Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 18
Advances in Stem Cell Therapy for Diabetic Foot Ulcers
Authors Wang B, Zhao G, Zhang J, Chen W, Yang S, Sun Y
Received 5 September 2025
Accepted for publication 21 October 2025
Published 29 October 2025 Volume 2025:18 Pages 4021—4034
DOI https://doi.org/10.2147/DMSO.S564011
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Halis Akturk
Bin Wang,1,2 Gang Zhao,2,3 Jiaqi Zhang,4 Wenyu Chen,2 Shanshan Yang,1 Yinuo Sun1
1Department of Surgery, The First Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine, Harbin, Heilongjiang, 150040, People’s Republic of China; 2First Clinical Medical College, Heilongjiang University of Traditional Chinese Medicine, Harbin, Heilongjiang, 150040, People’s Republic of China; 3Department of Peripheral Vascular Surgery, The First Affiliated Hospital of Heilongjiang University of Traditional Chinese Medicine, Harbin, Heilongjiang, 150040, People’s Republic of China; 4Department of Pharmaceutical Engineering, Harbin Labor Technician College, Harbin, Heilongjiang, 150500, People’s Republic of China
Correspondence: Gang Zhao, Email [email protected]
Abstract: Diabetic foot ulcers (DFU) are a severe and recurrent complication of diabetes that significantly increase the risk of infection, amputation, and mortality. Conventional therapies often fail to achieve complete healing due to the complex microenvironment characterized by ischemia, chronic inflammation, neuropathy, and oxidative stress. Stem-cell-based interventions offer a multifaceted therapeutic strategy by promoting angiogenesis, modulating immune responses, reducing oxidative damage, and enhancing extracellular matrix remodeling. This review provides a comprehensive analysis of major stem-cell sources including bone marrow-derived mesenchymal stem cells (BM-MSCs), adipose-derived stem cells (ADSCs), umbilical cord blood mesenchymal stem cells (UCB-MSCs), and induced pluripotent stem cells (iPSCs). Comparative evaluation highlights that ADSCs are advantageous for autologous use and easy harvesting, BM-MSCs have the longest clinical track record, UCB-MSCs offer low immunogenicity for allogeneic applications, and iPSCs provide customizable options but require genomic stability monitoring. Increasing evidence supports the use of cell-free approaches, particularly exosome and secretome-based therapies, which reproduce stem-cell paracrine effects while minimizing ethical and safety concerns. Integration of these biologics with advanced biomaterials and nanoplatforms further enhances local retention, controlled release, and wound microenvironment regulation. Despite encouraging results, challenges remain in standardizing cell preparation, optimizing dosage and delivery, and ensuring long-term safety and cost-effectiveness. Future directions include harmonizing clinical protocols, expanding exosome-based therapeutics, and conducting large multicenter trials to validate their efficacy in real-world DFU management.
Keywords: diabetic foot ulcer, stem cell therapy, mechanism of action, clinical application, diabetes, wound
Introduction
Diabetic foot ulcers (DFU) are one of the most common and severe complications in diabetic patients, with an increasing incidence rate. Globally, the prevalence of DFU represents a significant burden. According to the most recent International Diabetes Federation (IDF) Diabetes Atlas, the number of people with diabetes worldwide has exceeded 536 million and is projected to rise to 783 million by 2045.1 The prevalence of DFU globally is approximately 6.3%, with notable variations across regions; for instance, it can reach as high as 13.0% in North America and as low as 1.5% in Africa.2 DFU not only severely impacts patientsand#039; quality of life but also imposes a heavy economic burden on healthcare systems. It is estimated that about 18.6 million people develop DFU each year, with approximately 2 million requiring amputation as a result. In the United States, the direct treatment costs for diabetic foot ulcer patients are estimated between $9 billion and $13 billion annually. Additionally, the recurrence rate of DFU is high, with a lifetime recurrence rate ranging from 19% to 34%.3
DFU presents complex wounds that are difficult to heal and prone to recurrence, ultimately leading to amputation or even threatening life, placing a heavy burden on patients and their families. The foot is the primary site for diabetic complications, where neuropathy and vascular disease in the distal lower limbs cause infections or ulcers, leading to deep tissue destruction. The main symptoms include mild neuropathy, ischemic rest pain, DFU, Charcot’s joint disease, and neurogenic fractures, often accompanied by infection, immune deficiency, and lower limb vascular disease.4–6 The pathogenesis of DFU is extremely complex (see Figure 1), involving multiple pathological processes such as neuropathy, vascular disease, infection, immune abnormalities, biofilm formation, and mechanical stress interacting with each.7–10 These factors collectively contribute to the occurrence, development, and difficulty in healing of foot ulcers. Although traditional treatments have alleviated the condition to some extent, they have significant limitations and fail to address the underlying pathological issues of DFU. The high recurrence rate of DFU is a major challenge for traditional treatments. Surgical debridement and standard care, the recurrence rate of DFU remains high, with some patients requiring multiple amputations.11 Moreover, the presence of infection and chronic inflammation further exacerbates the difficulty in ulcer healing.4 Treatment for DFU typically requires long-term medical intervention, including multiple surgeries, medication, and nursing services. This not only imposes an economic burden on patients but also places a significant strain on healthcare systems.11 Traditional therapies primarily focus on symptom control, such as infection management and wound care, but they fail to effectively address the underlying causes of DFU, like diabetic neuropathy and chronic ischemia. In contrast, stem cell therapy has garnered significant attention due to its innovation and potential advantages. Stem cell therapy offers new possibilities for treating DFU through mechanisms that promote angiogenesis, improve nerve damage, and accelerate collagen deposition. For example, mesenchymal stem cells (MSCs) have been shown to differentiate into various cell types, including bone cells, cartilage cells, and fat cells, thereby facilitating wound healing. Additionally, adipose-derived stem cells (ADSCs) show promise in DFU treatment by improving the local microenvironment through the secretion of growth factors and anti-inflammatory agents. Stem cell therapy may serve as an effective supplement or alternative to traditional therapies, providing more efficient, cost-effective, and sustainable treatment options for DFU patients. This review synthesizes recent preclinical and clinical evidence to guide future therapeutic strategies. This article adheres to PRIOR guidelines for narrative reviews.12
 |
Figure 1 Pathogenesis of Diabetic Foot Ulcer (DFU). Schematic representation of the multifactorial mechanisms underlying DFU formation, including peripheral neuropathy, ischemia, oxidative stress, impaired angiogenesis, and chronic inflammation that collectively impair wound healing. |
Research Progress in Stem Cell Therapy
Traditional treatment methods include wound care, infection control, decompression, negative pressure wound therapy, skin substitutes, and skin grafting, but these approaches still have limitations in promoting wound healing and improving prognosis. In recent years, stem cell therapy has gained significant attention as an emerging treatment strategy. MSCs can accelerate the healing of DFUs through various mechanisms, including modulating inflammatory responses, promoting angiogenesis, recruiting immune cells, and secreting growth factors. For example, MSCs can secrete multiple cytokines and growth factors, such as vascular endothelial growth factor (VEGF) and epidermal growth factor (EGF), which promote the formation of new blood vessels and tissue regeneration in ulcerated areas.13 Additionally, MSCs have immunomodulatory effects, capable of suppressing abnormal immune responses and reducing inflammation-induced tissue damage. In terms of stem cell types, adipose-derived stem cells (ADSCs) and bone marrow mesenchymal stem cells (BM-MSCs) are two commonly studied types.14 ADSCs, due to their wide availability, ease of acquisition, and low immunogenicity, have become a research hotspot. Allo-ASC-DFU, developed by Anterogen in South Korea, is a drug based on ADSCs for treating DFUs. Its Phase II clinical trial (NCT02619877; Registration date - 2015-12-02) demonstrated that this therapy is safe and effective in improving wound healing in DFU patients.15 BM-MSCs also demonstrate promising therapeutic potential, as they can secrete various bioactive molecules to modulate the local microenvironment and promote tissue repair.16 Asko Andersen et al evaluated the safety of using BM-MSCs for local treatment in DFU patients. Interestingly, after a single treatment with the BM-MSC preparation, patients showed improved clinical outcomes over a six-month observation period, providing a safe and effective treatment method.17 However, stem cell therapy still faces numerous challenges in clinical application, such as the source of stem cells, standardization of preparation, survival rate, and immunogenicity, which need further optimization. Additionally, how to improve the survival rate and efficacy of stem cells at the ulcer site, and how to better regulate the immunogenicity of stem cells, are also issues that require further research.
