinoma after liver transplantation with nivolumab. J Clin Exper Hepatol. 2020;10(2):185–187. doi:10.1016/j.jceh.2019.11.009
119. Varkaris A, Lewis DW, Nugent FW. Preserved liver transplant after PD-1 pathway inhibitor for hepatocellular carcinoma. Off J Ame College Gastroenterol. 2017;112:1895–1896. doi:10.1038/ajg.2017.387
120. De Toni EN, Gerbes AL. Tapering of immunosuppression and sustained treatment with nivolumab in a liver transplant recipient. Gastroenterology. 2017;152(6):1631–1633. doi:10.1053/j.gastro.2017.01.063
121. Rammohan A, Reddy MS, Farouk M, Vargese J, Rela M. Pembrolizumab for metastatic hepatocellular carcinoma following live donor liver transplantation: the silver bullet? Hepatology. 2018;67(3):1166–1168. doi:10.1002/hep.29575
122. Pandey A, Cohen DJ. Ipilumumab for hepatocellular cancer in a liver transplant recipient, with durable response, tolerance and without allograft rejection. Immunotherapy. 2020;12(5):287–292. doi:10.2217/imt-2020-0014
123. Gassmann D, Weiler S, Mertens JC, et al. Liver allograft failure after nivolumab treatment—a case report with systematic literature research. Transplantation Direct. 2018;4(8):e376.
124. Friend BD, Venick RS, McDiarmid SV, et al. Fatal orthotopic liver transplant organ rejection induced by a checkpoint inhibitor in two patients with refractory, metastatic hepatocellular carcinoma. Pediatric Blood Cancer. 2017; 64(4):e26682.
125. DeLeon TT, Salomao MA, Aqel BA, et al. Pilot evaluation of PD-1 inhibition in metastatic cancer patients with a history of liver transplantation: the Mayo clinic experience. J Gastrointest Oncol. 2018;9(6):1054. doi:10.21037/jgo.2018.07.05
126. Zhuang L, Mou H-B, Yu L-F, et al. Immune checkpoint inhibitor for hepatocellular carcinoma recurrence after liver transplantation. Hepatobiliary & pancreatic diseases international. HBPD INT. 2020;19(1):91–93. doi:10.1016/j.hbpd.2019.09.011
127. Al Jarroudi O, Ulusakarya A, Almohamad W, Afqir S, Morere J-F. Anti-programmed cell death protein 1 (PD-1) immunotherapy for metastatic hepatocellular carcinoma after liver transplantation: a report of three cases. Cureus. 2020;12:10.
128. WANG G, TANG H, ZHANG Y, et al. Programmed death receptor (PD)-1 monoclonal antibody-induced acute immune hepatitis in the treatment; of recurrent hepatocellular carcinoma after liver transplantation: a case report. Organ Transplan. 2016;44–47.
