Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Advances in Targeted Therapy for Brain Metastases in Human Epidermal Growth Factor Receptor 2 (HER2)-Positive Breast Cancer: A Focus on ADCs and TKIs
Authors Rao B, Huo P, Lu J, Huang W
Received 30 October 2024
Accepted for publication 28 April 2025
Published 19 May 2025 Volume 2025:17 Pages 423—432
DOI https://doi.org/10.2147/BCTT.S503703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Pooja Advani
Bin Rao, Peicheng Huo, Jieming Lu, Wenwen Huang
Breast Surgery, Wuzhou Red Cross Hospital, Wuzhou City, Guangxi, 543002, People’s Republic of China
Correspondence: Bin Rao, Wuzhou Red Cross Hospital, Wuzhou, People’s Republic of China, Tel +86-0774-3832882, Email [email protected]
Aim: Brain metastasis remains a significant therapeutic challenge in HER2-positive breast cancer, contributing to poor prognosis and limited treatment options. This review aims to summarize recent advancements in targeted therapies for brain metastasis in HER2-positive breast cancer, with a focus on the efficacy, mechanisms, and clinical implications of antibody-drug conjugates (ADCs) and tyrosine kinase inhibitors (TKIs).
Methods: We conducted a comprehensive review of clinical trials, real-world studies, and preclinical research.
Main Content: This review summarizes the latest clinical and preclinical evidence on targeted therapies for brain metastasis in HER2-positive breast cancer. Key therapies, including trastuzumab deruxtecan (T-DXd) and tucatinib, are discussed, with a focus on their mechanisms, efficacy, and ability to overcome the blood-brain barrier (BBB). Clinical trials such as HER2CLIMB and DESTINY-Breast03, as well as real-world studies, are highlighted to demonstrate the superior intracranial response rates and survival benefits of these therapies.
Conclusion: ADCs and TKIs represent a paradigm shift in the management of brain metastases, offering new hope for patients with HER2-positive breast cancer. Future research should focus on optimizing combination therapies, exploring novel biomarkers, and addressing resistance mechanisms to further improve outcomes. This review underscores the importance of continued innovation in targeted therapies for brain metastasis.
Keywords: breast cancer, targeted therapy, antibody-drug conjugates, ADCs, human epidermal growth factor receptor 2-positive, HER2-positive
Current Treatment Status
Brain metastasis has emerged as one of the most significant therapeutic challenges in the management of human epidermal growth factor receptor 2 (HER2)-positive breast cancer, occurring in approximately 30–50% of patients with advanced disease.1 It is associated with poor prognosis, significant morbidity, and diminished quality of life, as metastatic lesions in the central nervous system (CNS) often lead to debilitating neurological symptoms such as headaches, seizures, and cognitive decline.2 Historically, the treatment of brain metastasis has relied heavily on localized therapies, including surgery, whole-brain radiotherapy (WBRT), and stereotactic radiosurgery (SRS).3 While these traditional approaches can provide symptomatic relief and local control, they are often associated with significant side effects, including neurocognitive decline, and do not address systemic disease progression.
Despite the development of novel therapeutic agents that have revolutionized the treatment landscape for advanced HER2-positive breast cancer, localized therapies continue to play a pivotal role in managing brain metastasis.3 According to the 2023 CSCO Breast Cancer Guidelines, the first-line treatment for brain metastasis should primarily consist of localized therapies, with anti-HER2 drugs offering an alternative in HER2-positive patients with manageable symptoms, allowing for a delay in radiotherapy.
The optimization of treatment outcomes for brain metastasis in HER2-positive breast cancer increasingly relies on the identification of predictive biomarkers and the stratification of patients based on molecular and clinical characteristics.4 Biomarkers such as HER2 expression levels, blood-brain barrier (BBB) permeability markers, and circulating tumor DNA (ctDNA) have shown promise in guiding treatment decisions and predicting response to targeted therapies like antibody-drug conjugates (ADCs) and tyrosine kinase inhibitors (TKIs). In recent years, the use of systemic therapies such as antibody-drug conjugates (ADCs) and tyrosine kinase inhibitors (TKIs) has marked a paradigm shift in the treatment of brain metastases.5 These therapies have demonstrated the potential to overcome some of the limitations of traditional treatments, such as resistance and side effects, by targeting the molecular pathways driving tumor growth. While the blood-brain barrier (BBB) has traditionally posed a significant obstacle to the effective delivery of systemic therapies, recent advancements in ADCs and TKIs have shown promising activity against brain metastases, offering hope for better clinical outcomes. The growing understanding of BBB permeability and the development of agents that can efficiently cross it are key factors in the success of these new treatments, paving the way for more effective management of brain metastases in HER2-positive breast cancer patients.
Clinical Strategies
Large Molecule Monoclonal Antibodies
Previous reports indicated that the use of trastuzumab in HER2-overexpressed patients with brain metastasis indeed showed a prolonged overall survival (OS) rate. Compared to patients who were not treated with trastuzumab, the median time to brain metastasis increased from 10 to 15 months (P = 0.035). Moreover, the median time from diagnosis of brain metastasis to death extended from 4.0 to 14.9 months (P = 0.0005).6 The subgroup analysis of brain metastasis patients in the CLEOPATRA study revealed that docetaxel combined with trastuzumab and pertuzumab (referred to as pertuzumab group) significantly extended the median progression-free survival (PFS) (11.9 vs 15 months, HR 0·69, 95% CI 0·59–0·81 P = 0.0049) and OS (34.4 vs 26.3 months, (HR 0·86, 95% CI 0·51–1·43 P = 0.114) compared to the docetaxel combined with trastuzumab (referred to as control treatment group)7. In another instance, the PATRICIA study demonstrated the efficacy and safety attributes of trastuzumab and pertuzumab treatment at a high dosage for brain metastasis.8 In the treatment with pertuzumab combined with a high dose of trastuzumab (6 mg/kg weekly), the objective remission rate (ORR) for CNS metastasis was 11%. The clinical benefit rates (CBR) at 4 and 6 months were over half. These results suggested that the dual-target treatment combining pertuzumab and trastuzumab was more effective than trastuzumab alone in controlling brain metastasis.
