")
Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 15
Adherence to Antiretroviral Therapy and Associated Factors Among HIV-Infected Children in Public Health Institutions of Adwa, Axum, and Shire Towns of Tigray, Northern Ethiopia: A Cross-Sectional Study
Authors Tesfahunegn TB, Berhe N, Abraha TH , Hintsa S , Yohanes G, Desta K, Alema HB , Hagos E, Gidey G , Teshahunegn GB
Received 20 September 2020
Accepted for publication 28 June 2021
Published 3 May 2023 Volume 2023:15 Pages 217—224
DOI https://doi.org/10.2147/HIV.S282938
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Tadis Brhane Tesfahunegn,1 Negassie Berhe,2 Teklehaymanot Huluf Abraha,1 Solomon Hintsa,3 Goitom Yohanes,1 Kahsay Desta,4 Haileselasie Berhane Alema,5 Elsa Hagos,6 Gebreamlak Gidey,7 Gebreyesus Brhane Teshahunegn8
1Department of Reproductive Health, College of Health Sciences, Aksum University, Aksum, Ethiopia; 2Department of Human Nutrition, College of Health Sciences, Aksum University, Aksum, Ethiopia; 3Department of Epidemiology, College of Health Sciences, Aksum University, Aksum, Ethiopia; 4School of Medicine, College of Health Sciences, Aksum University, Aksum, Ethiopia; 5Department of Public Health, College of Health Sciences, Aksum University, Aksum, Ethiopia; 6Department of Medical Laboratory, College of Health Sciences, Aksum University, Aksum, Ethiopia; 7Department of Midwifery, College of Health Sciences, Aksum University, Aksum, Ethiopia; 8College of Agriculture, Aksum University, Shire, Ethiopia
Correspondence: Haileselasie Berhane Alema Department of Public Health, College of Health Sciences, Aksum University, P.O.Box: 298, Aksum, Ethiopia Tel +251914006933 Email [email protected]
Background: Antiretroviral therapy (ART) provision was among the major challenge of treatments. Maintaining the optimal level of adherence among children living with HIV/AIDS is a pivotal step towards achieving treatment success. However, there are limited studies on child’s ART adherence. Therefore, this study aimed to assess the level of adherence to antiretroviral therapy and associated factors among HIV-infected children in health institutions of Adwa, Axum, and Shire towns, Tigray, Northern Ethiopia.
Methods: An institutional-based cross-sectional study was conducted among human immunodeficiency virus (HIV)-infected children in between February and April, 2016. A total of 255 children who were taking antiretroviral therapy in the randomly selected three health facilities from Adwa, Axum and Shire towns were included. Data were collected using pretested and structured questionnaires using a face-to-face interview. The collected data were entered into Epi Info version 7 and then exported to SPSS version 21 for analysis. Bivariate and multivariate binary logistic regression models were used to determine the factors associated with adherence to antiretroviral therapy among HIV-infected children.
Results: A total of the 255 study participants were included in the study. The level of ART adherence among HIV-positive children was 212 (84.8%). Knowledge of caregivers about ART treatment (AOR = 2.78, 95% CI: 1.18, 6.53), occupational status (AOR = 4.78, 95% CI: 1.26, 18.91), appointment to ART less than two months (AOR = 3.05, 95% CI: 1.21, 7.70) and use of memory aids (AOR = 4.58, 95% CI: 1.73, 12.13) were independently associated with adherence to ART.
Conclusion: The level of adherence to antiretroviral therapy was low. Healthcare providers should reinforce adherence intervention and counseling sessions during follow-up and address the proper use of medication reminders to help children take their drugs appropriately.