129. Qiu J, Tang W, Du C. Immune checkpoint inhibitors in patients with recurrent hepatocellular carcinoma after liver transplantation: a case report and literature review. Current Cancer Drug Targets. 2020;20(9):720–727. doi:10.2174/1568009620666200520084415
130. Luo Y, Teng F, Fu H, Ding GS. Immunotherapy in liver transplantation for hepatocellular carcinoma: pros and cons. World J Gastrointest Oncol. 2022;14(1):163–180. doi:10.4251/wjgo.v14.i1.163
131. Schnickel GT, Fabbri K, Hosseini M, et al. Liver transplantation for hepatocellular carcinoma following checkpoint inhibitor therapy with nivolumab. Ame J Transplan. 2022;22(6):1699–1704. doi:10.1111/ajt.16965
132. Benson AB, D’Angelica MI, Abbott DE, et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J National Comprehen Cancer Network. 2021;19(5):541–565. doi:10.6004/jnccn.2021.0022
133. Cheng A-L, Hsu C, Chan SL, Choo S-P, Kudo M. Challenges of combination therapy with immune checkpoint inhibitors for hepatocellular carcinoma. J Hepatol. 2020;72(2):307–319. doi:10.1016/j.jhep.2019.09.025
134. Farsaci B, Donahue RN, Coplin MA, et al. Immune consequences of decreasing tumor vasculature with antiangiogenic tyrosine kinase inhibitors in combination with therapeutic vaccines. Cancer Immunol Res. 2014;2(11):1090–1102. doi:10.1158/2326-6066.CIR-14-0076
135. Sunay MM, Foote JB, Leatherman JM, et al. Sorafenib combined with HER-2 targeted vaccination can promote effective T cell immunity in vivo. Inter Immunopharmacol. 2017;46:112–123. doi:10.1016/j.intimp.2017.02.028
136. Hodi FS, O’day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. New England J Med. 2010;363(8):711–723. doi:10.1056/NEJMoa1003466
137. Morita M, Fujino M, Jiang G, et al. PD‐1/B7‐H1 interaction contribute to the spontaneous acceptance of mouse liver allograft. Ame J Transplan. 2010;10(1):40–46. doi:10.1111/j.1600-6143.2009.02859.x
138. Li W, Zheng XX, Kuhr CS, Perkins JD. CTLA4 engagement is required for induction of murine liver transplant spontaneous tolerance. Ame J Transplan. 2005;5(5):978–986. doi:10.1111/j.1600-6143.2005.00823.x
139. Zhang P, Zhu G, Li L, et al. Immune checkpoint inhibitor therapy for malignant tumors in liver transplantation recipients: a systematic review of the literature. Transplant Rev. 2022;36(4):100712. doi:10.1016/j.trre.2022.100712
140. Colmenero J, Tabrizian P, Bhangui P, et al. De novo malignancy after liver transplantation: risk assessment, prevention, and management—guidelines from the ILTS-SETH consensus conference. 2022;106:e30–e45 doi:10.1097/TP.0000000000003998
141. Bhat M, Mara K, Dierkhising R, watt KD. Gender, race and disease etiology predict de novo malignancy risk after liver transplantation: insights for future individualized cancer screening guidance. Transplantation. 2019;103(1):91–100. doi:10.1097/TP.0000000000002113
142. Jiang J, Huang H, Chen R, Lin Y, Ling Q. Immunotherapy for hepatocellular carcinoma recurrence after liver transplantation, can we harness the power of immune checkpoint inhibitors? Front Immunol. 2023;14:1092401. doi:10.3389/fimmu.2023.1092401
143. Jiang Y, Villeneuve PJ, Fenton SS, Schaubel DE, Lilly L, Mao Y. Liver transplantation and subsequent risk of cancer: findings from a Canadian cohort study. Liver Transplan. 2008;14(11):1588–1597. doi:10.1002/lt.21554
144. Haagsma EB, Hagens VE, Schaapveld M, et al. Increased cancer risk after liver transplantation: a population-based study. J Hepatol. 2001;34(1):84–91. doi:10.1016/S0168-8278(00)00077-5
145. Yang Z, Sun J, Zhuang L, Mou H, Zheng S. Preliminary evaluation of atezolizumab plus bevacizumab as salvage treatment for recurrent hepatocellular carcinoma after liver transplantation. Liver Transplantation. 2022;28(5):895–896. doi:10.1002/lt.26416
146. Mou L, Tian X, Zhou B, et al. Improving outcomes of tyrosine kinase inhibitors in hepatocellular carcinoma: new data and ongoing trials. Front Oncol. 2021;11:752725. doi:10.3389/fonc.2021.752725
147. Llovet JM, Ricci S, Mazzaferro V, et al. Sorafenib in advanced hepatocellular carcinoma. New England J Med. 2008;359(4):378–390. doi:10.1056/NEJMoa0708857
