Back to Journals » Journal of Pain Research » Volume 18
Advances in Electroacupuncture for Treatment of Knee Osteoarthritis: Mechanisms, Efficacy, and Future Directions
Received 28 May 2025
Accepted for publication 23 September 2025
Published 30 September 2025 Volume 2025:18 Pages 5083—5108
DOI https://doi.org/10.2147/JPR.S543346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Xiaohong Wu,1 Sikang Li,1 Mengmeng Wu2
1Department of Acupuncture and Moxibustion, Wuhu Traditional Chinese Medicine Hospital, Anhui College of Traditional Chinese Medicine, Wuhu, Anhui, People’s Republic of China; 2Geriatric Department, The Second Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui, People’s Republic of China
Correspondence: Mengmeng Wu, Geriatric Department, The Second Affiliated Hospital of Anhui University of Chinese Medicine, Hefei, Anhui, People’s Republic of China, Email [email protected]
Abstract: Knee osteoarthritis (KOA) is a common chronic degenerative joint disease marked by progressive cartilage loss, subchondral bone remodeling, and synovial inflammation, resulting in persistent pain, functional disability, and diminished quality of life. Electroacupuncture (EA), a modality combining traditional acupuncture with electrical stimulation, has gained attention as a non-pharmacological intervention for KOA. Growing evidence suggests that EA not only reduces pain and enhances joint mobility but also modulates diverse biological processes—such as neuroendocrine signaling, inflammatory cascades, cartilage metabolism, and local hemodynamics. Mechanistically, EA acts through multi-target mechanisms, including suppression of pro-inflammatory mediators, promotion of anti-inflammatory and chondroprotective factors, and regulation of critical signaling pathways such as NF-κB, MAPK, and Wnt/β-catenin. Additionally, EA engages central and peripheral neuromodulatory systems involving opioid, serotonergic, and cannabinoid receptors, underpinning its analgesic properties. Despite encouraging outcomes, current support derives predominantly from small-scale clinical trials with short follow-up periods, underscoring the necessity for large-scale, randomized controlled studies with rigorous designs to establish standardized protocols and validate long-term benefits. This review synthesizes contemporary understanding of EA’s mechanisms and efficacy in KOA management, addressing ongoing challenges and outlining future directions for refining EA-based strategies within integrated treatment frameworks.
Keywords: knee osteoarthritis, electroacupuncture, analgesia, inflammation, cartilage repair, biological mechanisms
Introduction
Knee osteoarthritis (KOA) is a common degenerative joint disease, primarily characterized by the gradual destruction of articular cartilage, narrowing of the joint space, and the formation of bone spurs, often leading to pain, stiffness, and functional impairment.1 According to global research, epidemiological data indicate that approximately 10% to 15% of adults are affected, with a higher incidence in the elderly population.2 Due to its substantial morbidity and disability rates, KOA exerts dual physical and psychological impacts on patients and poses a significant burden on families and society.3 The disease arises from an imbalance between joint tissue repair and degradation, with central pathological processes involving the degeneration and breakdown of articular cartilage, although the precise mechanisms remain incompletely understood.4 Current knowledge of KOA pathogenesis encompasses genetic, biomechanical, inflammatory, and aging-related mechanisms.5 Moreover, OA is a whole-joint disorder involving interactions among multiple tissues including cartilage, synovium, subchondral bone, ligaments, and menisci.6 For instance, cartilage degradation products in OA activate synovial inflammation and reduce protective joint capacity, leading to abnormal stress on bone.7 Activated synovium releases destructive cytokines that directly attack cartilage and worsen the joint environment.8 Concurrently, subchondral bone sclerosis diminishes shock-absorbing functionality and exacerbates cartilage breakdown through biochemical crosstalk, while osteophyte formation further disrupts joint architecture.9 Additionally, injuries to ligaments and menisci directly cause mechanical instability, abnormally increasing load on other joint tissues and accelerating wear.3 Accumulating evidence suggests that the holistic nature of KOA implies that therapies targeting a specific tissue or systemic interventions (eg, weight loss) can produce beneficial ripple effects across the joint.6 For example, inhibiting bone remodeling may reduce mechanical stress on subchondral bone and indirectly benefit cartilage;10 potent anti-inflammatory interventions can simultaneously suppress synovitis and cartilage inflammation;11 and weight loss alleviates loading on cartilage, bone, and synovium through both biomechanical and biochemical mechanisms.12 Meniscal pathology may also ameliorate with treatment for KOA.13
Current management primarily involves non-steroidal anti-inflammatory drugs (NSAIDs), such as etoricoxib and celecoxib, which selectively inhibit prostaglandin synthesis to reduce joint swelling and pain through anti-inflammatory effects. However, issues including side effects, adverse reactions, and transient efficacy remain concerning.14 Although glucosamine sulfate aims to support cartilage repair by replenishing cartilage matrix, delaying degradation, and restoring chondrocyte activity-thereby improving articular cartilage function-its effects are slow-onset, often requiring long-term use as an adjunct therapy.15 In severe advanced cases, surgical options such as unicompartmental knee arthroplasty, total knee replacement, and high tibial osteotomy are available. Nonetheless, factors including high cost, prolonged recovery, and risk of complications limit their adoption.16 Therefore, identifying safer and more effective treatment strategies remains a priority in clinical research.
Electroacupuncture (EA), an integrative modality combining traditional acupuncture with modern electrical stimulation, has a long history of use in clinical practice within traditional Chinese medicine. It is recognized for its effects in warming meridians, promoting Qi and blood circulation, reducing inflammation, and alleviating pain. Valued for its rapid onset, efficacy, cost-effectiveness, and favorable safety profile, EA enhances acupuncture effects through electrical stimulation of acupoints, improving local blood flow, relieving pain, and restoring joint function.17 In recent years, EA has gained increasing attention in KOA management, with preliminary studies demonstrating promising outcomes in pain relief and functional improvement.18,19 Research indicates that EA significantly alleviates muscular pain, joint stiffness, and numbness in KOA patients, while also enhancing immune function, contributing to its broad clinical application.20 Furthermore, EA modulates chondrocyte proliferation and apoptosis, inhibits extracellular matrix (ECM) degradation, attenuates chondrocyte degeneration, and facilitates the repair of damaged cartilage, thereby effectively ameliorating clinical symptoms of KOA.21
The mechanisms underlying EA’s efficacy in KOA involve synergistic multi-target and multi-pathway effects. It not only downregulates pro-inflammatory factors such as IL-1β, TNF-α, and MMPs but also upregulates protective factors including TGF-β and TIMP-1, thereby suppressing inflammatory responses and delaying cartilage matrix degradation.22 Additionally, EA modulates signaling pathways such as MAPK, NF-κB, and PI3K/Akt, inhibiting inflammation and apoptosis at genetic and protein levels, promoting cartilage repair, and reducing osteophyte formation.23 At the cellular level, EA helps maintain water metabolism balance by reducing aquaporin 3 (AQP3) expression24 and regulates mitochondrial function and the Bcl-2/Bax ratio to inhibit apoptosis.25 Moreover, EA improves peri-articular muscle strength and biomechanical balance, optimizes load distribution across the joint, and reduces abnormal stress on cartilage, thereby slowing degenerative processes.26 In terms of analgesia, EA activates multiple pain regulatory systems including cannabinoid receptors (CB1R/CB2R), serotonin (5-HT) receptors, and μ/δ-opioid receptors, effectively inhibiting peripheral and central sensitization to pain.27,28 Clinical studies confirm that EA monotherapy-particularly when using dense-sparse wave patterns and higher current intensities-outperforms manual acupuncture in alleviating pain and improving joint function, effects correlated with modulation of inflammatory cytokines such as TNF-α and IL-1β.22 EA is also frequently combined with moxibustion, herbal medicine, pharmaceuticals, manual therapy, and physical interventions to form integrated treatment protocols. These combination strategies often yield superior outcomes in joint function and inflammatory markers compared to monotherapies.29 Other mechanisms include regulation of the TLR4/NF-κB and Wnt/β-catenin pathways, inhibition of synovitis and cartilage degradation, and multi-level holistic effects achieved through modulation of pain-related factors and improved biomechanical equilibrium.23 In summary, EA exerts multi-pathway, multi-target regulatory effects on inflammatory responses, signaling pathways, and cellular metabolism, effectively inhibiting cartilage degradation, promoting tissue repair, alleviating pain, and improving knee joint function. It represents a synergistic and mechanism-rich therapeutic approach for KOA.
Despite recent advances in both clinical and basic research on EA for KOA, a comprehensive synthesis of findings is lacking. This review aims to summarize the fundamental principles of EA, its clinical applications in analgesia and functional improvement, and elucidate its mechanisms-both in peripheral and central nervous systems for pain relief-and its chondroprotective effects mediated through suppression of inflammatory responses and retardation of joint degeneration.
Basic Principles and Techniques of EA
Definition and Operation Method of EA
EA is a new therapy that combines traditional acupuncture with electrical stimulation by introducing electric current into the acupuncture needles to enhance the efficacy of acupuncture. During EA treatment, after the needle is inserted into the acupoint and qi is obtained, a small amount of electric current that the human body could tolerate is applied to the needle, thereby stimulating the acupoint to achieve therapeutic effects. Its advantages include the combination of two types of stimulation, needling and electrical current, which could improve efficacy; the parameters of electrical stimulation, such as waveform, frequency, and intensity, are easier to control and have strong repeatability; EA replaces manual needling, saving labor and improving treatment efficiency, thus benefiting more patients.30 The operation method of EA typically involves selecting appropriate acupoints, then using specialized EA equipment to insert the needle into the skin and apply low-frequency or high-frequency current through electrodes. During the operation, the practitioner needs to adjust the intensity, frequency, and waveform of the current based on the patient’s specific condition and response to achieve the best therapeutic effect.31 EA has a wide range of applications, commonly used in pain management, neurological rehabilitation, musculoskeletal diseases, and other treatments.32 Research shows that EA could inhibit synovial inflammation, reduce inflammatory stimulation;33 suppress cartilage degeneration, repair cartilage tissue;5 regulate the expression of related pain receptors, exert analgesic effects;28 thereby improving clinical symptoms such as limited activity due to knee joint pain and enhancing the quality of life of patients.
Differences Between EA and Traditional Acupuncture
EA and AM exhibit distinct differences in the management of KOA, particularly in their modes of stimulation and mechanisms of action. EA delivers continuous electrical current to specific acupoints (eg, ST34, ST35, SP10), providing consistent and quantifiable stimulation parameters. This approach more effectively modulates pain pathways and inflammatory responses, with notable efficacy in suppressing pro-inflammatory cytokines such as TNF-α and IL-1β.22,34,35 In contrast, AM relies on manual needle manipulation (eg, lifting, thrusting, and rotating) to elicit the deqi sensation. Its effects are oriented more toward systemic regulation of Qi and blood, functional recovery, and particularly excel in alleviating joint stiffness and improving long-term functional capacity.36–38
In terms of clinical efficacy, EA demonstrates superior short-term analgesic effects and enhancement of joint mobility, attributable to its ability to promote the release of endogenous opioids and activate descending pain inhibitory pathways.39–41 While AM may exhibit less immediate pain relief compared to EA, it offers unique advantages in ameliorating depressive symptoms, enhancing quality of life, and improving functional mobility-particularly in patients with deficiency patterns such as kidney and marrow insufficiency in KOA.42–44 Furthermore, AM emphasizes pattern-based acupoint selection and highly individualized treatment strategies, aligning with the holistic principles of Traditional Chinese Medicine.45,46
From the perspectives of applicability and patient tolerance, EA’s adjustable electrical parameters make it more suitable for individuals tolerant to stronger stimulation. It also integrates readily with modern rehabilitation therapies, such as extracorporeal shockwave treatment, forming comprehensive therapeutic regimens.47,48 Conversely, AM is often better suited for patients sensitive to electrical stimulation or those presenting with complex deficiency patterns. It demonstrates sustained benefits in long-term symptom management and relapse prevention.38,43,49 Thus, in clinical practice, the choice or combination of EA and AM should be tailored to the patient’s specific condition], syndrome pattern, and treatment goals to optimize therapeutic outcomes (Table 1).
