Back to Journals » Infection and Drug Resistance » Volume 19
Addressing Antimicrobial Resistance: A Point Prevalence Survey Using AWaRe Indicators from Outpatient Settings of Multan, Pakistan
Authors Alam M, Rasool MF ![]() , Haseeb A
, Haseeb A ![]() , Altowayan WM
, Altowayan WM ![]() , Alqasoumi A, Khakwani M, Saleem Z
, Alqasoumi A, Khakwani M, Saleem Z
Received 23 January 2026
Accepted for publication 12 May 2026
Published 28 May 2026 Volume 2026:19 592798
DOI https://doi.org/10.2147/IDR.S592798
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Muniba Alam,1 Muhammad Fawad Rasool,1 Abdul Haseeb,2 Waleed Mohammad Altowayan,3 Abdulmajeed Alqasoumi,3 Mehnaz Khakwani,4 Zikria Saleem3
1Department of Pharmacy Practice, Faculty of Pharmacy, Bahauddin Zakariya University, Multan, Pakistan; 2Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 3Department of Pharmacy Practice, College of Pharmacy, Qassim University, Qassim, Saudi Arabia; 4Department of Obstetrics and Gynaecology, Nishtar Medical University, Multan, Pakistan
Correspondence: Waleed Mohammad Altowayan, Email [email protected]
Background/Objective: Antimicrobial resistance (AMR) is an escalating public health concern in low- and middle-income countries (LMICs), including Pakistan, where primary care (PC) settings play a significant role in driving inappropriate antibiotic use. This study aimed to evaluate antibiotic prescribing patterns in outpatient departments (OPDs) of hospitals in Multan, Pakistan.
Methodology: Data were collected from the OPDs of two hospitals in Multan during two 4-month periods: September to December 2023 and January to April 2024, using the Global Point Prevalence Survey (GPPS) methodology. The GPPS protocol was followed for data collection, and the WHO AWaRe indicators were applied to determine the appropriateness of antibiotic prescriptions in PC settings.
Results: Of 1208 patients attending OPDs, 409 (33.85%) received at least one antibiotic. A total of 532 antibiotics were prescribed, of which 65.2% belonged to the Access group, with amoxicillin–clavulanic acid being the most frequently prescribed agent. However, only 41 prescriptions (7.7%) were compliant with WHO AWaRe recommendations, indicating a high level of inappropriate prescribing. Antibiotic use was particularly high for respiratory symptoms such as sore throat, cough, and nasal congestion, which are predominantly viral in origin. While Ophthalmology and Dermatology OPDs had the lowest prescribing rates, Pulmonology and Paediatrics OPDs showed the highest.
Conclusion: The study concluded that antibiotic prescribing was frequent in PC OPDs in Multan, with inadequate compliance with WHO AWaRe recommendations, regardless of the excessive use of Access antibiotics. Targeted ASP efforts are necessary to minimize inappropriate antibiotic prescribing.
Plain Language Summary: Antibiotic resistance occurs when bacteria no longer respond to medicines used to treat infections. This has become a serious global health problem, particularly in countries such as Pakistan, where many patients seek treatment in hospital outpatient departments (OPDs). Understanding how antibiotics are prescribed in these settings is important for improving their appropriate use.
This study examined antibiotic prescribing patterns in the OPDs of two hospitals in Multan, Pakistan, between 2023 and 2024. Data were collected on how frequently antibiotics were prescribed, the clinical reasons for prescribing them, and whether the prescriptions followed the World Health Organization (WHO) AWaRe (Access, Watch, Reserve) classification.
The findings showed that about one-third of patients visiting the OPDs received an antibiotic. Most prescribed antibiotics belonged to the WHO “Access” group, which includes medicines recommended for common infections; however, only a small proportion of prescriptions fully complied with WHO guidance. Antibiotics were most frequently prescribed in pediatric and pulmonology clinics, particularly for symptoms such as cough, sore throat, and nasal congestion.
These findings highlight frequent antibiotic use in outpatient settings and indicate opportunities to improve prescribing practices. Strengthening antimicrobial stewardship programs, providing evidence-based guidance, and supporting prescribers through education may help promote more appropriate antibiotic use and reduce the risk of antimicrobial resistance.
Keywords: antimicrobial prescribing patterns, primary care, outpatients, WHO AWaRe classification, antimicrobial stewardship, multi-drug resistance, global point prevalence survey, public health, infectious diseases
Introduction
Antimicrobial resistance (AMR), known as a major global health threat, contributing to increased mortality, morbidity, and considerable economic burden worldwide.1 Along with the necessity to enhance surveillance and the rational use of antibiotics, new infectious diseases are contributing to the global challenge of antimicrobial resistance.2 The World Health Organization (WHO) (2019) predicted that drug-resistant ailments were linked to approximately 1.27 million deaths in the world and were also attributable to 4.95 million deaths.3 The Review on AMR, commissioned by the UK government, warned that resistant infection may be responsible for up to 10 million deaths annually by 2050.4,5 Although some have challenged the forecasts.6,7 The World Health Organisation (WHO) and other groups acknowledge the spread of AMR as a critical issue that requires a global action plan (GAP) to address.8 In our interconnected world, AMR regards no limits, thus affecting all regions and populations. However, low- and middle-income countries (LMICs) are expected to bear approximately 80% of the 10 million AMR-related mortality, owing to the high burden of infectious diseases.9
To counter the increasing menace of AMR, Pakistan has designed the National Action Plan (NAP) in accordance with the WHO GAP and aimed at improving awareness, strengthening surveillance, optimizing the usage of antimicrobials, and amplifying infection prevention and control practices.10 Nonetheless, there are still difficulties connected with its implementation, especially in an outpatient environment where the data related to surveillance is minimal.
However, the limited availability of data on antimicrobial prescribing poses a substantial challenge in taking action, such as developing and implementing an effective antimicrobial stewardship program (ASP) in LMICs. This growing threat is further amplified by the strong connection between AMR and antimicrobial use, notably involving broad-spectrum antibiotics.11,12 Outpatient departments (OPDs), which are foundational to PC and serve as the first line of contact for patients, play an essential role in antimicrobial prescribing practices. They are structured to provide accessible, ongoing, and patient-centered care, as highlighted in the Alma-Ata declaration in support of Universal Health Coverage (UHC), along with Sustainable Development Goals (SDGs).13 A major cause of AMR in the community is the escalating use and misuse of antibiotics, especially broad-spectrum agents.3 As an example, the WHO identifies the excessive use and abuse of antibiotics in human medicine and in agricultural situations as critical factors in the rising occurrence of drug-resistant pathogens.3 Respiratory and other common infections are often treated with empirical therapy in outpatient settings, without sufficient diagnostic investigations, thereby promoting improper antibiotic use.
Antibiotics are frequently prescribed in outpatient settings and contribute to AMR due to high levels of irrational use.9 Pakistan faces a high burden of antibiotic consumption, where irrational prescribing and inadequate infection prevention practices further pose a notable challenge to managing infection and controlling AMR.10,14 As a result, Pakistan has encountered serious public health challenges such as multidrug-resistant (MDR) tuberculosis, outbreaks of extended drug-resistant (XDR) typhoid, and high rates of resistance of isolates producing metallo-beta-lactamase (MBL) and extended-spectrum beta-lactamase (ESBL), with resistance extending to third-generation cephalosporins, and last-resort antibiotics like carbapenem and colistin.15,16
The factors that influence this phenomenon are numerous. In the Pakistani outpatient settings, the variables such as empiric prescribing in the absence of strong diagnostic testing, free access to antibiotics in the absence of prescriptive authority, and lack of patient education would all promote misuse of antimicrobial agents. The WHO specifically emphasizes that improper prescription, over-the-counter (OTC) sale of antibiotics, poor infection prevention and control measures, and use of antimicrobials in agricultural setups all promote antimicrobial resistance in Pakistan.17 Local studies echo these concerns: common contributing factors include injudicious antibiotic use, lack of diagnostics, unregulated pharmacies and self-medication, and gaps in prescriber training.18 More likely, the effect of outpatient clinics and the community pharmacies is that they are significant contributors to the antimicrobial pressure propelling the development of resistance in Pakistan.