Keywords: HIV, adherence, ART, children, Ethiopia
Introduction
Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) is a major public health problem.1,2 More than 36 million people are living with HIV worldwide 2018.3 According to the President’s Emergency Plan for AIDS Relief (PEPFAR’s) report, 610,335 people are living with HIV /AIDS and 13,556 AIDS death annually in Ethiopia. Sixteen percent of people living with HIV/AIDS in Ethiopia are children (age <19 years old). Among children living with HIV at global level, 43% accessed ART.24 In Ethiopia, only 33% of children aged below 15 years had access to ART.25 In East Africa, studies revealed that the prevalence of adherence to antiretroviral therapy among children living with HIV as 79% in Kabale district of Uganda,26 93.3% in central Ethiopia,27 and 78.6% in North West Ethiopia.3 Antiretroviral therapy (ART) has proven to be the most effective treatment method for people living with HIV.4,5
Adherence means the client accepts, agrees, and correctly follows a prescribed treatment by healthcare provider. ART has proven to be the most effective treatment method for people living with HIV/AIDS.4,5 It improves the prognosis of HIV-infected patients, reduces HIV-related morbidity and mortality, and reduces other opportunistic infections.29–31 Inadequate adherence to ART increases the risk of treatment failure and ART drug resistance,24,28 immunological decline resulting in opportunistic infections,32 and HIV disease progression.33
In Ethiopia, ART provision has the major challenges. Despite the efforts made over the last decades, still universal access to ART remains low.11 In East Africa, studies reveal that the prevalence of adherence to antiretroviral therapy among children living with HIV was 79% in Kabale district, Uganda,12 93.3% in Central Ethiopia,13 and 78.6% in North West Ethiopia.3 Several factors affect the level of treatment adherence among children living with HIV are caregiver’s educational level if the child knows HIV-positive status,3 and caregiver’s knowledge about ART, caregivers’ who knew their HIV status.12
Maintaining the optimal level of adherence among children living with HIV/AIDS is a pivotal step towards achieving treatment success.14 According to the Ethiopian Pediatric HIV care and treatment guideline, disclosure of children (less than 12 years) with HIV-positive status and the medication is unwilling to the child. This is a challenge in administering doses while the parent is at work or travelled to other place and affects medication adherence. As a result, HIV will develop drug resistance if the drug adherence is poor. Meanwhile, the limited accessibility of second-line therapy in Ethiopia due emphasizes should be given for adherence and preservation of first-line regimens. Moreover, assessment and support of adherence is fundamental to successful antiretroviral therapy and prevention of drug resistance. So, this study could help to the health policy makers to design appropriate intervention modalities based on evidences to improve antiretroviral therapy (ART) adherence among children. Therefore, this study aimed to assess the level of pediatrics antiretroviral therapy adherence and associated factors among HIV-infected children in health institutions of Adwa, Axum, and Shire towns, Tigray, Northern Ethiopia.
Methods
Study Setting
An institutional-based quantitative cross-sectional study was conducted in health institutions of Adwa, Axum and Shire town in Tigray region, Ethiopia from February to April 2016. The selected town consists of 3 government hospitals and six health centers that provide ART services with over 250 health professionals. All children who were taking antiretroviral therapy (ART) in the selected health institutions were the source population and children aged >2 months to 15 years receiving antiretroviral therapy (ART) for at least 2 months were included in the study. About 270 HIV-positive children were on ART at health institutions of Adwa, Axum and Shire town that provide pediatric ART medication were included in the study. These health facilities provide ART services children living with HIV who registered to pediatric ART clinic.
Sample Size Determination
For this study, sample size determination was not required as the study was included all children who are currently receiving ART medication in the health institutions of Adwa, Axum and Shire towns. All 270 children with HIV positive were included in the study but 15 children were not attended in the facilities during data collection period. So, all 255 children who are on ART were included in the study.
Data Collection Procedures
Data were collected using pretested and structured questionnaire administered by face to face interviewers with caregivers. The content of the questionnaire included socio-demographic characteristics of caregivers and children, knowledge of caregivers about ART regimen, treatment adherence, and healthcare system and patient health provider relationship. The questionnaires were pre-tested on 25 children out of the study area. Based on the feedback obtained from the pre-test, an appropriate modification was made on the questionnaire. A questionnaire was adapted from different literatures,2,4,14,15 which was prepared in English and then translated into Tigrigna (local language), and back-translated to ensure consistency. Two days of training was provided to data collectors and supervisors. Data were collected by nine bachelor degree nurse professionals.
Data Entry and Analysis
The collected data were checked, coded and entered into Epi-info version 6 and then exported to SPSS version 21 for analysis. Descriptive statistics were computed and presented by percentage, mean to determine adherence level. Bivariate and multivariate binary logistic regression models were used to determine the factors associated with adherence to antiretroviral therapy among HIV-infected children. All variables with P<0.2 in the bivariate logistic regression model were included in the multivariate logistic regression. Variables associated with adherence were determined in multiple logistic regression at P-value <0.05 and AOR of 95% CI. The model fitness was checked using Hosmer and Lemeshow goodness-of-fit test statistics (P = 0.70).
Operational Definitions
Good adherence of ART medication: Adherence of ART medication was measured as, caregivers self report for antiretroviral therapy (ART) medication who has been missed less than 3 doses in the past seven days and children with ART medications adhered >95% of the prescribed doses categorized as Good adherence.2,4,14,15
Knowledge of caregiver on children ART adherent: caregivers who scored equal and above the overall mean value for adherence knowledge assessment question score was categorized as good knowledge.