Mechanism of Action in Stem Cell Therapy for DFUs
Despite differences in origin, most stem-cell types converge on a set of core regenerative mechanisms. These include (1) angiogenesis through secretion of VEGF, FGF-2, and PDGF activating PI3K/AKT and MAPK pathways; (2) immunomodulation, notably macrophage polarization from M1 to M2 phenotypes mediated by TSG-6, IL-10, and exosomal miRNAs; (3) antioxidant and anti-apoptotic protection via SOD, GPx, and Nrf2/HO-1 signaling; and (4) ECM remodeling that enhances fibroblast proliferation and keratinocyte migration. Subsequent sections highlight distinctive features of each stem-cell source while referencing these shared pathways to avoid redundancy.
Anti-Inflammatory and Immune Regulation
Stem cell therapy reshapes the microenvironment of DFU wounds through multi-mechanism coordinated regulation, demonstrating significant advantages that surpass traditional treatment limitations (see Figure 2). DFU wounds are often in a chronic inflammatory state, where inflammatory responses are one of the key factors leading to delayed wound healing. MSCs secrete various cytokines and chemokines, such as IL-10 and TGF-β, which can significantly reduce the levels of pro-inflammatory cytokines like TNF-α and IL-6, thereby suppressing inflammatory responses.18 MSCs can reduce the infiltration of inflammatory cells and the release of inflammatory mediators by upregulating the expression of IL-10, thus promoting wound healing. In the inflammatory environment of DFU, the proportion of M1 macrophages (pro-inflammatory) is higher, while the proportion of M2 macrophages (anti-inflammatory) is lower.19 MSCs can promote the polarization of M1 to M2 by secreting specific cytokines and exosomes, increasing the number of M2 macrophages, thereby reducing inflammatory responses and promoting tissue repair. NF-κB is a key transcription factor regulating inflammatory responses. By inhibiting the activation of the NF-κB signaling pathway, MSCs reduce the expression of pro-inflammatory cytokines, thereby exerting an anti-inflammatory effect. Li et al found that miRNAs such as20 and miR-21-231 can target the NF-κB signaling pathway in MSCs, further suppressing inflammatory responses. In addition to these mechanisms, MSCs also exert anti-inflammatory effects through other pathways. HO-1 (heme oxygenase-1) is an important antioxidant and anti-inflammatory enzyme that can reduce oxidative stress and inflammatory response. Overexpression of HO-1 in DFU can enhance the anti-inflammatory ability of MSCs, thus promoting wound healing.21
 |
Figure 2 Factors Stimulating Endothelial Cell Proliferation and Migration. Illustration showing molecular and cellular factors such as VEGF, FGF, PDGF, TGF-β, nitric oxide, and hypoxia-inducible pathways that promote angiogenesis and tissue regeneration during diabetic wound healing. |
MSCs possess immunosuppressive properties and can modulate immune responses through various mechanisms, reducing immune rejection and creating a favorable immune microenvironment for wound healing. MSCs inhibit the proliferation and activation of T cells and B cells by secreting immune regulatory factors such as IDO. This immunosuppressive effect reduces immune cell infiltration and alleviates inflammatory responses. In a study by Husakova et al, MSCs were applied to a diabetic mouse model of foot ulcers, systematically evaluating the immunomodulatory effects of MSCs.22 The results showed that MSCs significantly inhibited T cell activation and proliferation by secreting indoleamine 2,3-dioxygenase (IDO). IDO degrades tryptophan to produce immunosuppressive metabolites, thereby inhibiting T cell activation. Compared to the control group, the treatment group treated with MSCs exhibited significantly reduced T cell infiltration, lessened inflammatory responses, and accelerated wound healing. This study provides important evidence for the role of MSCs in promoting DFU healing through immunomodulatory effects and highlights the critical role of IDO-mediated immunosuppressive mechanisms. MSCs can also promote the transformation of macrophages from the pro-inflammatory M1 type to the anti-inflammatory M2 type. M2 macrophages can secrete anti-inflammatory factors, further suppressing inflammatory responses and promoting tissue repair.23 MSCs significantly promoted macrophage polarization to M2 type through the TSG-6-mediated mechanism,24 thereby improving the healing process of DFU.
Promotion of Angiogenesis
A key pathological feature of DFU is poor local blood circulation, leading to tissue hypoxia and inadequate nutrient supply. Stem cells can secrete various angiogenic factors, such as VEGF, FGF, and PDGF. These factors directly stimulate the proliferation and migration of endothelial cells, thereby promoting the formation of new blood vessels (see Figure 2). MSCs can improve angiogenesis in DFU areas by secreting factors like VEGF.19 Additionally, ADSCs can also promote vascular neogenesis by secreting factors such as VEGF and FGF-2. These factors not only promote the proliferation and migration of endothelial cells but also enhance their survival capabilities, thus accelerating the angiogenesis process. Furthermore, stem cells promote angiogenesis through exosomes. Exosomes are small vesicles secreted by stem cells, containing multiple proteins, mRNA, and miRNA molecules that can function in target cells to regulate their biological functions. MSC-derived exosomes (MSC-Exos) can promote the proliferation and migration of endothelial cells through molecules such as miR-125a, thereby promoting angiogenesis.25 Specifically, the expression of miR-125a in exosomes can inhibit endothelial cell apoptosis and promote their proliferation and migration.26 Moreover, miR-106a-5p promotes angiogenesis through the FGF4/p38MAPK signaling pathway, a mechanism with potential application value in DFU treatment.25 Stem cells promote angiogenesis by activating specific signaling pathways. MSCs can enhance the proliferation and migration of endothelial cells27 by activating the PI3K/AKT signaling pathway. Stem cells not only promote angiogenesis through the secretion of factors and exosomes but also play a role through direct contact with endothelial cells. For example, ADSCs can form tight junctions with endothelial cells and promote their proliferation and migration by secreting various signaling molecules.28 This intercellular interaction not only enhances the effectiveness of angiogenesis but also improves the specificity and efficacy of treatment.
