Back to Journals » Journal of Pain Research » Volume 18
Advanced Age as a Consideration in Spinal Cord Stimulation
Authors McCormick RJ, Schatman ME ![]() , Brenner GJ
, Brenner GJ
Received 30 October 2025
Accepted for publication 4 November 2025
Published 7 November 2025 Volume 2025:18 Pages 5911—5918
DOI https://doi.org/10.2147/JPR.S577787
Checked for plagiarism Yes
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Robert J McCormick,1 Michael E Schatman,2,3 Gary J Brenner1
1Department of Anesthesia, Critical Care, and Pain Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts, USA; 2Department of Anesthesiology, Perioperative Care and Pain Medicine, NYU Grossman School of Medicine, New York, NY, USA; 3Department of Population Health – Division of Medical Ethics, NYU Grossman School of Medicine, New York, NY, USA
Correspondence: Michael E Schatman, Department of Anesthesiology, Perioperative Care & Pain Medicine, NYU Grossman School of Medicine, 550 First Avenue, New York, NY, 10016, USA, Tel +1 425-647-4880, Email [email protected]
Introduction
The use of spinal cord stimulation (SCS) for the management of chronic pain involves the application of electrical stimulus to the dorsal aspect of the spinal cord. SCS carries FDA approval for several indications, including intractable low back and leg pain. The application of SCS involves the surgical placement of an insulated wire with multiple electrodes (known as leads), typically in the dorsal aspect of the epidural space, which are then connected to an implantable pulse generator (IPG), which is surgically implanted subcutaneously in the gluteal region. A permanent implant is generally performed subsequent to a successful “trial”, in which a SCS lead is placed percutaneously in the epidural space and connected to an external pulse generator, which is adhered to the patient’s back and worn for a trial period. Substantial pain relief, certainly greater than 50%, is generally considered necessary for a trial to be deemed successful.1,2
There are several commercially available SCS systems and a multitude of studies, including clinical trials, generally supporting the efficacy of SCS.1,2 However, the use of spinal cord stimulation for the management of chronic pain in the elderly is very poorly studied. Persons over the age of 80 are sometimes referred to as the “extreme elderly.”3 This population is expected to triple in size by 2050.4 Yet, clinical trials for SCS tend to focus on a much younger population, as a 2023 Cochrane review of 13 SCS clinical trials determined the average age of subjects in these trials to range from 47 to 59 years old.5 In some cases, the extreme elderly are explicitly excluded from clinical trials.6,7 Here, we describe a case of a patient who underwent an SCS trial and permanent SCS system implantation, both without complication, at age 96, continued analgesia reported nearly 7 years later.
Case Report
Note: The patient described in this report provided written consent prior to the initiation of the writing of the manuscript to have the details of his treatment and accompanying images published.
A 95-year-old male, VV, with a past medical history notable for prostate cancer managed with leuprolide as well as osteoporosis, initially presented to the Massachusetts General Hospital Center for Pain Medicine for evaluation of bilateral low back pain, which was worse on the right. His back pain had been present for approximately 1 year and reportedly began consequent to a compression fracture of the L2 vertebral body. The pain worsened in the setting of two additional compression fractures at L1 and L4 in the year prior to the initial pain clinic visit. Associated symptoms included bilateral hip pain, left buttock pain, and left anterolateral thigh numbness. He reported that his pain, which becomes quite severe with any activity, was having a significant impact on his ability to perform even basic activities of daily living. Eighteen months prior to the initial visit, he was able to ambulate independently without a walker and was also driving independently. By the time of the initial evaluation at our clinic, he required a walker to ambulate and was walking a maximum of 100 feet, and this only a few days per week. Additionally, he was leaving the house only for medical appointments, was no longer driving a car, and was sleeping in a hospital bed located in his living room as he could not ascend a flight of stairs to his bedroom. The patient stated that he had essentially no quality of life. His physical examination was notable for paraspinal and gluteal muscle tenderness to palpation, as well as exacerbation of his reported baseline pain with lumbar extension and rotation bilaterally. Neurologic examination of his lower extremities was unremarkable. MRI prior to initial visit, which had been obtained before the L4 compression fracture, was indicative of chronic compression fractures at L1 and L2, as well as multilevel degenerative changes in the lumbar spine and a grade 1 anterolisthesis at L4/L5 (Figure 1).