Despite their clinical benefits, large molecule monoclonal antibodies face significant challenges, particularly in the context of brain metastasis. One major limitation is their poor penetration of the BBB, which restricts their ability to reach therapeutic concentrations in the CNS. Studies have shown that the concentration of trastuzumab in CSF is approximately 420 times lower than in plasma, highlighting the BBB’s restrictive nature.9 Additionally, acquired resistance to HER2-targeted therapies is a common issue, often driven by mechanisms such as HER2 heterogeneity, activation of alternative signaling pathways (eg, PI3K/AKT/mTOR), and upregulation of drug efflux pumps.10 These resistance mechanisms can significantly reduce the long-term efficacy of monoclonal antibodies.
Small Molecule Tyrosine Kinase Inhibitors (TKIs)
The large-sized molecular drugs are traditionally considered less effective due to their difficulty in entering the brain through the highly complex BBB. Therefore, several efforts have been dedicated towards the development of small molecule TKIs for the treatment of brain metastasis in breast cancer. Notably, some of the reports yielded encouraging data.
Lapatinib
In the Phase II LANDSCAPE trial, the clinical advantages of combining lapatinib with capecitabine in treating HER2-positive metastatic breast cancer patients with untreated brain metastasis were assessed.11 In this study, the clinicians reported a CNS-ORR (Central Nervous System-Objective Response Rate) of 65.9%(95% CI 50.1–79.5%), the CNS-PFS rate of 5.5 months (95% CI: 4.5–6.1 months), and the median time to radiotherapy of 8.3 months(95% CI 5.4–9.1 months). However, in a meta-analysis of 8 studies involving patients with HER2-positive metastatic breast cancer with brain metastasis,12 the CNS-ORR for the combination of lapatinib and capecitabine was only 29% (95% CI 18.5–42.7%).
Neratinib
In the phase II TBCRC 022 trial13, the combination of neratinib and capecitabine was applied to treat patients with HER2-positive CNS metastasis who were naïve to TKI therapy. The results showed a CNS-ORR of 49% (95% CI, 32–66%), with a median PFS of 5.5 months (95% CI: 0.8–18.8 months) and a median OS of 13.3 months (95% CI: 2.2–27.6 months). In one instance, a patient cohort that had previously received lapatinib treatment was closed due to slow enrollment. Interestingly, the CNS-ORR of the cohort study was 33%, with a median PFS of 3.1 months (95% CI: 0.7–14.6 months) and a median OS of 15.5 months (95% CI: 0.8–23.7 months). In another instance, the phase II NEfERT-T trial14 that allowed the inclusion of patients with stable brain metastasis resulted in a lower CNS recurrence rate in the combinatorial group treated with neratinib and paclitaxel compared to the trastuzumab and paclitaxel treatment group (8.3% vs 17.3%,relative risk, 0.48; 95% CI, 0.29–0.79; P = 0.002). The Phase III NALA trial included patients with stage-IV HER2-positive metastatic breast cancer who received ≥2 lines of prior anti-HER2 therapy.15 After randomizing into neratinib plus capecitabine vs lapatinib plus capecitabine treatment groups, the neratinib treatment group showed certain intracranial activity, with fewer patients requiring intervention for symptomatic CNS metastasis over the lapatinib treatment group (22.8% vs 29.2%,HR = 0.71, 95% CI: 0.54–0.93; P = 0.043).
Tucatinib
Tucatinib shows high selectivity for the kinase domain of HER2 with minimal inhibition of the epidermal growth factor receptor. The pivotal phase III HER2CLIMB trial enrolled 612 patients with HER2-positive metastatic breast cancer who had previously received trastuzumab, pertuzumab, and trastuzumab emtansine (T-DM1). Further, these patients were randomly assigned in a 2:1 ratio to receive tucatinib + trastuzumab + capecitabine (referred to as tucatinib treatment group) or placebo + trastuzumab + capecitabine (control treatment group). Among the recruited 291 patients with brain metastasis, 198 patients in the tucatinib treatment group (including 80 with stable and 118 with active brain metastasis) and 93 patients in the control treatment group (37 with stable and 56 with active brain metastasis) were determined. Further, the updated subgroup analysis of brain metastasis from the study16 showed a significant extension in median OS by 9.1 months (21.6 vs 12.5 months, CI, 18.1–28.5 vs 11.2–16.9; p<0.05) in the tucatinib treatment group at a median follow-up of 29.6 months. In the patients with active brain metastasis (21.4 vs 11.8 months) and stable brain metastasis (21.6 vs 16.4 months), the median PFS was recorded as 9.9 months (95% CI, 8.4–11.7 months), which was significantly better than the placebo group (4.2 months) (95% CI, 3.6–5.7 months). Concerning the intracranial response, both the treatment groups showed a significant difference in the median CNS-PFS (9.9 vs 4.2 months, P<0.05), with active brain metastasis patients at 9.6 vs 4.0 months (P<0.05) and stable brain metastasis patients at 13.9 vs 5.6 months(P<0.05). It should be noted that these findings were consistent with the overall trend of benefit in the brain metastasis population. In addition, the intracranial ORR in the tucatinib group was 47.3%(95% CI, 33.7%–61.2%), which was significantly higher than 20.0% (95% CI, 5.7%–43.7%) in the placebo group (P<0.05), with a median duration of response (DOR) of 8.6 months (95% CI: 5.5–10.3 months) vs 3.0 months (95% CI: 3.0–10.3 months, P<0.05).
