Back to Journals » Journal of Hepatocellular Carcinoma » Volume 9
Advanced Hepatocellular Carcinoma in Adults Without Cirrhosis: A Single-Institution Retrospective Review
Authors Altshuler E ![]() , Richhart R, Aryan M, King W, Pan K, Mathavan A, Mathavan A, Rodriguez D, Paudel B
, Richhart R, Aryan M, King W, Pan K, Mathavan A, Mathavan A, Rodriguez D, Paudel B ![]() , Northern N, Ramnaraign B, Sahin I, Fabregas, JC
, Northern N, Ramnaraign B, Sahin I, Fabregas, JC
Received 19 August 2022
Accepted for publication 22 October 2022
Published 19 December 2022 Volume 2022:9 Pages 1299—1307
DOI https://doi.org/10.2147/JHC.S384438
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmed Kaseb
Ellery Altshuler,1 Raymond Richhart,1 Mahmoud Aryan,2 William King,1 Kelsey Pan,1 Akash Mathavan,1 Akshay Mathavan,1 Diana Rodriguez,1 Bishal Paudel,1 Nathan Northern,1 Brian Ramnaraign,3 Ilyas Sahin,3 Jesus C Fabregas3
1Department of Internal Medicine, University of Florida College of Medicine, Gainesville, FL, USA; 2Department of Internal Medicine, University of Alabama Birmingham College of Medicine, Birmingham, AL, USA; 3Division of Hematology and Oncology, University of Florida College of Medicine, Gainesville, FL, USA
Correspondence: Jesus C Fabregas, Department of Hematology and Oncology, University of Florida College of Medicine, 1600 SW Archer Road, Gainesville, FL, 32608, USA, Tel +1 305-389-6231, Email [email protected]
Background: Although up to one in five cases of hepatocellular carcinoma (HCC) occurs in patients without cirrhosis, there is scarce literature characterizing non-cirrhotic HCC (NCHCC). Existing NCHCC research is primarily limited to surgical case series and there is a lack of data on unresectable NCHCC.
Aim: The purpose of this retrospective review was to compare the characteristics of unresectable NCHCC and cirrhotic hepatocellular carcinoma (CHCC).
Methods: A retrospective chart review of adult patients with unresectable HCC treated from 2007 to 2017 was performed at the University of Florida Shands Hospital. The data set was stratified into two cohorts: NCHCC and CHCC. Continuous variables were compared using Wilcoxon-Mann–Whitney tests and Kruskal–Wallis rank-sum tests. Categorical variables were compared using Pearson’s Chi-squared tests and Fisher’s exact tests. Overall survival was explored utilizing the Kaplan-Meier and log-rank method.
Results: There were 1494 adult patients included in the final analysis, including 264 patients (17.7%) with NCHCC and 1230 patients (82.3%) with CHCC. Median age was 61.0 years old and median follow-up time was 30.2 months. NCHCC patients were older than CHCC patients (66.3 years vs 61.9 years; p < 0.0001). NHCC tumors were larger than CHCC tumors (7.92 ± 4.85 vs 4.38 ± 3.12 cm; p < 0.0001) and more likely to be associated with distant metastases (23.35% vs 15.91%; p = 0.0055). There was no difference in overall survival, with a median of 23.5 months in NCHCC and 22.4 months in CHCC (p = 0.9196).
Conclusion: Our findings suggest that unresectable NCHCC and CHCC have unique characteristics but similar overall survival. To the best of our knowledge, this is the largest comparison of CHCC and NCHCC.
Keywords: hepatocellular carcinoma, cirrhosis, non-cirrhotic
Introduction
Liver cancer is the sixth most common malignancy globally and the third most common cause of cancer-related death.1 About 90% of liver malignancies are classified as hepatocellular carcinoma (HCC).2 Prevalence is highest in places with high rates of hepatitis B virus (HBV) and hepatitis C virus (HCV).3 While most HCC develops in the background of long-standing cirrhosis, non-cirrhotic HCC (NCHCC) accounts for up to 20% of all cases.4 The mechanisms by which HCC arises in cirrhotic and non-cirrhotic patients may be both be related to states of chronic inflammation, though inherited diseases, germline mutations, and genotoxic substances likely play a more important role in NCHCC.3 Additionally, chronic inflammation, in the form of non alcoholic fatty liver disease, for example, may contribute to the development of HCC in patients who have not yet developed cirrhosis.4 While the proportion of NCHCC is expected to increase, this subgroup has not been extensively characterized.4 The main clinical characteristics, treatment patterns and prognosis of NCHCC are relatively unknown. Moreover, it is unclear if there is a difference in survival as compared with CHCC. Surgical resection is the mainstay of curative-intent treatment in NCHCC.3 Because non-tumoral hepatocytes are relatively normal in NCHCC, the risk of liver failure after resection is much lower than in the setting of CHCC.5,6 When NCHCC is resectable, 5-year survival rates are 40–70%.7 Because most patients without cirrhosis do not receive screening for HCC, however, diagnosis is often made in an advanced disease state.3
Because most literature on NCHCC comes from surgical studies, there is a lack of data on unresectable NCHCC.2,5,6 To fill this research gap, we reviewed all cases of unresectable NCHCC at our hospital over a ten-year period. The purpose of this retrospective review was to define the characteristics and long-term outcomes of unresectable NCHCC and compare them to CHCC.