 |
Figure 1 Sagittal T2-weighted MRI of the lumbar spine, demonstrating compression fractures at L1 and L2, grade 1 anterolisthesis of L4 on L5, and multilevel disc desiccation and degenerative changes. |
Prior to his initial visit, VV had been previously evaluated for back pain by primary care, physiatry, spine surgery, rheumatology, and another pain management clinic. His pain was being managed with acetaminophen, a low dosage of gabapentin, a low dosage of tramadol, and topical lidocaine patches. Oxycodone had previously been prescribed but was discontinued due to side effects. He had previously completed physical therapy with reportedly limited benefit. Initial procedural interventions included right lumbar L3-L4, L4-L5, and L5-S1 medial branch blocks, as well as trigger point injections to the gluteal muscles. Initial diagnostic medial branch blocks were positive in that they provided greater than 80% relief of his right-sided low back pain. However, the patient later developed a deep venous thrombosis and pulmonary embolism, which required systemic anticoagulation with enoxaparin. It was thought that the risk of bleeding during the medial branch radiofrequency ablation (RFA) if anticoagulation was not held, as well as the risk of a cardioembolic event if anticoagulation were stopped, outweighed the potential benefit of this procedure. During this time, he presented to the emergency department for severe pain on multiple occasions and continued to experience functional decline at home despite additional medication trials, including pregabalin and duloxetine. Several months later when it became medically permissible to hold enoxaparin, he underwent right lumbar L3-L4, L4-L5, and L5-S1 medial branch radiofrequency ablations. Unfortunately, these were reportedly not effective in relieving his pain.
During this time (following the medial branch RFAs), VV again presented to the emergency department for pain control and was referred to palliative care for help with symptom management given his worsening pain. By this time, VV was spending essentially all his time in bed. Consequent to this pain-associated major decline in functional status and quality of life, the idea of palliative sedation was discussed, and additional opioid treatments were utilized, including tapentadol and another trial of oxycodone. Additional trigger point injections (VV had found the initial set to be helpful, albeit transiently) and muscle relaxants were trialed as well. As somewhat of a last resort prior to further considering palliative sedation, the possibility of spinal cord stimulation was discussed with VV and his family. They expressed interest in moving forward with this therapy, and he subsequently underwent a psychological evaluation prior to a SCS trial. During this consultation, he was diagnosed with an adjustment disorder, although no psychological contraindication to spinal cord stimulation was identified.
At the subsequent appointment, which was nine months after VV’s initial pain clinic visit, a spinal cord stimulator trial lead was placed percutaneously. The epidural space was accessed at the L1-L2 interlaminar space. A single lead was placed in the left paramedian aspect of the dorsal epidural space, with the active component of the lead spanning from the top of the T7 vertebral body to the bottom of the T8 vertebral body (Figure 2). At follow-up one week later, VV reported 80% relief of his pain during the trial rating his pain as 1/10 according to the numeric rating scale (NRS). During the period just prior to the SCS trial, VV had rated his maximum pain as 9–10/10 on the NRS, and scored his global impression of change during the trial as “much improved.” Based on these results, a decision was made to proceed with a permanent SCS implant.
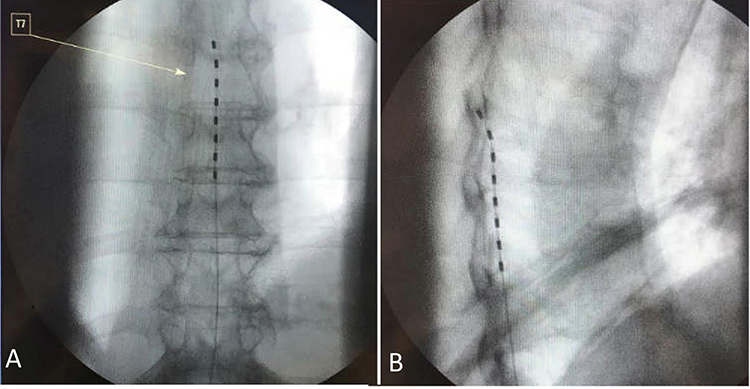 |
Figure 2 (A) AP fluoroscopic view of SCS trial lead placed in the epidural space spanning from the level of the top of the T7 vertebral body through the level of the bottom of the T8 vertebral body. (B) Lateral fluoroscopic view of SCS trial lead placed in the dorsal aspect of the epidural space. |
Three weeks later, at age 96, and approximately 10 months following the initial pain clinic visit, VV underwent surgical implantation of a SCS system. A decision was made to place only a single SCS lead to mitigate the risk of clinically significant bleeding associated with lead placement. The epidural space was again accessed via the L1-L2 interlaminar space. The SCS lead was placed in the midline of the dorsal epidural space spanning from the bottom of the T6 vertebral body to the T8 vertebral bodies (Figure 3). The IPG was implanted in the left gluteal region. There were no complications during or subsequent to the surgery.
