Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Adiponectin Paradox More Evident in Non-Obese Than in Obese Patients with Diabetic Microvascular Complications
Authors Satoh K, Nagasawa K, Takebe N ![]() , Kinno H, Shozushima M, Onodera K, Oda T
, Kinno H, Shozushima M, Onodera K, Oda T ![]() , Hasegawa Y, Satoh J, Ishigaki Y
, Hasegawa Y, Satoh J, Ishigaki Y
Received 2 September 2022
Accepted for publication 11 January 2023
Published 23 January 2023 Volume 2023:16 Pages 201—212
DOI https://doi.org/10.2147/DMSO.S387744
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Ken Satoh,1 Kan Nagasawa,1 Noriko Takebe,1 Hirofumi Kinno,1 Masaharu Shozushima,1 Ken Onodera,1 Tomoyasu Oda,1 Yutaka Hasegawa,1 Jo Satoh,2 Yasushi Ishigaki1
1Division of Diabetes, Metabolism and Endocrinology, Department of Internal Medicine, Iwate Medical University, Yahaba, Japan; 2Department of Diabetes, Tohoku Medical and Pharmaceutical University, Wakabayashi Hospital, Sendai, Japan
Correspondence: Yasushi Ishigaki, Division of Diabetes, Metabolism and Endocrinology, Department of Internal Medicine, Iwate Medical University, 2-1-1 Idai-Dori, Yahaba, Iwate, 028-3695, Japan, Tel +81 19 613 7111, Fax +81 19 907 8270, Email [email protected]
Aims/Introduction: Adiponectin is generally regarded as a beneficial molecule, protecting against insulin resistance and atherosclerosis, and its serum levels are low in individuals with obesity as well as in those with type 2 diabetes (T2DM). However, several clinical studies have shown associations between high adiponectin values and major health concerns. These conflicting findings are termed the “adiponectin paradox”. Similarly, these paradoxical adiponectin elevations were observed in patients with diabetic microvascular complications. This cross-sectional study aimed to identify differences in factors, including adiponectin, related to diabetic vascular complications between non-obese and obese patients.
Materials and Methods: Study patients with T2DM were non-obese (n=197) or obese (n=197), matched by a propensity score model adjusted with age and gender. Independent factors for each of the microvascular complications were determined using multivariate logistic regression analyses.
Results: The prevalence of nephropathy was high in obese T2DM patients. In addition to long diabetes duration, elevated adiponectin was a common characteristic of patients with microvascular complications. Logistic regression analyses for microvascular complications revealed adiponectin to be highly related to retinopathy (odds ratio [OR], 1.138; 95%confidence intervals [CI], 1.004– 1.289, p< 0.001), nephropathy (OR, 1.192; CI, 1.077– 1.319, p< 0.001) and neuropathy (OR, 1.217; CI, 1.071– 1.384, p< 0.001), in non-obese patients. In contrast, the association between adiponectin values and complications was modest in obese patients.
Conclusion: Adiponectin regulation in response to vascular damage differed between non-obese and obese patients, suggesting that adiponectin regulation is compromised by fat accumulation. Assuming that paradoxical elevation of adiponectin in vascular damage is a compensatory response, we speculate that responsive upregulation might be insufficient in obese patients. These newly-recognized differences in adiponectin values might lead to novel insights into adiponectin regulation and our understanding of the adiponectin paradox.
Keywords: diabetic complications, obesity, adiponectin
Introduction
Chronic hyperglycemia induces vascular complications in individuals with diabetes mellitus, thereby limiting their abilities of daily life and life expectancy. The major diabetic microvascular complications, attributable to functional damage of capillary blood vessels, are retinopathy, nephropathy and neuropathy.1 The molecular mechanisms underlying these forms of vascular damage are considered to mainly be chronic exacerbation of oxidative stress derived from increased activity of the polyol pathway, excessive activation of protein kinase C and accumulation of advanced glycation end-products.1 Several risk factors, mainly chronic hyperglycemia and diabetes duration2 as well as obesity,3 have been reported to promote diabetic microvascular complications.
As indicated by epidemiological studies, obesity exacerbates a wide range of metabolic disorders, including type 2 diabetes mellitus (T2DM), resulting in the progression of vascular complications.4 Additionally, adiposity is attributed to chronic inflammation5 which induces endothelial dysfunction6 and blood coagulation disorders which exert a suppressive effect on the microcirculation.7 However, the impacts of adipose accumulation on diabetic microvascular complications remain controversial. Several clinical reports have shown progression of chronic kidney disease, including diabetic nephropathy, to be significantly associated with a high body mass index (BMI).8 Prior studies have, however, obtained controversial results regarding the positive and negative impacts of obesity on diabetic retinopathy.9,10 Similarly, the relationship between obesity and diabetic neuropathy has yet to be fully clarified.11,12 In addition to determining the relevance of obesity to microvascular complications, it is important to identify obesity-related factors involved in the development of diabetic microangiopathy.