Nevertheless, full statistics of the outpatient use of antibiotics continue to be deficient despite the acute state of affairs. To inform the process of stewardship, systematic tracking of prescriptions is a fundamental requirement, but most of the existing point-prevalence studies (PPS) have focused on the patients admitted to hospitals.19 The Global Point Prevalence Survey (Global-PPS) initiative has created a global system of observing antibiotic use in hospitals, and it was recently expanded with an outpatient module in 2023. As far as we know, there is no published prevalence study carried out in Pakistani outpatient departments. This gap is of significant importance: although documented in Pakistan using a previous point prevalence survey, the level of inpatient antibiotic use is exceptionally high (about 70%, it is necessary to extend the surveillance to the outpatient population to achieve a comprehensive view of antibiotic use.
Pakistan can be discussed as a good example that is representative of these worldwide trends. The country demonstrates very high antibiotic prescription rates; one study formally places Pakistan as the third-largest consumer of antibiotics in the context of low- and middle-income countries, despite estimating that about 50% of these prescriptions are unwarranted.20 It was found in an analysis that a single antimicrobial agent was given to at least 67% of the cohort of patients, and surgical prophylaxis was the most common indication, occurring in 40% of those.18 WHO estimates that over 200,000 deaths per year in Pakistan are currently associated with AMR.20 Indeed, Pakistan has faced major AMR crises in recent years: it ranks among the highest-burden countries for multidrug-resistant tuberculosis, and it experienced outbreaks of extensively drug-resistant Salmonella Typhi in 2016 (with ~100% fluoroquinolone resistance). In light of such challenges, OPDs in Pakistan are a significant source of AMR. Factors like insufficient diagnostic skills, weak surveillance systems, cultural beliefs, inappropriate prescribing and dispensing practices, unregulated practices, and patient expectations all of which notably contribute to antimicrobial misuse and resistance.21,22 Antimicrobial resistance concerns are made more challenging due to high rates of infectious diseases in Pakistan, particularly drug-resistant infection outbreaks such as widespread drug-resistant typhoid.23
The WHO reported that Pakistan is fifth in the prevalence of multidrug-resistant Tuberculosis (TB) in the world. Furthermore, the nation still struggles with antimicrobial-resistant pneumococcal disease, which causes the death of around 20,000 children under five years old, with 2 outbreaks of multidrug-resistant Salmonella infections being reported, with full resistance to fluoroquinolones.24 Given the significant role of OPDs in AMR, systematic monitoring of antibiotic use is necessary. Point Prevalence surveys (PPS), for decades, have played an essential role in assessing the use of antibiotics, following the methods designed by the European Centre for Disease Prevention and Control (ECDC), Global-PPS, and the WHO.12
Even though Pakistan has a lot of problems with the use of antibiotics and resistance, most of the data we have comes from hospitals, and there is not much information from OPDs. The recent inclusion of outpatient settings in the Global Point Prevalence Survey presents a significant opportunity to rectify this gap.
Conducting a PPS is an essential activity for an antimicrobial stewardship program to advance improvements in antibiotic prescribing practices. Hundreds of studies worldwide have utilized PPS to assess antibiotic use and resistance in inpatient hospital settings.1,4,5,25–27 However, no PPS studies have yet been conducted in OPDs, as this methodology has only recently been adapted for such contexts by the GPPS. In Pakistan, where inpatient antibiotic use is alarmingly high at around 70%, it is crucial to extend these assessments to outpatient settings to gain a comprehensive understanding of antibiotic practices. The objective of this study is to evaluate current prescribing practices using PPS and to address antimicrobial resistance by identifying quality indicators based on WHO AWaRe criteria from outpatient settings of hospitals in Multan, Pakistan.
Materials and Methods
Study Design: Point Prevalence Survey
The Global-PPS approach was used to conduct a multicenter PPS of antibiotic use in the OPDs of hospitals in Pakistan. This standardized Global PPS (GPPS) approach, being a web-based tool, documents and monitors antimicrobial prescribing and resistance at the patient level in various health institutions globally, providing quantifiable measures for implementing ASP.
Study Settings: OPDs of Hospitals
The first PPS study in the OPDs of Pakistan was conducted in Multan, Punjab. The study focused on Punjab, Pakistan’s most populous province. The hospitals chose to join voluntarily. The survey includes two hospitals in Multan, Punjab, providing a comprehensive picture of current antibiotic prescribing patterns in OPDs.
Data Collection Tool
Standardized paper data-collection forms were used at the patient level. The GPPS Outpatient data form for Year 2023 (April version) was used to collect the data. The outpatient data collection form consists of 3 different parts. The first part was the Unit form. One form was to be filled out for each unique unit or room included in the survey. The unit form included the date of survey, the persons completing the form, the name of the institution, the name of the unit, the type of specialty (outpatient unit), the total number of prescribers present in the unit/room during the timeslot of the survey, and timeslot data gathering on the day of the study. The other part of the form consists of the Outpatient Form. This form needs to be filled out for every outpatient who visited the outpatient department and was not admitted to the hospital for more than 24 hours, or who slept overnight within the survey timeslot.
The outpatient form consisted of the unit’s name, the room within the unit, survey number, patient age group, gender, and presenting symptoms. The third part of the form is to be filled in only if an antibiotic was prescribed to the patient during that timeslot. This form included: detailed patient age, current patient weight, weight at the time of birth, either the antibiotic was prescribed on the basis, whereas 191 were inappropriate, and 300 indications lacked enquired about the comorbidity of the patient, and information about the antibiotic ie, generic name of the antimicrobial agent, prescription/course (ongoing or new), single unit dose of the antimicrobial, unit of antimicrobial (g, mg, IU etc), doses/day, route (Oral, IM, IV), Prescribed/intended duration of therapy (N days/Unknown), Clinical diagnosis, Indication type, local guidelines exist for diagnosis (Yes, No, not indicated, unknown), were drugs prescribed according to guidelines, is the dosing of medication according to guidelines (yes, no, not indicated, unknown), is the duration of drug prescribed according to guidelines (yes, no, unknown, not indicated).
Inclusion and Exclusion Criteria
All outpatients seen by the physician during the time slot defined in the PPS protocol were included. Patients who were not admitted to the hospital as inpatients and did not need an overnight admission or hospital stay were termed outpatients. Such patients are seen by the consultant or medical officers, either by appointment or without one. Patients undergoing consultation after a minimum monitoring duration or occupying a bed or seat following the surveillance period and awaiting transfer to an inpatient ward were excluded.
Variables
Objectives
- Percentage of prescribed antibiotics belonging to Access, Watch, or Reserve classification (AWaRe).
- Frequency of prescriptions with an inappropriate pattern of antibiotic prescribing.
- Prevalence of adherence with prescribing standards of AWaRe guidelines.
Exposures
- Prescribing pattern of antibiotics in outpatient settings.
- Categorization of antibiotics prescriptions according to AWaRe classification.
Potential Confounders
- Socioeconomic profile of the patients
- Access to diagnostic tools
- Influence of season on infection prevalence
- Workload of the prescriber
Effect Modifiers
- Co-morbidities of the patient
- Different age groups
- Sort of outpatient settings
- Extent of prescribers’ knowledge on AWaRe indicators
Denominator Data and Numerator Data
Denominator data is gathered at the patient level, with a minimal set of information obtained for each consultation or visit during the survey period. Detailed patient and antimicrobial usage information is gathered for antimicrobial-treated patients (numerator). 191 were inappropriate, microbials, including antibacterials for systemic use (J01), anti-mycotics and antifungals for systemic use (J02 & D01BA), anti-tuberculosis drugs (J04A), intestinal anti-infective antibiotics (A07AA), anti-protozoal used as antibacterial agents, nitro-imidazole derivatives (P01AB), antivirals for systemic use (J05), anti-malarials (P01B). Topical antibiotics are excluded from the survey.