Pyrotinib
The phase III PHENIX trial included 31 patients with stable brain metastasis. The subgroup analysis indicated that the combination of pyrotinib and capecitabine significantly prolonged the median PFS rate compared to placebo and capecitabine (6.9 vs 4.2 months, P = 0.011).17 Specifically, the phase II PERMEATE study explored the clinical benefit of the combination of pyrotinib and capecitabine in treating HER2-positive patients with active brain metastasis18. The enrolled patients (n=78) were divided into two cohorts, in which cohort A received no prior radiotherapy (n=59) and cohort B received progression after radiotherapy (n=19). Accordingly, cohort A demonstrated a CNS-ORR of 74.6% and a median PFS of 11.3 months, while cohort B displayed a CNS-ORR of 42.1% and a median PFS of 5.6 months.
Overall, these studies collectively demonstrated the efficacy of small-molecule TKIs in treating brain metastasis in breast cancer patients, likely related to their easier penetration of the BBB as small molecules. Although no direct head-to-head comparisons were available, a horizontal comparison of several TKIs in treating brain metastasis, particularly the performance of tucatinib plus trastuzumab plus capecitabine, indicated this dual-target combination as a potentially promising treatment choice in the field of HER2-positive breast cancer brain metastasis.
Antibody-Drug Conjugates (ADCs) Drugs
T-DM1
T-DM1 was the first ADC drug approved in the field of breast cancer. Notably, this T-DM1 suffers from similar limitations to trastuzumab in penetrating the BBB due to its large biomolecular structure. Nevertheless, the clinical data of T-DM1 indicated that it possesses certain intracranial activity. In the EMILIA study, a subgroup analysis of patients with brain metastasis showed that the median PFS in the T-DM1 treatment group was comparable to the combination treatment group of lapatinib and capecitabine (5.9 vs 5.7 months; HR = 1.00; P = 1.000). Nevertheless, the median OS rate in the T-DM1 treatment group showed a significantly higher rate of 26.8 months compared to the lapatinib plus capecitabine group (12.9 months, HR = 0.38; P = 0.008).19 In addition, the KAMILLA study recorded the clinical data of the 398 patients with baseline brain metastasis receiving T-DM1 treatment, including those with untreated asymptomatic brain metastasis or those who had received radiotherapy more than 14 days prior to enrollment as well as patients with controlled brain disease. Notably, the median OS was recorded as 18.9 (95% CI 17.1–21.3) months, along with the median PFS rate of 5.5 (95% CI 5.3–5.6) months.20
Trastuzumab Deruxtecan (T-DXd)
T-DXd has emerged as one of the novel anti-HER2 ADC drugs. Recently, it has been recognized as the most efficient drug in the treatment of brain metastasis in HER2-positive breast cancer. In its multi-center, single-arm, phase II DESTINY-Breast01 study, 24 patients treated with stable brain metastasis were enrolled. According to the latest results published in Cancer Discovery in October 2022, the ORR, PFS, and DOR rates were 58.3%[95% CI, 36.6–77.9%], 18.1 months(95% CI, 6.7–18.1 months)., and 16.9 (95% CI, 5.7–16.9)months, respectively, comparable to the overall study population.21
The DESTINY-Breast03, a phase III clinical study, compared the efficacy and safety of T-DXd with T-DM1 in the second-line treatment for HER2-positive advanced breast cancer. Among the 82 patients with stable brain metastasis selected for this study, the median PFS for the T-DXd group was significantly better than that of the T-DM1 group (15 vs 3 months). The recorded ORR values were 67.4% and 20.5%, respectively, with intracranial ORR rates of 63.9% and 33.4%.22
Against the backdrop of intracranial benefits of T-DXd, two ongoing phase II trials, named TUXEDO-1 and DEBBRAH, specifically assessed the efficacy of T-DXd in patients with brain metastasis. In the TUXEDO-1 study, patients (n=15) with newly diagnosed brain metastasis or progression after local treatment in the metastatic disease phase (ie, active brain metastasis) were recruited. The updated data at a median follow-up of 12 months23 showed that the median PFS rate for enrolled patients was 14 months(95% CI 11.0 - not recorded), with the best overall intracranial ORR of 73.3%(95% CI: 48.1–89.1%), meeting the predefined primary study endpoint (CNS response rate assessed by RANO-BM criteria). To this end, the patients in the DEBBRAH study were divided to treat HER2-positive or HER2-low expressing advanced breast cancers with CNS disease into five cohorts, including (1) HER2-positive advanced breast cancer with stable brain metastasis after radiotherapy and/or surgery, (2) HER2-positive or HER2-low expressing advanced breast cancer with asymptomatic untreated brain metastasis, (3) HER2-positive advanced breast cancer with brain metastasis progressing after local treatment, (4) HER2-low expressing advanced breast cancer with brain metastasis progressing after local treatment, and (5) HER2-positive or HER2-low expressing advanced breast cancer with leptomeningeal carcinomatosis (LMC). The data for cohorts 1, 2, and 3 in HER2-positive breast cancer brain metastasis revealed that cohort 1 showed a 16-week PFS rate of 87.5% (95% CI, 47.3–99.7; P < 0.001).24 After the data cutoff, several patients (n=3, 37.5%) experienced progressive disease (PD) (1 intracranial, 2 extracranial). In cohort 2, 2 patients achieved intracranial partial response (PR, n=50%) with an intracranial ORR of 50%, and no patients experienced intracranial PD. In cohort 3, 4 patients attained the intracranial PR (44.4%) with an intracranial ORR of 44.4%. In addition, a patient (11.1%) showed stable disease (SD) lasting ≥24 weeks, 3 patients (33.3%) exhibited SD <24 weeks, and 1 patient (11.1%) showed PD. Together, 4 patients (44.4%) experienced PD across the three cohorts at the time of data cutoff. The intracranial ORR of patients with active brain metastasis (cohorts 2 and 3) was 46.2%.
