Back to Journals » Infection and Drug Resistance » Volume 19
Admission D-Dimer for Early Risk Stratification of in-Hospital Mortality in Adults with Non-HIV Cryptococcal Meningitis: A Retrospective Cohort Study
Authors Wu Q, Xiao X, Zhou H, Chen S, Hu J, Wang Z, Zeng W ![]()
Received 17 May 2026
Accepted for publication 8 July 2026
Published 17 July 2026 Volume 2026:19 625174
DOI https://doi.org/10.2147/IDR.S625174
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Qiong Wu,1 Xiangzhi Xiao,2 Huashan Zhou,3 Sufen Chen,4 Jue Hu,4 Zhen Wang,4 Wengao Zeng2
1Department of Neurosurgery, The Affiliated Changsha Central Hospital, Hengyang Medical School, University of South China, Changsha, Hunan, People’s Republic of China; 2Department of Internal Medicine, The Second Hospital of Changsha (West Branch of Changsha Hospital for Maternal & Child Health Care), Changsha, Hunan, People’s Republic of China; 3Department of Pathology, The Second Hospital of Changsha (West Branch of Changsha Hospital for Maternal & Child Health Care), Changsha, Hunan, People’s Republic of China; 4Department of Neurology, The Affiliated Changsha Central Hospital, Hengyang Medical School, University of South China, Changsha, Hunan, People’s Republic of China
Correspondence: Wengao Zeng, Department of Internal Medicine, The Second Hospital of Changsha (West Branch of Changsha Hospital for Maternal & Child Health Care), Changsha, Hunan, People’s Republic of China, Tel +8613357311022, Email [email protected]
Background: Cryptococcal meningitis (CM) is a life-threatening central nervous system fungal infection. In adults without human immunodeficiency virus (HIV) infection, early prognostic indicators remain limited. D-dimer reflects activation of coagulation and fibrinolysis and may provide prognostic information in severe infections, but its significance in non-HIV CM is unclear.
Methods: We retrospectively included consecutive adults with microbiologically confirmed non-HIV CM admitted to a tertiary teaching hospital from January 2012 to December 2023. The primary outcome was all-cause in-hospital mortality. Missing data were handled using multiple imputation. Candidate predictors were selected using least absolute shrinkage and selection operator regression across five imputed datasets. Multivariable analysis used Firth’s penalized logistic regression, and coefficients were pooled according to Rubin’s rules. Model performance was assessed using receiver operating characteristic analysis, calibration plots, decision curve analysis, and bootstrap internal validation.
Results: Among 104 patients, 22 (21.2%) died during hospitalization. Admission D-dimer was independently associated with in-hospital mortality (odds ratio [OR] 1.41, 95% confidence interval [CI] 1.03– 1.94, P = 0.033). Cerebral infarction, cerebrospinal fluid (CSF) adenosine deaminase (ADA), and CSF cryptococcal antigen positivity were retained in the exploratory model but were not statistically significant. The model showed acceptable apparent discrimination (area under the receiver operating characteristic curve [AUC] 0.793, 95% CI 0.675– 0.911). Bootstrap internal validation yielded an optimism-corrected AUC of 0.753 and calibration slope of 0.790. Log-transformed D-dimer showed directionally consistent results.
Conclusion: Elevated admission D-dimer was independently associated with in-hospital mortality in adults with non-HIV CM. D-dimer may help early risk stratification, but the exploratory model requires external validation before clinical implementation.
Keywords: cryptococcal meningitis, non-HIV, D-dimer, cerebral infarction, CSF cryptococcal antigen, in-hospital mortality, risk stratification
Introduction
Cryptococcal meningitis (CM) remains one of the most devastating fungal infections of the central nervous system, with outcomes that are often determined by delayed diagnosis, neurological complications, and early clinical deterioration.1–3 Although classically associated with human immunodeficiency virus (HIV) infection, the epidemiological profile of CM has changed in recent years.4,5 Increasing use of immunosuppressive therapies, expansion of organ transplantation programs, and global population aging have contributed to a growing number of cases occurring in individuals without HIV infection.6,7 Compared with HIV-associated CM, non-HIV CM occurs in patients with more heterogeneous immune backgrounds, including immunocompromised and apparently immunocompetent hosts. This clinical heterogeneity may lower the initial suspicion of CM in some patients, thereby delaying diagnosis and complicating early prognostic assessment.3,8,9
Early identification of patients at high risk of adverse outcomes is therefore essential for optimizing clinical management. However, reliable prognostic biomarkers for non-HIV CM remain incompletely defined.10–12 Reported predictors often reflect advanced neurological involvement, such as cerebral infarction, hydrocephalus, intracranial hypertension, or impaired consciousness, and may therefore have limited value for very early risk stratification.10,11,13 A readily available admission biomarker that captures systemic severity before irreversible neurological deterioration would be clinically useful.