Materials and Methods
Design
A retrospective chart review of adult patients treated from 2007 to 2017 was performed at the University of Florida Shands Hospital, a large academic tertiary care medical center in Gainesville, Florida, USA. Patients were identified using the ICD 10 code (International classification of diseases, 10th revision) of HCC (C22.0) and were included only if their tumor was considered unresectable Approval for this study was obtained from the University of Florida Institutional Review Board.
Patient Population and Data Collection
Our study population included adult patients 18 years and older. Demographic information included age at diagnosis, sex, race, body mass index (BMI), and smoking status. Records were evaluated for prior diagnoses of diabetes mellitus type 2, coronary artery disease, and hypertension.
For patients with cirrhosis, the etiology was recorded. The presence of cirrhosis complications, including esophageal varices, spontaneous bacterial peritonitis, hepatic encephalopathy, and hepatorenal syndrome were documented. Baseline labs and Child-Pugh scores were recorded from the time of HCC diagnosis. Tumor characteristics, treatment modalities, and cancer outcomes were also noted. Patients were excluded if follow-up period was under two years or if records were incomplete.
Statistical Analysis
Statistical review was performed by Hanzhi Gao, a biostatistician from the University of Florida College of Medicine. The data set was stratified into two cohorts: NCHCC and CHCC. Raw comparisons were made between the groups in terms of demographics, past medical history, labs at HCC diagnosis, and other HCC-related data. Continuous variables were compared using Wilcoxon-Mann–Whitney tests and Kruskal–Wallis rank-sum tests. Categorical variables were compared using Pearson’s Chi-squared tests and Fisher’s exact tests. Overall survival was explored utilizing the Kaplan-Meier and log-rank method. Univariate survival analysis was performed with Cox regression analyses. All statistical tests were two-sided, and the significance level was set at 0.05. Analyses were conducted using SPSS 28.0.1.0 (142) (IBM Corp, Armonk, NY).
Results
Patient Characteristics