Data Collection Procedure
A multidisciplinary team was assembled, including physicians, pharmacists, and residents who were familiar with patient notes and had sufficient knowledge of patient guidelines. The process of obtaining approval from the institution’s ethical review boards and forming a multidisciplinary team for data collection in the outpatient department took approximately 3 months. Hence, the data collection time frames for both hospitals are separate. Data were collected within predefined time frames: September–December 2023 (hospital A) and January–April 2024 (hospital B). Department-wise prescribing of antibiotics: of the 199 patients visiting the Ear, Nose, and Throat outpatient department (Table 1), only 80 (40.2%) were prescribed antibiotics for at least 4 hours. The approximate starting hour was 9:00 a.m., without minutes, and the ending time was 1:00 p.m., whereas in most OPDs, where prescribers arrived after 9:00 a.m., the starting time was 10:00 a.m. and the ending time was 2 p.m. When the physician was available in the OPD, the physicians collaborated to read the prescriptions and complete the outpatient data collection form. One OPD was covered on one day, as per the feasibility of the collaborators and OPD staff.
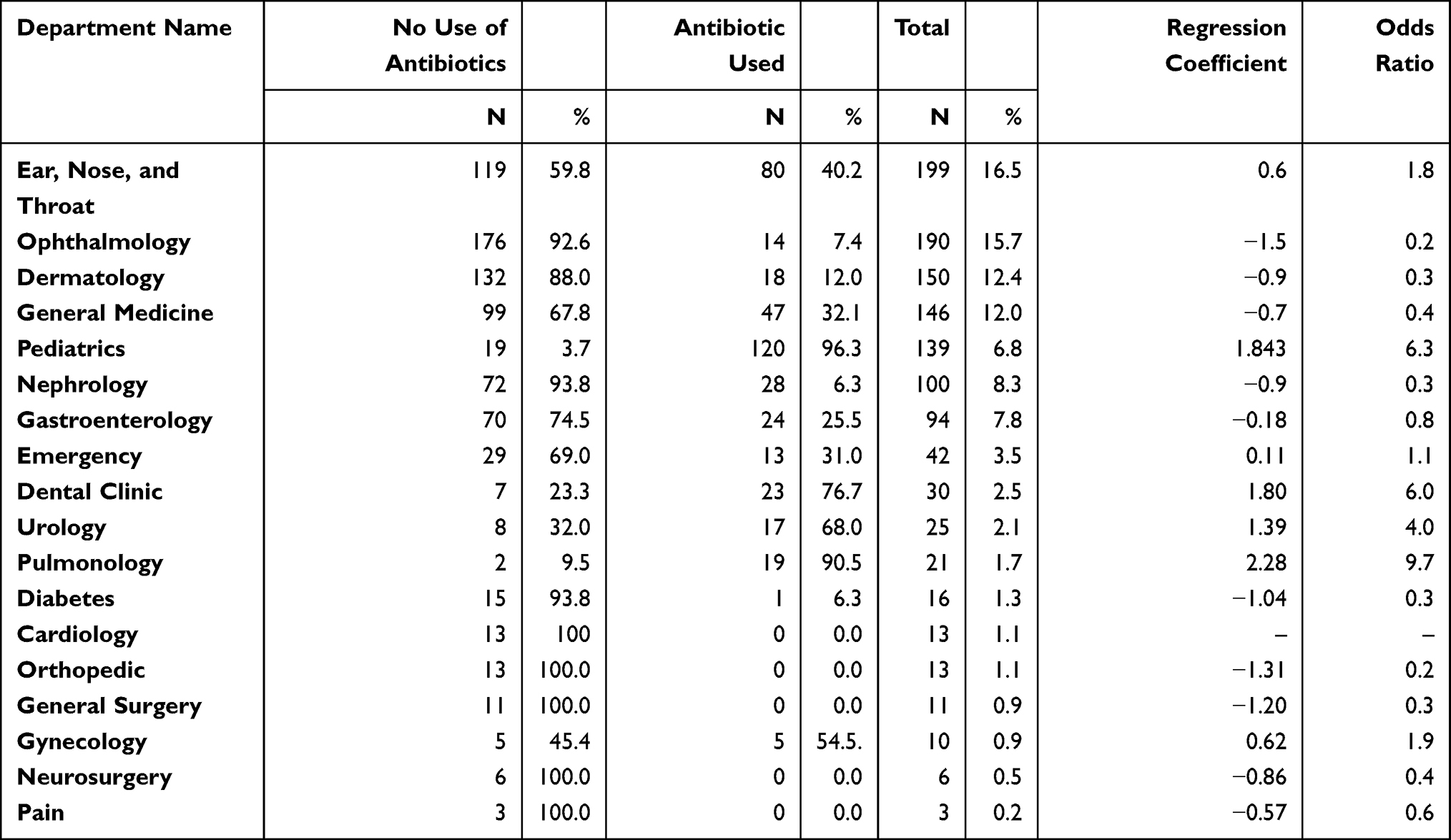 |
Table 1 Antibiotic Use and Prescribing Pattern Across Outpatient Departments |
Statistical Analysis
Data were entered into the GPPS site. Upon completion of data entry, the results were downloaded from the form as Excel files. For analysis, the data were imported into IBM SPSS Statistics version 25. Multivariable logistic regression analysis was conducted to identify factors associated with antibiotic prescribing. The dependent variable was antibiotic prescribing (yes/no), and the independent variables included demographic characteristics (age group and gender), presenting clinical symptoms, and outpatient department. Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were reported. A p-value of less than 0.05 was considered statistically significant. Adjustment for hospital-level and seasonal variation was not performed in the regression analysis.
Results
A total of 1208 patients were included in the study, of whom 409 (33.85%) received at least one antibiotic. Overall, 532 antibiotic prescriptions were recorded. Appropriateness assessment was performed at the prescription level, of which 41 prescriptions (7.7%) were compliant with WHO AWaRe recommendations.
Antibiotic Use Prevalence
A total of 2 hospitals were surveyed in the point prevalence study conducted in South Punjab, Pakistan. Basic patient data from both hospitals treated with antibiotics is presented in Table 2 (Quality Indicators of antibiotic use). Hospital A had 817 patients who visited the outpatient department during the survey period, whereas hospital B had 391; thus, a total of 1208 patients are included in this survey. Of 1208 patients, 409 were prescribed antibiotics, for a prevalence rate of 33.85%. Total antibiotic course use is 532 (39.9%), with an average of 1.3 antibiotics per patient. Of 532 antibiotics, 347 were in the Access group, 182 were in the Watch group, and three were not classified into any group. Of the total antibiotics prescribed, 519 (97.6%) were prescribed for the oral department. At the same time, only 13 (2.4%) of the antibiotics were included as ongoing antibiotic therapies, and 519 (97.6%). Only 41 of the indications were prescribed antibiotics according to the AWaRe guidelines, whereas 191 were inappropriate, and 300 indications had no appropriate diagnosis data related to antibiotic prescribing.
