Back to Journals » Patient Preference and Adherence » Volume 20
Adherence to Electronic Patient-Reported Outcome Measures: A Null-Results Review of Measure-Related Effects on Response Rates in Routine Care
Authors Mukowski-Kickhöfel R ![]() , Otto LR
, Otto LR ![]() , Rogge AA
, Rogge AA ![]()
Received 28 August 2025
Accepted for publication 10 November 2025
Published 13 January 2026 Volume 2026:20 563659
DOI https://doi.org/10.2147/PPA.S563659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ramón Morillo-Verdugo
Rebecca Mukowski-Kickhöfel,1,2,* Lisa R Otto,1,2,* Alizé A Rogge1,2
1Center for Patient-Centered Outcomes Research (CPCOR), Charité – Universitätsmedizin, Berlin, Germany; 2Medizinische Klinik m.S. Psychosomatik, Charité – Universitätsmedizin, Berlin, Germany
*These authors contributed equally to this work
Correspondence: Alizé A Rogge, Email [email protected]
Abstract: This systematic review focuses on measure-related effects of PROMs on patient acceptance, adherence, and response rates in routine clinical care. The review received no external funding and was registered on medRxiv [medRxiv 2024.06.13.24308883] prior to its execution. It was conducted in accordance with PRISMA guidelines. Studies in English or German from the past ten years including patients ≥ 18 years in routine care with multiple measurement time points were included. Reports on clinical trials in terms of drug or intervention research as well as study protocols were excluded. A literature search across MEDLINE, Embase [Ovid], CINAHL, PsychArticles, PsycInfo [Ebsco], Scopus and Web of Science identified n = 420 potentially relevant publications. The data were retrieved from the data banks on 31st of January 2024. In the full-text screening, no study met the predefined inclusion criteria, therefore no risk of bias assessment or result synthesis was performed. This unexpected finding underscores a significant research gap. It indicates that the effects of instrument-inherent properties (like structure or wording) on patient adherence to PRO assessments have not been evaluated in routine care settings. The design of PROMs can have a potential influence on patient participation and the resulting data quality, which is especially relevant in light of the rising use of PRO assessments in routine care and the growing interest in real-world evidence data. Due to its search window of 10 years, its restriction to articles published in English or German, and its focus on routine care settings, the review may have excluded qualitative research and early works on adherence in routine care. Overall our review highlights the need for future research focusing on intrinsic PROM characteristics and how they relate to patients’ acceptance and adherence in order to explore the full potential of real-world data.
Keywords: patient-reported outcomes, PROs, patient-reported outcome measures, PROMs, adherence, routine care, response rate, acceptance
Introduction
Patient-reported outcomes (PROs) are a critical component of clinical research and healthcare, representing the direct input of patients on their health status, symptoms, or the impact of disease and treatment on their daily lives. Traditionally, PROs have been collected within the context of randomized controlled trials (RCTs), where they are often used to assess the effectiveness of medical interventions from the patient’s perspective.1 While RCTs provide a controlled environment, PROs are increasingly recognized as valuable in routine clinical care,2 supporting more personalized care, enhancing communication between patients and the care team, and provide real-time insights into treatment effectiveness and quality of life.3 One notable initiative in this area is H2O (Health Outcomes Observatory), which aims to systematically collect PROs across diverse patient populations and clinical contexts, aiming to demonstrate the potential of PROs to improve patient-centered care.4
Despite their importance, collecting PROs effectively in clinical care5 faces significant challenges, including a lack of infrastructure for electronic data collection, such as technical equipment and data integration with the electronic health systems (EHS), as well as limited commitment from healthcare providers due to unawareness of the relevance of PRO data or difficulties integrating this additional task into the clinical workflows.6,7
In addition to the implementation challenges, reasons for an unsuccessful systematic assessment of PROs may also lie within the patient-reported outcome measure (PROM) itself. Especially in routine care settings, where a sustained adherence to PRO assessment is very much based on continuous patient compliance, PROMs need to be attractive enough for patients to complete them. A good PROM-to-patient-fit needs to consider health literacy, relevance of the item content to the patient and their care, as well as timing and frequency of the assessment. In some cases, patients may not fully understand the importance of completing PROs or may find the process burdensome, leading to lower engagement.8–11
While implementation barriers are well documented, a research gap exists regarding the influence of PROM-specific factors on adherence. High response rates are essential to ensure that the collected PRO data is representative and reliable.12 Incomplete or biased data can undermine the conclusions drawn from PROs, leading to inaccurate assessments of treatment efficacy or patient well-being.
