Back to Journals » Cancer Management and Research » Volume 14
Advanced Nasopharyngeal Carcinoma: Current and Emerging Treatment Options
Authors Jiromaru R, Nakagawa T, Yasumatsu R
Received 5 July 2022
Accepted for publication 7 September 2022
Published 12 September 2022 Volume 2022:14 Pages 2681—2689
DOI https://doi.org/10.2147/CMAR.S341472
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Seema Singh
Rina Jiromaru,1 Takashi Nakagawa,1 Ryuji Yasumatsu2
1Department of Otorhinolaryngology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan; 2Department of Otorhinolaryngology Head and Neck Surgery, Faculty of Medicine, Kindai University, Osaka, Japan
Correspondence: Ryuji Yasumatsu, Department of Otorhinolaryngology Head and Neck Surgery, Faculty of Medicine, Kindai University, 377-2 Onohigashi, Osaka, 589-0014, Japan, Tel +81-72-3660221, Fax +81-72-3682252, Email [email protected]
Abstract: Nasopharyngeal carcinoma (NPC) has seen improved treatment outcomes and a decrease in incidence worldwide in recent years due to developments in medicine and improved public health. However, 70% of cases are still diagnosed at advanced stages and these advanced NPC cases show a poor prognosis. Reports on current and future treatment in advanced NPC are summarized. Chemoradiotherapy is the mainstay of treatment for advanced NPC. The administration of platinum agents as a concurrent drug and intensity modulated radiotherapy (IMRT) is the most appropriate irradiation method, and is associated with high local control rates. For induction and adjuvant chemotherapy, platinum-based two- or three-drug combination chemotherapy is recommended. The tumour volume, plasma Epstein-Barr virus (EBV)-DNA levels, and the tumour site are used to determine the indication for adjuvant and neo-adjuvant chemotherapy. The tolerability of induction chemotherapy is controversial, and the indications and timing should be carefully considered in each case. Chemotherapy is used for patients with distant metastasis. Gemcitabine/cisplatin is the first-line regimen. The efficacy of immune checkpoint inhibitor (ICI) treatment has recently been reported for NPC and, as in other areas of the head and neck, it is expected to be effective for patients with recurrent/distant metastasis. Trials are underway for various uses of ICIs, including induction chemotherapy, postoperative treatment, and use in combination with chemoradiotherapy. Immunotherapy for NPC, an EBV-associated cancer, has been reported to have some efficacy with immunotherapy used in other EBV-associated cancers. Immunotherapy may be introduced for NPC in the future, depending on the results of clinical trials. Future changes in the treatment of NPC are expected to include risk classification based on plasma EBV-DNA levels and the development of personalized treatment with individual selection of timing and type of therapy.
Keywords: nasopharyngeal carcinoma, therapy, Epstein-Barr virus
Introduction
Nasopharyngeal carcinoma (NPC) is a rare cancer with a global age-standardised incidence rate of <1 in 100,000,1 with 133,354 new cases and 80,000 deaths per year in a total of 185 countries in 2020.2 In high prevalence areas (eg, North Africa, East Asia), incidence rates of 4–12 per 100,000 population are observed, with regional variations.3 Due to lifestyle and environmental changes, the incidence in Hong Kong, a high prevalence area, has decreased by 30% in 20 years in comparison to the 1980s, and the incidence is decreasing worldwide.4,5 Survival rates have also shown an increase due to improved diagnostic imaging, early detection through mass screening and improved tumour control with the introduction of intensity-modulated radiotherapy (IMRT).4 However, 75.4% of cases of NPC are still detected at an advanced stage (stage III–IV), and the 10-year survival rates for stage III and IV cases are 74–79% and 46–56%, respectively, and are reported to be particularly poor in stage IV cases.6–8 The current treatment and prospects in advanced-stage NPC, including NPC with distant metastasis from the outset, are summarized and reported.
Characteristics of Nasopharyngeal Carcinoma
The characteristics of NPC include being an EBV-associated tumour and its high prevalence in some areas. Nasopharyngeal carcinoma is classified by its histopathology into keratinizing, non-keratinizing and basal cell types.9 Among non-keratinizing types, 69–93% are said to be EBV-associated tumours.10,11 Human papilloma virus (HPV) infection has also been associated with NPC in a few reports.;12–14 however, the response to treatment has been mixed. Accordingly, the NCCN guideline does not recommend HPV infection tests.15 The pathogenesis of non-virus-associated tumours remains unclear.
Risk factors for the development of NPC have been reported to be associated with alcohol and smoking habits in keratinizing NPCs, and with N-nitrosamine-rich salted-food and EBV infection in non-keratinizing NPC.9 Prognostic factors other than TNM classification that have been reported include a history of smoking, mutational signatures relevant to DNA repair pathways, the overexpression of serglycin and p53, chromatin modification, ERBB-PI3K signalling, and elevated serum levels of EBV-DNA.15,16 Among these, the NCCN guidelines point to the tumour volume and plasma EBV-DNA levels as high-risk factors.15 The plasma EBV-DNA levels have been reported as an independent prognostic factor for the prognosis and distant metastasis. Various studies are currently underway on the usefulness of EBV-DNA as a predictor of the treatment response to chemoradiotherapy (CRT).