Accumulating evidence suggests that dysregulation of the inflammation–coagulation axis plays an important role in the pathophysiology of severe infections.14–16 Systemic inflammatory responses can activate coagulation pathways, promote endothelial injury, and induce microvascular thrombosis, thereby contributing to organ dysfunction.17–21 D-dimer, a degradation product of cross-linked fibrin, reflects activation of coagulation and fibrinolysis and has been widely investigated as a prognostic biomarker in sepsis and other infectious diseases.22–24 However, the clinical significance of D-dimer in fungal infections of the central nervous system has not been well established.25–27
Cerebral infarction is a recognized complication of cryptococcal meningitis and has been consistently associated with poor neurological outcomes.28–30 Cerebral venous sinus thrombosis has also recently been described in previously healthy patients with cryptococcal meningitis and may represent another thrombotic mechanism linking infection, D-dimer elevation, and adverse outcomes.31 Whether systemic coagulation activation, reflected by elevated D-dimer levels, contributes to mortality through cerebrovascular complications or through broader systemic inflammatory, endothelial, and microvascular mechanisms remains uncertain.14,17,19,28–31
Therefore, this study aimed to determine whether admission D-dimer is associated with in-hospital mortality in adults with microbiologically confirmed non-HIV cryptococcal meningitis. We further examined the contribution of cerebral infarction and other routinely available inflammatory or microbiological markers to an exploratory risk-stratification model designed to support early identification of high-risk patients in neuroinfectious disease practice.
Methods
Study Design and Population
This retrospective cohort study was conducted at a tertiary teaching hospital and included consecutive adult patients (≥18 years) diagnosed with non-HIV CM between January 2012 and December 2023. Diagnosis required microbiological confirmation from cerebrospinal fluid (CSF), including positive India ink staining, cryptococcal culture, or CSF cryptococcal antigen, combined with compatible clinical and radiological findings. Patients with confirmed HIV infection or hospital stays shorter than 24 hours were excluded from the analysis.
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for observational cohort studies. Because the prognostic model was exploratory and internally validated only, model-related reporting was additionally guided by relevant items from the Transparent Reporting of a multivariable prediction model for Individual Prognosis Or Diagnosis (TRIPOD) reporting framework.
The study protocol was approved by the Ethics Committee of Changsha Central Hospital (Approval No. 20240106). The requirement for informed consent was waived due to the retrospective design of the study. All patient data were handled confidentially and analyzed anonymously, and the study was conducted in accordance with the Declaration of Helsinki.
Data Collection
Demographic characteristics, comorbidities, clinical manifestations, laboratory results within 24 hours of admission, CSF cryptococcal antigen status, CSF adenosine deaminase (ADA), other CSF parameters, and documented neuroimaging findings were extracted from electronic medical records. The routinely extracted laboratory tests included blood inflammatory and coagulation markers (including D-dimer, C-reactive protein, procalcitonin, neutrophil count, platelet count, prothrombin time, activated partial thromboplastin time, international normalized ratio, and fibrinogen), biochemical indices (including albumin, fasting blood glucose, creatinine, uric acid, bilirubin fractions, alanine aminotransferase, and lipid indices), and CSF measurements (including opening pressure, white blood cell count, glucose, protein, chloride, ADA, India ink staining, fungal culture, and cryptococcal antigen). Cerebral infarction was diagnosed based on neuroimaging, including magnetic resonance imaging or computed tomography available during admission, but the retrospective records did not allow reliable distinction between infarction present at admission and infarction newly detected or occurring during hospitalization. Admission D-dimer was defined as the first D-dimer measurement obtained within 24 hours after hospital admission. We rechecked the laboratory reporting records and confirmed that all D-dimer values were reported in the same unit, mg/L. D-dimer was therefore analyzed as a continuous variable without unit conversion. Laboratory results were extracted as reported in the hospital electronic medical record and laboratory information systems. Because this retrospective cohort covered a long study period from 2012 to 2023, detailed historical information on assay platforms, reagent manufacturers, and reference intervals for all laboratory variables could not be consistently retrieved. Therefore, laboratory variables were analyzed according to the values, units, and hospital reference intervals recorded in the original laboratory reports where available. CSF cryptococcal antigen positivity referred to documented positive CSF cryptococcal antigen testing in the available medical records; antigen titers were not consistently available and were therefore not analyzed. Cerebral venous sinus thrombosis could not be systematically extracted from the retrospective records.
Outcome Definition
The primary endpoint was all-cause in-hospital mortality.
Statistical Analysis
All statistical analyses were performed using R (version 4.5.3), and a two-sided P value <0.05 was considered statistically significant.
Because D-dimer values were right-skewed, their distribution was inspected visually and summarized as median with interquartile range. A sensitivity analysis using log-transformed D-dimer was performed to assess the robustness of the association.
Missingness was assessed before analysis. Missing values were present in several laboratory variables, with the highest missingness observed for triglycerides (5.77%) and 3.85% missingness for CSF ADA. Missing data were handled using multiple imputation by chained equations. Five imputed datasets were generated with 10 iterations. Twelve clinically plausible candidate predictors were evaluated at the start of least absolute shrinkage and selection operator (LASSO) selection: D-dimer, age, cerebral infarction, CSF protein, fasting blood glucose, CSF ADA, CSF cryptococcal antigen positivity, activated partial thromboplastin time, disease duration, CSF chloride, headache, and hepatitis B. Candidate predictors were selected using LASSO regression across the imputed datasets. D-dimer was prespecified as the primary exposure of interest based on biological plausibility and prior evidence, and it was selected by LASSO in all five imputed datasets. Variables selected in at least two imputed datasets were considered for the final exploratory model, and the number of predictors was constrained according to an events-per-variable (EPV) threshold of at least 5. Potential confounding by comorbidities and severity-related variables was addressed within this constrained variable-selection framework; variables not retained in the final model were interpreted descriptively because the number of deaths limited the number of covariates that could be reliably adjusted for.