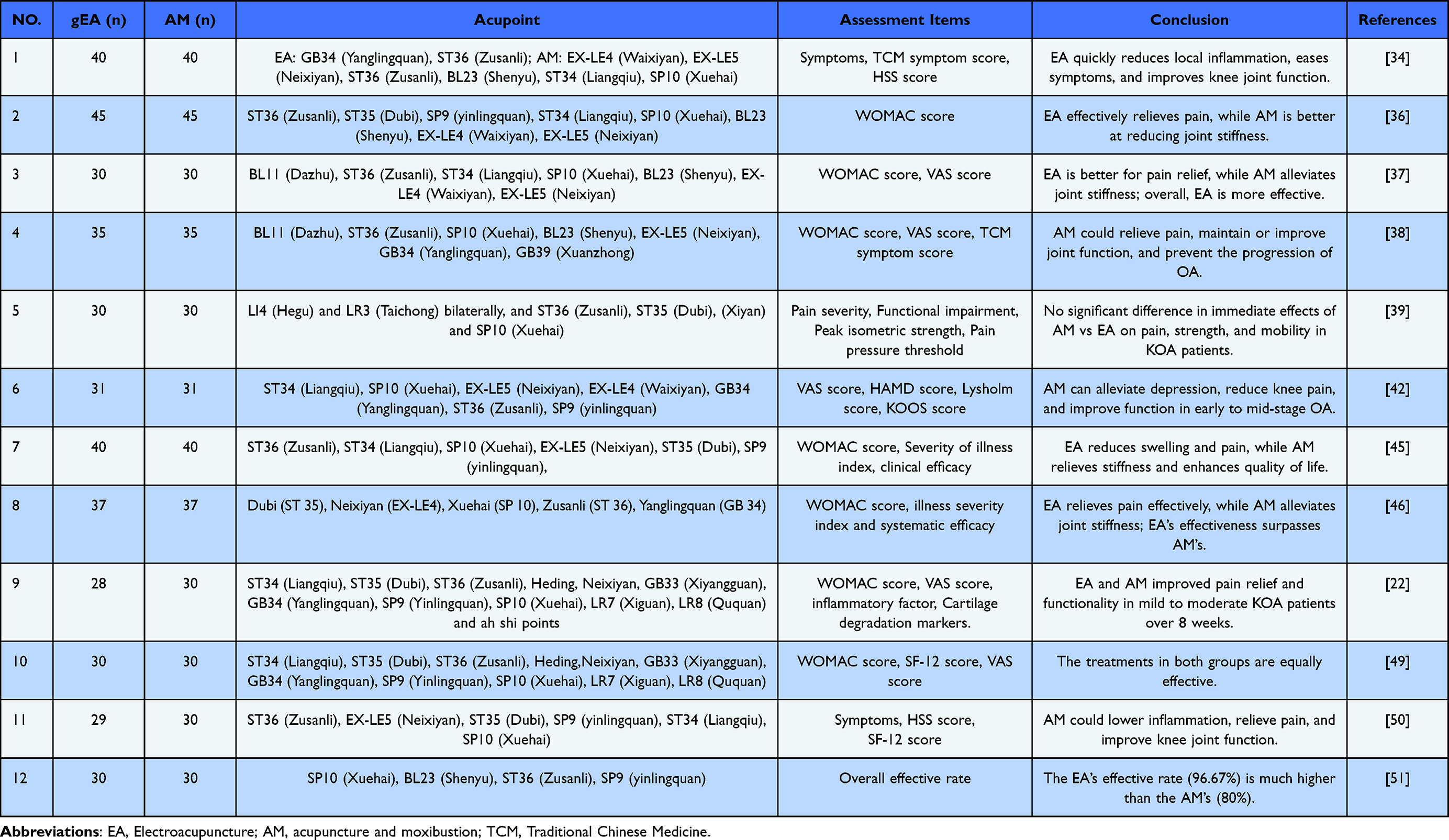 |
Table 1 Efficacy Comparison Between EA and AM in the Treatment of KOA |
Relationship Between Stimulation Parameters of EA and Effects
EA exerts its therapeutic effects in KOA through carefully selected stimulation parameters, each playing a distinct role in neuromodulation and clinical efficacy. A data mining study showed that the two most commonly connected acupoints for EA are Neixiyan-Dubi and Liangqiu-Xuehai (Figure 1), with the most frequently used stimulation parameters being sparse wave, dense wave, 2 Hz, 2/100 Hz, tolerable intensity, 30 min/session, treated once every other day, for a total treatment duration of 4 weeks.52 The waveform and frequency are particularly significant: dilatational waves (eg, 2/100 Hz) are most commonly employed for their ability to simultaneously activate multiple opioid receptors and reduce neural adaptation, thereby enhancing analgesic and anti-inflammatory outcomes.47,52,53 In contrast, low-frequency continuous waves (2–5 Hz) predominantly activate μ-opioid pathways to alleviate pain, while higher frequencies (15–100 Hz) are more effective in reducing muscle spasms and modulating local inflammation.54–56 The selection of appropriate waveform and frequency thus directly influences neurotransmitter release and subsequent pain modulation.
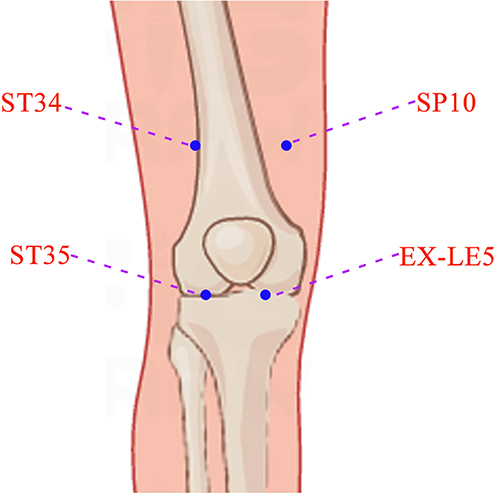 |
Figure 1 The Two Top Commonly Connected Acupuncture Points (lateral: “Liangqiu” (ST34) and “Dubi” (ST35), medial: “Xuehai” (SP10) and “Neixiyan” (EX-LE5)). |
Current intensity and treatment scheduling are equally critical in achieving optimal results. Intensity must be individualized to a patient’s tolerance level, typically ranging between 2–5 mA, as stronger yet tolerable stimulation has been associated with more pronounced and sustained analgesia through enhanced Aδ and C-fiber engagement.57–59 Regarding treatment regimen, a session duration of 20–30 minutes applied 3 times per week over 4–6 weeks has been consistently adopted in clinical protocols to balance efficacy and practicality.60–62 Intensive treatment within this window facilitates cumulative biological effects-including reduced pro-inflammatory cytokines and improved functional mobility-without compromising patient adherence.59,63
The interplay of these parameters ultimately determines the effectiveness of EA in managing KOA. Longer treatment courses (≥4 weeks) with adequate session frequency are necessary to address chronic pain mechanisms, such as central sensitization and synovitis, and to promote longer-lasting functional improvements.58,59 Tailoring parameters to specific clinical presentations-for instance, using higher frequencies for acute inflammatory pain and lower frequencies for chronic dysfunction-can further optimize outcomes.64,65 Future studies should focus on stratified patient analyses to establish phenotype-specific parameter recommendations, advancing toward personalized EA applications in osteoarthritis therapy (Table 2).
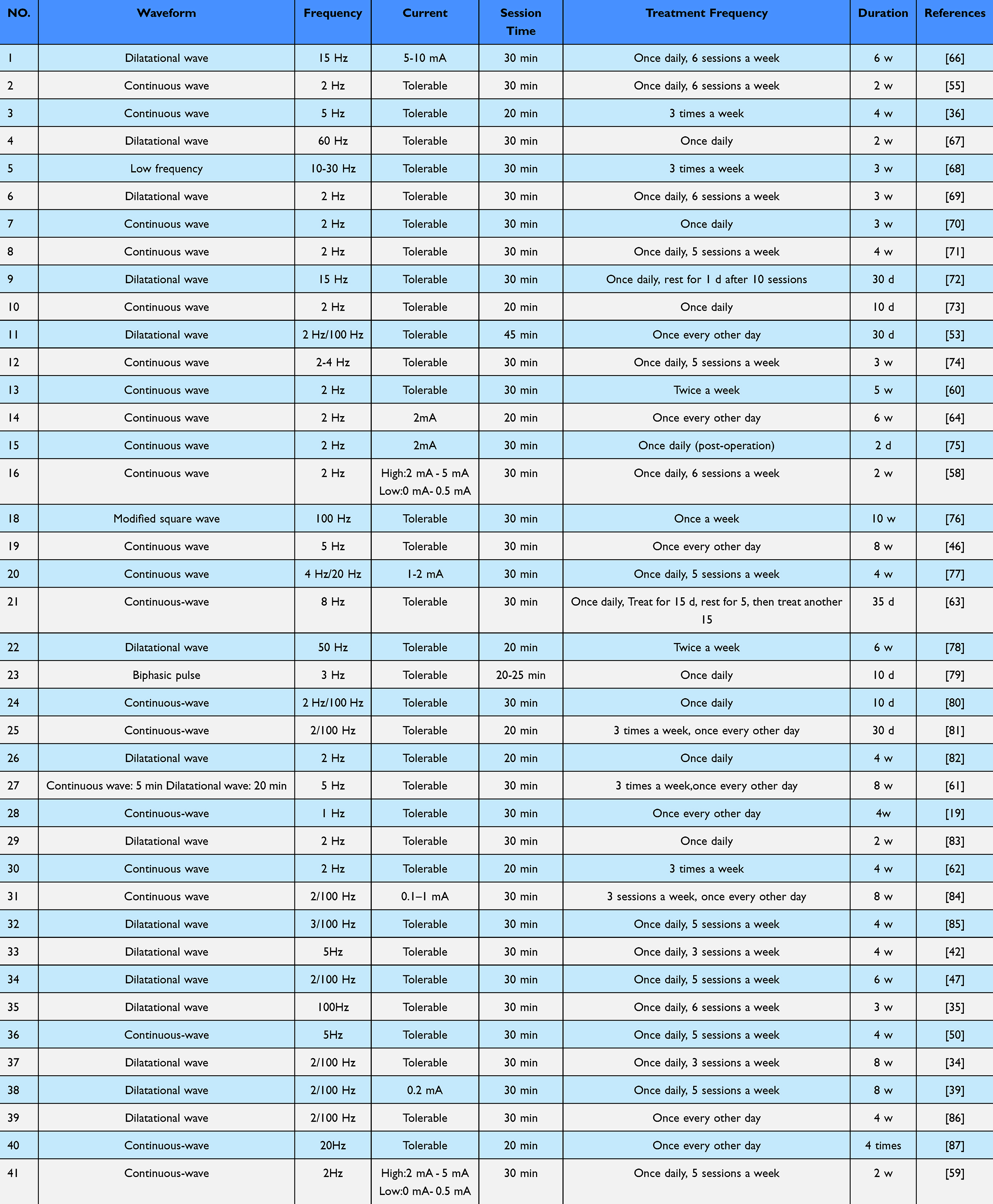 |
Table 2 Parameters of EA Treatment for KOA |
The Impact of EA on KOA Pain
Physiological Basis of Pain Mechanisms
KOA is a common degenerative joint disease with a complex pain mechanism involving various physiological and biochemical pathways. Chronic pain is one of the main symptoms in KOA patients, primarily consisting of peripheral nociceptive pain and central sensitization pain.88 In terms of joint injury and inflammation, the pain in KOA mainly originates from damage to the articular cartilage, synovial inflammation, and sensitization of peripheral nerves. The degeneration of articular cartilage and osteophyte formation could lead to increased mechanical load within the joint, stimulating nerve endings and releasing inflammatory mediators such as prostaglandins and cytokines, which further promote the activation of pain receptors.89 In terms of signaling molecules and pathways, interactions among the nerve growth factor (NGF)/TrkA signaling pathway, calcitonin gene-related peptide (CGRP), CCL2/CCR2 signaling pathway, tumor necrosis factor-alpha (TNF-α), interleukin-1 beta (IL-1β), NLRP3 inflammasome, and Wnt/β-catenin signaling pathway play a role in the generation and maintenance of OA pain, affecting both the peripheral and central nervous systems. For example, NGF is produced in joint tissues through the upregulation of cytokines like TNF, leading to sensitization of the nervous system.90 CGRP is expressed in nociceptive neurons and participates in pain signal transmission.91 The CCL2/CCR2 signaling pathway plays a central role in OA pain behavior.92 TNF-α and IL-1β, as pro-inflammatory cytokines, are critical but have limited clinical treatment effects.93 The NLRP3 inflammasome is involved in the production of active IL-1β,94 while abnormal activation of the Wnt/β-catenin signaling pathway is associated with chronic pain.95 A review confirmed that EA produces a greater analgesic effect than manual acupuncture (MA) for different types of pain.96 Studies have found that EA could effectively reduce the levels of inflammatory mediators in the joint by modulating local inflammatory responses and promoting blood circulation, thereby alleviating pain.97
EA treatment could upregulate the expression of miR-214 in OA knee cartilage, which may participate in the expression of proteins involved in apoptosis and pain transmission by inhibiting its downstream targets, thus exerting therapeutic effects.98 EA combined with extracorporeal shock wave (ESW) therapy could significantly reduce the levels of inflammatory factors such as nitric oxide (NO), interleukin-1 beta (IL-1β), tumor necrosis factor-alpha (TNF-α), and matrix metalloproteinase-3 (MMP-3) in joint synovial fluid, while increasing the levels of superoxide dismutase (SOD) and transforming growth factor-beta1 (TGF-β1). These changes help reduce joint inflammatory responses, improve joint microcirculation, relieve muscle spasms, and positively impact joint mobility.48 Additionally, the mechanism of action of EA may also be related to the regulation of the central nervous system, as EA stimulation could activate analgesic pathways in the spinal cord and brain, inhibit spinal dorsal horn afferent neurons, reduce the transmission of pain signals, and promote the release of endogenous analgesic substances such as endorphins and brain-derived neurotrophic factor (BDNF).40
Clinical Evidence of EA’s Analgesic Effects
In recent years, the effectiveness of EA in managing KOA pain has been supported by an increasing number of clinical studies. A randomized controlled trial showed that patients in the EA treatment group had significantly better pain scores and functional assessments than the control group, with effects lasting for several weeks.99 Another study indicated that EA could effectively improve joint function in KOA patients and reduce the need for traditional analgesics, thereby lowering the risk of drug-related side effects.100 Furthermore, different parameter settings for EA (such as frequency and intensity) have also been shown to significantly impact pain relief, with appropriate parameter selection enhancing treatment effects.101 In a large cohort study based on KOA patients, it was found that the β-diversity of the gut microbiome was significantly correlated with knee joint WOMAC scores, and the abundance of streptococci was significantly related to the severity of knee joint effusion, indicating that gastrointestinal microbiota directly contribute to pain and inflammation associated with knee osteoarthritis.102 Overall, existing clinical evidence suggests that EA, as a non-invasive treatment method, has a good effect on pain relief in patients with knee osteoarthritis.