Initial Treatment
Radiotherapy is the standard therapy in NPC and an essential treatment modality in non-disseminated NPC.15,16 In early-stage cases, radiotherapy (RT) alone is indicated for stage I and RT in combination with chemotherapy is indicated for stage II. In these cases, radiotherapy targeting the primary tumour and selected cervical lymph nodes is recommended.15–18
With regard to radiotherapy, the last decade has seen a shift from conventional 2DRT and 3DRT to IMRT.19 In patients who receive IMRT, the local control and 5-year disease specific survival (DSS) rates are reported to be 80–90% and 85%, respectively, and the overall survival (OS) rate (80%) is superior to that of patients who receive 3DRT (DSS: 81%, OS: 73%) and 2DRT (DSS: 80%, OS: 71%).20–23 In addition to treatment efficacy, the late effects of radiation, IMRT have been reported to be favourable in comparison to conventional RT. The ability of IMRT to modulate the shape and intensity of the radiation beam and to minimise the dose to the organ at risk (OAR) has been shown to reduce the late effects on the patient’s quality of life after treatment, such as dysphagia and xerostomia.19,24 In reducing these late effects, the introduction of adaptive radiotherapy (ART) has also been used in recent years to reduce the radiation dose of OAR.25 ART involves changing the irradiation plan in response to changes in tumour volume during treatment and optimizing the irradiation coverage during the course of irradiation. It is a useful technique in NPC, where tumour volume changes are likely to occur.25,26
In NPC with locally advanced disease and lymph node metastases, concurrent CRT (CCRT) is the standard treatment.15,16 The combination of radiotherapy with chemotherapy was reported in NPC-9902 and showed significantly better treatment control in patients with T3-4N0-1 NPC when fractionated irradiation was compared to treatment with or without chemotherapy.27 The biological effect is higher with fewer irradiations (higher dose per fraction) when the total dose is the same. A fraction size of 2.0–2.12 Gy, in five fractions per week, to a total prescribed dose of 70 Gy in 33–35 fractions was used in the Intergroup 0099 and RTOG 0225 trials, with acceptable toxicity for adequate efficacy.28 As for accelerated irradiation, the difference in treatment efficacy between the chemotherapy group and the non-combination group has not been established. Furthermore, it has been reported that accelerated fractionated radiation in advanced NPC (twice daily to reduce repopulation and thus shorten the treatment period) has no therapeutic benefit over conventional irradiation.27,29
Blanchard et al reported an analysis of the landmark Intergroup 0099 randomized trial of CCRT as standard treatment for locally advanced NPC with or without adjuvant chemotherapy.30 The addition of chemotherapy to RT was found to be the most effective factor for OS. The addition of adjuvant or neo-adjuvant chemotherapy to simple RT has no significant benefit and CCRT is the most fundamental treatment modality for NPC.
Adjuvant and Neo-Adjuvant Chemotherapy
The NCCN guidelines recommend that induction chemotherapy (ICT) or adjuvant chemotherapy (ACT) should be considered in high-risk cases with N1 or higher or T3 or higher.15 The American Society of Clinical Oncology (ASCO)/Chinese Society of Clinical Oncology (CSCO) guidelines recommend ICT at ≥T3 or N2-3, while ACT is recommended in the absence of ICT.31
Majed et al reported that the addition of ACT was associated with superior progression-free survival (PFS) and local control, while the addition of ICT was associated with superior in PFS, local and distant metastasis control in a Phase III trial comparing the effect of ACT with gemcitabine/cisplatin/5-FU in combination with RT or CRT in N2-3 NPC to that of CRT alone.32 Similar results were reported for NPC-0501.33 Adjuvant chemotherapy added to CRT was associated with the highest survival rate, while the best effect on distant control was achieved with ICT. There were problems with completion rates in NPC-0501, with 83% and 67% of patients receiving all three cycles of ICT and ACT, respectively. In addition, 38% and 53% of patients received all three cycles of chemotherapy in combination with RT before and after the ICT and ACT, respectively.33 This leaves the question of the tolerability of ICT in doubt. Zhang et al reported a Phase II study of gemcitabine/cisplatin as ICT, in which CRT was combined with gemcitabine (1 mg/m2)/cisplatin (80 mg/m2) for 3 cycles every 3 weeks for 3-year.34 The relapse-free survival (RFS) rates in the CRT plus gemcitabine/cisplatin group and CRT without gemcitabine/cisplatin group were 85.3% and 76.5%, respectively (hazard ratio for recurrence or death, 0.51; 95% confidence interval [CI], 0.34–0.77; P=0.001).
Gemcitabine/cisplatin or cisplatin/5-FU/docetaxel have been used as ICT regimens.15,34 Cisplatin/5-FU is the most recommended ACT regimen.17,35 Reports are also available on carboplatin/5-FU and capecitabine. In a recent network meta-analysis comparing DC, docetaxel/cisplatin, GP, gemcitabine/cisplatin and PX, cisplatin/capecitabine as ICT, all showed improved OS. GP and PX tended to be more useful as ICT in the IMRT group, while DC tended to be more useful in the non-IMRT group. It was also reported that gemcitabine-based IC in combination with two drugs contributed more to the improvement of OS than triple combination and taxane-based ICT regimens.36
Treatment of Recurrent and Distant Metastatic Cases
It has been reported that 15–30% of patients with locally advanced NPC will develop local recurrence and/or distant metastases in the future.37 For NPC with recurrent and distant metastasis, treatment options are limited by the fact that the majority of patients receive CRT in their initial treatment, and local resection is anatomically difficult. Chemotherapy is the main treatment for recurrent and distant NPC.
The standard of care for recurrent and distant NPC is multi-agent chemotherapy, including platinum-based agents. In a phase III study by Hong et al, which evaluated the efficacy of cisplatin plus gemcitabine in recurrent/distant metastasis NPC (R/MNPC) (GEM20110714), the authors compared GP (gemcitabine 1 g/m2 once daily on days 1 and 8 and cisplatin 80 mg/m2 once daily on day 1; n=5181) and FP (fluorouracil 4 g/m2 in continuous intravenous infusion over 96 hours and cisplatin 80 mg/m2 once daily on day 1; n=5181).38 The probability of 5-year OS in the GP arm versus the FP arm was 19.2% (95% CI, 13.6–25.5) versus 7.8% (95% CI, 4.3–12.6; P=0.001). The probability of 5-year PFS was 7.6% (95% CI, 3.9–12.9) in the GP arm versus 0% in the FP arm (P=0.001). The results showed that cisplatin/gemcitabine is category 1 for first-line treatment for R/MNPC.15 Other proposed regimens include combinations of CDDP, PTX, carboplatin and cetuximab.
