Back to Journals » Infection and Drug Resistance » Volume 19
Adult Empyema Caused by Refractory Methicillin-Resistant Staphylococcus aureus Treated Using Linezolid as Salvage Therapeutic Option: A Report of Two Cases
Authors Seki M ![]() , Nagai T, Ozawa K
, Nagai T, Ozawa K
Received 16 May 2026
Accepted for publication 8 July 2026
Published 10 July 2026 Volume 2026:19 625227
DOI https://doi.org/10.2147/IDR.S625227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hazrat Bilal
Masafumi Seki,1 Takuya Nagai,1,2 Konosuke Ozawa1,2
1Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Hidaka City, Saitama, Japan; 2Division of Clinical Training Center, Saitama Medical University, Moroyama-cho, Saitama, Japan
Correspondence: Masafumi Seki, Division of Infectious Diseases and Infection Control, Saitama Medical University International Medical Center, Yamane 1397-1, Hidaka City, Saitama, 350-1298, Japan, Tel +81-42-984-4392, Fax +81-42-984-0280, Email [email protected]
Background: The pathogenesis and treatment of pulmonary lesions caused by methicillin-resistant Staphylococcus aureus (MRSA) infection have been unclear because MRSA has usually been considered a colonizer.
Case Series: Two adult cases of MRSA empyema were treated using linezolid (LZD) because they were refractory to the glycopeptides vancomycin (VCM) and teicoplanin (TEIC). Case 1 was a 50-year-old man with a history of lung cancer and pneumothorax who was admitted with pulmonary empyema with a severe dry cough. MRSA empyema was diagnosed because only MRSA was detected by video-assisted thoracoscopy (VATS) from his effusions. He was initially treated using VCM for 10 days, but his inflammatory markers and condition did not so improve; therefore, VCM was switched to LZD. His condition improved with LZD for 14 days. Case 2 was a 77-year-old man with pharyngeal cancer who was admitted with respiratory failure. He was diagnosed with MRSA empyema because only MRSA was detected from his pleural effusions on pleural drainage. He received a TEIC drip infusion for 10 days, but his respiratory status did not so improve; therefore, his treatment was switched to LZD. His condition improved with LZD for 14 days.
Conclusion: MRSA empyema was diagnosed in these two cases because only MRSA was detected from pleural effusions. Both patients finally improved following the switch from glycopeptide antibiotics to LZD. These findings suggest MRSA as the true cause of the infections and that LZD, rather than VCM and TEIC, might be effective in cases of MRSA empyema.
Keywords: empyema, methicillin-resistant Staphylococcus aureus, MRSA, linezolid, teicoplanin, vancomycin
Introduction
Empyema is a severe pulmonary complication of bacterial infection and usually develops from pneumonia.1,2 Antibiotics are the main treatment, but drainage might be needed in addition to antibiotics to efficiently eliminate the causal pathogens.1,2
Representative pathogens are aerobic bacteria related to the common causes of pneumonia, such as Streptococcus pneumoniae, Haemophilus influenzae, and gram-negative enterobacteria, such as Escherichia coli and Klebsiella pneumoniae.1 Anaerobes are also known to cause empyema.1
Among bacteria, methicillin-resistant Staphylococcus aureus (MRSA) might also be a representative pathogen related to empyema, although MRSA has generally been considered to be a colonizer with pulmonary epithelial cells, rather than an infective agent.3–7 However, some cases might be considered to be MRSA empyema, and they must be treated, excluding other pathogens, with anti-MRSA glycopeptide agents, including vancomycin (VCM) and teicoplanin (TEIC).1,3
In this report, two adult cases of MRSA empyema are presented. While VCM and TEIC were used to treat empyema initially, the patients’ conditions did not improve. Therefore, linezolid (LZD), an anti-MRSA agent known to have good tissue penetration and strong bactericidal effects, was used although larger studies are required to confirm its benefits.8
This report and related analyses were approved by the Institutional Review Board of Saitama Medical University International Medical Center on July 6, 2022 (#2022-030) and registered as UMIN000047690. The patients whose specimens were analyzed provided written, informed consent to have any accompanying images and their case details published. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Case Series
Case 1
A 50-year-old man with non-small cell lung carcinoma received chemotherapy with four courses of anticancer drugs, and nearly complete remission was achieved. One month later, he was admitted to our hospital with high fever and chest pain. Empyema was diagnosed because his chest X-ray and computed tomography (CT) showed abnormal shadows and pleural effusions in the right lung on admission (day 0) (Figure 1A and B). Laboratory data were as follows: white blood cell (WBC) count 6.00 ×103/μL; C-reactive protein (CRP) 22.2 mg/dL; and hemoglobin A1c (HbA1c) 6.3%, suggesting diabetes mellitus (DM).
