")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Adjunctive Rufinamide in Children with Lennox-Gastaut Syndrome: A Literature Review
Authors Balagura G, Riva A , Marchese F , Verrotti A, Striano P
Received 30 November 2019
Accepted for publication 14 January 2020
Published 5 February 2020 Volume 2020:16 Pages 369—379
DOI https://doi.org/10.2147/NDT.S185774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Ganna Balagura,1,2 Antonella Riva,2 Francesca Marchese,2 Alberto Verrotti,3 Pasquale Striano1,2
1Department of Neurosciences, Rehabilitation, Ophthalmology, Genetics, and Maternal and Child Health, University of Genoa, Genoa, Italy; 2Pediatric Neurology and Muscular Diseases Unit, IRCCS ‘G. Gaslini’ Institute, Genoa, Italy; 3Department of Pediatrics, University of L’Aquila, L’Aquila, Italy
Correspondence: Pasquale Striano Email [email protected]
Abstract: Lennox-Gastaut syndrome (LGS) is a severe, childhood-onset, developmental epileptic encephalopathy, with different etiologies and co-morbidities. Seizure treatment in LGS represents a major challenge; new antiepileptic drugs (AEDs) are developed to especially address seizures resulting in high morbidity and mortality, such as drop seizures. Rufinamide (RFN) is one of the latest AEDs licensed for patients with LGS. Its mechanism of action involves sodium channels in a way that is unrelated to other AEDs. Here we discuss the use of adjunctive RFN in children and adolescents with LGS and its efficacy and safety profile, based on a systematic literature review. RFN shows a very favorable profile in terms of adverse events and drug-interactions in children. It is particularly effective on tonic-atonic seizures and spasms, impacting on the quality of life of the patients. Further studies are needed to clarify the interaction profile with the newest AEDs for LGS and to assess correlations between the etiology of LGS and drug response to individualize treatment and maximize efficacy.
Keywords: rufinamide, Lennox-Gastaut, epilepsy, children
Introduction