With the recent development of endoscopic techniques, good results of endoscopic resection of locally recurrent NPC have also been reported in recent years: Liu et al reported a multi-centre phase III trial in patients with locally recurrent NPC with a history of irradiation. The 3-year overall survival rate was 85.8% (95% CI, 78.9–92.7) in the endoscopic nasopharyngectomy (ENPG) group and 68.0% (95% CI, 58.6–77.4) in the IMRT group (hazard ratio 0.47, 95% CI, 0.29–0.76; p=0.0015).39
With regard to adverse events, the incidence of grade 3 or higher adverse events was reported to be 5% in the ENPG group and 26% in the IMRT group. Local endoscopic resection resulted in higher survival rates and fewer adverse events. Although long-term results need to be accumulated since the follow-up period is less than 5 years, surgery may be recommended for patients with resectable local recurrence.
Future Treatment
EBV-DNA and Treatment Strategy
Almost 100% of non-keratinizing NPCs are reported to be associated with EBV, in contrast to 30–100% of keratinizing NPCs, although there is considerable variation between reports. In recent retrospective studies, plasma EBV-DNA has been reported to be a strong prognostic factor.40,41
NRG-HN001 (NCT02135042), which was initiated by the NRG Oncology Cooperative Group, uses post-RT plasma EBV-DNA measurements to divide NPC patients into low- and high-risk groups. The study design is based on the hypothesis that the low-risk group will not require ACT and that the high-risk group will benefit from ACT. The results are not yet available. Other studies include a study to determine EBV-DNA at 2–3 months after the completion of radiotherapy in order to examine recurrence and survival (NCT03981224), a study to investigate the prognostic value of PET combined with the quantity of EBV-DNA as a predictor of prognosis in post-treatment follow-up of patients with locally advanced NPC (NCT03601390), a study to examine the prognostic value of the tumour volume and EBV-DNA as a marker of the cisplatin-based chemotherapy response (NCT01365208), and a number of ongoing clinical trials related to the volume of EBV-DNA. Measurement and monitoring of EBV-DNA before, after, or during the initiation of treatment may be important for future treatment selection and the prognosis (Table 1).
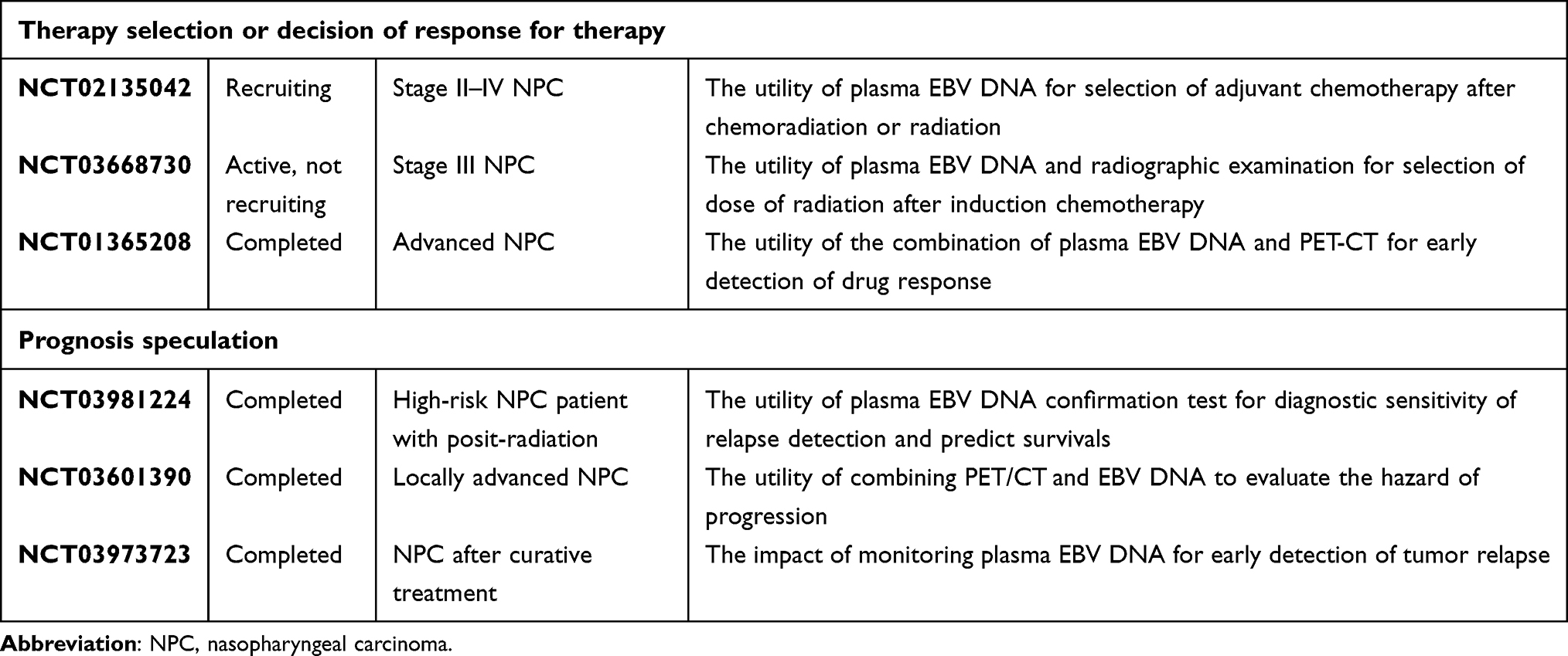 |
Table 1 Trials Associated with EBV-DNA and Nasopharyngeal Carcinoma |
Immune Checkpoint Inhibitors
In recent years, immune checkpoint inhibitors (ICIs) have been investigated as one of the most important treatments for NPC. Programmed cell death ligand 1 (PD-L1) is expressed in approximately 90% of EBV-associated NPCs.42 The expression of PD-L1 is closely associated with recurrence or metastasis of NPC and the clinical course of the patients.43 Functional polymorphisms in the CTLA-4 gene have also been reported to be associated with susceptibility to NPC in Chinese patients, demonstrating that the inhibition of PD-1/CTLA-4 significantly enhances the ability of T cells to produce the anti-tumour cytokine IFN-γ against the EBV antigen.44
Currently, ICI therapy is approved for the treatment of squamous cell carcinoma of the head and neck.45 The anti-tumour activity and safety profile of pembrolizumab was first reported for R/MNPC in the KEYNOTE028 trial.46 The overall response rate (ORR) and disease control rate were approximately 25% and 60%, respectively, and toxicity was consistent with the use of ICIs in other diseases. In a phase II international trial (NCI-9742), 44 patients with refractory NPC were enrolled in a clinical trial of nivolumab (human IgG4 anti-PD-1 monoclonal antibody). The 1-year OS rate after nivolumab treatment was increased in comparison to data reported in similar populations.47 While these positive data, KEYNOTE 122, a phase III trial comparing chemotherapy with pembrolizumab monotherapy in platinum-pretreated R/MNPC, reported that pembrolizumab did not prolong OS (median OS was 17.2 months with pembrolizumab and 15.3 months with chemotherapy; hazard ratio 0.90; 95% CI, 0.67–1.19; p = 0.2262).48 In this study, capecitabine, gemcitabine, and docetaxel were the chemotherapy regimens being compared. Since this study was analysed in patients with PDL-1 combined positive score (CPS) 1% or higher, the results may have been different if only groups with high CPS scores were compared. Recently, the concept of PFS2 has emerged, which is expected to enhance the efficacy of second-line therapy after ICI administration. Therefore, as one of the most important agents for advanced NPC, the accumulation of long-term results, cases, and trials of ICIs is awaited.