148. Abou-Alfa GK, Meyer T, Cheng A-L, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. New England J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
149. Lencioni R, Kudo M, Erinjeri J, et al. EMERALD-1: a phase 3, randomized, placebo-controlled study of transarterial chemoembolization combined with durvalumab with or without bevacizumab in participants with unresectable hepatocellular carcinoma eligible for embolization. Ame Soc Clin Oncol. 2024;42(3_suppl):LBA432–LBA432. doi:10.1200/JCO.2024.42.3_suppl.LBA432
150. Marron TU, Fiel MI, Hamon P, et al. Neoadjuvant cemiplimab for resectable hepatocellular carcinoma: a single-arm, open-label, phase 2 trial. Lancet Gastroenterol Hepatol. 2022;7(3):219–229. doi:10.1016/S2468-1253(21)00385-X
151. Shi Y-H, Ji Y, Liu W-R, et al. A phase Ib/II, open-label study evaluating the efficacy and safety of Toripalimab injection (JS001) or combination with Lenvatinib as a neoadjuvant therapy for patients with resectable hepatocellular carcinoma (HCC). Cancer Res. 2021;81(13_Supplement):486. doi:10.1158/1538-7445.AM2021-486
152. Peeraphatdit T, Wang J, Odenwald MA, Hu S, Hart J, Charlton MR. Hepatotoxicity from immune checkpoint inhibitors: a systematic review and management recommendation. Hepatology. 2020;72(1):315–329. doi:10.1002/hep.31227
153. Montano-Loza AJ, Rodríguez-Perálvarez ML, Pageaux GP, Sanchez-Fueyo A, Feng S. Liver transplantation immunology: immunosuppression, rejection, and immunomodulation. J Hepatol. 2023;78(6):1199–1215. doi:10.1016/j.jhep.2023.01.030
154. Topalian SL, Hodi FS, Brahmer JR, et al. Safety, activity, and immune correlates of anti–PD-1 antibody in cancer. New England J Med. 2012;366(26):2443–2454. doi:10.1056/NEJMoa1200690
155. Cui TM, Liu Y, Wang JB, Liu LX. Adverse effects of immune-checkpoint inhibitors in hepatocellular carcinoma. OncoTargets and Therapy. 2020;Volume 13:11725–11740. doi:10.2147/OTT.S279858
156. Ong M, Ibrahim AM, Bourassa-Blanchette S, Canil C, Fairhead T, Knoll G. Antitumor activity of nivolumab on hemodialysis after renal allograft rejection. J ImmunoTherapy Cancer. 2016;4(1):1–5. doi:10.1186/s40425-016-0171-8
157. Riella LV, Paterson AM, Sharpe AH, Chandraker A. Role of the PD-1 pathway in the immune response. Ame J Transplan. 2012;12(10):2575–2587. doi:10.1111/j.1600-6143.2012.04224.x
158. Weber J, Thompson JA, Hamid O, et al. A randomized, double-blind, placebo-controlled, phase II study comparing the tolerability and efficacy of ipilimumab administered with or without prophylactic budesonide in patients with unresectable stage III or IV melanoma. Clin Cancer Res. 2009;15(17):5591–5598. doi:10.1158/1078-0432.CCR-09-1024
159. Wolchok JD, Kluger H, Callahan MK, et al. Nivolumab plus ipilimumab in advanced melanoma. New England J Med. 2013;369(2):122–133. doi:10.1056/NEJMoa1302369
160. Curran MA, Montalvo W, Yagita H, Allison JP. PD-1 and CTLA-4 combination blockade expands infiltrating T cells and reduces regulatory T and myeloid cells within B16 melanoma tumors. 2010;107:4275–4280 doi:10.1073/pnas.0915174107
161. Herz S, Höfer T, Papapanagiotou M, et al. Checkpoint inhibitors in chronic kidney failure and an organ transplant recipient. Europ J Cancer. 2016;67:66–72. doi:10.1016/j.ejca.2016.07.026
162. Blazar BR, Carreno BM, Panoskaltsis-Mortari A, et al. Blockade of programmed death-1 engagement accelerates graft-versus-host disease lethality by an IFN-γ-dependent mechanism. J Immunol. 2003;171(3):1272–1277. doi:10.4049/jimmunol.171.3.1272
163. Shen B, Guo Z, Huang P, et al. Immunotherapy and Antivascular Targeted Therapy in Patients’ Treatment with Concurrent Malignant Tumors after Organ Transplantation: opportunity or Challenge. J Immunol Res. 2022;2022:6440419. doi:10.1155/2022/6440419
164. Buchbinder EI, Desai A. CTLA-4 and PD-1 pathways: similarities, differences, and implications of their inhibition. Ame J Clin Oncol. 2016;39(1):98–106. doi:10.1097/COC.0000000000000239
165. Rowshanravan B, Halliday N, Sansom DM. CTLA-4: a moving target in immunotherapy. Blood J Ame Soc Hematol. 2018;131:58–67.