Lennox-Gastaut syndrome (LGS) is a severe, childhood-onset, developmental epileptic encephalopathy characterized by the triad: drug-resistant epilepsy (featuring tonic, atonic, and atypical absence seizures), intellectual disability, and EEG abnormalities (diffuse slow spike-and-wave complexes and fast activity bursts).1,2
Lennox-Gastaut Syndrome may have different underlying causes, identifiable in almost two-thirds of patients. The etiology ranges from infectious causes, vascular or traumatic brain damage, congenital brain malformations, to genetic disorders or metabolic diseases.3
Besides seizures, LG syndrome carries a burden of cognitive impairment, which often worsens over time, alongside with behavioral and psychiatric problems, and motor impairment, based on the underlying cause.3 Drug-resistant epilepsy heavily influences the quality of life of the patient and the family, increasing the risk of morbidity and mortality, and minimizing the developmental potential.
Anti-seizure treatment in LGS usually includes a combination of different antiepileptic drugs (AEDs):4 valproate (VPA), lamotrigine (LTG), and topiramate (TPM) are often first-line drugs, whereas second-line options include levetiracetam (LEV), clobazam (CLB), zonisamide (ZNS), and rufinamide (RFN).3 Despite new AEDs are becoming available for the seizure treatment in LGS, this remains a big challenge for epileptologists. Here, we review the therapeutic role of rufinamide in pediatric LGS patients.
Literature Search
We reviewed the papers (English language only) on rufinamide treatment in children and adolescents with LGS through a Literature search on PubMed until September 2019. The terms “rufinamide” and “Lennox-Gastaut” were used in this systematic search. We included randomized controlled trials (RCTs), case reports, and open-label studies. Moreover, we searched for additional articles through review of the reference lists of published reviews. Overall, 23 papers were found eligible out of 333 search results (Table 1).