Advantages and Challenges of EA in Pain Management
The advantages of EA in pain management mainly lie in its non-pharmacological nature and lower risk of side effects. Compared to traditional drug treatments, EA not only effectively alleviates pain but also improves patients’ quality of life and reduces drug dependence.49 Additionally, the therapeutic effects of EA are often relatively long-lasting, allowing patients to continue enjoying good pain control after treatment.39 However, EA still faces some challenges in practical application, including insufficient standardization of treatment and the influence of individual differences. Different patients may respond significantly differently to EA, and how to develop personalized EA treatment plans requires further research.31 Moreover, although the efficacy of EA has received some clinical evidence support, verifying its long-term effects and safety in large, multi-center randomized controlled trials remains an important direction for future research.37
Research on EA for Improving Knee Joint Function
Selection of Functional Assessment Indicators
The selection of functional assessment indicators is fundamental to evaluating EA efficacy in KOA, with pain intensity scales serving as the primary endpoint for analgesic effect. The Visual Analog Scale (VAS) is most widely employed due to its sensitivity in capturing subjective pain perception.103 Studies consistently demonstrate that EA leads to more significant and rapid VAS reductions compared to AM, a difference attributed to its sustained electrical stimulation and stronger activation of endogenous opioid pathways.34,37,46 While AM also alleviates pain, its effects on VAS are often more gradual, reflecting its reliance on manual needle manipulation and holistic regulatory mechanisms rather than targeted neuromodulation.
For evaluating physical function, joint-specific scales such as the WOMAC and HSS provide nuanced insights into domain-specific improvements.104,105 The WOMAC, in particular, is valuable for its ability to dissect outcomes into pain, stiffness, and physical function subscales. EA consistently shows superior performance in enhancing physical function-such as walking and stair climbing-linked to its anti-inflammatory and neuromuscular modulation effects.36,41,49 In contrast, AM frequently demonstrates comparable or even greater efficacy in reducing joint stiffness, suggesting a stronger influence on local soft tissue compliance and microcirculation through biomechanical needle manipulation.36,37
Beyond pain and joint-specific metrics, broader patient-reported outcomes such as the SF-12 and KOOS quality-of-life scales capture the holistic impact of treatment.106 These tools reveal distinctive strengths of AM, particularly in improving mental health components and overall well-being, which align with its traditional focus on systemic balance and Qi regulation.43,45 In cases of deficiency patterns like kidney and marrow insufficiency, AM shows pronounced benefits in alleviating secondary symptoms such as fatigue and mood disturbances, underscoring the importance of pattern-specific evaluation in traditional Chinese medicine interventions.38,50
Incorporating psychological and syndrome-specific instruments-such as the Hamilton Depression Scale (HAMD) or TCM symptom scores-enables a more comprehensive efficacy profiling. These assessments highlight therapeutic dimensions beyond conventional orthopaedic metrics, emphasising AM’s role in addressing comorbidity and personalised dysfunction.42,45 A multimodal evaluation strategy is thus essential, as it clarifies that EA excels in biomechanical pain and functional recovery, whereas AM offers broader benefits in stiffness, mental well-being, and holistic regulation. Future clinical trials should adopt integrated assessment protocols to fully elucidate the complementary strengths of EA and AM (Tables 1 and 3).
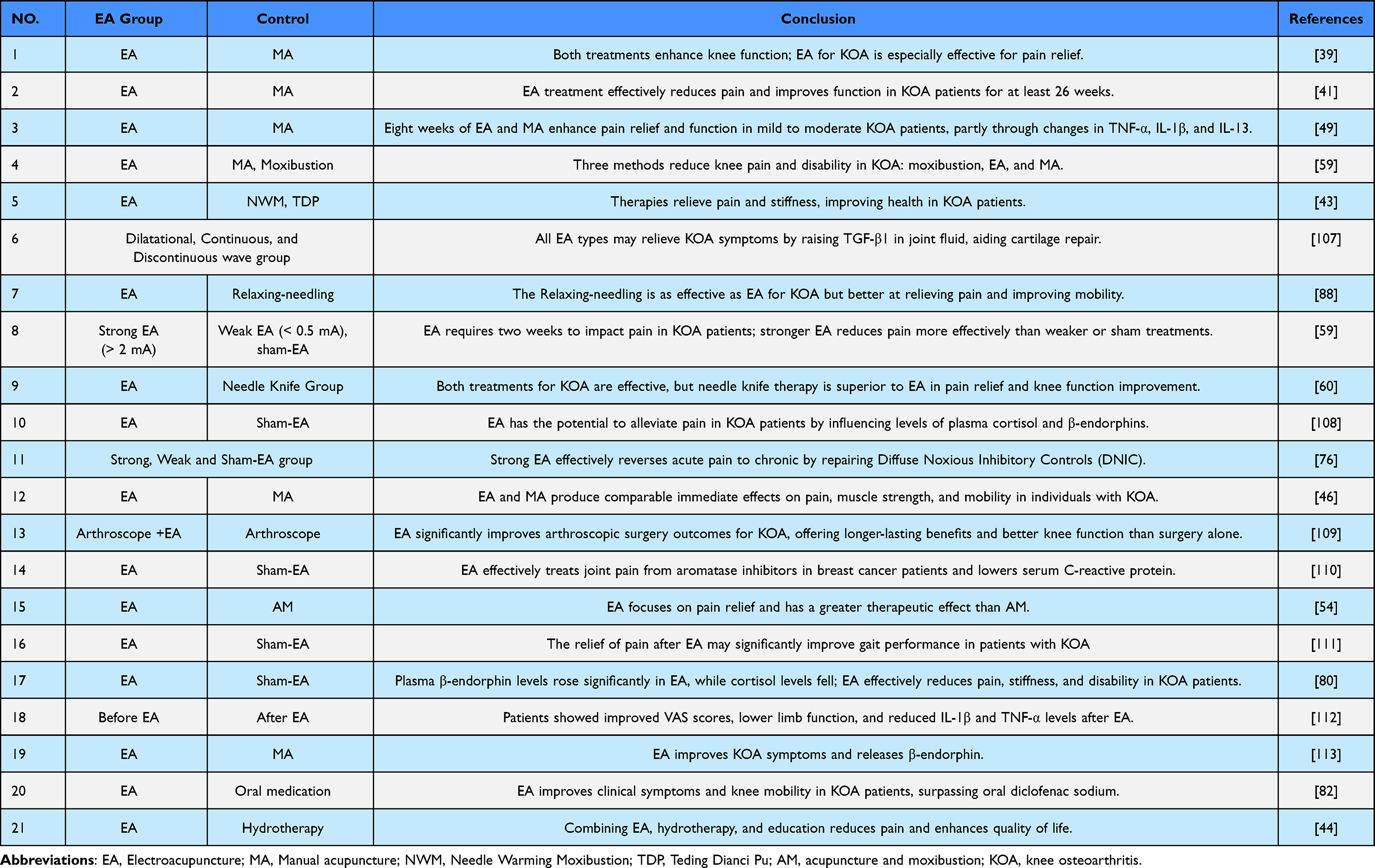 |
Table 3 The Impact of EA on Pain and Knee Joint Function in Patients with KOA |
Summary and Analysis of Clinical Trial Results
Clinical trials directly comparing EA and AM provide robust evidence for their efficacy in treating KOA, yet reveal distinct therapeutic profiles shaped by their mechanisms and application. Meta-analyses of these studies consistently confirm that both interventions are significantly superior to sham acupuncture or wait-list controls, but they excel in different clinical domains. EA demonstrates pronounced advantages in rapid analgesia and objective functional improvement, largely attributable to its quantifiable, intensity-dependent neurostimulation that effectively modulates pain pathways and local inflammation.41,49,59 In contrast, AM shows sustained benefits in enhancing joint flexibility, reducing stiffness, and improving quality of life, aligning with its holistic approach to regulating Qi and blood circulation.36,37,43
A detailed analysis of outcome measures clarifies this divergence. In studies utilizing the VAS and WOMAC pain subscale, EA frequently achieves greater and faster reduction in pain scores. This is mechanistically linked to its ability to elicit strong endogenous opioid release and suppress pro-inflammatory cytokines (eg, TNF-α, IL-1β), particularly when higher current intensities (2–5 mA) and mixed frequencies (2/100 Hz) are applied.40,59 Conversely, AM, while effective for pain relief, often yields more gradual analgesia but excels in the WOMAC stiffness subscale and functional mobility tests. Furthermore, EA has also been found to improve joint function by modulating inflammatory responses, a mechanism that may be related to the regulation of the Wnt/β-catenin signaling pathway.114 This suggests its mode of action-relying on deqi sensation and manual manipulation-may more effectively influence periarticular soft tissue compliance and proprioceptive function.37,46,111
The long-term and holistic outcomes further differentiate these modalities. Trials incorporating quality-of-life measures such as SF-12 or KOOS reveal that AM often leads to greater improvement in mental health components and overall well-being, especially in patients with underlying deficiency patterns like kidney and marrow insufficiency.42–44 EA, particularly when combined with modern rehabilitation techniques like extracorporeal shockwave therapy, shows strong performance in restoring muscle strength and biomechanical function, as quantified by isokinetic testing and performance-based assessments.48,61,115 Furthermore, the sustainability of treatment effects favors EA in some studies; its modulation of central sensitization leads to prolonged analgesic periods, whereas AM’s benefits on stiffness and functional adaptation appear to accumulate over a longer treatment course.38,41,58 (Tables 1 and 3).
In conclusion, the collective evidence from clinical trials advocates for a tailored and integrated treatment strategy. EA serves as a powerful tool for controlling inflammatory pain and facilitating rapid functional recovery, ideal for patients with acute exacerbations or significant pain-related disability. AM offers a multifaceted approach addressing stiffness, psychological distress, and overall well-being, making it suitable for chronic management and patients with systemic imbalance. Future research should prioritize standardized protocol reporting and head-to-head trials that employ a comprehensive battery of outcomes to fully define the roles of each modality within personalized KOA treatment algorithms.
EA: Biological Mechanisms
EA is a therapeutic approach that combines traditional acupuncture with electrical stimulation, demonstrating promising efficacy in recent years for pain management, inflammation modulation, and cartilage protection. Research into its biological mechanisms has deepened, revealing the multifaceted roles in neuromodulation, inflammatory responses, and chondroprotection.
Neuromodulation Mechanisms
EA activates the peripheral nervous system by stimulating specific acupoints, thereby regulating central nervous system responses. This mechanism primarily involves the release of neurotransmitters and the activation of neural pathways. Peripheral pain sensation originates from local tissues in the knee joint, while central pain sensation arises from the central nervous system, namely the spinal cord and brain. The specific mechanisms of central pain disorders include central sensitization in the spinal cord and disruptions in ascending and descending pathways from the brain to the spinal cord. Pain occurrence in KOA patients is related to an imbalance in the function or structure of ascending and descending pathways, mainly manifested at the spinal and brain levels.116 EA treatment could modulate the descending pain control system. Signals from the descending pain pathways originate from the anterior cingulate cortex, hypothalamus, and amygdala, reaching the spinal dorsal horn through the periaqueductal gray (PAG) and the rostral ventromedial medulla (RVM), enhancing or inhibiting nociception directly or indirectly.117
The descending pathways include both pain and analgesic mechanisms, with the analgesic mechanisms mediated by 5-HT, endogenous opioids, and others. Low-frequency (2 Hz) and high-frequency (100 Hz) EA could mediate analgesia through the body’s μ and δ opioid receptors and κ receptors, respectively,118 with the analgesic effect of low-frequency EA being more significant than that of high-frequency.56 Additionally, EA could upregulate the expression of 5-HT2A receptors in the dorsal spinal cord of mice with knee osteoarthritis, and it could also increase the expression of GABAA receptors and KCC2, a protein that controls the inhibitory function of GABAA receptors.119 Injecting 5-HT1 and 5-HT3 receptor antagonists could reduce the analgesic effect of EA.120 Pro-inflammatory factor TNF-α enhances the expression and activity of MMPs, increasing the destructive power of inflammatory cells, thereby destroying joint cartilage, degrading cartilage matrix, and promoting further inflammation. Anti-inflammatory cytokine IL-10 promotes the synthesis of cartilage proteoglycans, protects joint cartilage, prevents the degeneration of joint cartilage, and further alleviates the condition of KOA. Studies have shown that 2 Hz low-frequency EA could upregulate IL-10 levels and downregulate TNF-α levels,65 which is important for maintaining the balance of pro-inflammatory/anti-inflammatory cytokines in cartilage tissue, reducing spinal nociceptive sensitization, delaying OA progression, and relieving pain. Other studies have shown that 1 Hz/15 Hz also alleviates synovial inflammation and referred pain behavior in rats with KOA by activating local sympathetic noradrenergic signals.121 Other neuromodulation mechanisms of EA treatment for KOA are shown in Table 4 and Figure 2.