166. Khoja L, Butler MO, Kang SP, Ebbinghaus S, Joshua AM. Pembrolizumab. J Immunotherap Cancer. 2015;3(1):1–13. doi:10.1186/s40425-015-0078-9
167. Collins LK, Chapman MS, Carter JB, Samie FH. Cutaneous adverse effects of the immune checkpoint inhibitors. Curr Probl Cancer. 2017;41(2):125–128. doi:10.1016/j.currproblcancer.2016.12.001
168. Mir H, Alhussein M, Alrashidi S, et al. Cardiac complications associated with checkpoint inhibition: a systematic review of the literature in an important emerging area. Canadian J Cardiol. 2018;34(8):1059–1068. doi:10.1016/j.cjca.2018.03.012
169. Linsley PS, Greene JL, Brady W, Bajorath J, Ledbetter JA, Peach R. Human B7-1 (CD80) and B7-2 (CD86) bind with similar avidities but distinct kinetics to CD28 and CTLA-4 receptors. Immunity. 1994;1(9):793–801. doi:10.1016/S1074-7613(94)80021-9
170. Schneider H, Mandelbrot DA, Greenwald RJ, et al. Cutting edge: CTLA-4 (CD152) differentially regulates mitogen-activated protein kinases (extracellular signal-regulated kinase and c-Jun N-terminal kinase) in CD4+ T cells from receptor/ligand-deficient mice. J Immunol. 2002;169(7):3475–3479. doi:10.4049/jimmunol.169.7.3475
171. Francisco LM, Salinas VH, Brown KE, et al. PD-L1 regulates the development, maintenance, and function of induced regulatory T cells. J Exper Med. 2009;206(13):3015–3029. doi:10.1084/jem.20090847
172. Wing K, Onishi Y, Prieto-Martin P, et al. CTLA-4 control over Foxp3 + regulatory T cell function. Science. 2008;322(5899):271–275. doi:10.1126/science.1160062
173. Peggs KS, Quezada SA, Chambers CA, Korman AJ, Allison JP. Blockade of CTLA-4 on both effector and regulatory T cell compartments contributes to the antitumor activity of anti–CTLA-4 antibodies. J Exper Med. 2009;206(8):1717–1725. doi:10.1084/jem.20082492
174. Freeman GJ, Long AJ, Iwai Y, et al. Engagement of the PD-1 immunoinhibitory receptor by a novel B7 family member leads to negative regulation of lymphocyte activation. J Exper Med. 2000;192(7):1027–1034. doi:10.1084/jem.192.7.1027
175. Kim SI. Bacterial infection after liver transplantation. World J Gastroenterol. 2014;20(20):6211. doi:10.3748/wjg.v20.i20.6211
176. Long C, Peng W, Zhao J, Wan Q. The influence of invasive candida infections on prognosis and analysis of their risk factors after liver transplantation. Clin Ther. 2024;46(12):1041–1048. doi:10.1016/j.clinthera.2024.09.012
177. George AS, Fernandez CJ, Eapen D, Pappachan JM. Organ-specific adverse events of immune checkpoint inhibitor therapy, with special reference to endocrinopathies. touchREV Endocrinol. 2021;17(1):21–32. doi:10.17925/EE.2021.17.1.21
178. Breitkopf R, Treml B, Bukumiric Z, Innerhofer N, Fodor M, Rajsic S. Invasive fungal infections: the early killer after liver transplantation. J Fungi. 2023;9(6):655. doi:10.3390/jof9060655
179. Breitkopf R, Treml B, Senoner T, Bukumirić Z, Rajsic S. Invasive fungal breakthrough infections under targeted echinocandin prophylaxis in high-risk liver transplant recipients. J Fungi. 2023;9(2):272. doi:10.3390/jof9020272
180. Scolarici M, Jorgenson M, Saddler C, Smith J. Fungal infections in liver transplant recipients. J Fungi. 2021;7(7):524. doi:10.3390/jof7070524
181. Liu M, Zhu Z, Sun L. Risk factors of invasive fungal infection in recipients after liver transplantation: a systematic review and meta-analysis. Front Med. 2021;8:687028. doi:10.3389/fmed.2021.687028
182. Zhang W, Wang W, Kang M, et al. Bacterial and fungal infections after liver transplantation: microbial epidemiology, risk factors for infection and death with infection. Ann Transplan. 2020;25:e921591. doi:10.12659/AOT.921591
183. Neyra KM, Brizendine KD. Retrospective study evaluating the performance of risk factors for invasive mold infections in liver transplantation. Transplant Infect Dis. 2020; 22(1):e13223.