Inhibition of Oxidative Stress and Apoptosis
Stem cell therapy in DFU has shown significant efficacy, one of its mechanisms being to promote tissue repair and regeneration by inhibiting oxidative stress and apoptosis. Oxidative stress and apoptosis are key factors in the pathogenesis of DFU, and stem cell therapy intervenes in these processes through multiple pathways, thereby improving the healing of DFU. Oxidative stress refers to the process where excessive reactive oxygen species (ROS) damage cells when the balance between oxidation and antioxidation is disrupted. In DFU, oxidative stress not only leads to cellular dysfunction but also exacerbates inflammatory responses and tissue damage. Stem cells can secrete various antioxidant enzymes, such as superoxide dismutase (SOD) and glutathione peroxidase (GPx), which can clear ROS from the body and reduce oxidative stress-induced cell damage.29 Kaempferol reduces ROS levels by downregulating the ROS/FoxO signaling pathway, thus protecting BM-MSCs from oxidative stress-induced apoptosis.30 Additionally, Nrf2 is activated under oxidative stress conditions and enhances cellular antioxidant capacity by upregulating the expression of antioxidant genes such as HO-1 and GSH. Research indicates that overexpression of Nrf2 can significantly reduce the apoptosis rate of BM-MSCs and improve their antioxidant capacity.31
Apoptosis is an indispensable factor in the healing process of DFU. Oxidative stress-induced apoptosis primarily occurs through the activation of pro-apoptotic proteins such as caspase-3 and Bax, while simultaneously reducing the expression of anti-apoptotic protein Bcl-2.32 Additionally, oxidative stress can further exacerbate cellular damage by activating the autophagy pathway. Stem cell therapy inhibits apoptosis through multiple pathways. miR-210 plays a crucial role in H2O2-induced apoptosis in endothelial and cardiomyocytes. miR-210 can inhibit H2O2-induced apoptosis in H9c2 cells, with mechanisms possibly involving regulation of the cell cycle, DNA repair, and cell proliferation.33 Furthermore, N-acetylcysteine (NAC) can protect BM-MSCs from oxidative stress-induced apoptosis by activating the PI3K-Akt signaling pathway, upregulating the expression of FOXO3, FOXO4, and FOXO6 genes, as well as anti-apoptotic Bcl-2.34
Promotion of Tissue Regeneration
MSCs possess the ability to differentiate in multiple directions and can directly participate in wound tissue repair. Additionally, the growth factors and cytokines secreted by MSCs can promote the proliferation and differentiation of endogenous cells, accelerating wound healing. The repair of DFU wounds requires a large number of fibroblasts to synthesize collagen and rebuild the extracellular matrix. In their study published in,35 Assi et al injected MSCs into diabetic rat foot ulcer models to investigate the role of MSCs in promoting tissue regeneration. The results showed that MSCs can differentiate into fibroblasts and secrete collagen and other extracellular matrix components. MSCs promote fibroblast differentiation and function by activating the TGF-β/Smad signaling pathway.36 Compared to the control group, the wound granulation tissue formation in the MSC treatment group was significantly better, with increased collagen deposition and faster wound healing, and this study not only confirmed that MSCs directly participate in wound repair by differentiating into fibroblasts but also provided new insights into the regulatory mechanisms of the TGF-β/Smad signaling pathway in tissue regeneration. MSCs can secrete various growth factors, such as EGF, FGF, and TGF-β, which promote the proliferation and differentiation of endogenous cells. These growth factors can accelerate wound healing and reduce healing time. Ziegler’s research found that MSCs significantly promoted the epithelialization and collagen deposition in DFU wounds through the secretion of EGF and FGF.36
Stem-Cell–Derived Exosomes in Diabetic Foot Ulcer Therapy
Stem-cell–derived exosomes have recently emerged as a powerful cell-free regenerative strategy for diabetic foot ulcers (DFUs), offering many of the reparative advantages of mesenchymal stem cells (MSCs) while avoiding risks such as immune rejection, tumorigenicity, and poor engraftment.37 These nanosized extracellular vesicles (30–150 nm) carry diverse cargos including proteins, lipids, mRNAs, and regulatory microRNAs that mediate intercellular communication and reproduce the paracrine actions of their parent cells.38–40 Two recent comprehensive reviews Wang H et al,41 and Wang J et al42 have summarized the latest advances in this field, emphasizing that exosomes derived from bone-marrow, adipose, and umbilical-cord MSCs exert coordinated effects on inflammation, angiogenesis, oxidative stress, and tissue remodeling in DFU models.
These studies41,42 demonstrate that MSC-derived exosomes (MSC-Exos) deliver miRNAs such as miR-125a, miR-132, miR-146a, and miR-106a-5p, which activate the FGF4/p38MAPK, PI3K/AKT, and TGF-β/Smad pathways to stimulate endothelial cell proliferation, migration, and neovascularization within ischemic wound beds. They also modulate macrophage polarization from the pro-inflammatory M1 to the reparative M2 phenotype and suppress activation of the NLRP3 inflammasome, thereby reducing cytokine overexpression (IL-6, TNF-α, IL-1β) and promoting resolution of inflammation. Exosomes isolated from adipose-derived MSCs and hair-follicle MSCs further accelerate re-epithelialization and collagen deposition by transferring lncRNA H19 and antioxidant enzymes that mitigate reactive-oxygen-species accumulation. In both rodent and large-animal DFU models, exosome treatment enhanced granulation tissue formation, increased capillary density and VEGF/CD31 expression, and shortened wound-closure time compared with untreated controls.41,42
To address the short in-vivo half-life and rapid clearance of free vesicles, recent experimental approaches have embedded exosomes in hydrogels, extracellular-matrix scaffolds, and nanofiber composites, achieving sustained local release and superior healing efficacy.43,44 These reports41,42 also stress the need for standardization of exosome isolation and quality control, optimization of dosage and delivery routes, and large-scale, GMP-compliant production systems to enable clinical translation. The accumulating evidence positions MSC-derived exosomes as a next-generation therapeutic platform for DFU harnessing the regenerative and immunomodulatory capacity of stem cells in a safer, more controllable, and clinically adaptable form.45
Types and Sources of Stem Cells
Combined Bone Marrow-Derived Multipotent Mesenchymal Stem Cells (BM-MSCs)
Stem cell therapy has shown significant potential in the treatment of DFU, and different types of stem cells have shown their own advantages and limitations in the treatment of DFU (see Table 1). Comparatively, the stem-cell types used for DFU, ADSCs offer the easiest harvest and highest yield, making them ideal for autologous applications with strong paracrine and angiogenic effects. BM-MSCs remain the most extensively studied, showing reliable safety and vascular regeneration but require invasive collection and are limited by donor-age variability. UCB-MSCs provide an allogeneic, “off-the-shelf” option with low immunogenicity and consistent potency, though availability and scalability can be constrained. iPSC-derived cells hold the greatest potential for personalized therapy and unlimited expansion, yet long-term genomic stability and cost remain major challenges. Thus, the choice of cell source should balance accessibility, safety, immunologic profile, and translational feasibility rather than assuming one universally superior type.