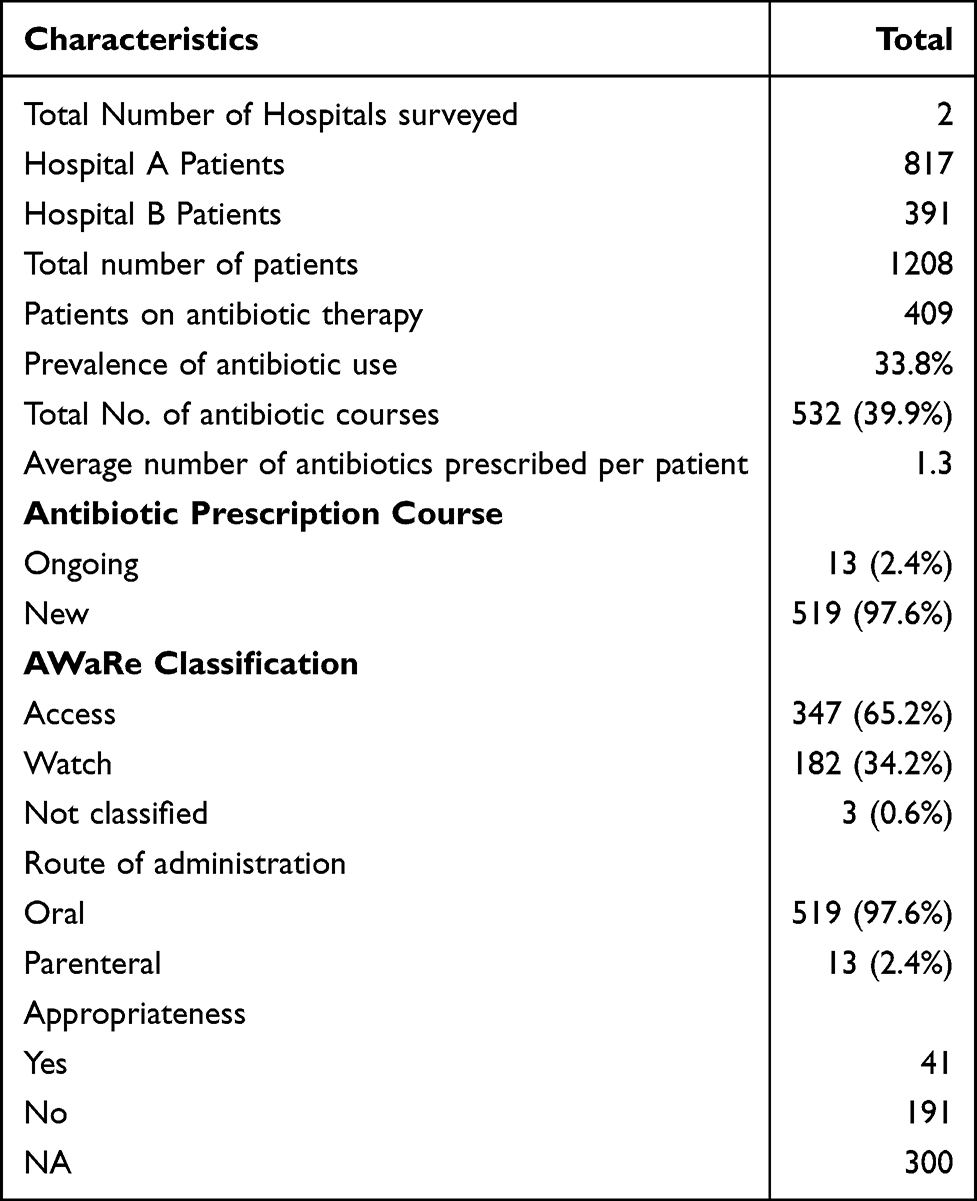 |
Table 2 Quality Indicators of Antibiotic Use |
Patterns and Determinants of Antimicrobial Prescribing in OPDs
Antibiotic use was more prevalent among females (190 [30.7%]) visiting the OPD, as mentioned in Table 3 (Antimicrobial prescription rate by gender, age group, and clinical symptoms), whereas only 141 (27.8%) male patients were prescribed antibiotics. Among all patients visiting the OPDs of both hospitals, adults comprised the majority (75%). Out of these, only 257 (28.3%) adults were prescribed antibiotics. Antibiotics were prescribed more frequently to children than to adults; among children, who comprised 24.7% of the population, 51% received antibiotic prescriptions. Among all clinical symptoms, the most common indications for antibiotic use were sore throat (151, 95.57%), cough (146, 79.35%), and nasal congestion (132, 87.42%). Minimal antibiotics were prescribed for symptoms such as diarrhea with blood (only one patient visited OPD with this indication and was prescribed an antibiotic), temperature/sub-febrile (out of two patients visiting OPD, one received an antibiotic), and ear pain (7/15.91% of patients received antibiotics).
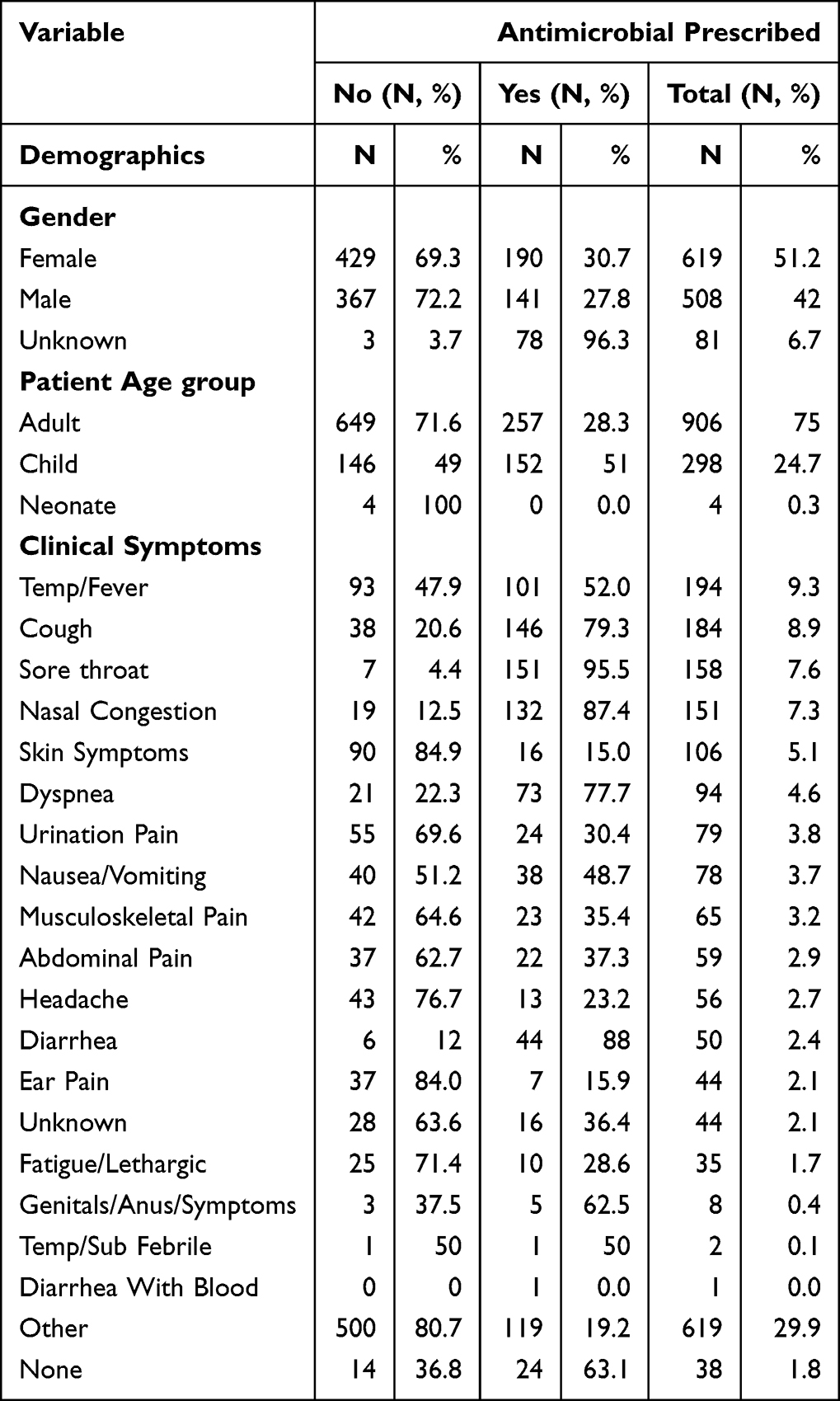 |
Table 3 Antimicrobial Prescription Rate by Gender, Age Group, and Clinical Symptoms |
Factors Associated with Antibiotic Prescribing: Multivariable Logistic Regression Analysis
Multivariable logistic regression analysis highlighted several symptoms significantly associated with antibiotic prescribing (Table 4). Respiratory symptoms, including cough (OR 0.33, 95% CI 0.19–0.58, p < 0.001), sore throat (OR 0.03, 95% CI 0.01–0.07, p < 0.001), and nasal congestion (OR 0.34, 95% CI 0.17–0.66, p = 0.002), were associated with markedly lower odds of antibiotic prescribing following adjustment. Similarly, diarrhea (OR 0.04, 95% CI 0.02–0.11, p < 0.001) and genital/anal symptoms (OR 0.09, 95% CI 0.02–0.42, p = 0.002) were also associated with reduced likelihood of use of antibiotics.