Several lines of evidence point to adipocytokines having pathophysiologic roles in disorders related to obesity.13 Adiponectin, a major adipocytokine with anti-atherogenic as well as anti-diabetic properties, is abundant in the circulation.14 Numerous experimental studies have demonstrated the beneficial properties of adiponectin as regards energy metabolism,14 inflammation15 and cell proliferation, which appear to protect against insulin resistance and/or atherosclerosis.16 In line with the observations made in various in vitro and in vivo studies, serum adiponectin levels are reportedly low in obese individuals and patients with T2DM.17 However, several clinical studies have identified associations between high circulating adiponectin levels and major health concerns.18 Similarly, these paradoxical elevations of adiponectin were observed in patients with the major diabetic microvascular complications, ie, retinopathy,19,20 nephropathy19 and neuropathy.21 Both the mechanisms and the related clinical characteristics underlying these adiponectin elevations in patients with diabetic complications have yet to be clarified.
We aimed to elucidate the contributions of obesity as well as obesity-related factors to diabetic vascular complications. T2DM patients with BMI exceeding 32 kg/m2 were enrolled as the study group with obesity, while patients with a BMI in the 20 kg/m2 to 25 kg/m2 range served as a non-obese group. We compared factors possibly influencing diabetic microvascular complications, including adipocytokine levels and abdominal fat distributions, between the non-obese and obese patients with T2DM.
Materials and Methods
Study Patients
The patients enrolled in this cross-sectional study were recruited from those with T2DM admitted to Iwate Medical University Hospital during the period from January 2005 to May 2020. Enrolled patients were excluded if they had any malignancy, emergent infectious diseases or a hyperglycemic crisis, such as diabetic ketoacidosis or hyperosmolar hyperglycemic state. All enrolled patients were 20 to 75 years of age. In total, 4237 patients were informed by an opt-out consent form via the internet and intranet at our hospital. This protocol, entitled “The retrospective study of evaluating the clinical course and complications in the patients with obesity”, received its ethics approval from the Institutional Review Board of Iwate Medical University (Approval number: MH2018-543). Considering that the clinical information was retrospectively collected in routine practice for patients with T2DM, the Ethics Committee approved that no informed consent was required.
We retrospectively identified 283 patients as “obese”, ie, BMI over 32 kg/m2. While BMI over 25 kg/m2 has been a fixed criterion for obesity according to the Japan Society for the Study of Obesity and is the accepted Asian-specific cut-off value for the World Health Organization report,22 a high cut-off value was used herein for recruitment of Japanese patients with morbid obesity, with the overall aim of obtaining a marked obesity phenotype in comparison with non-obese patients. In order to minimize selection bias, a propensity score (PS) matching analysis was applied to select “non-obese” patients whose BMI ranged from 20 kg/m2 to 25 kg/m2. The predictors matched in the PS model included age and gender. PS matching uses a nearest-neighbor algorithm to match the obese group with the non-obese group, at a 1:1 ratio, in the final dataset. For matching, the logit of the PS was used, with a caliper distance of less than 0.1 standard deviations.23 Subsequent to the PS matching analysis, 197 obese patients were matched with 197 non-obese patients.
The study was conducted in accordance with guidelines established by the Declaration of Helsinki.
Clinical and Biochemical Measurements
We obtained standard anthropometric measurements, including weight, height and blood pressure, for all patients. Blood and urine were collected for hematologic, biochemical, and endocrinologic investigations in the morning after a 12-hour overnight fast. The measured parameters and measurement methods were as follows; low density lipoprotein cholesterol (LDL-C); using a direct assay method (Sekisui Medical Co., Tokyo, Japan), serum concentrations of C-peptide (S-CPR); chemiluminescent Enzyme Immunoassay, high molecular weight adiponectin; a latex particle-enhanced turbidimetric assay system, leptin; enzyme-linked immunosorbent assay (SRL, Inc. Tokyo, Japan).
Criteria for Defining Comorbidity and Diabetic Complications
Hypertension was defined as systolic blood pressure (BP) ≥ 140mmHg and/or diastolic BP ≥ 90mmHg and/or taking antihypertensive medication. Dyslipidemia was defined as LDL-C ≥ 140mg/dL and/or triglycerides (TG) ≥ 150mg/dL and/or high-density lipoprotein cholesterol (HDL-C) < 40mg/dL and/or taking antihyperlipidemic medication.
Diabetic retinopathy was diagnosed by ophthalmologists, based on the international clinical diabetic retinopathy scales.24 Diabetic nephropathy was defined as urine albumin excretion (UAE) ≥ 30 mg/g creatinine.25 Diabetic neuropathy was defined as the presence of two of the following three findings, ie, typical subjective symptoms of symmetrical distal neuropathy, bilaterally decreased Achilles tendon reflexes or an inability to sense vibration.25
Measurements of baPWV, Carotid Artery IMT and Abdominal CT
The brachial ankle pulse wave velocity (baPWV) was measured using an automatic waveform analyzer (BP-203RPE; Colin Co., Komaki, Japan). The intima-media thickness (IMT) of the carotid arteries was measured using ultrasound diagnostic equipment (LOGIQ 500, GE Yokogawa Medical Systems Corp., Hino, Tokyo, Japan) and the max IMT, the thickest portion detected in the scanned regions, was determined as described in our previous publication.26 Volumes of both the visceral fat area (VFA) and the subcutaneous fat area (SFA) were analyzed using abdominal computed tomography (CT) images at the level of the umbilicus, based on criteria established by the Japan Society for the Study of Obesity.