Moreover, an exploratory pooled analysis described the characteristics of patients with baseline brain metastasis, either treated/stable or untreated/active, in the DB01, 02, and 03 studies. The analysis assessed the exploratory pooled efficacy of T-DXd through a blinded independent central review toward evaluating its safety profile compared to the control treatment group.25 Among the recruited patients (n=148) with baseline brain metastasis subjected to T-DXd treatment, 104 patients (70.3%) were previously treated, and 44 patients (29.7%) were untreated. In the control treatment group of patients (n=83), 58 patients (69.9%) were previously treated, and 25 patients (30.1%) were untreated. The results showed that the median treatment duration with T-DXd was 12.7 months, compared to 5.6 months in the control treatment group. Moreover, the T-DXd treatment group demonstrated significant efficacy in both treated/stable and active brain metastasis patients compared to the control treatment group. The intracranial ORR values for the T-DXd and control treatment groups were 45.2% vs 27.6% for stable brain metastasis and 45.5% vs 12.0% for active brain metastasis. The complete response (CR) rates were 16.3% vs 3.4% for stable brain metastasis and 15.9% vs 0% for active brain metastasis. The intracranial PFS values for the T-DXd and the control groups were 12.3 months vs 8.7 months for stable brain metastasis and active brain metastasis, 18.5 months vs 4.0 months. The intracranial DOR for T-DXd and the control treatment groups were 12.3 months vs 11.0 months for stable brain metastasis and 17.5 months vs not applicable (NA) for active brain metastasis.
In a meta-analysis incorporating data from 10 studies, 336 patients with HER2-positive advanced breast cancer with brain metastasis were evaluated for the efficacy and safety of T-DXd treatment. The results showed a median PFS of 15 months, an ORR of 61%, and an intracranial ORR of 62%. Notably, no significant differences were observed in ORR and intracranial ORR values between clinical trials and observational studies. Moreover, the CBR was 80% (95% CI: 52–94%) with an intracranial CBR of 69% (95% CI 54–82%). The ORR value in patients with stable brain metastasis was slightly higher (64%) compared to patients with active brain metastasis (61%). However, no significant difference between the two groups was observed (P = 0.78).26
The ROSET-BM, a multicenter, retrospective case study, presented data involving 104 hER2-positive advanced breast cancer patients with brain/LMC metastasis.27 The median PFS rate was 16.1 months without reaching the median OS rate. The median time to treatment failure (TTF) was 9.7 months. Stratified by type of brain metastasis, the median PFS value for patients with active brain metastasis was recorded as 13.4 months without reaching the median OS. For patients with stable brain metastasis, the median PFS rate was recorded as 14.6 months without reaching the median OS.
Moreover, neither median PFS nor OS rates for LMC patients were attained. Among the enrolled patients (n= 89) with available brain imaging data, the intracranial ORR value was recorded as 62.7%, with a 6-month intracranial CBR value of 70.6%, and a median intracranial PFS of 16.1 months. The intracranial ORR value for active brain metastasis in patients stratified by brain metastasis type was recorded as 54.1%, with a 6-month intracranial CBR of 62.2% and a median intracranial PFS of 16.1 months. For stable brain metastasis, the intracranial ORR was denoted as 100%, with a 6-month intracranial CBR of 100%. However, the median intracranial PFS rate was not attained. For LMC patients, the intracranial ORR value was recorded as 77.8%, with a 6-month intracranial CBR of 88.9% and a median intracranial PFS value of 12.2 months.
In addition, several ongoing studies on T-DXd for breast cancer brain metastasis include DESTINY-Breast12 28 and HER2CLIMB-04.29 DESTINY-Breast12 is a phase IIIb/IV study evaluating the efficacy and safety of T-DXd in patients with HER2-positive advanced or metastatic breast cancer with or without brain metastasis who have received prior treatment. The DESTINY-Breast12 study is conducted randomly on 500 patients into two cohorts at a ratio of 1:1, including baseline without brain metastasis (cohort 1) and baseline with brain metastasis (cohort 2, untreated brain metastasis not requiring immediate local treatment or previously treated stable or progressive brain metastasis).
To this end, HER2CLIMB-04 is a phase II clinical study evaluating the clinical efficacy of tucatinib plus T-DXd in patients with HER2-positive inoperable, locally advanced, or metastatic breast cancer who have received ≥2 prior anti-HER2 treatments. After validating the safety of the drug combination (tucatinib plus T-DXd), the patients (n=60) enrolled and divided into cohorts at the ratio of 1:1 with and without a history of brain metastasis (including patients with active brain metastasis). The study aims to explore the efficacy and safety considerations of combining two of the most promising drugs for brain metastasis. These studies, from monotherapy to combination therapy, comprehensively cover both stable and active brain metastasis, aiming to further explore the therapeutic potential of T-DXd for breast cancer brain metastasis. Nevertheless, future results are eagerly anticipated to demonstrate the clinical efficacy.