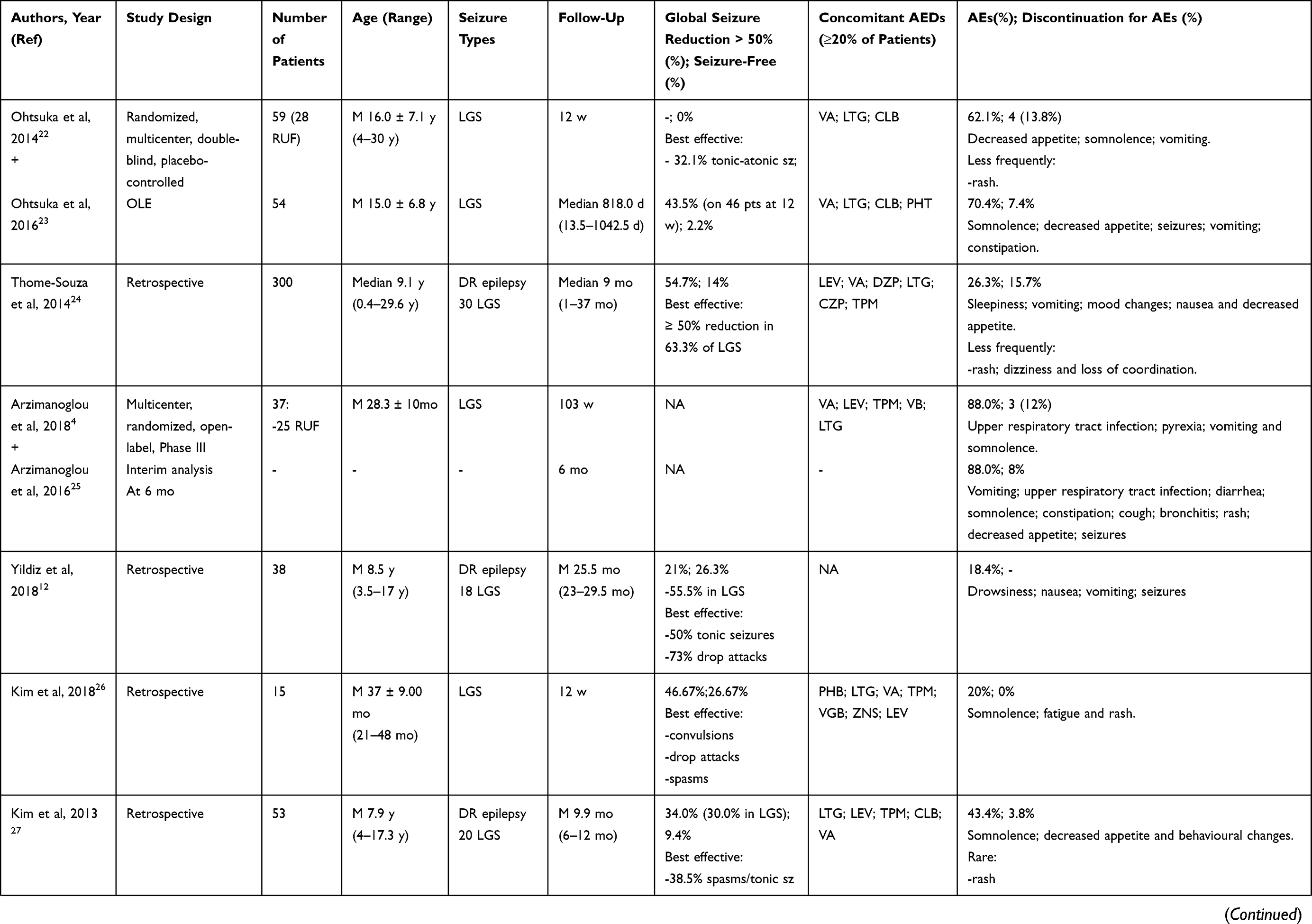 | 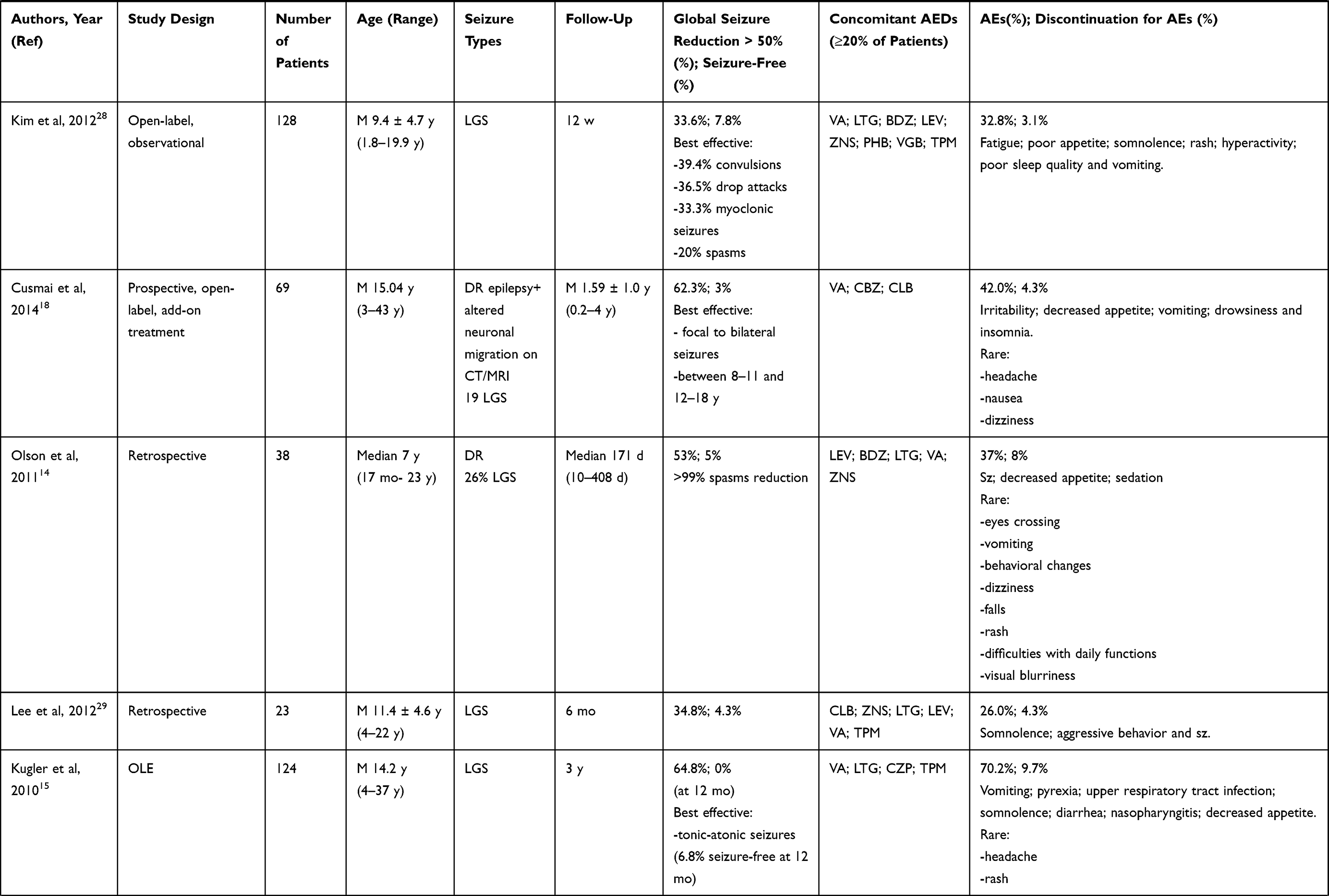 | 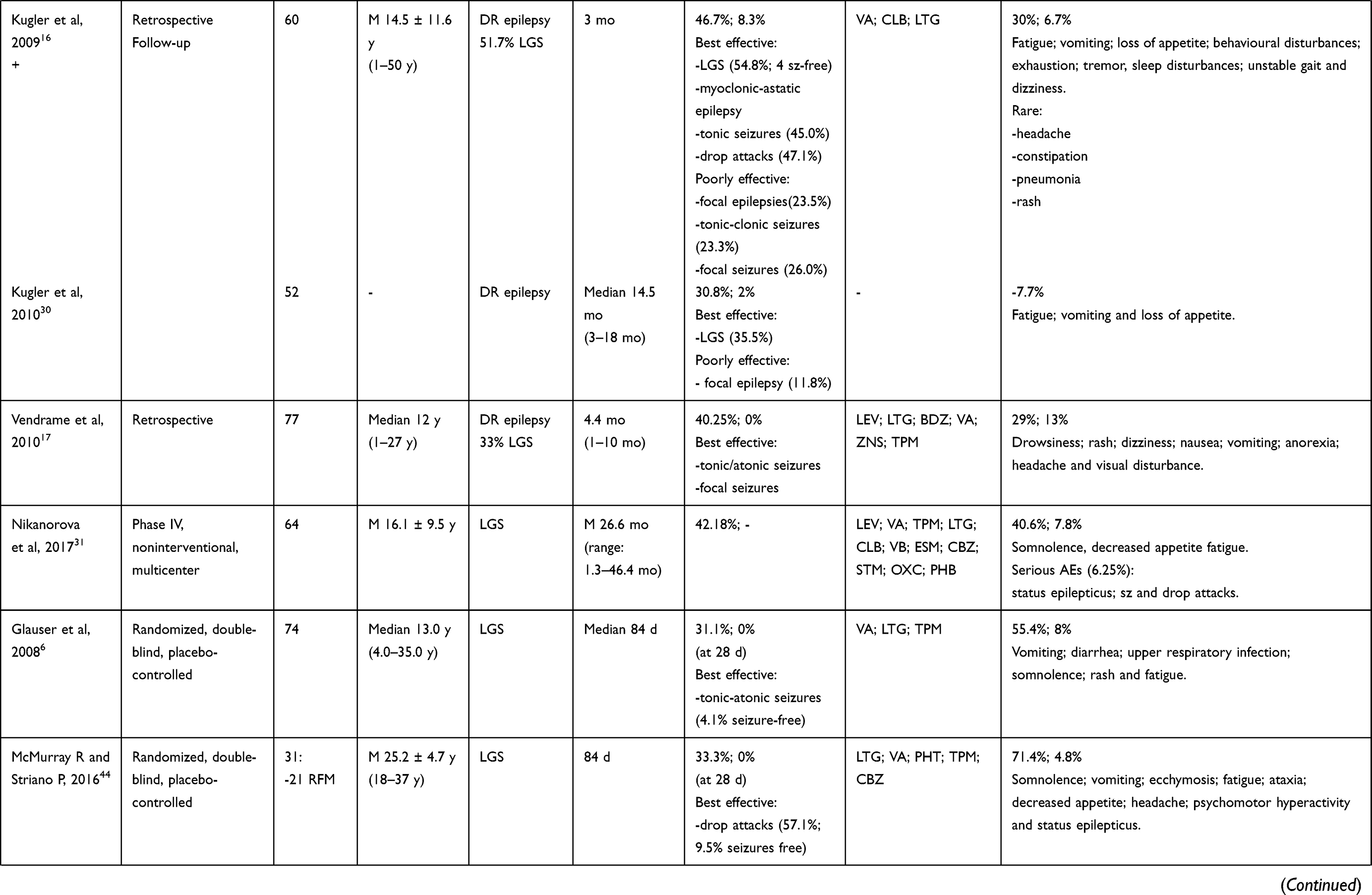 | 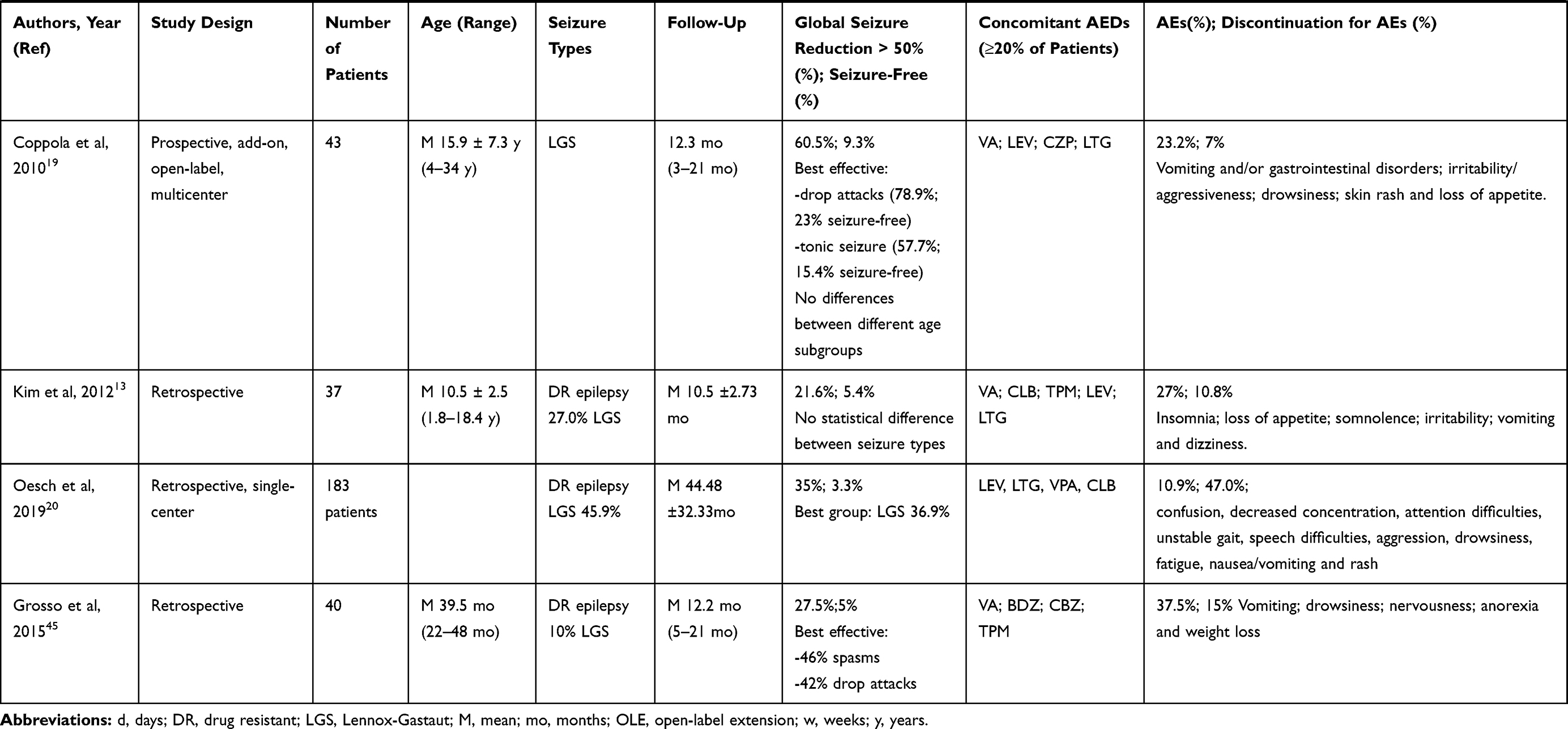 |
Table 1 Reviewed Clinical Studies for RUF Use in Pediatric Population |
Rufinamide: Pharmacodynamics and Pharmacokinetics
Rufinamide (1-[2,6-difluorobenzyl]-1H-1,2,3-triazole-4-carboxamide) was developed in the late 90s as a triazole derivative.5 However, it was designed only in 2017 as an orphan drug for adjunctive therapy in LGS in EU and US, following a large RCT.6
From in vitro and in vivo studies, RFN exhibits mechanisms of action unrelated to the other AEDs, mainly limiting sodium-dependent action potentials7 (Figure 1). At therapeutic range, RFN prolongs the inactivation phase, thus suppressing neuronal hyper-excitability; however, it was proved to directly inhibit the activation of Nav1.1 (encoded by SCN1A).8 At increased concentrations, RFN also inhibits the human recombinant metabotropic glutamate receptor subtype 5 (mGluR5).9 No effects are reported on benzodiazepine, adrenergic, tryptophan, histamine or cholinergic receptors.9
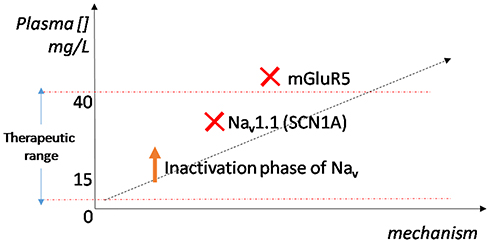 |
Figure 1 Putative mechanisms of action of rufinamide at increasing plasma concentrations. |
RFN is administered orally, with different starting and maximum recommended dosages based on patient’s age, weight and VPA co-medication. In children younger than 4 years, the drug should be started at 10 mg/kg/day, at the maximum dose of 45 mg/kg/day, or 30 mg/kg/day if combined with valproate. In patients older than 4 years, the starting dose is 200 mg per day, with the maximum dose depending on the weight (more or less than 30 kg) and the VPA intake.10
Rufinamide shows a non-linear pharmacokinetics and its oral bioavailability is 85% at lower doses.11 The absorption is not directly proportional to the dosage; however, food intake increases bioavailability and peak plasma concentrations, which are reached within 6 hrs.10