Results
Socio-Demographic Characteristics of Caregivers and Children
Out of the 255 study participants (5 questionnaires were incomplete), 250 responded to the questionnaires properly, a response rate of 98.03%. Of all the respondents, 219 (87.6%) were females. The mean age (±SD) of the caregivers was 37.5 (±9.1) years. Two hundred twenty-two (88.8%) of the participants were Orthodox Christian followers. Among the caregivers 106 (42.4%) were not able to read and write. Ninety-eight (39.2%) of the caregiver interviewed were married. Regarding sex of the caregivers, 219 (87.6%) were females (Table 1).
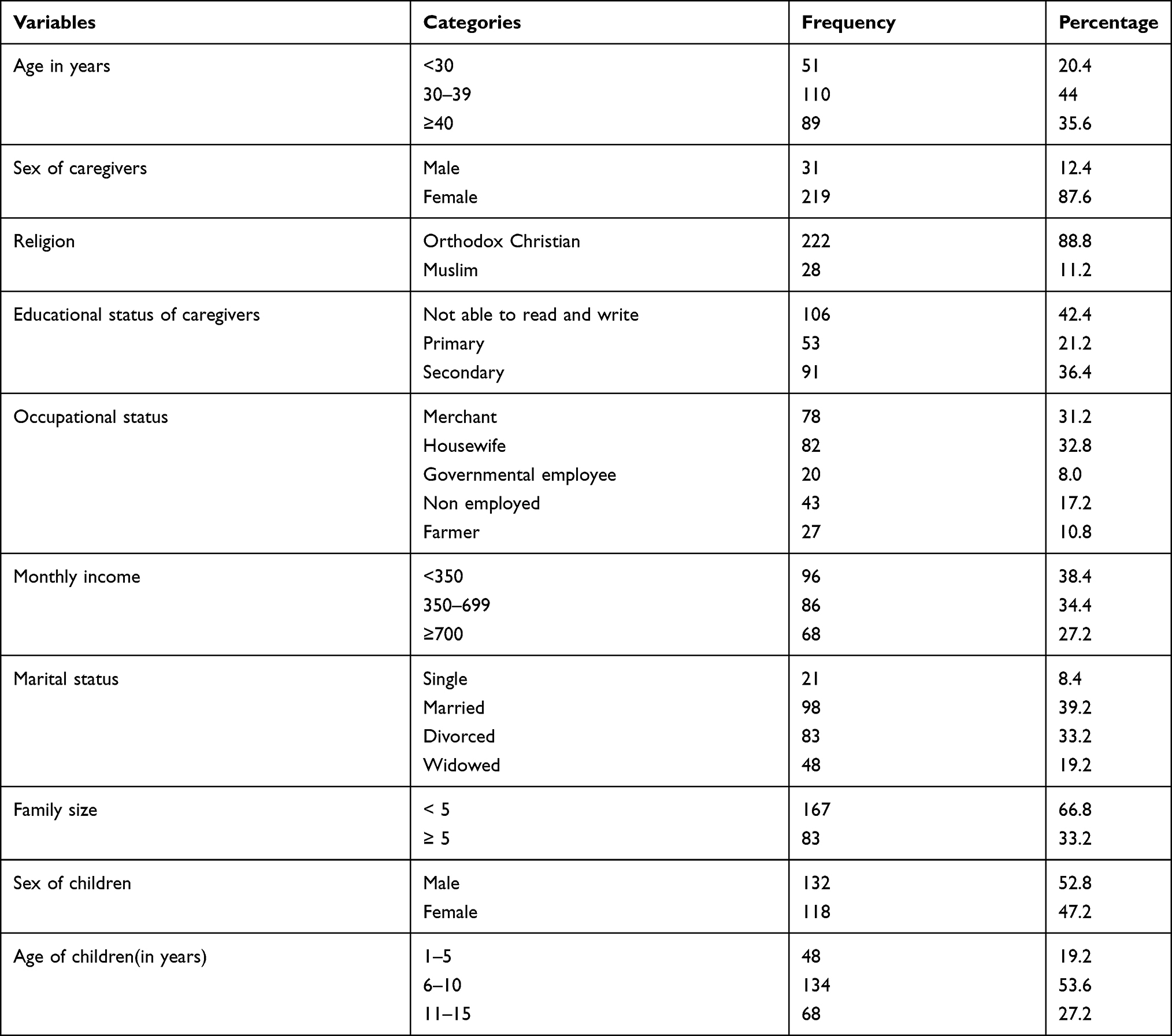 |
Table 1 Socio-Demographic Characteristics of the Caregivers and Children at Adwa, Axum and Shire Health Institutions, Tigray, North Ethiopia, 2016 (n = 250) |
Treatment and Social Support Related Characteristics
Of the participants, 198 (79.2%) reported that their children were using memory aids as reminders for their time schedule of ART medications. More than two-thirds 106 (64%) of the caregivers were knowledgeable about ART. One hundred twenty-six (50.4%) of the children had an appointment to ART less than two months. One hundred sixty-seven (66.8%) participants reported that their children HIV status was not disclosed to other community members in their surroundings. In addition to this, 193 (77.2%) caregivers revealed that there is no any social support regarding ART (Table 2).