 |
Figure 1 Radiological findings of the Case 1 patient on admission (A and B) and at day 27 (C and D). On admission, there are abnormal shadows and pleural effusions in the right lung in chest X-ray (A) and computed tomography (B), but these shadows and effusions in chest X-ray (C) and computed tomography (D) improve after drainage and antibiotic therapy using linezolid. Arrows indicate the abnormal shadows and pleural effusions. |
Drainage of the right thorax by video-assisted thoracoscopy (VATS) was performed, and MRSA alone was detected on day 3. MRSA was also isolated from his nose, but considered just colonized because it was asymptomatic. The susceptibility of the MRSA isolated from this patient is shown on the left in Table 1. The minimum inhibitor concentrations (MICs) of isolated bacteria were determined by a Phenix M-50 system (Becton Dickinson, Franklin Lakes, NJ, USA) and Lysys@S4 (Shimazu Diagnostics, Tokyo, Japan) based on the broth microdilution method. MRSA was confirmed by MRSA-CI selection agar (Kyokuto, Tokyo, Japan).
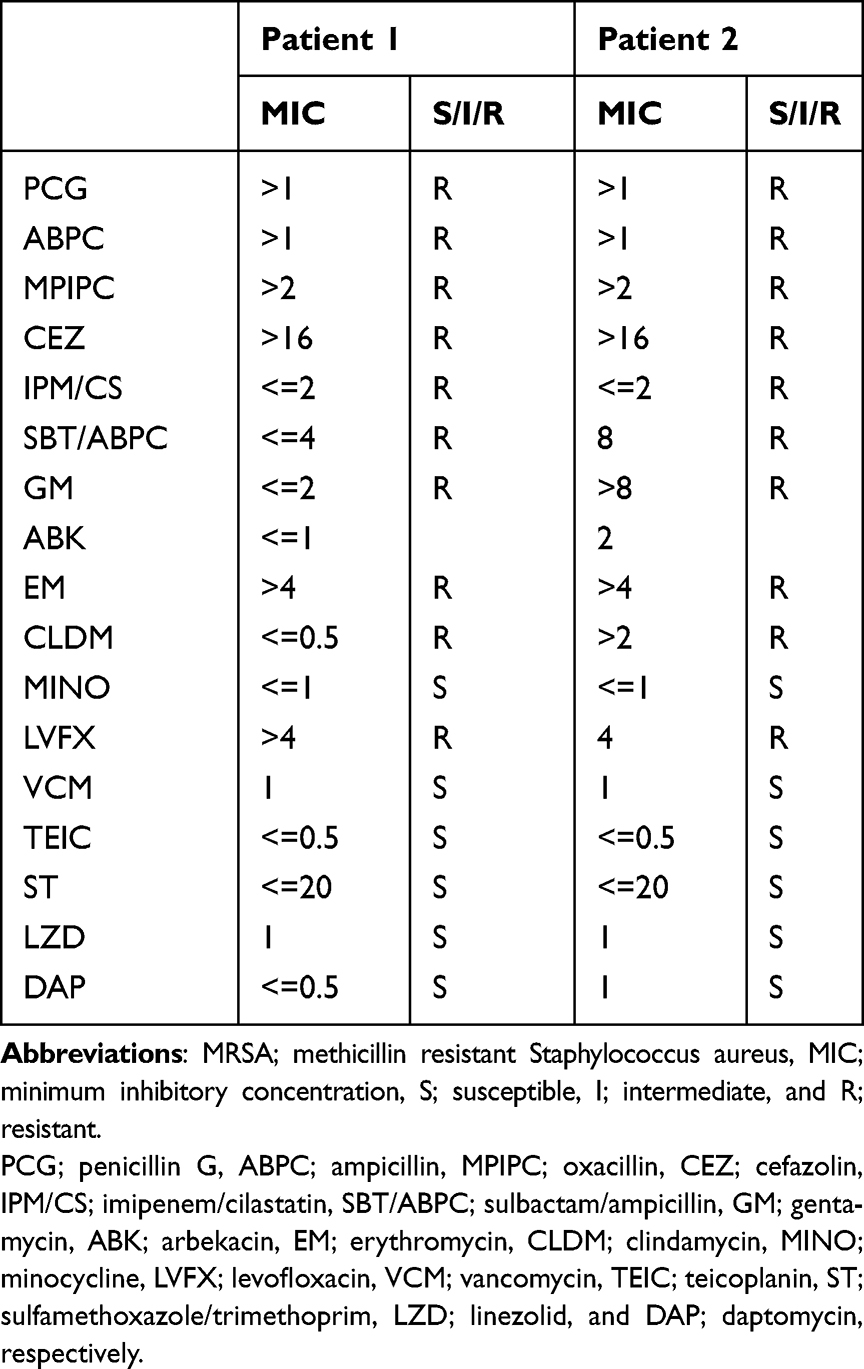 |
Table 1 Drug Susceptibilities of the MRSA Isolated from the Patients |