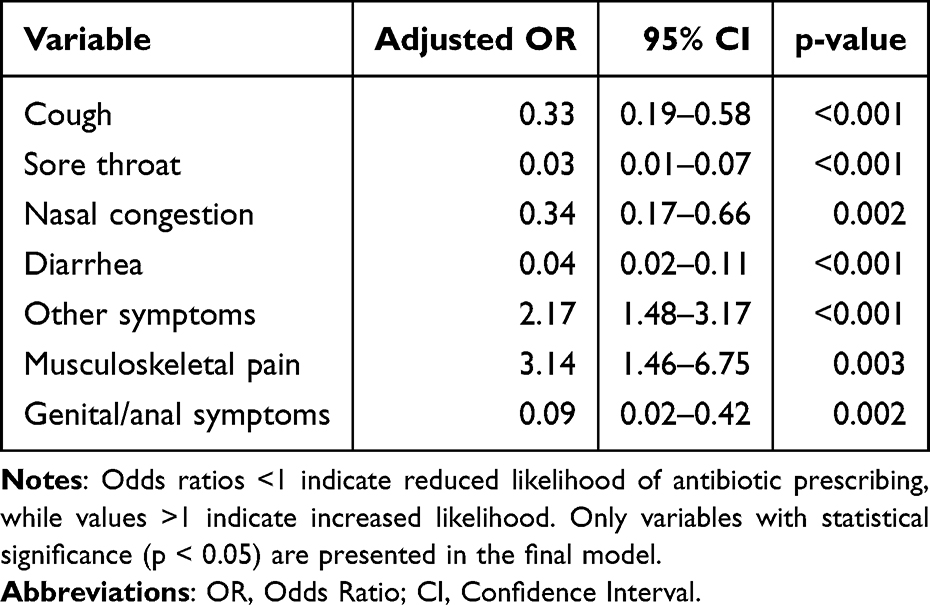 |
Table 4 Multivariable Logistic Regression Analysis of Factors Associated with Antibiotic Prescribing |
In contrast, musculoskeletal pain (OR 3.14, 95% CI 1.46–6.75, p = 0.003) and other symptoms (OR 2.17, 95% CI 1.48–3.17, p < 0.001) were associated with increased odds of antibiotic prescribing. This apparent discrepancy between high crude prescribing rates and lower adjusted odds indicates the necessity of multivariable analysis, showing that respiratory symptoms may not independently drive antibiotic prescribing when other clinical factors are considered. Others, including clinician judgement, perceived severity of illness, patient expectations, and diagnostic uncertainty, are likely to influence prescribing decisions in outpatient settings. The category of “other symptoms should be viewed with caution, because it is a heterogeneous group of clinical presentations. The regression model did not include adjustment for hospital site or data collection period.
Antibiotic Consumption and Practice of Prescription in the Different Outpatient Settings of Hospitals
Upon reviewing the department-wise prescribing of antibiotics, it was observed that, among 199 patients visiting the Ear, Nose, and Throat outpatient department, as demonstrated in Table 1 (Antibiotic use and prescribing pattern across outpatient departments), only 80 (40.2%) were prescribed antibiotics, with a coefficient of 0.62 and an odds ratio of 1.85. One hundred ninety patients presented to the Ophthalmology OPD, and 14 (7.4%) were prescribed antibiotics. In the general medicine OPD, 47 (32.1%) of 146 patients were prescribed antibiotics. In the pediatrics department, 120 of 139 patients (96.3%) were prescribed antibiotics. Whereas in cardiology, OPD (13), Orthopedics (13), General surgery (11), Neurosurgery (6), and pain patients visited the OPD on that day, none of them were prescribed antibiotics. Compared with ophthalmology (−1.50;0.22) and dermatology (−0.97;0.38), departments such as pulmonology and pediatrics show a positive coefficient with a high odds ratio, indicating a strong trend toward antibiotic prescribing. In the ear, nose, and throat (ENT) department, the prescribing rate was 40.2%, with a moderate coefficient of −0.62 and an odds ratio of 1.85, indicating that antibiotics are commonly prescribed. Still, the likelihood is lower than in departments like Pediatrics or Pulmonology. Meanwhile, the emergency and general medicine departments showed 31.4% and 32.1%, with 0.11 and −0.75 coefficients, indicating balanced antibiotic prescribing.
Prevalence by Indications
The majority of patients were prescribed antibiotics for community-acquired infections rather than for medical or surgical prophylaxis; the unknown cases are shown in Table 5 (Indications and antibiotics). For community-acquired infections, amongst all the antibiotics prescribed, Amoxicillin and beta-lactamase was most commonly prescribed, 125 (64.1), whereas Sulphamethoxazole-trimethoprim was the second most prescribed antibiotic, 38 (59.4).
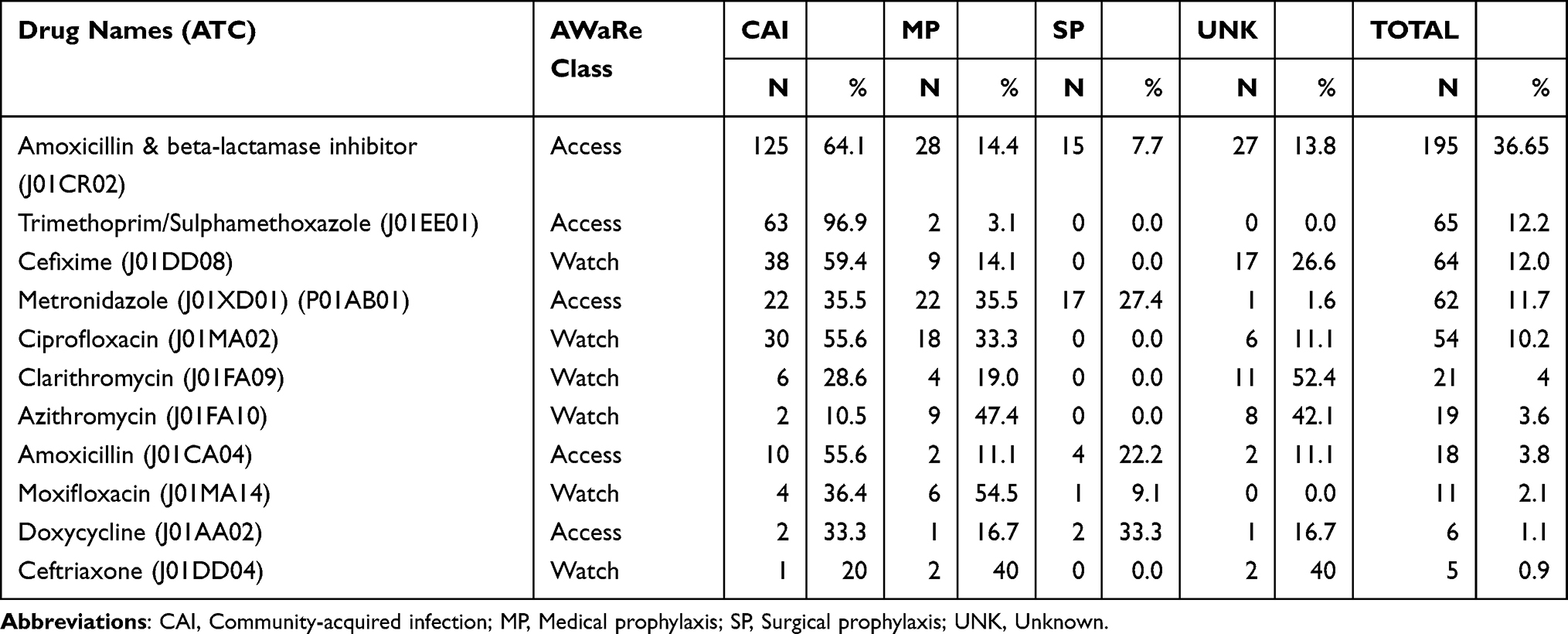 |
Table 5 Indications and Antibiotics |
Amoxicillin and a beta-lactamase inhibitor accounted for the majority of medical prophylaxis (28 [14.4]), followed by metronidazole (22 [35.5]). For surgical prophylaxis, Metronidazole was the most commonly prescribed antibiotic, 17 (27.4), and amoxicillin and beta lactamase were on the second priority, 15 (7.7) whereas in case of unknown indication, amoxicillin and beta-lactamase were accounted for preferably, 27 (13.8%), and clarithromycin,11 (52.4%), was the second most commonly antibiotic prescribed.