Therefore, we aim to identify PROM-specific factors in this systematic literature review that lead to an increase or decrease in patients’ adherence to PRO assessments in routine care. This review will exclusively focus on the structure and content of PROMs as influential factors for acceptance, adherence, and response rates.
Materials and Methods
Before the review was conducted, it was registered on medRxiv [medRxiv 2024.06.13.24308883].13 The systematic literature review was guided by the PRISMA14 framework. According to the primary research question, a search strategy was formed to identify instrument characteristics (e.g. structure or content of the PROMs) that either increase or decrease patient response rates. Reports meeting the inclusion criteria (patients aged 18 or older in a routine care setting with multiple medical contacts, see Table 1) were considered for the abstract screening. Reports on clinical trials or study protocols were excluded (Table 1). The effects of factors related to the implementation of PRO assessments have been described previously and were not part of this systematic review. The search terms (Table 2) were left deliberately broad to ensure maximum sensitivity and retrieval of potentially relevant studies. The data were retrieved from the databases on January 31st 2024.
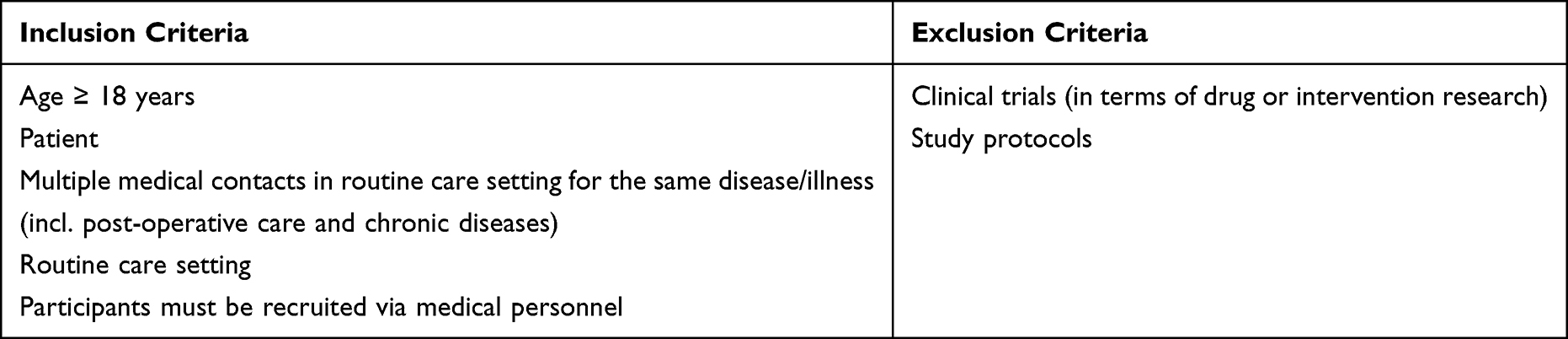 |
Table 1 Inclusion Criteria |
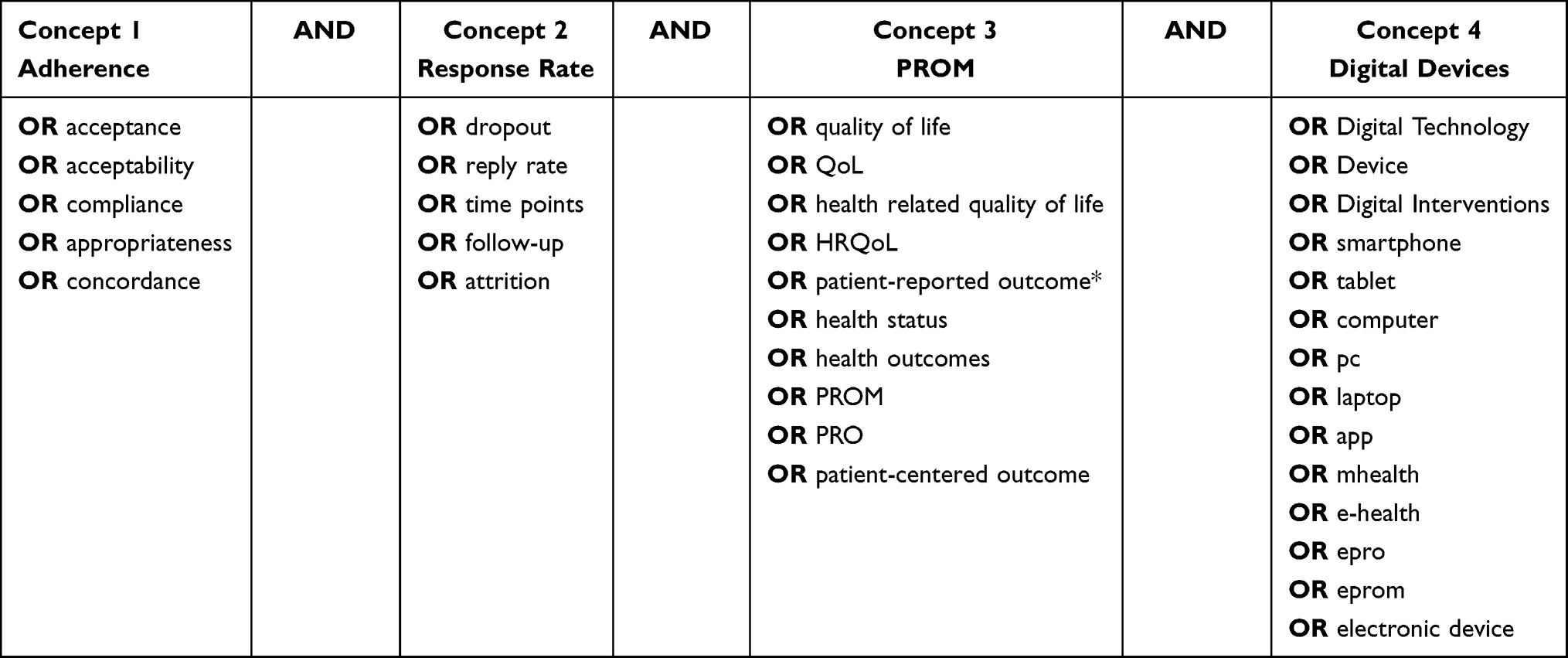 |
Table 2 Search Strategy |
The following databases were searched: MEDLINE, Embase [Ovid], CINAHL, PsychArticles, PsycInfo [EBSCO], Scopus and Web of Science. In addition, grey literature was included to minimize the risk of bias. Owing to the authors’ language skills, the review covers studies published in English and German. Reports on various study designs – including systematic reviews, observational studies, and qualitative studies – across all settings that were published in the last 10 years up to January 2024 were included for title and abstract screening. The 10-year time frame was chosen to ensure that the included studies reflect current clinical practices, technologies, and methodological standards in electronic PRO collection. The collaboration tool Rayyan15 was used to organize the screening of titles and abstracts and for the full-text reviews.