About 30% of plasma RFN binds to human serum proteins, almost entirely to albumin,10,11 minimizing the risk of displacement of other protein-bound compounds. The therapeutic mean plasma concentration of RFN is estimated 15–30 mg/L.9 Half-life is between 6 and 10 hrs. Main metabolic pathways in the liver are hydrolysis of the carboxylamide group and oxidative cleavage at the benzylic carbon atom,11 without the involvement of cytochrome P450.10 The greatest part of the metabolites (inactive) are excreted in urines.
RFN pharmacokinetics is not influenced by sex, renal impairment, or old age; however, children exhibit a lower clearance compared to adults and, in children 1–4 years the dosage must be calculated as mg/kg/day.9,10
RFN has no inhibitory activity on cytochrome P450 enzymes, but shows a modest induction of CYP3A4, which may decrease the levels of its pharmacological substrates. In the retrospective population pharmacokinetic analysis of pooled data from Phase II/III placebo-controlled studies, RFN have been shown to increase around 15% the clearance of carbamazepine (CBZ), LTG, phenytoin (PHT), and phenobarbital (PB), especially in children.9 Other medications should also be considered, e.g. oral contraceptives, olanzapine.10 Therefore, therapeutic drug monitoring should be performed on the concomitant medications, especially in case of a narrow therapeutic index.
On the other hand, RFN levels are not modified by concomitant LTG, TPM, and benzodiazepines, while CBZ, PHT, PB, vigabatrin, and primidone reduce by 25–46% the RFN plasma concentrations, particularly in children.9
VPA increases RFN plasma concentrations at an extent that can reach 70% in children, probably due to inhibition of the metabolizing enzymes: a careful dosage adjustment is needed in case of young children, weighting less than 30 kg, and the maximum dose cannot exceed 30 mg/kg/day.10 RFN is characterized by an overall favorable interaction profile compared with the older AEDs.
Profile of Rufinamide in Children with LGS
Results of the literature search are summarized in Table 1.