Between 2007 and 2017, there were 1494 adult patients treated for unresectable HCC at the University of Florida Health system for whom adequate records existed. Among these patients, 264 (17.7%) had NCHCC while 1230 (82.3%) had CHCC. For all patients, median age was 61.0 years old and median follow-up time was 30.2 months. Characteristics of patients with NCHCC and CHCC are provided in Table 1. Among the 1230 patients with cirrhosis, there were 716 patients (58.2%) with hepatitis C cirrhosis, 143 patients (11.6%) with alcoholic cirrhosis, and 63 patients (5.1%) with NASH cirrhosis. There were 9 patients (0.8%) with autoimmune hepatitis and 7 patients (0.6%) with alpha-1 antitrypsin deficiency. The remaining 292 patients (23.7%) had cirrhosis that was either described as either multifactorial, cryptogenic, or unspecified.
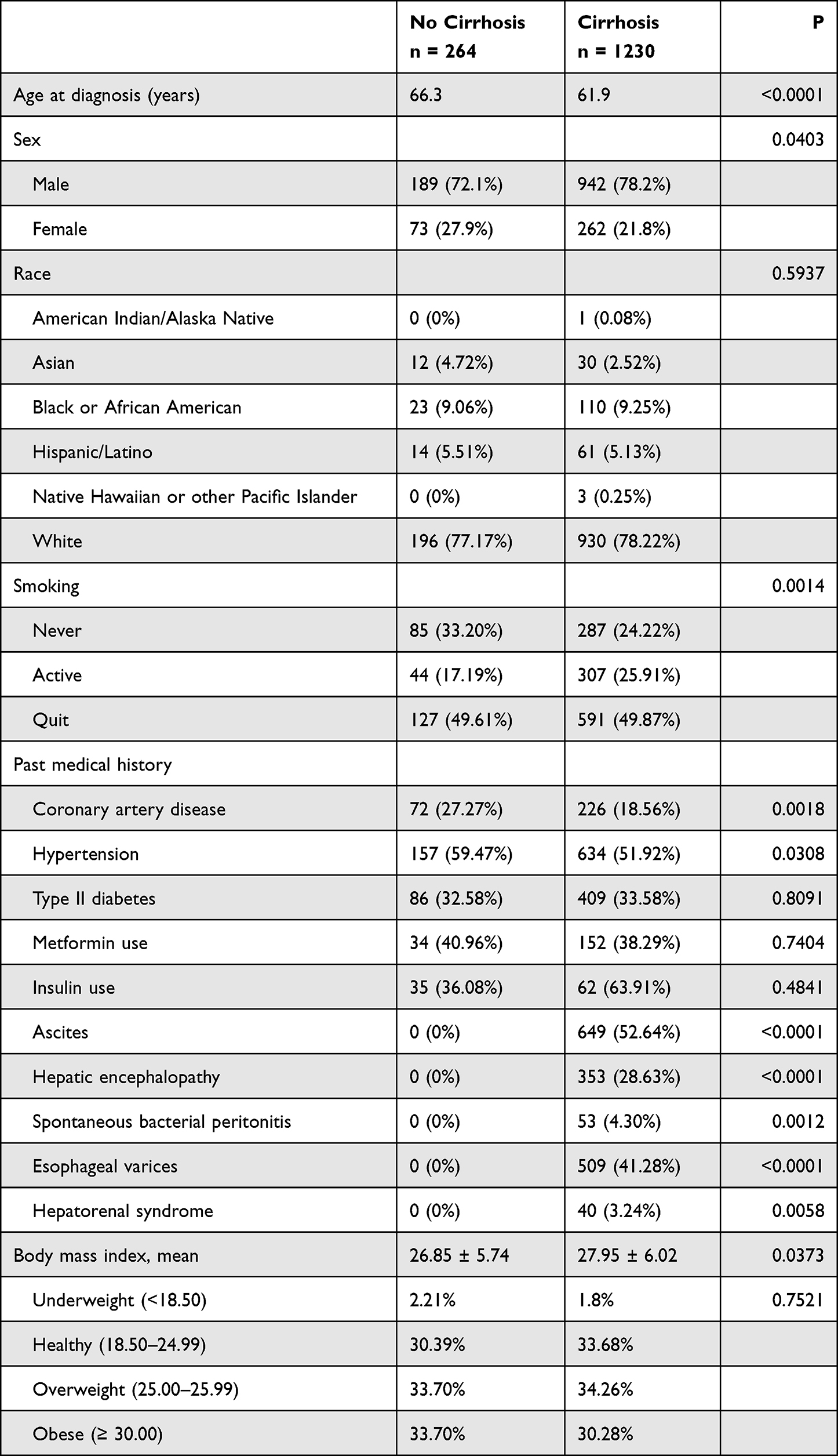 |
Table 1 Baseline Characteristics of Hepatocellular Carcinoma Patients with and without Cirrhosis |
Male predominance was higher in CHCC than in NCHCC (78.2% vs 72.1%; p = 0.0403), corresponding roughly to ratios of 3.5:1 in CHCC and 2.5:1 in NCHCC, respectively. Stigmata of decompensated cirrhosis were not found in the medical history of any NCHCC patient: 0 patients with NCHCC had a history of ascites, hepatic encephalopathy, spontaneous bacterial peritonitis, esophageal varices, or hepatorenal syndrome.
NCHCC patients were more likely than CHCC patients to have a history of coronary artery disease (27.27% vs 18.56%; p = 0.0018) and hypertension (59.47 vs 51.92%; p = 0.0308). Patients with NCHCC were also more likely to have never smoked (33.20% vs 24.22%; p = 0.00014). Mean BMI was slightly higher in patients with CHCC than in NCHCC (27.95 vs 26.85; p = 0.0373). There was no significant difference in diagnosis of type II diabetes (p = 0.8091), metformin use (p = 0.7404), or insulin use (p = 0.4841).
On average, NCHCC patients were older than CHCC patients (66.3 years vs 61.9 years; p < 0.0001). However, the age distribution in NCHCC was bimodal (Figure 1). There was a higher proportion of NCHCC patients in the youngest two age groups, those aged 18–29 (3.0% vs 0.40%; p < 0.0001) and 30–39 (4.6% vs 1.0%; p < 0.0001), and also in the oldest two age groups, patients aged 70–79 (35.5% vs 15.5%; p < 0.0001), and 80 and above (12.2% vs 3.5%; p < 0.0001).
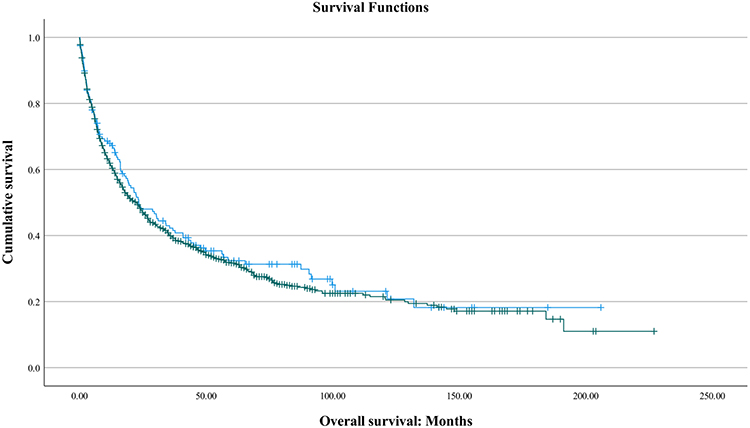 |