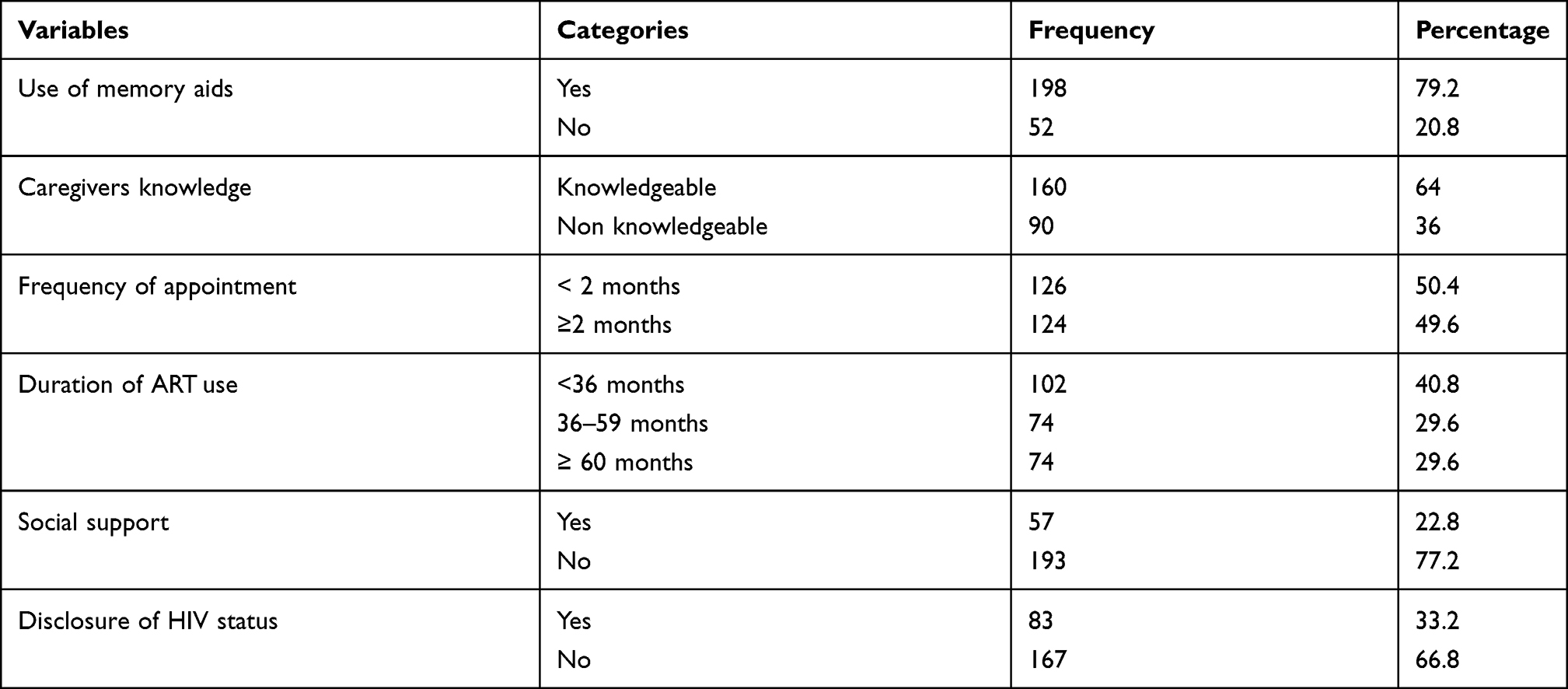 |
Table 2 Treatment and Social Support Related Characteristics of Caregivers and Children at Adwa, Axum and Shire Health Institutions, Tigray, North Ethiopia, 2016 (n = 250) |
Adherence to ART Among the Children
Based on self-report and pill counts during the past three and seven days, 220 (88%) and 212 (84.8%) of the total children were taking greater than 95% of the total prescribed ART doses respectively. According to the care givers report, the level of adherence to ART among children was 205 (82%) in the one-month recall period before the survey.
Factors Associated with Adherence to ART Medication Among Children
The multivariate logistic regression analysis showed that secondary and above educational status of the caregivers, knowledge of caregivers about ART treatment, occupational status, appointment to ART less than two months and use of memory aids were independently associated with adherence to ART.