Efficacy Data
Rufinamide has proven to be particularly effective in LGS when compared with other syndromes and unspecified drug-resistant epilepsies, with seizure reduction rates (<50%) ranging from 26% to 65% among all the studies.4,6,12–31 In particular, LGS takes the best advantage from RFN than Dravet Syndrome does,12,32 which may be explained by the RFN’s inhibitory action on voltage-gated sodium channels.33
All but one13 reviewed studies show a meaningful difference in terms of efficacy in different seizure types subgroups. Drop-attacks, spasms, and tonic seizures show the highest response rates reaching 73%, 99% and 50% reduction.12,14 On the other hand, focal seizures have a much more “fluctuating” response showing only a 26.0% reduction in two studies;15,16 whereas in another17 the response to RFN is good (46.7% of patients with >50% response rate). However, many of the seizure types mentioned may have an unrecognized focal onset, and the studies do not always clarify the semiology (motor vs non-motor) of the “focal” seizures analyzed. Therefore, the efficacy data per seizure type must be taken cautiously. In summary, RFN has an overall excellent effect on seizures that may potentially lead to a fall, having a great benefit on the morbidity of the patients.
We evaluated whether there is a correlation between the efficacy of RFN and the patients’ age range. In fact, a prospective, open-label, add-on treatment study18 reported rufinamide to be best effective in patients aged 8–11 and 12–18 years. Whereas no statistical difference between age subgroups is found in another prospective, add-on, open-label, multicenter study.19 This may be due to the different initial characteristics of patients included in the studies: DR epilepsies with altered neuronal migration on CT/MRI (comprising 19 LGS) and only LGS.
Most of the clinical studies evaluating RFN in LGS rely on “drop seizures” frequency to evaluate the efficacy, as these are easily countable and less prone to misinterpretation by the caregivers. However, LGS is characterized by many different seizure types, which still influence the patient’s quality of life and developmental potential. In the effort to better assess the total seizure burden in LGS, other endpoints have also been developed and used to evaluate the therapy impact. In a post hoc analysis,34 the quality of life (QoL) endpoint was introduced, evaluating seizure-free days in rufinamide vs. placebo. Patients treated with adjunctive RFN reported a mean number of seizure-free days 42.2% greater than in placebo group. This important endpoint can assess the actual impact of a medication on the everyday life of patients and caregivers, in terms of days that can be proficiently spent for social, cognitive and motor development.
LGS has a heterogeneous range of etiologies. Studies correlating the etiology and the AEDs response in LGS are lacking. An attempt was made by a study which recruited a more or less homogeneous population with disorders of neuronal migration, and obtained a response rate of 62.3%; however, rufinamide response was not significantly different in focal vs. bilateral diffuse neuronal migration disorder.18
A large retrospective study20 analyzed possible correlations in patients with drug-resistant epilepsies, 45% with LGS. Patients with LGS, a history of encephalopathy or tonic/atonic seizures reached the best seizure reduction in the group (seizure reduction >50% in 36.9%). The study did not identify any significant correlation between the etiology type and outcome. However, patients with structural malformation of cortical development achieved a 40% in response rate; patients carrying mutations in DEPDC5, KCNQ2, MMACHC, SPATA5 genes achieved >90% of seizure reduction; one patient with SCN8A and 2 with focal cortical dysplasia were seizure-free. On the other hand, the patient with Dravet syndrome experienced a worsening of seizures.20 More studies are needed to clarify whether some etiologies may have a better response to RFN than others, in the wake of an individualized approach to therapy.
Treatment-Related Adverse Events
The majority of available studies evaluated rufinamide efficacy in a period <3 years. The discontinuation rate in both retrospective and prospective studies is up to 15%, and is due to worsening seizures or severe but rare adverse events (AEs). However, the short and variable follow-up period among the reviewed studies constitute a bias.
The common reported AEs were vomiting, decreased appetite, somnolence, upper respiratory tract infections, mood changes, followed by constipation, diarrhea, seizures, drowsiness. Rash, headache and loss of coordination were reported as overall rare. In a recent Cochrane review of six randomised, double-blind, placebo-controlled trials the adverse events significantly associated with rufinamide were: headache, dizziness, somnolence, vomiting, nausea, fatigue and diplopia.35 After post-marketing analyses, we have a more comprehensive view of the side effects and their epidemiology, as reported in Table 2, however real-world data are still lacking.