Figure 1 Age distribution of patients without (left) and with (right) cirrhosis. A bimodal age distribution is observed in NCHCC. Patients with NCHCC had higher proportions of patients in the youngest two age groups, those aged 18–29 (3.0% vs 0.40%; p <0.0001) and 30–39 (4.6% vs 1.0%; p < 0.0001) also in the oldest two age groups, those aged 70–79 (35.5% vs 15.5%; p < 0.0001), and 80 and above (12.2% vs 3.5%; p < 0.0001). On average, patients with NCHCC were older than patients with CHCC (66.3 years vs 61.9 years; p < 0.0001). |
Disease Characteristics
NCHCC tumors were larger than those of CHCC (7.92 ± 4.85 vs 4.38 ± 3.12 cm; p < 0.0001) (Table 2). Patients with NCHCC were more likely to present with distant metastases (23.35% vs 15.91%; p = 0.0055). On laboratory evaluation, NCHCC were associated with higher sodium levels (138.0 5± 3.78 vs 137.16 ± 4.14; p = 0.0014), higher platelets (248.99 ± 122.06 vs 133.01 ± 80.07; p < 0.0001), lower bilirubin (1.1 9± 2.88 vs 1.76 ± 2.43; p = <0.0001), and lower INR (1.16 ± 0.32 vs 1.30 ± 0.63; p < 0.0001). There was no significant difference in AFP in NCHCC and CHCC at the time of diagnosis (5950.14 ng/mL ± 16,471.02 ng/mL vs 3856.5 6 ng/mL ± 20,128.45 ng/mL; p = 0.8015) or at the time of disease progression (1989.17 ng/mL ± 3841.81 ng/mL vs 67,607.99 ng/mL ± 734,541.70 ng/mL; p = 0.6438). As compared to CHCC, NCHCC was less likely to be treated with TACE (32.8% vs 49.7%; p < 0.0001). There was no difference in likelihood of receiving Y-90 (19.5% vs 20.9%; p = 0.6363). A lower percentage of patients with NCHCC received systemic therapy; however, this difference was not significant (18.9% vs 22.0%; p = 0.0562).
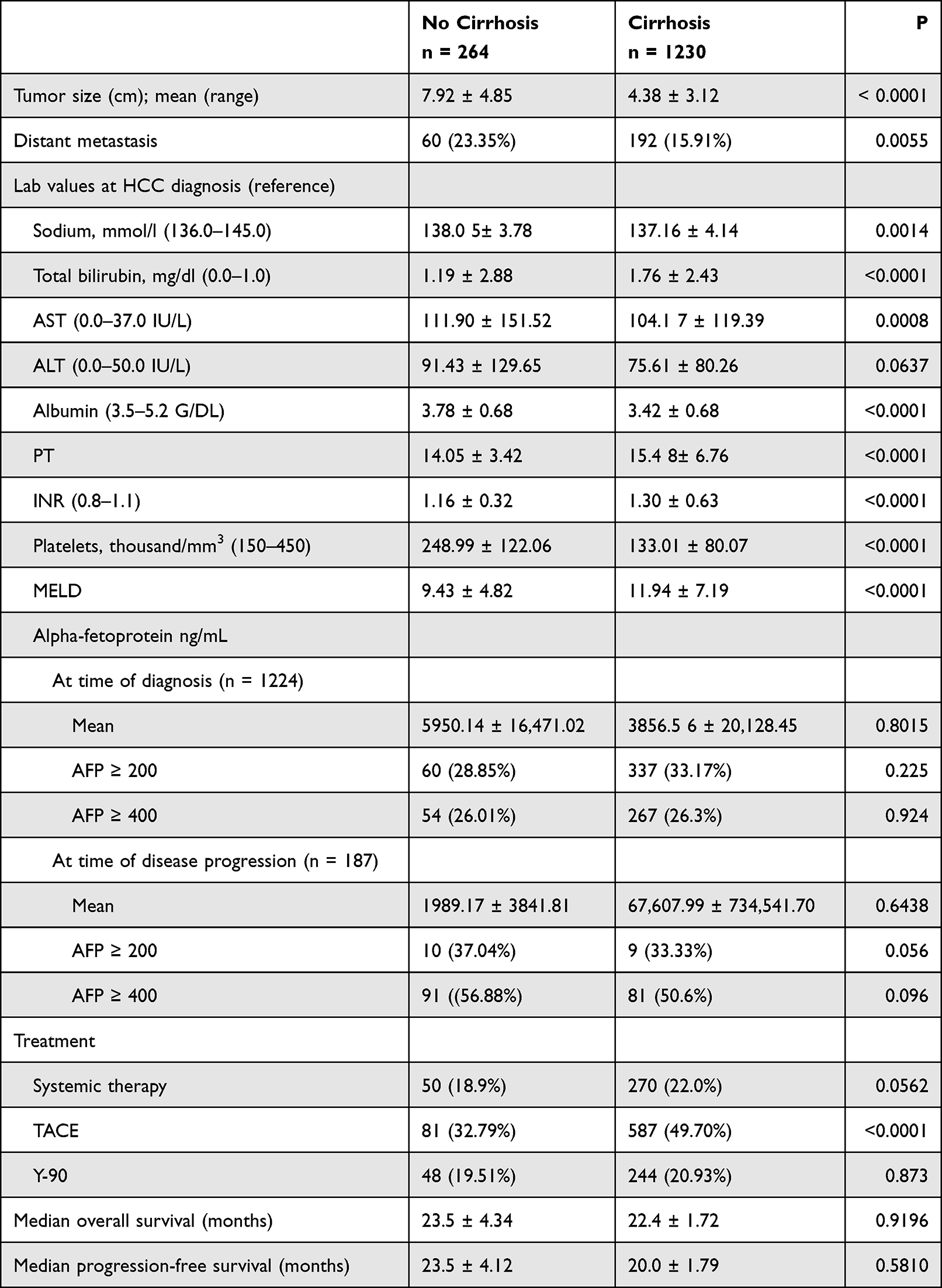 |
Table 2 Hepatocellular Carcinoma Disease Characteristics |
Survival Analysis
There was no significant difference in overall survival, which was 23.5 ± 4.43 months in NCHCC and 22.4 ± 1.72 months in CHCC (p = 0.9196) (Table 3, Figure 2). There was also no difference in median progression-free survival, which was 23.5 ± 4.12 months in NCHCC and 20.0 ± 1.79 months in CHCC (p = 0.581). On univariate analysis of NCHCC, increased risk of death was observed with age ≥65 (HR 1.605, 95% CI: 1.059–2.431; p = 0.023). For patients with CHCC, increased risk of death was observed with size ≥3.5 cm (HR 1.558, 95% CI: 1.318–1.814; p < 0.0001), BMI (HR 1.250, 95% CI: 1.028–1.519; p = 0.028), and age ≥65 (HR 1.204, 95% CI: 1.020–1.422; p = 0.030).