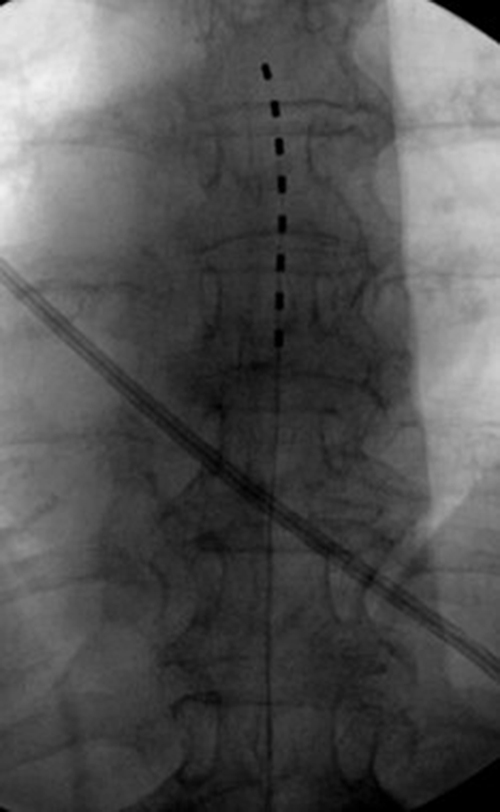 |
Figure 3 Intra-operative fluoroscopic image showing SCS permanent lead in the epidural space, spanning from the level of the middle of the T6 vertebral body through the level of the bottom of the T8 vertebral bodies. |
At one to two weeks post-implant, NRS pain scores ranged from 1–3/10. By one-month post-implant, he was able to ascend and descend stairs despite having developed a new compression fracture at L5, which was managed with kyphoplasty. At 2 months post-implant, his walking tolerance had improved to 800 feet, and he was able to discard his home hospital bed and resume sleeping in his upstairs bedroom full-time. At 4 months, he was able to walk around the block and had been tapered off pregabalin. By 18 months post-implant, his walking tolerance had improved to 5 minutes, which he was doing several days per week. He also had resumed activities he enjoyed such as going to restaurants and staying in hotels. At 22 months post-implant, his walking tolerance was up to 15 minutes, and he began using a stationary bike. He continues to follow with our pain clinic for intermittent SCS re-programming, as well as undergoing trigger point injections of the thoracic and lumbosacral musculature – the latter at VV’s request and his good response to the intervention.
Approximately 2 years post-SCS implant, his internal pulse generator (IPG) displayed an “end of life message”, and required replacement. He underwent IPG replacement without complication. VV experienced mild IPG site discomfort shortly after initial replacement, but this resolved over time. Otherwise, he has reportedly not experienced issues related to the SCS system.
Currently, VV is nearly 103 years old and close to 7 years removed from SCS implantation. He continues to undergo regular trigger point injections. The patient has been tapered off duloxetine, and is walking up to 1 mile, which he reportedly does frequently. He continues to reside at his home and sleep in his upstairs bedroom, as it is now much easier for him to ascend and descend stairs. Further, the patient continues to enjoy going to restaurants, working in his home office, doing repairs around his house, and spending time with family.