Children whose caregivers with secondary and above educational status were 3.8 times more likely to be adherent to ART than those children whose caregivers with educational status of unable to read and write (AOR = 3.8, 95% CI: 1.30, 11.17). Children with knowledgeable caregivers about ART treatment were 4.78 times more likely to be adherent than their counterparts (AOR = 4.78, 95% CI: 1.26, 18.91). Children with appointment to ART less than two months were 3.05 times more likely to be adherent than those with appointment of two months and beyond (AOR = 3.05, 95% CI: 1.21, 7.70). This study also showed that children who used memory aids were 4.58 times more likely to be adherent than those who did not use memory aids (AOR = 4.58, 95% CI: 1.73, 12.13) (Table 3).
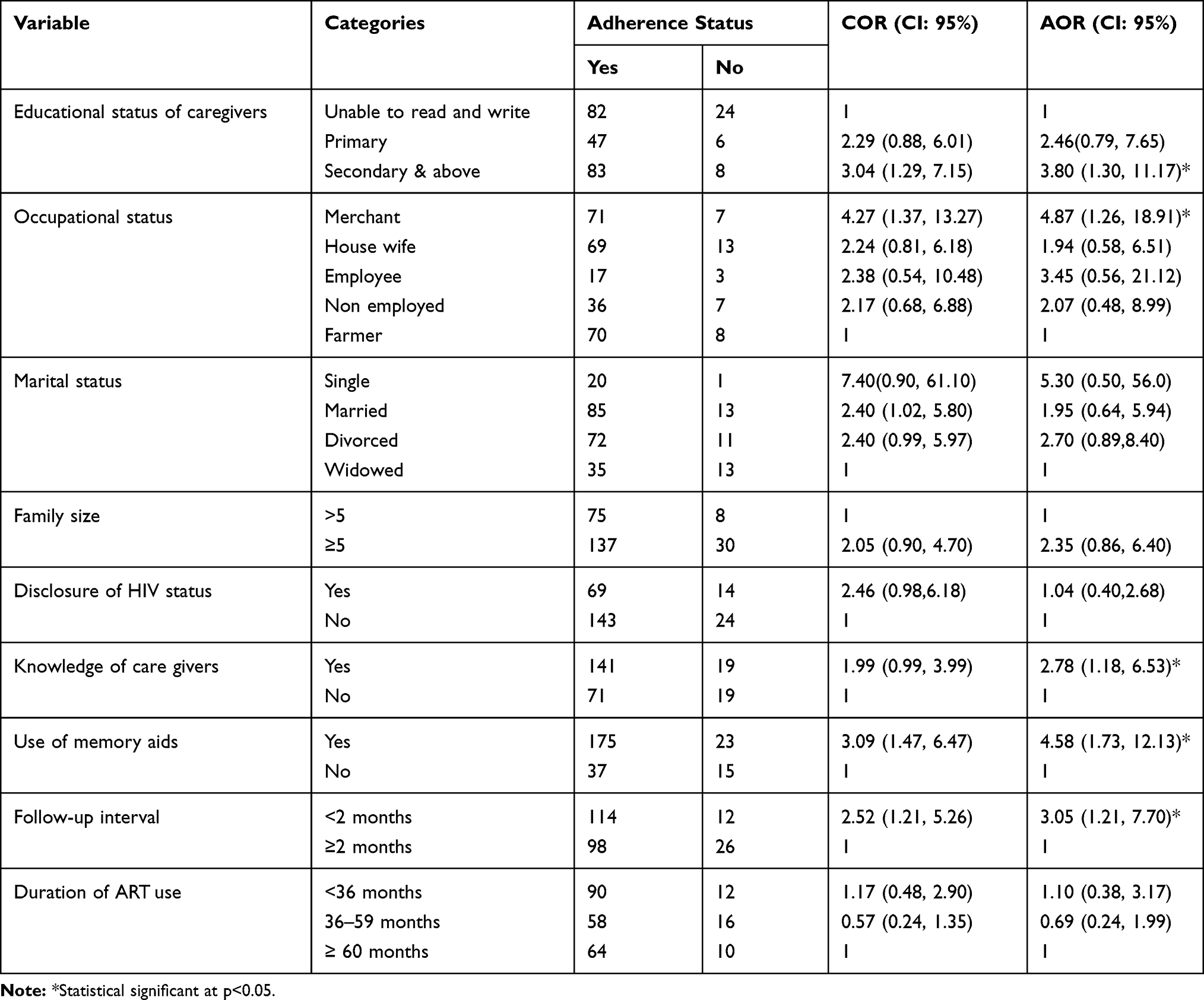 |
Table 3 Bivariate and Multivariate Logistic Regression Analysis of the Factors Associated with Adherence to ART Among HIV-Positive Children, at Adwa, Axum and Shire Towns Health Institutions, Tigray, Northern Ethiopia, 2016 (n = 250) |
Discussion
Based on self-report and pill counts, among the total children taking ART drugs during the past seven days 84.8% (95% CI; 80.0–89.2) of them took greater than 95% of the total prescribed doses. Different studies from Ethiopia such as Gondar University Hospital, North west Ethiopia,2 Debre Markos Referral Hospital, Ethiopia,4 Hiwot Fana and Dil-Chora Hospital in Eastern Ethiopia,5 Mekelle Hospital, Northern Ethiopia,6 a systematic review and meta‑analysis in Ethiopia,7 and a study from a rural pediatric cohort in South Africa9 reported almost similar adherence level to ART as 90.4%, 88.6%, 90.7%, 90.3%, 88.7%, and 87.8%, respectively. However, the finding of this study is inconsistent with the other studies reported from different settings. Studies study from Ethiopia,14 Uganda,10 North India,13 and a study from Thailand12 who have reported a higher level of adherence to ART which is 93.3%, 97.3%, 95.3%, and 98.8% of the respondents, respectively. Nevertheless, studies from South Wollo Zone Hospitals, Ethiopia,3 Fiche Hospital, Ethiopia,8 and Togo, West Africa11 reported a lower level of adherence to ART among the children as 78.6%, 64.2%, and 58%, respectively. The difference might be due to fully subsidize, experience on side effects of treatments, differences in the measurement of adherence assessment used, socio-demographic and cultural background of study participants, and the difference of patient-healthcare provider relationships in different settings.