There have been recent reports of ICIs combined with conventional therapy as well as monotherapy alone. The standard chemotherapy for R/MNPC is a combination of gemcitabine/cisplatin, as mentioned above, but recently there have been reports of better results with the combination of ICI. In the international double-blind Phase 3 study (NCT03581786) by Mai et al, 289 R/MNPC patients with recurrent or metastatic disease and no prior chemotherapy were randomized to receive toripalimab, a human anti-PD-1 monoclonal antibody, or placebo and gemcitabine/cisplatin every 3 weeks for up to 6 cycles combination, followed by randomization to receive either alone or placebo.49 An analysis of PFS detected a significant improvement in PFS in the toripalimab group compared to the placebo group: median PFS was 11.7 versus 8.0 months, hazard ratio (HR) = 0.52 (95% confidence interval (CI): 0.36–0.74), P = 0.0003.49 Similar to this trial, a randomized, double-blind, phase 3 trial by Yang et al done at 28 hospitals in China (NCT03707509) used camrelizumab (200 mg on day 1) with gemcitabine plus cisplatin and maintenance monotherapy after 4–6 cycles.50 The progression-free survival was significantly longer in the camrelizumab group (median 9.7 months [95% CI, 8.3–11.4]) than in the placebo group (median 6–9 months [5.9–7.3]; hazard ratio 0.54 [95% CI, 0.39–0.76]; one-sided p=0.0002). In both studies, G3 or higher treatment-related adverse events were 70–89% more frequent in the ICI group, but the rates were similar to those in the respective placebo groups. However, immune-related adverse events (irAEs) (39.7% versus 18.9%) and grade ≥3 irAEs (7.5% versus 0.7%) were more frequent in the toripalimab arm versus the placebo arm.49 In addition, treatment-related deaths occurred in five (4%) patients in the camrelizumab group (two unknown causes of death, one multiple organ dysfunction syndrome, one pharyngeal haemorrhage, and one arrhythmia) and one (<1%) patient in the placebo group (unknown cause of death).50 The efficacy of the combination of ICI and existing regimens was reported, but there were treatment-related deaths, and the duration and dose of the combination should be thoroughly discussed.
Although NCI-9742 found no association between OS and EBV- DNA clearance, several trials have been conducted on the relationship between EBV and ICI treatment efficacy. An ongoing trial will measure the ORR and clearance efficiency of EBV-DNA by administering pembrolizumab (NCT03544099) to patients without clinically R/MNPC after radical CRT and in whom plasma EBV-DNA is detected. Sixty-three patients have been enrolled in the trial. Another trial (NCT03267498) is investigating the efficacy of nivolumab in combination with CRT in patients with stage II–IVB NPC. A clinical trial investigating the efficacy of CTLA-4 inhibitors is also underway (NCT02834013).
Other ongoing ICI-related trials include the utility of neoadjuvant and adjuvant ICI therapy in combination with CCRT for advanced-stage cases (NCT03925090, NCT05397769, NCT04833257, NCT04907370, NCT03984357) or the efficacy of ICI in combination with PARP inhibitor for R/MNPC (NCT04825990, NCT04978012, NCT05162872) (Table 2). Thus, it is anticipated that regimens for the use of ICIs will change in the future, with more reports on the impact of timing of use on survival and the effects of combining ICIs with other drugs.
