")
Back to Journals » International Journal of Women's Health » Volume 11
Adolescent and young adult couples’ views of intravaginal practices: a qualitative analysis of a pilot study
Authors Moise IK, de Joya E, Caplan B , Rodriguez VJ , Butts S, Chisembele M, Weiss SM, Jones DL, Alcaide ML
Received 14 July 2018
Accepted for publication 27 September 2018
Published 18 January 2019 Volume 2019:11 Pages 49—56
DOI https://doi.org/10.2147/IJWH.S180233
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Imelda K Moise,1,2 Evan de Joya,1 Benjamin Caplan,1 Violeta J Rodriguez,3 Stefani Butts,3 Maureen Chisembele,4 Stephen M Weiss,3 Deborah L Jones,3 Maria L Alcaide3
1Department of Geography and Regional Studies, University of Miami, Coral Gables, FL, USA; 2Department of Public Health Sciences, University of Miami Miller School of Medicine, Miami, FL, USA; 3Department of Psychiatry and Behavioral Sciences, University of Miami Miller School of Medicine, Miami, FL33136, USA; 4Department of Obstetrics and Gynecology, University of Zambia, Lusaka, Zambia
Purpose: In this study, we evaluated the risk behaviors that are drivers of the HIV epidemic among adolescent girls and young women in Zambia using a focus group research technique.
Subjects and methods: Eighteen adolescent couples (n=18 females and 18 males) aged 16–24 participated in six focus groups discussions (3 per gender) convened at three health facilities in Lusaka, Zambia. Focus group moderators utilized a set of open-ended questions to guide the 60-minute sessions. The focus group audio recordings were transcribed, coded, and analyzed using qualitative content analysis in Nvivo 11.
Results: Three themes and four subthemes were identified relating to adolescent and young adult couples’ knowledge, views, and male partner attitudes toward intravaginal practices (IVPs). The first theme, knowledge and rationale for IVPs, consisted of the subthemes relating to why adolescents and young adult couples engage in IVPs and assessed their knowledge of health risks associated with IVPs. The second theme, attitudes toward IVPs, consisted of the subtheme willingness to stop or support partner to discontinue IVP and practices toward IVP and strategies for changing. The third theme, strategies for changing IVPs, consisted of the subtheme raise awareness.
Conclusion: IVPs used for cleaning purposes were perceived as essential to enhancing hygiene, health, and sexual satisfaction for both girls and boys. However, couples expressed concern about the health effects of IVPs used for tightening and a desire for learning more about this practice as well as stopping it.
Keywords: bacterial vaginosis, sexually transmitted infection, Zambia, focus groups, HIV
Introduction
Intravaginal practices (IVPs), defined as a set of behaviors undertaken by women to tighten, dry, and clean the vagina for hygiene, health, and sexuality-related reasons (eg, cloth, paper, or fingers and a variety of products) pose a major public health concern in sub-Saharan Africa (SSA).1–3 A recent meta-analysis concluded that women who used specific IVP are at nearly 20% greater risk of incident bacterial vaginosis (BV) compared to women who do not use IVP and a 30% increased risk of acquiring HIV.1 BV is also associated with acquisition of HIV.4 In contrast, a pilot intervention to reduce IVP and BV in HIV-infected women in Zambia reported a decrease in self-reported use of IVPs at 12 months and increased the importance placed on health when considering engagement in IVP.5 Surprisingly, the views of adolescents (girls and boys) on IVPs have not been closely examined.