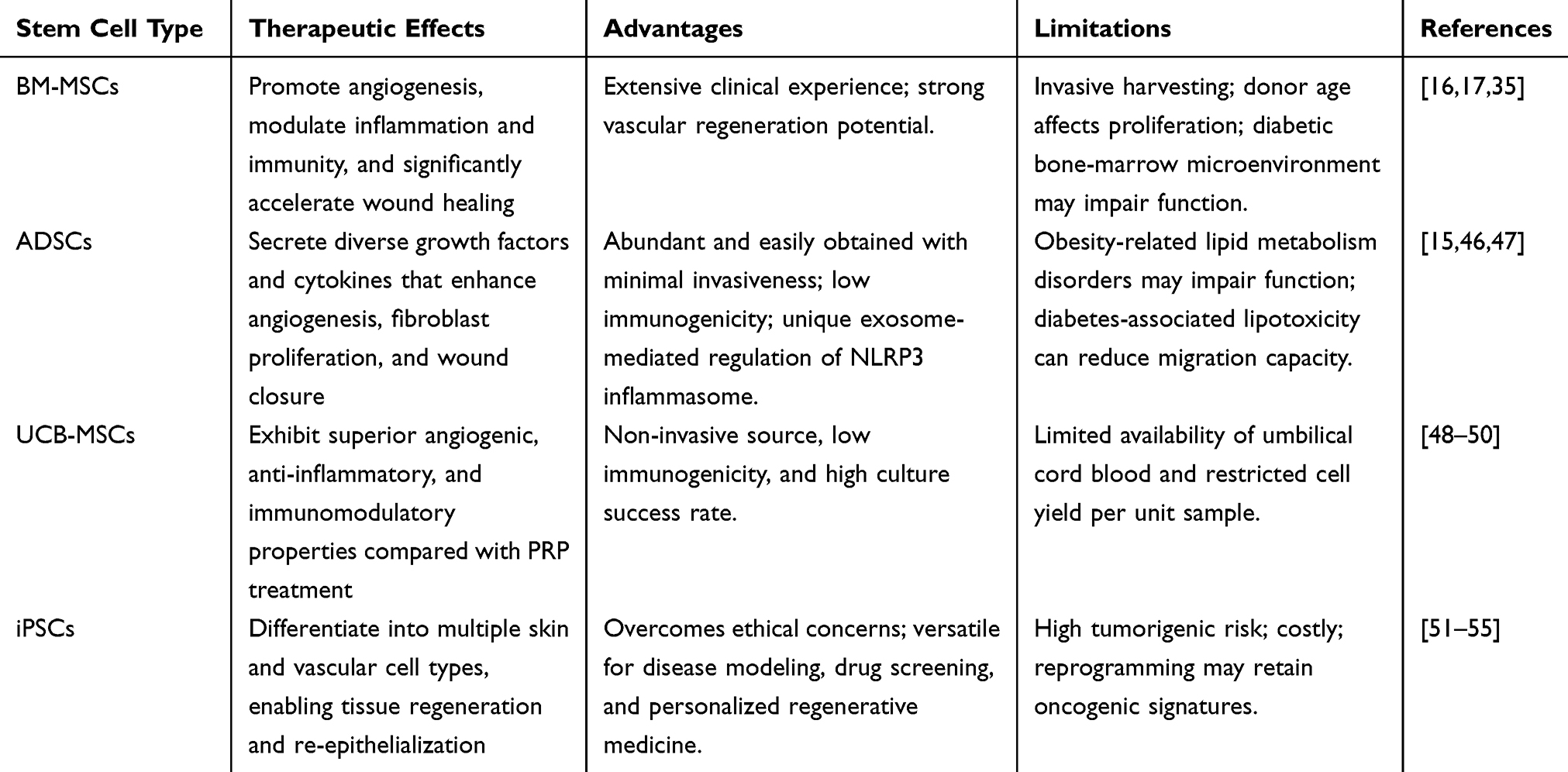 |
Table 1 Comparative Overview of Stem Cell Types Used in Diabetic Foot Ulcer (DFU) Therapy: Efficacy, Advantages, and Limitations |
BM-MSCs are a type of adult stem cell with the potential for self-renewal and multi-directional differentiation, primarily derived from bone marrow. They can differentiate into various cell types such as osteoblasts, chondrocytes, and adipocytes, playing a crucial role in tissue repair and immune regulation. BM-MSCs have significant potential in the treatment of DFU, exerting their effects through mechanisms like wound healing promotion, anti-inflammatory action, and autophagy (see Figure 3). Conditioned medium (MSC-CM) secreted by BM-MSCs can significantly improve the wound healing process in rat models of DFU, reducing the level of inflammatory factor IL-1β, increasing the expression of cell proliferation index Ki67, angiogenesis index CD31, and GSDMD, while also decreasing apoptosis.56 Research has shown that transplantation of BM-MSCs can significantly enhance the speed and quality of wound healing in patients with DFU, reduce amputation rates, and lower complication rates.4 However, invasive procedures for bone marrow collection may increase patient risks, and donor age significantly affects cell proliferation capacity. Additionally, in autologous transplantation, abnormal bone marrow microenvironment in diabetic patients may weaken cell function, requiring strategies such as gene editing to optimize.
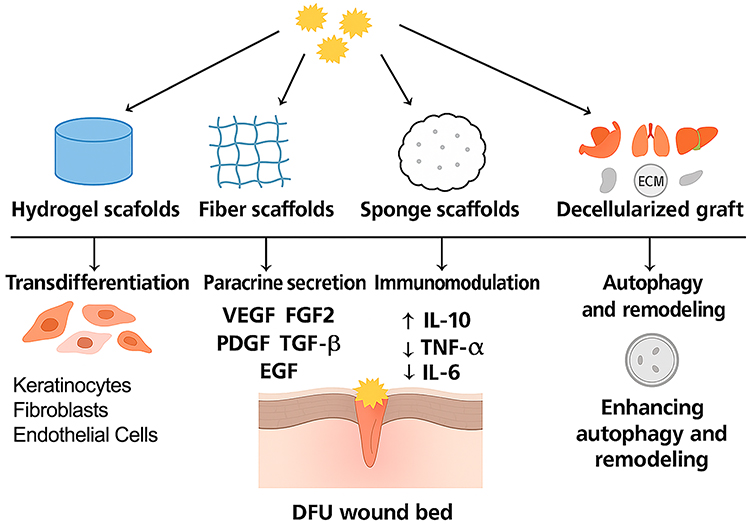 |
Figure 3 Scaffold-assisted mechanisms of BM-MSC–mediated healing in diabetic foot ulcers (DFUs). BM-MSCs can be incorporated into various biocompatible scaffolds such as hydrogels, fiber scaffolds, sponge scaffolds, and decellularized grafts to enhance their regenerative potential in DFU repair. Once delivered to the wound microenvironment, BM-MSCs promote healing through multiple coordinated mechanisms: (i) transdifferentiation into keratinocytes, fibroblasts, and endothelial cells that restore epidermal and vascular integrity; (ii) paracrine secretion of growth factors (VEGF, FGF2, PDGF, TGF-β, EGF) that stimulate angiogenesis and fibroblast proliferation; (iii) immunomodulation via upregulation of IL-10 and downregulation of TNF-α and IL-6 to resolve inflammation; and (iv) autophagy and extracellular-matrix remodeling, collectively accelerating re-epithelialization and wound closure. |
Adipose-Derived Mesenchymal Stem Cells (ADSCs)
ADSCs are MSCs extracted from adipose tissue and possess the potential for self-renewal and multi-directional differentiation. They can differentiate into various cell types, such as adipocytes, chondrocytes, and osteoblasts, and have immune regulatory functions that can control excessive immune responses. The acquisition of ADSCs is simple, involving local liposuction under local anesthesia, and they are easy to expand in vitro. ADSCs promote angiogenesis and cell proliferation by secreting multiple growth factors and cytokines, thereby accelerating the healing of DFU. Embedding ADSCs in platelet-rich plasma (PRF) for DFU treatment significantly improves patient healing rates.46 Research has found that ADSCs can reduce inflammatory responses in DFU patients by inhibiting the expression of inflammatory factors, and AD-MSC exosomes enhance skin healing in diabetic mice by regulating the expression of NLRP3-related proteins.47 By promoting wound healing, reducing inflammation, and improving tissue regeneration, ADSCs offer new treatment options for DFU patients. However, abnormal lipid metabolism in obese patients may affect cell function, and diabetes-related lipotoxicity can reduce the migratory ability of ADSCs. In terms of long-term safety, their angiogenic properties raise concerns about the risk of complications such as diabetic retinopathy.