Statistical Analysis
Continuous variables were expressed as medians (25th–75th percentile). Categorical variables were expressed as number and percentage. The two groups were compared using the chi-square test for categorical variables and the Mann–Whitney U-test for continuous variables. We employed multivariate logistic regressions to assess the associations of various potential factors with diabetic complications. Odds ratios (OR) and 95% confidence intervals (CI) were calculated to estimate the strength of associations between diabetic complications and clinical parameters. A p value <0.05 was regarded as indicating a statistically significant difference. Statistical analyses were performed using SPSS version 25 (SPSS Japan Inc., Tokyo, Japan).
Results
Diabetic Nephropathy Prevalence Was High in Obese T2DM Patients
The clinical characteristics of the enrolled patients, categorized as non-obese and obese, are summarized in Table 1. Based on PS matching, age and gender were similar in the two groups. The median BMI was 23.0 kg/m2 in the non-obese group and 35.1 kg/m2 in the obese group. Patients with obesity had significantly higher values for diabetes duration, hepatic enzymes including aspartate aminotransferase (AST), alanine aminotransferase (ALT) and gamma-glutamyl transferase (γ-GT), uric acid (UA), UAE, S-CPR, leptin and abdominal fat area, as reflected by both VFA and SFA. In contrast, the values for hemoglobin A1c (HbA1c), estimated glomerular filtration rate (eGFR) and adiponectin were significantly lower in the obese than in those in the non-obese patients. The chi-square test revealed significant differences for both hypertension and dyslipidemia. Collectively, the patients with obesity had metabolic disorder comorbidities more often than the non-obese patients. Diabetic retinopathy tended to be more severe in the non-obese. For example, 8 patients were diagnosed as having proliferative retinopathy in this group, while none of the obese group had this complication (data not shown). Conversely, the prevalence of diabetic nephropathy was higher in the obese group, as shown in Table 1. Unexpectedly, the subclinical atherosclerosis values were higher in the non-obese patients.
 |
Table 1 Characteristics of the Study Patients |
Long Diabetes Duration and High Adiponectin Levels Were Also Common in Patients with Diabetic Microvascular Complications
Aiming to clarify the differences in factors related to the prevalence of diabetic complications between non-obese and obese patients, we compared the presence or absence of each complication between the two groups. Common characteristics for having microvascular complications, ie, retinopathy (Table 2), nephropathy (Table 3) and neuropathy (Table 4), were long diabetes duration in both the non-obese and the obese group. As to diabetic retinopathy, related factors were quite similar in the two groups, eg, having hypertension, low values of hepatic enzyme, S-CPR and VFA values, and a high adiponectin level. These data indicated that patients with retinopathy tended to have mild insulin resistance and hepatic steatosis in both groups (Table 2). As to nephropathy, hyperuricemia and a high baPWV value were factors commonly related to the presence of nephropathy. In addition, having hypertension and high adiponectin were related to the presence of nephropathy only in the non-obese group (Table 3). In those with neuropathy, a low VFA value, as well as high adiponectin and PWV values, were factors related to the presence of neuropathy only in the non-obese group. On the other hand, advanced age, female gender, low ALT, S-CPR and eGFR values, and high leptin and max IMT values were found to be related to neuropathy in obese patients (Table 4).