In this study, educational status of caregivers was positively associated with adherence to ART. Children whose caregivers had secondary and above education were 3.8 times more likely to be adherent to ART compared to children whose caregivers were illiterate. This is in line with the study in Fiche Hospital, Ethiopia, which reported caregivers of children with higher education were less likely to be non-adherent than the non-educated caregivers.8
This study revealed that children caregivers’ merchant occupation was positively associated with adherence to ART compared with caregivers’ farmer occupations. Children with caregivers’ merchant occupation were 4.87 times more likely to be adherent to ART compared to children whose caregivers’ were farmer occupation. This could be because those employed caregivers in urban areas may have better awareness about ART treatments than those farmers who are mostly in rural areas. It could also be related with educational status. This study revealed that those children from caregivers with higher education are more likely to be adherent to ART than those from no formal education caregivers.
The current study also revealed that with children knowledgeable caregivers about the disease were 2.78 times more likely to be adherent to ART than those who were not knowledgeable. This finding is similar to the other studies conducted in Gondar Poly Clinic, Ethiopia,2 South Wollo Zone Hospitals, Ethiopia,3 Hiwot Fana and Dil-Chora Hospitals in Eastern Ethiopia,5 two referral hospitals, Northwest Ethiopia,16 and a study of pediatric patients in Ethiopia.17 This can be explained that caregivers who have good knowledge on the importance of drug treatment was significantly associated with optimal adherence to ART.18 Those who are knowledgeable about the disease are more likely to give adequate care and increase the adherence status of their children.
Similarly, our study also showed that children whose caregivers used memory aids were 4.58 times more likely to be adherent to ART than those who did not use memory aids. This result is consistent with the studies conducted among the adults in different settings.1,15,19–21 This indicates that adherence interventions and counseling sessions by professionals should include memory aids and other reminders to help children take their drugs appropriately.
In this study, ART clinic follow-up interval of children less than two months was three times more likely adherent to ART than those with follow-up intervals of two months and beyond. This could be due to the recommended clinic ART follow-ups may be good indicators of better ART adherence. Different researches have already shown the dynamic character of ART treated patients’ adherence behaviors, influenced by the multiple factors varying from time to time.22,23 The findings of this study regarding shorter follow-up intervals may be good indicators to determine caregiver’s behavior to ART adherence.
Conclusion
This study showed that the level of children adherence to antiretroviral therapy was found to be low assuming it is lower than what is recommended by the World Health Organization, which is greater than 95%. Secondary and above educational status of the caregivers, knowledge of caregivers about ART treatment, a farmer by occupation, an appointment to ART less than two months and use of memory aids were independently associated with adherence to ART. Healthcare providers should reinforce adherence intervention and counseling sessions during follow-up and address the proper usage of medication reminders to help children take their drugs appropriately.
Limitation of the Study
The findings of this study should be interpreted with some limitations. Since this is the cross-sectional nature of study, which used a snapshot of adherence at one point in time may hinder the accuracy of adherence. Adherence assessment was based on the caregivers self-report, which may have resulted to prone recall bias and social desirability. There is no golden standard to measure adherence of children ART medication. And, this study measured adherence based on caregivers self report of missed doses self-reporting may overestimate the rate of adherence to medication. Moreover, the study was also not triangulated with qualitative study design were some of the limitation.