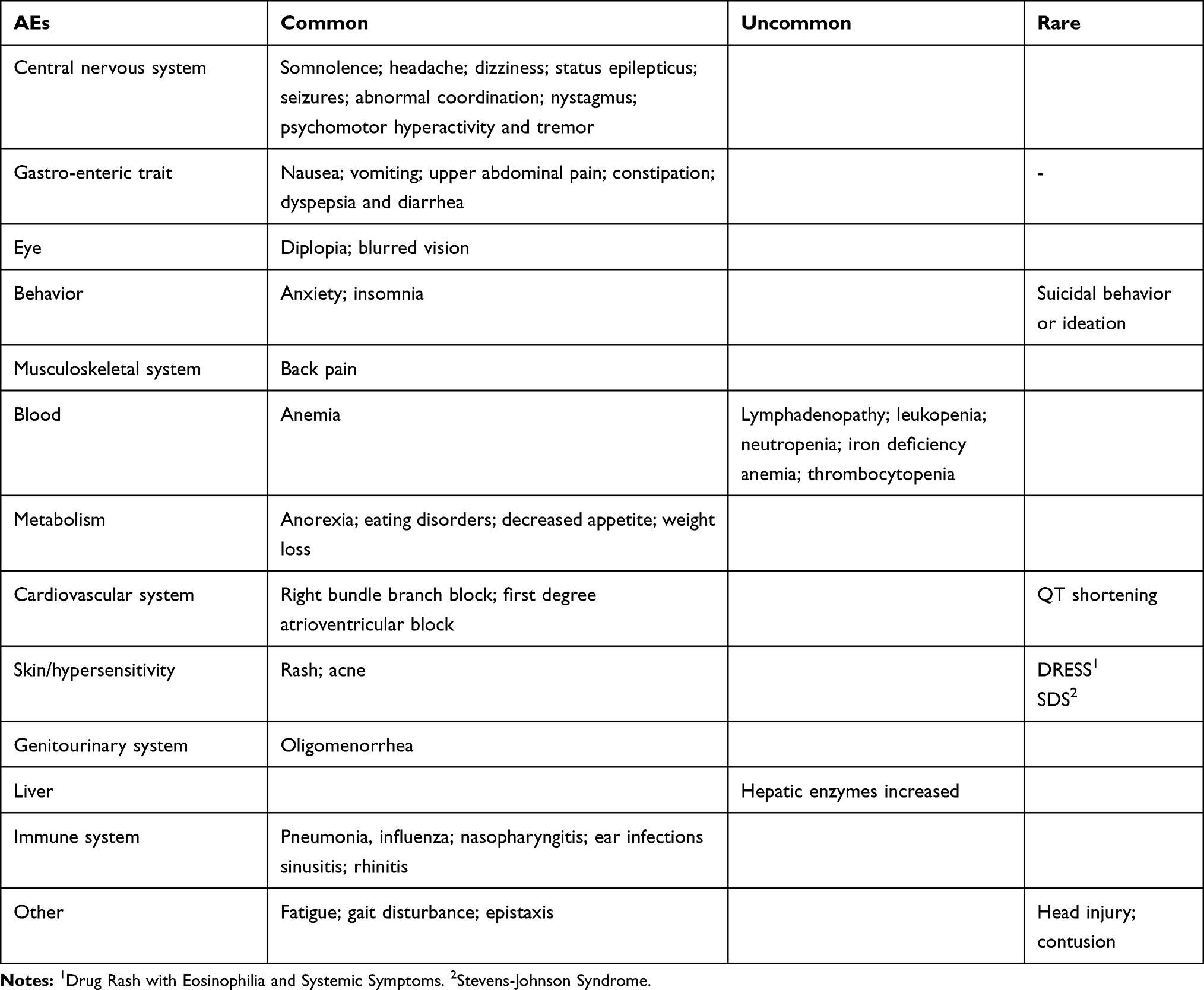 |
Table 2 Overview of the Reported Adverse Events in Rufinamide Treatment |
The side effects concerning the digestive system, e.g. vomit and decreased appetite, are usually mild and does not lead to discontinuation. Weight loss is also commonly reported; however, in adults and adolescents, this side effect seems to be linked with a longest exposure to RFN.
The rash associated with RFN is usually mild, and only anecdotic cases have been reported with drug rash with eosinophilia and systemic symptoms (DRESS) syndrome36 and Stevens-Johnson Syndrome (SJS)37 associated to RFN treatment. Aromatic anticonvulsants are especially linked to anticonvulsant hypersensitivity syndrome (AHS), a potentially life-threatening condition, and there is a high degree of cross-reactivity among all these agents.38 RFN structure includes an aromatic ring; thus, it cannot be excluded that it can precipitate a serious reaction in a patient with anamnesis of AHS; therefore, patients with an history of AHS should avoid RUF, and skin rashes in RFN treatment should be appropriately investigated.
RFN has the ability to significantly shorten QT-intervals. While drug-induced QT-interval prolongation is a known-risk factor for ventricular arrhythmias, the pro-arrhythmic effect of shortening is uncertain; however, a cardiologic follow-up is recommended in the patients on long-term rufinamide treatment.39
From a meta-analysis of five randomized-controlled trials,40 it seems that AEs associated with RFN are dose-independent. Given the non-linear pharmacokinetics of RUF, therapeutic drug monitoring should be performed to assess the optimum range balancing efficacy and adverse events individually.
Comedications
We reported the co-medications taken by ≥20% of patients in each study reviewed (Table 1). VPA resulted the most used AED across all reviewed studies, followed by benzodiazepines, LTG, TPM and LEV. There is no specific combination of AEDs that seem to be more effective in children with LGS when RFN is co-administered. Studies evaluating the response of combination therapy per seizure types and underlying etiology would be useful.
Recently, two new AEDs are under spotlight for the treatment of LGS: highly purified pharmaceutical grade cannabidiol (hpCBD) and fenfluramine (FFA). hpCBD has already been approved by FDA and EMA as adjunctive therapy in LGS;41 FFA proved to be effective in LGS in an open-label study42 and a randomized placebo-controlled trial is currently ongoing.43 hpCBD have been proved to slightly increase the serum levels of RFN at progressive doses,21 therefore, this effect should be considered when prescribing the two drugs, especially if CLB or VPA are co-administered. FFA has been administered in patients taking RUF; however, there are no data about pharmacokinetic or pharmacodynamic interactions.42
Conclusions
LGS is clinical condition with many different underlying etiologies, ranging from genetic causes to structural, infective, and unknown causes. Various co-morbidities are associated, from cognitive to motor impairment. The available therapies are mainly symptomatic, aimed at controlling seizures and psychiatric co-morbidities, and do not impact significantly on the natural history of the disease. Nevertheless, seizure control represents a major challenge, and an effective control can favorably impact on the quality of life. Most of the available AEDs are applied in co-treatment in LGS, and novel drugs are re-directed towards LGS, Rufinamide being one of the latest. Both in randomized controlled trials and open-label studies, Rufinamide have proven to be particularly effective in reducing tonic-atonic seizures, and broadly, seizures associated with falls in LGS. RFN shows an overall very favorable profile of safety and tolerability, with mostly mild side effects, and a good interaction profile with other AEDs. These features have gained RFN a place in the recommended second-line adjunctive AEDs in LGS. However, pediatric population carries several peculiarities in terms of pharmacokinetics and response to therapy compared to adults. Therapeutic drug monitoring is recommended when initiating RFN therapy, taking into account a non-linear pharmacokinetics and the individual differences, in order to identify the efficacious and tolerable range for this promising drug. Future studies will clarify the place of RFN alongside the newest emerging AEDs in terms of timing of administration and co-medications.
The variability of etiologies in LGS is a challenge to evaluate the treatment efficacy in this syndrome. Therefore, further larger studies are needed to assess a correlation between etiology and drug response, in order to address a more precise and personalized approach to therapy and maximize the developmental potential and quality of life of the patients.