 |
Table 2 Comparison of Factors Related to Diabetic Retinopathy Within Each Group |
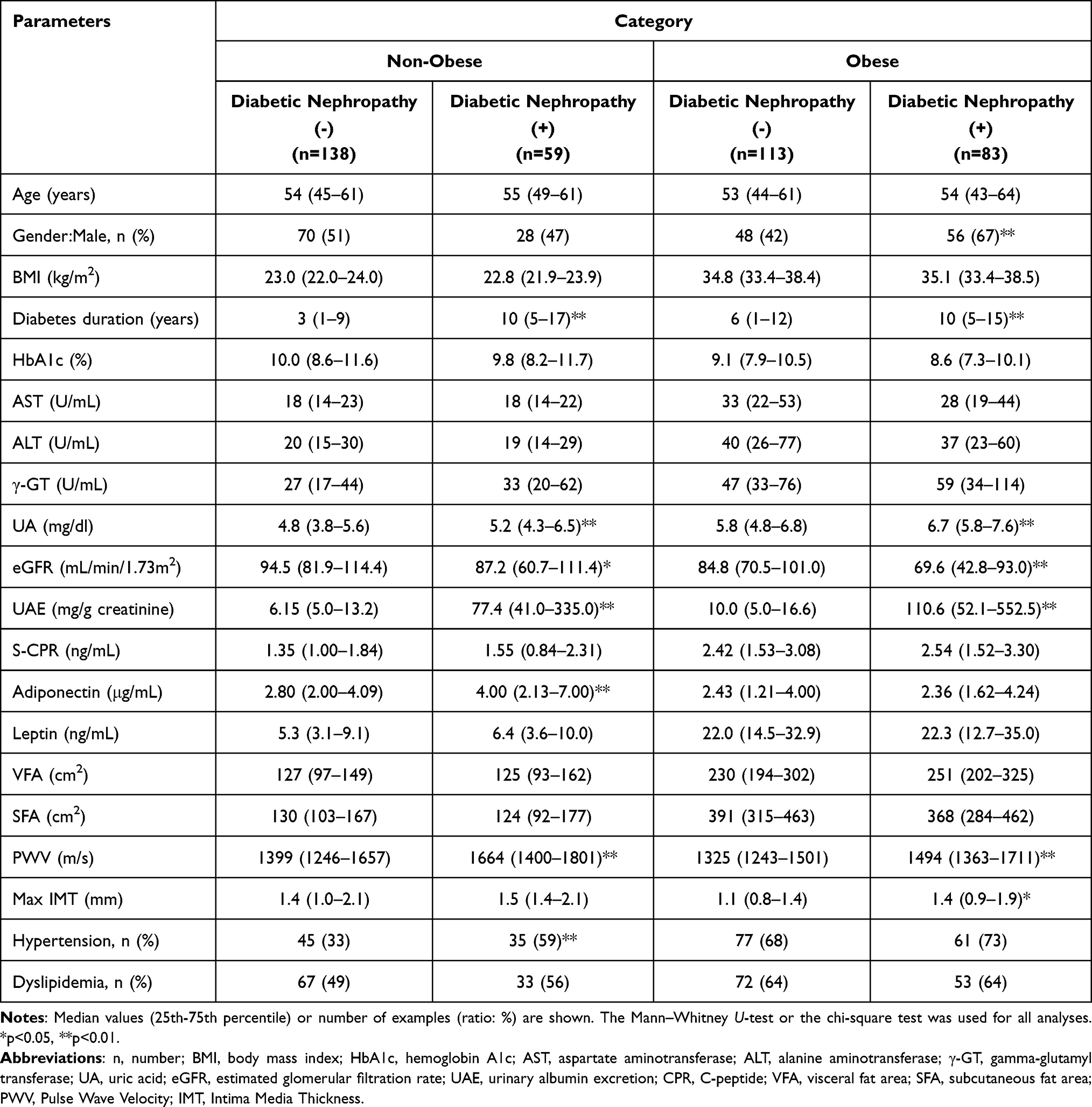 |
Table 3 Comparison of Factors Related to Diabetic Nephropathy Within Each Group |
 |
Table 4 Comparison of Factors Related to Diabetic Neuropathy Within Each Group |
Multiple Regression Analyses Revealed the Adiponectin Level to Be Highly Related to Microvascular Complications, Only in Non-Obese Patients
Multiple logistic regression analyses were performed to identify variables independently related to the presence of each the three major diabetic complications, with age, gender, diabetes duration, hypertension, dyslipidemia, and values of HbA1c, ALT, UA, eGFR and adiponectin as explanatory variables in the non-obese and obese groups (Table 5). Logistic analysis revealed diabetes duration to be independently associated with the presence of microvascular complications in both groups. It is noteworthy that adiponectin was revealed to be a variable independently related to retinopathy (OR, 1.138; 95% CI, 1.004–1.289, p<0.001), nephropathy (OR, 1.192; 95% CI, 1.077–1.319, p<0.001) and neuropathy (OR, 1.217; 95% CI, 1.071–1.384, p<0.001), but only in the non-obese group. In contrast, the relationships between microvascular complications and adiponectin values were found to be weaker on multivariate analyses in the obese group. Interestingly, the serum level of leptin, a major adipocytokine regulating energy metabolism as well as adiponectin, showed no association with diabetic microvascular complications.
 |
Table 5 Multivariate Logistic Regression Analysis for the Presence of Diabetic Vascular Complications Within the Non-Obese and Obese Groups |
Discussion
A major observation made in this study was the involvement of significantly elevated serum adiponectin in diabetic microvascular complications, in non-obese, but not in obese, diabetic patients. This finding highlights the difference in the adiponectin regulation in response to vascular damage between non-obese and obese patients, suggesting that the physiological impact of adiponectin in microvascular complications changes as body weight increases.
The relationships between obesity and diabetes complications remain controversial. In Asian females with T2DM, a higher waist-hip ratio was shown to be associated with the severity of retinopathy.10 Another meta-analysis of 27 studies showed that elevated BMI did not increase the risk of retinopathy.9 In our current study, 48% of non-obese patients, but 62% of those who were obese, had no signs of retinopathy, suggesting that patients with a high BMI tended to be less prone to the development of retinopathy. Several clinical studies have demonstrated a strong association between obesity and the development of diabetic nephropathy.3,8 As is well known, obesity itself leads to the progression of proteinuria and glomerulomegaly, ie, obesity-related glomerulopathy.27 Consistent with prior studies, the proportion of patients with preexisting albuminuria was significantly higher in obese than in non-obese patients in our present study. However, we were not able to clearly demonstrate relationships between obesity and diabetic neuropathy.