Discussion
For a multitude of reasons, SCS may not be offered as therapy for patients beyond an arbitrary age. We posit that while there are perhaps myriad reasons for this nonfeasance, the role of ageism in pain medicine8–10 and in society, broadly, cannot be understated. Some studies have demonstrated lower likelihood of a successful trial11,12 and greater likelihood of explanation13 in older patients, although others have not identified any difference in outcomes in those over 65 years of age,14 or even over 75 years,15 compared to younger patients. Chronic neck and back pain are prevalent in the extreme elderly, even in those in their 10th and 11th decades of life.16 Management strategies for these patients are often limited. There are strong recommendations against the use of a number of pain medications, such as certain skeletal muscle relaxants and tricyclic antidepressants, in elderly patients,17 while other classes of analgesics, including opioids, gabapentinoids, NSAIDs, and SNRIs must be used with caution in the elderly due to side effects, drug–drug interactions, and the presence of co-morbid conditions.17–19 The elderly population, particularly the extreme elderly, historically have been determined to have elevated complication rates when undergoing back surgery, and thus operative options for pain may not be offered. However, as in all populations, nonsurgical management may not be effective for these patients.20–22 The lack of options for these patients can have a major effect on quality of life. Chronic pain in the elderly is associated with both anxiety and depression,23 and functional limitations and pain in the elderly have been identified as predictive of suicidal ideation and suicide attempts.24 Despite a paucity of studies, SCS has been used increasingly in the extreme elderly population, as there was a 115% increase in SCS trials and a 324% increase in trial-to-permanent SCS placement rate in patients 85 years of age and greater between 2009 and 2018.24 That being said, the rate of SCS trials in the 85 and over population in 2018 was just 23 per 100,000 Medicare recipients, with the rate of trial-to-permanent SCS placement of only 15 per 100,000. Both rates are numerically lower than the rates for the <65, 65–74, and 75–84 populations, which were each at a minimum of 51 per 100,000 Medicare patients for trials and at least 32 per 100,000 receiving Medicare for trial-to-permanent.24
There are several reasons that clinicians may be hesitant regarding use of SCS in the extreme elderly, though the validity of these concerns can certainly be questioned. One such concern for many likely relates to an increased risk of complications, including post-operative infection. Advanced age is considered a risk factor for spine infections of all etiologies, and likewise, advanced age is associated with poor prognosis associated with spinal infection.25 However, one large retrospective study of over 6000 patients who underwent SCS used regression analysis to determined that increasing age was associated with a lower risk of SCS-related infection.26 It has also been opined that there is an increased risk of epidural hematoma as a complication of SCS surgery in the elderly, although there is a paucity of data to support this claim.27 Incidental dural puncture, which can lead to post-dural puncture headache among other complications, is a potential complication of SCS, although one investigation also identified an association between older age and decreased risk of a payer-claim for incidental dural puncture.28
Other possible factors that may impede the broader use of SCS in the elderly and advanced elderly include concerns regarding general risks of undergoing anesthesia and surgery. One such concern that must be assessed as an aspect of the patient selection process prior to SCS surgery is overall anesthetic risk.29 Aging is associated with several physiological changes such as reduced beta-receptor responsiveness, reduced cardiac compliance, decline in lung function, and decrease in renal function, among others. With aging also comes increased sensitivity to medications, including anesthetics. Post-operative delirium and cognitive dysfunction are also more common in elderly patients.30 Frailty, which is most common in the elderly, is associated with post-operative morbidity and mortality31 and elderly patients are at increased risk for critical respiratory events during recovery from general anesthesia.32 However, general anesthesia is not typically required for SCS trial lead placement or permanent system implantation. Furthermore, one study determined no association between age and unplanned readmission within 30 days post-SCS surgery.33
Lastly, an additional concern in this population is the higher prevalence of cognitive impairment compared to younger individuals, as some publications advise against implanting those with cognitive impairment.34 Some groups have also proposed a life expectancy of greater than 12 months as one of the selection criteria for SCS.35 These factors may lead to advanced elderly patients not being selected for this therapy, as predicting life expectancy becomes challenging in extreme elderly populations and cognitive impairment can be prevalent, although it is certainly not ubiquitous in this group and should not be assumed.