Umbilical Cord Blood Mesenchymal Stem Cells (UCB-MSCs)
UCB-MSCs are MSCs isolated from umbilical cord blood, characterized by high self-renewal capacity and multi-directional differentiation potential, capable of differentiating into multiple lineages such as adipocytes, osteoblasts, and chondrocytes.48 Additionally, UCB-MSCs exhibit strong immune regulatory functions, inhibiting the proliferation of T cells and B cells, and reducing inflammatory responses.49 These properties make UCB-MSCs highly valuable in regenerative medicine and tissue repair. UCB-MSCs participate in the treatment of DFU through mechanisms such as promoting angiogenesis, anti-inflammatory effects, and immune regulation. UCB-MSCs can promote wound healing and reduce infection risks.50 However, clinical applications are limited by the scarcity of umbilical cord blood resources; a single unit of umbilical cord blood can only yield about 2×10^5 MSCs, which need to be expanded to the 3rd-5th generation in vitro to meet therapeutic needs. Moreover, cell viability loss during cryopreservation and thawing may affect the stability of therapeutic effects.
Induced Pluripotent Stem Cells (iPSCs)
iPSCs can be generated through various types of somatic cells such as fibroblasts, peripheral blood mononuclear cells, and urine cells.51 These cells are reprogrammed using specific transcription factors (such as OCT4, SOX2, LIN28, and KLF4) into pluripotent iPSCs.52 Optimized methods during the reprogramming process, such as the use of small molecule inhibitors, further enhance the efficiency and quality of iPSCs generation. iPSCs can differentiate into multiple cell types, including keratinocytes, fibroblasts, and endothelial cells, which are used to repair damaged skin and blood vessels. Keratinocytes derived from iPSCs can effectively promote regeneration in the skin. iPSCs can be obtained from patient-derived skin fibroblasts or blood cells and converted into pluripotent stem cells through reprogramming technology.53 These cells have the ability to differentiate into various cell types, including neurons, immune cells, endothelial cells, and smooth muscle cells. Research indicates that fibroblasts from DFU patients can be successfully converted into iPSCs, which can then differentiate into smooth muscle cells for simulating pathological processes in DFU, such as wound healing, angiogenesis, and cell proliferation.54 iPSCs can be combined with biomaterials to construct tissue engineering scaffolds for repairing damaged skin and tissues. Cells derived from iPSCs can also be combined with biomaterials like collagen to form bioactive tissue engineering scaffolds.55 However, iPSCs technology still faces some challenges in clinical application, such as the reprogramming process may leave residual oncogenic genes, differentiation efficiency varies by batch, GMP production cycle is up to 4–6 months, and treatment costs are 5–8 times that of other stem cell therapies. The characteristics and therapeutic applications of the major stem cell types used for DFU treatment are summarized in Figure 4.
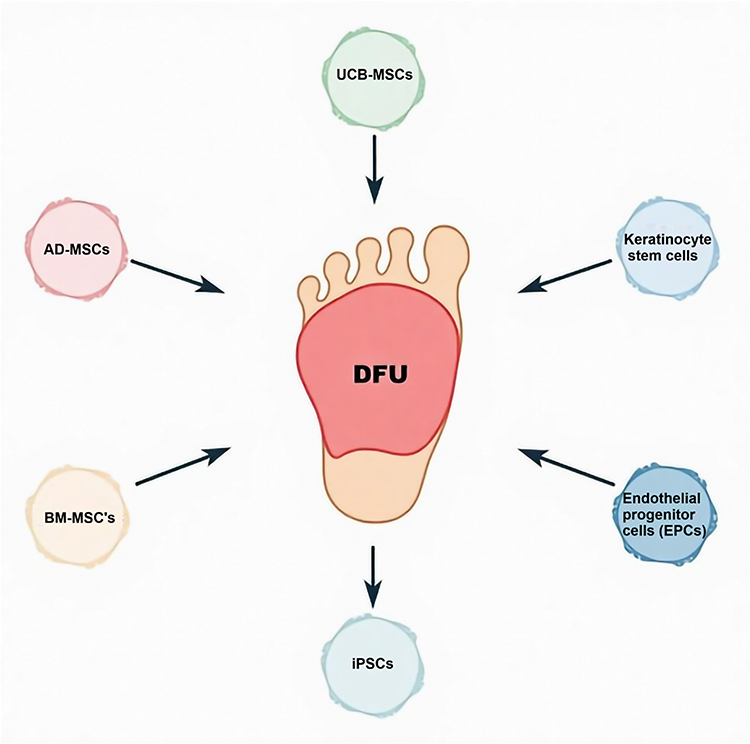 |
Figure 4 Overview of Cell-Based Therapeutic Strategies for Diabetic Foot Ulcers. Summary diagram highlighting diverse stem-cell-based interventions BM-MSCs, ADSCs, UCB-MSCs, iPSCs, and stem-cell-derived exosomes and their modes of action such as angiogenesis promotion, inflammation reduction, and ECM remodeling, integrated with emerging adjuncts like biomaterials and nanotechnology. |
Combined Application of Stem Cells and Other Treatments
DFU is a complex chronic wound that requires multidisciplinary collaboration and comprehensive treatment strategies. In recent years, stem cell therapy has shown significant potential in the treatment of DFU, particularly stem cells derived from sources such as MSCs and iPSCs. These cells improve the healing of DFU through various mechanisms, including promoting angiogenesis, inhibiting inflammatory responses, differentiating into vascular endothelial and osteoblast cells, and secreting growth factors.57 However, despite the promising results of stem cell therapy in treating DFU, its use alone still has some limitations. Researchers have recently explored combined treatment strategies to enhance therapeutic outcomes. Biomaterials can be integrated with stem cells to improve the effectiveness of DFU treatment. Combination of autologous BM-MSCs and dermal fibroblasts with chitosan-based biomaterials significantly reduced patient pain and observed a noticeable reduction in ulcer area within 48 hours after treatment and after eight months of treatment, the ulcers were almost completely healed, and vascular CT results indicated good vascular healing. Photo-biomodulation therapy, which stimulates cell activity through light exposure, can further enhance the therapeutic effects of stem cells. Moreover, P-MSCs hydrogels have also demonstrated excellent therapeutic outcomes, successfully preventing amputations in DFU patients.58 Combining photo-biomodulation with ADSCs can significantly enhance the treatment outcomes of DFU, indicating that the combined use of stem cells and growth factors can further improve efficacy under specific conditions.59 The integration of physical therapy with stem cell therapy has been proven to promote the migration and proliferation of stem cells, thereby improving the healing of DFU. LLLT is a non-invasive treatment method that stimulates cell proliferation, migration, and differentiation through photo-biomodulation. A review describes how low-level laser therapy (LLLT), as a physical therapy, can promote cell proliferation and angiogenesis, and when combined with stem cell therapy, may further enhance the treatment outcomes of DFU.60 Nanomaterials possess unique physical and chemical properties that can enhance the biological functions of stem cells. Research indicates that stem cells encapsulated in nanoparticles can more effectively deliver growth factors and antioxidants to damaged tissues,61 offering new strategies for the treatment of DFU.
Recent work by Rajendran et al,62 Wei et al63 and Gong et al64 further integrates mesenchymal stem-cell–derived exosomes with nanoengineered and responsive scaffolds, enabling sustained release and microenvironment modulation that improves angiogenesis, re-epithelialization, and infection control in chronic DFU where they demonstrated that exosome-loaded hydrogels and dynamic matrix composites accelerate wound closure and vascular remodeling compared with conventional carriers.
However, the long-term toxicity and biocompatibility of nanomaterials still require further investigation.