An ampicillin/sulbactam (ABPC/SBT) 3-g drip infusion (div) three times per day was started on admission but was switched to VCM 1 g div twice per day on day 3. However, inflammatory markers remained elevated, with a WBC count of 8.47 ×103/μL and CRP of 7.02 mg/dL although the trough and peak of VCM; 11.3μg/mL and 30.5μg/mL, respectively, were well controlled by the therapeutic dose monitoring (TDM) to maintain the area under curve (AUC) 24h 400–600 mg he/L. The effusion in the chest radiography and isolation of MRSA from the chest effusions had been also remained. Therefore, VCM was switched to linezolid (LZD) div 0.6 g twice per day on day 13. After 14 days on LZD (day 27), the laboratory results improved, with a WBC count of 6.54 ×103/μL and CRP of 1.70 mg/dL. His chest X-rays and CT also showed significant improvement (Figure 1C and D). MRSA disappeared from his chest effusions.
Case 2
A 77-year-old man with hypopharyngeal cancer underwent surgery and achieved nearly complete remission. Two months later, he was admitted to our hospital with high fever and chest pain. Empyema was diagnosed because his chest X-ray and CT showed abnormal shadows and pleural effusions in the left lung on admission (day 0) (Figure 2A and B). His WBC count was 11.11 ×103/μL, and CRP was 24.7 mg/dL.