184. Kang W-H, Song G-W, Lee S-G, et al. A multicenter, randomized, open-label study to compare micafungin with fluconazole in the prophylaxis of invasive fungal infections in living-donor liver transplant recipients. J Gastrointest Surg. 2020;24(4):832–840. doi:10.1007/s11605-019-04241-w
185. Rinaldi M, Bartoletti M, Ferrarese A, et al. Breakthrough invasive fungal infection after liver transplantation in patients on targeted antifungal prophylaxis: a prospective multicentre study. Transplant Infect Dis. 2021;23(4):e13608.
186. Husain S, Tollemar J, Dominguez EA, et al. Changes in the spectrum and risk factors for invasive candidiasis in liver transplant recipients: prospective, multicenter, case-controlled study1. Transplantation. 2003;75(12):2023–2029. doi:10.1097/01.TP.0000065178.93741.72
187. Andes DR, Safdar N, Baddley JW, et al. The epidemiology and outcomes of invasive Candida infections among organ transplant recipients in the United States: results of the transplant-associated infection surveillance network (TRANSNET). Transplant Infect Dis. 2016;18(6):921–931. doi:10.1111/tid.12613
188. Raghuram A, Restrepo A, Safadjou S, et al. Invasive fungal infections following liver transplantation: incidence, risk factors, survival, and impact of fluconazole‐resistant Candida parapsilosis (2003‐2007). Liver Transplan. 2012;18(9):1100–1109. doi:10.1002/lt.23467
189. Righi E, Carnelutti A, Baccarani U, et al. Treatment of Candida infections with fluconazole in adult liver transplant recipients: is TDM‐guided dosing adaptation helpful? Transplant Infect Dis. 2019;21(4):e13113.
190. Saliba F, Delvart V, Ichaï P, et al. Fungal infections after liver transplantation: outcomes and risk factors revisited in the MELD era. Clin Transplant. 2013;27(4):E454–E61.