Recent evidence suggests that in SSA, a disconnect exists between adolescents and their parents regarding perception of risk and protective factors that influence their participation in risky sexual behaviors, particularly in areas with increasing rates of HIV among adolescent girls and young women.6 These differing perceptions may hinder adolescents’ ability to exercise control over their sexual and reproductive health and may interfere with health promotion efforts. Most importantly, to the degree that parents fail to understand adolescents’ desire and motivations, they also fail to recognize potentially important means of providing adolescents with healthy alternatives to risky behaviors such as IVP. Additionally, for health providers, this represents a missed opportunity to intervene and improve adolescent sexual and reproductive health. This issue is increasingly important for addressing adolescents’ and young adults’ sexual reproductive needs because SSA bears the greatest burden of sexually transmitted infections including HIV.7,8
In Zambia, female initiation rites, marking the “coming of age” for girls and young women, serve to introduce them to the cultural, gender, and sexual norms that they are expected to follow as women, perpetuating specific culturally driven IVP.4,9 While these initiation practices are a more formal introduction to womanhood, a recent study conducted by Scorgie et al in KwaZulu-Natal, South Africa found that knowledge about such practices is also “garnered through informal and implicit processes of information-sharing and gossip with close female friends, neighbors and members of one’s peer group”.10
In Tanzania, Uganda, and Zambia, women use IVPs without explicitly informing their partners, while men express suspicion of IVP, drawing associations between IVP and infidelity and promiscuity.11,12 Further, the body of research on IVPs seldom includes men, though studies that have included men indicate that they may play a valuable role in better understanding IVPs in SSA and that behaviors preferred by men for sexual satisfaction are the most difficult to influence.4,13,14 This is not to suggest that men’s views should be considered the gold standard from which we develop and implement women’s health programs; rather, we suggest that programs developed without a comprehensive understanding of the target population may be less likely to succeed, particularly when there is a conflict between the goals and objectives of the target population.
The objective of this study is to explore adolescent and young adult couples’ knowledge, attitudes, and practices toward IVPs in Lusaka, Zambia, in order to develop targeted IVP interventions for this age group and, ultimately, decrease the risk of BV and HIV among this highly vulnerable population.
Subjects and methods
Study area
The study took place in Lusaka, the largest and the capital city of Zambia. The 2010 national census projected a population of nearly 2.2 million people and an annual growth rate of 4.6%, making it the fastest growing city in the country. In Lusaka, the majority of the population lives within city limits (84.7%) and around 39.5% of the population is younger than age 15.15 The poverty rate stands at 13%. Recent estimates put population density at 1,001.2 persons per square kilometer, an increase from the estimated 63.5 persons per square kilometer in 2000, a reflection of the city’s rapid population growth. The incidence of poverty is generally higher in rural areas than urban areas and varies among households.16
Within the Lusaka health district, there are six distinct health zones. District health services comprise three increasingly specialized health service delivery system structures, with the first level being community-level health services such as district hospitals, health centers, and health posts, the second level being provincial and general hospitals, and the third level being all central or specialist hospitals. Zambian Ministry of Health data indicate a significantly higher HIV prevalence among girls aged 15–19 than their male peers.6 Our previous study also found widespread use of IVPs among women in the city.2 “Youth-Friendly Corner”, a program aimed at providing a place for young people to get information about their health, treatment, and psychosocial support, has been launched in most of the hospitals and clinics, though its primary focus is the prevention of HIV/AIDS and sexually transmitted infections through voluntary counseling and testing.13
Study design
Data were collected using focus groups and a semi-structured question guide during February 2017 and utilizing focus groups. Data presented in this report are part of a large national qualitative study aimed at exploring vulnerability of adolescent girls and young women to HIV in Zambia. Results from the primary study have been previously published.1–3,4,5,17 Focus group discussions were held with adolescent and young adult couples in one urban and two peri-urban public health facilities of Lusaka city, Zambia.
Study population and sample
The study participants included adolescent and young adult boys and girls (aged between 16 and 24 years) who had visited a Youth-Friendly Corner for counseling on sexual and reproductive health topics. In order to be eligible for participation in the interview, adolescents and young adults must have resided in the area for >6 months; those who had lived there for <6 months were excluded because the investigators thought they would not have had enough local experience on IVPs in the area. In addition, adolescents and young adults aged below 16 or above 24 years were excluded from participation.
Selection of study participants was done using a self-selection sampling technique, a non-probability sampling technique. This technique was used to optimize inclusion of respondents who were willing to participate, maximizing the effectiveness of data collection efforts, and because the consideration of subjects representative of the entire population was not an objective of this study.14 To begin with, with the help of the district health manager, we identified the two health facilities with the highest HIV prevalence rates in the district and the largest hospital in the district for selection and inclusion in the study.