Abbreviations
AIDS, Acquired Immune Deficiency Syndrome; HIV, Human Immune Virus; ART, antiretroviral therapy; SPSS, Statistical Package for Social Science; WHO, World Health Organization.
Data Sharing Statement
All relevant data are within the paper. The SPSS data sets are not permitted to be provided to other bodies, as outlined by the ethics committee who approved the study. However, the datasets used to analyze for the study can be available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
Ethical clearance was obtained from the Institutional Ethical Review Committee (IRC) of the College of Health Sciences of Aksum University and the permission letter was obtained from concerned officials at a different level. Before interview informed written consent was obtained from caregivers. To preserve confidentiality of respondent, anonymous data collection technique was used and all data collection procedure was conducted in compliance with the Declaration of Helsinki.
Acknowledgments
The authors are highly grateful to all participants of the study, supervisors of data collection, and data collectors for their worthy efforts and participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no specific funding for this work.
Disclosure
The authors declare that they have no competing interests.
References
1. Amberbir A, Woldemichael K, Getachew S, Girma B, Deribe K. Predictors of adherence to antiretroviral therapy among HIV-infected persons: a prospective study in Southwest Ethiopia. BMC Public Health. 2008;8(1):265. doi:10.1186/1471-2458-8-265
2. Dachew BA, Tesfahunegn TB, Birhanu AM. Adherence to highly active antiretroviral therapy and associated factors among children at the University of Gondar Hospital and Gondar Poly Clinic, Northwest Ethiopia: a cross-sectional institutional based study. BMC Public Health. 2014;14(1):875. doi:10.1186/1471-2458-14-875
3. Arage G, Tessema GA, Kassa H. Adherence to antiretroviral therapy and its associated factors among children at South Wollo Zone Hospitals, Northeast Ethiopia: a cross-sectional study. BMC Public Health. 2014;14(1):365. doi:10.1186/1471-2458-14-365
4. Asmare M, Aychiluhem M, Ayana M, Jara D, Kajon A. Level of ART adherence and associated factors among HIV sero-positive adult on highly active antiretroviral therapy in Debre Markos Referral Hospital, Northwest Ethiopia. J Antivir Antiretrovir. 2014;6(3):40–42. doi:10.4172/jaa.1000093
5. Zegeye S, Sendo E. Adherence to antiretroviral therapy among HIV-infected children attending Hiwot Fana and Dil-Chora art clinic at referral hospitals in Eastern Ethiopia. J HIV Clin Sci Res. 2015;14(008).
6. Gultie T, Sebsibie G. Factors affecting adherence to pediatrics antiretroviral therapy in Mekelle Hospital, Tigray Ethiopia. Int J Public Health. 2015;4(1):1–6.
7. Endalamaw A, Tezera N, Eshetie S, Ambachew S, Habtewold TD. Adherence to highly active antiretroviral therapy among children in Ethiopia: a systematic review and meta-analysis. AIDS Behav. 2018;22(8):2513–2523. doi:10.1007/s10461-018-2152-z
8. Feyissa A. Magnitude and associated factors of non-adherence to highly active antiretroviral therapy among children in Fiche Hospital, North Shewa, Ethiopia 2016. J Pharm Care Health Syst. 2017;4(1).
9. Smith C, Gengiah TN, Yende-Zuma N, Upfold M, Naidoo K. Assessing adherence to antiretroviral therapy in a rural paediatric cohort in KwaZulu-Natal, South Africa. AIDS Behav. 2016;20(11):2729–2738. doi:10.1007/s10461-016-1419-5
10. Haberer J, Kiwanuka J, Nansera D, Ragland K, Mellins C. Multiple measures reveal antiretroviral adherence successes and challenges in HIV-infected Ugandan children. PLoS One. 2012;7(5):e36737. doi:10.1371/journal.pone.0036737
11. Polisset J, Ametonou F, Arrive E, Aho A, Perez F. Correlates of adherence to antiretroviral therapy in HIV-infected children in Lome, Togo, West Africa. AIDS Behav. 2009;13(1):23–32. doi:10.1007/s10461-008-9437-6
12. Kang E, Delzell DA, Chhabra M, Oberdorfer P. Factors associated with high rates of antiretroviral medication adherence among youth living with perinatal HIV in Thailand. Int J STD AIDS. 2015;26(8):534–541. doi:10.1177/0956462414545524
13. Seth A, Gupta R, Chandra J, Maheshwari A, Kumar P, Aneja S. Adherence to antiretroviral therapy and its determinants in children with HIV infection–experience from Paediatric Centre of Excellence in HIV Care in North India. AIDS Care. 2014;26(7):865–871. doi:10.1080/09540121.2013.859649
14. Biressaw S, Abegaz WE, Abebe M, Taye WA, Belay M. Adherence to antiretroviral therapy and associated factors among HIV infected children in Ethiopia: unannounced home-based pill count versus caregivers’ report. BMC Pediatr. 2013;13(1):132. doi:10.1186/1471-2431-13-132
15. Tadios Y, Davey G. Antiretroviral treatment adherence and its correlates in Addis Ababa, Ethiopia. Ethiop Med J. 2006;44(3):237–244.