Multivariable modeling was performed using Firth’s penalized logistic regression in each imputed dataset to mitigate small-sample bias and potential separation. Regression coefficients were pooled according to Rubin’s rules. Model discrimination was assessed using the area under the receiver operating characteristic curve (AUC), and calibration was evaluated using calibration plots and the calibration slope. Internal validation was performed using bootstrap resampling with 1000 iterations to estimate optimism-corrected performance. Decision curve analysis was used to evaluate potential clinical utility.
An exploratory mediation analysis was conducted to examine whether cerebral infarction mediated the association between D-dimer and in-hospital mortality using a quasi-Bayesian approach with 1000 simulations. Given the observational design and limited sample size, the mediation analysis was considered exploratory.
Results
Clinical, Laboratory, and Neuroimaging Characteristics
Clinical, laboratory, cerebrospinal fluid, and documented neuroimaging characteristics are summarized in Table 1. A total of 104 patients were included, with a median age of 53 years (interquartile range [IQR], 41–62); 58.7% were male. Twenty-two patients (21.2%) died during hospitalization. Non-survivors were older, had more frequent documented cerebral infarction on available neuroimaging, and exhibited lower serum albumin levels and higher inflammatory markers, including C-reactive protein and procalcitonin, suggesting greater systemic illness severity. Because the timing of cerebral infarction could not be reliably distinguished as pre-existing, present at admission, or newly occurring during hospitalization, this variable should be interpreted as a documented clinical/neuroimaging finding rather than a baseline characteristic. Admission D-dimer levels tended to be higher among non-survivors than among survivors, although the between-group difference did not reach conventional statistical significance in the univariate comparison (P = 0.055). In non-survivors, D-dimer values ranged from 0.02 to 17.80 mg/L, with an IQR of 0.65–3.80 mg/L. Exploratory Spearman rank correlations among non-survivors showed that D-dimer correlated positively with procalcitonin (rho = 0.689) and C-reactive protein (rho = 0.395) and negatively with albumin (rho = −0.484). D-dimer was prespecified as the primary exposure of interest and was selected by LASSO in all five imputed datasets.
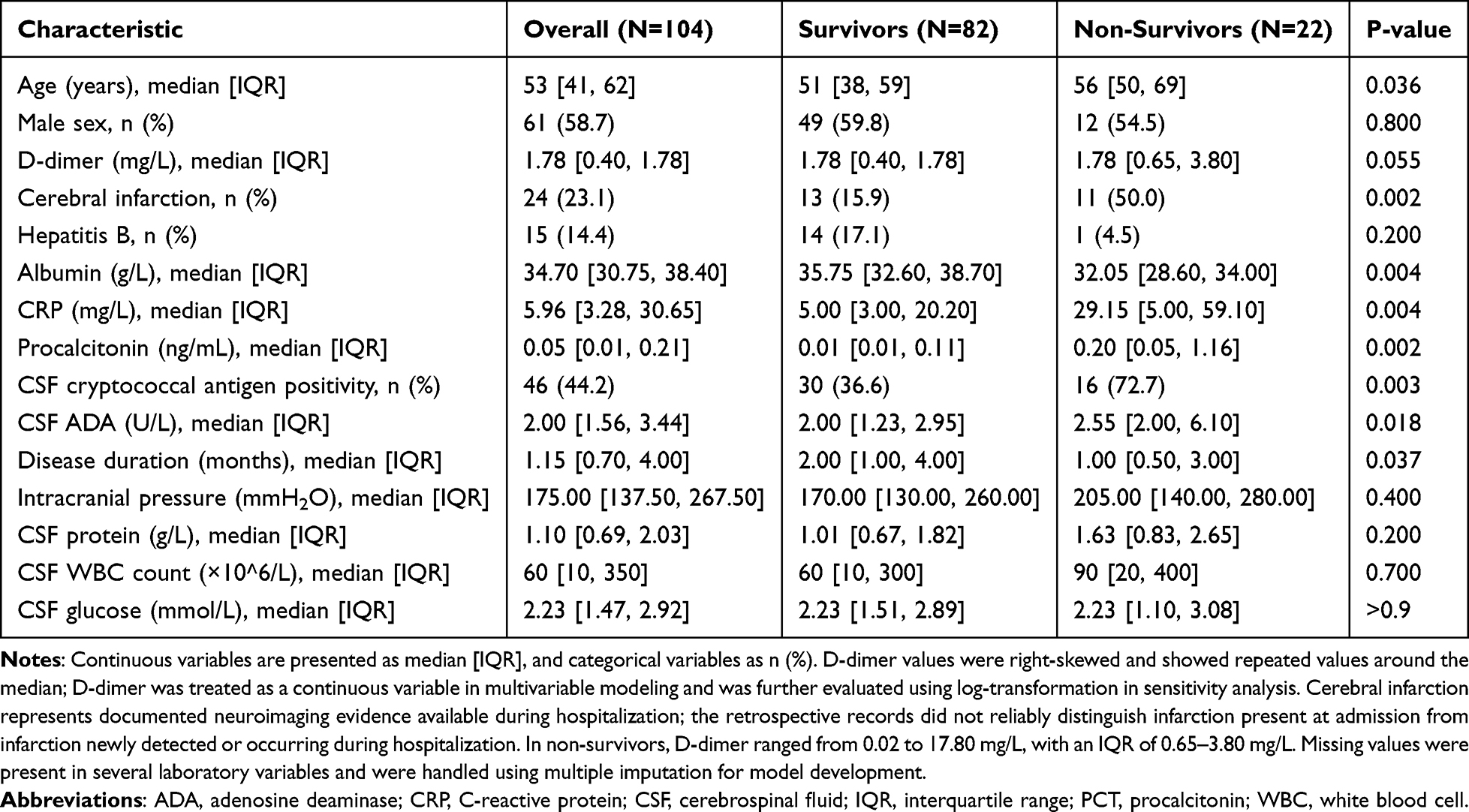 |
Table 1 Clinical, Laboratory, and Neuroimaging Characteristics of Patients |
Multivariable Analysis
Twelve candidate predictors were initially evaluated. Across the five imputed datasets, D-dimer was selected in all datasets, cerebral infarction in four datasets, and CSF ADA, CSF cryptococcal antigen positivity, CSF protein, fasting blood glucose, headache, and hepatitis B in three datasets. Under the prespecified EPV constraint, the final exploratory model included four predictors: D-dimer, cerebral infarction, CSF ADA, and CSF cryptococcal antigen positivity. The EPV was 5.5.