Adiponectin is widely recognized as an adipocytokine with beneficial effects on insulin resistance,17 inflammation15 and atherosclerosis, as demonstrated by numerous in vitro and in vivo analyses.14 However, large scale studies and meta-analyses have suggested associations between high adiponectin values and the incidence of future cardiovascular events.18,28 Likewise, an independent association of high adiponectin values has been observed with several disorders, such as coronary heart diseases,18 peripheral artery diseases,29 heart failure,30 chronic kidney disease and cancer.31 Furthermore, in the field of diabetes, strong correlations of adiponectin levels with diabetic vascular complications have been reported for both type 132 diabetes and T2DM.19,33 Similarly, our present study revealed increased adiponectin levels in patients with microvascular complications, in both the non-obese and the obese group. These conflicting findings, a beneficial impact on metabolic and vascular biology, while high serum concentrations are associated with diseases, is called the “adiponectin paradox”.18
As noted above, based on an abundance of basic research data, adiponectin is thought to play various beneficial roles in vascular biology. As to macrovascular complications, adiponectin deficient mice showed severe atherosclerosis and neointimal arterial injury, and adiponectin administration restored neointimal proliferation.34 In addition, peripheral arterial calcification was reported to be associated with serum adiponectin levels in patients with T2DM, and vascular adiponectin deposition was already observable at early stages of calcification.35 Regarding diabetic retinopathy, adiponectin deficient mice showed marked increases in retinal tumor necrosis factor (TNF)- α mRNA levels as compared to control mice, and administering adiponectin exerted a suppressive effect on pathological neovascularization.36 Additionally, adiponectin ameliorated hyperglycemia-induced dysfunction and angiogenesis in human retinal endothelial cells through mediating several pathways, including those of the high mobility group-B1 (HMGB1) or the p38 mitogen-activated protein family of kinases (MAPK), via upregulation of adiponectin receptor1 (AdipoR1) and AdipoR2.37 Recently, binding to T-cadherin was found to induce adiponectin accumulation in the neointima, contributing to protection from vascular damage.38 In addition, T-cadherin-dependent localization of adiponectin was identified in the retinal vascular endothelium of diabetic mice, suggesting it to play a role in preventing the development of diabetic retinopathy.39 Similarly, increased albuminuria in adiponectin deficient mice was reduced by adiponectin administration.40 In podocytes, adiponectin enhanced AMP-activated protein kinase (AMPK) through binding to AdipoR1, resulting in reduced oxidative stress and inflammation in the kidneys.41 As to peripheral nerves, activation of adiponectin signals induced AMPK through both AdipoR1 and AdipoR2, leading to increased cell viability of neurons under hyperglycemic conditions.42 Taken together, these observations indicate increased serum adiponectin concentrations to possibly be a compensatory mechanism involved in vascular injury repair processes.
A novel finding of this study is that adiponectin elevation was strongly associated with the presence of diabetic complications only in the non-obese, not in the obese, diabetic patients. In fact, these paradoxical increases in adiponectin were also observed in obese patients, but the increments were comparatively small. Moreover, the association between adiponectin values and diabetic complication development did not reach statistical significance according to multivariable logistic regression analyses, partly because of dysregulation of adiponectin expression in obese patients. Downregulation of adiponectin gene expression in enlarged adipocytes is a well-known finding.43 One of the mechanisms underlying low adiponectinemia in obese patients is considered that visceral fat accumulation raises the levels of inflammatory cytokines such as TNF-α44 and interleukin-6,45 which inhibit adiponectin transcription by suppressing gene promoters, such as peroxisome proliferator-activated receptor response element46 and CCAAT-enhanced-binding proteins.43 While the mechanisms underlying obesity-associated reductions in adiponectin have yet to be fully elucidated, augmentation of a negative regulatory mechanism might be involved in suppressed upregulation of adiponectin in response to diabetic microvascular damage in obese T2DM patients. Since suppressive mechanisms acting on adiponectin expression depending on visceral fat accumulation are common, the difference in adiponectin upregulation, which is a compensatory response to tissue injury repair processes, between non-obese and obese patients might be generalizable to other health concerns associated with the “adiponectin paradox”.
The expressions of adiponectin receptors, AdipoR1 and AdipoR2, are generally decreased in patients with T2DM and obesity.47 For example, AdipoR expression in skeletal muscle cells was downregulated with a five-fold increase in serum adiponectin levels in patients with heart failure.48 Attenuation of adiponectin signals, including the receptor-mediated pathway, might lead to an elevated serum adiponectin concentration. These responses aimed at maintaining adiponectin function may account for the concept of “adiponectin resistance”.49 While obese patients are also in a state of “adiponectin resistance”, downregulation of adiponectin gene expression with obesity might weaken this incremental response. In a previous report, T-cadherin deficiency was significantly associated with high circulating levels of adiponectin, due to an inability of adiponectin to bind to T-cadherin-expressing cells.50 In this context, high serum concentrations of adiponectin reflect its decreased accumulation in the injured organ or tissue such as vascular endothelial cells, possibly resulting in failure to benefit from the protective effects of adiponectin observed in patients with the so-called “adiponectin paradox”. Since basal levels of adiponectin are generally low in obese patients, T-cadherin mediated regulation of the serum adiponectin level would presumably be minimal.