Disclosure
P.S. has received speaker fees and participated at advisory boards for Biomarin, Zogenyx, and GW Pharmaceuticals, and has received research funding from ENECTA srl, GW Pharmaceuticals, Kolfarma srl., and Eisai. The authors report no other conflicts of interest in this work.
References
1. Aicardi J, Levy Gomes A. Clinical and electroencephalographic symptomatology of the ‘genuine’ lennox-gastaut syndrome and its differentiation from other forms of epilepsy of early childhood. Epilepsy Res Suppl. 1992;6:185–193.
2. Berg AT, Berkovic SF, Brodie MJ, et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE commission on classification and terminology, 2005–2009. Epilepsia. 2010;51:676–685. doi:10.1111/j.1528-1167.2010.02522.x
3. Asadi-Pooya AA. Lennox-gastaut syndrome: a comprehensive review. Neurol Sci. 2018;39:403. doi:10.1007/s10072-017-3188-y
4. Arzimanoglou A, Ferreira J, Satlin A, et al. Evaluation of long-term safety, tolerability, and behavioral outcomes with adjunctive rufinamide in pediatric patients (≥1 to <4 years old) with lennox-gastaut syndrome: final results from randomized study 303. Eur J Paediatr Neurol. 2019;23(1):126–135. doi:10.1016/j.ejpn.2018.09.010
5. Cheung WK, Kianifard F, Wong A, et al. Intra- and inter-subject variabilities of CGP 33101 after replicate single oral doses of two 200-mg tablets and 400-mg suspension. Pharm Res. 1995;12(12):1878–1882. doi:10.1023/A:1016275402723
6. Glauser T, Kluger G, Sachdeo R, Krauss G, Perdomo C, Arroyo S. Rufinamide for generalized seizures associated with lennox-gastaut syndrome. Neurology. 2008;70(21):1950–1958. doi:10.1212/01.wnl.0000303813.95800.0d
7. White HS, Franklin MR, Kupferberg HJ, Schmutz M, Stables JP, Wolf HH. The anticonvulsant profile of rufinamide (CGP 33101) in rodent seizure models. Epilepsia. 2008;49(7):1213–1220. doi:10.1111/j.1528-1167.2008.01552.x
8. Gilchrist J, Dutton S, Diaz-Bustamante M. Nav1.1 modulation by a novel triazole compound attenuates epileptic seizures in rodents. ACS Chem Biol. 2014;9:1204–1212. doi:10.1021/cb500108p
9. Perucca E, Cloyd J, Critchley D, Fuseau E. Rufinamide: clinical pharmacokinetics and concentration-response relationships in patients with epilepsy. Epilepsia. 2008;49:1123–1141. doi:10.1111/epi.2008.49.issue-7
10. Stephen JL, Brodie MJ. Pharmacotherapy of epilepsy: newly approved and developmental agents. CNS Drugs. 2011;25(2):89–107. doi:10.2165/11584860-000000000-00000
11. Inovelon® Summary of Product Characteristics. 2019.
12. Yıldız EP, Hızlı Z, Bektaş G, et al. Efficacy of rufinamide in childhood refractory epilepsy. Turk J Pediatr. 2018;60(3):238–243. doi:10.24953/turkjped.2018.03.002
13. Kim JY, Lee CG, Yu HJ, Nam SH, Lee J, Lee M. The efficacy and tolerability of rufinamide in intractable pediatric epilepsy. J Epilepsy Res. 2012;2(2):33–37. doi:10.14581/jer.12009
14. Olson HE, Loddenkemper T, Vendrame M, et al. Rufinamide for the treatment of epileptic spasms. Epilepsy Behav. 2011;20(2):344–348. doi:10.1016/j.yebeh.2010.11.023
15. Kluger G, Glauser T, Krauss G, Seeruthun R, Perdomo C, Arroyo S. Adjunctive rufinamide in lennox-gastaut syndrome: a long-term, open-label extension study. Acta Neurol Scand. 2010;122(3):202–208. doi:10.1111/j.1600-0404.2010.01334.x
16. Kluger G, Kurlemann G, Haberlandt E, et al. Effectiveness and tolerability of rufinamide in children and adults with refractory epilepsy: first European experience. Epilepsy Behav. 2009;14(3):491–495. doi:10.1016/j.yebeh.2008.12.013
17. Vendrame M, Loddenkemper T, Gooty VD, et al. Experience with rufinamide in a pediatric population: a single center’s experience. Pediatr Neurol. 2010;43(3):155–158. doi:10.1016/j.pediatrneurol.2010.04.003
18. Cusmai R, Verrotti A, Moavero R, et al. Rufinamide for the treatment of refractory epilepsy secondary to neuronal migration disorders. Epilepsy Res. 2014;108(3):542–546. doi:10.1016/j.eplepsyres.2014.01.013
19. Coppola G, Grosso S, Franzoni E, et al. Rufinamide in children and adults with lennox-gastautsyndrome: first Italianmulticenterexperience. Seizure. 2010;19(9):587–591. doi:10.1016/j.seizure.2010.09.008
20. Gabriela O, Bozarth XL. Rufinamide efficacy and association with phenotype and genotype in children with intractable epilepsy: a retrospective single center study. Epilepsy Res. 2019;106211. doi:10.1016/j.eplepsyres.2019.106211
21. Gaston TE, Bebin EM, Cutter GR, Liu Y, Szaflarski JP. Interactions between cannabidiol and commonly used antiepileptic drugs. Epilepsia. 2017;58:1586–1592. doi:10.1111/epi.13852
22. Ohtsuka Y, Yoshinaga H, Shirasaka Y, Takayama R, Takano H, Iyoda K. Rufinamide as an adjunctive therapy for lennox-gastaut syndrome: a randomized double-blind placebo-controlled trial in Japan. Epilepsy Res. 2014;108(9):1627–1636. doi:10.1016/j.eplepsyres.2014.08.019