Following the systematic search of databases, a grey literature search was conducted for additional reports that were not detected through the systematic database search aiming to minimize the risk of bias. Additionally, the reference lists of the identified papers and existing reviews were examined to identify further relevant articles.
All titles were initially screened and by one author (AR) and duplicates were removed automatically by the Rayyan15 tool. In case of uncertainty during the title screening, a discussion took place between all authors involved. The abstracts of the remaining titles were reviewed by AR and either of the other two authors (RMK, or LO). The authors used the Rayyan15 tool to identify conflicts in study evaluations. To minimize the risk of bias, all authors met when discrepancies occurred to resolve them transparently through discussion.
“Patient-reported outcome measures” were interpreted narrowly to only include studies that focus on patients or people recruited in a medical context. As no studies met the predefined inclusion criteria, no data were extracted, transformed, or synthesized and the procedures for data preparation, synthesis, risk of bias assessment, and certainty evaluation could not be applied.
Results
An initial literature search in the databases identified n = 420 papers.
Additionally, n = 10 articles were handpicked by the authors and included in the first step of the systematic review. Prior to screening, n = 19 duplicate records were removed using the collaboration tool Rayyan.15 Following title screening conducted by one author (AR), n = 119 articles remained for abstract screening by AR and either of the other two (LO, RMK) authors. As shown in Figure 1, study protocols and background literature were excluded for “wrong publication type”. Articles describing studies in a non-routine care setting, or investigating non-patients in a non-medical care setting were excluded for the “wrong study design” or “wrong population”, respectively. Any studies not focusing on PROM characteristics and their effect on adherence were classified as “wrong outcome”. After screening the abstracts, n = 89 articles were removed. Therefore, n = 30 articles were assessed in the full-text screening. Table S1 of the Supplemental Material shows the articles selected for the full-text screening.