This study has several limitations. First, because of the cross-sectional study design, our results do not rule out incidental associations. Thus, further prospective studies designed to elucidate serial changes in adiponectin values in both non-obese and obese patients are required. Second, adiponectin levels are known to be gender dependent, but we designed this study to investigate the effects of BMI, not of gender. While the patients enrolled in our two groups were matched for gender based on propensity scores, the effect of gender on adipocytokine levels cannot be fully ruled out. Third, the diagnosis of diabetic neuropathy, which is based on having two of the following three findings, ie, diminished Achilles’ tendon reflex, inability to sense vibration and symptoms of distal neuropathy, is somewhat difficult due to the ambiguity of these features. As a result, the number of patients confirmed to have neuropathy was small as compared to those with the other two major complications. Fourth, since adiponectin clearance depends on the glomerular filtration rate,51 the effects of diabetic nephropathy progression cannot to be fully excluded in our patients. Fifth, we were not able to exclude the influences of treatments, such as thiazolidinedione,44 angiotensin converting enzyme inhibitors and angiotensin receptor blockers, which can raise serum adiponectin values. Finally, the differences in adiponectin effects among organs or sizes of adipocytes must be confirmed by in vitro functional studies. Further examinations are required to resolve these issues.
In conclusion, adiponectin elevations in accordance with the development of diabetic microvascular complication were clearly demonstrated in non-obese T2DM patients. In contrast, these relationships were far less evident, showing only slight statistical significance on multivariable logistic regression analyses, in obese patients. These newly-recognized differences in adiponectin values in response to microvascular damage between non-obese and obese patients might lead to novel insights into adiponectin regulation and our understanding of the adiponectin paradox.
Acknowledgments
This work was supported by Grants-in-Aid for Scientific Research (18K08523), to Y.I., from the Japan Society for the Promotion of Science.
Disclosure
None of the authors has any conflicts of interest to disclose for this work.
References
1. Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes. 2005;54(6):1615–1625. doi:10.2337/diabetes.54.6.1615
2. Nathan DM, Genuth S, Lachin J, et al. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329(14):977–986.
3. Man REK, Gan ATL, Fenwick EK, et al. The relationship between generalized and abdominal obesity with diabetic kidney disease in type 2 diabetes: a multiethnic asian study and meta-analysis. Nutrients. 2018;10(11):1685. doi:10.3390/nu10111685
4. Carr DB, Utzschneider KM, Hull RL, et al. Intra-abdominal fat is a major determinant of the National Cholesterol Education Program Adult Treatment Panel III criteria for the metabolic syndrome. Diabetes. 2004;53(8):2087–2094. doi:10.2337/diabetes.53.8.2087
5. Suzuki T, Gao J, Ishigaki Y, et al. ER stress protein CHOP mediates insulin resistance by modulating adipose tissue macrophage polarity. Cell Rep. 2017;18(8):2045–2057. doi:10.1016/j.celrep.2017.01.076
6. Steinberg HO, Chaker H, Leaming R, Johnson A, Brechtel G, Baron AD. Obesity/insulin resistance is associated with endothelial dysfunction. Implications for the syndrome of insulin resistance. J Clin Invest. 1996;97(11):2601–2610. doi:10.1172/JCI118709
7. Purdy JC, Shatzel JJ. The hematologic consequences of obesity. Eur J Haematol. 2021;106(3):306–319. doi:10.1111/ejh.13560
8. Kovesdy CP, Furth SL, Zoccali C. Obesity and kidney disease: hidden consequences of the epidemic. Am J Nephrol. 2017;45(3):283–291. doi:10.1159/000458467
9. Zhou Y, Zhang Y, Shi K, Wang C. Body mass index and risk of diabetic retinopathy: a meta-analysis and systematic review. Medicine. 2017;96(22):e6754. doi:10.1097/MD.0000000000006754
10. Man RE, Sabanayagam C, Chiang PP, et al. Differential association of generalized and abdominal obesity with diabetic retinopathy in asian patients with type 2 diabetes. JAMA Ophthalmol. 2016;134(3):251–257. doi:10.1001/jamaophthalmol.2015.5103
11. Sampath Kumar A, Arun Maiya G, Shastry BA, Vaishali K, Maiya S, Umakanth S. Correlation between basal metabolic rate, visceral fat and insulin resistance among type 2 diabetes mellitus with peripheral neuropathy. Diabetes Metab Syndr. 2019;13(1):344–348. doi:10.1016/j.dsx.2018.10.005