A month prior to the interview, the first and the last authors of the study contacted the staff members in charge of respective health facilities’ Youth-Friendly Corners to inform them about the study. We held face-to-face meetings with the staff members in charge of the respective Youth-Friendly Corners. We then attended sexual and reproductive health sessions on 3 days to recruit and explain the purpose and objectives of the study to adolescents and young adult couples attending these facilities. Adolescent and young adult couples who were willing to participate in the study were asked to return to the Youth-Friendly Corner for the focus group at the date and time that was agreed upon.
Data collection
The focus groups were held during February 2017 to capture adolescent and young adult couples’ knowledge, attitudes, and practices regarding IVPs and to assess male partners’ influence on the use of IVPs. Each focus group facilitator was provided with a guide including 12 questions related to knowledge and attitudes of IVPs. Six focus groups were planned and held, two at each of the three health facilities (n=36, 18 male and 18 female). The six focus groups were convened based on Patient-Reported Outcomes Measurement Information System (PROMIS®) guidelines, which suggest the use of at least three focus groups of 6–12 participants each, which can be adjusted, based on the needs of study participants.18 In this study, data saturation was determined to be reached before the conclusion of each of the focus groups; therefore, additional focus groups were not needed.
To create an environment conducive for participants to freely express their views, the focus groups were separated by gender and were facilitated by two trained moderators of the same gender. Key benefits of defining the moderator/assistant roles have been previously described.2,23,24
To ensure privacy and confidentiality, each focus group was held in the conference room of the health facility and the duration of the interviews was limited to an hour. The discussions were conducted in Nyanja, the local language in the area. Before each discussion, written consent was obtained from each participant by requesting him or her to read and sign the consent form, which was translated into the local language. Research assistants read the consent form aloud for those who could not read.
Data analysis
Data from the focus group discussions included audio recordings and detailed summaries written by each moderator. Recordings from the discussions were transcribed verbatim using a professional service. The transcripts were parsed into meaning units, defined as “words, sentences or paragraphs containing aspects related to each other through their content and context”.7 A preliminary coding structure was developed a priori incorporating themes identified through a literature review and an initial review of the transcripts. Two research assistants trained in Nvivo 11 performed an initial coding, with each meaning unit coded to one of the nodes identified in the preliminary coding structure. After the initial coding, the research team, including the two research assistants, met to identify the emerging themes and develop a finalized coding structure and performed a second coding. Coding results from the two research assistants were checked for inter-rater reliability using the Kappa statistic.
Ethics approval
The ethics research committee at the University of Miami in Florida and the University of Zambia approved ethical clearance. All participants signed informed consent in their language of preference. In Zambia, the age for consenting for research without parent’s consent is 16 years. Thus, participants under 18 years provided informed assent, and informed consent was obtained from their parent or legal guardian.
Results
Thirty-six participants (50% per gender), aged 16–24 years, participated in this research study. Participants were married or unmarried, but in romantic relationships. The results presented here consist of three themes: theme A, knowledge and rationale for IVP; theme B, attitudes toward IVP; and theme C, strategies for changing IVP (Table 1). Cohen’s Kappa statistic demonstrated substantial moderate level of agreement (0.81, 95% CI 0.67–0.96, P<0.001). Each theme included one or two subthemes. Following is an illustration of quotes from different focus group discussions.
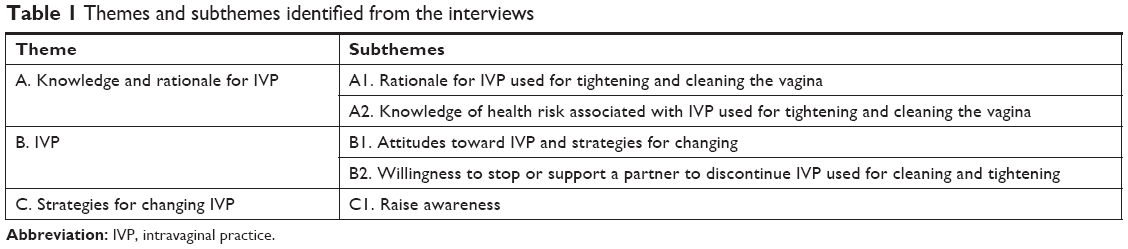 | Table 1 Themes and subthemes identified from the interviews |
Theme A: “Knowledge and rationale for IVP used for tightening and cleaning”
This theme describes reasons for using IVP, the level of awareness, and rationale indicated about IVP. The subthemes identified were rationale for IVP used to tighten and clean the vagina and knowledge of health risk. Most couples described a need for cleansing for hygiene purposes, but participants’ views were mixed on tightening.