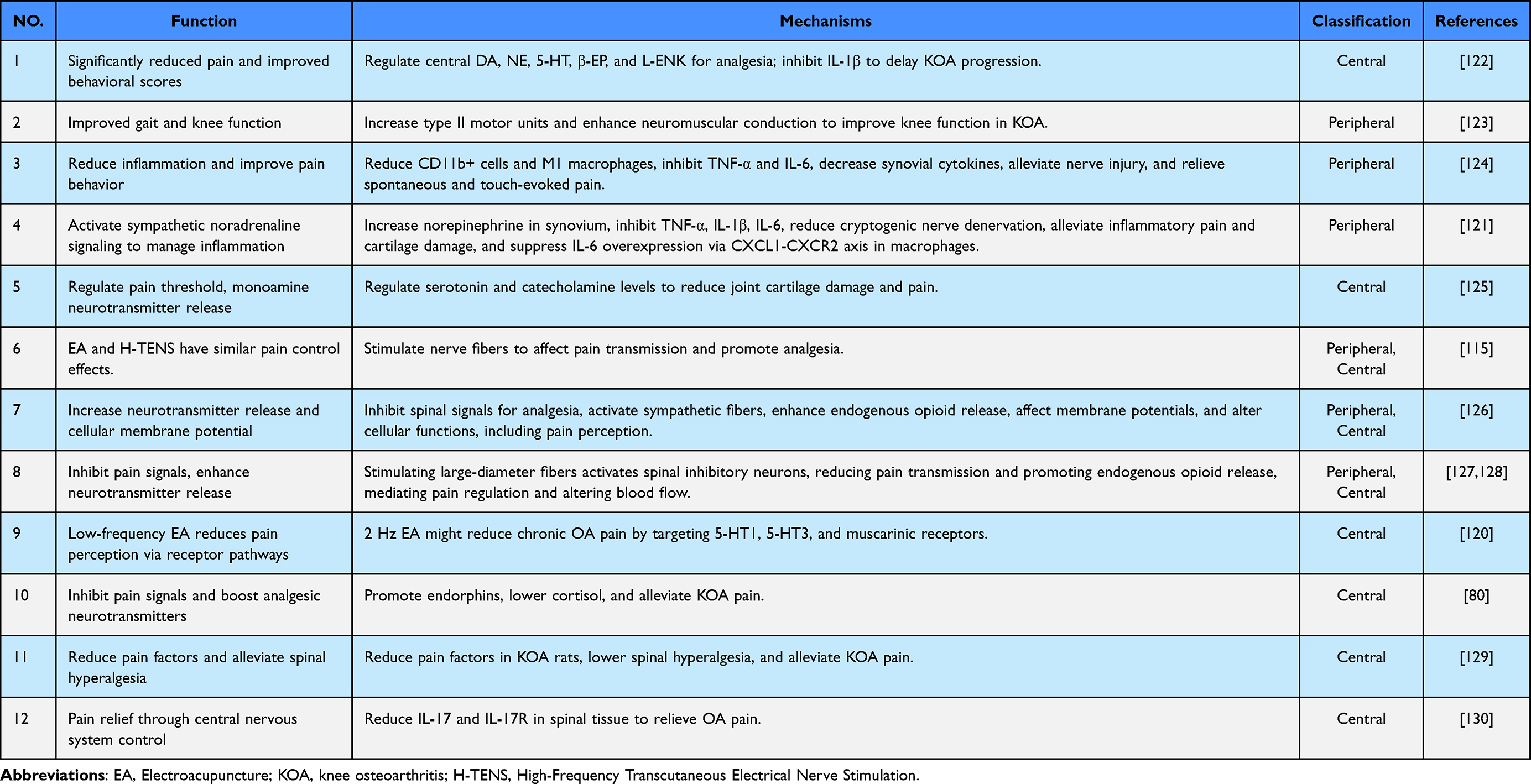 |
Table 4 The Neuromodulatory Mechanisms of EA in KOA |
 |
Figure 2 Mechanisms of EA in alleviating KOA Pain (By Figdraw). EA alleviates KOA pain through synergistic peripheral and central mechanisms. Peripherally, it suppresses inflammation by downregulating pro-inflammatory cytokines (TNF-α, IL-6, IL-1β), reduces M1 macrophage infiltration, elevates norepinephrine levels, and enhances neuromuscular control. Centrally, it facilitates the release of neurotransmitters including 5-HT, NE, β-EP, and ENK, activates μ-opioid receptor signaling pathways, and engages descending pain inhibitory systems, ultimately leading to effective analgesia, attenuated inflammatory responses, and improved motor function and affective state. |
Regulation of Inflammatory Responses
EA exerts its anti-inflammatory effects in KOA through sophisticated regulation of multiple signaling pathways, which collectively mitigate synovitis, reduce cartilage degradation, and alleviate pain. The clinical efficacy of EA is closely associated with its ability to simultaneously target various inflammatory cascades, rebalancing the joint microenvironment from a catabolic, inflammatory state toward a more homeostatic, reparative condition. The following analysis elaborates on key inflammatory pathways modulated by EA and links these mechanisms to observed clinical outcomes.
The NF-κB and MAPK pathways are central regulators of inflammatory responses in KOA. EA significantly inhibits NF-κB activation, reducing nuclear translocation of p65 and downstream production of pro-inflammatory cytokines such as TNF-α, IL-1β, and IL-6.23,131–133 This suppression correlates clinically with reduced joint swelling, pain relief, and improved mobility. Similarly, EA dampens MAPK signaling-particularly p38 and JNK phosphorylation-leading to decreased expression of matrix-degrading enzymes like MMP-13 and ADAMTS5.134–136 Patients receiving EA show lower levels of MMPs and slower radiographic progression, underscoring how these molecular effects translate into cartilage preservation and functional improvement.
EA effectively inhibits the NLRP3 inflammasome, a key complex involved in the cleavage and activation of IL-1β.131,137,138 By reducing the expression of NLRP3, ASC, and caspase-1, EA limits pyroptosis-a highly inflammatory form of cell death-and decreases IL-1β levels in synovial fluid. This mechanism is particularly relevant for patients with significant synovitis and effusion. Clinically, EA-treated individuals exhibit not only reduced pain and swelling but also improved joint function, reflecting the role of NLRP3 in driving symptom severity and structural damage.
Beyond inhibiting inflammation, EA promotes tissue repair through growth factor pathways. EA upregulates TGF-β1, which enhances the synthesis of collagen and proteoglycans while counteracting IL-1β-induced inflammation.139–141 Additionally, EA modulates BMP-2/Smad1/5/8 signaling, stimulating chondrogenesis and inhibiting aberrant subchondral bone remodeling.142,143 Studies have found that EA could improve intestinal function in rats with irritable bowel syndrome, indicating its potential in regulating intestinal inflammation.144 These anabolic effects contribute to the long-term benefits of EA, including sustained functional improvement and delayed disease progression, particularly in patients with early to moderate KOA.
EA also impacts upstream innate immune receptors. It suppresses TLR4 and its adaptor MyD88, thereby inhibiting NF-κB activation and cytokine production.145,146 Moreover, EA enhances SIRT1 expression, which deacetylates HMGB1 and mitigates its pro-inflammatory effects.147,148 These actions lead to reduced synovitis and lower levels of systemic inflammatory markers, which are associated with pain reduction and improved quality of life in KOA patients.
EA’s regulation of inflammatory responses in KOA is multi-targeted and synergistic. By concurrently inhibiting NF-κB, MAPK, NLRP3, and TLR4/MyD88 pathways while promoting TGF-β and BMP-2-mediated repair, EA addresses both inflammatory symptoms and structural deterioration. These mechanisms explain its efficacy in reducing pain, improving joint function, and modifying disease progression, supporting its use as a complementary strategy for KOA management. Further research should focus on optimizing EA parameters to maximize these anti-inflammatory and pro-reparative effects. Other studies on the regulation of inflammatory responses by EA are shown in Figure 3 and Table 5.
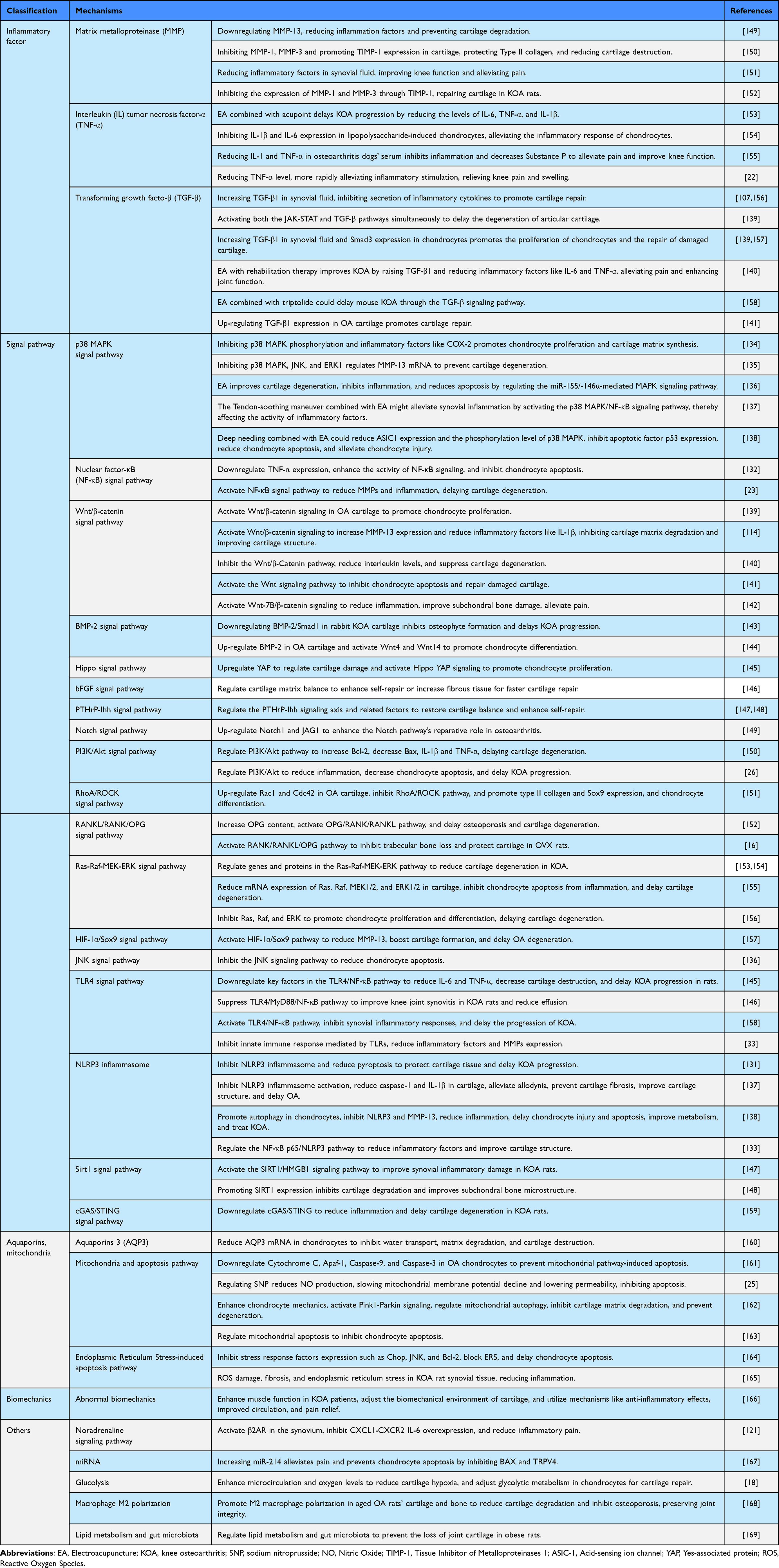 |
Table 5 Related Pathways and Mechanisms of EA Treatment for KOA |
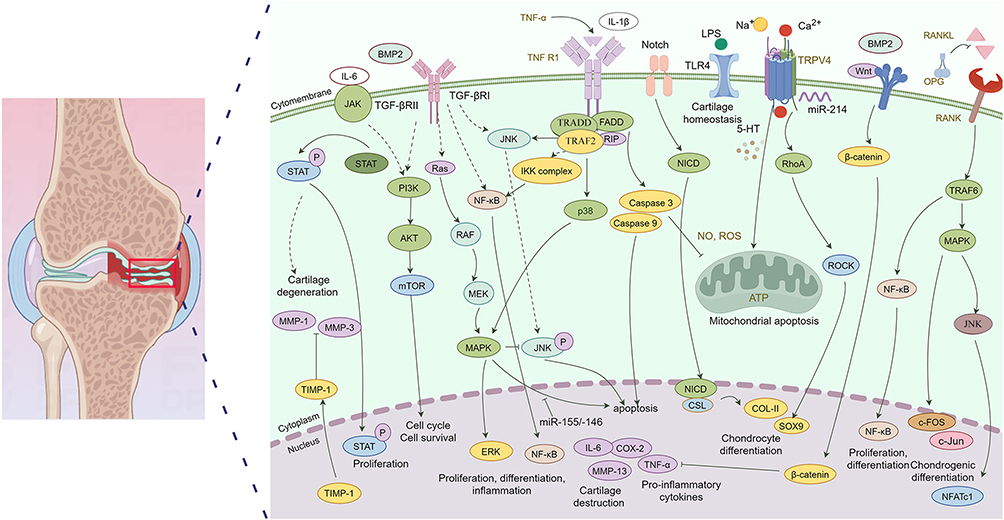 |
Figure 3 Mechanisms of EA in Treating KOA through Inhibition of Inflammatory Responses and Cartilage Repair (By Figdraw). Pro-inflammatory factors such as TNF-α and IL-1β induce inflammatory responses, expression of matrix-degrading enzymes (eg, MMPs), and apoptosis by activating the NF-κB and MAPK pathways (including JNK/p38). In contrast, the BMP2/Wnt pathway promotes chondrogenic differentiation (upregulation of SOX9) via Smad1/5/8 and β-catenin; however, its overactivation can lead to hypertrophy and degeneration. The Notch pathway inhibits differentiation and synergizes with NF-κB to exacerbate inflammation. TGF-β counteracts inflammation through Smad2/3 and promotes matrix synthesis (eg, upregulation of COL-I and TIMP-1) to maintain homeostasis. Additionally, miRNAs (eg, miR-146a exerting anti-inflammatory effects and miR-155 promoting inflammation) and oxidative stress (via ROS/Caspase) further fine-tune this balance. The interplay among these pathways determines chondrocyte fate: an imbalance favoring inflammatory and catabolic signals leads to degeneration, whereas reparative and anabolic signals support homeostasis. These findings suggest that effective therapeutic strategies may require multi-target interventions, such as suppressing NF-κB while enhancing TGF-β/BMP2 signaling. |
Mechanisms of Cartilage Protection
Beyond its potent anti-inflammatory effects, EA plays a crucial role in directly preserving articular cartilage structure and function in KOA. This protection is achieved through multi-faceted mechanisms that promote anabolic metabolism, inhibit catabolic processes, enhance chondrocyte survival, and regulate subchondral bone remodeling. These actions collectively slow cartilage degeneration and contribute to long-term joint integrity, which is fundamental to sustaining clinical efficacy beyond mere symptom relief.