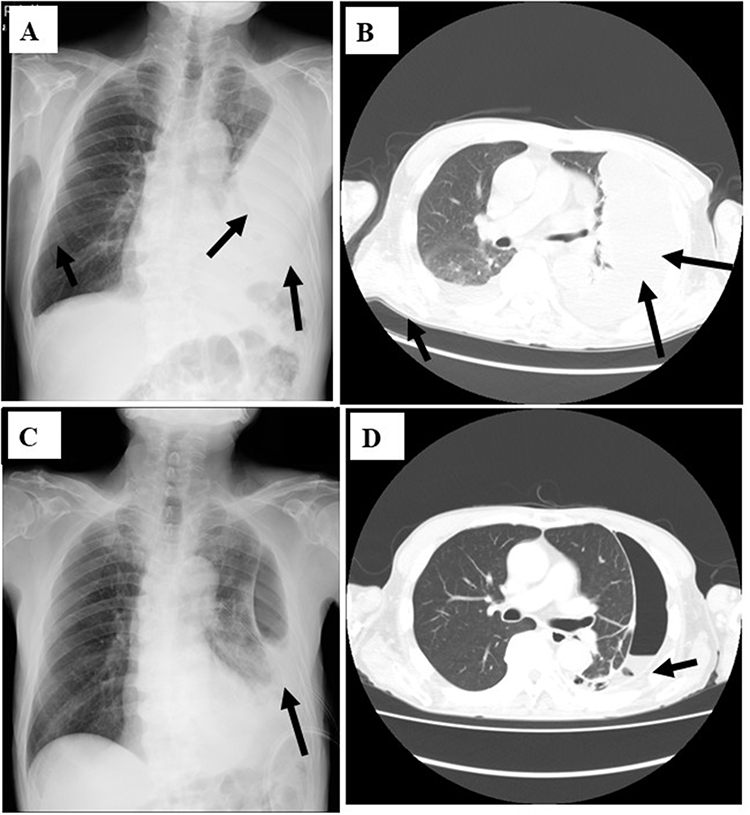 |
Figure 2 Radiological findings of the Case 2 patient on admission (A and B) and at day 24 (C and D). On admission, there are abnormal shadows and pleural effusions in the left lung in chest X-ray (A) and computed tomography (B), but these shadows and effusions in chest X-ray (C) and computed tomography (D) improve after drainage and antibiotic therapy using linezolid. Arrows indicate the abnormal shadows and pleural effusions. |
Drainage of the left thorax was performed, and MRSA alone was detected on day 3. The MICs of isolated MRSA were determined as described same as Case 1, where MRSA was also isolated from her nose but considered just colonized because it was asymptomatic. The susceptibility of the MRSA isolated from this patient is shown on the right in Table 1. An ABPC/SBT 3-g drip infusion (div) three times per day was started on admission but was switched to TEIC 0.4 g div twice per day for the first two days, followed by 0.2 g div twice per day on day 3. However, inflammatory markers remained elevated, with a WBC count of 9.24 ×103/μL and CRP of 12.02 mg/dL although the trough of TEIC; 13.2 μg/mL was well controlled by the TDM. The effusion in the chest radiography and isolation of MRSA from the chest effusions had also remained. Therefore, TEIC was switched to LZD div 0.6 g twice per day from day 10. After 14 days on LZD (day 24), the inflammatory markers were improved, with a WBC count of 5.23 ×103/μL and CRP of 1.16 mg/dL. His chest X-rays and CT had also improved significantly (Figure 2C and D). MRSA disappeared from her chest effusions.
Discussion
Empyema is the accumulation of pus within the pleural space and can be a serious complication of pneumonia, requiring extensive treatment with antibiotics and adequate drainage.1,2
In this report, two cases of empyema thought to be caused by MRSA infection treated initially by VCM/TEIC followed by LZD were presented. Isolation of MRSA is usually only considered to indicate colonization, not infection;5,6 however, in a patient hospitalized with community-acquired pneumonia complicated by empyema, the Infectious Diseases Society of America (IDSA) guidelines recommend empirical treatment for MRSA while awaiting culture results.4 Once MRSA is confirmed, the recommended antibiotic regimen includes 7 to 21 days of VCM div 600 mg twice per day, div or oral LZD 600 mg twice per day, or div or oral clindamycin 600 mg 3 times per day.4 MRSA was found to be one of the major pathogens in cases of hospital-acquired pneumonia and ventilator-associated pneumonia (VAP), and treatment for MRSA might be critical in these cases because MRSA was detected significantly more frequently in non-survivors of VAP in our previous study.9 Furthermore, our meta-analysis strongly suggested that MRSA pneumonia and empyema should be treated as such when only MRSA is isolated from respiratory specimens, including nose, sputum and pleural effusions.10
Both patients in the two cases presented showed typical radiographic findings on chest X-ray and CT with high levels of inflammatory markers, and only MRSA was isolated from their pleural effusions. High inflammation due to non-isolated pathogens, such as anaerobes was suspected, but ABPC/ABT was not effective in both cases. Empyema cases usually show higher inflammation, compared with pneumonia cases.1–3 They finally improved with administration of anti-MRSA agents. These findings suggest that the present patients truly had MRSA empyema and highlight the benefits of anti-MRSA agent administration.