16. Azmeraw D, Wasie B. Factors associated with adherence to highly active antiretroviral therapy among children in two referral hospitals, northwest Ethiopia. Ethiop Med J. 2012;50(2):115–124.
17. Biadgilign S, Deribew A, Amberbir A, Deribe K. Adherence to highly active antiretroviral therapy and its correlates among HIV infected pediatric patients in Ethiopia. BMC Pediatr. 2008;8(1):53. doi:10.1186/1471-2431-8-53
18. Xu L, Munir K, Kanabkaew C, Le Coeur S, Thorne C. Factors influencing antiretroviral treatment suboptimal adherence among perinatally HIV-infected adolescents in Thailand. PLoS One. 2017;12(2):e0172392. doi:10.1371/journal.pone.0172392
19. Malcolm S, Ng J, Rosen R, Stone V. An examination of HIV/AIDS patients who have excellent adherence to HAART. AIDS Care. 2003;15(2):251–261. doi:10.1080/0954012031000068399
20. Spire B, Duran S, Souville M, Leport C, Raffi F, Moatti J-P. Adherence to highly active antiretroviral therapies (HAART) in HIV-infected patients: from a predictive to a dynamic approach. Soc Sci Med. 2002;54(10):1481–1496. doi:10.1016/S0277-9536(01)00125-3
21. World Health Organization. From access to adherence: the challenges of antiretroviral treatment: studies from Botswana, Tanzania and Uganda. In: From Access to Adherence: The Challenges of Antiretroviral Treatment: Studies from Botswana, Tanzania and Uganda. World Health Organization; 2006.
22. Carrieri P, Cailleton V, Le VM, et al. The dynamic of adherence to highly active antiretroviral therapy: results from the French National APROCO cohort. J Acquir Immune Defic Syndr. 2001;28(3):232–239. doi:10.1097/00042560-200111010-00005
23. Nieuwkerk PT, Sprangers MA, Burger DM, et al. Limited patient adherence to highly active antiretroviral therapy for HIV-1 infection in an observational cohort study. Arch Intern Med. 2001;161(16):1962–1968. doi:10.1001/archinte.161.16.1962
24. PEPFAR Ethiopia. Country/Regional Operational Plan (COP/ROP) 2017: strategic direction summary. Ethiopia. 2017.
25. World Health Organization. Antiretroviral Therapy (ART) Coverage Among All Age Groups. Sweizerland: Genieva; 2017.
26. Martin S, Elliott-DeSorbo DK, Wolters PL, et al. Patient, caregiver and regimen characteristics associated with adherence to highly active antiretroviral therapy among HIV-infected children and adolescents. Pediatr Infect Dis J. 2007;26(1):61–67. doi:10.1097/01.inf.0000250625.80340.48
27. Prendergast A, Tudor-Williams G, Jeena P, Burchett S, Goulder P. International perspectives, progress, and future challenges of paediatric HIV infection. Lancet. 2007;370(9581):68–80. doi:10.1016/S0140-6736(07)61051-4
28. Nischal KC, Khopkar U, Saple DG. Improving adherence to antiretroviral therapy. Indian J DermatolVenereolLeprol. 2005;71(5):316–320.
29. Memirie ST. Clinical outcome of children on HAART at police referral hospital, Addis Ababa, Ethiopia. Ethiop Med J. 2009;47(2):159–164.
30. Mea K, Buck WC, Wanless SR. Mortality and clinical outcomes in HIV-infected children on antiretroviral therapy in Malawi, Lesotho, and Swaziland. Pediatrics. 2012;130(3):591–599. doi:10.1542/peds.2011-1187
31. Vreeman RC, Nyandiko WM, Ayaya SO, Walumbe EG, Marrero DG, Inui TS. The perceived impact of disclosure of pediatric HIV status on pediatric antiretroviral therapy adherence, child well-being, and social relationships in a resource-limited setting. AIDS Patient Care STDS. 2010;24(10):639–649. doi:10.1089/apc.2010.0079
32. Paterson DL, Swindells S, Mohr J, et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med. 2000;133(1):21–30. doi:10.7326/0003-4819-133-1-200007040-00004
33. Harries AD, Gomani P, Teck R, et al. Monitoring the response to antiretroviral therapy in resource-poor settings: the Malawi model. Trans R Soc Trop Med Hyg. 2004;98(12):695–701. doi:10.1016/j.trstmh.2004.05.002
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.