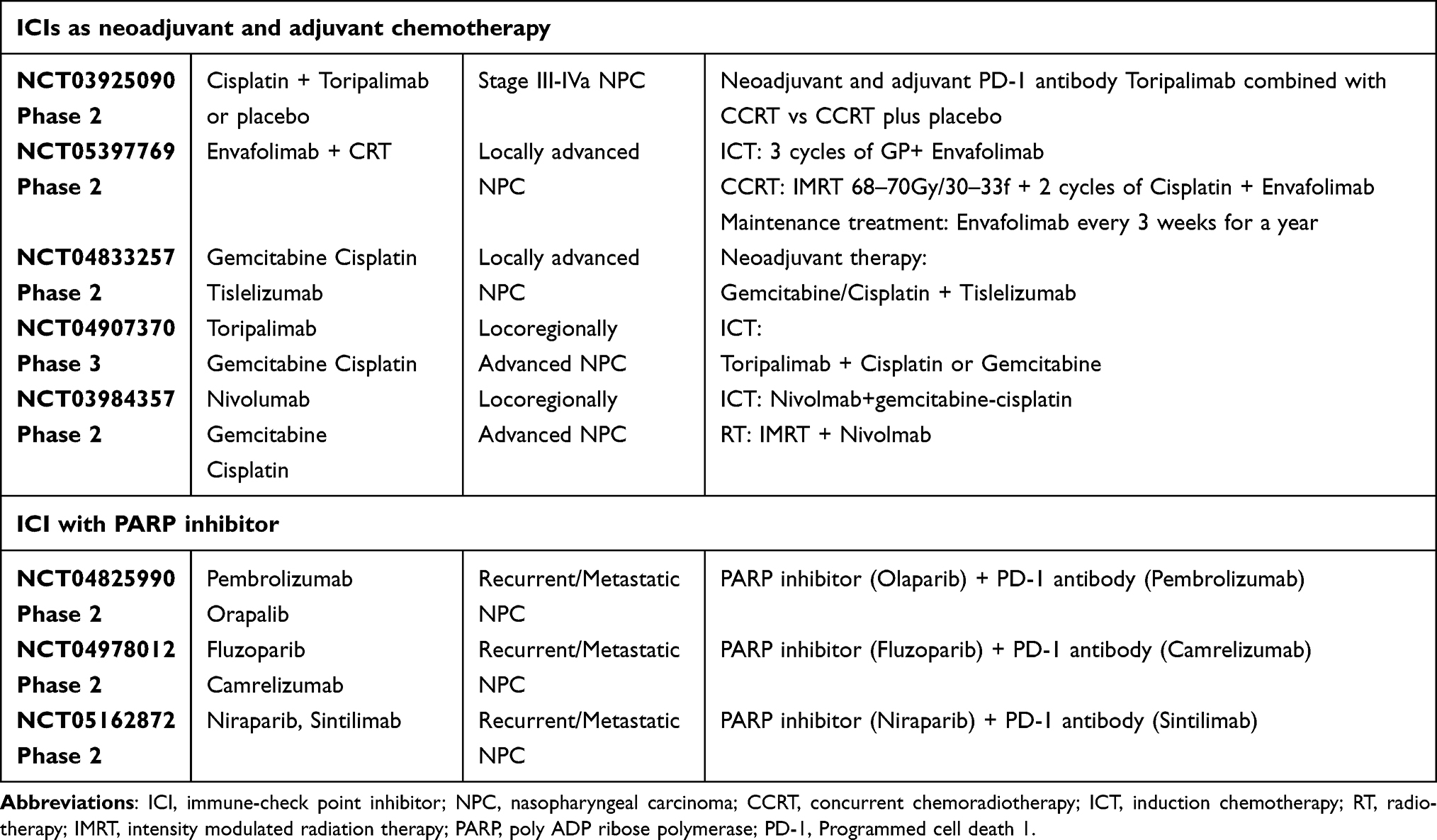 |
Table 2 Trials Associated with Nasopharyngeal Carcinoma and Immune-Checkpoint Inhibitor |
EBV Infection and Immunotherapy
EBV-related NPC is usually a state of immune dysfunction.51,52 Furthermore, the first-line treatment is chemotherapy and radiotherapy, which tends to be immunosuppressive. This shift from a suppressive situation to immune activation is expected to be a prognostic factor. Cytokine-induced killer (CIK) and chimeric antigen receptor T-cell immunotherapy (CAR-T) have been used for EBV-related haematological tumours and have been validated at the in vitro level in the same EBV-related NPV.53 CAR-T has shown effective anti-tumour activity in melanoma, leukaemia and lymphoma, and is seen as a promising strategy for EBV-related NPC. However, post-operative lymphoproliferative disorder (PTLD), for which immunotherapy is said to be useful, has an EBV type 3 antigen, while NPC has a type 2 antigen; thus, the efficacy of immunotherapy needs to be verified in practice. Lutzky et al inserted a set of duplicated peptides of EBNA1, LMP1 and LMP2 into replication-deficient adenovirus, which was reported to maximally activate host immune responses against all three viral proteins presented in NPCs (NCT01147991).54 The use of LMP2A peptides as a vaccine has also been reported to benefit the clinical outcomes of patients with stage II/III NPC.55 A trial is currently underway in NCT01094405 to test the efficacy of the MVA EBNA1/LMP2 vaccine in patients with residual, or R/MNPC. Dendritic cells (DCs), the most potent antigen-presenting cells, play a key role in the activation of CD4+ and CD8+ T cells, triggering a robust T-cell immune response against tumour antigens. Enhanced CD8+ T-cell responses were observed in 9 of 16 NPC patients who were inoculated with LMP2 peptide epitope-pulsed autologous DCs. In addition, 2 of 16 patients achieved partial remission.56 An ongoing Phase I study (NCT03282617) is underway in which patients with locally advanced or locally recurrent/metastatic NPC are treated with a DC vaccine called CD137L-DC-DC-EBV-VAX.
Molecularly Targeted Drugs
Numerous studies have discussed the combination of epidermal growth factor receptor (EGFR) antibodies and radiation; however, there is still no consensus on the treatment.57 A phase II study comparing RT with cetuximab and CRT with cisplatin reported no clear difference in 3-year disease-free survival, but reported a trend toward more side effects (mainly mucositis and acneiform rash as grade 4 adverse effects) in the cetuximab group, which made it difficult to continue treatment.58 The 5-year OS of patients with locally advanced NPC who received nimotuzumab was inferior to that of those who received cisplatin in combination with RT (63.9% versus 81.4%, p = 0.024), although there were no severe side effects, as was observed with cetuximab.59 In patients of ≥60 years of age, it showed equal efficacy and was associated with less nausea and gastrointestinal side effects in comparison to cisplatin, suggesting that it may be an effective treatment option for locally advanced NPC in patients of ≥60 years of age. Regarding anti-EGFR antibodies in patients with recurrent metastasis, a phase II study of cisplatin/5-FU in combination with nimotuzumab achieved an ORR of 71.4% and the only toxicity was grade 3/4 leukopenia.60 This may be the treatment of choice for platinum-refractory R/MNPC.