23. Ohtsuka Y, Yoshinaga H, Shirasaka Y, Takayama R, Takano H, Iyoda K. Long-term safety and seizure outcome in Japanese patients with lennox-gastaut syndrome receiving adjunctive rufinamide therapy: an open-label study following a randomized clinical trial. Epilepsy Res. 2016;121:1–7. doi:10.1016/j.eplepsyres.2016.01.002
24. Thome-Souza S, Kadish NE, Ramgopal S, et al. Safety and retention rate of rufinamide in 300 patients: a single pediatric epilepsy center experience. Epilepsia. 2014;55(8):1235–1244. doi:10.1111/epi.12689
25. Arzimanoglou A, Ferreira JA, Satlin A, et al. Safety and pharmacokinetic profile of rufinamide in pediatric patients aged less than 4 years with lennox-gastaut syndrome: an interim analysis from a multicenter, randomized, active-controlled, open-label study. Eur J Paediatr Neurol. 2016;20(3):393–402. doi:10.1016/j.ejpn.2015.12.015
26. Kim SH, Kang HC, Lee JS, Kim HD. Rufinamide efficacy and safety in children aged 1–4 years with lennox-gastaut syndrome. Brain Dev. 2018;40(10):897–903. doi:10.1016/j.braindev.2018.07.020
27. Kim SH, Lee JH, Ryu HW, et al. Short-term efficacy and tolerability of rufinamide adjunctive therapy in children with refractory generalized epilepsy. Epileptic Disord. 2013;15(1):49–54. doi:10.1684/epd.2013.0557
28. Kim SH, Eun SH, Kang HC, et al. Rufinamide as an adjuvant treatment in children with lennox-gastautsyndrome. Seizure. 2012;21(4):288–291. doi:10.1016/j.seizure.2012.02.006
29. Lee EH, Yum MS, Ko TS. Effectiveness and tolerability of rufinamide in children and young adults with lennox-gastaut syndrome: a single center study in Korea. Clin Neurol Neurosurg. 2013;115(7):926–929. doi:10.1016/j.clineuro.2012.09.021
30. Kluger G, Haberlandt E, Kurlemann G, et al. First European long-term experience with the orphan drug rufinamide in childhood-onset refractory epilepsy. Epilepsy Behav. 2010;17(4):546–548. doi:10.1016/j.yebeh.2010.01.005
31. Nikanorova M, Brandt C, Auvin S, McMurray R. Real-world data on rufinamidetreatment in patients with lennox-gastaut syndrome: results from a Europeannoninterventional registry study. Epilepsy Behav. 2017;76:63–70. doi:10.1016/j.yebeh.2017.08.026
32. Striano P, McMurray R, Santamarina E, Falip M. Rufinamide for the treatment of lennox-gastaut syndrome: evidence from clinical trials and clinical practice. Epileptic Disord. 2018;20(1):13–29. doi:10.1684/epd.2017.0950
33. Mueller A, Boor R, Coppola G, et al. Low long-term efficacy and tolerability of add-on rufinamide in patients with dravet syndrome. Epilepsy Behav. 2011;21(3):282–284. doi:10.1016/j.yebeh.2011.04.057
34. Auvin S, Williams B, McMurray R, Kumar D, Perdomo C, Malhotra M. Novel seizure outcomes in patients with lennox‐gastaut syndrome: post hoc analysis of seizure‐free days in rufinamide study 303. Epilepsia Open. 2019;4:275–280. doi:10.1002/epi4.12314
35. Panebianco M
36. Shahbaz S, Sivamani RK, Konia T, Burrall B. A case of Drug Rash with Eosinophilia and Systemic Symptoms (DRESS) related to rufinamide. Dermatol Online J. 2013;19(4):4.
37. Chambel M, Mascarenhas MI, Regala J, Gouveia C, Prates S. Clinical Stevens-Johnson syndrome and rufinamide: a clinical case. Allergol Immunopathol (Madr). 2013;41(1):68–69. doi:10.1016/j.aller.2011.12.004
38. Knowles SR, Dewhurst N, Shear NH. Anticonvulsant hypersensitivity syndrome: an update. Expert Opin Drug Saf. 2012;11(5):767–778. doi:10.1517/14740338.2012.705828
39. Schimpf R, Veltmann C, Papavassiliu T, et al. Drug-induced QT-interval shortening following antiepileptic treatment with oral rufinamide. Heart Rhythm. 2012;9(5):776–781. doi:10.1016/j.hrthm.2012.01.006
40. Xu Z, Zhao H, Chen Z. The efficacy and safety of rufinamide in drug-resistant epilepsy: a meta-analysis of double-blind, randomized, placebo controlled trials. Epilepsy Res. 2016;120:104–110. doi:10.1016/j.eplepsyres.2016.01.001
41. Epidiolex. Summary of Product Characteristics. 2019.
42. Lagae L, Schoonjans AS, Gammaitoni AR, Galer BS, Ceulemans B. A pilot, open-label study of the effectiveness and tolerability of low-dose ZX008 (fenfluramine HCl) in lennox-gastaut syndrome. Epilepsia. 2018;59(10):1881–1888. doi:10.1111/epi.14540
43. A study to investigate the long-term safety of ZX008 (fenfluramine hydrochloride) oral solution in children and adults with epileptic encephalopathy including dravet syndrome and lennox-gastaut syndrome. ClinicalTrials.gov Identifier: NCT03936777.
44. McMurray R, Striano P. Treatment of adults with Lennox-Gastaut syndrome: further analysis of efficacy and safety/tolerability of rufinamide. Neurol Ther. 2016;5(1):35–43. doi:10.1007/s40120-016-0041-9
45. Grosso S, Coppola G, Dontin SD, et al. Efficacy and safety of rufinamide in children under four years of age with drug-resistant epilepsies. Eur J Paediatr Neurol. 2014;18(5):641–645. doi:10.1016/j.ejpn.2014.05.001
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.