In the pooled Firth penalized logistic regression model, higher admission D-dimer was independently associated with in-hospital mortality (odds ratio [OR] 1.41, 95% confidence interval [CI] 1.03–1.94, P = 0.033). Cerebral infarction showed a directionally increased risk but did not reach statistical significance (OR 2.63, 95% CI 0.83–8.30, P = 0.100). CSF ADA and CSF cryptococcal antigen positivity were also retained in the model but were not statistically significant (Table 2).
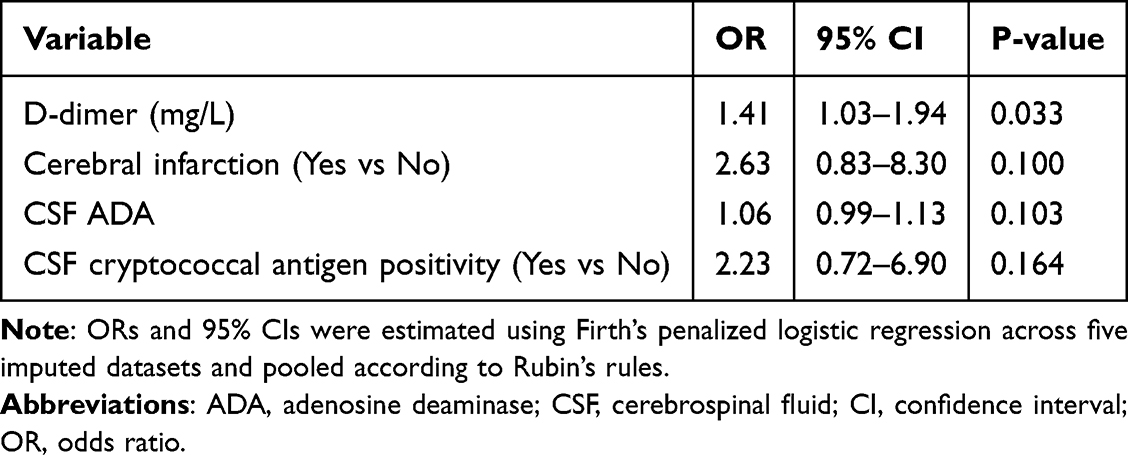 |
Table 2 Pooled Firth’s Penalized Logistic Regression Analysis of in-Hospital Mortality Across Five Imputed Datasets |
Sensitivity Analysis
In the sensitivity analysis using log-transformed D-dimer, higher log-D-dimer remained associated with in-hospital mortality (OR 3.09, 95% CI 1.16–8.25, P = 0.024), supporting the robustness of the primary association.
Model Performance
The final exploratory model demonstrated acceptable apparent discrimination, with an AUC of 0.793 (95% CI 0.675–0.911) (Figure 1). Bootstrap internal validation with 1000 resamples yielded an optimism-corrected AUC of 0.753, an optimism-corrected calibration slope of 0.790, and a shrinkage factor of 0.861, suggesting moderate model stability. Calibration analysis showed acceptable overall agreement between predicted and observed mortality probabilities (Figure 2). Decision curve analysis suggested potential net benefit across clinically relevant threshold probabilities, with model net benefit ranging from 0.0288 to 0.2036 (Figure 3). An exploratory nomogram was constructed to visualize the retained predictors and the structure of the exploratory model (Figure 4).