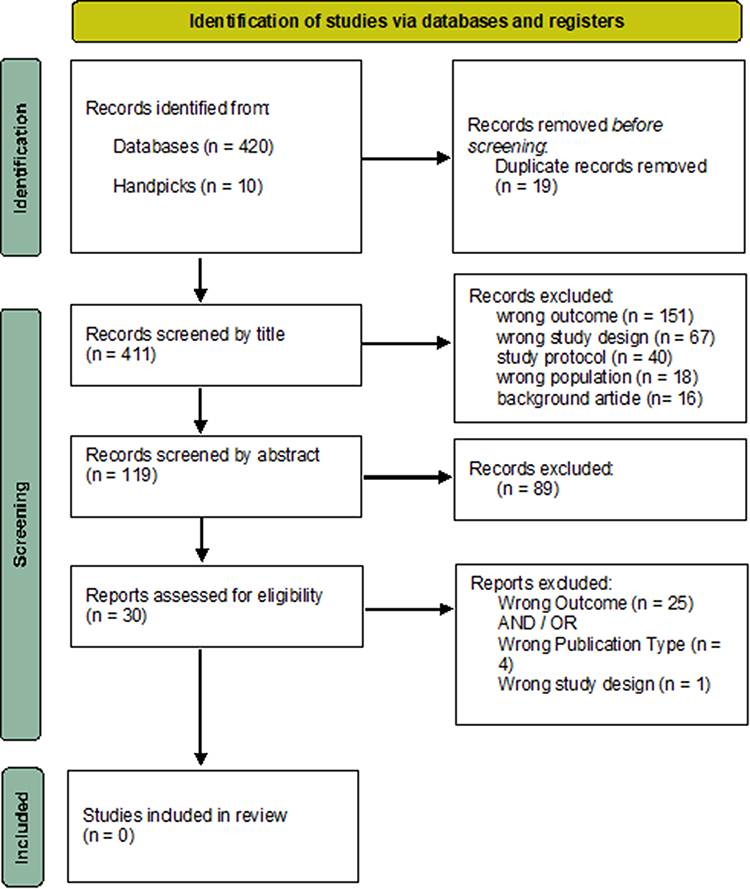 |
Figure 1 PRISMA 202011 flow diagram depicts the flow of information through the different phases of the systematic review. |
Figure 2 illustrates the distribution of main topics across the articles that were reviewed during the full-text screening. The articles predominantly addressed technology acceptance (n = 17) and implementation (n = 9). Three of the screened articles focused on the development of PROMs or electronic patient-reported outcome measures (ePROMs). One was a guideline on PRO assessment, covering instrument selection, score interpretation, and response recommendations. One article16 was excluded due to its study design, despite containing information about adherence related to PROM content, as its primary focus was the development process of a PROM. As a result of the full-text screening, n = 0 articles met the inclusion criteria. As no studies were included, no formal risk of bias assessment was performed. Consequently, there are no summary statistics, tables or plots showing the results. Since no synthesis was conducted, this review does not present summary estimates, measures of heterogeneity, sensitivity or bias analyses, nor an assessment of the overall certainty of the evidence.
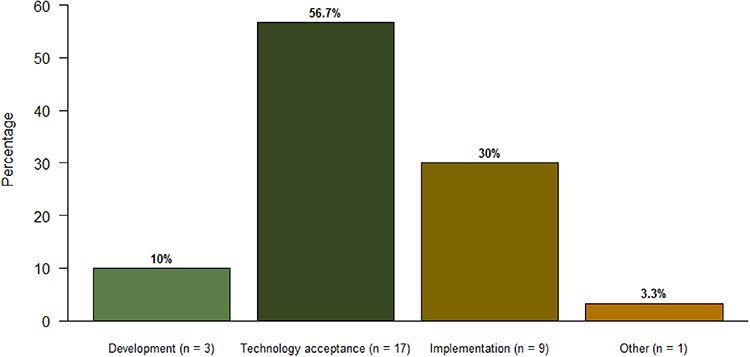 |
Figure 2 Primary focus areas of the screened articles. |
Discussion
In this systematic literature review, we aimed to investigate whether specific structural or content-related characteristics of PROMs influence patient adherence and response rates in routine clinical care. Previous systematic reviews have covered general barriers to implementing PRO assessments in clinical studies and routine care. In contrast, the current review focused specifically on PROM-intrinsic factors that influence response rates in routine care.