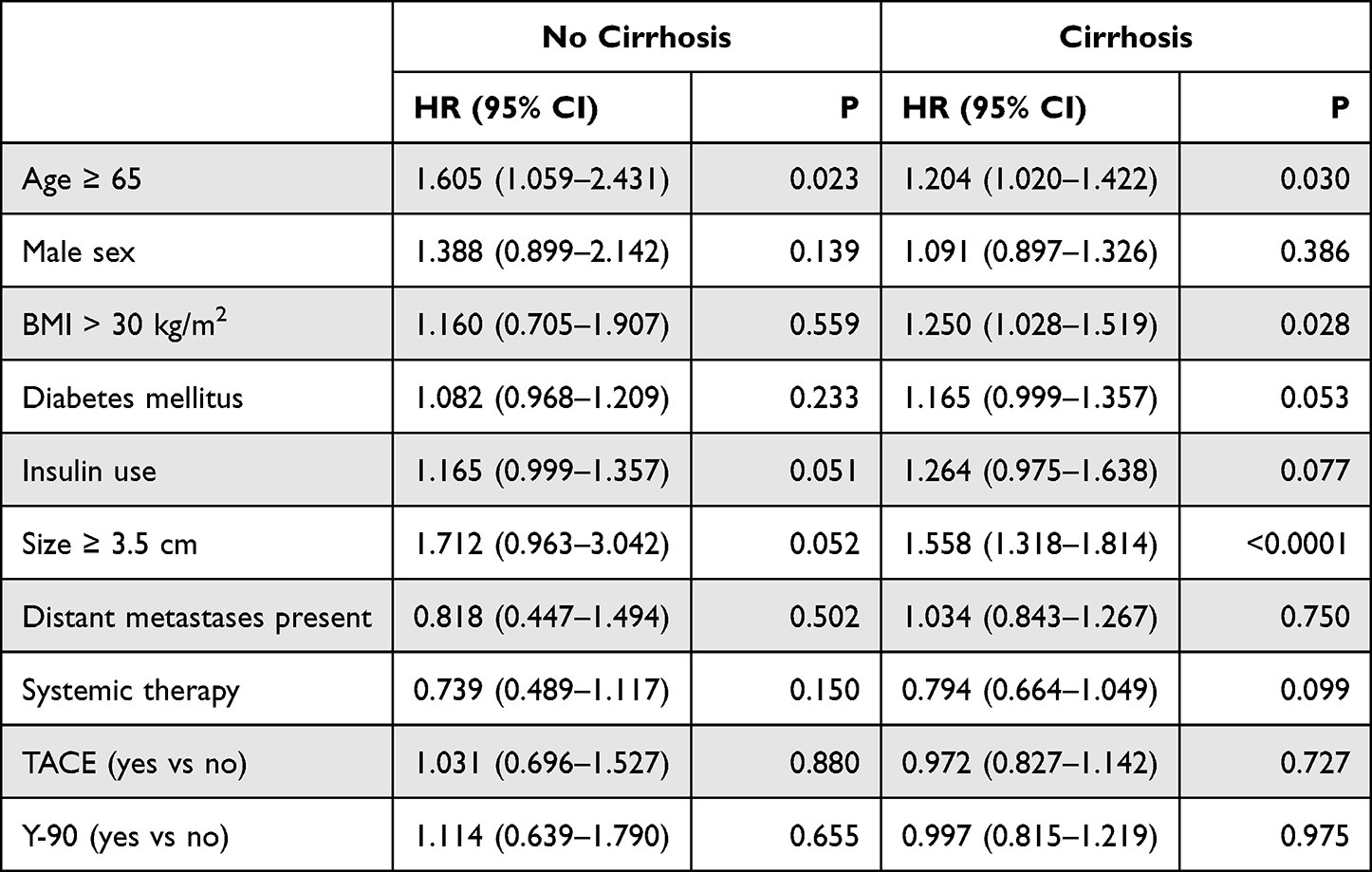 |
Table 3 Univariate Survival Analysis |
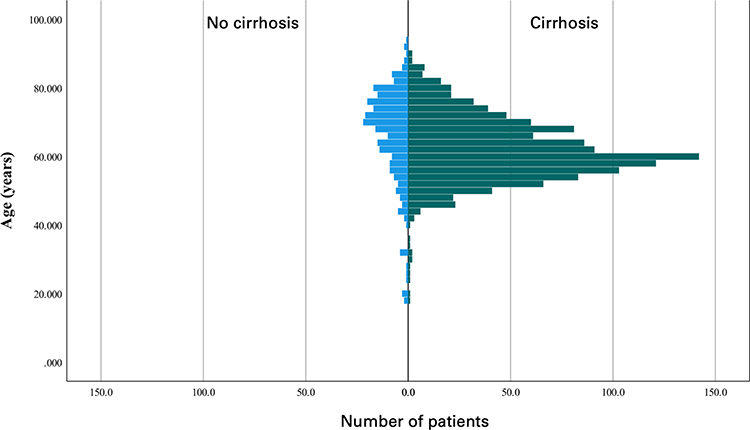 |
Figure 2 Kaplan-Meier survival curve depicting outcomes for patients with no cirrhosis (blue) and cirrhosis of any etiology (green). The curve shows that there was no significant difference in overall survival between groups. Median overall survival was 23.5 ± 4.34 months for patients without cirrhosis and 22.4 ± 1.72 months for patients with cirrhosis (p = 0.9196). |
Discussion/Conclusion
In this retrospective study, there was no statistically significant difference in OS between NCHCC and CHCC. Most literature on NCHCC has focused on resectable cases and, as a result, unresectable NCHCC has not been well studied. In this retrospective review, we collected data on cases of unresectable HCC and analyzed factors associated with NCHCC. To the best of our knowledge, this study is the largest analysis of NCHCC conducted to date. Our evidence supports some previously identified trends among unresectable NCHCC but also contradicts certain findings. Our data emphasize the need to understand NCHCC and CHCC as distinct entities with unique patient populations and disease characteristics.
Although NCHCC were larger and more likely to be associated with distant metastases, there was no difference in overall survival. This finding differs from the largest previously conducted analyses of NCHCC and CHCC, which took place in Germany and the Netherlands. In a German analysis of 1066 HCC including both resectable and unresectable disease, Weinmann and colleagues reported that NCHCC had an increased OS of 25.9 vs 14.3 months (P=0.0013).8 Likewise, in an unselected Dutch cohort including 1221 HCC, van Meer and colleagues reported superior outcomes in NCHCC, with the absence of cirrhosis carrying a hazard ratio of 0.49 (0.38–0.63). Two older, smaller studies also found improved outcomes in NCHCC.9,10 By contrast, a study of 571 patients by Shute and colleagues did not report a difference in survival between CHCC and