The efficacy of various therapies (eg, CNS-ORR, PFS, OS) is summarized in Table 1.
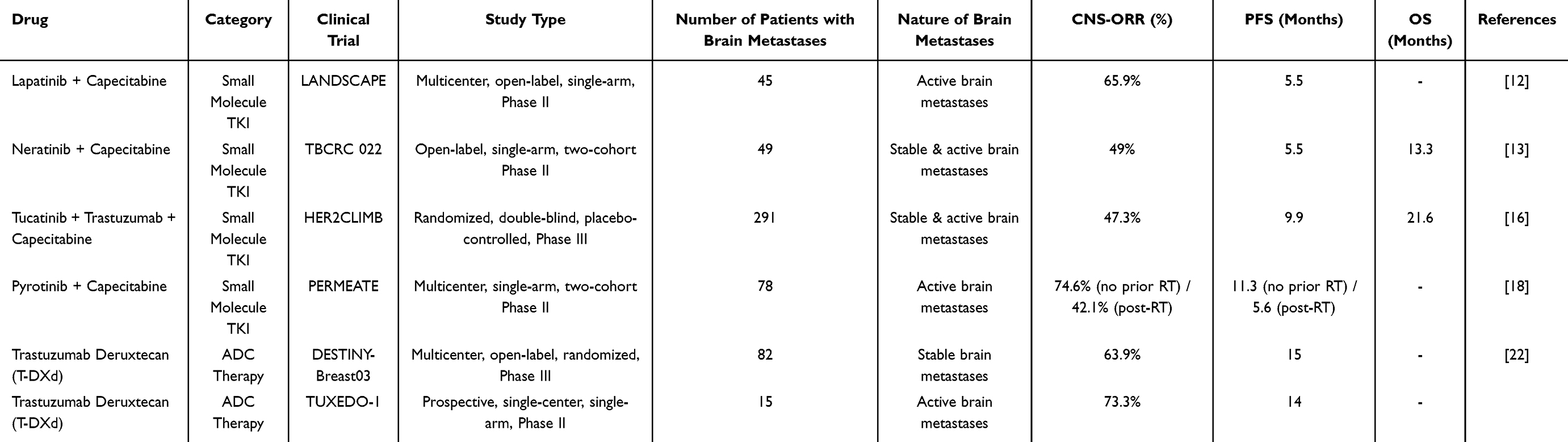 |
Table 1 Comparison of Key Systemic Therapies for HER2-Positive Breast Cancer with Brain Metastases |
Mechanism of T-DXd
Several clinical studies have confirmed the value of T-DXd in treating brain metastasis in breast cancer, challenging the traditional belief that large-molecule drugs are ineffective in this context.30 The BBB typically protects the brain by preventing large molecules or harmful substances from entering. However, this protective function can be a “double-edged sword” for patients with brain metastasis undergoing systemic treatment, as it also limits drug delivery to the brain. Previous studies have shown that poor treatment efficacy in these patients is often linked to the inability of certain drugs to cross the BBB.31
During brain metastasis, the BBB’s integrity is often compromised.31 In addition, the effects of whole-brain radiation therapy (WBRT) may increase the permeability of the barrier, allowing more drugs to reach the brain. For example, in HER2-positive breast cancer patients with brain metastasis treated with trastuzumab, the concentration of the drug in the cerebrospinal fluid increased significantly after WBRT, indicating improved drug delivery to the brain.32
T-DXd’s effectiveness in treating brain metastasis is closely related to its unique structure and mechanism of action. It is an antibody-drug conjugate (ADC) that consists of a monoclonal antibody linked to a powerful chemotherapy drug. The antibody specifically targets tumor cells, while the attached drug payload is delivered directly to the cancer cells. This design allows T-DXd to remain stable in the bloodstream, minimizing off-target effects. The drug payload is highly potent and can penetrate tumor cells, even those adjacent to the primary tumor, where it can kill additional cancer cells through a “bystander effect.”.33–35 These features make T-DXd particularly effective in treating brain metastasis in breast cancer, offering a promising therapeutic approach. With ongoing research and further clinical data, there is significant potential for T-DXd to play a key role in treating brain metastasis in the future.
Targeted Strategy
With the emergence of several innovative anti-HER2 drugs, TKIs, and ADCs have become the most promising treatments for brain metastasis in breast cancer patients. In the case of HER2-positive breast cancer brain metastasis, several reported clinical studies primarily focused on small molecule TKIs, exhibiting excellent therapeutic efficacy in patients with active brain metastasis. In addition, several drugs, like pyrotinib and tucatinib, demonstrated effective intracranial activity. The advent of the ADC drug T-DXd, following small molecule TKIs, presented another effective treatment option for breast cancer brain metastasis. The pooled analysis of brain metastasis populations in the DB01, 02, and 03 clinical trials and the meta-analysis of T-DXd in HER2-positive breast cancer brain metastasis confirmed the therapeutic benefits of T-DXd in patients with stable and active brain metastasis. These findings provided new treatment options for these patients, enriching the evidence base for novel ADC drugs in treating brain metastasis in breast cancer patients. T-DXd showed excellent intracranial efficacy in both stable and active brain metastasis in HER2-positive breast cancer. It is increasingly recognized that these advances in drug therapy have been gradually changing the treatment philosophy for brain metastasis. The 2023 CSCO guidelines prioritize localized therapies, reflecting regional practices, but the evidence supporting ADCs and TKIs is likely to influence future updates, further integrating these therapies into standard care. However, the 2023 ESMO guidelines highlight the growing role of ADCs and TKIs in HER2-positive breast cancer brain metastases, recommending T-DXd for stable brain metastases and tucatinib plus chemotherapy for active brain metastases. The 2023 ESMO guidelines for metastatic breast cancer recommend that treatment should be stratified based on brain metastasis status for second-line treatment of HER2-positive metastatic breast cancer. T-DXd is the sole recommendation for patients with stable brain metastasis or unknown brain metastasis status. In contrast, tucatinib combined with chemotherapy is the preferred first-line treatment for breast cancer with brain metastasis that requires no immediate local intervention.29
Limitations of Current Therapies
In real-world clinical settings, the integration of targeted therapies such as T-DXd, tucatinib, and pyrotinib presents several challenges. While these therapies have demonstrated promising efficacy in clinical trials, their successful implementation in practice depends on factors such as patient selection, which varies from clinical trial populations, and the need to combine systemic treatments with localized therapies like surgery and radiotherapy. Moreover, accessibility remains a significant barrier, with the high cost of these therapies limiting access for many patients, particularly in low-income or resource-limited settings. Geographic and institutional variability also plays a role, as not all regions or healthcare systems have timely access to these treatments. Furthermore, adapting healthcare systems to incorporate these advanced therapies requires training healthcare providers, monitoring patients effectively, and ensuring efficient drug administration.