EA actively stimulates pathways responsible for cartilage matrix synthesis and chondrocyte viability. By activating the Wnt/β-catenin signaling pathway in a controlled manner, EA upregulates anabolic factors and transcription factors like SOX9, which are essential for the production of type II collagen and aggrecan.114,141,142 Conversely, it avoids detrimental overactivation of Wnt signaling, which is associated with osteophyte formation. Furthermore, EA enhances the BMP-2/Smad1/5/8 pathway, promoting chondrogenic differentiation and repairing cartilage defects.143,144 Clinically, this translates to improved cartilage morphology on imaging and better scores on joint structure-related evaluation tools, indicating a true disease-modifying potential.
A key mechanism for cartilage preservation is the inhibition of excessive chondrocyte apoptosis. EA modulates several critical anti-apoptotic pathways.161 It activates the PI3K/Akt signaling pathway, leading to increased expression of the anti-apoptotic protein Bcl-2 and decreased expression of the pro-apoptotic protein Bax.26,150 This balance protects chondrocytes from cytokine-induced death. Additionally, EA reduces endoplasmic reticulum (ER) stress and subsequent apoptosis by downregulating markers like GRP78 and CHOP.164,165 By promoting mitochondrial homeostasis and mitigating oxidative stress, EA helps maintain chondrocyte viability, which is crucial for preventing the decline in cellularity that characterizes OA progression. This cytoprotective effect underpins the long-term sustainability of clinical improvements in pain and function.
EA exerts protective effects on the osteochondral unit by modulating bone metabolism. It influences the RANKL/RANK/OPG pathway, a central regulator of osteoclast activity. EA treatment increases the expression of osteoprotegerin (OPG), a decoy receptor for RANKL, thereby inhibiting excessive osteoclastogenesis and preventing subchondral bone resorption.16,152 This helps maintain the mechanical support for overlying cartilage and reduces pathological crosstalk between bone and cartilage. The stabilization of subchondral bone structure is a critical factor in slowing the overall progression of KOA, contributing to preserved joint space and reduced pain during weight-bearing activities.
EA enhances cellular quality control mechanisms by activating autophagy and mitophagy-processes that clear damaged organelles and proteins. Through upregulation of the Pink1-Parkin signaling pathway, EA promotes the clearance of dysfunctional mitochondria, reducing oxidative stress and preventing apoptosis in chondrocytes.162 This is particularly important in the stressed, nutrient-deficient environment of the OA joint. Furthermore, EA-mediated inhibition of the NLRP3 inflammasome is also linked to enhanced autophagy, creating a feedback loop that further suppresses inflammation and cell death.138 By bolstering these innate cellular repair processes, EA helps chondrocytes withstand metabolic and inflammatory insults, thereby preserving tissue integrity and delaying degeneration.
The cartilage-protective mechanisms of EA are comprehensive, targeting anabolic-catabolic imbalance, cell survival, subchondral bone homeostasis, and cellular waste clearance. By synergistically promoting matrix synthesis (via Wnt/β-catenin, BMP-2), inhibiting apoptosis (via PI3K/Akt), regulating bone turnover (via OPG/RANKL/RANK), and enhancing autophagy, EA addresses the fundamental pathophysiology of KOA. These actions underpin its ability to not only alleviate symptoms but also potentially modify disease progression, offering a compelling non-pharmacological strategy for preserving joint structure and function. Future research should focus on standardizing EA protocols that maximize these chondroprotective effects for different stages of KOA. Other mechanisms of cartilage protection regulated by EA are shown in Figure 3 and Table 5.
Clinical Applications and Future Research Directions of EA
Current Status and Limitations of Clinical Applications
As a therapeutic approach that combines traditional acupuncture with modern EA technology, EA has gradually gained recognition in clinical applications in recent years. It is mainly used in pain management, neurological rehabilitation, disease treatment, and other fields. Studies have shown that EA could work by regulating the nervous system, promoting blood circulation, and improving local metabolism. However, there are still some limitations to the clinical application of EA. Firstly, the variability in individual responses to treatment poses challenges for the standardization of EA. Secondly, research on the optimal stimulation parameters (such as frequency, intensity, and duration) of EA is insufficient, and there is a lack of unified clinical guidelines. Additionally, the long-term effects and safety of EA still need further verification, especially in specific populations such as the elderly and patients with chronic diseases. Therefore, although EA shows potential in clinical practice, its application still needs to be continuously improved with the support of scientific research.
Hotspots and Trends in Future Research
The hotspots in future research on EA mainly focus on mechanism exploration, personalized treatment, and new application fields. Firstly, the mechanisms of action of EA still need further research. Recent studies have shown that EA may exert therapeutic effects by regulating neurotransmitters, affecting inflammatory responses, and promoting nerve regeneration, among other pathways.170 Secondly, with the development of precision medicine, personalized EA treatment will become an important trend. Researchers are exploring how to develop personalized EA treatment plans based on the specific conditions of patients (such as pathological types, genetic characteristics, etc.) to improve efficacy.171 Additionally, the application of EA in new fields is also attracting attention, such as in the management of cancer-related symptoms, mental health, and sports injury rehabilitation.172 These research directions will not only promote the scientific development of EA but also provide new treatment options for clinical practice.
In conclusion, the application prospects of EA in treatment of KOA are broad. With further verification of its effectiveness and safety, EA is expected to become an important component of KOA management. Future research should not only continue to explore the efficacy of EA but also pay attention to its combined application with other treatment methods, aiming to provide more comprehensive treatment plans for KOA patients through multidisciplinary integration.
Abbreviations
5-HT, 5-Hydroxytryptamine; AKT, Protein Kinase B; APC, Anaphase-Promoting Complex; ATP, Adenosine Triphosphate; BAD, BCL2-Associated Agonist of Cell Death; BMP2, Bone Morphogenetic Protein 2; C-FOS, FBJ Osteosarcoma Oncogene; Caspase-3, Cysteine-ASPartic protease-3; Caspase-9, Cysteine-ASPartic protease-9; c-Jun, v- jun avian sarcoma virus 16 oncogene homolog; COL-I, Collagen Type I; COX-2, cyclooxygenase – 2; CSL, CBF1/Suppressor of Hairless/LAG-1; ERK, Extracellular signal-Regulated Kinase; FADD, Fas-Associated Death Domain; GSK-3β, Glycogen Synthase Kinase-3 beta; HES/HEY, Hairy and Enhancer of Split/HES-related with YRPW motif, IKK complex, Inhibitor of NF-κB Kinase complex; IL-1β, Interleukin-1 beta; IL-6, Interleukin-6; IRAK, Interleukin-1 Receptor-Associated Kinase; JAK, Janus Kinase; JNK, c-Jun N-terminal Kinase; LRP, LDL-Receptor-related Protein; MAPK, Mitogen-Activated Protein Kinase; MEK, MAPK/ERK Kinase; MMP-1, Matrix Metalloproteinase-1; MMP-3, Matrix Metalloproteinase-3; MMP-13, Matrix Metalloproteinase-13; mTOR, mechanistic Target Of Rapamyc; MyD88, Myeloid Differentiation primary response 88; NF-κB, Nuclear Factor - kappa B; NFATc1, Nuclear Factor of Activated T-cells, cytoplasmic 1; NICD, Notch IntraCellular Domain; NO, Nitric Oxide; OPG, Osteoprotegerin; PI3K, Phosphatidylinositol 3-Kinase; PTEN, Phosphatase and Tensin Homolog; QcOx-2, Quiescin sulfhydryl oxidase 2; RANK, Receptor Activator of Nuclear factor κB; RANKL, Receptor Activator of Nuclear factor κB Ligand; RhoA, Ras Homolog gene family, member A; RIP, Receptor-Interacting Protein; ROCK, Rho-associated Coiled-coil-containing protein Kinase; ROS, Reactive Oxygen Species; SOCS1, Suppressor Of Cytokine Signaling 1; SOX9, SRY-Box Transcription Factor 9; STAT, Signal Transducer and Activator of Transcription; TGF-β1, Transforming Growth Factor-beta 1; TGF-βRI, Transforming Growth Factor-beta Receptor I; TGF-βRII, Transforming Growth Factor-beta Receptor II; TIMP-1, Tissue Inhibitor of Metalloproteinases-1; TLR4, Toll-Like Receptor 4; TNF-α, Tumor Necrosis Factor-alpha; TNF-R1, Tumor Necrosis Factor Receptor 1; TRADD, TNFRSF1A-Associated via Death Domain; TRAF2, TNF Receptor-Associated Factor 2; TRAF6, TNF Receptor-Associated Factor 6; TRPV4, Transient Receptor Potential Vanilloid 4; Wnt, Wingless-type; MMTV integration site family.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Development of this review was supported by Wuhu City Science and Technology Program Project (2024kj094) and National Key Specialty in Geriatrics with Competitive Advantage (Approval No. 90, 2024, NATCM).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Darlow B, Belton J, Brown M, et al. Making sense of osteoarthritis: a narrative review. Osteoarthritis Cartilage. 2025;33(1):17–26. doi:10.1016/j.joca.2024.09.012
2. Steinmetz JD, Culbreth GT, Haile LM, GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990-2020 and projections to 2050: a systematic analysis for the global burden of disease study 2021. Lancet Rheumatol. 2023;5(9):e508–e522. doi:10.1016/S2665-9913(23)00163-7
3. Primorac D, Molnar V, Rod E, et al. Knee osteoarthritis:a review of pathogenesis and state-of-the-art non-operative therapeutic considerations. Genes. 2020;11(8):854. doi:10.3390/genes11080854
4. Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. 2019;393(10182):1745–1759. doi:10.1016/S0140-6736(19)30417-9
5. Tong L, Yu H, Huang X, et al. Current understanding of osteoarthritis pathogenesis and relevant new approaches. Bone Res. 2022;10(1):60. doi:10.1038/s41413-022-00226-9
6. Tang S, Zhang C, Oo WM, et al. Osteoarthritis. Nat Rev Dis Primers. 2025;11(1):10. doi:10.1038/s41572-025-00594-6
7. Sun L, Wang Y, Kan T, et al. Elevated expression of Piezo1 activates the cGAS-STING pathway in chondrocytes by releasing mitochondrial DNA. Osteoarthritis Cartilage. 2025;33(5):601–615. doi:10.1016/j.joca.2025.02.778
8. Wei J, Yang X, Ge X, et al. Therapeutic effects of fire needling acupuncture on pain relief and cartilage protection in MIA-Induced knee osteoarthritis rats: the role of macrophage polarization in synovium and angiogenesis in subchondral bone. J Inflamm Res. 2025;18:7459–7475. doi:10.2147/JIR.S518829
9. Zhao C, Kong K, Liu P, et al. Regulating obesity-induced osteoarthritis by targeting p53-FOXO3, osteoclast ferroptosis, and mesenchymal stem cell adipogenesis. Nat Commun. 2025;16(1):4532. doi:10.1038/s41467-025-59883-z
10. Ziemian SN, Witkowski AM, Wright TM, et al. Early inhibition of subchondral bone remodeling slows load-induced posttraumatic osteoarthritis development in mice. J Bone Miner Res. 2021;36(10):2027–2038. doi:10.1002/jbmr.4397
11. Liu W, Guo NY, Wang JQ, et al. Osteoarthritis: mechanisms and therapeutic advances. MedComm. 2025;6(8):e70290. doi:10.1002/mco2.70290
12. Bliddal H, Bays H, Czernichow S, et al. Once-Weekly semaglutide in persons with obesity and knee osteoarthritis. N Engl J Med. 2024;391(17):1573–1583. doi:10.1056/NEJMoa2403664
13. Atik I, Gul E, Atik S. Evaluation of the relationship between knee osteoarthritis and meniscus pathologies. Malawi Med J. 2024;36(1):48–52. doi:10.4314/mmj.v36i1.8
14. Xu F. Li BP.Therapeutic efficacy of ozone injection into the knee for the osteoarthritis patient along with oral celecoxib and glucosamine. J Clin Diagn Res. 2017;11(9):UC01–UC03.