191. Sharpe MD, Ghent C, Grant D, Horbay GL, McDougal J, Colby WD. Efficacy and safety of itraconazole prophylaxis for fungal infections after orthotopic liver transplantation: a prospective, randomized, double-blind study. Transplantation. 2003;76(6):977–983. doi:10.1097/01.TP.0000085653.11565.52
192. Cruciani M, Mengoli C, Malena M, Bosco O, Serpelloni G, Grossi P. Antifungal prophylaxis in liver transplant patients: a systematic review and meta‐analysis. Liver Transplan. 2006;12(5):850–858. doi:10.1002/lt.20690
193. Evans J, Morris P, Knight S. Antifungal prophylaxis in liver transplantation: a systematic review and network meta-analysis. Ame J Transplan. 2014;14(12):2765–2776. doi:10.1111/ajt.12925
194. Champiat S, Lambotte O, Barreau E, et al. Management of immune checkpoint blockade dysimmune toxicities: a collaborative position paper. Ann Oncol. 2016;27(4):559–574. doi:10.1093/annonc/mdv623
195. Haanen J, Obeid M, Spain L, et al. Management of toxicities from immunotherapy: ESMO clinical practice guideline for diagnosis, treatment and follow-up☆. Ann Oncol. 2022;33(12):1217–1238. doi:10.1016/j.annonc.2022.10.001
196. Palaz F, Ozsoz M, Zarrinpar A, Sahin I. CRISPR in targeted therapy and adoptive T cell immunotherapy for hepatocellular carcinoma. J Hepatocell Carcinoma. 2024;11:975–995. doi:10.2147/JHC.S456683
197. Ozer M, Goksu SY, Akagunduz B, George A, Sahin I. Adoptive cell therapy in hepatocellular carcinoma: a review of clinical trials. Cancers. 2023;16(1):15. doi:10.3390/cancers16010015
198. Wang V, Gauthier M, Decot V, Reppel L, Bensoussan D. Systematic review on CAR-T cell clinical trials up to 2022: academic center input. Cancers. 2023;16(1):15.
199. Gao X, Mi Y, Guo N, et al. Cytokine-induced killer cells as pharmacological tools for cancer immunotherapy. Front Immunol. 2017;8:774. doi:10.3389/fimmu.2017.00774
200. Takayama T, Sekine T, Makuuchi M, et al. Adoptive immunotherapy to lower postsurgical recurrence rates of hepatocellular carcinoma: a randomised trial. Lancet. 2000;356(9232):802–807. doi:10.1016/S0140-6736(00)02654-4
201. Lee JH, Lee JH, Lim YS, et al. Adjuvant immunotherapy with autologous cytokine-induced killer cells for hepatocellular carcinoma. Gastroenterology. 2015;148(7):1383–91.e6. doi:10.1053/j.gastro.2015.02.055
202. Xu L, Wang J, Kim Y, et al. A randomized controlled trial on patients with or without adjuvant autologous cytokine-induced killer cells after curative resection for hepatocellular carcinoma. Oncoimmunology. 2016;5(3):e1083671.
203. Cho JY, Kwon SH, Lee EK, Lee JH, Kim HL. Cost-effectiveness of adjuvant immunotherapy with cytokine-induced killer cell for hepatocellular carcinoma based on a randomized controlled trial and real-world data. Front Oncol. 2021;11:728740. doi:10.3389/fonc.2021.728740
204. Yoon JS, Song BG, Lee JH, et al. Adjuvant cytokine-induced killer cell immunotherapy for hepatocellular carcinoma: a propensity score-matched analysis of real-world data. BMC Cancer. 2019;19(1):523. doi:10.1186/s12885-019-5740-z
205. Lee JH, Lee JH, Lim YS, et al. Sustained efficacy of adjuvant immunotherapy with cytokine-induced killer cells for hepatocellular carcinoma: an extended 5-year follow-up. Cancer Immunol Immunother. 2019;68(1):23–32. doi:10.1007/s00262-018-2247-4
206. Yu R, Yang B, Chi X, et al. Efficacy of cytokine-induced killer cell infusion as an adjuvant immunotherapy for hepatocellular carcinoma: a systematic review and meta-analysis. Drug Des Devel Ther. 2017;11:851–864. doi:10.2147/DDDT.S124399