Challenges and Limitations of Stem Cell Therapy
Despite the significant potential of stem cell therapy in treating diabetic foot ulcers (DFU), its clinical application still faces a series of challenges and limitations, primarily concerning safety, therapeutic consistency, production costs, and ethical issues. A thorough analysis of these limitations and the proposal of optimization strategies are crucial for advancing stem cell therapy from laboratory research to clinical practice. The infinite proliferative capacity of stem cells is at the core of their therapeutic potential but also poses a risk of tumorigenesis. In particular, iPSCs and ESCs may retain oncogenes during reprogramming or differentiation, leading to uncontrolled cell proliferation after transplantation. iPSCs can form teratomas under certain conditions, especially when not fully differentiated into target cell types. To address this issue, researchers are optimizing reprogramming techniques to reduce the residual oncogenes and using gene editing technologies (such as CRISPR-Cas9) to screen and modify stem cells, ensuring their safety and controllability.65 Transplanted stem cells may be recognized by the host immune system as foreign substances, triggering an immune rejection response and leading to transplant failure. This problem is particularly pronounced in allogeneic stem cell transplants. Although autologous stem cells (such as iPSCs) theoretically avoid immune rejection, their preparation is complex and costly. To reduce the risk of immune rejection, researchers are exploring combined immunomodulatory strategies, such as using engineered stem cells that secrete immunosuppressive factors (like IDO) or combining them with immunosuppressive drugs. In complex microenvironments such as diabetic foot ulcers, transplanted stem cells may have low survival rates due to hypoxia, inflammation, and metabolic disorders. High glucose and low oxygen environment of DFU wounds significantly inhibits the activity and survival of stem cells.66 To improve cell survival rates, researchers are developing smart-responsive biomaterials (such as hypoxia-responsive hydrogels) to provide a suitable microenvironment for stem cells and enhancing their adaptability through pre-treatment techniques (such as hypoxic preconditioning). The process of stem cell differentiation into specific cell types is difficult to control precisely, which can lead to the generation of non-target cells and affect treatment outcomes. For example, iPSCs may produce non-functional cells when differentiating into endothelial or fibroblastic cells due to improper signaling pathway regulation. To address this issue, researchers are using single-cell RNA sequencing technology to accurately analyze stem cell differentiation pathways and developing engineered exosomes to guide stem cell differentiation by delivering specific signaling molecules.67 The production of stem cells requires strict quality control and standardized procedures, and is costly, limiting its widespread application. For instance, the preparation of iPSCs involves complex reprogramming techniques and long-term in vitro culture, resulting in a production cycle that can last several months and significantly higher costs compared to traditional therapies. To reduce production costs, researchers are promoting the development of scaled-up production technologies and exploring non-integrated reprogramming techniques to simplify the preparation process. The translation of stem cell therapy from laboratory to clinical application faces numerous challenges, including ensuring the safety, efficacy, and reproducibility of treatments. Despite encouraging progress, several translational barriers remain. Patient heterogeneity including differences in age, diabetic control, comorbid vascular disease, and local wound microbiome can profoundly influence stem-cell viability, engraftment, and paracrine activity, complicating standardization of outcomes across trials.68 Moreover, long-term safety requires continued surveillance, since genomic instability, unintended differentiation, or pro-angiogenic overactivity could potentially lead to fibrosis or neoplasia after transplantation.68,69 Current follow-ups in most DFU studies rarely extend beyond 12 months, leaving long-term durability and recurrence rates uncertain.69,70 Addressing these gaps will require multicenter trials with stratified enrollment, harmonized outcome measures, and extended post-treatment monitoring to ensure durable and safe clinical benefit.
Stem cell therapy shows great potential in the treatment of diabetic foot ulcers, but its clinical application still requires overcoming a series of challenges. Through technological innovation, optimizing production processes, strengthening ethical oversight, and long-term safety research, it is hoped that stem cell therapy can make the leap from experimental studies to clinical applications, providing new solutions for the treatment of diabetic foot ulcers.
Conclusion
Stem-cell-based strategies offer a promising therapeutic option for chronic diabetic foot ulcers through convergent mechanisms including pro-angiogenic signaling, immunomodulation via M2 macrophage polarization, reduction of oxidative stress, and support of extracellular matrix remodeling. However, clinical translation still depends on achieving standardization, safety, and durability of benefit. The choice of cell source should be contextual rather than fixed: ADSCs provide the most accessible autologous option with high yield; BM-MSCs have the strongest clinical record and safety profile; UCB-MSCs allow low-immunogenic, off-the-shelf use; and iPSC-derived products offer customization but require careful genomic stability monitoring. Future research should focus on optimizing protocols that define source, dose, and delivery route; integrating stem cells with biomaterials and nanoplatforms to improve cell retention and paracrine activity; and expanding cell-free therapies such as exosome- and secretome-based products to enhance scalability and safety. Large multicenter studies with extended follow-up are essential to validate long-term outcomes, confirm safety, and establish cost-effectiveness so that stem-cell-derived therapies can be integrated safely and consistently into clinical practice for diabetic wound care.
Data Sharing Statement
Data sharing is not applicable as no datasets were generated or analyzed in this review.
Acknowledgments
The authors thank colleagues for their insights during manuscript preparation.
Author Contributions
Bin Wang (B.W.): Conceptualization, Writing – Original Draft, Visualization, Project Administration. Gang Zhao (G.Z.): Supervision, Writing – Review & Editing, Resources. Jiaqi Zhang (J.Z.): Writing – Review & Editing, Methodology, Formal Analysis, Data Curation. Wenyu Chen (W.C.): Writing – Review & Editing, Investigation, Validation. Shanshan Yang (S.Y.): Writing – Review & Editing, Validation, Visualization. Yinuo Sun (Y.S.): Writing – Review & Editing, Visualization, Software. All authors have read and approved the final version of this paper, agreed on the journal to which the article has been submitted, and agree to take full responsibility for the integrity and accuracy of the work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that there is no conflicts of interest.
References
1. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diab Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
2. Zhang Y, Liu H, Yang Y, et al. Incidence and risk factors for amputation in Chinese patients with diabetic foot ulcers: a systematic review and meta-analysis. Front Endocrinol. 2024;15:1405301. doi:10.3389/fendo.2024.1405301
3. Barshes NR, Sigireddi M, Wrobel JS, et al. The system of care for the diabetic foot: objectives, outcomes, and opportunities. Diabetic Foot Ankle. 2013;4(1):21847. doi:10.3402/dfa.v4i0.21847
4. Rai V, Moellmer R, Agrawal DK. Stem cells and angiogenesis: implications and limitations in enhancing chronic diabetic foot ulcer healing. Cells. 2022;11(15):2287. doi:10.3390/cells11152287
5. Ahmad J. The diabetic foot. Diabetes & metabolic syndrome. Clin Res Rev. 2016;10(1):48–60.
6. Xu Y, Xu J, Chen S, et al. Identifying potential pathogenesis and immune infiltration in diabetic foot ulcers using bioinformatics and in vitro analyses. BMC Med Genomic. 2023;16(1):313. doi:10.1186/s12920-023-01741-2
7. Shi H, Zhang Z, Yuan X, et al. PROS1 is a crucial gene in the macrophage efferocytosis of diabetic foot ulcers: a concerted analytical approach through the prisms of computer analysis. Aging. 2024;16(8):
8. Khan MS, Jahan N, Khatoon R, et al. The diabetic foot ulcer: biofilm, antimicrobial resistance, and amputa tion. Int J Diab Develop Countri. 2025;45(3):568–579. doi:10.1007/s13410-024-01423-4
9. Jones AD, De Siqueira J, Nixon JE, et al. Plantar shear stress in the diabetic foot: a systematic review and meta‐analysis. Diabetic Medicine. 2022;39(1):e14661. doi:10.1111/dme.14661
10. Basit A, Basit KA, Fawwad A, et al. Vitamin D for the treatment of painful diabetic neuropathy. BMJ Open Diabetes Res Care. 2016;4(1):e000148. doi:10.1136/bmjdrc-2015-000148
11. Xia Y, Wu P, Chen H, et al. Advances in stem cell therapy for diabetic foot. Front Genetic. 2024;15:1427205. doi:10.3389/fgene.2024.1427205
12. Gates M, Gates A, Pieper D, et al. Reporting guideline for overviews of reviews of healthcare interventions: development of the PRIOR statement. BMJ. 2022;2022:378.