As we discussed, pain management options can be limited by side effects and risk profile for the elderly, particularly the extreme elderly. Our patient had already been evaluated by several specialists, including a spine surgeon, and had failed conservative management including physical therapy, opioid and non-opioid pain medications, and percutaneous interventions prior to presenting to our clinic for a second opinion at age 95. By the time he reached age 96, he was debilitated to the point that he spent most of his time in bed. Pain was preventing him from completing basic daily tasks, participating in activities that he enjoyed, and maintaining his quality of life.
Choosing to proceed with SCS surgery in an extreme elderly patient is a complicated decision. In this case, the four pillars of medical ethics36 were utilized to help guide this decision. Certainly, there is risk involved with any surgical intervention, naturally including implanted devices, and this had to be weighed against the potential benefits of SCS for our patient. The balance of non-maleficence and beneficence must be sought for every medical decision. In our case, it was important to consider justice as well to ensure that any potential bias against the use of SCS in the elderly did not affect decision making. Approaching the case with ageist biases, as mentioned earlier, would certainly have been a violation of the principle of justice. The ethical pillar of autonomy was also of particular importance in this case. As this was a complex situation, it was vital that VV and his family members understood all aspects of the choice at hand so that a shared decision with informed consent could be made between patients, family, and medical providers.
We surmise that many providers, including perhaps some of VV’s previous providers, may be hesitant to place an SCS or perform other surgical intervention on a patient of such advanced age with medical comorbidities and would cite the principles of nonmaleficence and justice in doing so. While we recognize that it is certainly our job as physicians to first do no harm, we argue that there is harm in allowing an extreme elderly patient to live out what time he has remaining with essentially no quality of life, particularly if there is still a potential treatment option available. In this case, SCS was VV’s remaining option, and we believed that the potential benefit in terms of improving his quality of life and helping him regain the independence and functionality that was so vital to him outweighed both any potential risks related to the surgery and implant itself and the risk of allowing him to continue in a state of pain so severe and disabling that palliative care had been seriously considered. This thought process was extensively shared with the patient and his family to guide shared decision-making and to ensure that there was clear informed consent prior to proceeding with these interventions. We would encourage others reading this analysis to use a similar ethics-guided decision-making process when considering the use of spinal cord stimulation in their extreme elderly patients.
Conclusion
Today, at age 102, with the aid of a spinal cord stimulator, VV’s level of pain, functional status, and quality of life have all substantially improved. He underwent a SCS trial, permanent SCS implant, and later IPG replacement surgery without complication. This is not to suggest that all advanced elderly with appropriate pain-related indications for SCS should be offered the treatment modality. There are risks involved associated with SCS that must be considered, particularly in patients of advanced age who tend to have more comorbidities compared to younger individuals as well as a shorter life expectancy. As with any procedure, a risk-benefit approach must be utilized and thoroughly discussed with the patient. In this case, maintaining some degree of mobility and independence was of high importance to the patient, and this priority aided in the decision to proceed with SCS, which was made via shared decision making between the patient and his providers.
This case illustrates an excellent outcome with SCS in an extreme elderly patient. In the future, more studies on SCS outcomes will be required in both the elderly and extreme elderly populations to strengthen the evidence that can be included in these risk-benefit discussions with patients. We also advocate for the inclusion of extreme elderly patients in SCS clinical trials to better understand the efficacy and risk profile of SCS in this population. Lastly, we advocate for an ethical approach to treating pain and utilizing SCS in the extreme elderly. Such an approach should be free of bias against the extreme elderly, should extensively consider the potential improvement in overall quality of life that can be associated with SCS as well as the risk to quality of life that can be associated with not offering the therapy, and should respect patient autonomy by utilizing shared decision making. What we are strongly advocating is a patient-centered approach to care that does not disenfranchise individuals from consideration of spinal cord stimulation (or other pain-related therapies) based solely on age.
Disclosure
Michael E Schatman is a senior medical advisor for Apurano Pharma. The authors report no other conflicts of interest in this work.
References
1. Kapural L, Deering J, Gilmore C. Spinal Cord Stimulation, Peripheral Nerve Stimulation, Restorative Neurostimulation, Deep Brain Stimulation, and Motor Cortex Stimulation. Practical Management of Pain.