Drug resistance further complicates the use of these therapies. Mechanisms such as HER2 heterogeneity, reduced internalization of ADCs, lysosomal dysfunction, and upregulation of drug efflux pumps can limit the long-term efficacy of treatments like T-DXd. Additionally, the tumor microenvironment (TME) and blood-brain barrier (BBB) pose unique challenges in brain metastases, restricting drug delivery and promoting resistance. Addressing these resistance mechanisms through combination therapies, next-generation ADCs, and biomarker-driven strategies is essential to improving outcomes.
Addressing these challenges—ranging from accessibility and cost to drug resistance—is crucial to ensuring that these life-changing therapies are available and effective for all eligible patients.
Conclusions
Brain metastasis remains a common and challenging complication of HER2-positive advanced breast cancer, significantly impacting patient prognosis and quality of life. The development of anti-HER2 therapeutic drugs, particularly antibody-drug conjugates (ADCs) like trastuzumab deruxtecan (T-DXd), has revolutionized the treatment landscape. T-DXd, with its unique mechanism and ability to penetrate the blood-brain barrier (BBB), has subverted the traditional belief that small molecule drugs are more effective in treating brain metastasis. Clinical trials such as DEBBRAH have demonstrated T-DXd’s promising efficacy in leptomeningeal carcinomatosis (LMC), with a median overall survival (OS) of 13.3 months and prolonged stabilization in 71.4% of patients.1 Real-world analyses further support its intracranial activity, showing an 88% disease control rate in active brain metastasis.2 These advancements highlight the potential of ADCs to address unmet needs in this difficult-to-treat population.
Looking ahead, the combination of systemic therapies, such as ADCs and tyrosine kinase inhibitors (TKIs), with localized treatments like radiotherapy and surgery, offers a promising approach to improving outcomes. For example, preclinical evidence suggests that radiotherapy-induced BBB disruption may enhance the delivery of ADCs to brain metastases.3 Additionally, exploring novel biomarkers, such as BBB permeability markers and CSF-based liquid biopsies, could enable personalized treatment strategies and improve response prediction. Overcoming resistance mechanisms, optimizing the sequencing of therapies, and addressing LMD remain critical areas for future research. Incorporating patient-reported outcomes (PROs) to assess quality of life and cognitive function will ensure that therapies not only extend survival but also enhance well-being.
In conclusion, the continuous advancement of therapeutic drugs, combined with a multidisciplinary approach integrating systemic and localized treatments, holds great promise for improving the prognosis and quality of life of patients with HER2-positive breast cancer brain metastasis. Future research should focus on validating these findings in larger cohorts, optimizing treatment combinations, and addressing remaining gaps to deliver more effective and patient-centered care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zimmer AS, Van Swearingen AED, Anders CK. HER2-positive breast cancer brain metastasis: a new and exciting landscape. Cancer Rep. 2022;5(4):e1274. doi:10.1002/cnr2.1274
2. Soffietti R, Pellerino A. Brain Metastasis from HER2-Positive Breast Cancer: an Evolving Landscape. Clin Cancer Res. 2023;29(1):8–10. doi:10.1158/1078-0432.CCR-22-2853
3. Bailleux C, Eberst L, Bachelot T. Treatment strategies for breast cancer brain metastases. Br J Cancer. 2021;124(1):142–155. doi:10.1038/s41416-020-01175-y
4. Hosonaga M, Saya H, Arima Y. Molecular and cellular mechanisms underlying brain metastasis of breast cancer. Cancer Metastasis Rev. 2020;39(3):711–720. doi:10.1007/s10555-020-09881-y
5. Niu L, Lv H, Zhang M, et al. Clinical diagnosis and treatment of breast cancer with brain metastases and establishment of a prognostic model: a 10-year, single-center, real-world study of 559 cases. Ann Transl Med. 2021;9(16):1331. doi:10.21037/atm-21-3734
6. Park YH, Park MJ, Ji SH, et al. Trastuzumab treatment improves brain metastasis outcomes through control and durable prolongation of systemic extracranial disease in HER2-overexpressing breast cancer patients. Br J Cancer. 2009;100(6):894–900. doi:10.1038/sj.bjc.6604941
7. Swain SM, Miles D, Kim SB, et al. Pertuzumab, trastuzumab, and docetaxel for HER2-positive metastatic breast cancer (CLEOPATRA): end-of-study results from a double-blind, randomized, placebo-controlled, Phase 3 study. Lancet Oncol. 2020;21(4):519–530. doi:10.1016/S1470-2045(19)30863-0
8. Lin NU, Pegram M, Sahebjam S, et al. Pertuzumab plus high-dose trastuzumab in patients with progressive brain metastases and HER2-positive metastatic breast cancer: primary analysis of a phase II study. J Clin Oncol. 2021;39(24):2667–2675. doi:10.1200/JCO.20.02822
9. Bachelot T, Romieu G, Campone M, et al. Lapatinib plus capecitabine in patients with previously untreated brain metastases from HER2-positive metastatic breast cancer (LANDSCAPE): a single-group Phase 2 study. Lancet Oncol. 2013;14(1):64–71. doi:10.1016/S1470-2045(12)70432-1