Subtheme A1: Rationale for IVP used to tighten and clean the vagina
The subtheme of rationale for IVP used for tightening and cleaning describes why couples engage in IVP. Reasons for using IVP varied, but, in general, a recurrent theme in the interviews was a sense of awareness among men for IVP cleaning and tightening than drying. These views surfaced mainly in relation to the question, “Can someone describe how young adult girls clean, tighten or dry the vagina?” Two discrete reasons emerged from this. First, according to men, women bathed and used salts and creams for tightening. Second, women sometimes inserted substances such as “nsuko”, a powder made of crushed dry tobacco, which raised concern among men as they were worried that the use of this substance increases the susceptibility to infection. But couples highlighted vagina cleaning as significant because they perceived IVP cleaning as promoting vaginal health and hygiene.
Cleaning, of course, has to be there. A woman has to clean her vagina.
A woman has to clean her vagina in order to do away with bad smells.
It is good for women to wash the vagina … for hygiene’s sake. [Male group]
Hygiene reasons.
Everybody cleans.
I think we would have a bad smell, if not cleaning. [Female group]
Subtheme A2: Knowledge of health risk associated with IVP used to tighten and clean the vagina
The knowledge of health risk associated with IVP subtheme describes the level of knowledge among couples who use IVP. We observed that while some girls indicated not using IVP for tightening, a few indicated using IVP 2–3 days before engaging in sexual intercourse. According to these girls, they learned about tightening in both formal and informal settings from peers, mothers, and grandmothers at an early age (during initiation rituals or once they start to engage in sexual activities). The earliest age mentioned for starting IVP was 10 or 11 years. However, when asked as to why girls practice tightening, opinions were mixed.
The majority of girls relayed the belief that tightening IVPs are necessary for their partner’s satisfaction:
Because we are told to satisfy boyfriends. [Female group]
When the vagina is tightened, the man enjoys sex more. [Female group]
This view was echoed by a male participant who relayed thus:
They do that when going to meet a man. That is when they are making sure the vagina is tightened for the man. [Male group]
For a small number of male participants, “the vagina being wider and loose” (male group) is the reason for tightening the vagina. However, in three cases, male participants indicated that a tight vagina provides more pleasure in intercourse for both the male and female involved.
When the vagina is tightened, it is more sensational and the girl can get more satisfaction.
Men, like to listen to a girl cry. Like, ‘Ah’. She likes that. Even girls, I think they like that. Therefore, the tightening of the vagina is to make the man feel good. Feel nice. [Male group]
Commenting on the same question, one of the boys expressed concern over the pain this may cause to his partner:
Because if she tightens her vagina, it means she is creating a problem. [Male group]
Surprisingly, the knowledge regarding the health risks associated with IVP used for tightening was high among couples. Most were aware of at least one health risk.
You can have cervical cancer and other infections caused by the used chemicals.
It is very easy to get HIV/AIDS because of the friction it causes when having sex.
I have heard that inserting fingers and cleaning the vagina can lead to cancer and other bacterial in the hands that go into the vagina. [Female group]
I would mind because if the vagina is tightened during sexual intercourse, it can cause a woman bruises. You are creating a problem then.
… so the chances of the man getting STIs they are very high. [Male group]
Theme B: “Attitudes toward IVPs and strategies for changing”
The attitudes toward IVP subtheme describe how couples learn about IVPs and the commonly used products. Girls reported using a wide range of products applied in a variety of ways inside the vagina for tightening, such as sniff and soap, salt, cream, and cold water for cleaning.
Soap for cleaning. Soap. Normal water for cleaning and tightening. Also salts. Yes, salts for cleaning.
When I wash or tighten the vagina, I use basic cream. It is called ReTight.
Just water. Cold water most especially. The others use lemons. [Female group]
Girls reported learning about IVP from elderly women – family members, peers, and neighbors:
My mom told me I didn’t have to do anything just go to your grandma and she would tell you. Yes and neighbors. [Female group]
Subtheme B1: Attitudes toward IVPs used for tightening and cleaning
The second subtheme described attitudes regarding IVP and implied a group-level willingness to cease tightening IVP if educated about the associated health risks, though participants were resistant to the notion of stopping IVP. The subtheme identified was willingness to stop or support partner to discontinue IVP. Most of the boys expressed some concerns, but were willing to support their partners’ quit attempt.