Discussion
Antimicrobial resistance is a global concern, mainly affecting the local hospitals and communities. Surveillance of antibiotic use is essential for rationalizing antibiotic prescribing, controlling the emergence of multidrug-resistant microorganisms, assessing policy efficiency, finding areas for quality improvement, and educating policymakers.28 A point prevalence survey was conducted, for the first time in Multan, Pakistan, assessing antibiotic prescriptions in the PC. The primary goals of this study were to analyze existing trends in antibiotic prescribing practices in hospitals in South Punjab, Pakistan, and to identify specific areas for improving antibiotic prescribing quality.
To date, to the best of our knowledge, no study using the PPS methodology in PC has been conducted worldwide; thus, the results are not comparable to those of any survey. Therefore, we have compared our present study with research studies that adopted methodologies other than PPS. In our study (Table 2), the point prevalence of antibiotic use in 2 hospitals was 33.85%, and the total number of antibiotic courses was 532 (39.9), averaging 1.3 antibiotics per patient. This prevalence is comparable to studies from other LMICs, where outpatient antibiotic usage ranges from 25% to 50% or even greater.29–31 In many countries, like South India, the antibiotic prescribing rate is relatively low, ie, 17.5, reflecting a lower consumption of antibiotics.32
A total of 1208 patients were included in this survey, including data from both hospitals, of whom 409 were prescribed antibiotics in the outpatient departments. There is an over-reliance on these antibiotics, indicating a need for stricter prescribing guidelines and improved stewardship. This pattern aligns with the global concern about the misuse of broad-spectrum antibiotics,33–37 highlighting the necessity for targeted interventions to promote the use of “Access” antibiotics, which are deemed safer and less prone to resistance.
The antibiotics were distributed according to the AWaRe classification, with 65.2% in the “Access” group, 34.2% in the “Watch” group, and 0.6% unclassified. The relatively high percentage of “access” group antibiotics is encouraging, as these are the first-line treatment recommendations. We have found somewhat similar results in a study,38 In patients who encountered “Access” and “watch” antibiotics, the rates were 59% and 39.3%, respectively.
However, our findings are higher than the findings of the study,11,31 where the “Access” and “Watch” groups accounted for 45–52% and 43–51% of all antibiotics prescribed per month, respectively. Similarly, in another study, the access group of antibiotics accounted for the highest proportion of access antibiotics (47.37%) in the prescriptions, followed by the Watch group, which made up to 38.35%, and the unclassified group accounted for 13.53%39 Regarding “Watch” group antibiotics, the prescribing rate is higher among children (66.7%) and adults (42.9%), as compared to our study.40 Nevertheless, the notable use of “Watch” antibiotics, according to our findings, demands better adherence to guidelines and the education of health professionals on the selection of appropriate antibiotics, as “Watch” antibiotics are more likely to promote resistance. All three unclassified antibiotics (0.3%) were prescribed irrationally and should be avoided owing to a lack of efficacy and potential for causing harm to the patients.
Regarding route of administration, the vast majority of antibiotics were given orally (97.6%), whereas just 2.4% were administered parenterally. Somehow similar findings, ie, antibiotics prescribed to be taken orally (75%) and to be administered intravenously (25%), have been presented by a study41 relevant to prescribing trends of antibiotics in upper respiratory tract infections among the OPD of Hospitals. The preference of healthcare professionals (HCPs) for oral administration may reflect the type of infections being treated, patients’ condition, or hospital protocols that prioritize less invasive routes when feasible. The total number of antibiotics prescribed by the oral route was 519 (97.6%), whereas 13 (2.4%) were prescribed for parenteral administration.
According to our findings, the appropriateness of the use of antibiotics, according to “AWaRe” classification, was evaluated and revealed that a highly notable percentage,191 out of 242 (79%) of antibiotics were identified as inappropriate. Only 17% of the antibiotic courses evaluated were appropriate, and 4% were not applicable. Such an alarmingly low appropriateness rate underscores the immediate need to implement an antimicrobial stewardship program (ASP) to ensure the judicious and efficient use of antibiotics.
The data were collected from hospitals that serve both adults and pediatrics, so patients of all ages were included in this study. The distribution of antibiotic prescriptions across age groups is a significant trend. According to our research, across all age groups, adults received a greater proportion of antibiotic prescriptions (57.3%), whereas 42.6% of children visiting the OPD received antibiotics.
Among neonates, 0% had been prescribed an antibiotic. Similar results were found in another study, in which patients with fever received antibiotics.42 According to that, 11.7% of the adults received antibiotics, whereas only 5% of the children were prescribed antibiotics. The alignment of these findings indicates that adults are more likely to present indications warranting antimicrobial use. In contrast, lower prescription rates among neonates may reflect cautious prescribing practices aimed at avoiding potentially harmful side effects.
The high antibiotic prescribing frequency among pediatric patients can be explained by many factors, but this can be a collection of factors, such as diagnosis uncertainty, an increased number of infectious symptoms, and expectations of the caregivers about the use of antibiotics. In resource-constrained outpatient settings, low accessibility to diagnostic instruments can also contribute to empirical prescribing. Also, the administration of AWaRe “Watch” antibiotics to this group is the issue that can lead to the increase of antimicrobial resistance, which means that specific antimicrobial stewardship interventions can be beneficial in the pediatric outpatient setting.
Upper respiratory tract infection (URTI), commonly pharyngitis, amongst all indications studied, was the one with the most of the “access” group antibiotic prescribed, whereas “watch” was mainly found to be prescribed for “other” indications that were either unknown or not mentioned in the list given on GPPS forms (Table 2). These findings need to be interpreted with care, since microbiological confirmation was not available to establish the difference between viral and bacterial etiologies. As cough, sore throat, and nasal congestion are the most typical respiratory symptoms in viral infections, the observed patterns in prescribing could indicate overuse of antibiotics when these are not clinically indicated.
Our study demonstrated an association between presenting symptoms and antibiotic prescribing (Table 3). Symptoms such as sore throat, cough, and nasal congestion showed high rates of antibiotic prescribing (95.57%, 79.35%, and 87.42%, respectively), indicating a strong tendency to prescribe antibiotic for respiratory symptoms. These conditions are predominantly viral in origin and generally do not require antibiotic treatment. Similar findings have been reported in previous studies12,43 where upper respiratory tract infections were identified as a leading indication for antibiotic use. However, multivariable logistic regression analysis (Table 4) revealed that these respiratory symptoms were associated with lower odds of antibiotic prescribing after adjustment. This suggests that prescribing decisions may be influenced by additional clinical or contextual factors beyond presenting symptoms alone.
The most prevalent reason for prescribing antibiotics was URTI, accounting for 62.6% of cases. The regression analysis revealed that specific symptoms, especially respiratory-related symptoms, were not independently associated with increased antibiotic prescribing after adjustment. This indicates that other clinical or contextual factors may influence prescribing decisions.
Departments like Pulmonology, Pediatrics, and Dental demonstrated high rates of antibiotic prescribing, ie, 90.5%, 96.3%, and 76.7%, respectively, as shown in Table 4. This data provides an analysis of antibiotic use, presenting coefficients and odds ratios to evaluate the likelihood of antibiotic prescribing in the specified departments.