10. Gallardo A, Lerma E, Escuin D, et al. Increased signalling of EGFR and IGF1R, and deregulation of PTEN/PI3K/Akt pathway are related with trastuzumab resistance in HER2 breast carcinomas. Br J Cancer. 2012;106(8):1367–1373. doi:10.1038/bjc.2012.85
11. Petrelli F, Ghidini M, Lonati V, et al. The efficacy of lapatinib and capecitabine in HER-2 positive breast cancer with brain metastases: a systematic review and pooled analysis. Eur J Cancer Oxf Engl. 2017;84:141–148. doi:10.1016/j.ejca.2017.07.024
12. Freedman RA, Gelman RS, Anders CK, et al. TBCRC 022: a Phase II Trial of Neratinib and Capecitabine for Patients With Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer and Brain Metastases. J Clin Oncol. 2019;37:1081–1089. doi:10.1200/JCO.18.01511
13. Awada A, Colomer R, Inoue K, et al. Neratinib plus paclitaxel vs trastuzumab plus paclitaxel in previously untreated metastatic ERBB2- positive breast cancer: the NEfERT-T randomized clinical trial. JAMA Oncol. 2016;2(12):1557–1564. doi:10.1001/jamaoncol.2016.0237
14. Saura C, Oliveira M, Feng YH, et al. Neratinib Plus Capecitabine Versus Lapatinib Plus Capecitabine in HER2-Positive Metastatic Breast Cancer Previously Treated With ≥ 2 hER2-Directed Regimens: phase III NALA Trial. J Clin Oncol. 2020;38(27):3138–3149. doi:10.1200/JCO.20.00147
15. Lin NU, Murthy RK, Abramson V, et al. Tucatinib vs Placebo, Both in Combination With Trastuzumab and Capecitabine, for Previously Treated ERBB2 (HER2)-Positive Metastatic Breast Cancer in Patients With Brain Metastases: updated Exploratory Analysis of the HER2CLIMB Randomized Clinical Trial. JAMA Oncol. 2023;9(2):197–205. doi:10.1001/jamaoncol.2022.5610
16. Yan M, Bian L, Hu X, et al. Pyrotinib plus capecitabine for human epidermal growth factor receptor 2-positive metastatic breast cancer after trastuzumab and taxanes (PHENIX): a randomized, double-blind, placebo-controlled phase 3 study. Transl Breast Cancer Res. 2020;1:13. doi:10.21037/tbcr-20-25
17. Yan M, Ouyang Q, Sun T, et al. Pyrotinib plus capecitabine for patients with human epidermal growth factor receptor 2-positive breast cancer and brain metastases (PERMEATE): a multicentre, single-arm, two-cohort, phase 2 trial. Lancet Oncol. 2022;23(3):353–361. doi:10.1016/S1470-2045(21)00716-6
18. Krop IE, Lin NU, Blackwell K, et al. Trastuzumab emtansine (T-DM1) versus lapatinib plus capecitabine in patients with HER2-positive metastatic breast cancer and central nervous system metastases: a retrospective, exploratory analysis in EMILIA. Ann Oncol. 2015;26(1):113–119. doi:10.1093/annonc/mdu486
19. Montemurro F, Delaloge S, Barrios CH, et al. Trastuzumab emtansine (T-DM1) in patients with HER2-positive metastatic breast cancer and brain metastases: exploratory final analysis of cohort 1 from KAMILLA, a single-arm phase IIIb clinical trial. Ann Oncol. 2020;31(10):1350–1358. doi:10.1016/j.annonc.2020.06.020
20. Jerusalem G, Park YH, Yamashita T, et al. Trastuzumab Deruxtecan in HER2-Positive Metastatic Breast Cancer Patients with Brain Metastases: a DESTINY-Breast01 Subgroup Analysis. Cancer Discov. 2022;12(12):2754–2762. doi:10.1158/2159-8290.CD-22-0837
21. Hurvitz S, Kim SB, Chung WP, et al. Abstract GS3-01: trastuzumab deruxtecan (T-DXd; DS-8201a) vs. trastuzumab emtansine (T-DM1) in patients (pts) with HER2+ metastatic breast cancer (mBC): subgroup analyses from the randomized phase 3 study DESTINY-Breast03. Cancer Res. 2022;82(4_Supplement):GS3–01. doi:10.1158/1538-7445.SABCS21-GS3-01
22. Bartsch R, Berghoff AS, Furtner J, et al. Trastuzumab deruxtecan in HER2-positive breast cancer with brain metastases: a single-arm, phase 2 trial. Nat Med. 2022;28(9):1840–1847. doi:10.1038/s41591-022-01935-8
23. Pérez-García JM, Vaz Batista M, Cortez P, et al. Trastuzumab deruxtecan in patients with central nervous system involvement from HER2-positive breast cancer: the DEBBRAH trial. Neuro Oncol. 2023;25(1):157–166. doi:10.1093/neuonc/noac144
24. Hurvitz SA, Modi S, Li W, et al. A pooled analysis of trastuzumab deruxtecan (T-DXd) in patients (pts) with HER2-positive (HER2+) metastatic breast cancer (mBC) with brain metastases (BMs) from DESTINY-Breast (DB) −01, −02, and −03. Ann Oncol. 2023;34:S335–6. doi:10.1016/j.annonc.2023.09.554
25. Michelon IF, Vilbert MS, Marinho AD, et al. 414P Trastuzumab deruxtecan for HER2-positive breast cancer brain metastasis: a systematic review and meta-analysis. Ann Oncol. 2023;34:S357. doi:10.1016/j.annonc.2023.09.591
26. Yamanaka T, Nikura N, Nomura H, et al. Abstract PD7-01: trastuzumab deruxtecan for the treatment of patients with HER2-positive breast cancer with brain and/or leptomeningeal metastases: a multicenter retrospective study (ROSET-BM study). Cancer Res. 2023;83(5_Supplement):D7–01. doi:10.1158/1538-7445.SABCS22-PD7-01
27. Lin NU, Ciruelos E, Jerusalem G, et al. Open-label, multinational, multicenter, phase 3b/4 study of trastuzumab deruxtecan (T-DXd) in patients with or without baseline brain metastasis with previously treated advanced/metastatic human epidermal growth factor receptor 2–positive breast cancer: DESTINY-Breast12.2021 ESMO.335TiP. Oncology Research and Treatment. 2022;45:23–24.