Subtheme B2: Willingness to stop or support a partner to discontinue IVP
The subtheme of willingness to stop or support a partner to discontinue IVP describes how the girls felt about stopping cleaning and tightening via IVP and their male partner’s level of support for an attempt to quit. Overall, couples demonstrated a willingness to stop tightening, but not cleaning. One girl participant summarized this view as follows:
Only tightening, but not for cleaning. [Female participant]
The following are the views of adolescent and young adult boys:
I would support her if she probably stops tightening the vagina.
Yes, I would support her all the way, but the cleaning part is a must.
Yes, I support that. She is my partner. [Male group]
Theme C: Strategies for changing IVP among adolescents and young adult couples
The third theme describes the strategies for changing IVP. The subtheme identified was raise awareness. The couples articulated the desire for a less-stigmatized discussion in diverse settings such as Youth-Friendly Corners, schools, reproductive health clinics, and in small group sessions.
Subtheme C1: Raise awareness
The subtheme of raise awareness indicates a desire for more information and discussions that are more inclusive:
Everyone has different opinions. [Female group]
Yeah, because we’ve learned something just here. [Male group]
The couples considered focus group discussions to be an integral part of “learning to keeping vaginas healthy” (female group) as they provided a safe environment for both girls and boys to gather, discuss, and learn things beneficial for their relationships. They believed that learning in different settings would challenge them to find ways of interacting and discussing the issues effectively with other young people who have different experiences, as illustrated in the female group conversation below:
We would discuss about it and the best would be in a group like this.
Having sessions where we have a Youth-Friendly Corner.
Maybe just being the few of you in a group. You can get a lot of information.
Yes, girls will be comfortable with girls, because we all have the same interest.
At the clinic.
By surrounding ourselves with grandmas.
At home. [Female group]
There was an overwhelmingly positive reaction when asked if there was interest in learning more about IVPs. All the 18 girls responded affirmatively. Boys were interested in learning how these practices were harmful to women and how to change them. As one boy said,
I would feel good, learning is important.
Another commented,
To learn about all these practices, know their importance and how to deal with them. [Male group]
However, some of the girls expressed doubt that their partners would be interested in learning more about IVPs. One girl felt that her boyfriend would not be comfortable participating in a group setting “because it would be very uncomfortable for him to open up. He might be talking to other boys … or cheating so; he might feel insecure about opening up in a group”. Other girls felt as follows:
If a boy is having sex with a girl, he has to be concerned; he needs to know how a girl keeps her vagina cleaned. [Female group]
Others felt that a girl’s health should be their partner’s first priority.
Discussion
This study evaluated IVPs among adolescent young adult couples in Lusaka, Zambia. The main finding was that the IVPs for cleansing purposes were perceived as beneficial to enhancing hygiene, health, and sexual satisfaction for both girls and boys; however, couples expressed concern about the health effects of IVPs used for tightening and a desire for learning more about this practice as well as stopping it.