207. Cai XR, Li X, Lin JX, et al. Autologous transplantation of cytokine-induced killer cells as an adjuvant therapy for hepatocellular carcinoma in Asia: an update meta-analysis and systematic review. Oncotarget. 2017;8(19):31318–31328. doi:10.18632/oncotarget.15454
208. Su Y, Yang G, Ma Y, et al. the efficacy and safety of dendritic cells co-cultured with cytokine-induced killer cell therapy in combination with TACE-predominant minimally-invasive treatment for hepatocellular carcinoma: a meta-analysis. Clin Lab. 2016;62(04/2016):599–608. doi:10.7754/Clin.Lab.2015.150804
209. Li YC, Zhao L, Wu JP, Qu CX, Song QK, Wang RB. Cytokine-induced killer cell infusion combined with conventional treatments produced better prognosis for hepatocellular carcinoma patients with barcelona clinic liver cancer B or earlier stage: a systematic review and meta-analysis. Cytotherapy. 2016;18(12):1525–1531. doi:10.1016/j.jcyt.2016.09.002
210. He G, Zheng C, Huo H, et al. TACE combined with dendritic cells and cytokine-induced killer cells in the treatment of hepatocellular carcinoma: a meta-analysis. Int Immunopharmacol. 2016;40:436–442. doi:10.1016/j.intimp.2016.09.015
211. Paijens ST, Vledder A, de Bruyn M, Nijman HW. Tumor-infiltrating lymphocytes in the immunotherapy era. Cell Mol Immunol. 2021;18(4):842–859. doi:10.1038/s41423-020-00565-9
212. Jiang SS, Tang Y, Zhang YJ, et al. A phase I clinical trial utilizing autologous tumor-infiltrating lymphocytes in patients with primary hepatocellular carcinoma. Oncotarget. 2015;6(38):41339–41349. doi:10.18632/oncotarget.5463
213. Schoenberg MB, Li X, Li X, et al. The predictive value of tumor infiltrating leukocytes in Hepatocellular Carcinoma: a systematic review and meta-analysis. Eur J Surg Oncol. 2021;47(10):2561–2570. doi:10.1016/j.ejso.2021.04.042
214. Fucà G, Reppel L, Landoni E, Savoldo B, Dotti G. Enhancing chimeric antigen receptor T-cell efficacy in solid tumors. Clin Cancer Res. 2020;26(11):2444–2451. doi:10.1158/1078-0432.CCR-19-1835
215. Billingsley MM, Singh N, Ravikumar P, Zhang R, June CH, Mitchell MJ. Ionizable lipid nanoparticle-mediated mRNA delivery for human CAR T cell engineering. Nano Letters. 2020;20(3):1578–1589. doi:10.1021/acs.nanolett.9b04246
216. Spranger S, Dai D, Horton B, Gajewski TF. Tumor-residing batf3 dendritic cells are required for effector T cell trafficking and adoptive T cell therapy. Cancer Cell. 2017;31(5):711–23.e4. doi:10.1016/j.ccell.2017.04.003
217. Caruana I, Savoldo B, Hoyos V, et al. Heparanase promotes tumor infiltration and antitumor activity of CAR-redirected T lymphocytes. Nat Med. 2015;21(5):524–529. doi:10.1038/nm.3833
218. Zhou Y, Wei S, Xu M, et al. CAR-T cell therapy for hepatocellular carcinoma: current trends and challenges. Front Immunol. 2024;15:1489649. doi:10.3389/fimmu.2024.1489649
219. Kalathil SG, Thanavala Y, Tian R. Natural killer cells and t cells in hepatocellular carcinoma and viral hepatitis: current status and perspectives for future immunotherapeutic approaches. Cells. 2021;11(1):10. doi:10.3390/cells11010010
220. Ohira M, Kobayashi T, Tanaka Y, et al. Adoptive immunotherapy with natural killer cells from peripheral blood CD34(+) stem cells to prevent hepatocellular carcinoma recurrence after curative hepatectomy: a study protocol for an open-label, single-arm phase I study. BMJ Open. 2022;12(11):e064526.