NCHCC.5 Of note, in the same cohort, NCHCC tumors twice as large as CHCC tumors (8 cm vs 4 cm), a finding replicated in our cohort.11 The larger tumor size and higher prevalence of metastases in both our cohort and the Dutch cohort is likely due in part to the lack of HCC screening in patients without cirrhosis.12
The patient characteristics in our cohort were similar to those reported previously. As a percentage of the whole, NCHCC accounted for 17.7% of all cases, a similar proportion to the 15–20% reported in unselected HCC cohorts in Western countries,5,8,11,13–15 though higher proportions have been reported in surgical case series.16 In Africa and Asia, where rates of hepatitis B and C are higher and CHCC is more common, the proportion of NCHCC is likely lower.3,17 Previous studies have suggested a male predominance of around 75% in NCHCC and 85% in CHCC.11,18 Our cohort was similar, with a male predominance of 72% in NCHCC and 78% in CHCC. NCHCC has been reported to have a bimodal age distribution and CHCC a normal age distribution,19 this also being the case in our cohort: compared to CHCC, patients with NHCC had higher proportions of the youngest and oldest patients.
It has been suggested that NCHCC represents cancer arising in a damaged liver in a pathophysiological process similar to that seen in CHCC. Based on a small review of NCHCC at their institution, Schute and colleagues concluded that most cases of NCHCC are the result of liver damage sustained due to metabolic syndrome.5 They suggest that while patients with metabolic syndrome may not meet criteria for cirrhosis, the chronic liver damage due to non-alcoholic fatty liver disease (NAFLD) leads to HCC.5 To support this claim, they reference the fact that diabetes has been established as a risk factor for HCC.5,20 They also point out that many patients with NCHCC had severe liver dysfunction (more than a fifth had ascites) and therefore may have had undiagnosed NAFLD.5 Another explanation is that there was undiagnosed compensated cirrhosis in the NCHCC group.