Knowledge and rationale for engaging in IVP include tightening and cleaning the vagina, primarily for hygiene, health, and sexual satisfaction purposes. Attitudes toward IVP concern willingness to stop or support the partner to discontinue IVP used for cleaning and tightening. The girls interviewed indicated having learned about IVPs in both formal and informal settings from peers, mothers, and grandmothers as early as age 10 or 11, soon after the onset of puberty and prior to becoming sexually active. These results are in line with those of previous studies on IVP3,4 which reported that women are introduced to IVPs at an early age by elderly women and use is motivated by male sexual preferences. This finding is also in agreement with Mwenda’s finding which showed that although practices such as IVP may place women at risk for sexually transmitted diseases, these practices are customary in many parts of Africa, culturally driven, and difficult to change.9
Attitudes toward IVP, particularly the willingness to stop or support a partner’s discontinuation of IVP used for tightening, were influenced by the negative health effects of tightening. Both boys and girls reported tightening the vagina in preparation for or during sexual intercourse as a means of increasing pleasure for the man and sometimes the woman, while cleaning IVPs are believed to keep girls clean, free from disease, and sexually desirable.8 Responses suggest that the promotion of tightening cessation in a prevention program would not pose an issue, as adolescents and young adults understand the health impacts associated with IVPs. In a previous study, Sivapalasingam et al implemented a behavioral intervention to reduce IVP use among HIV-1 uninfected Kenyan women and found that group counseling was effective in reducing IVPs for 3 months.20 However, the majority of the couples in the present study appreciated the use of focus groups and claimed that focus groups would provide a safe environment to gather, discuss, and learn things that could help their relationships. Focus groups have been regarded as an appropriate method of data collection for helping collect young person’s perspectives on a variety of issues related to health and well-being.21 This view is also consistent with that of Levine and Zimmerman, who suggested that if young participants are acknowledged as experts, then “the results are likely to have high face validity and can be useful in the development of programs and services”.10 Lewis, however, emphasized how challenging it can be to hold focus groups with young people as they can adopt themes adopted previously by other young people, other than adopting their own opinion.11
In this study, female and male focus groups were conducted separately. Female participants in this study identified this as an advantage, indicating that it allowed them to express perceptions freely. This benefit was also expressed in a study by Liefooghe et al.12
Limitations
A limitation of this study is the self-selection sampling technique used to optimize the inclusion of participants, which may have influenced the heterogeneity of the study participants and our ability to acquire a great diversity of themes, which is the ultimate goal of qualitative research.22 An additional uncontrolled factor is the possibility that because the participants were motivated to visit a Youth-Friendly Corner to access sexual reproductive health services, thus their experiences may be subject to bias than if other participants participated.
Furthermore, while these focus group discussion findings provide valuable insight into the perceptions adolescents and young adults hold regarding IVP, they are limited in that participants may have shared what they believe are the correct perceptions, or the perceptions expected by the researchers, rather than their real opinions. Because couples never communicated about IVPs, their use of negative health effects prior to the focus groups, their comments may have partly been in response to their assumption rather than their partners’ actual views. Future studies on the current topic are, therefore, recommended.
Lastly, to maintain anonymity and confidentiality of the study participants, the study neither collected participants’ personal information nor required identification of study participants. Thus, discussion comments could not be sorted by individual sociodemographic characteristics such as age, relationship status, education, and employment.
Conclusion
This study is the first to describe knowledge, attitudes, and IVPs among adolescent and young couples and to evaluate strategies for changing IVPs. Results offer insight for a more nuanced understanding of adolescent and young adult couples’ knowledge, views, and male partners’ attitudes toward IVPs. The qualitative observations are essential in order to design and implement further research focused on changing IVPs, specifically for adolescents and young adults in Zambia. Although couples expressed concern about the health effects of IVPs used for tightening, they expressed a desire for learning more about this practice as well as stopping it, which indicates that a community-based education program may be effective in improving the knowledge of IVPs and ultimately reducing the prevalence of IVPs. On the other hand, we found positive perceptions in regard to IVPs used for cleaning purposes, with most participants viewing them as essential to enhance hygiene, health, and sexual intercourse for both girls and boys.
The strong cultural component influencing IVPs suggests that involving the community, including traditional marriage counselors, should be a critical component to design IVP interventions and decrease the risk for HIV infection among this vulnerable population.
Acknowledgments
We would like to thank the adolescents and young adults who participated in this study, as well as the participating health facilities for providing us access to the study participants. This work was supported by grants from USAID though Pact AID61181600001, the NIH K23HD074489, the Miami CFAR P30AI073961 and the University of Miami Provost Research Award.