221. Jiang Y, Chen Y, Chen L, et al. Impaired circulating CD56(dim) NK cells are associated with decompensation of HBV-related cirrhosis. Hum Immunol. 2020;81(1):32–40. doi:10.1016/j.humimm.2019.11.006
222. Kawarabayashi N, Seki S, Hatsuse K, et al. Decrease of CD56(+)T cells and natural killer cells in cirrhotic livers with hepatitis C may be involved in their susceptibility to hepatocellular carcinoma. Hepatology. 2000;32(5):962–969. doi:10.1053/jhep.2000.19362
223. Liu P, Chen L, Zhang H. Natural killer cells in liver disease and hepatocellular carcinoma and the NK cell-based immunotherapy. J Immunol Res. 2018;2018:1206737. doi:10.1155/2018/1206737
224. Geller MA, Miller JS. Use of allogeneic NK cells for cancer immunotherapy. Immunotherapy. 2011;3(12):1445–1459. doi:10.2217/imt.11.131
225. Sun B, Yang D, Dai H, et al. Eradication of hepatocellular carcinoma by NKG2D-based CAR-T cells. Cancer Immunol Res. 2019;7(11):1813–1823. doi:10.1158/2326-6066.CIR-19-0026
226. Shi D, Shi Y, Kaseb AO, et al. Chimeric antigen receptor-glypican-3 T-cell therapy for advanced hepatocellular carcinoma: results of phase I trials. Clin Cancer Res. 2020;26(15):3979–3989. doi:10.1158/1078-0432.CCR-19-3259
227. Yang F, Zheng X, Koh S, et al. Messenger RNA electroporated hepatitis B virus (HBV) antigen-specific T cell receptor (TCR) redirected T cell therapy is well-tolerated in patients with recurrent HBV-related hepatocellular carcinoma post-liver transplantation: results from a phase I trial. Hepatol Int. 2023;17(4):850–859. doi:10.1007/s12072-023-10524-x
228. Loh K, Khan K, Kroemer A. CAR-NK therapy: translating a novel immunotherapy treatment to solid organ transplantation. Transplantation. 2020;104(8):1523–1524. doi:10.1097/TP.0000000000003267
229. Pan QZ, Liu Q, Zhou YQ, et al. CIK cell cytotoxicity is a predictive biomarker for CIK cell immunotherapy in postoperative patients with hepatocellular carcinoma. Cancer Immunol Immunother. 2020;69(5):825–834. doi:10.1007/s00262-020-02486-y
230. Harada N, Shimada M, Okano S, et al. IL-12 gene therapy is an effective therapeutic strategy for hepatocellular carcinoma in immunosuppressed mice. J Immunol. 2004;173(11):6635–6644. doi:10.4049/jimmunol.173.11.6635
231. Hirata M, Kita Y, Saito S, et al. Increase in natural killer cell activity following living‐related liver transplantation. Transplant Inter. 1998;11:S185–S8.
232. Ohira M, Ishiyama K, Tanaka Y, et al. Adoptive immunotherapy with liver allograft–derived lymphocytes induces anti-HCV activity after liver transplantation in humans and humanized mice. J Clin Invest. 2009;119(11):3226–3235. doi:10.1172/JCI38374
233. Ishiyama K, Ohdan H, Ohira M, Mitsuta H, Arihiro K, Asahara T. Difference in cytotoxicity against hepatocellular carcinoma between liver and periphery natural killer cells in humans. Hepatology. 2006;43(2):362–372. doi:10.1002/hep.21035
234. Ohira M, Ohdan H, Mitsuta H, et al. Adoptive transfer of TRAIL-expressing natural killer cells prevents recurrence of hepatocellular carcinoma after partial hepatectomy. Transplantation. 2006;82(12):1712–1719. doi:10.1097/01.tp.0000250935.41034.2d
235. Takeda K, Hayakawa Y, Smyth MJ, et al. Involvement of tumor necrosis factor-related apoptosis-inducing ligand in surveillance of tumor metastasis by liver natural killer cells. Nat Med. 2001;7(1):94–100. doi:10.1038/83416
236. Imaoka Y, Ohira M, Nakayama T, et al. Evaluating predictors of quality in liver NK cells among deceased donors. Cell Transplan. 2024;33:09636897241283289. doi:10.1177/09636897241283289
237. Tanimine N, Ohira M, Kurita E, et al. Impact of KIR-HLA genotype on natural-killer-cell-based immunotherapy for preventing hepatocellular carcinoma after living-donor liver transplantation. Cancers. 2024;16(3):533. doi:10.3390/cancers16030533
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.