13. Wan X, Ni X, Xie Y, et al. Research progress and application prospect of adipose-derived stem cell secretome in diabetes foot ulcers healing. Stem Cell Res Ther. 2024;15(1):279. doi:10.1186/s13287-024-03912-z
14. Yu X, Liu P, Li Z, et al. Function and mechanism of mesenchymal stem cells in the healing of diabetic foot wounds. Front Endocrinol. 2023;14:1099310. doi:10.3389/fendo.2023.1099310
15. Liu W-S, Liu Y, Gao J, et al. Biomembrane-based nanostructure-and microstructure-loaded hydrogels for promoting chronic wound healing. Int J Nanomed. 2023;18:385–411. doi:10.2147/IJN.S387382
16. Wu S, Zhou Z, Li Y, et al. Advancements in diabetic foot ulcer research: focus on mesenchymal stem cells and their exosomes. Heliyon. 2024;10(17).
17. Mahmoudvand G, Karimi Rouzbahani A, Razavi ZS, et al. Mesenchymal stem cell therapy for non-healing diabetic foot ulcer infection: new insight. Front Bioengineer Biotechnol. 2023;11:1158484. doi:10.3389/fbioe.2023.1158484
18. Li T, Ma Y, Wang M, et al. Platelet-rich plasma plays an antibacterial, anti-inflammatory and cell proliferation-promoting role in an in vitro model for diabetic infected wounds. Infect Drug Resistanc. 2019;Volume 12:297–309. doi:10.2147/IDR.S186651
19. Leal EC, Carvalho E. Heme oxygenase-1 as therapeutic target for diabetic foot ulcers. Int J Mol Sci. 2022;23(19):
20. Liang Z-H, Pan N-F, Lin -S-S, et al. Exosomes from mmu_circ_0001052-modified adipose-derived stem cells promote angiogenesis of DFU via miR-106a-5p and FGF4/p38MAPK pathway. Stem Cell Res Ther. 2022;13(1):336. doi:10.1186/s13287-022-03015-7
21. Xiong Y, Song J, Huang X, et al. Exosomes derived from mesenchymal stem cells: novel effects in the treatment of ischemic stroke. Front Neurosci. 2022;16:899887. doi:10.3389/fnins.2022.899887
22. Chen LY, Kao T-W, Chen -C-C, et al. Frontier review of the molecular mechanisms and current approaches of stem cell-derived exosomes. Cells. 2023;12(7):1018. doi:10.3390/cells12071018
23. Lo Sicco C, Reverberi D, Balbi C, et al. Mesenchymal stem cell-derived extracellular vesicles as mediators of anti-inflammatory effects: endorsement of macrophage polarization. Stem Cells Translational Med. 2017;6(3):1018–1028. doi:10.1002/sctm.16-0363
24. Rautiainen S, Laaksonen T, Koivuniemi R. Angiogenic effects and crosstalk of adipose-derived mesenchymal stem/stromal cells and their extracellular vesicles with endothelial cells. Int J Mol Sci. 2021;22(19):10890. doi:10.3390/ijms221910890
25. Molagoda IMN, Lee KT, Choi YH, et al. Anthocyanins from hibiscus syriacus L. inhibit oxidative stress-mediated apoptosis by activating the Nrf2/HO-1 signaling pathway. Antioxidants. 2020;9(1):42. doi:10.3390/antiox9010042
26. Sharma N, Biswas S, Al-Dayan N, et al. Antioxidant role of kaempferol in prevention of hepatocellular carcinoma. Antioxidants. 2021;10(9):1419. doi:10.3390/antiox10091419
27. Zhang F, Yan Y, Peng W, et al. PARK7 promotes repair in early steroid-induced osteonecrosis of the femoral head by enhancing resistance to stress-induced apoptosis in bone marrow mesenchymal stem cells via regulation of the Nrf2 signaling pathway. Cell Death Dis. 2021;12(10):940. doi:10.1038/s41419-021-04226-1
28. Gharibi B, Farzadi S, Ghuman M, et al. Inhibition of Akt/mTOR attenuates age-related changes in mesenchymal stem cells. Stem Cells. 2014;32(8):2256–2266. doi:10.1002/stem.1709
29. Diao H, Liu B, Shi Y, et al. MicroRNA-210 alleviates oxidative stress-associated cardiomyocyte apoptosis by regulating BNIP3. Biosci Biotechnol Biochem. 2017;81(9):1712–1720. doi:10.1080/09168451.2017.1343118
30. Ma Z, Song G, Liu D, et al. N-Acetylcysteine enhances the therapeutic efficacy of bone marrow-derived mesenchymal stem cell transplantation in rats with severe acute pancreatitis. Pancreatology. 2019;19(2):258–265. doi:10.1016/j.pan.2019.01.004
31. Assi R, Foster TR, He H, et al. Delivery of mesenchymal stem cells in biomimetic engineered scaffolds promotes healing of diabetic ulcers. Regen Med. 2016;11(3):245–260. doi:10.2217/rme-2015-0045
32. Ziegler T, Cakl T, Schauer J, et al. Treatment of second to third-degree burns in a 2-day-old infant: a case report. Int J Surg Case Rep. 2019;61:195–198. doi:10.1016/j.ijscr.2019.07.035
33. Husakova J, Echalar B, Kossl J, et al. The effects of immunosuppressive drugs on the characteristics and functional properties of bone marrow-derived stem cells isolated from patients with diabetes mellitus and peripheral arterial disease. Biomedicines. 2023;11(7):1872. doi:10.3390/biomedicines11071872
34. Di G, Du X, Qi X, et al. Mesenchymal stem cells promote diabetic corneal epithelial wound healing through TSG-6-dependent stem cell activation and macrophage switch. Invest Ophthalmol Vis Sci. 2017;58(10):4344–4354. doi:10.1167/iovs.17-21506
35. Xu YF, Wu Y-X, Wang H-M, et al. Bone marrow-derived mesenchymal stem cell-conditioned medium ameliorates diabetic foot ulcers in rats. Clinics. 2023;78:100181. doi:10.1016/j.clinsp.2023.100181
36. Khalil C, Chaker D, Salameh R, et al. Autologous adipose-derived mesenchymal stem cells embedded in platelet -rich fibrin in diabetic foot ulcers. Open J Regenerat Med. 2021;10(2):19–30. doi:10.4236/ojrm.2021.102002
37. Morabbi A, Karimian M. Therapeutic potential of exosomal lncRNAs derived from stem cells in wound healing: focusing on mesenchymal stem cells. Stem Cell Res Therap. 2025;16(1):62. doi:10.1186/s13287-025-04200-0
38. Panda B, Sharma Y, Gupta S, et al. Mesenchymal stem cell-derived exosomes as an emerging paradigm for regenerative therapy and nano-medicine: a comprehensive review. Life. 2021;11(8):784. doi:10.3390/life11080784
39. Su C, Zhang J, Yarden Y, et al. The key roles of cancer stem cell-derived extracellular vesicles. Signal Transduc Targeted Ther. 2021;6(1):109. doi:10.1038/s41392-021-00499-2
40. Yang S, Sun Y, Yan C. Recent advances in the use of extracellular vesicles from adipose-derived stem cells for regenerative medical therapeutics. J Nanobiotechnol. 2024;22(1):316. doi:10.1186/s12951-024-02603-4
41. Wang H, Wu S, Bai X, et al. Mesenchymal stem cell-derived exosomes hold promise in the treatment of diabetic foot ulcers. Int J Nanomed. 2025;20:5837–5857. doi:10.2147/IJN.S516533