In our cohort of NCHCC, it is unlikely that there were many cases of undiagnosed decompensated cirrhosis; none had a history of ascites, hepatic encephalopathy, spontaneous bacterial peritonitis, or esophageal varices. It is possible, however, that cases of asymptomatic compensated cirrhosis were missed. There were few signs of undiagnosed NAFLD, either, in our cohort: there were no differences in metformin use, insulin use, or rates of obesity between NCHCC and CHCC, and BMI was lower in NCHCC, though the presence of ascites in the CHCC group may have contributed to this. Based on our data, we conclude that NCHCC may arise in the absence of chronic inflammation associated with CHCC.
The pathophysiological etiologies of NCHCC and CHCC have been better elucidated in recent years and support the theory that the two arise from distinct mechanisms. CHCC is characterized by p53 alterations, often as a result of aberrant Wnt/β-catenin hyperactivation.21 NCHCC is more frequently associated with inactivation of global gene methylation, p14 inactivation, and p21 overexpression.21 In short, CHCC represents a stepwise process involving an insult, regenerative nodules, and dysplasia, leading to cancer while NCHCC represents de novo carcinogenesis.22
Our study had several limitations. For one, the retrospective nature makes it impossible to draw causal inferences. Tumor grade and definitive stage were not recorded and could represent confounding variables not accounted in the analysis and represent major limitations to the study. Rates of viral hepatitis and alcohol use disorder were not gathered in the NHCC population, thus making it difficult to assess the rate of subclinical liver damage in the patients. Additionally, our data set comes from the time before the onset of the immunotherapy era. Since the approval of combination atezolizumab and bevacizumab in 2020, unresectable HCC treatment has now changed and this change is not reflected in our data set. Importantly, the diagnosis of cirrhosis was not definitively excluded in all patients in the NCHCC group; thus making distinctions between the groups less reliable. Finally, NCHCC had a bimodal age distribution but was treated as a homogenous group although older and younger patients likely have distinct clinical characteristics.
Our findings suggest that unresectable NCHCC and CHCC have unique characteristics but similar overall survival. We found that NCHCC tumors were nearly twice as large as CHCC tumors and more likely to present with distance metastases. In contrast to previous analyses of NCHCC, we found no survival difference between NCHCC and CHCC. To the best of our knowledge, this analysis represents the largest comparison of CHCC and NCHCC.
Data Sharing Statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Statement of Ethics
This study has been granted an exemption from requiring ethics approval. Patient consent was not required by the IRB as all data was deidentified and the study was retrospective and involved no intervention. Patient data and confidentiality were respected in accordance with the Declaration of Helsinki.
Study Approval Statement
This study protocol was reviewed and approved by the University of Florida Internal Review Board. This study has been granted an exemption from requiring ethics approval.
Author Contributions
Ellery Altshuler and Raymond Ricchart designed the study. Mahmoud Aryan participated in the acquisition analysis and interpretation of the data. Ellery Altshuler, Diana Rodriguez, Nathan Norther, Bishal Paudel, Brian Ramnaraign, Ilyas Sahin, and Jesus Fabregas drafted the initial manuscript. Jesus Fabregas revised the article critically for important intellectual content. All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There are no funding sources.
Disclosure
Dr Jesus C Fabregas is part of the institutional research for Ipsen, BMS, Merck, Pfizer, Genentech, and Natera, outside the submitted work. The authors have no other conflicts of interest to declare in this work.
References
1. Zhuo Y, Chen Q, Chhatwal J. Hepatocellular carcinoma, translational precision medicine approaches. Mol Transl Med. 2019;5:53–67.
2. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. doi:10.1038/s41572-020-00240-3
3. Desai A, Sandhu S, Lai JP, Sandhu DS. Hepatocellular carcinoma in non-cirrhotic liver: a comprehensive review. World J Hepatol. 2019;11(1):1–18. doi:10.4254/wjh.v11.i1.1
4. Lee DH, Lee JM. Primary malignant tumours in the non-cirrhotic liver. Eur J Radiol. 2017;95:349–361. doi:10.1016/j.ejrad.2017.08.030
5. Schütte K, Schulz C, Poranzke J, et al. Characterization and prognosis of patients with hepatocellular carcinoma (HCC) in the non-cirrhotic liver. BMC Gastroenterol. 2014;14(1):117. doi:10.1186/1471-230X-14-117
6. Giannini EG, Marenco S, Bruzzone L, et al. Hepatocellular carcinoma in patients without cirrhosis in Italy. Digest Liver Dis. 2013;45(2):164–169. doi:10.1016/j.dld.2012.08.018
7. Mergental H, Adam R, Ericzon BG, et al. Liver transplantation for unresectable hepatocellular carcinoma in normal livers. J Hepatol. 2012;57(2):297–305. doi:10.1016/j.jhep.2012.03.022
8. Weinmann A, Koch S, Niederle IM, et al. Trends in epidemiology, treatment, and survival of hepatocellular carcinoma patients between 1998 and 2009. J Clin Gastroenterol. 2014;48(3):279–289. doi:10.1097/MCG.0b013e3182a8a793
9. Nzeako UC, Goodman ZD, Ishak KG. Hepatocellular carcinoma in cirrhotic and noncirrhotic livers: a clinico-histopathologic study of 804 North American Patients. Am J Clin Pathol. 1996;105(1):65–75. doi:10.1093/ajcp/105.1.65
10. Smalley SR, Moertel CG, Hilton JF, et al. Hepatoma in the noncirrhotic liver. Cancer. 1988;62(7):1414–1424. doi:10.1002/1097-0142(19881001)62:7<1414::AID-CNCR2820620729>3.0.CO;2-7
11. Meer S, Erpecum KJ, Sprengers D, et al. Hepatocellular carcinoma in cirrhotic versus noncirrhotic livers. Eur J Gastroen Hepat. 2016;28(3):352–359. doi:10.1097/MEG.0000000000000527
12. Desai A, Sandhu S, Lai JP, Sandhu DS. Hepatocellular carcinoma in non-cirrhotic liver: a comprehensive review. World J Hepatol. 2019;11(1):1–18.