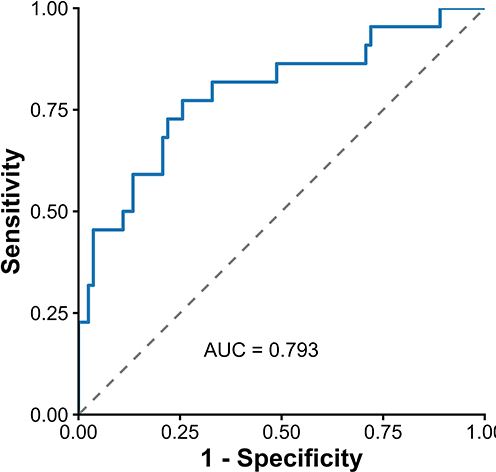 |
Figure 1 Receiver operating characteristic curve of the exploratory risk-stratification model. The model demonstrated acceptable apparent discrimination for in-hospital mortality, with an area under the receiver operating characteristic curve (AUC) of 0.793 (95% CI 0.675–0.911). The grey dashed diagonal line represents the no-discrimination reference line, corresponding to an AUC of 0.5. AUC, area under the receiver operating characteristic curve. |
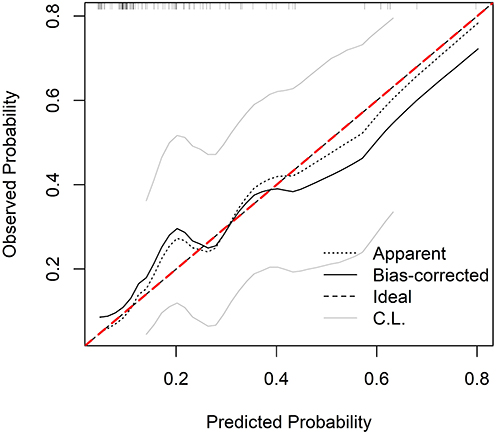 |
Figure 2 Calibration plot of the exploratory risk-stratification model. The calibration plot compares predicted and observed probabilities of in-hospital mortality. The red dashed diagonal line represents ideal calibration, where predicted probabilities equal observed probabilities. Bootstrap internal validation yielded an optimism-corrected calibration slope of 0.790, indicating moderate model stability. |
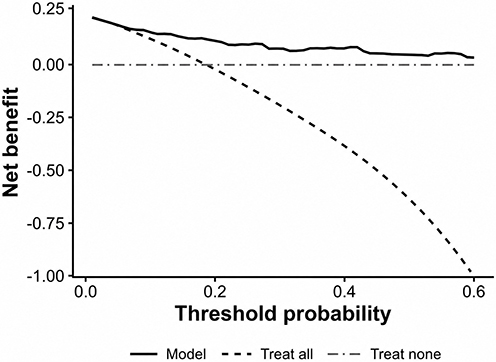 |
Figure 3 Decision curve analysis of the exploratory risk-stratification model. The decision curve evaluates the potential clinical net benefit of using the model across different threshold probabilities for predicting in-hospital mortality. The solid line represents the model, the dashed curve represents the treat-all strategy, and the horizontal dash-dotted line at zero represents the treat-none strategy. The model showed potential net benefit across clinically relevant threshold probabilities, with model net benefit ranging from 0.0288 to 0.2036. |
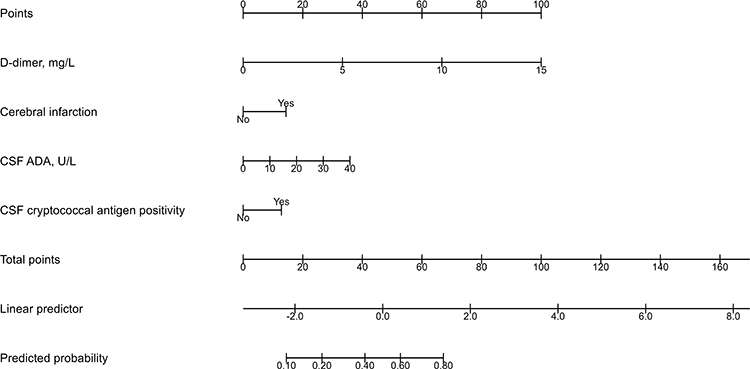 |
Figure 4 Exploratory nomogram illustrating the structure of the risk-stratification model for in-hospital mortality in adults with non-HIV cryptococcal meningitis. The nomogram includes admission D-dimer, cerebral infarction, CSF adenosine deaminase, and CSF cryptococcal antigen positivity. It is intended for visualization of the exploratory model only and requires external validation before clinical application. Abbreviation: ADA, adenosine deaminase. |
Mediation Analysis
In the exploratory mediation analysis, the total effect of D-dimer on in-hospital mortality was statistically significant (estimate 0.0439, 95% CI 0.0018–0.0825, P = 0.044). However, the average causal mediation effect through cerebral infarction was not significant (estimate 0.0030, 95% CI −0.0197 to 0.0287, P = 0.754), and the average proportion mediated was small and not statistically significant (5.6%, P = 0.718). These findings suggest that overt cerebral infarction did not substantially mediate the association between D-dimer and mortality.
Discussion
In this retrospective cohort of adults with non-HIV cryptococcal meningitis, elevated admission D-dimer was independently associated with in-hospital mortality after LASSO variable selection across imputed datasets and pooled Firth penalized logistic regression. The association remained robust in the sensitivity analysis using log-transformed D-dimer. Cerebral infarction, CSF ADA, and CSF cryptococcal antigen positivity were retained in the exploratory model but did not reach statistical significance after multivariable adjustment. These findings suggest that D-dimer may serve as a routinely available marker of disease severity and may support early risk stratification in neuroinfectious disease practice.