2. Linderoth B, Meyerson BA. Spinal Cord and Brain Stimulation. In: Wall & Melzack’s Textbook of Pain.
3. Wang AY, Olmos M, Ahsan T, et al. Safety and feasibility of spinal anesthesia during simple and complex lumbar spine surgery in the extreme elderly (≥80 years of age). Clin Neurol Neurosurg. 2022;219:107316. doi:10.1016/j.clineuro.2022.107316
4. An Aging World 2015. Census.gov. Available at: https://www.census.gov/library/publications/2016/demo/P95-16-1.html.
5. Traeger AC, Gilbert SE, Harris IA, Maher CG. Spinal cord stimulation for low back pain. Cochrane Database Syst Rev. 2023;3(3):CD014789. doi:10.1002/14651858.CD014789.pub2
6. Mekhail N, Levy RM, Deer TR, et al. Long-term safety and efficacy of closed-loop spinal cord stimulation to treat chronic back and leg pain (Evoke): a double-blind, randomised, controlled trial. Lancet Neurol. 2020;19(2):123–134. doi:10.1016/S1474-4422(19)30414-4
7. Rigoard P, Ounajim A, Bouche B, et al. Comparison of spinal cord stimulation, dorsal root ganglion stimulation, and association of both in patients with refractory chronic back and/or lower limb neuropathic pain: a prospective, randomized, double-blind, cross-over trial (BOOST-DRG Study). Neuromodulation J Int Neuromodulation Soc. 2025;28(2):283–296. doi:10.1016/j.neurom.2024.10.003
8. Makris UE, Higashi RT, Marks EG, et al. Ageism, negative attitudes, and competing co-morbidities--why older adults may not seek care for restricting back pain: a qualitative study. BMC Geriatr. 2015;15:39. doi:10.1186/s12877-015-0042-z
9. Lane P, Smith D. Culture, ageing and the construction of pain. Geriatrics. 2018;3(3):40. PMID: 31011078; PMCID: PMC6319244. doi:10.3390/geriatrics3030040
10. LaRowe LR, Patidar S, Goetzinger A, Margolies S, Mace RA. Chronic pain management in an aging population: current challenges and policy-based solutions. Int J Forensic Ment Health. 2025;12(1):102–109. doi:10.1177/23727322241307916
11. Odonkor C. Fantastic four: age, spinal cord stimulator waveform, pain localization and history of spine surgery influence the odds of successful spinal cord stimulator trial. Pain Physician. 2020;1;23(1;1):E19–E30. doi:10.36076/ppj.2020/23/E19
12. Huang KT, Martin J, Marky A, et al. A national survey of spinal cord stimulation trial-to-permanent conversion rates. Neuromodulation Technol Neural Interface. 2015;18(2):133–140. doi:10.1111/ner.12199
13. Han JL, Murphy KR, Qasim hussaini SM, et al. Explantation rates and healthcare resource utilization in spinal cord stimulation. Neuromodulation J Int Neuromodulation Soc. 2017;20(4):331–339. doi:10.1111/ner.12567
14. Bondoc M, Hancu M, DiMarzio M, et al. Age as an independent predictor of adult spinal cord stimulation pain outcomes. Stereotact Funct Neurosurg. 2022;100(1):1–7. doi:10.1159/000517426
15. Higashiyama N, Tamura S, Sugawara T. Efficacy of spinal cord stimulation for failed back surgery syndrome in elderly patients: a retrospective study. Pain Res Manag. 2023;2023:2136562. doi:10.1155/2023/2136562
16. Hartvigsen J, Christensen K. Pain in the back and neck are with us until the end: a nationwide interview-based survey of Danish 100-year-olds. Spine. 2008;33(8):909–913. doi:10.1097/BRS.0b013e31816b45f1
17. 2023 American Geriatrics Society Beers Criteria® Update Expert Panel. American geriatrics society 2023 updated AGS Beers Criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2023;71(7):2052–2081. doi:10.1111/jgs.18372
18. Gazelka HM, Leal JC, Lapid MI, Rummans TA. Opioids in older adults: indications, prescribing, complications, and alternative therapies for primary care. Mayo Clin Proc. 2020;95(4):793–800. doi:10.1016/j.mayocp.2020.02.002
19. Wilder-Smith OHG. Opioid use in the elderly. Eur J Pain. 2005;9(2):137–140. doi:10.1016/j.ejpain.2004.07.011
20. Sivaganesan A, Zuckerman S, Khan I, et al. predictive model for medical and surgical readmissions following elective lumbar spine surgery: a national study of 33,674 patients. Spine. 2019;44(8):588–600. doi:10.1097/BRS.0000000000002883
21. Raffo CS, Lauerman WC. Predicting morbidity and mortality of lumbar spine arthrodesis in patients in their ninth decade. Spine. 2006;31(1):99–103. doi:10.1097/01.brs.0000192678.25586.e5
22. Cloyd JM, Acosta FL, Ames CP. Complications and outcomes of lumbar spine surgery in elderly people: a review of the literature. J Am Geriatr Soc. 2008;56(7):1318–1327. doi:10.1111/j.1532-5415.2008.01771.x
23. Mookerjee N, Schmalbach N, Antinori G, et al. Association of risk factors and comorbidities with chronic pain in the elderly population. J Prim Care Community Health. 2024;15:21501319241233463. doi:10.1177/21501319241233463
24. Manchikanti L, Pampati V, Vangala BP, et al. Spinal cord stimulation trends of utilization and expenditures in fee-for-service (FFS) medicare population from 2009 to 2018. Pain Physician. 2021;24(5):293–308.