15. Eaton CB, Sayeed M, Ameernaz S. Sex differences in the association of skin advanced glycation endproducts with knee osteoarthritis progression. Ar Thritis Res Ther. 2017;19(1):36. doi:10.1186/s13075-017-1226-z
16. Deyle GD, Allen CS, Allison SC, et al. Physical therapy versus glucocorticoid injection for osteoarthritis of the knee. N Engl J Med. 2020;382(15):1420–1429. doi:10.1056/NEJMoa1905877
17. Li XB, Gao F, Zhao W. Effect of different electroacupuncture intensities on chronic pain in patients with knee osteoarthritis. Shanghai J Acu-Mox. 2023;42(07):730–736.
18. Ma WW, Du M, Lu J, et al. Electroacupuncture improves articular microcirculation and attenuates cartilage hypoxia in a male rabbit model of knee osteoarthritis. J Tradit Complement Med. 2024;14(4):414–423. doi:10.1016/j.jtcme.2024.01.002
19. Ma J, Chu XY, Liu HS, et al. Effect of acupotomy combined with electroacupuncture on knee function of patients with knee osteoarthritis. Acupuncture Res. 2024;49(4):398–402. doi:10.13702/j.1000-0607.20230087
20. Lin F, Xiang L, Wu L, et al. Positioning regulation of organelle network via Chinese microneedle. Sci Adv. 2024;10(16):eadl3063. doi:10.1126/sciadv.adl3063
21. Zhou J, Zhong PR, Liao Y, et al. Electroacupuncture ameliorates subchondral bone deterioration and inhibits cartilage degeneration in ovariectomised rats. Acupunct Med. 2018;36(1):37–43. doi:10.1136/acupmed-2016-011258
22. Shi GX, Tu JF, Wang Q, et al. Effect of electro-acupuncture(EA)and manual acupuncture(MA)on markers of inflammation in knee osteoarthritis. J Pain Res. 2020;13:2171–2179. doi:10.2147/JPR.S256950
23. Wu GW, Chen J, Huang YM, et al. Electroacupuncture delays cartilage degeneration by modulating nuclear factor-κB signaling pathway. Chin J Integr Med. 2019;25(9):677–683. doi:10.1007/s11655-018-2916-8
24. Gomes A, Silva DA, Rodrigues CMP, et al. The emerging role of micro RNAs in aquaporin regulation. Front Chem. 2018;6:238. doi:10.3389/fchem.2018.00238
25. Lin J, Wu GW, Chen J, et al. Electroacupuncture inhibits sodium nitroprusside-mediated chondrocyte apoptosis through the mitochondrial pathway. Mol Med Rep. 2018;18(6):4922–4930. doi:10.3892/mmr.2018.9498
26. Shi XW, Yu WJ, Wang T, et al. Electroacupuncture alleviates cartilage degradation:improvement in cartilage biomechanics via pain relief and potentiation of muscle function in a rabbit model of knee osteoarthritis. Biomed Pharmacother. 2020;123:109724. doi:10.1016/j.biopha.2019.109724
27. Fan JJ, Yuan PW, Zheng J, et al. Study on mechanism of electroacupuncture therapy for chronicpain in knee osteoarthritis based on MAPK signaling pathway mediated by spinalcannabinoid receptor CB2.Chinese. J Immunol. 2021;37(13):1582–1586.
28. Yuan XC, Wang YY, Tian LX, et al. Spinal 5-HT2A receptor is involved in electroacupuncture inhibition of chronic pain. Mol Pain. 2022;18:1–12.
29. Guo JM, Xiao Y, Cai TY, et al. Chinese medicine involving triple rehabilitation therapy for knee osteoarthritis in 696 outpatients: a multi-center, randomized controlled trial. Chin J Integr Med. 2021;27(10):729–736. doi:10.1007/s11655-021-3488-6
30. Zhang Q, Zhou M, Huo M, et al. Mechanisms of acupuncture-electroacupuncture on inflammatory pain. Mol Pain. 2023;19:17448069231202882. doi:10.1177/17448069231202882
31. Li PQ, Dang SJ, Li FL, et al. World federation of acupuncture-moxibustion societies (WFAS) technical benchmark of acupuncture and moxibustion: eelectroacupuncture. WJAM. 2024;34:227–230.
32. Wei YY, Xi Q, Guo Y. Review on the development and application of electroacupuncture apparatus in the past 5 years in China. J Acupunct Tuina Sci. 2019;17(4):284–288. doi:10.1007/s11726-019-1120-0
33. Ruan A, Wang Q, Ma Y, et al. Efficacy and mechanism of electroacupuncture treatment of rabbits with different degrees of knee osteoarthritis: a study based on synovial innate immune response. Front Physiol. 2021;12:642178. doi:10.3389/fphys.2021.642178
34. Li LT. Difference of therapeutic effect between electroacupuncture and warm acupuncture in patients with knee osteoarthritis due to blood stasis. Guide Chin Med. 2023;21:142–144.
35. Liu Y, Wu H. Effect of electroacupuncture on knee osteoarthritis and relevant inflammatory factors:A randomized clinical trial. WJAM. 2022;32:329–335.
36. Zhou WC. Clinical comparative study of electro-acupuncture and acupuncture debate temperature on kidney Marrow deficiency syndrome of knee osteoarthritis. J Emergency Traditional Chin Med. 2014;23:1521–1523.
37. Lu JJ, Ouyang BS. Comparison of clinical effects between electroacupuncture and warm needling moxibustion in treating Knee Osteoarthritis of blood stasis obstruction pattern. Western J Tradit Chin Med. 2014;27:119–121.
38. Ouyang BS, Gao J, Yang HZ, et al. Comparison of the clinical efficacy of warm acupuncture and electroacupuncture in the treatment of knee osteoarthritis of Yang deficiency and cold coagulation type. Chin J Rehabil Med. 2011;26:255–257.
39. Plaster R, Vieira WB, Alencar FAD, et al. Immediate effects of electroacupuncture and manual acupuncture on pain, mobility and muscle strength in patients with knee osteoarthritis: a randomised controlled trial. Acupunct Med. 2014;32(3):236–241. doi:10.1136/acupmed-2013-010489
40. Ho TJ, Lin CF, Chen JK, et al. Electroacupuncture attenuates inflammatory pain via peripheral cannabinoid receptor type 1 signaling pathway in mice. PLoS One. 2023;18(12):e0295432. doi:10.1371/journal.pone.0295432
41. Tu JF, Yang JW, Shi GX, et al. Efficacy of intensive acupuncture versus sham acupuncture in knee osteoarthritis: a randomized controlled trial. Arthritis Rheuma. 2021;73(3):448–458. doi:10.1002/art.41584
42. Li YJ, Liang XS, Fang XX, et al. A comparative study of electroacupuncture therapy versus needle-warming moxibustion therapy for treatment of early-and mid-stage knee osteoarthritis. J Trad Chin Orthop Trauma. 2023;35:12–16.
43. Zhang LL, Yuan HX. Effectiveness and clinical benefit of a therapy of combined non-pharmaceutical traditional Chinese medicine for knee osteoarthritis: a randomized controlled study. J Tradit Chin Med. 2020;40(3):447–454. doi:10.19852/j.cnki.jtcm.2020.03.013
44. Elisabet SV, Carina KS, Kerstin J. Comparison between electro-acupuncture and hydrotherapy, both in combination with patient education and patient education alone, on the symptomatic treatment of osteoarthritis of the Hip. Clin J Pain. 2004;20(179):185.
45. Zhang YX. Clinic effect comparison of electroacupuncture and moxibustion for knee osteoarthritis of kidney and marrow deficiency. Med Recapitulate. 2013;19:1903–1905.
46. Gao J, Ouyang BS, Zhang Y, et al. Comparison of the clinical therapeutic effects between electroacupuncture and warming needle moxibustion for knee osteoarthritis of kidney deficiency and marrow insufficiency pattern/syndrome. Chin Acupunc Moxibustion. 2012;32:395–398.
47. Hu WL, Xie B, Tan J. Combination therapy of electroacupuncture with acupoint-to-acupoint penetration needling and Mulligan mobilization with movement for mild-to-moderate knee osteoarthritis:A randomized controlled study. J Hunan Univ Chin Med. 2023;43:1486–1491.
48. Liu SF, Chen QD, Zhang QG, et al. Electroacupuncture combined with extracorporeal shock wave therapy improves pain symptoms and inflammatory factor levels in knee osteoarthritis patients. Heliyon. 2023;9(10):e20771. doi:10.1016/j.heliyon.2023.e20771
49. Wang TQ, Li YT, Wang LQ, et al. Electroacupuncture versus manual acupuncture for knee osteoarthritis: a randomized controlled pilot trial. Acupunc Med. 2020;38(5):291–300. doi:10.1177/0964528419900781
50. Deng CH, Deng WJ. Comparison of the efficacy of electroacupuncture and warm acupuncture in the treatment of knee osteoarthritis with kidney deficiency and marrow deficiency. China Prac Med. 2020;15:171–173.
51. Qian W. Comparative analysis of the efficacy of electroacupuncture and warm acupuncture in the treatment of knee osteoarthritis due to kidney deficiency and marrow deficiency. J Integ Trad Chin West Med Cardiovasc Dis. 2016;4:161–164.
52. Li YX, Liu D, Fang ZY, et al. Data mining of acupoint spectrum and stimulation parameters in electro-acupuncture treatment of knee osteoarthritis. Chin Med Herald. 2023;20:17–22.
53. Dai QP, Qiu ML, Yuan XJ, et al. Clinical observation of different electro-acupuncture frequency for knee osteoarthritis. Prog Mod Biomed. 2011;11:3655–3657.
54. Samuel SR, Maiya GA. Application of low frequency and medium frequency currents in the management of acute and chronic pain-a narrative review. Indian J Palliat Care. 2015;21(1):116–120. doi:10.4103/0973-1075.150203
55. Tian W, Shen LL, Huang GF, et al. Clinical study on improving WOMAC and VAS scores of patients with knee arthritis of different courses by electroacupuncture. Clin Acupunct Moxibust. 2015;31:26–28.
56. Kim JH, Min BI, Na HS, et al. Relieving effects of electroacupuncture on mechanical allodynia in neuropathic pain model of inferior caudal trunk injury in rat: mediation by spinal opioid receptors. Brain Res. 2004;998(2):230–236. doi:10.1016/j.brainres.2003.11.045
57. Zhao Y, Li ZH, Wu H, et al. Optimal scheme of electroacupuncture instrument for the treatment of knee osteoarthritis based on artificial intelligence. Technol Innovation Application. 2023;13:41–44.
58. Shen LL, Huang GF, Ian W T, et al. Electroacupuncture inhibits chronification of the acute pain of knee osteoarthritis: study protocol for a randomized controlled trial. Trials. 2015;16(1):131. doi:10.1186/s13063-015-0636-y
59. Lv ZT, Shen LL, Zhu B, et al. Effects of intensity of electroacupuncture on chronic pain in patients with knee osteoarthritis: a randomized controlled trial. Arthritis Res Ther. 2019;21(1):120. doi:10.1186/s13075-019-1899-6
60. Li Q, Tang YG, Yong Y, et al. Comparing the effectiveness of electroacupuncture with different grades of knee osteoarthritis: a prospective study. Cell Physiol Biochem. 2016;39(6):2331–2340. doi:10.1159/000447925
61. Zhou LY, Qu B, Zhang J, et al. A study on effects of electroacupuncture treatment on lower limb muscle strength in elderly patients with knee osteoarthritis based on isokinetic muscle strength test. Geriatrics Health Care. 2024;30:840–845.
62. Xue K, Wu J, Bao J, et al. Clinical study of electroacupuncture combined with exercise therapy in improving the balance function of patients with knee osteoarthritis. J Acupunct Tuina Sci. 2024;22(1):32–40. doi:10.1007/s11726-024-1420-x
63. Wu MX, Li XH, Lin MN, et al. Clinical study on the treatment of knee osteoarthritis of Shen-Sui insufficiency syndrome type by electroacupuncture. Chin J Integr Med. 2010;16(4):291–297. doi:10.1007/s11655-010-0513-1
64. Gang JH, Mi YQ, Wang HM. Clinical efficacy comparison between electroacupuncture and meloxicam in the treatment of knee osteoarthritis at the early and middle stage: a randomized controlled trial. Acupuncture Res. 2016;36:467–470.