The high rate of antibiotic prescription in these departments is attributed to the nature and types of conditions being treated, which involve infections that require antibiotic therapy. Whereas departments like ophthalmology (7.4%) and dermatology exhibited lower rates of antibiotic use, demonstrating judicious antibiotic use. No such data are available to date regarding the association between OPDs and antimicrobial prescribing. According to another study, a high antibiotic prescribing rate was observed in the ENT and surgical OPD, ie, 36.8% and 36%, respectively.44
The most commonly prescribed antibiotic in the hospitals’ OPDs surveyed is amoxicillin with a beta-lactamase inhibitor, accounting for 36.65% of all antibiotic prescriptions. Amoxicillin and beta-lactamase inhibitors are predominantly used for community-acquired infections (CAP) (64.1%) and medical prophylaxis (14.4%) of the total prescriptions in this category. Such common prescribing practice of amoxicillin and beta-lactamase inhibitor indicates its broad-spectrum efficacy and frequent empirical use for the treatment of initial infections. A study45 highlights the use of amoxicillin and a beta-lactamase inhibitor in outpatient therapy and also addresses the challenges posed by antibiotic resistance and the need for appropriate dosing. According to another study, a systematic review, amoxicillin combined with clavulanic acid is the most commonly prescribed antibiotic (50–60%) of the prescriptions, primarily for respiratory tract infections.46
The second most common drug prescribed in the outpatient departments was trimethoprim/Sulphamethoxazole, accounting for 12.22% of total prescriptions, mainly for CAP (96.9%) across all other categories, reflecting its effectiveness in treating various infections. Another study has indicated the sensitivity of trimethoprim/Sulphamethoxazole.47 Cefixime was the third most common antibiotic prescribed overall, mainly for CAP (59.4%). Frequent prescribing of amoxicillin and beta-lactamase inhibitor, trimethoprim/Sulphamethoxazole, and Cefixime reflects the importance of empirical therapy in the management of bacterial infections and underscores the need for continuous monitoring of antibiotic use to prevent the development of resistance.
Our study also shows seasonal changes in antibiotic prescribing, with a higher rate during a specific period of the year. Such a pattern is most likely linked to the seasonal incidence of respiratory tract infections, which prompt antibiotic use. Indeed, it’s exciting to consider the implications of our findings for future PC practice.
The implications for the future, as per the findings of our study, include strengthening antimicrobial stewardship programs (ASP), improving surveillance, implementing public awareness campaigns, and implementing interventional policies that may restrict the use of “watch” and “reserve” classes of antibiotics. A high antibiotic prescribing rate for symptoms such as sore throat and cough suggests a greater need for improved diagnostic practices to differentiate between viral and bacterial infections, thereby minimizing unnecessary antibiotic prescribing. Departments with a high rate of antibiotic prescribing may benefit from targeted interventions. Variations in prescribing patterns may be partially explained by hospital differences or seasonal trends.
Limitations
This study has several limitations. First, it is a cross-sectional point prevalence survey and thus fails to measure period-specificity trends or causal associations; it is a measurement of the behaviors of antibiotic prescribing. Second, it is possible that the results would not be as generalizable to other locations or healthcare settings since the study was confined to two hospitals in Multan. Third, in the case of respiratory diseases, there was insufficient microbiological data to determine viral versus bacterial infection, as the data were collected in two different time periods. Excluding the existence of Hawthorne effect becomes unattainable because prescribers might have adapted their practices due to awareness that they were under observation. Also, prescribing appropriateness was determined based on AWaRe indicators and clinical documentation which might be affected by poor or unreliable record-keeping. The regression analysis also did not take into account seasonal or hospital-level changes that might have changed prescribing trends.
Conclusion
This study has shown how antibiotic prescriptions are high in outpatient clinics, a high proportion of Watch antibiotics are used, and poor dose compliance with the WHO AWaRe guidelines. These findings reveal the necessity of specific ASP measures in the outpatient care environment and point to the considerable deficiencies in prescribing quality. When interpreting the results, the limitations of the study, including the cross-sectional nature thereof, the small sample of hospitals, the absence of microbiological confirmation, and the potential seasonal shift, have to be considered. Despite these constraints, the study justifies the implementation of systematic surveillance and stewardship strategies to promote reasonable antibiotic usage and provides valuable baseline data regarding the outpatient practice of antibiotic prescribing.
Abbreviations
AWaRe, Access, Watch, Reserve; AMR, Antimicrobial resistance; LMICs, Lower-middle-income countries; OPDs, Outpatient Departments; GPPS, Global Point Prevalence Survey; GDP, Gross Domestic Product; ASP, Antimicrobial Stewardship Program; AMU, Antimicrobial usage; UHC, Universal Health Coverage; SDGs, Sustainable Development Goals; MDR, multi-drug resistant; XDR, Extended Drug Release; ESBL, Extended-Spectrum beta lactamase (ESBL); PPS, Point Prevalence Surveys; ECDC, European Centre for Disease Prevention and Control (ECDC); WHO, World Health Organization; CAI, Community-acquired infection; MP, Medical Prophylaxis; SP, Surgical Prophylaxis; UNK, Unknown; ENT, Eyes, nose, throat; PCC, Primary Care Practice; g, gram; mg, milligram; IU, International Units; IM, Intra-muscular; IV, Intra-venous.
Data Sharing Statement
Data are available on request from the corresponding author.
Ethical Statement
Ethical approval was obtained from the Human Ethics Approval Committee of the Department of Pharmacy Practice with this reference number 822-EAC-PP-23.
Acknowledgments
The researchers would like to thank the Deanship of Graduate Studies and Scientific Research at Qassim University for financial support (QU-APC-2026).
Funding
The authors declared that financial support was not received to conduct this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Naylor NR, Atun R, Zhu N, et al. Estimating the burden of antimicrobial resistance: a systematic literature review. Antimicrob Resist Infect Control. 2018;7(1):58. doi:10.1186/s13756-018-0336-y
2. Tabish SA. Recent trends in emerging infectious diseases. Int J Health Sci. 2009;3(2):V–14.
3. World Health Organization. Antimicrobial resistance. Available from: https://www.who.int/news-room/fact-sheets/detail/antimicrobial-resistance#:~:text=,income%20countries%20are%20most%20affected.
4. O’Neill J. Tackling drug-resistant infections globally: final report and recommendations. 2016.
5. O’neill J. Antimicrobial resistance: tackling a crisis for the health and wealth of nations. Rev Antimicrob Resist. 2014;2014:1.
6. de Kraker ME, Stewardson AJ, Harbarth S. Will 10 million people die a year due to antimicrobial resistance by 2050? PLoS Med. 2016;13(11):e1002184. doi:10.1371/journal.pmed.1002184
7. NOfA H. NOAH response to final O Neill AMR review report July 2016. 2016. Available from: https://www.thelancet.com/action/showPdf?pii=S0140-6736%2821%2902724-0.
8. Wolrd Health Organization, Programme UUNE, Health WOfA. Implementing the Global Action Plan on Antimicrobial Resistance: First Quadripartite Biennial Report. World Health Organization; 2023.
9. Sulis G, Sayood S, Gandra S. Antimicrobial resistance in low-and middle-income countries: current status and future directions. Exp Rev Anti Infective Ther. 2022;20(2):147–160. doi:10.1080/14787210.2021.1951705
10. Saleem Z, Godman B, Azhar F, et al. Progress on the national action plan of Pakistan on antimicrobial resistance (AMR): a narrative review and the implications. Exp Rev Anti Infective Ther. 2022;20(1):71–93. doi:10.1080/14787210.2021.1935238
11. Hou J, Long X, Wang X, et al. Global trend of antimicrobial resistance in common bacterial pathogens in response to antibiotic consumption. J Hazard Mater. 2023;442:130042. doi:10.1016/j.jhazmat.2022.130042
12. Saleem Z, Hassali MA, Godman B, et al. Point prevalence surveys of antimicrobial use: a systematic review and the implications. Exp Rev Anti Infective Ther. 2020;18(9):897–910. doi:10.1080/14787210.2020.1767593
13. Physicians AAoF. The declaration of Astana and what it means for the global role of NAPCRG and WONCA. Anna Family Med. 2020;2020:1.
14. Alam M, Saleem Z, Haseeb A, et al. Tackling antimicrobial resistance in primary care facilities across Pakistan: current challenges and implications for the future. J Infection Public Health. 2023;16:97–110. doi:10.1016/j.jiph.2023.10.046
15. Qamar FN, Yousafzai MT, Khalid M, et al. Outbreak investigation of ceftriaxone-resistant Salmonella enterica serotype Typhi and its risk factors among the general population in Hyderabad, Pakistan: a matched case-control study. Lancet Infect Dis. 2018;18(12):1368–1376. doi:10.1016/S1473-3099(18)30483-3
16. Latif S, Anwar MS, Ahmad I. Bacterial pathogens responsible for blood stream infection (BSI) and pattern of drug resistance in a tertiary care hospital of Lahore. Biomedica. 2009;25(2):101–105.
17. World Health Organization. Antimicrobial resistance contributes to 200,000 annual deaths in Pakistan; WHO and the NIH call for action.