12. Oh TJ, Lee JE, Choi SH, Jang HC. Association between body fat and diabetic peripheral neuropathy in middle-aged adults with type 2 diabetes mellitus: a preliminary report. J Obes Metab Syndr. 2019;28(2):112–117. doi:10.7570/jomes.2019.28.2.112
13. Matsushita Y, Hasegawa Y, Takebe N, et al. Serum C-X-C motif chemokine ligand 14 levels are associated with serum C-peptide and fatty liver index in type 2 diabetes mellitus patients. J Diabetes Investig. 2021;12(6):1042–1049. doi:10.1111/jdi.13438
14. Maeda N, Funahashi T, Matsuzawa Y, Shimomura I. Adiponectin, a unique adipocyte-derived factor beyond hormones. Atherosclerosis. 2020;292:1–9. doi:10.1016/j.atherosclerosis.2019.10.021
15. Ouchi N, Walsh K. Adiponectin as an anti-inflammatory factor. Clin Chim Acta. 2007;380(1–2):24–30. doi:10.1016/j.cca.2007.01.026
16. Aljafary MA, Al-Suhaimi EA. Adiponectin system (rescue hormone): the missing link between metabolic and cardiovascular diseases. Pharmaceutics. 2022;14(7):1430. doi:10.3390/pharmaceutics14071430
17. Matsuzawa Y, Funahashi T, Kihara S, Shimomura I. Adiponectin and metabolic syndrome. Arterioscler Thromb Vasc Biol. 2004;24(1):29–33. doi:10.1161/01.ATV.0000099786.99623.EF
18. Menzaghi C, Trischitta V. The adiponectin paradox for all-cause and cardiovascular mortality. Diabetes. 2018;67(1):12–22. doi:10.2337/dbi17-0016
19. Rodríguez AJ, Nunes Vdos S, Mastronardi CA, Neeman T, Paz-Filho GJ. Association between circulating adipocytokine concentrations and microvascular complications in patients with type 2 diabetes mellitus: a systematic review and meta-analysis of controlled cross-sectional studies. J Diabetes Complications. 2016;30(2):357–367. doi:10.1016/j.jdiacomp.2015.11.004
20. Yang HS, Choi YJ, Han HY, et al. Serum and aqueous humor adiponectin levels correlate with diabetic retinopathy development and progression. PLoS One. 2021;16(11):e0259683. doi:10.1371/journal.pone.0259683
21. Nigro E, Scudiero O, Monaco ML, et al. New insight into adiponectin role in obesity and obesity-related diseases. Biomed Res Int. 2014;2014:658913. doi:10.1155/2014/658913
22. Consultation, WHO Expert. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
23. Takebe N, Tanno K, Ohmomo H, et al. Weight gain after 20 years of age is associated with unfavorable lifestyle and increased prevalence of metabolic disorders. Diabetes Metab Syndr Obes. 2021;14:2065–2075. doi:10.2147/DMSO.S300250
24. Wilkinson CP, Ferris FL, Klein RE, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110(9):1677–1682. doi:10.1016/S0161-6420(03)00475-5
25. Araki E, Goto A, Kondo T, et al. Japanese clinical practice guideline for diabetes 2019. Diabetol Int. 2020;11(3):165–223. doi:10.1007/s13340-020-00439-5
26. Hangai M, Takebe N, Honma H, et al. Association of advanced glycation end products with coronary artery calcification in Japanese subjects with type 2 diabetes as assessed by skin autofluorescence. J Atheroscler Thromb. 2016;23(10):1178–1187. doi:10.5551/jat.30155
27. Wei L, Li Y, Yu Y, et al. Obesity-related glomerulopathy: from mechanism to therapeutic target. Diabetes Metab Syndr Obes. 2021;14:4371–4380. doi:10.2147/DMSO.S334199
28. Borges MC, Lawlor DA, de Oliveira C, White J, Horta BL, Barros AJ. Role of adiponectin in coronary heart disease risk: a Mendelian randomization study. Circ Res. 2016;119(3):491–499. doi:10.1161/CIRCRESAHA.116.308716
29. Dieplinger B, Haltmayer M, Poelz W, Mueller T. Value of adiponectin as predictor of 5-year all-cause mortality in patients with symptomatic peripheral arterial disease: results from the Linz Peripheral Arterial Disease (LIPAD) study. Clin Chim Acta. 2009;408(1–2):87–91. doi:10.1016/j.cca.2009.07.014
30. Kizer JR, Benkeser D, Arnold AM, et al. Associations of total and high-molecular-weight adiponectin with all-cause and cardiovascular mortality in older persons: the Cardiovascular Health Study. Circulation. 2012;126(25):2951–2961. doi:10.1161/CIRCULATIONAHA.112.135202
31. Chong DQ, Mehta RS, Song M, et al. Prediagnostic plasma adiponectin and survival among patients with colorectal cancer. Cancer Prevent Res. 2015;8(12):1138–1145. doi:10.1158/1940-6207.CAPR-15-0175
32. Frystyk J, Tarnow L, Hansen TK, Parving HH, Flyvbjerg A. Increased serum adiponectin levels in type 1 diabetic patients with microvascular complications. Diabetologia. 2005;48(9):1911–1918. doi:10.1007/s00125-005-1850-z
33. Fan X, Wu Q, Li Y, et al. Association between adiponectin concentrations and diabetic retinopathy in patients with type 2 diabetes: a meta analysis. Chin Med J. 2014;127(4):765–771.