Vascular endothelial growth factor (VEGF) is often pointed out to be associated with a predisposition toward bleeding and the NCCN guideline mentions a tendency to avoid its use for recurrence in previously irradiated sites.15 An ongoing trial is testing the benefit of Phase 2/3 chemotherapy in combination with EGFR and VEGF agents in patients with PD on ICI therapy for R/MNPC (NCT05063552).
Conclusion
Treatment for advanced nasopharyngeal carcinoma is expected to become more personalized in the future. Plasma EBV-DNA is expected to be the main indicator for personalized therapy, and the timing and combination of the use of immunotherapy and existing treatments will need to be selected according to individual circumstances. It is expected to be used to determine the addition of ACT or NACT based on the amount of EBV-DNA prior to treatment, or to determine additional treatment based on the amount of EBV-DNA after treatment. In addition, the efficacy of ICI for recurrent metastases remains controversial, but it is certain to remain one of the major treatment options in the future as the use of multiple agents and the timing of their use are being validated.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. doi:10.3322/caac.20107
2. Sung H, Ferlay J, Siegel R, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Centre for Health Protection [homepage on the Internet]. Hong Kong: health topics; [updated January 4, 2022; cited January 4, 2022]. Available from: http://www.chp.gov.hk/en/healthtopics/content/25/54.html/.
4. Chua MLK, Wee JTS, Hui EP, et al. Nasopharyngeal carcinoma. Lancet. 2016;387:1012–1024. doi:10.1016/S0140-6736(15)00055-0
5. Lee AW, Foo WF, Mang O, et al. Changing epidemiology of nasopharyngeal carcinoma in Hong Kong over a 20-year period (1980–1999): an encouraging reduction in both incidence and mortality. Int J Cancer. 2003;103(5):680–685. doi:10.1002/ijc.10894
6. Wu LR, Zhang XM, Xie XD, et al. Validation of the 8th edition of AJCC/UICC staging system for nasopharyngeal carcinoma: results from a non-endemic cohort with 10-year follow-up. Oral Oncol. 2019;98:141–146. doi:10.1016/j.oraloncology.2019.09.029
7. Wang L, Wu Z, Cheng W, et al. Efficacy of concurrent chemoradiotherapy in subgroups of stage III nasopharyngeal carcinoma: an analysis based on 10-year follow-up. Radiat Oncol. 2021;16(1):215. doi:10.1186/s13014-021-01929-9
8. Chen L, Zhang Y, Lai SZ, et al. 10-year results of therapeutic ratio by intensity-modulated radiotherapy versus two-dimensional radiotherapy in patients with nasopharyngeal carcinoma. Oncologist. 2019;24(1):e38–e45. doi:10.1634/theoncologist.2017-0577
9. Peterson BF, Bell D, El-Mofty SK, et al. Nasopharyngeal carcinoma. In: El-Nagger AK, Chan JKC, Grandis JR, Takata T, Slootweg PJ, editors. World Health Organization Classification of Head and Neck Tumours. Lyon: IARC; 2017:65–71.
10. Chan KH, Gu YL, Ng F, et al. EBV specific antibody-based and DNA-based assays in serologic diagnosis of nasopharyngeal carcinoma. Int J Cancer. 2003;105(5):706–709. doi:10.1002/ijc.11130
11. Dardari R, Hinderer W, Lang D, et al. Antibody responses to recombinant Epstein-Barr virus antigens in nasopharyngeal carcinoma patients: complementary test of C\ZEBRA protein and early antigens p54 and p138. J Clin Microbiol. 2001;39(9):3164–3170. doi:10.1128/JCM.39.9.3164-3170.2001
12. Dogan S, Hedberg ML, Ferris RL, et al. Human papilloma virus and Epstein-Barr virus in nasopharyngeal carcinoma in a low-incidence population. Head Neck. 2014;36(4):511–516. doi:10.1002/hed.23318
13. Robinson M, Suh YE, Paleri V, et al. Oncogenic human papillomavirus-associated nasopharyngeal carcinoma: an observational study of correlation with ethnicity, histological subtype and outcome in a UK population. Infect Agent Cancer. 2013;8(1):30. doi:10.1186/1750-9378-8-30
14. Stenmark MH, McHugh JB, Schipper M, et al. Nonendemic HPV-positive nasopharyngeal carcinoma: association with poor prognosis. Int J Radiat Oncol Biol Phys. 2014;88(3):580–588. doi:10.1016/j.ijrobp.2013.11.246
15. Pfister DG, Spencer S, Adkins D, et al. National comprehensive cancer network guidelines version 2.2022. Head Neck Cancers. 2022. Available from: https://www.nccn.org/guidelines/guidelines.
16. Bossi P, Chan AT, Trama LL, et al. Nasopharyngeal carcinoma: ESMO-EURACAN clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2021;32(4):452–465. doi:10.1016/j.annonc.2020.12.007
17. Al-Sarraf M, LeBlanc M, Giri PG, et al. Chemoradiotherapy versus radiotherapy in patients with advance nasopharyngeal cancer: Phase III randomized Intergroup study 0099. J Clin Oncol. 1998;16(4):1310–1317. doi:10.1200/JCO.1998.16.4.1310
18. Masterson L, Howard J, Gonzalez-Cruz J, et al. Immune checkpoint inhibitors in advanced nasopharyngeal carcinoma: beyond an era of chemoradiation? Int J Cancer. 2020;146(8):2305–2314. doi:10.1002/ijc.32869
19. Kam MK, Teo PML, Chau RMC, et al. Treatment of nasopharyngeal carcinoma with intensity-modulated radiotherapy: the Hong Kong experience. Int J Radiat Oncol Biol Phys. 2004;60(5):1440–1450. doi:10.1016/j.ijrobp.2004.05.022
20. Tham IWK, Hee SW, Yao RMC, et al. Treatment of nasopharyngeal carcinoma using intensity-modulated radiotherapy-the national cancer centre Singapore experience. Int J Radiat Oncol Biol Phys. 2009;75(5):1481–1486.