42. Wang J, Liang YJ, Pan X. Advances in the role of stem cell-derived exosomes in diabetic foot wound healing. Diabetes Metab Syndr Obes. 2025;18:2767–2781. doi:10.2147/DMSO.S521095
43. Palani N, Nagendran S, Mendonce KC, et al. Exosome nanofiber hybrid therapeutics for targeted diabetic wound healing: hypoxia-enhanced ADSC exosomes and PI3K/Akt pathway modulation. Regenerat Engineer Transl Med. 2025. doi:10.1007/s40883-025-00465-2
44. Zhang C, Zhou X, Wang D, et al. Hydrogel-loaded exosomes: a promising therapeutic strategy for musculoskeletal disorders. J Clin Pharmac Therap. 2023;2023(1):1105664. doi:10.1155/2023/1105664
45. Levy O, Kuai R, Siren EMJ, et al. Shattering barriers toward clinically meaningful MSC therapies. Sci Advanc. 2020;6(30):
46. Vazirzadeh M, Azarpira N, Vosough M, et al. Galactosylation of rat natural scaffold for MSC differentiation into hepatocyte-like cells: a comparative analysis of 2D vs. 3D cell culture techniques. Biochem Biophysic Rep. 2023;35:101503. doi:10.1016/j.bbrep.2023.101503
47. Lotfinejad P, Shamsasenjan K, Baradaran B, et al. Immunomodulatory effect of human umbilical cord blood-derived mesenchymal stem cells on activated T-lymphocyte. Iranian J Allergy Asthma Immunol. 2021;20(6):711–720. doi:10.18502/ijaai.v20i6.8022
48. Lopes L, Setia O, Aurshina A, et al. Stem cell therapy for diabetic foot ulcers: a review of preclinical and clinical research. Stem Cell Res Ther. 2018;9(1):188. doi:10.1186/s13287-018-0938-6
49. Luo Q, Wang N, Que H, et al. Pluripotent stem cell-derived hepatocyte-like cells: induction methods and applications. Int J Mol Sci. 2023;24(14):11592. doi:10.3390/ijms241411592
50. Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell. 2006;126(4):663–676. doi:10.1016/j.cell.2006.07.024
51. Casaroli-Marano RP, Nieto-Nicolau N, Martínez-Conesa E, et al. Potential role of induced pluripotent stem cells (IPSCs) for cell-based therapy of the ocular surface. J Clin Med. 2015;4(2):318–342. doi:10.3390/jcm4020318
52. Argentati C, Tortorella I, Bazzucchi M, et al. Harnessing the potential of stem cells for disease modeling: progress and promises. J Personalized Med. 2020;10(1):8. doi:10.3390/jpm10010008
53. Ren Y, Zhang S, Liang Y, et al. Feeder cells treated with ethanol can be used to maintain self‐renewal and pluripotency of human pluripotent stem cells. FEBS Open Bio. 2023;13(2):279–292. doi:10.1002/2211-5463.13538
54. Yan J, Liang J, Cao Y, et al. Efficacy of topical and systemic transplantation of mesenchymal stem cells in a rat model of diabetic ischemic wounds. Stem Cell Res Therap. 2021;12(1):220. doi:10.1186/s13287-021-02288-8
55. Huang H, Xin R, Li X, et al. Physical therapy in diabetic foot ulcer: research progress and clinical application. Int Wound J. 2023;20(8):3417–3434. doi:10.1111/iwj.14196
56. Yang H, Zhang Y, Du Z, et al. Hair follicle mesenchymal stem cell exosomal lncRNA H19 inhibited NLRP3 pyroptosis to promote diabetic mouse skin wound healing. Aging. 2023;15(3):791–809. doi:10.18632/aging.204513
57. Wu J, Chen L-H, Sun S-Y, et al. Mesenchymal stem cell-derived exosomes: the dawn of diabetic wound healing. World J Diab. 2022;13(12):1066. doi:10.4239/wjd.v13.i12.1066
58. O’Loughlin A, O’Brien T. Topical stem and progenitor cell therapy for diabetic foot ulcers. In: Stem Cells in Clinic and Research. IntechOpen; 2011.
59. Hou C, Chang Y-F, Yao X. Supramolecular adhesive materials with antimicrobial activity for emerging biomedical applications. Pharmaceutics. 2022;14(8):1616. doi:10.3390/pharmaceutics14081616
60. Zhang X, Li W, Wei G, et al. A rapid-crosslinking antimicrobial hydrogel with enhanced antibacterial capabilities for improving wound healing. Front Physiol. 2023;14:1206211. doi:10.3389/fphys.2023.1206211
61. Kim C-D, Koo K-M, Kim H-J, et al. Recent advances in nanomaterials for modulation of stem cell differentiation and its therapeutic applications. Biosensors. 2024;14(8):407. doi:10.3390/bios14080407
62. Rajendran A, Rajan RA, Balasubramaniyam S, et al. Nano delivery systems in stem cell therapy: transforming regenerative medicine and overcoming clinical challenges. Nano TransMed. 2025;4:100069. doi:10.1016/j.ntm.2024.100069
63. Wei S, Dong J, Hu Q, et al. Advances in Mesenchymal Stem Cells and Their Derivatives for Promoting Peripheral Nerve Regeneration. 13. Burns & Trauma; 2025:
64. Gong H, Yang L, Li Y, et al. Metal-polyphenol nanocomposite hybrid hydrogel: a multifunctional platform for treating diabetic foot ulcers through metabolic microenvironment reprogramming. Biomaterials. 2025;322:123414. doi:10.1016/j.biomaterials.2025.123414
65. Yu Q, Qiao G-H, Wang M, et al. Stem cell-based therapy for diabetic foot ulcers. Front Cell Develop Biol. 2022;10:812262. doi:10.3389/fcell.2022.812262
66. Bogomiakova ME, Sekretova EK, Anufrieva KS, et al. iPSC-derived cells lack immune tolerance to autologous NK-cells due to imbalance in ligands for activating and inhibitory NK-cell receptors. Stem Cell Res Ther. 2023;14(1):77. doi:10.1186/s13287-023-03308-5
67. Haneef K, Salim A, Hashim Z, et al. Chemical hypoxic preconditioning improves survival and proliferation of mesenchymal stem cells. Appl Biochem Biotechnol. 2024;196(7):3719–3730. doi:10.1007/s12010-023-04743-z
68. Panda D, Nayak S. Stem cell-based tissue engineering approaches for diabetic foot ulcer: a review from mechanism to clinical trial. Stem Cell Rev Rep. 2024;20(1):88–123. doi:10.1007/s12015-023-10640-z
69. El Hage R, Knippschild U, Arnold T, et al. Stem cell-based therapy: a promising treatment for diabetic foot ulcer. Biomedicines. 2022;10(7):1507. doi:10.3390/biomedicines10071507
70. Guo J, Dardik A, Fang K, et al. Meta-analysis on the treatment of diabetic foot ulcers with autologous stem cells. Stem Cell Res Therap. 2017;8(1):228. doi:10.1186/s13287-017-0683-2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Advances in Yupingfeng San Research: Multi-Target Mechanisms and Clinical Evidence
Gao S, Wang Y, Li X, Zheng L, Zhan Z, Wang J
Drug Design, Development and Therapy 2026, 20:603491
Published Date: 18 May 2026