Following PRISMA guidelines, we conducted a comprehensive search across seven databases for studies published within the last 10 years up to January 2024. Despite this broad and systematic approach, no studies met the inclusion criteria. This unexpected result highlights a significant gap in the literature and suggests that potential biases inherent in PROM design may be underexplored factors influencing patient participation and data quality.
One possible explanation for the absence of evidence is publication bias. Studies on the structure and content of PROMs in routine care may have been conducted but not published due to non-significant results. This highlights the value of this null-results review, as the publication of null findings can expose important research gaps. Another possible explanation in this area is that research on PROMs has historically focused more on implementation logistics—such as reminder systems, communication strategies, and technological platforms—rather than critically examining the instruments themselves, apart from their validity evidence. This is surprising given the well-documented presence of gender, racial, and other sociodemographic biases in healthcare tools, including PROMs.17,18 While there is growing awareness that such measures may not be equally accessible or relevant to all patients, more attention needs to be paid to how contextual assumptions of PROMs may actively shape or limit who responds to them and how.19 Unlike other areas where behavioral science is routinely applied—such as optimizing reminder frequency or tailoring digital nudges—the structure and content of PROMs have only as of late been treated as variables with measurable impact on response,18,20 adherence over time, and equity. This oversight suggests a methodological blind spot in PROM research, where the measure is too often treated as a neutral tool rather than a potentially active agent in shaping patient engagement.
This review has several limitations. First, we restricted our search to studies published in the last 10 years to reflect the rapid evolution of electronic PROMs and their integration into clinical workflows. However, this may have led to a selection bias and excluded relevant foundational work. Second, our inclusion criteria specifically targeted studies that investigated the impact of PROM-specific structural or content-related factors on adherence in clinical care settings, potentially omitting valuable insights from research that addressed similar concepts through other terminology (e.g., patient preference) and methods, including qualitative interviews and observational designs. Additionally, while many studies document decreased adherence among specific populations—such as lower response rates among Black males completing prostate cancer PROMs21 —they rarely investigate which specific aspects of the measures themselves contribute to these disparities. Future research should therefore systematically investigate which structural and content-related features of PROMs contribute to differential engagement to address this research gap. For example, mixed-methods designs that examine the underlying “mechanisms of action” of PROMs in routine care settings, could shed light on the intrinsic PROM features related to assessment adherence. Understanding different patient perceptions, motives, interpretations, and interactions with PROMs across cultures, languages, clinical contexts, and life situations is essential for developing targeted assessments that genuinely meet patients where they are.22
Poor adherence to PRO assessments may be explained by psychological factors deriving from the patients themselves. Applying frameworks such as the Health Belief Model10 and Self-Determination Theory,11 it could very well be possible that patients who perceive limited personal benefit, low relevance, or reduced autonomy in completing questionnaires are less likely to engage consistently. Understanding motivational barriers could further support the implementation of patient-centered approaches to PROM development and implementation.
Bridging this research gap could not only inform the design of more suitable PROMs but also empower patients22 and guide clinicians, developers, and policymakers in recognizing that patients’ preferences extend beyond the simple acceptance of a measure to deeper issues of relevance, resonance, and trust. If we are to achieve meaningful, large-scale implementation of PROs, we must move beyond surface-level optimization and understand the functional dynamics that influence how PROMs perform in everyday clinical practice, where patient motivations, constraints, and lived experiences shape treatment outcomes in ways that randomized controlled trials often overlook.
Conclusion
In this study, we uncovered the absence of evidence on the impact of structural or content-related characteristics of PROMs on patient adherence and response rates in routine clinical care. This highlights a critical gap in the current literature. It also raises the possibility that inherent design elements of PROMs may contribute to nonresponse bias, specifically their structure and content - an area that has received limited attention but warrants further investigation. Our findings underscore the need for targeted research to evaluate how PROM-specific characteristics impact their utility and integration into clinical workflows, ensuring that value-based healthcare and patient-centered care are embedded not only in research but also in routine clinical practice.