Previous studies have reported associations between neurological complications, particularly cerebral infarction, and poor outcomes in non-HIV cryptococcal meningitis.10,29 In the present cohort, documented cerebral infarction was more frequent among non-survivors and was retained during exploratory variable selection. However, because the retrospective records did not reliably establish whether infarction was pre-existing, present at admission, or developed during hospitalization, this finding should not be interpreted as a pure baseline difference. Its association with in-hospital mortality also did not reach statistical significance after multivariable adjustment. Thus, our findings do not confirm cerebral infarction as an independent prognostic factor in this cohort. Rather, admission D-dimer remained independently associated with in-hospital mortality, suggesting that coagulation activation may capture prognostic information not fully explained by overt cerebral infarction. The lower albumin and higher C-reactive protein and procalcitonin levels observed among non-survivors also indicate that systemic inflammation, possible bacterial co-infection or sepsis, nutritional status, and overall illness severity may contribute to both D-dimer elevation and mortality. Because only 22 deaths occurred, these related variables could not all be included simultaneously in the final model without overfitting, and residual confounding should be considered when interpreting the association between D-dimer and mortality.
Accumulating evidence suggests that severe infections are characterized by complex interactions among inflammation, coagulation activation, and endothelial dysfunction.14,17,19,32,33 Endothelial injury induced by systemic inflammation may further exacerbate coagulation activation and microvascular thrombosis. In cryptococcal meningitis, these processes may be particularly relevant because infection-induced inflammatory responses occur within the confined intracranial compartment. Microvascular thrombosis and endothelial dysfunction may impair cerebral perfusion, exacerbate neuronal injury, and contribute to neurological deterioration. Elevated D-dimer levels may therefore reflect systemic activation of the coagulation cascade and serve as an indirect marker of infection severity and endothelial injury.34–36
The prognostic relevance of D-dimer may be particularly important in cryptococcal meningitis because this infection affects the central nervous system and may be complicated by cerebral infarction, vasculopathy, and cerebral venous sinus thrombosis.29–31 The exploratory mediation analysis suggested that overt cerebral infarction did not substantially mediate the association between D-dimer and mortality. Although the total effect of D-dimer was statistically significant, the average causal mediation effect through cerebral infarction was small and not significant. This finding supports the possibility that D-dimer may reflect broader systemic and microvascular processes, rather than merely serving as a marker of clinically apparent ischemic stroke.37,38 However, the retrospective records did not allow systematic identification of cerebral venous sinus thrombosis or reliable distinction between recent and old cerebral infarction at admission, so these mechanisms require targeted prospective evaluation.
CSF ADA and CSF cryptococcal antigen positivity were retained during exploratory variable selection, but neither variable reached statistical significance in the final multivariable model. CSF ADA should be interpreted cautiously because it is more commonly used as an adjunctive marker for tuberculous meningitis and is not a specific prognostic biomarker for cryptococcal meningitis. CSF cryptococcal antigen positivity may reflect microbiological confirmation or possible organism burden, but antigen titers were not analyzed in this study. These variables should therefore be regarded as exploratory covariates rather than primary prognostic findings.
From a clinical perspective, D-dimer measurement is inexpensive, widely available, and routinely performed in many hospitals. Early identification of patients with markedly elevated D-dimer levels may therefore facilitate closer monitoring and prompt clinicians to consider more aggressive supportive management. D-dimer elevation has also been investigated in other invasive infections and systemic mycoses, including candidemia in critically ill patients, where coagulation and inflammatory abnormalities may accompany poor outcomes.25,39 Nevertheless, the present model should be interpreted as an exploratory risk-stratification tool rather than a validated clinical prediction model.
Several limitations should be acknowledged. First, this was a retrospective single-center study with a modest sample size and only 22 in-hospital deaths, which limited the number of predictors that could be reliably evaluated. Second, although multiple imputation, Firth’s penalized regression, and bootstrap internal validation were used to reduce bias from missing data, small-sample bias, and optimism, external validation was not available. Therefore, the proposed model should be regarded as exploratory and hypothesis-generating rather than ready for direct clinical implementation. Third, detailed treatment and management variables, including antifungal regimen, timing of antifungal initiation, serial intracranial pressure management, and treatment modifications during hospitalization, were not consistently available in the retrospective dataset and therefore could not be incorporated into the multivariable model. Residual confounding from these factors cannot be excluded. Fourth, comorbidities and systemic conditions that may alter D-dimer levels or affect all-cause in-hospital mortality, such as sepsis, active thrombosis, malignancy, immune disease, diabetes, liver disease, or other inflammatory conditions, could not be fully adjusted for because of the limited number of outcome events and incomplete retrospective documentation. Fifth, although all D-dimer values were confirmed to be reported in the same unit of mg/L, detailed historical information on assay platforms, reagent manufacturers, and reference intervals for all laboratory variables could not be consistently retrieved across the 2012–2023 study period. Therefore, potential assay-platform or reference-interval heterogeneity could not be fully excluded, although D-dimer unit consistency was verified. Sixth, cerebral venous sinus thrombosis and the timing of cerebral infarction could not be systematically extracted, so the relative contributions of arterial infarction, venous thrombosis, and systemic coagulation activation remain uncertain. Seventh, variable selection was constrained by the small number of outcome events, and the inclusion of CSF ADA and CSF cryptococcal antigen positivity should be interpreted as exploratory. Despite these limitations, the study used a prespecified statistical workflow, multiple imputation, penalized regression, and bootstrap internal validation to mitigate important methodological limitations and provides preliminary evidence for the role of admission D-dimer in early risk stratification.