65. Jiao QR, Ding MQ, Man L, et al. Efficacy of electroacupuncture in treatment of knee arthritis and its effect on levels of IL-10 and TNF-α in serum. Liaoning J Tradit Chin Med. 2018;45:2186–2188.
66. Huang J, Yang LW. Clinical observation of Electro-acupuncture combined with oral glucosamine hydrochloride capsules for the treatment of knee osteoarthritis. West Chin Med J. 2014;29:30–33.
67. Yang CX. Clinical study on warm acupuncture combined with electroacupuncture in the treatment of knee osteoarthritis due to liver and kidney deficiency. J Basic Chin Med. 2014;20:1550–1551.
68. Guo CQ, Si T, Wen JM, et al. Effects of acupotomy therapy on the pain symptoms in patients with knee osteoarthritis:a randomized controlled clinical trial. Tianjin J Traditional Chin Med. 2012;29:35–38.
69. Song HY, Wang K. Clinical research on osteoarthritis treated by herbs-partition moxibusition combined with ultrashort wave. Henan Traditional Chin Med. 2016;36:888–889.
70. Hu SR, Yin LH, Li WY. Clinical study on acupotomy improving symptoms of knee osteoarthritis. Jiangxi Med J. 2009;44:1093–1095.
71. Huang JJ, Su CH, Fang JF, et al. A clinical study on treating the Shibi type of knee-osteoarthritis by eletroacupunture and warm needling at 10 special acupoints. Clin J Chinese Med. 2016;8:43–45.
72. Huang P, Zeng J. Clinical study of thermal moxibustion combined with traditional chinese medicine ion-introduction for knee osteoarthritis. Clin Acupunct Moxibust. 2013;29:17–19.
73. Li SF, Lin ZP, Lu P, et al.Clinical research on treating knee osteoarthritis by small knife acupuncture. Clin J Chinese Med. 2015;7:39–40.
74. Ding Y, Wang YX, Shi X, et al. Effect of ultrasound-guided acupotomy vs electro-acupuncture on knee osteoarthritis:a randomized controlled study. J Traditional Chin Med. 2016;36(4):444–449. doi:10.1016/S0254-6272(16)30060-7
75. Tzeng CY, Chang SL, Wu CC, et al. Single-blinded, randomised preliminary study evaluating the effects of 2 Hz electroacupuncture for postoperative pain in patients with total knee arthroplasty. Acupunct Med. 2015;33(4):284. doi:10.1136/acupmed-2014-010722
76. Weiner DK, Moore CG, Morone NE, et al. Efficacy of periosteal stimulation for chronic pain associated with advanced knee osteoarthritis: a randomized, controlled clinical trial. Clin Ther. 2013;35(11):1703–1720. doi:10.1016/j.clinthera.2013.09.025
77. Zhu Y, Chen RL, Miao FR, et al. Clinical observation on the therapeutic effect of drugs-paste separated moxibustion combined with electroacupunture for knee osteoarthritis patients of cold-damp type. Acupuncture Res. 2010;35(4):293–297.
78. Suarez-Almazor ME, Looney C, Liu Y, et al. A randomized controlled trial of acupuncture for osteoarthritis of the knee: effects of patient-provider communication. Arthritis Care Res. 2010;62(9):1229–1236. doi:10.1002/acr.20225
79. Ahsin S, Saleem S, Bhatti AM, et al. Clinical and endocrinological changes after electro-acupuncture treatment in patients with osteoarthritis of the knee. Pain. 2009;147(1):60–66. doi:10.1016/j.pain.2009.08.004
80. Taechaarpornkul W, Suvapan D, Theppanom C, et al. Comparison of the effectiveness of six and two acupuncture point regimens in osteoarthritis of the knee: a randomised trial. Acupunct Med. 2009;27(1):3–8. doi:10.1136/aim.2008.000067
81. Wu ZH, Bao F. Observation on therapeutic effects of electroacupuncture for the treatment of knee osteoarthritis. Chin J Orthop Trauma. 2008;21(3):170–172.
82. Zhou T, Chen CF, Qian YL, et al. Clinical analysis of low-frequency electro-acupuncture for knee osteoarthritis. Shanghai J Traditional Chin Med. 2015;49:56–57.
83. Wei W, Wang JJ. Clinical observation on the treatment of knee osteoarthritis with mild moxibustion combined with electroacupuncture. Res Integrated Tradit Chin Western Med. 2024;16:92–95.
84. Wang XZ, Wang RK, Liu Q, et al. Electroacupuncture versus exercise in patients with knee osteoarthritis: study protocol for a randomized controlled trial. PLoS One. 2024;19(6):e0305105–e0305105. doi:10.1371/journal.pone.0305105
85. Zhou LL, Yi LC, Wu YJ, et al. Electroacupuncture versus exercise in patients with knee osteoarthritis: study protocol for a randomized controlled trial. Chinese Foreign Med Res. 2023;21:166–169.
86. Chen Y, Jia YJ, Lu JH, et al. Comparision of therapertic effect of different acupuncture methods for knee osteoarthritis. Acupunct Res. 2020;45:569–573.
87. Liang YF, Li WX, Ma Y, et al. Comparison of therapeutic effect of soft-tissue relaxing needling and electroacupuncture for knee osteoarthritis. Acupunct Res. 2019;44:439–442.
88. Cohen E, Lee YC. A mechanism-based approach to the management of osteoarthritis pain. Curr Osteoporos Rep. 2015;13(6):399–406. doi:10.1007/s11914-015-0291-y
89. Zhao Y, Wang X, Zhang D. A Retrospective study on the efficacy of two different rehabilitation interventions on KOA: shock wave therapy vs. Biomed Res Int. 2024;2024:9831817.
90. Malfait AM, Miller RE, Miller RJ. Basic mechanisms of pain in osteoarthritis: experimental observations and new perspectives. Rheum Dis Clin N Am. 2021;47(2):165–180. doi:10.1016/j.rdc.2020.12.002
91. Iyengar S, Ossipov MH, Johnson KW. The role of calcitonin gene-related peptide in peripheral and central pain mechanisms including migraine. Pain. 2017;158(4):543–559. doi:10.1097/j.pain.0000000000000831
92. Miller RE, Tran PB, Das R, et al. CCR2 chemokine receptor signaling mediates pain in experimental osteoarthritis. Proc Natl Acad Sci USA. 2012;109(50):20602–20607. doi:10.1073/pnas.1209294110
93. Kapoor M, Martel-Pelletier J, Lajeunesse D, et al. Role of proinflammatory cytokines in the pathophysiology of osteoarthritis. Nat Rev Rheumatol. 2011;7(1):33–42. doi:10.1038/nrrheum.2010.196
94. Zhou YQ, Tian XB, Tian YK, et al. Wnt signaling: a prospective therapeutic target for chronic pain. Pharmacol Ther. 2022;231:107984. doi:10.1016/j.pharmthera.2021.107984
95. Swanson KV, Deng M, Ting JP. The NLRP3 inflammasome: molecular activation and regulation to therapeutics. Nat Rev Immunol. 2019;19(8):477–489. doi:10.1038/s41577-019-0165-0
96. Manheimer E, Cheng K, Linde K, et al. Acupuncture for peripheral joint osteoarthritis. Cochrane Database Syst Rev. 2010;1:CD001977.
97. Liu SB, Wang ZF, Su YS, et al. Somatotopic organization and intensity dependence in driving distinct NPY-Expressing sympathetic pathways by electroacupuncture. Neuron. 2020;108(3):436–450.e7. doi:10.1016/j.neuron.2020.07.015
98. Cao Y, Tang S, Nie X, et al. Decreased miR-214-3p activates NF-kappaB pathway and aggravates osteoarthritis progression. EBioMedicine. 2021;65:103283. doi:10.1016/j.ebiom.2021.103283
99. Wang Q, Lv H, Sun ZT, et al. Effect of electroacupuncture versus sham electroacupuncture in patients with knee osteoarthritis: a pilot randomized controlled trial. Evid Based Complement Alternat Med. 2020;2020(1):1686952. doi:10.1155/2020/1686952
100. Mou J, Wang Q, Wu J, et al. The effect of Fu’s subcutaneous needling in treating knee osteoarthritis patients: a randomized controlled trial. Explore. 2024;20(4):562–571. doi:10.1016/j.explore.2023.12.015
101. Cai FH, Li FL, Zhang YC, et al. Research on electroacupuncture parameters for knee osteoarthritis based on data mining. Eur J Med Res. 2022;27(1):162. doi:10.1186/s40001-022-00795-9
102. Boer CG, Radjabzadeh D, Medina-Gomez C, et al. Intestinal microbiome composition and its relation to joint pain and inflammation. Nat Commun. 2019;10(1):4881. doi:10.1038/s41467-019-12873-4
103. Hawker GA, Mian S, Kendzerska T, et al. High correlation of VAS pain scores after 2 and 6 weeks of treatment with VAS pain scores at 12 weeks in randomised controlled trials in rheumatoid arthritis and osteoarthritis: meta-analysis and implications. Arthritis Res Ther. 2016;18(1):73. doi:10.1186/s13075-016-0972-7
104. Wang F, Liu G, Shi J, et al. Effects of glucosamine hydrochloride combined with non-steroidal anti-inflammatory drugs on symptoms and HSS scores in patients with knee osteoarthritis. Pak J Pharm Sci. 2023;36(3 Special):921–925.
105. Du P, Yan Y, Yin S, et al. Correlation between coronal position sequence of lumbar and WOMAC score in Knee Osteoarthritis (KOA) in standard standing position. Adv Ther. 2024;41(7):2924–2935. doi:10.1007/s12325-024-02898-7
106. Webster KE, Feller JA. Comparison of the short form-12 (SF-12) health status questionnaire with the SF-36 in patients with knee osteoarthritis who have replacement surgery. Knee Surg Sports Traumatol Arthrosc. 2016;24(8):2620–2626. doi:10.1007/s00167-015-3904-1
107. Huang DE, Qin Y, Lin MN, et al. Clinical efficacy of different waves of electroacupuncture on knee osteoarthritis and its effect on TGF-β1 in joint fluid. Chin Acupunc Moxibustion. 2020;40:370–374.
108. Javier M, Sandra C, Pilar S, et al. Electro-acupuncture for treatment of knee pain from osteoarthritis and the possible endocrinology changes: a study protocol for a randomized controlled trial. Trials. 2015;16(1):248. doi:10.1186/s13063-015-0766-2
109. Yin Y, Zhao Y. Case controll study on the synergistic effects of electroacupuncture on knee osteoarthritis after arthroscopic debrideMent. China J Orthop Trauma. 2014;27:287–290.
110. Oh B, Kimble B, Costa DSJ, et al. Acupuncture for treatment of arthralgia secondary to aromatase inhibitor therapy in women with early breast cancer: pilot study. Acupunct Med. 2013;31(3):264–271. doi:10.1136/acupmed-2012-010309
111. Lu TW, Wei IP, Liu YH, et al. Immediate effects of acupuncture on gait patterns in patients with knee osteoarthritis. Chin Med J. 2010;123(2):165–172.
112. Xu FY, Gan JH, Li WP, et al. Effect of electroacupuncture on the level of IL-1β and TNF-α in patients with osteoarthritis. Chin Acupuncture Moxibustion. 2009;29(7):529–531.
113. Ronald WJ, Emad ST, Peter WJ, et al. A blinded randomised trial of acupuncture (manual and electroacupuncture) compared with a non-penetrating sham for the symptoms of osteoarthritis of the knee. Acupunct Med. 2008;26(2):69–78. doi:10.1136/aim.26.2.69
114. Zhang YY, Li XH, Wu MX. Effect of electroacupuncture at Wnt/β-catenin signaling pathway on inhibiting cartilage degeneration in rats with knee osteoarthritis. Chin Acupuncture Moxibustion. 2019;39:1081–1086.
115. Shi XW, Yu WJ, Zhang W, et al. A comparison of the effects of electroacupuncture versus transcutaneous electrical nerve stimulation for pain control in knee osteoarthritis: a Bayesian network meta-analysis of randomized controlled trials. Acupunct Med. 2021;39(3):163–174. doi:10.1177/0964528420921193
116. Arendt-Nielsen L, Nie H, Laursen MB, et al. Sensitization in patients with painful knee osteoarthritis. Pain. 2010;149(3):573–581. doi:10.1016/j.pain.2010.04.003
117. Gao N, Shi H, Hu S, et al. Acupuncture enhances dorsal raphe functional connectivity in knee osteoarthritis with chronic pain. Front Neurol. 2021;12:813723. doi:10.3389/fneur.2021.813723
118. Chen XH, Han JS. Analgesia induced by electroacupuncture of different frequencies is mediated by different types of opioid receptors: another cross-tolerance study. Behav Brain Res. 1992;47(2):143–149. doi:10.1016/S0166-4328(05)80120-2
119. Dong R, Yu B, Chen L, et al. The 5-HT(2A) receptor potassium-chloride cotransporter 2 signaling pathway in a rat incision pain model. Exp Ther Med. 2016;12(6):3583–3588. doi:10.3892/etm.2016.3807
120. Seo BK, Sung WS, Park YC, et al. The electroacupuncture-induced analgesic effect mediated by 5-HT1, 5-HT3 receptor and muscarinic cholinergic receptors in rat model of collagenase-induced osteoarthritis. BMC Complement Altern Med. 2016;16(1):212. doi:10.1186/s12906-016-1204-z
121. Chen W, Zhang XN, Su YS, et al. Electroacupuncture activated local sympathetic noradrenergic signaling to relieve synovitis and referred pain behaviors in knee osteoarthritis rats. Front Mol Neurosci. 2023;16:1069965. doi:10.3389/fnmol.2023.1069965
122. Zheng XH, Lin J, Wang ZZ, et al. Research of the analgesic effects and central nervous system impact of electroacupuncture therapy in rats with knee osteoarthritis. Heliyon. 2024; 10:e21825.