In addition, elevation of inflammatory markers persisted in the present cases despite the administration of the glycopeptide antibiotics VCM and TEIC. Therefore, they were switched to LZD, which is the first available antibiotic agent in the oxazolidinone class, and shows a strong but bacteriostatic effect against MRSA.11 LZD has been shown to have epithelial lining fluid concentrations several-fold higher than serum concentrations, and this has been perceived as a significant advantage over VCM.12 On the basis of the better penetration of LZD into respiratory secretions than VCM, LZD has demonstrated a survival advantage in patients with documented MRSA nosocomial pneumonia. Recent guidelines indicate that LZD may be preferred over glycopeptide antibiotics for MRSA pneumonia.4,13 Two meta-analyses also showed the clinical and microbiological advantages of LZD over VCM in the treatment of MRSA pulmonary infections, including pneumonia and empyema.14,15 In fact, LZD showed more effectiveness than VCM or TEIC in the present cases. These findings suggest that use of LZD rather than VCM and/or TEIC might be recommended in the treatment of not only MRSA pneumonia, but also MRSA empyema.
Due to limitations, we first presented the advantage of treatment by LZD, compared with VCM/TEIC; however, the results were based on only two cases although we found the preliminary data and meta-analysis. Second, we could not show the detailed laboratory, microbiological, and radiography data, however, predefined criteria to be considered the treatment success, such as decrease in inflammation markers (WBC and CRP), disappearance of causative pathogens, and improvement of chest X-ray/CT findings, did not achieved in both cases. From the view of antimicrobial stewardship settings, we should be more clear the antibiotic uses in refractory cases according to the guideline and guidance.16 Third, microbiological characterization of the MRSA isolates was limited to phenotypic antimicrobial susceptibility testing. No molecular investigations, such as SCCmec typing, virulence gene detection, molecular typing, or whole-genome sequencing, were performed. From the phenotypic antimicrobial susceptibility testing data, the isolated MRSA from two patients might be hospital-acquired SCC mec II, and non-toxin, such as Panton-Valentine Leukocidin (PVL) producing types.17,18 LZD is also suggested clinically effective against PVL-positive MRSA.18 Detailed microbiological investigation should be also performed simultaneously with clinical study.
In conclusion, two cases of MRSA empyema were successfully treated using an anti-MRSA agent. Only MRSA was isolated from their pleural effusions, and LZD had better effectiveness than VCM/TEIC. Further investigations with large sample sizes and detailed patient information will be needed to establish the indications for using an anti-MRSA agent such as LZD, rather than VCM or TEIC, for treating MRSA empyema.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shen KR, Bribriesco A, Crabtree T, et al. The American Association for thoracic surgery consensus guidelines for the management of empyema. J Thorac Cardiovasc Surg. 2017;153:e129–6. doi:10.1016/j.jtcvs.2017.01.030
2. Shiraishi Y, Omasa M, Yamashita S, et al. Guidelines for the treatment of empyema (The Japanese Association for Chest Surgery). Gen Thorac Cardiovasc Surg. 2025;73:312–327. doi:10.1007/s11748-025-02119-0
3. Dixon JL, Papaconstantinou HT, Pruszynski J, Rascoe PA, Reznik SI. Methicillin-resistant staphylococcus aureus colonization and empyema: does it matter? Surg Infect. 2015;16:583–587. doi:10.1089/sur.2014.050