Author contributions
IKM, MLA, and MC conducted the focus groups. EDJ and BC transcribed the audio recordings and performed the first coding. IKM drafted the initial manuscript. SMW, and DLJ participated in the study design and data analysis and reviewed the final manuscript. VJR and SB served as observers of the focus groups. All authors contributed toward data analysis, drafting and revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Alcaide ML, Chisembele M, Malupande E, et al. A bio-behavioral intervention to decrease intravaginal practices and bacterial vaginosis among HIV infected Zambian women, a randomized pilot study. BMC Infect Dis. 2017;17(1):338. | ||
Alcaide ML, Chisembele M, Mumbi M, Malupande E, Jones D. Examining targets for HIV prevention: intravaginal practices in urban Lusaka, Zambia. AIDS Patient Care STDS. 2014;28(3):121–127. | ||
Alcaide ML, Mumbi M, Chitalu N, Jones DL. An intervention to decrease intravaginal practices in HIV-infected women in Zambia: a pilot study. J Assoc Nurses AIDS Care. 2013;24(3):219–226. | ||
Alcaide ML, Rodriguez VJ, Fischl MA, Jones DL, Weiss SM. Addressing intravaginal practices in women with HIV and at-risk for HIV infection, a mixed methods pilot study. Int J Womens Health. 2017;9:123–132. | ||
Butts SA, Parmley LE, Alcaide ML, et al. Let us fight and support one another: adolescent girls and young women on contributors and solutions to HIV risk in Zambia. Int J Womens Health. 2017;9:727–737. | ||
Government of Zambia, National AIDS Council. Zambia country report: monitoring the declaration of commitment on HIV and AIDS and the universal access biennial report. Vol. 72. Lusaka, Zambia: Ministry of Health; 2014. | ||
Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112. | ||
Hilber AM, Francis SC, Chersich M, et al. Intravaginal practices, vaginal infections and HIV acquisition: systematic review and meta-analysis. PLoS One. 2010;5(2):e9119. | ||
Mwenda KK. Labia elongation under African customary law: a violation of women’s rights? Int J Hum Rights. 2006;10(4):341–357. | ||
Scorgie F, Smit JA, Kunene B, Martin-Hilber A, Beksinska M, Chersich MF. Predictors of vaginal practices for sex and hygiene in KwaZulu-Natal, South Africa: findings of a household survey and qualitative inquiry. Cult Health Sex. 2011;13(4):381–398. | ||
Lewis A. Group child interviews as a research tool. Br Educ Res J. 1992;18(4):413–421. | ||
Liefooghe R, Michiels N, Habib S, Moran MB, De Muynck A. Perception and social consequences of tuberculosis: a focus group study of tuberculosis patients in Sialkot, Pakistan. Soc Sci Med. 1995;41(12):1685–1692. | ||
National Youth Constitutional Assembly. The World Program of Action for Youth (WPAY): youth perspective evaluation report, Zambia. Vol. 30. Lusaka, Zambia: National Youth Constitutional Assembly; 2005. | ||
Panacek EA, Thompson CB. Sampling methods: selecting your subjects. Air Med J. 2007;26(2):75–78. | ||
Central Statistical Office. Census of Population and Housing Preliminary Report. Lusaka, Zambia: Central Statistical Office; 2010. | ||
USAID, 2018. Zambia: Nutrition Profile. Available from: https://www.usaid.gov/sites/default/files/documents/1864/Zambia-Nutrition-Profile-Mar2018-508.pdf. Accessed May 18, 2018. | ||
Z-CHHP. Assessing HIV vulnerability in priority populations: a community based formative research in Zambia. Lusaka, Zambia: Pact, Inc.; 2016. | ||
Mcrackan TR, Velozo CA, Holcomb MA, et al. Use of adult patient focus groups to develop the initial item bank for a cochlear implant quality-of-life instrument. JAMA Otolaryngol Head Neck Surg. 2017;143(10):975–982. | ||
Krueger RA, Casey MA. Focus Groups: A Practical Guide for Applied Research. Thousand Oaks (CA): SAGE Publications Inc.; 2014. | ||
Sivapalasingam S, McClelland RS, Ravel J, et al. An effective intervention to reduce intravaginal practices among HIV-1 uninfected Kenyan women. AIDS Res Hum Retroviruses. 2014;30(11):1046–1057. | ||
Peterson-Sweeney K. The use of focus groups in pediatric and adolescent research. J Pediatr Health Care. 2005;19(2):104–110. | ||
Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. | ||
Moise IK, Mulhall PF. Providers’ perspectives on case management of a Healthy Start Program: A qualitative study. PLoS One. 2016;11(5):e0154668. | ||
Moise IK, Green DL, Toth J, Mulhall PF. Evaluation of an authority innovation-decision: Brief alcohol intervention for pregnant women receiving women, infants, and children services at two Illinois health departments. Subst Use Misuse. 2014;49(7):804–812. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.