123. Li Y, Zhang YH, Shen LY, et al. Effect of electroacupuncture stimulation in the innervation zone on knee function score in elderly patients with knee osteoarthritis. Geriatrics Health Care. 2023;29:794–797.
124. Chen W, Li HC, Wan HY, et al. Effect of electroacupuncture on spontaneous pain during the synovial inflammatory response stage and allodynia at the later stage in rats with knee osteoarthritis. Chin Acupunc Moxibustion. 2022;42:1385–1393.
125. Ji B, Guo CQ, Jin Y, et al. Effects of acupotome and electro-acupuncture on pain threshold and monoamine-neurotransmitters of central nerves in rats with knee osteoarthritis. Chin J Pathophysiol. 2010;26:1091–1095.
126. Carlos RM, María BA, Vanesa AP, et al. Current advances and novel research on minimal invasive techniques for musculoskeletal disorders. Disease-a-Month. 2021;67(10):101210. doi:10.1016/j.disamonth.2021.101210
127. Jan MB, Mark IJ, Rodrigo ABLM, et al. Short-term efficacy of physical interventions in osteoarthritic knee pain. A systematic review and meta-analysis of randomised placebo-controlled trials. BMC Musculoskelet Disord. 2007;8(1):51. doi:10.1186/1471-2474-8-51
128. Kathleen AS, Deirdre W. Transcutaneous electrical nerve stimulation: basic science mechanisms and clinical effectiveness. J Pain. 2003;4(3):109–121. doi:10.1054/jpai.2003.434
129. Yang KW, Yuan PW, Dong B, et al. Effects of electroacupuncture on pain behavior and pain-related factors in spinal cord dorsal horn and dorsal root ganglia of rats with knee osteoarthritis. Acupunct Res. 2020;45:818–822.
130. Chen H, Yang M. Electroacupuncture regulates pain and its effect on IL-17 and IL-17R expression of spinal cord in New Zealand rabbit with osteoarthritis. Chongqing Med J. 2017;46:2326–2329.
131. Zhang W, Zhang L, Yang S, et al. Electroacupuncture ameliorates knee osteoarthritis in rats via inhibiting NLRP3 inflammasome and reducing pyroptosis. Mol Pain. 2023;19:17448069221147792. doi:10.1177/17448069221147792
132. Wang K, Wu H, Chi M, et al. Electroacupuncture inhibits apoptosis of splenic lymphocytes in traumatized rats through modulation of the TNF-α/NF-κB signaling pathway. Mol Med Rep. 2015;11(1):237–241. doi:10.3892/mmr.2014.2740
133. Zhang XQ, Qing L, Xue P, et al. Effects of different acupuncture and moxibustion methods on articular cartilage morphology and NF-κB p65/NLRP3 pathway in rats with knee osteoarthritis. Acupunct Res. 2023;48:185–191.
134. Wang SJ, Fang JQ, Ma J, et al. Influence of electroacupuncture on p38-mitogen activated protein kinase in substantia nigra cells of rats with Parkinson disease model. Chin Acupuncture Moxibustion. 2013;33:329–333.
135. Liao Y, Li XH, Li N, et al. Electroacupuncture protects against articular cartilage erosion by inhibiting mitogen-activated protein kinases in a rat model of osteoarthritis. Acupunct Med. 2016;34(4):290–295. doi:10.1136/acupmed-2015-010949
136. Lin J, Wu GW, Fu CL, et al. Effect of serum of the rats after electroacupuncture on the gene expression of apoptotic chondrocyte C-Myc, C-Fos and C-Jun induced by tumor necrosis factor α. Fujian J Trad Chinese Med. 2018;49:20–23.
137. Wang ZK, Chen M, Wang B, et al. Electroacupuncture alleviates osteoarthritis by suppressing NLRP3 inflammasome activation in guinea pigs. Evid Based Complement Alternat Med. 2020;2020(1):5476064. doi:10.1155/2020/5476064
138. Yuke Z, Bo D, Rui C, et al. To investigate the mechanism of electroacupuncture in the treatment of knee osteoarthritis in rats based on the autophagy -Nlrp3 signaling pathway of chondrocytes. Osteoarthritis Cartilage. 2022; 30:S317–S318.
139. Wu MX, Li XH, Li L, et al. Effect of electroacupuncture on JAK-STAT signal transduction pathway in chondrocyte of osteoarthritis rats. Rehab Med. 2011;21:21–23.
140. Lin FX. Effect of electroacupuncture combined with comprehensive rehabilitation on pain, joint function and TGF-β1 level of joint fluid in patients with knee osteoarthritis. J Clin Pathol Res. 2022;42:917–923.
141. Bao F, Wang DH, Wang FQ, et al. Effect of electro-acupuncture on expression of transforming growth factor-β1in the cartilage of experimental rats with knee osteoarthritis. Chin J Rehabil T heory Pract. 2008;14:345–346.
142. Shao XG, Tao HX, Yang WZ, et al. Effects of electroacupuncture on regulating the expressions of BMP2/Smad1 in impaired cartilage of experimental rabbits with knee osteoarthritis. Chin J Rehabil Med. 2015;30:655–660.
143. Xue X, You Y, Tao J, et al. Electro-acupuncture at points of Zusanli and Quchi exerts anti-apoptotic effect through the modulation of PI3K/Akt signaling pathway. Neurosci Lett. 2014;558:14–19. doi:10.1016/j.neulet.2013.10.029
144. Zhang L, Yu C, Chen B, et al. Modulation of colonic function in irritable bowel syndrome rats by electroacupuncture at ST25 and the neurobiological links between ST25 and the colon. Front Neurosci. 2022;16:930489. doi:10.3389/fnins.2022.930489
145. Wang ZZ, Lin J, Zeng ZM, et al. Effect of Electroacupuncture knee Tri-acupuncture on the expression of TLR4 and p-NF-κBp65 protein in rats with knee osteoarthritis. Shenzhen J Integr Traditional Chin West Med. 2024;34:17–21.
146. ZQi Z, Yang YJ, Ma XD, et al. Mechanism of electroacupuncture penetration needling for relieving synovial inflammation of knee osteoarthritis through TLR4/MyD88/NF-κB signal pathway. Acupunct Res. 2023;48:353–358.
147. Huang WT, Li B, Chen H, et al. The impact of electroacupuncture intervention on synovial structure and SIRT1/HMGB1 signaling pathway in rats with knee osteoarthritis. Yunnan J Trad Chin Med Mater Med. 2022;43:74–78.163.
148. Huang XR, Hu LZ, Wang JL, et al. Effects of electroacupuncture on the expression of proteins related to degradation of articular cartilage and subchondral bone in KOA rats. Tradit Chin Med Rehab. 2024;1:10–15.
149. Tao J, Chen B, Gao Y, et al. Electroacupuncture enhances hippocampal NSCs proliferation in cerebral ischemia-reperfusion injured rats via activation of notch signaling pathway. Int J Neurosci. 2014;124(3):204–212. doi:10.3109/00207454.2013.840781
150. Zhang YY, Jiang XY, Li XH, et al. Effect of electroacupuncture on chondrocyte apoptosis in knee osteoarthritis rat based on PI3K/Akt signaling pathway. Rehab Med. 2019;29:30–36.
151. Li F, Lu K, Gong B, et al. Effect of electroacupuncture on the expression of RhoA and ROCK after focal cerebral infarction in rats. Laser Journal. 2014;35:70–72.
152. Sun GH, Liao Y, Liao Y, et al. Electroacupuncture intervention improves cartilage degeneration and subchondral bone osteoporosis of knee-joint possibly by adjusting OPG/RANK/RANKL signaling in ovariectomized rats. Acupunct Res. 2018;43:781–787.
153. Yu J, Zhao C, Luo X. The effects of electroacupuncture on the extracellular signal-regulated kinase 1/2/P2X3 signal pathway in the spinal cord of rats with chronic constriction injury. Anesth Analg. 2013;116(1):239–246. doi:10.1213/ANE.0b013e31826f0a4a
154. Chen HH, Shao X, Li L, et al. Electroacupuncture serum inhibits TNF-α-mediated chondrocyte inflammation via the Ras-RafMEK1/2-ERK1/2 signaling pathway. Mol Med Rep. 2017;16(5):5807–5814. doi:10.3892/mmr.2017.7366
155. Fu CL, Lin J, Zhao ZS, et al. Electroacupuncture inhibits the ultrastructural degeneration of osteoarthritic chondrocytes mediated by Ras/Raf/MEK1/2/ERK1/2 signaling pathways. Chin J Tissue Eng Res. 2017;21:5134–5139.
156. Fu CL, Chen HH, Zhu DY, et al. Electroacupuncture delays articular cartilage degeneration in osteoarthritis via Ras-Raf-MEK1/2-ERK1/2 signaling pathway. Chin J Tissue Eng Res. 2017;21:3790–3795.
157. Chen XT, Yu DB, Lin YY, et al. Mechanism of electroacupuncture maintaining cartilage homeostasis and antiinflammation through HIF-1α and SOX-9 in rabbit knee osteoarthritis. J Liaoning Univ Traditional Chin Med. 2024;26:210–214.
158. Yin YS, Ruan AM, Liu MY, et al. Mechanism study of efficacy of electroacupuncture on signaling pathway in synovial tissue of rabbits with knee osteoarthritis. Chin J Traditl Med Traumatol Orthopedics. 2021;29:1–4.
159. Jia FY, Li MM, Wang JL, et al. Effects of electroacupuncture on inflammatory response and cGAS/ STING signaling pathway in rats with anterior cruciate ligament rupture. J Traditional Chinese Med Pharm. 2024;30(1):6.
160. Yu JH, Li YX, Chen B, et al. Effect of electro-acupuncture on AQP3 expression in chondrocytes of osteoarthritis. Clin Acupunct Moxibust. 2020;36:60–64.
161. Quan RF, Chen RL, MXn D, et al. Anti-apoptotic signal transduction mechanism of electroacupuncture in acute spinal cord injury. Acupunct Med. 2014;32(6):463–471. doi:10.1136/acupmed-2014-010526
162. Xing LF, Chen XL, Guo CQ, et al. Electroacupuncture exerts chondroprotective effect in knee osteoarthritis of rabbits through the mitophagy pathway. J Pain Res. 2023;16:2871–2882. doi:10.2147/JPR.S416242
163. Wu GW, Zheng CS, Li XH, et al. Effect of electroacupuncture on chondrocyte apoptosis and cartilage matrix of experimental rats with knee osteoarthritis. Rehab Med. 2017;27(5):22–28. doi:10.3724/SP.J.1329.2017.05022
164. Chen HL, Qi H, Liu XJ, et al. Effect of electroacupuncture pretreatment on apoptotic neurons and expression of GRP 78. Acupunct Res. 2014;52:431–436.
165. Fan YZ, Wu YC, Zhang JF, et al. Study of the inhibiting effects of ear point sticking plus electroacupuncture on synovial fibrosis and endoplasmic reticulum stress in knee osteoarthritis model rats. Shanghai J Acu-Mox. 2024;43(8):906–914.
166. Shi XW, Battulga O, Wang DF, et al. Effects of electroacupuncture on articular cartilage pathology and viscoelastic mechanical properties in a rabbit model of early knee osteoarthritis. J Hunan Univ Chin Med. 2021;14:72–78.
167. He J, Zuo J, Fan XC, et al. Electro-acupuncture modulated miR-214 expression to prevent chondrocyte apoptosis and reduce pain by targeting BAX and TRPV4 in osteoarthritis rats. Braz J Med Biol Res. 2024;57:e13238. doi:10.1590/1414-431x2024e13238
168. Huang XR, Zhou J, Sun GH, et al. Effect of electroacupuncture on articular cartilage and subchondral polarization⁃related protein expression in aged rats. J Pra Med. 2023;39:1473–1479.
169. Xie LL, Zhao YL, Yang J, et al. Electroacupuncture prevents osteoarthritis of high-fat diet-induced obese rats. BioMed Res Internat. 2020;2020(1):9380965. doi:10.1155/2020/9380965
170. Xin YY, Wang JX, Xu AJ. Electroacupuncture ameliorates neuroinflammation in animal models. Acupunct Med. 2022;40(5):474–483. doi:10.1177/09645284221076515
171. Lin J, Li J, Huang J, et al. Enhancement of motor learning and corticospinal excitability: the role of electroacupuncture and motor training in healthy volunteers. Med Sci Monit. 2024;30:e943748. doi:10.12659/MSM.943748
172. Wang H, Qu S, Zhou T, et al. Current perspectives and trend of acupuncture in breast cancer-related symptoms: a bibliometric study. J Pain Res. 2023;16:4165–4180. doi:10.2147/JPR.S442151
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.