4. Liu C, Bayer A, Cosgrove SE, et al. Clinical practice guidelines by the infectious diseases society of america for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children: executive summary. Clin Infect Dis. 2011;52:285–292. doi:10.1093/cid/cir034
5. Seki M, Watanabe A, Mikasa K, Kadota J, Kohno S. Revision of the severity rating and classification of hospital-acquired pneumonia in the Japanese Respiratory Society guidelines. Respirology. 2008;13:880–885. doi:10.1111/j.1440-1843.2008.01348.x
6. Sakaguchi M, Shime N, Fujita N, Fujiki S, Hashimoto S. Current problems in the diagnosis and treatment of hospital-acquired methicillin-resistant Staphylococcus aureus pneumonia. J Anesth. 2008;22:125–130. doi:10.1007/s00540-007-0600-4
7. Nagaoka K, Yanagihara K, Harada Y, et al. Predictors of the pathogenicity of methicillin-resistant Staphylococcus aureus nosocomial pneumonia. Respirology. 2014;19:556–562. doi:10.1111/resp.12288
8. Pickens CI, Wunderink RG. Methicillin-resistant Staphylococcus aureus hospital-acquired pneumonia/ventilator-associated Pneumonia. Semin Respir Crit Care Med. 2022;43:304–309. doi:10.1055/s-0041-1740583
9. Seki M, Takimoto A, Inoue M, Niiyama K, Masuoka A, Kotajima F. Clinical differences between survivors and non-survivors of ventilator-associated pneumonia: the roles of Sulbactam/Ampicillin and Methicillin-Resistant Staphylococcus aureus. Infect Drug Resist. 2024;27:5875–5879. doi:10.2147/IDR.S497536
10. Fujikura Y, Ohno T, Seki M, Mitsutake K. Is administration of anti-MRSA drugs recommended for patients with pneumonia when MRSA is isolated from respiratory specimens? A systematic review and meta-analysis. J Infect Chemother. 2024;30:88–91. doi:10.1016/j.jiac.2023.09.002
11. Stevens DL, Herr D, Lampiris H, Hunt JL, Batts DH, Hafkin B. Linezolid versus vancomycin for the treatment of methicillin-resistant Staphylococcus aureus infections. Clin Infect Dis. 2002;34:1481–1490. doi:10.1086/340353
12. Stevens DL, Dotter B, Madaras-Kelly K. A review of linezolid: the first oxazolidinone antibiotic. Expert Rev Anti Infect Ther. 2004;2:51–59. doi:10.1586/14787210.2.1.51
13. Kalil AC, Murthy MH, Klompas M, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: 2016 clinical practice guidelines by the infectious diseases society of America and the American thoracic society. Clin Infect Dis. 2016;63:e61–e111. doi:10.1093/cid/ciw353
14. Kato H, Hagiwara M, Asai N, et al. Meta-analysis of vancomycin versus linezolid in pneumonia with proven methicillin-resistant Staphylococcus aureus. J Glob Antimicrob Resist. 2021;24:98–105. doi:10.1016/j.jgar.2020.12.009
15. Jung YJ, Hong SB, Hong S-B, et al. Effect of vancomycin plus rifampicin in the treatment of nosocomial methicillin-resistant Staphylococcus aureus pneumonia. Crit Care Med. 2010;38:175–180. doi:10.1097/CCM.0b013e3181b9ecea
16. Seki M. Optimizing antimicrobial use in Japan: strategies for dosage, combination therapy, de-escalation, oral switching, duration, and guideline adherence. Clin Pharmacol. 2025;17:227–233. doi:10.2147/CPAA.S539674
17. Yamada K, Yanagihara K, Hara Y, et al. Clinical features of bacteremia caused by methicillin-resistant Staphylococcus aureus in a tertiary hospital. Tohoku J Exp. 2011;224:61–67. doi:10.1620/tjem.224.61
18. Yanagihara K, Kihara R, Araki N, et al. Efficacy of linezolid against Panton-Valentine leukocidin (PVL)-positive meticillin-resistant Staphylococcus aureus (MRSA) in a mouse model of haematogenous pulmonary infection. Int J Antimicrob Agents. 2009;34:477–481. doi:10.1016/j.ijantimicag.2009.06.024
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Targeted Antibiotics for Lower Respiratory Tract Infection with Corynebacterium striatum
Zhang H, Tan X, Zhang Z, Yang X, Wang L, Li M, Shi D, Li Y, Li J, Li Z, Liao X
Infection and Drug Resistance 2023, 16:2019-2028
Published Date: 4 April 2023