Acknowledgments
This research received no external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Willke RJ, Burke LB, Erickson P. Measuring treatment impact: a review of patient-reported outcomes and other efficacy endpoints in approved product labels. Controlled Clin Trials. 2004;25(6):535–7. doi:10.1016/j.cct.2004.09.003
2. Dreyer NA. Strengthening evidence-based medicine with real-world evidence. Lancet Healthy Longev. 2022;3(10):e641–e642. doi:10.1016/S2666-7568(22)00214-8
3. Graupner C, Kimman ML, Mul S, et al. Patient outcomes, patient experiences and process indicators associated with the routine use of patient-reported outcome measures (PROMs) in cancer care: a systematic review. Support Care Cancer. 2021;29(2):573–593. doi:10.1007/s00520-020-05695-4
4. Stamm T, Mosor E, Andrews MR, et al. Building a value-based care infrastructure in Europe: the health outcomes observatory. NEJM Catalyst Innov Care Deliv. 2021;2(3). doi:10.1056/cat.21.0158
5. Franzoi MA, Ferreira AR, Lemaire A, et al. Implementation of a remote symptom monitoring pathway in oncology care: analysis of real-world experience across 33 cancer centres in France and Belgium. Lancet Regional Health - Europe. 2024;44:101005. doi:10.1016/j.lanepe.2024.101005
6. Dreyer NA. Advancing a framework for regulatory use of real-world evidence: when real is reliable. Therap Innov Regulatory Sci. 2018;52(3):362–368. doi:10.1177/2168479018763591
7. Lehmann J, Dragan T, Rammant E, et al. Exploring the integration of patient-reported outcome measures in clinical practice: a cross-sectional survey of EORTC healthcare professionals. Eur J Cancer. 2025;220:115333. doi:10.1016/j.ejca.2025.115333
8. Nguyen H, Butow P, Dhillon H, Sundaresan P. A review of the barriers to using Patient‐Reported Outcomes (PROs) and Patient‐Reported Outcome Measures (PROMs) in routine cancer care. J Medl Radiat Sci. 2021;68(2):186–195. doi:10.1002/jmrs.421
9. Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018;9:353–367. doi:10.2147/PROM.S156279
10. Alyafei A, Easton-Carr R. The health belief model of behavior change. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024.
11. Deci EL, Ryan RM. The “what” and “why” of goal pursuits: human needs and the self-determination of behavior. Psychol Inq. 2000;11(4):227–268. doi:10.1207/S15327965PLI1104_01
12. Takvorian SU, Anderson RT, Gabriel PE, et al. Real-world adherence to patient-reported outcome monitoring as a cancer care quality metric. JCO Oncol Pract. 2022;18(9):e1454–e1465. doi:10.1200/OP.21.00855
13. Mukowski-Kickhöfel R, Otto L, Rogge A. Improving adherence to electronic patient-reported outcomes: study protocol for a systematic literature review and subsequent qualitative interviews. Health Syst Qual Improvement. 2024. doi:10.1101/2024.06.13.24308883
14. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021:n71. doi:10.1136/bmj.n71
15. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan—a web and mobile app for systematic reviews. Syst Rev. 2016;5(1):210. doi:10.1186/s13643-016-0384-4
16. Väyrynen K, Chen A, Leskelä RL, et al. Introducing standard patient-reported measures (PRMs) into routine maternity care: a pre-implementation qualitative study on women’s perspectives in Finland. BMC Health Serv Res. 2023;23(1):845. doi:10.1186/s12913-023-09818-5
17. Shin D, Meade S, Scariano G, et al. Improving equitable collection and analysis of PROMIS global health data over time following spine surgery: characterizing survey non-response and missing data. Spine J. 2025;25(10):2299–2311. doi:10.1016/j.spinee.2025.04.022
18. Stephens AR, Bender NR, El-Hassan R, Patel RK. Evidence of non-response bias in patient reported outcome measurement information system surveys. Intervent Pain Med. 2025;4(2):100588. doi:10.1016/j.inpm.2025.100588
19. Tuinenburg A, Determann D, Quik EH, et al. Evaluating comprehensibility of 157 Patient-Reported Outcome Measures (PROMs) in the Nationwide Dutch Outcome-Based Healthcare Program: more Attention for Comprehensibility of PROMs is needed. Patient. 2025;18(1):65–76. doi:10.1007/s40271-024-00710-w
20. Long PA, Huberts AS, Di Torrero AN, et al. The mere-measurement effect of patient-reported outcomes: a systematic review and meta-analysis. Qual Life Res. 2025;34(5):1211–1220. doi:10.1007/s11136-025-03909-y
21. Lillard JW, Moses KA, Mahal BA, George DJ. Racial disparities in Black men with prostate cancer: a literature review. Cancer. 2022;128(21):3787–3795. doi:10.1002/cncr.34433
22. Aiyegbusi OL, Cruz Rivera S, Kamudoni P, et al. Recommendations to promote equity, diversity and inclusion in decentralized clinical trials. Nat Med. 2024;30(11):3075–3084. doi:10.1038/s41591-024-03323-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.