18. Shaikh Q, Sarfaraz S, Rahim A, et al. WHO point prevalence survey to describe the use of antimicrobials at a tertiary care center in Pakistan: a situation analysis for establishing an antimicrobial stewardship program. Antibiotics. 2022;11(11):1555. doi:10.3390/antibiotics11111555
19. G PPS. Why a Global-PPS? Available from: https://www.global-pps.com/.
20. Khan A. The Silent Threat: how Antimicrobial Resistance is Putting Pakistan’s Health at Risk. 2025. Available from: https://jhpiego.org/our-stories/p/amr-putting-pakistans-health-at-risk/.
21. Godman B, Haque M, McKimm J, et al. Ongoing strategies to improve the management of upper respiratory tract infections and reduce inappropriate antibiotic use particularly among lower and middle-income countries: findings and implications for the future. Curr Med Res Opin. 2020;36(2):301–327. doi:10.1080/03007995.2019.1700947
22. Raheem M, Anwaar S, Aziz Z, Raja SA, Saif-ur-Rehman N, Mubarak N. Adherence to the core elements of outpatient antibiotic stewardship: a cross-sectional survey in the tertiary care hospitals of Punjab, Pakistan. Infect Drug Resist. 2020;Volume 13:3833–3841. doi:10.2147/IDR.S268574
23. Khan M, Khattak MT, Gul A, Riaz M, Tu Zahra F. A comparable risk of extensively drug-resistant typhoid fever in the pediatric cohort during the COVID-19 pandemic. Int J Health Sci. 2024;18(1):24.
24. Mustafa T, Niazi MRK, Lakdawala Z, Mirza S. Regional and national trends in consumption of antimicrobials in Pakistan; pre and post-COVID (2019–2021). Clinl Infect Dis. 2023;77(Supplement_7):S569–S577. doi:10.1093/cid/ciad647
25. Abubakar U, Salman M. Antibiotic use among hospitalized patients in Africa: a systematic review of point prevalence studies. J Racial Ethnic Health Disparit. 2024;11(3):1308–1329. doi:10.1007/s40615-023-01610-9
26. Haseeb A, Saleem Z, Maqadmi AF, et al. Ongoing strategies to improve antimicrobial utilization in hospitals across the Middle East and North Africa (MENA): findings and implications. Antibiotics. 2023;12(5):827. doi:10.3390/antibiotics12050827
27. Saleem Z, Godman B, Cook A, et al. Ongoing efforts to improve antimicrobial utilization in hospitals among African countries and implications for the future. Antibiotics. 2022;11(12):1824. doi:10.3390/antibiotics11121824
28. Saleem Z, Hassali MA, Versporten A, et al. A multicenter point prevalence survey of antibiotic use in Punjab, Pakistan: findings and implications. Exp Rev Anti Infective Ther. 2019;17(4):285–293. doi:10.1080/14787210.2019.1581063
29. Sánchez-Huesca R, Lerma A, Guzmán-Saldaña RM, Lerma C. Prevalence of antibiotics prescription and assessment of prescribed daily dose in outpatients from Mexico City. Antibiotics. 2020;9(1):38. doi:10.3390/antibiotics9010038
30. Nelson RG, Rosowsky A. Dicyclic and tricyclic diaminopyrimidine derivatives as potent inhibitors of Cryptosporidium parvum dihydrofolate reductase: structure-activity and structure-selectivity correlations. Antimicrob Agents Chemother. 2001;45(12):3293–3303. doi:10.1128/AAC.45.12.3293-3303.2001
31. Amponsah OKO, Nagaraja SB, Ayisi-Boateng NK, et al. High levels of outpatient antibiotic prescription at a district hospital in Ghana: results of a cross sectional study. Int J Environ Res Public Health. 2022;19(16):10286. doi:10.3390/ijerph191610286
32. Priyadharsini R, Ramasamy K, Amarendar S. Antibiotic-prescribing pattern in the outpatient departments using the WHO prescribing indicators and AWaRe assessment tool in a tertiary-care hospital in South India. J Fam Med Prim Care. 2022;11(1):74–78. doi:10.4103/jfmpc.jfmpc_527_21
33. Koya SF, Ganesh S, Selvaraj S, Wirtz VJ, Galea S, Rockers PC. Consumption of systemic antibiotics in India in 2019. Lancet Reg Health Southeast Asia. 2022;4:100025. doi:10.1016/j.lansea.2022.100025
34. Zirpe KG, Kapse US, Gurav SK, et al. Impact of an antimicrobial stewardship program on broad spectrum antibiotics consumption in the intensive care setting. Indian J Crit Care Med. 2023;27(10):737. doi:10.5005/jp-journals-10071-24543
35. Gandra S, Kotwani A. Need to improve availability of “access” group antibiotics and reduce the use of “watch” group antibiotics in India for optimum use of antibiotics to contain antimicrobial resistance. J Pharmaceut Policy Pract. 2019;12(1):20. doi:10.1186/s40545-019-0182-1
36. Sharland M, Gandra S, Huttner B, et al. Encouraging AWaRe-ness and discouraging inappropriate antibiotic use—the new 2019 Essential Medicines List becomes a global antibiotic stewardship tool. Lancet Infect Dis. 2019;19(12):1278–1280. doi:10.1016/S1473-3099(19)30532-8
37. Nguyen NV, NTT D, Nguyen CTK, et al. Community-level consumption of antibiotics according to the AWaRe (Access, Watch, Reserve) classification in rural Vietnam. JAC Antimicrob Resist. 2020;2(3):dlaa048. doi:10.1093/jacamr/dlaa048
38. Nguyen NV. Antibiotic Access and Use in the Community and the Feasibility to Implement Pharmacy Targeted Interventions. Open University (United Kingdom); 2023.
39. Mandal P, Asad M, Kayal A, Biswas M. Assessment of use of World Health Organization access, watch, reserve antibiotics and core prescribing indicators in pediatric outpatients in a tertiary care teaching hospital in Eastern India. Perspect Clin Res. 2023;14(2):61–67. doi:10.4103/picr.picr_22_22
40. Alshareef H, Alanazi A, Alatawi N, Eleshmawy N, Ali M. Assessment of antibiotic prescribing patterns at dental and primary health care clinics according to WHO access, watch, Reserve (aware) classification. Am J Infect Control. 2023;51(3):289–294. doi:10.1016/j.ajic.2022.07.009
41. Uttra AA, Mushtaq A, Ansari A, Abbas T, Hussain B. Evaluation of Prescribing Trends of Antibiotics in Upper Respiratory Tract Infections Among OPD in Hospitals of Punjab, Pakistan. 2020.
42. Holloway B, Chandrasekar H, Purohit M, et al. Antibiotic use before, during, and after seeking care for acute febrile illness at a hospital outpatient department: a cross-sectional study from rural India. Antibiotics. 2022;11(5):574. doi:10.3390/antibiotics11050574
43. Lunn AD. Reducing inappropriate antibiotic prescribing in upper respiratory tract infection in a primary care setting in Kolkata, India. BMJ Open Qual. 2018;7(4):e000217. doi:10.1136/bmjoq-2017-000217
44. Shyam S, Jaiswal S, Jayabalan A, Shergill S. A survey of out patient department prescriptions of selected departments of a tertiary care hospital on treatment practices of infections. Muller J Med Sci Res. 2021;12(1):26–32. doi:10.4103/mjmsr.mjmsr_44_20
45. Veeraraghavan B, Bakthavatchalam YD, Sahni RD. Orally administered amoxicillin/clavulanate: current role in outpatient therapy. Infect Dis Ther. 2021;10(1):15–25. doi:10.1007/s40121-020-00374-7
46. Mahmood RK, Gillani SW, Saeed MW, Hafeez MU, Gulam SM. Systematic review: study of the prescribing pattern of antibiotics in outpatients and emergency departments in the Gulf Region. Front Pharmacol. 2020;11:585051. doi:10.3389/fphar.2020.585051
47. Wegdan A, Hefzy E. Prevalence of Methicillin-resistant Staphylococcus aureus in skin and soft tissue infections: single center study. Fayoum Univ Med J. 2023;12(2):103–110. doi:10.21608/fumj.2023.323620
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.