21. Lai SZ, Li WF, Chen L, et al. How does intensity-modulated radiotherapy versus conventional two-dimensional radiotherapy influence the treatment results in nasopharyngeal carcinoma patients? Int J Radiat Oncol Biol Phys. 2011;80(3):661–668. doi:10.1016/j.ijrobp.2010.03.024
22. Zhang MX, Jing L, Shen GP, et al. Intensity-modulated radiotherapy prolongs the survival of patients with nasopharyngeal carcinoma compared with conventional two-dimensional radiotherapy: a 10-year experience with large cohort and long follow-up. Eur J Cancer. 2015;51(17):2587–2595. doi:10.1016/j.ejca.2015.08.006
23. Lee AWM, Ng WT, Chan LLK, et al. Evolution of treatment for nasopharyngeal cancer-success and setback in the intensity-modulated radiotherapy era. Radiother Oncol. 2014;110(3):377–384. doi:10.1016/j.radonc.2014.02.003
24. Chen YY, Zhao C, Wang J, et al. Intensity-modulated radiation therapy reduces radiation-induced trismus in patients with nasopharyngeal carcinoma: a prospective study with >5 years of follow-up. Cancer. 2011;117(13):2910–2916. doi:10.1002/cncr.25773
25. Chen AM, Daly ME, Cui J, et al. Clinical outcomes among patients with head and neck cancer treated by intensity-modulated radiotherapy with and without adaptive replanning. Head Neck. 2014;36(11):1541–1546. doi:10.1002/hed.23477
26. Yang H, Hu W, Wang W, et al. Replanning during intensity modulated radiation therapy improved quality of life in patients with nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys. 2013;85(1):e47–e54. doi:10.1016/j.ijrobp.2012.09.033
27. Lee AWM, Tung SY, Chan ATC, et al. Preliminary results of a randomized study (NPC-9902 Trial) on therapeutic gain by concurrent chemotherapy and/or accelerated fractionation for locally advanced nasopharyngeal carcinoma. Int J Radiat Oncol Phys. 2006;66(1):142–151. doi:10.1016/j.ijrobp.2006.03.054
28. Chen AM, Lee NY, Yang CC, et al. Comparison of intensity-modulated radiotherapy using helical tomotherapy and segmental multileaf collimator-based techniques for nasopharyngeal carcinoma: dosimetric analysis incorporating quality assurance guidelines from RTOG 0225. Technol Cancer Res Treat. 2010;9(3):291–298. doi:10.1177/153303461000900308
29. Lee AWM, Ngan RKC, Tung SY, et al. Preliminary results of trial NPC-0501 evaluating the therapeutic gain by changing from concurrent-adjuvant to induction-concurrent chemoradiotherapy, changing from fluorouracil to capecitabine, and changing from conventional to accelerated radiotherapy fractionation in patients with locoregionally advanced nasopharyngeal carcinoma. Cancer. 2015;121(8):1328–1338. doi:10.1002/cncr.29208
30. Blanchard P, Anne L, Marguet S, et al. Chemotherapy and radiotherapy in nasopharyngeal carcinoma: an update of the MAC-NPC meta-analysis. Lancet Oncol. 2015;16(6):645–655. doi:10.1016/S1470-2045(15)70126-9
31. Chen YP, Ismaila N, Chua MLK, et al. Chemotherapy in combination with radiotherapy for definitive-intent treatment of stage II-IVA nasopharyngeal carcinoma: CSCO and ASCO Guideline. J Clin Oncol. 2021;39:840–849. doi:10.1200/JCO.20.03237
32. Majed LR, Marguet S, Lee AWM, et al. What is the best treatment of locally advanced nasopharyngeal carcinoma? An individual patient data network meta-analysis. J Clin Oncol. 2017;35(5):498–505. doi:10.1200/JCO.2016.67.4119
33. Lee AWM, Ngan RKC, Ng WT, et al. NPC-0501 trial on the value of changing chemoradiotherapy sequence, replacing 5-fluorouracil with capecitabine, and altering fractionation for patients with advanced nasopharyngeal carcinoma. Cancer. 2020;126(16):3674–3688. doi:10.1002/cncr.32972
34. Zhang Y, Chen L, Hu GQ, et al. Gemcitabine and cisplatin induction chemotherapy in nasopharyngeal carcinoma. N Engl J Med. 2019;381(12):1124–1135. doi:10.1056/NEJMoa1905287
35. Chan ATC, Leung SFL, Ngan RKC, et al. Overall survival after concurrent cisplatin–radiotherapy compared with radiotherapy alone in locoregionally advanced nasopharyngeal carcinoma. J Natl Can Ins. 2005;97(7):536–939. doi:10.1093/jnci/dji084
36. Choi HCW, Chan SK, Lam KO, et al. The most efficacious induction chemotherapy regimen for locoregionally advanced nasopharyngeal carcinoma: a network meta-analysis. Front Oncol. 2021;11:626145. doi:10.3389/fonc.2021.626145
37. Lee AW, Ma BB, Ng WT, Chan AT. Management of nasopharyngeal carcinoma: current practice and future perspective. J Clin Oncol. 2015;33(29):3356–3364. doi:10.1200/JCO.2015.60.9347
38. Hong S, Zhang Y, Yu G, et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin as first-line therapy for recurrent or metastatic nasopharyngeal carcinoma: final overall survival analysis of GEM20110714 Phase III study. J Clin Oncol. 2021;39(29):3273–3282. doi:10.1200/JCO.21.00396
39. Liu YP, Wen YH, Tang J, et al. Endoscopic surgery compared with intensity-modulated radiotherapy in resectable locally recurrent nasopharyngeal carcinoma: a multicentre, open-label, randomized, controlled, phase 3 trial. Lancet Oncol. 2021;22(3):381–390. doi:10.1016/S1470-2045(20)30673-2