25. Duarte RM, Vaccaro AR. Spinal infection: state of the art and management algorithm. Eur Spine J off Publ Eur Spine Soc Eur Spinal Deform Soc Eur Sect Cerv Spine Res Soc. 2013;22(12):2787–2799. doi:10.1007/s00586-013-2850-1
26. Falowski SM, Provenzano DA, Xia Y, Doth AH. Spinal cord stimulation infection rate and risk factors: results from a united states payer database. Neuromodulation J Int Neuromodulation Soc. 2019;22(2):179–189. doi:10.1111/ner.12843
27. Deer TR, Lamer TJ, Pope JE, et al. The Neurostimulation Appropriateness Consensus Committee (NACC) safety guidelines for the reduction of severe neurological injury. Neuromodulation J Int Neuromodulation Soc. 2017;20(1):15–30. doi:10.1111/ner.12564
28. Hussain N, Karri J, Dimitrov T, et al. Incidence and predictors of inadvertent dural puncture after percutaneous spinal cord stimulation: a retrospective database analysis. Neuromodulation J Int Neuromodulation Soc. 2024;27(6):1068–1075. doi:10.1016/j.neurom.2022.06.008
29. Davanzo J, Brandmeir NJ. Surgical technique and patient selection for spinal cord stimulation for chronic pain. Neurol India. 2020;68:S213–S217. doi:10.4103/0028-3886.302462
30. Griffiths R, Beech F, Brown A, et al. Peri-operative care of the elderly 2014: association of anaesthetists of Great Britain and Ireland. Anaesthesia. 2014;69(1):81–98. doi:10.1111/anae.12524
31. Shem Tov L, Matot I. Frailty and anesthesia. Curr Opin Anaesthesiol. 2017;30(3):409–417. doi:10.1097/ACO.0000000000000456
32. Huang J, Yang J, Qi H, et al. Development and validation of a nomogram for predicting critical respiratory events during early anesthesia recovery in elderly patients. BMC Med Inform Decis Mak. 2024;24:257. doi:10.1186/s12911-024-02671-4
33. Elsamadicy AA, Sergesketter A, Ren X, et al. Drivers and risk factors of unplanned 30-day readmission following spinal cord stimulator implantation. Neuromodulation J Int Neuromodulation Soc. 2018;21(1):87–92. doi:10.1111/ner.12689
34. Sitzman BT, Provenzano DA. Best Practices in Spinal Cord Stimulation. Spine. 2017;42(14):S67–S71. doi:10.1097/BRS.0000000000002220
35. Deer TR, Mekhail N, Provenzano D, et al. The appropriate use of neurostimulation: avoidance and treatment of complications of neurostimulation therapies for the treatment of chronic pain. Neuromodulation Appropriateness Consensus Committee. Neuromodulation J Int Neuromodulation Soc. 2014;17(6):571–597. doi:10.1111/ner.12206
36. Beauchamp TL, Childress JF. Principles of Biomedical Ethics.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.