28. Hurvitz S, et al. HER2CLIMB-02: randomized, Double-Blind Phase 3 Trial of Tucatinib and Trastuzumab Emtansine for Previously Treated HER2-Positive Metastatic. Breast Cancer. 2023;2023:1.
29. Keith KC, Lee Y, Ewend MG, et al. Activity of trastuzumab- emtansine (T-DM1) in HER2- positive breast cancer brain metastases: a case series. Cancer Treat Commun. 2016;7:43–46. doi:10.1016/j.ctrc.2016.03.005
30. Podder V, Ranjan T, Gowda M, Camacho AM, Ahluwalia MS. Emerging Therapies for Brain Metastases in NSCLC, Breast Cancer, and Melanoma: a Critical Review. Curr Neurol Neurosci Rep. 2024;25(1):6. doi:10.1007/s11910-024-01388-1
31. Sevieri M, Mazzucchelli S, Barbieri L, et al. Ferritin nanoconjugates guide trastuzumab brain delivery to promote an antitumor response in murine HER2 + breast cancer brain metastasis. Pharmacol Res. 2023;196:106934. doi:10.1016/j.phrs.2023.106934
32. Stemmler HJ, Schmitt M, Willems A, et al. Ratio of trastuzumab levels in serum and cerebrospinal fluid is altered in HER2-positive breast cancer patients with brain metastases and impairment of blood-brain barrier. Anticancer Drugs. 2007;18(1):23–28. doi:10.1097/01.cad.0000236313.50833.ee
33. Ogitani Y, Aida T, Hagihara K, et al. DS-8201a, A Novel HER2-Targeting ADC with a Novel DNA Topoisomerase I Inhibitor, Demonstrates a Promising Antitumor Efficacy with Differentiation from T-DM1. Clin Cancer Res. 2016;22(20):5097–5108. doi:10.1158/1078-0432.CCR-15-2822
34. Nakada T, Masuda T, Naito H, et al. Novel antibody drug conjugates containing exatecan derivative-based cytotoxic payloads. Bioorg Med Chem Lett. 2016;26(6):1542–1545. doi:10.1016/j.bmcl.2016.02.020
35. Nakada T, Sugihara K, Jikoh T, et al. The Latest Research and Development into the Antibody-Drug Conjugate, [fam-] Trastuzumab Deruxtecan (DS-8201a), for HER2 Cancer Therapy. Chem Pharm Bull. 2019;67(3):173–185. doi:10.1248/cpb.c18-00744
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Breast Cancer: An Overview of Current Therapeutic Strategies, Challenge, and Perspectives
Wang J, Wu SG
Breast Cancer: Targets and Therapy 2023, 15:721-730
Published Date: 20 October 2023
Dysregulation of Fatty Acid Metabolism in Breast Cancer and Its Targeted Therapy
Chang Y, Du R, Xia F, Xu X, Wang H, Chen X
Breast Cancer: Targets and Therapy 2024, 16:825-844
Published Date: 29 November 2024
From Pioneering Discoveries to Innovative Therapies: A Journey Through the History and Advancements of Nanoparticles in Breast Cancer Treatment
Basingab FS, Alshahrani OA, Alansari IH, Almarghalani NA, Alshelali NH, Alsaiary AH, Alharbi N, Zaher KA
Breast Cancer: Targets and Therapy 2025, 17:27-51
Published Date: 21 January 2025
Emerging Targeted and Multimodal Therapeutic Strategies in Breast Cancer: A Comprehensive Review
Wu W, He Y, Zhang C
Breast Cancer: Targets and Therapy 2026, 18:575936
Published Date: 7 January 2026
ADPB Sensitivity in Breast Cancer is Correlated with LAT1 Expression: An in vitro Study of a Novel Theranostic Candidate
Kusumahstuti KP, Holik HA, Bashari MH, Achmad A, Shamsuddin S, Kartamihardja AHS
Breast Cancer: Targets and Therapy 2026, 18:564513
Published Date: 7 May 2026