34. Matsuda M, Shimomura I, Sata M, et al. Role of adiponectin in preventing vascular stenosis. The missing link of adipo-vascular axis. J Biol Chem. 2002;277(40):37487–37491. doi:10.1074/jbc.M206083200
35. Aubert CE, Liabeuf S, Amouyal C, et al. Serum concentration and vascular expression of adiponectin are differentially associated with the diabetic calcifying peripheral arteriopathy. Diabetol Metab Syndr. 2019;11:32. doi:10.1186/s13098-019-0429-7
36. Higuchi A, Ohashi K, Kihara S, Walsh K, Ouchi N. Adiponectin suppresses pathological microvessel formation in retina through modulation of tumor necrosis factor-alpha expression. Circ Res. 2009;104(9):1058–1065. doi:10.1161/CIRCRESAHA.109.194506
37. Bushra S, Al-Sadeq DW, Bari R, Sahara A, Fadel A, Rizk N. Adiponectin ameliorates hyperglycemia-induced retinal endothelial dysfunction, highlighting pathways, regulators, and networks. J Inflamm Res. 2022;15:3135–3166. doi:10.2147/JIR.S358594
38. Fujishima Y, Maeda N, Matsuda K, et al. Adiponectin association with T-cadherin protects against neointima proliferation and atherosclerosis. FASEB j. 2017;31(4):1571–1583. doi:10.1096/fj.201601064R
39. Sakaue TA, Fujishima Y, Fukushima Y, et al. Adiponectin accumulation in the retinal vascular endothelium and its possible role in preventing early diabetic microvascular damage. Sci Rep. 2022;12(1):4159. doi:10.1038/s41598-022-08041-2
40. Sharma K, Ramachandrarao S, Qiu G, et al. Adiponectin regulates albuminuria and podocyte function in mice. J Clin Invest. 2008;118(5):1645–1656. doi:10.1172/JCI32691
41. Esmaili S, Hemmati M, Karamian M. Physiological role of adiponectin in different tissues: a review. Arch Physiol Biochem. 2020;126(1):67–73. doi:10.1080/13813455.2018.1493606
42. Ma OK, Ronsisvalle S, Basile L, et al. Identification of a novel adiponectin receptor and opioid receptor dual acting agonist as a potential treatment for diabetic neuropathy. Biomed Pharmacother. 2022;158:114141. doi:10.1016/j.biopha.2022.114141
43. Parida S, Siddharth S, Sharma D. Adiponectin, obesity, and cancer: clash of the bigwigs in health and disease. Int J Mol Sci. 2019;20(10):2519. doi:10.3390/ijms20102519
44. Maeda N, Takahashi M, Funahashi T, et al. PPARgamma ligands increase expression and plasma concentrations of adiponectin, an adipose-derived protein. Diabetes. 2001;50(9):2094–2099. doi:10.2337/diabetes.50.9.2094
45. Fasshauer M, Kralisch S, Klier M, et al. Adiponectin gene expression and secretion is inhibited by interleukin-6 in 3T3-L1 adipocytes. Biochem Biophys Res Commun. 2003;301(4):1045–1050. doi:10.1016/S0006-291X(03)00090-1
46. Yamauchi T, Kamon J, Waki H, et al. The mechanisms by which both heterozygous peroxisome proliferator-activated receptor gamma (PPARgamma) deficiency and PPARgamma agonist improve insulin resistance. J Biol Chem. 2001;276(44):41245–41254. doi:10.1074/jbc.M103241200
47. Drolet R, Bélanger C, Fortier M, et al. Fat depot-specific impact of visceral obesity on adipocyte adiponectin release in women. Obesity. 2009;17(3):424–430. doi:10.1038/oby.2008.555
48. Van Berendoncks AM, Garnier A, Beckers P, et al. Functional adiponectin resistance at the level of the skeletal muscle in mild to moderate chronic heart failure. Circ Heart Fail. 2010;3(2):185–194. doi:10.1161/CIRCHEARTFAILURE.109.885525
49. Wang Y, Ma XL, Lau WB. Cardiovascular Adiponectin resistance: the critical role of adiponectin receptor modification. Trends Endocrinol Metabol. 2017;28(7):519–530. doi:10.1016/j.tem.2017.03.004
50. Matsuda K, Fujishima Y, Maeda N, et al. Positive feedback regulation between adiponectin and T-cadherin impacts adiponectin levels in tissue and plasma of male mice. Endocrinology. 2015;156(3):934–946. doi:10.1210/en.2014-1618
51. Obata Y, Yamada Y, Takahi Y, et al. Relationship between serum adiponectin levels and age in healthy subjects and patients with type 2 diabetes. Clin Endocrinol. 2013;79(2):204–210. doi:10.1111/cen.12041
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association of Serum Leptin and Adiponectin Concentrations with Type 2 Diabetes Biomarkers and Complications Among Saudi Women
Mohammed Saeed W, Nasser Binjawhar D
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2129-2140
Published Date: 13 July 2023
The New Challenge of Obesity - Obesity-Associated Nephropathy
Hao M, Lv Y, Liu S, Guo W
Diabetes, Metabolic Syndrome and Obesity 2024, 17:1957-1971
Published Date: 6 May 2024