13. Borie F, Bouvier A, Herrero A, et al. Treatment and prognosis of hepatocellular carcinoma: a population based study in France. J Surg Oncol. 2008;98(7):505–509. doi:10.1002/jso.21159
14. El-Serag HB. Hepatocellular Carcinoma. New Engl J Medicine. 2011;365(12):1118–1127. doi:10.1056/NEJMra1001683
15. Wörns MA, Bosslet T, Victor A, et al. Prognostic factors and outcomes of patients with hepatocellular carcinoma in non-cirrhotic liver. Scand J Gastroentero. 2012;47(6):718–728. doi:10.3109/00365521.2012.677952
16. Grazi GL, Cescon M, Ravaioli M, et al. Liver resection for hepatocellular carcinoma in cirrhotics and noncirrhotics. Evaluation of clinicopathologic features and comparison of risk factors for long‐term survival and tumour recurrence in a single centre. Aliment Pharm Therap. 2003;17(s2):119–129. doi:10.1046/j.1365-2036.17.s2.9.x
17. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–86. doi:10.1002/ijc.29210
18. Boudjema K, Compagnon P, DuPont-Bierre E, et al. Transplantation hépatique pour carcinome hépatocellulaire. Cancer Radiothérapie. 2005;9(6–7):458–463. doi:10.1016/j.canrad.2005.09.009
19. Perisetti A, Goyal H, Yendala R, Thandassery RB, Giorgakis E. Non-cirrhotic hepatocellular carcinoma in chronic viral hepatitis: current insights and advancements. World J Gastroentero. 2021;27(24):3466–3482. doi:10.3748/wjg.v27.i24.3466
20. Mazzotta AD, Pascale A, Cano L, et al. Number of hepatocellular carcinoma nodules in patients listed for liver transplantation within alpha‐fetoprotein score: a new prognostic risk factor. Transplant Int. 2021;34(5):954–963. doi:10.1111/tri.13858
21. Wang K, Qiu X, Zhao Y, Wang H, Chen L. The Wnt/β-catenin signaling pathway in the tumor microenvironment of hepatocellular carcinoma. Cancer Biol Med. 2022;19(3):305–318.
22. Gaddikeri S, McNeeley MF, Wang CL, et al. Hepatocellular carcinoma in the noncirrhotic liver. Am J Roentgenol. 2014;203(1):W34–47. doi:10.2214/AJR.13.11511
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Vitamin B6 Metabolic Pathway is Involved in the Pathogenesis of Liver Diseases via Multi-Omics Analysis
Mei M, Liu D, Tang X, You Y, Peng B, He X, Huang J
Journal of Hepatocellular Carcinoma 2022, 9:729-750
Published Date: 11 August 2022
Validation of Hepatocellular Carcinoma Risk Prediction Models in Patients with Hepatitis B-Related Cirrhosis
Cheng R, Xu X
Journal of Hepatocellular Carcinoma 2022, 9:987-997
Published Date: 12 September 2022
Sulfatase 2 Along with Syndecan 1 and Glypican 3 Serum Levels are Associated with a Prognostic Value in Patients with Alcoholic Cirrhosis-Related Advanced Hepatocellular Carcinoma
Mouhoubi N, Bamba-Funck J, Sutton A, Blaise L, Seror O, Ganne-Carrié N, Ziol M, N'Kontchou G, Charnaux N, Nahon P, Nault JC, Guyot E
Journal of Hepatocellular Carcinoma 2022, 9:1369-1383
Published Date: 28 December 2022
Identification of the Genotypes Circulating in the Ecuadorian Population Infected with the Hepatitis C Virus (HCV)
Moncayo M, Teran E, Reyes J, Yerovi G, Robalino M, Aguilar AC, Garzon-Chavez D
Risk Management and Healthcare Policy 2023, 16:1403-1409
Published Date: 3 August 2023
Comparison of Clinical Manifestations and Related Factors of Hepatocellular Carcinoma with Chronic Hepatitis B
Hou H, Liang L, Deng L, Ye W, Wen Y, Liu J
International Journal of General Medicine 2024, 17:2877-2886
Published Date: 25 June 2024