Conclusion
Elevated admission D-dimer was independently associated with increased in-hospital mortality in adults with non-HIV cryptococcal meningitis, and this association remained robust in a log-transformed sensitivity analysis. D-dimer may help support early risk stratification and identify patients who require closer monitoring during hospitalization. Further multicenter studies with prospective assessment of thrombotic complications including cerebral venous sinus thrombosis and external validation are needed before clinical implementation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tugume L, Ssebambulidde K, Kasibante J, et al. Cryptococcal meningitis. Nature Reviews Disease Primers. 2023;9(1):62. doi:10.1038/s41572-023-00472-z
2. Person AK, Crabtree-Ramirez B, Kim A, et al. Cryptococcal meningitis and clinical outcomes in persons with human immunodeficiency virus: a global view. Clin Infect Dis. 2023;76(12):2116–10. doi:10.1093/cid/ciad076
3. Cumagun PM, Moore MK, McCarty TP, et al. Cryptococcal meningoencephalitis in phenotypically normal patients. Pathogens. 2023;12(11):1303. doi:10.3390/pathogens12111303
4. Sloan DJ, Parris V. Cryptococcal meningitis: epidemiology and therapeutic options. Clin Epidemiol. 2014;6:169–182. doi:10.2147/CLEP.S38850
5. Zhao Z, Song W, Liu L, et al. Trends in clinico-epidemiological profile and outcomes of patients with HIV-associated cryptococcal meningitis in Shanghai, China, 2013–2023. Viruses. 2024;16(8):1333. doi:10.3390/v16081333
6. Teekaput C, Yasri S, Chaiwarith R. Cryptococcal meningitis: differences between patients with and without HIV-infection. Pathogens. 2023;12(3):427. doi:10.3390/pathogens12030427
7. Williamson PR, Jarvis JN, Panackal AA, et al. Cryptococcal meningitis: epidemiology, immunology, diagnosis and therapy. Nat Rev Neurol. 2017;13(1):13–24. doi:10.1038/nrneurol.2016.167
8. Pinheiro SB, Sousa ES, Cortez ACA, et al. Cryptococcal meningitis in non-HIV patients in the State of Amazonas, Northern Brazil. Braz J Microbiol. 2021;52(1):279–288. doi:10.1007/s42770-020-00383-1
9. Beardsley J, Sorrell TC, Chen SC. Central Nervous System Cryptococcal Infections in Non-HIV Infected Patients. J Fungi. 2019;5(3):71. doi:10.3390/jof5030071
10. Liang F, Li R, Yao M, et al. Deciphering prognostic indicators in non-HIV cryptococcal meningitis: constructing and validating a predictive Nomogram model. Med Mycol. 2024;62(9):myae092. doi:10.1093/mmy/myae092
11. Namie H, Takazono T, Hidaka Y, et al. The prognostic factors for cryptococcal meningitis in non-human immunodeficiency virus patients: an observational study using nationwide database. Mycoses. 2024;67(1):e13658. doi:10.1111/myc.13658
12. Jiang YK, Zhou L-H, Cheng J-H, et al. Anti-GM-CSF autoantibodies predict outcome of cryptococcal meningitis in patients not infected with HIV: a cohort study. Clin Microbiol Infect. 2024;30(5):660–665. doi:10.1016/j.cmi.2024.01.018