40. Tan LP, Tan GW, Sivanesan VM, et al. Systematic comparison of plasma EBV DNA, anti-EBV antibodies and miRNA levels for early detection and prognosis of nasopharyngeal carcinoma. Int J Cancer. 2020;146(8):2336–2347. doi:10.1002/ijc.32656
41. Peng L, Chen YP, Xu C, et al. A novel scoring model to predict benefit of additional induction chemotherapy to concurrent chemoradiotherapy in stage II-IVa nasopharyngeal carcinoma. Oral Oncol. 2018;86:258–265. doi:10.1016/j.oraloncology.2018.10.007
42. Chen BJ, Chapuy B, Ouyang J, et al. PD-L1 expression is characteristic of a subset of aggressive B-cell lymphomas and virus-associated malignancies. Clin Cancer Res. 2013;19(13):3462–3473. doi:10.1158/1078-0432.CCR-13-0855
43. Hsu MC, Hsiao JR, Chang KC, et al. Increase of programmed death-1-expressing intratumoral CD8 T cells predicts a poor prognosis for nasopharyngeal carcinoma. Mod Pathol. 2010;23(10):1393–1403. doi:10.1038/modpathol.2010.130
44. Xiao M, Qi F, Chen X, et al. Functional polymorphism of cytotoxic T-lymphocyte antigen 4 and nasopharyngeal carcinoma susceptibility in a Chinese population. Int J Immunogen. 2010;37(1):27–32. doi:10.1111/j.1744-313X.2009.00888.x
45. Balar AV, Weber JS. PD-1 and PD-L1 antibodies in cancer: current status and future directions. Cancer Immunol Immunother. 2017;66(5):551–564. doi:10.1007/s00262-017-1954-6
46. Ott PA, Bang YJ, Piha-Paul SA, et al. T-cell-inflamed gene-expression profile, programmed death ligand 1 expression, and tumor mutational burden predict efficacy in patients treated with pembrolizumab across 20 cancers: KEYNOTE-028. J Clin Oncol. 2019;37(4):318–327. doi:10.1200/JCO.2018.78.2276
47. Ma BBY, Lim WT, Goh BC, et al. Antitumor activity of nivolumab in recurrent and metastatic nasopharyngeal carcinoma: an international, multicenter study of the mayo clinic Phase 2 Consortium (NCI-9742). J Clin Oncol. 2018;36(14):1412–1418. doi:10.1200/JCO.2017.77.0388
48. Chan ATC, Lee VHF, Ahn M, et al. Results of KEYNOTE-122: a phase III study of pembrolizumab (pembro) monotherapy vs chemotherapy (chemo) for platinum-pretreated, recurrent or metastatic (R/M) nasopharyngeal carcinoma (NPC). Ann Oncol. 2021;32(supple5):S786–S817. doi:10.1016/j.annonc.2021.08.1268
49. Mai HQ, Chen QY, Chen D, et al. Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: a multicenter randomized phase 3 trial. Nat Med. 2021;27(9):1536–1543. doi:10.1038/s41591-021-01444-0
50. Yang Y, Qu S, Li J, et al. Camrelizumab versus placebo in combination with gemcitabine and cisplatin as first-line treatment for recurrent or metastatic nasopharyngeal carcinoma (CAPTAIN-1st): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2021;22(8):1162–1174. doi:10.1016/S1470-2045(21)00302-8
51. Lau KM, Cheng SH, Lo KW, et al. Increase in circulating Foxp3+CD4+CD25(high) regulatory T-cells in nasopharyngeal carcinoma patients. Br J Cancer. 2007;96(4):617–622. doi:10.1038/sj.bjc.6603580
52. Yip WK, Abdullah MA, Yusoff SM, et al. Increase in tumour-infiltrating lymphocytes with regulatory T-cell immunophenotypes and reduced zeta-chain expression in nasopharyngeal carcinoma patients. Clin Exper Immunol. 2010;155(3):412–422. doi:10.1111/j.1365-2249.2008.03793.x
53. Hong M, Tang K, Qian J, et al. Immunotherapy for EBV-associated nasopharyngeal carcinoma. Crit Rev Oncog. 2018;23(3–4):219–234. doi:10.1615/CritRevOncog.2018027528
54. Lutzky VP, Corban M, Heslop L, et al. Novel approach to the formulation of an Epstein-Barr virus antigen-based nasopharyngeal carcinoma vaccine. J Virol. 2010;84(1):407–417. doi:10.1128/JVI.01303-09
55. Li F, Song D, Lu Y, et al. Delayed-type hypersensitivity (DTH) immune response related with EBV-DNA in nasopharyngeal carcinoma treated with autologous dendritic cell vaccination after radiotherapy. J Immunother. 2013;36(3):208–214. doi:10.1097/CJI.0b013e31828bd87b
56. Lin CL, Lo WF, Lee TH, et al. Immunization with Epstein-Barr virus (EBV) peptide-pulsed dendritic cells induces functional CD8+ T-cell immunity and may lead to tumor regression in patients with EBV-positive nasopharyngeal carcinoma. Cancer Res. 2002;62(23):6952–6958.
57. Chen X, Liang R, Zhu X. Anti-EGFR therapies in nasopharyngeal carcinoma. Biomed Pharmacother. 2020;131:110649. doi:10.1016/j.biopha.2020.110649
58. Xu T, Liu Y, Dou S, et al. Weekly cetuximab concurrent with IMRT aggravated radiation-induced oral mucositis in locally advanced nasopharyngeal carcinoma: results of a randomized phase II study. Oral Oncol. 2015;51(9):875–879. doi:10.1016/j.oraloncology.2015.06.008
59. Wang F, Jiang C, Sun ZYQ, et al. Efficacy and safety of nimotuzumab plus radiotherapy with or without cisplatin-based chemotherapy in an elderly patient subgroup (Aged 60 and older) with nasopharyngeal carcinoma. Trans Oncol. 2018;11(2):338–345. doi:10.1016/j.tranon.2018.01.013
60. Zhao C, Miao J, Shen G, et al. Anti-epidermal growth factor receptor (EGFR) monoclonal antibody combined with cisplatin and 5-fluorouracil in patients with metastatic nasopharyngeal carcinoma after radical radiotherapy: a multicentre, open-label, phase II clinical trial. Ann Oncol. 2019;30(4):637–643. doi:10.1093/annonc/mdz020
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.