13. Pescador Ruschel MA, Thapa B. Cryptococcal meningitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026.
14. Aklilu A, Lai MS-L, Jiang Z, et al. Immunothrombosis in sepsis: cellular crosstalk, molecular triggers, and therapeutic opportunities—a review. Int J Mol Sci. 2025;26(13):6114. doi:10.3390/ijms26136114
15. Costantini TW, Kornblith LZ, Pritts T, et al. The intersection of coagulation activation and inflammation after injury: what you need to know. J Trauma Acute Care Surg. 2024;96(3):347–356. doi:10.1097/TA.0000000000004190
16. Lazzaroni MG, Piantoni S, Masneri S, et al. Coagulation dysfunction in COVID-19: the interplay between inflammation, viral infection and the coagulation system. Blood Rev. 2021;46:100745. doi:10.1016/j.blre.2020.100745
17. Zhu L, Dong H, Li L, et al. The mechanisms of sepsis induced coagulation dysfunction and its treatment. J Inflamm Res. 2025;18:1479–1495. doi:10.2147/JIR.S504184
18. Dolmatova EV, Wang K, Mandavilli R, et al. The effects of sepsis on endothelium and clinical implications. Cardiovasc Res. 2021;117(1):60–73. doi:10.1093/cvr/cvaa070
19. Maneta E, Aivalioti E, Tual-Chalot S, et al. Endothelial dysfunction and immunothrombosis in sepsis. Front Immunol. 2023;14:1144229. doi:10.3389/fimmu.2023.1144229
20. Cheng L, Cao Y, Liu S, et al. Unveiling the research advances of sepsis: pathogenesis, precise intervention and clinical perspective. Int J Surg. 2025;111(9):6260–6289. doi:10.1097/JS9.0000000000002668
21. Wang Y, Guan Q-N, Zhang Z-J, et al. Interaction between endothelial injury and immune response in septic shock: from basic research to clinical applications. Front Physiol. 2025;16:1627008. doi:10.3389/fphys.2025.1627008
22. Qu X, Wang S, Ye X, et al. Prognostic value of baseline plasma D-dimer levels in sepsis: a prospective cohort study. Pract Lab Med. 2025;46:e00498. doi:10.1016/j.plabm.2025.e00498
23. Wu K, Van Name J, Xi L. D-Dimer as biomarker for prognosis of coronary artery disease and heart failure: reappraisal of its central role. Cardiology. 2025;151:181–191. doi:10.1159/000546154
24. Jia M, Lin S, Zhang J, et al. D-dimer is a strong predictor of mortality in paediatric hematological-oncological patients with severe infections. J Infect Chemother. 2025;31(3):102593. doi:10.1016/j.jiac.2024.12.022
25. Lou Y, Yu F, Zhao Y, et al. A multimarker panel for diagnosis and prognosis prediction of fungal infections. Clin Exp Med. 2026;26(1):120. doi:10.1007/s10238-026-02038-1
26. Meini S, Sozio E, Bertolino G, et al. D-Dimer as biomarker for early prediction of clinical outcomes in patients with severe invasive infections due to Streptococcus pneumoniae and neisseria meningitidis. Front Med. 2021;8:627830. doi:10.3389/fmed.2021.627830
27. Wang Y, Wei H, Shen L, et al. Immunological predictors of post infectious inflammatory response syndrome in HIV-negative immunocompetent cryptococcal meningitis. Front Immunol. 2022;13:895456. doi:10.3389/fimmu.2022.895456.
28. Ellis JP, Kalata N, Joekes EC, et al. Ischemic stroke as a complication of cryptococcal meningitis and immune reconstitution inflammatory syndrome: a case report. BMC Infect Dis. 2018;18(1):520. doi:10.1186/s12879-018-3386-0
29. Tu J, Zhang S, Liu Q, et al. Cerebral infarction in HIV-negative patients with cryptococcal meningitis: its predictors and impact on outcomes. BMC Infect Dis. 2022;22(1):825. doi:10.1186/s12879-022-07827-z
30. Mishra AK, Arvind VH, Muliyil D, et al. Cerebrovascular injury in cryptococcal meningitis. Int J Stroke. 2018;13(1):57–65. doi:10.1177/1747493017706240
31. Anjum SH, Hargarten J, Dulek B, et al. Cerebral venous thrombosis in previously healthy patients with cryptococcal meningitis. J Infect Dis. 2026;233(2):e561–e569. doi:10.1093/infdis/jiaf653
32. Jacobi J. The pathophysiology of sepsis-2021 update: part 1, immunology and coagulopathy leading to endothelial injury. Am J Health Syst Pharm. 2021;79(5):329–337. doi:10.1093/ajhp/zxab380
33. Girardis M, David S, Ferrer R, et al. Understanding, assessing and treating immune, endothelial and haemostasis dysfunctions in bacterial sepsis. Intensive Care Med. 2024;50(10):1580–1592. doi:10.1007/s00134-024-07586-2
34. Manzoor D, Bui C, Makhoul E, et al. Improvement in plasma D-dimer level in severe SARS-CoV-2 infection can be an indicator of fibrinolysis suppression: case reports. Medicine. 2021;100(15):e25255. doi:10.1097/MD.0000000000025255
35. Varikasuvu SR, Varshney S, Dutt N, et al. D-dimer, disease severity, and deaths (3D-study) in patients with COVID-19: a systematic review and meta-analysis of 100 studies. Sci Rep. 2021;11(1):21888. doi:10.1038/s41598-021-01462-5
36. Dumache R, Muresan CO, Laitin SMD, et al. COVID-19 organ injury pathology and D-Dimer expression patterns: a retrospective analysis. Diagnostics. 2025;15(15):1860. doi:10.3390/diagnostics15151860
37. Iba T, Tanigawa T, Wada H, et al. Recognizing coagulation disorders in sepsis in the emergency room: a narrative review. J Clin Med. 2026;15(2):488. doi:10.3390/jcm15020488
38. Zhou K, Chen Y, Pang J, et al. The endothelial-immunothrombotic storm in viral sepsis: lessons from COVID-19. Front Immunol. 2025;16:1681764. doi:10.3389/fimmu.2025.1681764
39. Yilmaz Karadag F, Ozturk Engin D, Buber AA, et al. Evaluation of candidemia cases in the intensive care unit of a tertiary training hospital during the period of COVID-19 pandemic. BMC Infect Dis. 2025;25(1):288. doi:10.1186/s12879-025-10688-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Nomogram for Predicting Overall Survival in Primary Central Nervous System Lymphoma: A Retrospective Study
Ling Y, Miao X, Zhou X, Ma J, Lin Z, Li Q, Zhang M, Ma Y, Chen B
Journal of Inflammation Research 2025, 18:2091-2103
Published Date: 10 February 2025